")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Analysis of the Cost and Case-mix of Post-acute Stroke Patients in China Using Quantile Regression and the Decision-tree Models
Authors Zhi M, Hu L, Geng F, Shao N, Liu Y
Received 16 February 2022
Accepted for publication 12 May 2022
Published 20 May 2022 Volume 2022:15 Pages 1113—1127
DOI https://doi.org/10.2147/RMHP.S361385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Mengjia Zhi,1 Linlin Hu,1 Fangli Geng,2 Ningjun Shao,3 Yuanli Liu1
1School of Health Policy and Management, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100710, People’s Republic of China; 2Ph.D. Program in Health Policy, Harvard University Graduate School of Arts and Sciences, Cambridge, MA, USA; 3Jinhua Healthcare Security Administration, Zhejiang, 321000, People’s Republic of China
Correspondence: Linlin Hu; Yuanli Liu, School of Health Policy and Management, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, 100710, People’s Republic of China, Tel/Fax +86 65105830, Email [email protected]; [email protected]
Purpose: Post-acute care is fast developing in China, yet a payment system for post-acute care has not been established. As stroke is the leading cause of mortality and disability in China, patients constitute a large share of post-acute-care patients among all hospitalized patients. This study was to identify the cost determinants and establish a case-mix classification of the post-acute care system for stroke patients in China.
Patients and Methods: A total of 5401 post-acute stroke patients in seven hospitals of Jinhua City from January 2018 to December 2020 were selected. Demographic characteristics, medical status, functional measures (eg, the Barthel Index, Mini-Mental State Examination, Gugging Swallowing Screen, Hamilton Depression Scale), and cost data were extracted. Generalized linear model (GLM) and quantile regression (QR) were conducted to determine the predictors of cost, and a case-mix classification model was established using the decision-tree analysis.
Results: The GLM regression revealed that gender, tracheostomy, complication or comorbidity (CC), activities of daily living (ADL), and cognitive impairment were the main variables significantly affecting the hospitalization expenses of post-acute stroke patients. The QR model showed that the gender, tracheostomy and CC factors had a more significant impact on per diem costs on the upper quantiles. In contrast, cognitive impairment had a more substantial effect on the lower quantiles, and ADL significantly impacted the central quantile. Using tracheostomy, CC, and ADL as node variables of the regression tree, 12 classes were generated. The case-mix classification performed reliably and robustly, as measured by the reduction in the variation statistic (RIV=0.46) and class-specific coefficients of variation (CV less than 1.0; range: 0.18– 0.81).
Conclusion: QR has strengths in comprehensively identifying cost predictors across cost groups. Tracheostomy, CC, and ADL significantly can predict the expenses of post-acute care for stroke patients. The established case-mix classification system can inform the future payment policy of post-acute care in China.
Keywords: cost, case-mix, post-acute care, stroke, quantile regression, decision-tree model
Introduction
Stroke has induced a heavy disease burden worldwide, especially in developing countries.1 Annually, more than 1.9 million people die of stroke, making it the most significant cause of death in China.2 Approximately 70% of stroke survivors are left with varying degrees of speech and physical dysfunction.3 Moreover, stroke is an expensive disease to live with, as stroke care is a long-term process.3 Not only are the expenses in the acute stage of stroke or surgical treatment high, but the long-term costs in the post-acute phase also bring a substantial economic burden to stroke patients, their families, and society.4
As far as recent reform, China’s health insurance payment system is transforming from retrospective to prospective payment.5 Although payment based on diagnosis-related groups (DRG) is utilized for acute care, the prospective payment method for China’s post-acute service system has not been developed yet.6 As delivered in many countries, post-acute care (PAC) is the kind of care aimed to assist recuperation of patients and facilitate independence or transition to continuing care in the community.7 Case-mix is a tool to classify varieties of patient conditions based on resource utilization.8 DRG, the case-mix that has been used as a payment system for acute inpatient services, has been piloted as a three-year project in 30 cities in China since 2019.5 However, DRG for post-acute episodes are not well classified and it is widely accepted that post-acute care requires a different classification measure because various clinical issues, modes of care, and resource use are different from other types of health care.9–12 Instead of being a short episode of care for an operation or acute treatment, post-acute services are time-consuming to maintain or improve the functional status of patients. Therefore, it is crucial to establish a reliable and well-validated case-mix classification system for post-acute care patients, especially those hospitalized for stroke in China, as the demand for post-acute care increases dramatically.
In China, a wealth of studies have spotlighted the costs of short-term hospitalization and early intensive care in the acute phase of stroke3,13–15 under DRG payment policy,4 however, there have been no previous studies exploring the case-mix of post-acute care. Several case-mix systems of post-acute care have been developed worldwide, among which the Resource Utilization Group Version III (RUG-III) is the most widely used.16 RUG-III was a per diem classification system applied in the United States in 1994, which grouped patients into 44 classes and explained 55.5% of the variance in per diem costs, based on the clinical characteristics, special needs, and a nursing dependency level called the Resource Utilization Group-Activities of Daily Living (RUG-ADL) score.17,18 A series of studies have been conducted to evaluate the effectiveness of RUG-III and have revealed various statistical performance levels, explaining 14.1% to 66.5% of the variance in per diem costs.18–22 Even though those international studies have identified several functional and other measures as independent variables for PAC costs, it is vital to study whether the factors identified by international studies will be sound predictors for PAC costs in Chinese settings.
In addition, most studies have used linear regression models to examine predictors of costs.23 However, the linear regression model cannot provide enough information about the underlying associations between costs and its predictors, as it focuses solely on the conditional mean of costs.24 Furthermore, the linear regression model is not robust in the face of statistical outliers and lacks flexibility in analyzing the predictors of costs.23 As cost data always have a skewed distribution, QR analysis is preferably employed because it allows for the study of individuals with extreme (low or high) costs.25
To address those gaps, our study established and validated the first case-mix classification that describes post-acute care for patients hospitalized for stroke. In addition, we investigated the determinants of the PAC costs for stroke through QR analysis. The study results can guide the payment policy for post-acute care in China.
Materials and Methods
Data Collection
In this study, seven hospitals, including three stand-alone rehabilitation hospitals and four rehabilitation units of acute care hospitals in Jinhua City, Zhejiang Province of southeast China, were selected. Post-acute stroke patients (patients with a primary stroke diagnosis and who were treated in rehabilitation or geriatric wards) hospitalized in the seven hospitals were selected from January 1, 2018 to December 31, 2020 with their medical records and functional assessment data extracted. The functional assessment data (BI, MMSE, HDS and GUSS) for each patient were routinely collected by medical staff in these hospitals at the point of admission. With the support of the local Healthcare Security Administration, medical insurance claims data for these patients on the medical cost they incurred were extracted. A flowchart showed the selection of study patients in Figure 1. Patients had to meet the following inclusion criteria to be eligible: with a primary diagnosis of stroke, treated in rehabilitation or geriatric wards, with complete medical cost data and functional assessment data (BI, MMSE, HDS and GUSS) at admission and no data quality issues, ≥18 years of age, alive at the point of discharge, with a length of stay more than three days. The exclusion criteria is: lack of stroke diagnosis, invalid or missing medical cost data or functional assessment data (BI, MMSE, HDS or GUSS) at admission, <18 years of age, with an outcome of death or a length of stay of fewer than three days. Finally, 5401 stroke PAC patients were identified. Permission was obtained from the Medical Ethics Committee of the Chinese Academy of Medical Sciences & Peking Union Medical College to report the data for research purposes (Protocol number: X170315009).
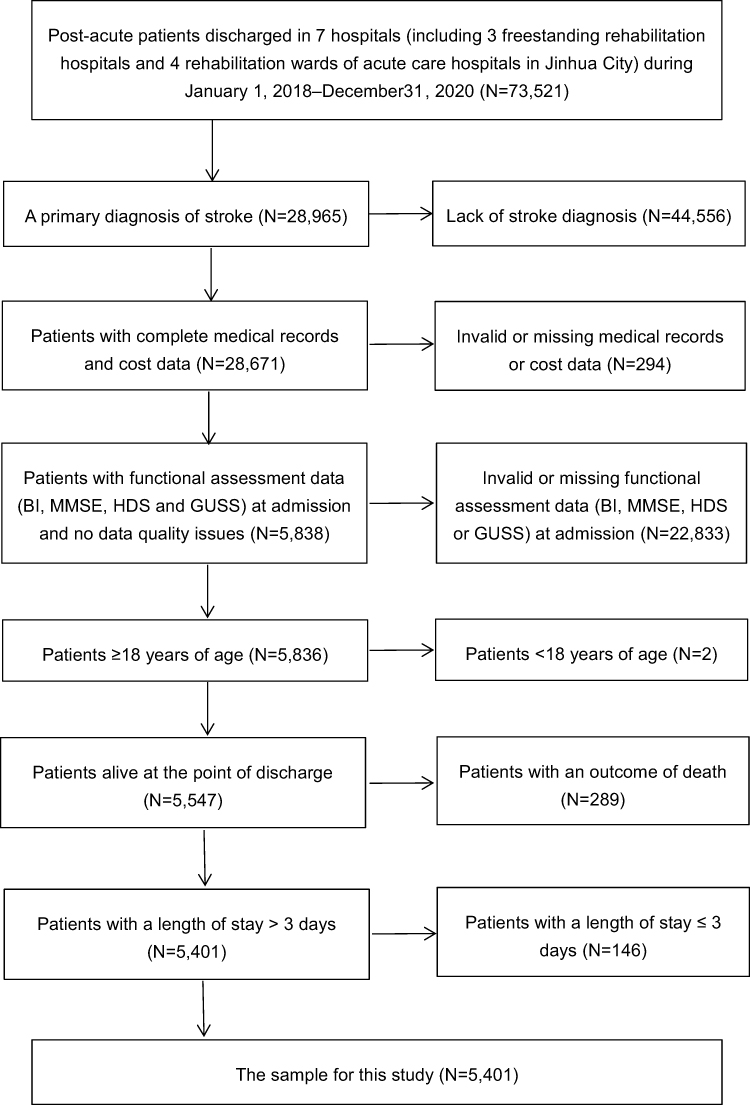 |
Figure 1 Selection of study patients. |
Dependent Variable
The dependent variable was the resource use of the patients, which was measured by total expenses per day in the hospital in this study. Staff time is usually used to reflect resource use under RUG-III.18 However, Acumen’s report proposed that staff time should only be documented during the seven-day look-back window preceding each assessment. The current data need not capture the exact number of minutes provided each day of a stay.26 Moreover, costs should be considered to better reflect differences in the relative resource use across patients.9,10 Therefore, in the present study, the measure of resource use was based on the costs during inpatient stays, which has been generally used in such studies in China.3,15 The expenses included the costs of rehabilitation therapy, nursing, clinical treatment, medications and drugs, laboratory tests and examination, medical equipment and materials, room and board, and others. The Consumer Price Index (CPI) of Jinhua City, published by the National Bureau of Statistics of the People’s Republic of China from 2018 to 2020 was used to revise all cost data and to compare cost data more scientifically. In addition, several studies have concluded that a per diem classification may be suitable for PAC, as the length of stay is not predictable9,10,18 and the Social Security Act in the United States also requires payment be made on a per diem basis.26 Thus, the dependent variable in the present study was the cost per day.
Independent Variables
There were three types of independent variables used to predict cost in this study: (1) patient demographic characteristics, including gender and age; (2) medical status measures: primary diagnosis (according to International Classification of Disease, 10th Edition, Clinical Modification codes), complication or comorbidity (CC), tracheostomy; (3) functional status data, including the Barthel Index (BI), Mini-mental State Examination (MMSE), Gugging Swallowing Screen (GUSS), and Hamilton Depression Scale (HDS). The following are explanations for some of the above measures.
Complication or Comorbidity
A complication refers to a medical condition directly caused by the principal diagnosis and has a causal relationship with the principal diagnosis; comorbidity refers to a medical condition that is not directly related to the principal diagnosis or complication, but has an impact on the resource consumption.27 A major complication or comorbidity (MCC) has a greater impact on resource consumption compared with a complication or comorbidity (CC).27 The official list of CCs and MCCs was published by the National Healthcare Security Administration of the People’s Republic of China in October 2019.
Barthel Index (BI)
Activities of daily living (ADL) is measured by the BI, the most widely used physical function assessment instrument developed by Barthel.28 It consists of 10 items: feeding, grooming, bathing, dressing, toilet use, transfers, walking, climbing stairs, bowel, and bladder control. The total score ranges from 0 (dependent) to 100 (independent). The present study calculated the ADL level using the following mapping: completely dependent (0–20), severely dependent (21–40), moderately dependent (41–60), and independent (61–100).29
Mini-mental State Examination (MMSE)
The MMSE is a widely used instrument designed to screen cognitive impairments, consisting of 30 items in seven domains, including orientation to time, orientation to place, registration, attention, calculation, spontaneous recall, language, and visual construction.30 Scores less than 24 are typically suggestive of cognitive impairment, with the total score ranging from 0 (lowest) to a perfect score of 30 (highest).31
Gugging Swallowing Screen (GUSS)
The swallowing function was assessed by the GUSS, which is presented as a reliable and sensitive screening tool for testing conditions such as swallowing, coughing, drooling, and voice changes.32 The present study considered scores less than 20 as a swallowing disorder, with the perfect score being 20.33
Hamilton Depression Scale (HDS)
The HDS is a measure of depressive symptoms that was developed by Hamilton and includes feelings such as guilt, suicide, sleep, work and interest, mental anxiety, somatic anxiety, gastrointestinal symptoms, weight loss, self-awareness, paranoid symptoms, obsessive–compulsive symptoms, feelings of hopelessness, and inferiority.34 For the 17-item version, scores of HDS can range from 0 to 24, while scores between 18 and 24 indicate depressive symptoms.35
Statistical Analysis
We first conducted a descriptive analysis by calculating the costs on a per diem basis for post-acute stroke inpatients, followed by univariate analysis for patients with different demographic characteristics, clinical features, and functional statuses. We performed the Mann–Whitney U-test and the Kruskal–Wallis H-test to analyze the differences of the per diem costs among the patients with binary and multi-categorical characteristics. Only the characteristics that were found with a statistically significant difference in the costs of daily services were included in the multivariate analysis.
Two models, GLM and QR, were employed. As the cost data were not normally distributed, a generalized linear model (GLM) with a gamma distribution and log-link function was fit to model the regression. QR is a modeling technique that leads to more comprehensive results owing to its ability to assess the effect of each predictor on any part of the costs distribution, whereas a linear regression can model only the conditional mean of the costs.24 To examine the effects of predictors at different points of the distribution of costs, this study used a QR model developed by Aheto.25 The quantile plots of predictor effects on the quantiles of costs in the model permit visual examination of the predictor effects on each quantile.
The key influencing factors of the costs per day in the GLM and QR were taken as classification nodes, and the resource utilization classification model was established by using the growing method of the chi-squared automatic interaction detector (CHAID), and the standard costs per day were calculated.25 The 10-fold cross-validation method was used to trim the decision-tree model automatically. The maximum tree depth was 3, the minimum number of cases in the parent node was 100, the minimum number of cases in the child node was 50, and the test level of the split node was α=0.05. Overall performance of the classification was assessed with the reduction in variance (RIV), the Kruskal–Wallis test for intergroup heterogeneity, and the coefficient of variation (CV) for homogeneity of cases within each group. Relative weight (RW) was the ratio of resource use for each group to the mean cost for all patients. Statistical analyses were conducted with IBM SPSS version 26; the statistical significance level was p<0.05.
Results
For the 5401 patients, the average cost per day was 567.33±384.42 RMB (89.51±60.648 USD), and the average length of stay was 19.44 days (Table 1). More males (58.7%) than females (41.3%) were included in this study, with an average age of 66.96 years old for all patients. There were 195 (3.6%) stroke patients with tracheostomy for hospital care, 1893 (35.0%) with CC, 1802 (33.4%) with MCC, 564 (10.4%) who were moderately dependent on ADL, 1026 (19.0%) who were severely dependent on ADL, 334 (6.2%) who were completely dependent on ADL, 1699 (31.5%) who had cognitive impairment, 1536 (28.4%) who had swallowing disorder, and 137 (2.5%) who had depressive symptoms. The per diem cost of the PAC stroke inpatients with different demographic information, clinical characteristics, and functional status are presented in Table 2. There were statistically significant differences (p<0.05) in the costs per day among the inpatients of a different gender, age, tracheostomy status, CC, ADL, cognitive impairment, swallowing disorder, and depressive symptoms.
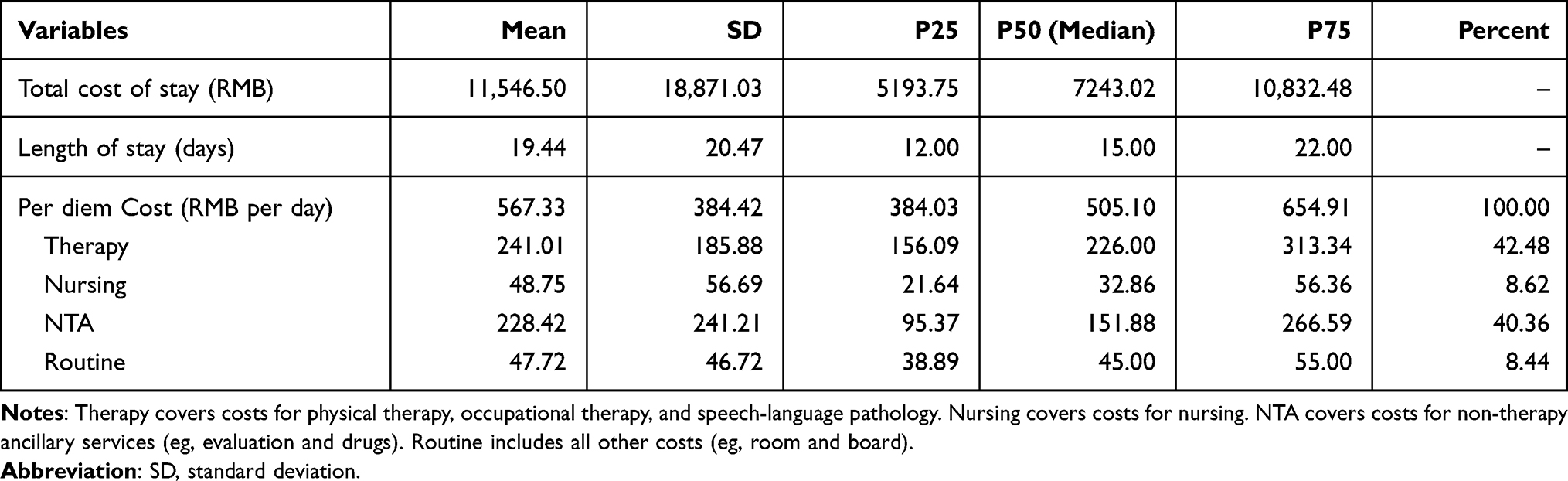 |
Table 1 Description of Cost and Length of Stay for PAC Stroke Inpatients (N=5401) |
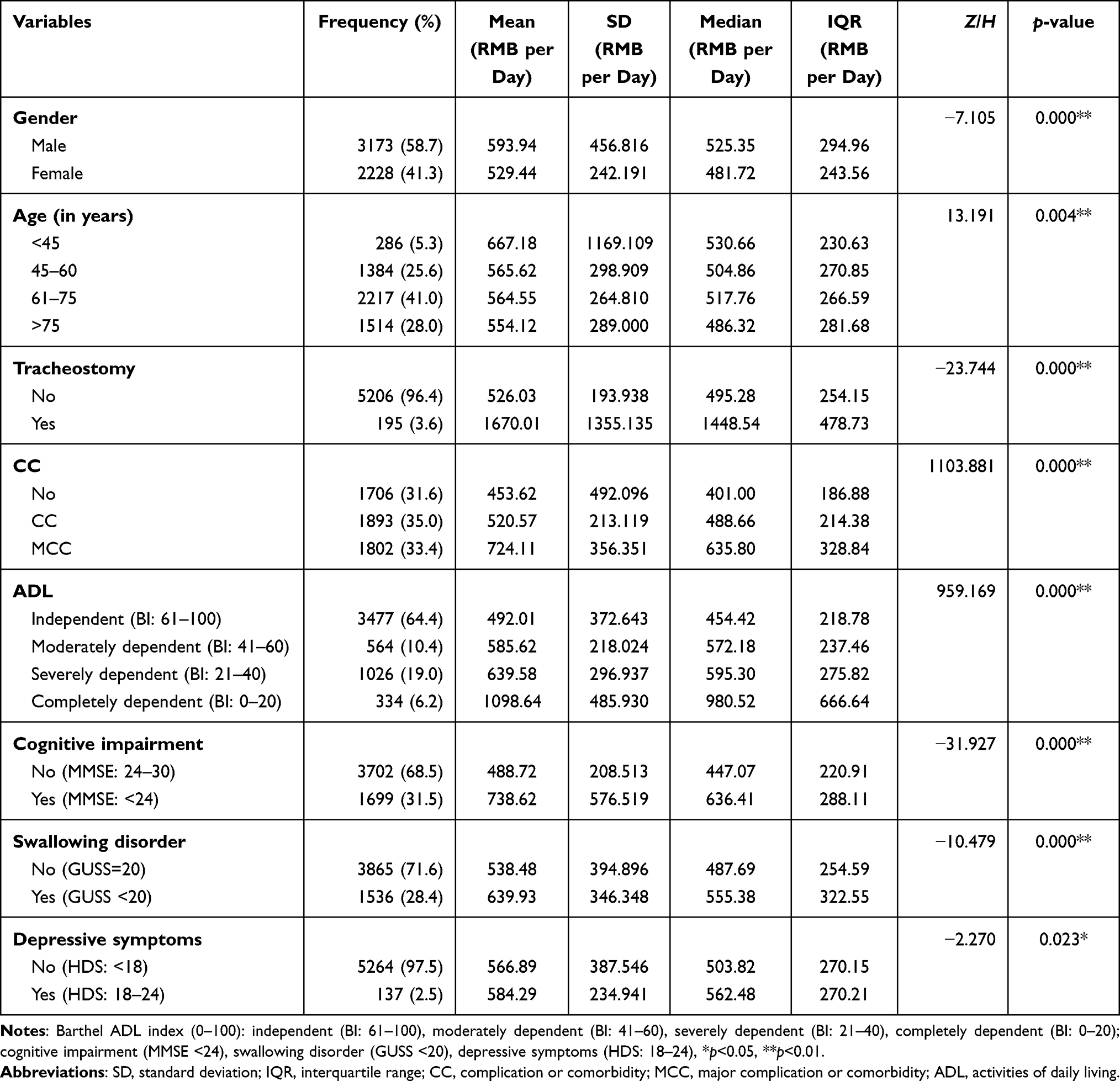 |
Table 2 Results of Univariate Analysis for PAC Stroke Inpatient Costs per Day (N=5401) |
Table 3 showed the result of GLM using log link and gamma distribution, three variables (ie, age, swallowing disorder, and depressive symptoms) were not statistically significant (p>0.05). After adjusting variables, five predictors (ie, gender, tracheostomy, CC, ADL, and cognitive impairment) were identified in the GLM regression (χ2=4153.410, p=0.000) in Table 4. The positive coefficients of male (β=0.038, 95%CI: 0.021–0.055, p=0.000), tracheostomy (β=0.840, 95%CI: 0.792–0.888, p=0.000), CC (β=0.120, 95%CI: 0.099–0.141, p=0.000), MCC (β=0.302, 95%CI: 0.280–0.324, p=0.000), moderately dependent on ADL (β=0.147, 95%CI: 0.120–0.175, p=0.000), severely dependent on ADL (β=0.222, 95%CI: 0.200–0.244, p=0.000), totally dependent on ADL (β=0.306, 95%CI: 0.267–0.344, p=0.000), and cognitive impairment (β=0.138, 95%CI: 0.118–0.158, p=0.000) increased costs. The effect of tracheostomy on costs was larger than the effect of other predictors. The assignment of variables are shown in Table 5, and the results of the GLM regression analysis are presented in Tables 3 and 4.
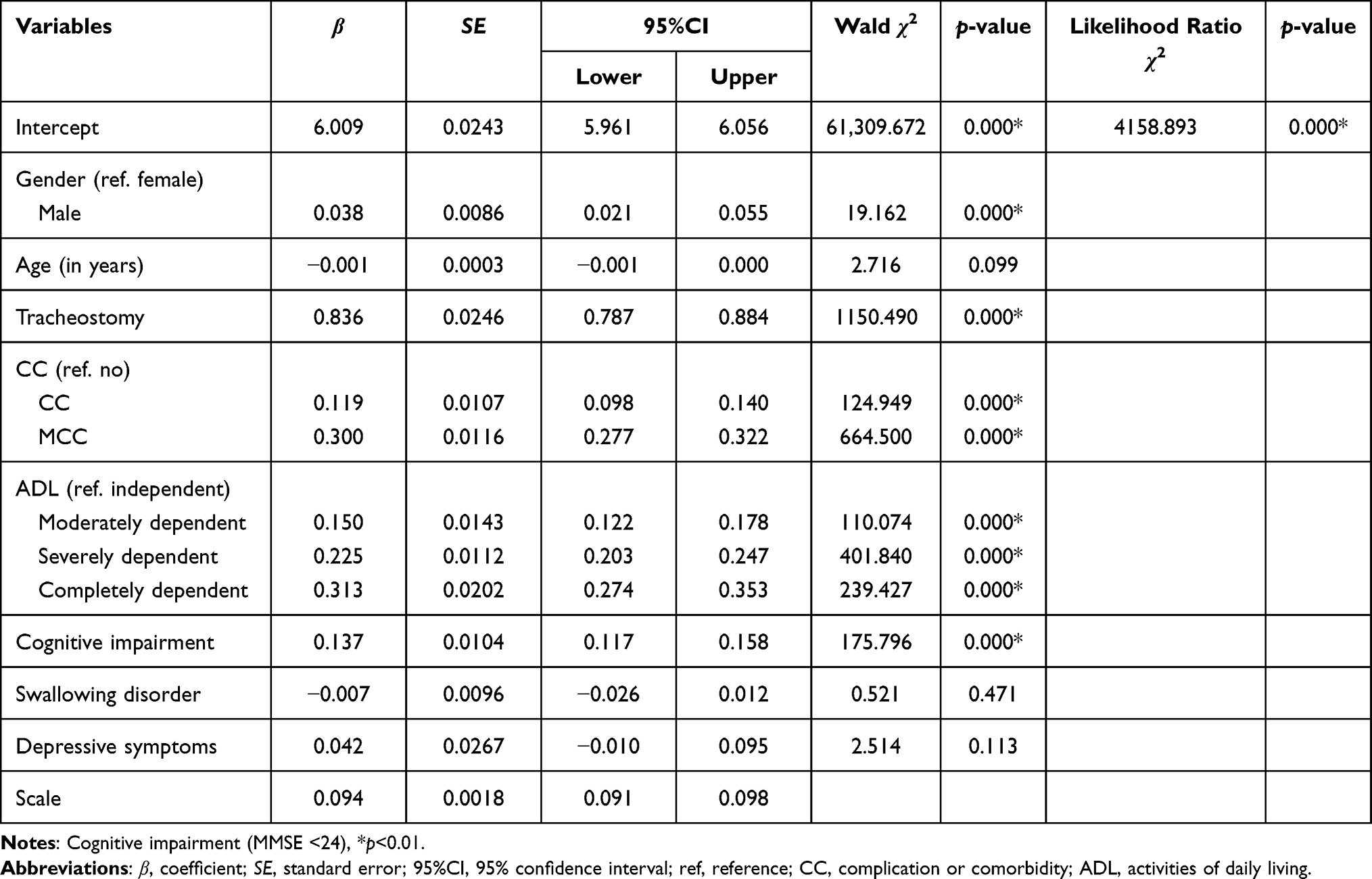 |
Table 3 Results I of Generalized Linear Model (GLM) Using Log Link and Gamma Distribution for PAC Stroke Inpatient Costs per Day (N=5401) |
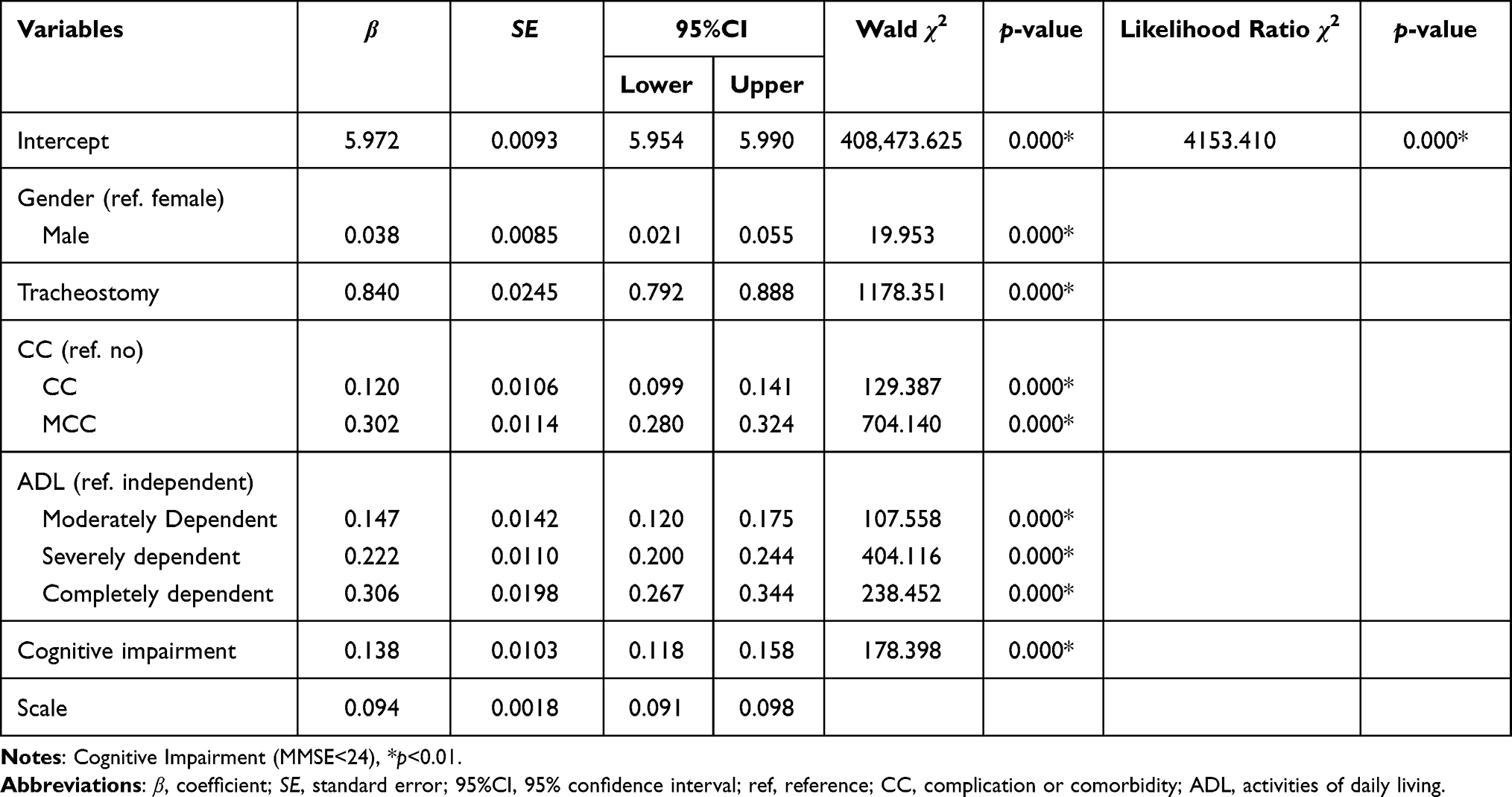 |
Table 4 Results II of Generalized Linear Model (GLM) Using Log Link and Gamma Distribution for PAC Stroke Inpatient Costs per Day (N=5401) |
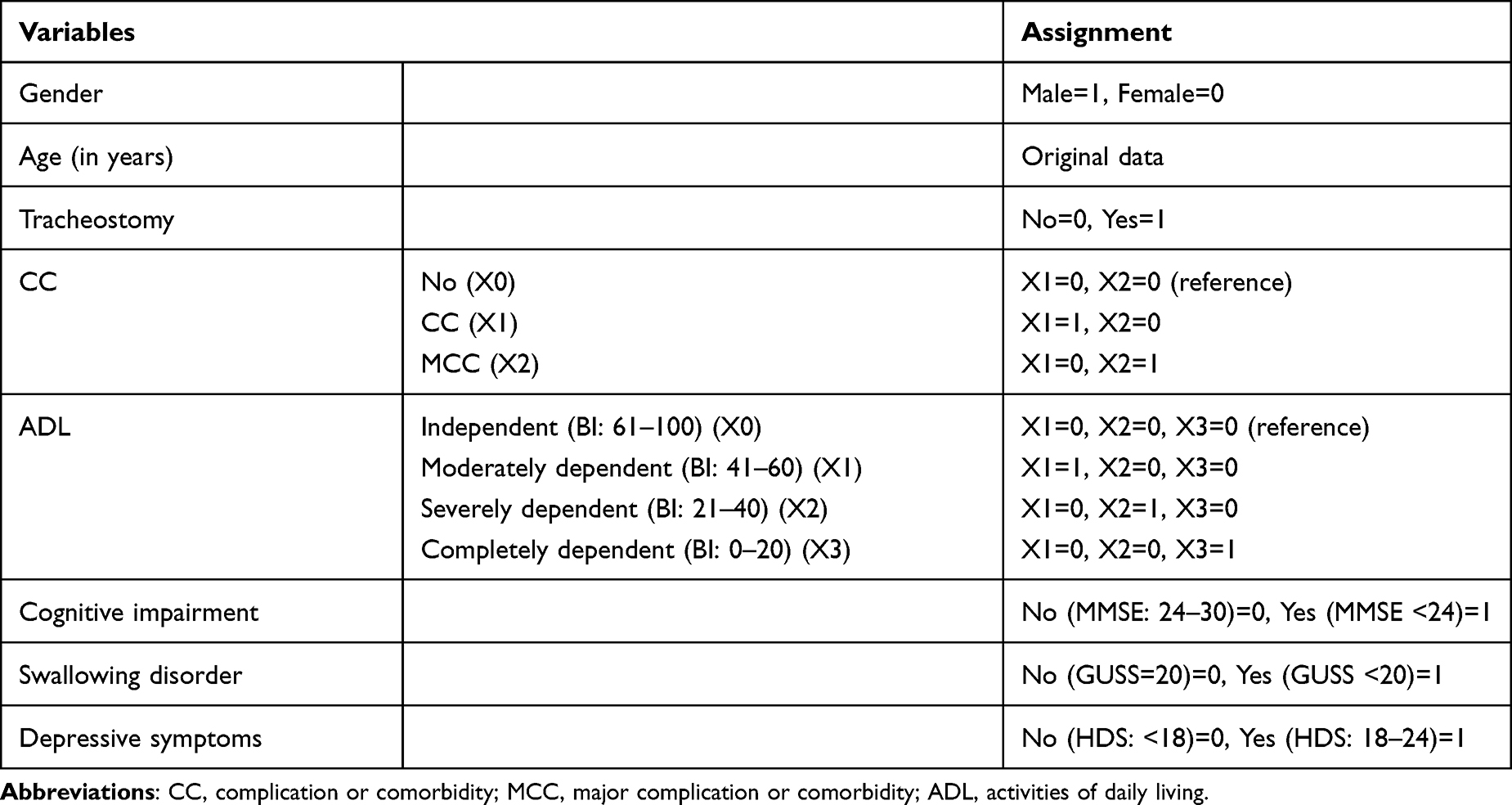 |
Table 5 The Assignment of Independent Variables in the Regression Model |
The QR results show significant differences among lower and upper quantiles in Table 6. The statistical significance between some variables (male, age, CC, moderately dependent on ADL, depressive symptoms) and per diem costs fluctuated across the seven quantiles, except for the swallowing disorder, which was not significant in costs per day across all quantiles. Moreover, predictors such as tracheostomy, MCC, ADL severely dependent, ADL completely dependent, and cognitive impairment increased per diem costs across all the quantiles. The effect of tracheostomy, CC, and MCC on per diem costs was more significant at the 95th quantiles than the effect at the lower quantiles. In contrast, the cognitive impairment effect on per day costs was more significant at the 5th quantile and smaller at the upper quantiles. ADL had a more significant effect on costs at the central quantile rather than the lower or upper quantiles. For instance, ADL severely dependent had a larger effect at the 90th quantile, while ADL moderately and completely dependent had a larger effect at the 75th quantiles. QR plots of slopes were developed to visually examine the impact of the predictors across selected quantiles (Figure 2).
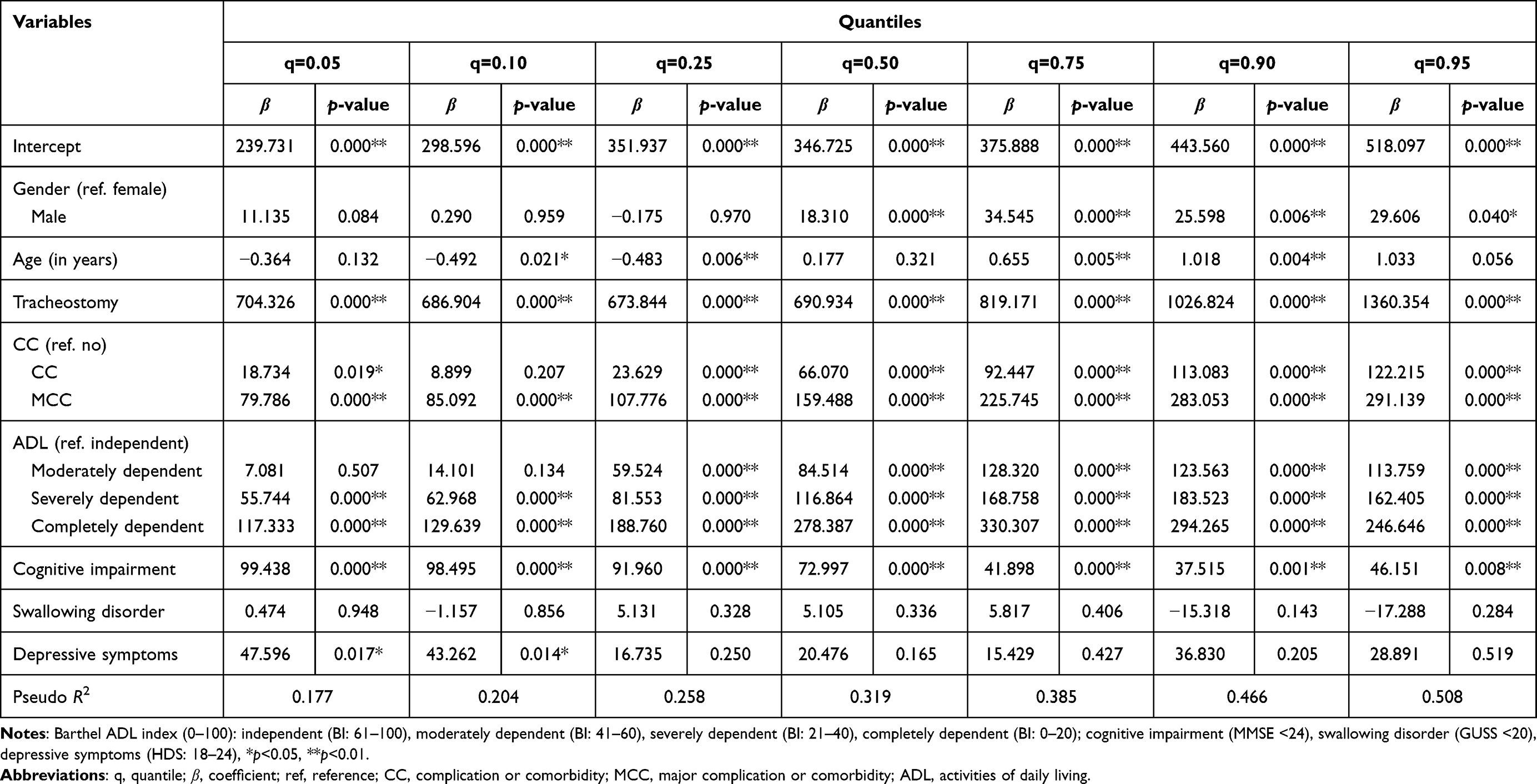 |
Table 6 Results of Multivariate Quantile Regression Analysis for Predictors of PAC Stroke Inpatient Costs per Day (N=5401) |
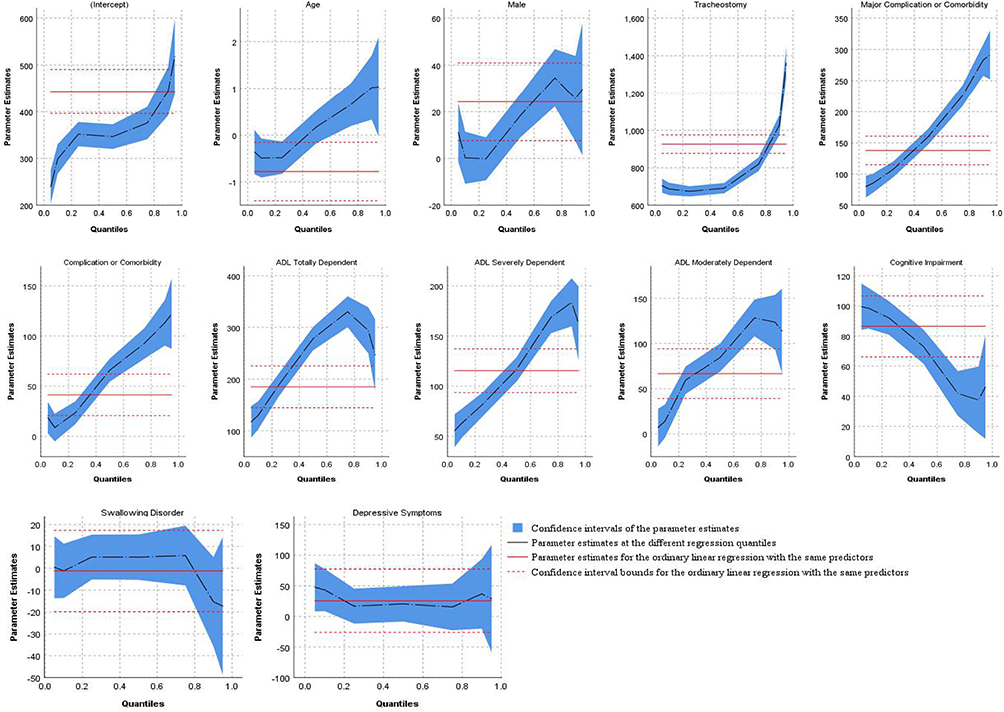 |
Figure 2 Quantile regression plot of predictors effect on quantiles of PAC stroke inpatient per diem costs distribution. |
Figure 3 shows the classification of the per diem costs for PAC stroke inpatients in China. Using classification and regression tree analysis, a regression tree was produced, in which PAC stoke patients were first split into two groups (tracheostomy and nontracheostomy). Second, patients without tracheostomy were subdivided into three groups by CC (without CC, with CC, and with MCC). Third, each branch was further classified by ADL, producing a classification with 12 classes. The “without CC” and “with MCC” branches were both split into four categories based on ADL, while the “with CC” branch was divided into three classes.
 |
Figure 3 Classification of the per diem costs for PAC stroke inpatients in China (N=5401). Abbreviations: CC, complication or comorbidity; MCC, major complication or comorbidity; ADL, activities of daily living. Notes: Barthel ADL index (0–100): independent (BI:61–100), moderately dependent (BI: 41–60), severely dependent (BI: 21–40), completely dependent (BI: 0–20). |
The RIV was as high as 0.46, reflecting a better grouping performance. Low CV (less than 1.0; range: 0.18–0.81) indicated slight variation and achieved better homogeneity within each group. The Kruskal–Wallis test was statistically significant (χ2=2090.662, p=0.000), indicating that the intergroup heterogeneity was good and the classification was reasonable. The RW for individual classes ranged from 0.67 (class 2) to 2.94 (class 1). Higher RW reflected more costs or services provided to patients in that group. The median cost was used to determine the group’s payment standard. Each group’s upper limit was calculated as the 75th quantile plus 1.5 times interquartile range (P75+1.5IQR), which defined cases with excess cost.6,36,37 After calculation, only 120 (2.22%) patients exceeded the upper limit of the cost control. Table 7 presents the statistical values of the per diem cost for all the groups.
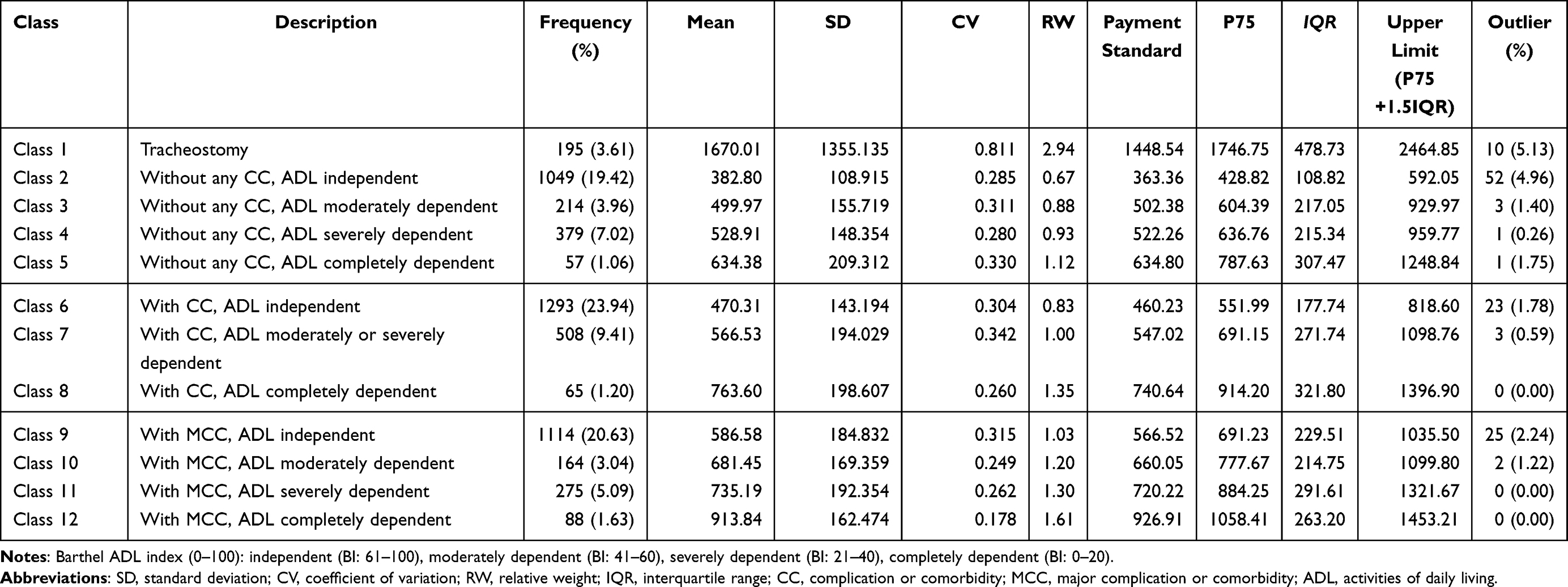 |
Table 7 The Case-mix Classification and the Standard Costs per Day of PAC Stroke Inpatients in China (RMB per Day) |
Discussion
Our study was the first to develop a case-mix classification of post-acute care for stroke patients in China. An important feature of our study was that we included several functional measures in predicting resource use, which was found to be relevant in other research.4,10,16 For the classification methodology, the key determinants (tracheostomy, CC, ADL, and cognitive impairment) were identified by QR and linear regression. Then the CHAID decision-tree analysis was conducted to provide statistics for classification. To date, this remains the only comprehensive QR study modeling the costs of PAC stroke patients in China. The following are the key points of discussion.
Four main variables, tracheostomy, CC, ADL, and cognitive impairment, were identified as the primary predictors of the per diem costs for PAC stroke inpatients in China. For tracheostomy, Acumen reported that tracheostomy was considered one of the best cost predictors for PAC because it is often performed in critically ill stroke patients who require intensive care and medical treatment.,26,4,10,16,26 Ikegami et al also proposed a high correlation between tracheostomy and the per diem cost.19 Similar to our findings, the cost of the tracheostomy group was significantly higher than that of the nontracheostomy groups, so its influence on the overall hospitalization cost cannot be ignored. For CC, Matizirofa et al proposed that CC contributed a larger proportion to total costs for stroke patients in South Africa.23 Khiaocharoen et al posited a strong relationship between CC and costs per day.10 Our results are similar; CCs such as hypertension, diabetes, and heart problems were the primary drivers of the medical costs for stroke patients. For physical function status, a study conducted by Williams et al proposed functionality, as measured by ADL, was the most important predictor of the cost, explaining 30% of the variance in total cost.38 Fries et al reported that ADL explained resource use well while ignoring most of the relatively rare heavy care patients.17 Similarly, it is generally believed that function limitation or disability on ADL will lead to more resource consumption owing to the high demand for living care, skin care, and rehabilitation training. Cognitive function also significantly affects cost. Eilertsen et al reported that cognitive impairment was associated with slightly higher resource use for residents without major medical problems and serious functional dependencies.7 Stineman et al considered that cognitive impairment was an important contributor to per diem cost.8 Similar to our findings, patients with cognitive impairment, most of whom have communication difficulty and poor compliance, require additional care and increase the cost burden. This study demonstrated that it is necessary to include function variables as cost determinants in classifying the cost of post-acute patients.
As to the QR model, traditionally, linear regression was used to identify predictors of medical cost, yet modeling with QR could be more appropriate in our settings. As shown in Figure 1, linear regression solely focuses on the mean missed critical information of the underlying relationship that might exist between the cost conditional distribution and its predictors, especially in the presence of skewed data. This is because the conditional distribution of costs not only differed by their means, but also by their lower and upper tails.23–25 Compared with linear regression, QR provided flexibility to analyze the cost predictors corresponding to quantiles of interest and was more robust to statistical outliers.23
The statistical performance of the case-mix classification system was favorable, with only 12 groups and an RIV of 0.46 for 5401 inpatients compared to other related case-mix classifications. Eilertsen et al conducted a classification for 290 stroke patients in rehabilitation facilities and 193 stroke patients in skilled nursing facilities (five groups, RIV=0.28).7 In contrast, a modified classification explained more variance in resource use (five groups, RIV=0.41).7 Furthermore, the RIV in the present study was better than that of the current Australian Aged Care Funding Instrument (ACFI) (64 groups, RIV=0.20),39 but lower than the RIV of the Australian National Aged Care Classification (AN-ACC) (13 groups, RIV=0.52)16 for 1877 aged care residents, as well the RUG-IV system used in the US (66 groups, RIV=0.62).18 A recent overview of international validation studies of the RUG-III case-mix system in eight countries and regions revealed an RIV value between 0.14 and 0.67 (22–53 groups),18 compared to which our results are also acceptable As a final point, setting the payment standards and upper limit for each group in Table 7 can help strengthen the management of cases with excess costs, effectively reducing the waste of resources and promoting equity and efficiency among payers, providers, and patients.
Limitations
Our study also has several limitations. First, this analysis was based on data drawn from seven hospitals in Jinhua City, further studies are needed when generalizing the results to the entire country. Second, as there are currently no uniform and mandate assessment instruments used in PAC settings in China, each institute uses a different set of assessment tools to measure patient severity and functional impairment levels. The function data in this study were collected by several assessment scales (BI, MMSE, GUSS, and HDS), but the assessments were not standardized across facilities. Therefore, it is necessary to develop standardized assessment tools for PAC settings in China and improve the quality of cross-setting data collection.
Conclusions
Identifying and quantifying cost drivers through QR models can benefit the cost study of post-acute care. We proposed a novel case-mix system closely classifying the level of resource use of post-acute stroke inpatients. The information generated from this study will be useful to facilitate the development of an appropriate payment method for post-acute-care patients in China. Due to the differences in payment and service systems across China, this case-mix also needs to be adjusted if promoted. In future research, studies should investigate the case-mix system for other diseases in Chinese PAC settings.
Ethics Approval
The facilities gathered the data routinely in clinical practice according to the requirement of the local Healthcare Security Administration. Permission has been obtained from the Medical Ethics Committee of the Chinese Academy of Medical Sciences & Peking Union Medical College to report the data for research purposes (Protocol number: X170315009). All the inpatients were informed about the study. Only the consenting patients were included, which secured a paper-written patient consent process. Such patient consent approach was approved by the Ethics Committee. As for the critically ill patients, their family members made the informed consent process and responded on their behalf. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
This work was supported by Jinhua Healthcare Security Administration in Zhejiang province in China. The authors wish to thank facilitators, doctors, nurses, computer programmers, research assistants, and all patients who participated in the present study.
Funding
This work was supported by the Fundamental Research Funds for the Central Universities (No. 3332020068) and the Medical and Health Innovative Engineering Program of Chinese Academy of Medical Sciences (2021-I2M-1-046). The funding agencies were not involved in the study design, data analysis, and manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Krishnamurthi RV, Takayoshi I, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the Global Burden of Disease Study 2017. Neuroepidemiology. 2021;54(2):171–179. doi:10.1159/000506396
2. Report on stroke prevention andtreatment in China Writing Group. Brief report on stroke prevention and treatment in China, 2019. Chi J Cerebrovasc Dis. 2020;17(5):272–281. [in Chinese]. DOI:10.3969/j.issn.1672-5921.2020.05.008.
3. Yan S, Ya L, Hua ZW, et al. Analysis of variance and multiple linear regression on the structure and influential factors of rehabilitation hospitalization costs of stroke patients. Jiangsu Healthc Adminis. 2020;31(5):617–621. [in Chinese]. doi:10.3969/j.issn.1005-7803.2020.05.020
4. Jinxuan Z, Qiuping M. Meta-analysis of nursing stroke survivors in convalescence in China in recent ten years. Chi Clini Nur. 2019;11(5):449–451. [in Chinese]. doi:10.3969/j.issn.1674-3768.2019.05.024
5. Zhang L, Sun L. Impacts of diagnosis-related groups payment on the healthcare providers’ behavior in China: a cross-sectional study among physicians. Risk Manag Healthc P. 2021;14:2263–2276. doi:10.2147/RMHP.S308183
6. Jia L, Qian S, Xiping S, et al. Exploratory research on patient care charging scheme model for patients with nervous system diseases based on RUG. Nur J Chi PLA. 2020;37(4):55–58. [in Chinese]. doi:10.3969/j.issn.1008-9993.2020.04.013
7. Eilertsen TB, Kramer AM, Hrincevich S, Hrincevich CA. Application of functional independence measure-function related groups and resource utilization groups-version III systems across post acute settings. Med Care. 1998;36(5):695–705. doi:10.1097/00005650-199805000-00009
8. Stineman MG. Case-mix measurement in medical rehabilitation. Arch Phys Med Rehab. 1995;76(12):1163–1170. doi:10.1016/S0003-9993(95)80127-8
9. Eagar K, Cromwell D. Classifying sub-acute and non-acute patients: results of the New South Wales Casemix Area Network study. Aust Health Rev. 1997;20(2):26–42. doi:10.1071/ah970026
10. Khiaocharoen O, Pannarunothai S, Zungsontiporn C, et al. Casemix classification payment for sub-acute and non-acute inpatient care, Thailand. J Med Assoc Thai. 2010;93(7):849–859.
11. Sala S, Soontornpipit P. Design and development of data model for thai sub acute and non acute patients. AMM. 2015;781(3):579–582. doi:10.4028/www.scientific.net/AMM.781.579
12. Khiaocharoen O, Pannarunothai S, Zungsontiporn C. Cost of acute and sub-acute care for stroke patients. J Med Assoc Thai. 2012;95(10):1266–1277.
13. Yong Y, Shuo L, Xi W, et al. the utilization of inpatient health services and influencing factors of hospitalization costs of urban stroke patients in China. Chi GP. 2020;23(13):1615–1620. [in Chinese]. doi:10.12114/j.issn.1007-9572.2020.00.091
14. Xiaoyan L, Yumei L. Analysis of hospitalization expenses of elderly patients with cerebral infarction. Chi Health Econ. 2021;40(8):34–36. [in Chinese].
15. Chen Z, Weiping J, Ying S. Analysis of the influence of paid by diagnosis-related groups on acute cerebral infarction. Chi Med Rec. 2019;20(4):43–45. [in Chinese]. doi:10.3969/j.issn.1672-2566.2019.04.017
16. Eagar K, Gordon R, Snoek MF, et al. The Australian National Aged Care Classification (AN‐ACC): a new casemix classification for residential aged care. Med J Aust. 2020;213(8):359–363. doi:10.5694/mja2.50703
17. Fries BE, Schneider DP, Foley WJ, et al. Refining a case-mix measure for nursing homes: resource utilization groups (RUG-III). Med Care. 1994;32(7):668–685. doi:10.2307/3766161
18. Turcotte LA, Poss J, Fries B, et al. An overview of international staff time measurement validation studies of the RUG-III case-mix system. Health Serv Ins. 2019;12:1–11. doi:10.1177/1178632919827926
19. Ikegami N, Fries BE, Takagi Y, et al. Applying RUG-III in Japanese long-term care facilities. Gerontologist. 1994;34(5):628–639. doi:10.1093/geront/34.5.628
20. Hirdes JP, Botz CA, Kozak J, et al. Identifying an appropriate case mix measure for chronic care: evidence from an Ontario pilot study. Healthc Manage Forum. 1996;9(1):40–46. doi:10.1016/S0840-4704(10)60943-X
21. Kim EK, Park HY, Kim CY. On the feasibility of a RUG-III based payment system for long-term care facilities in Korea. Taehan Kanho Hakhoe Chi. 2004;34(2):278–289. doi:10.4040/jkan.2004.34.2.278
22. Laine J. RUG-III for exploring the association between staffing levels and cost-efficiency in nursing facility care in Finland. Health Care Manage Rev. 2006;31(1):73–77. doi:10.1097/00004010-200601000-00010
23. Matizirofa L, Chikobvu D. Analysing and quantifying the effect of predictors of stroke direct costs in South Africa using quantile regression. BMC Public Health. 2021;21(1):1560–1568. doi:10.1186/s12889-021-11592-0
24. Koenker R, Hallock KF. Quantile regression. J Econ Perspec. 2015;15(4):143–156. doi:10.1097/00043426-200201000-00019
25. Aheto JMK. Simultaneous quantile regression and determinants of under-five severe chronic malnutrition in Ghana. BMC Public Health. 2020;20(1):644–655. doi:10.1186/s12889-020-08782-7
26. Acumen. Skilled nursing facilities patient-driven payment model technical report; 2018. Available from: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SNFPPS/Downloads/PDPM_Technical_Report_508.pdf.
27. National Healthcare Security Administration of the People’s Republic of China. China Healthcare Security Diagnosis Related Groups (CHS-DRG); 2019. Available from: http://www.nhsa.gov.cn/module/download/downfile.jsp?classid=0&filename=a3cbb51dc6354dd4b6a5ab09bec18121.pdf.
28. Mahoney FI, Barthel DW. Functional evaluation: the barthel index: a simple index of independence useful in scoring improvement in the rehabilitation of the chronically Ill. Md State Med J. 1965;1(14):56–61.
29. Peng LN, Lu WH, Liang CK, et al. Functional outcomes, subsequent healthcare utilization, and mortality of stroke postacute care patients in Taiwan: a Nationwide Propensity Score-matched Study. JAMDA. 2017;18(11):990–997. doi:10.1016/j.jamda.2017.06.020
30. Folstein M, Folstein S, Mchugh P. “Mini-mental state”: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
31. Tombaugh TN, Mcintyre NJ. The mini-mental state examination: a comprehensive review. J Am Geriatr Soc. 1992;40(9):922–935. doi:10.1111/j.1532-5415.1992.tb01992.x
32. Park KD, Kim TH, Lee SH. The gugging swallowing screen in dysphagia screening for patients with stroke: a systematic review. IJNS. 2020;107:103588. doi:10.1016/j.ijnurstu.2020.103588
33. Trapl M, Enderle P, Nowotny M, et al. Dysphagia bedside screening for acute-stroke patients: the gugging swallowing screen. Stroke. 2007;38(11):2948–2952. doi:10.1161/STROKEAHA.107.483933
34. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiat. 1960;23(1):56–62. doi:10.1136/jnnp.23.1.56
35. Miller IW, Bishop S, Norman WH, et al. The modified hamilton rating scale for depression: reliability and validity. Psychiat Res. 1985;14(2):131–142. doi:10.1016/0165-1781(85)90057-5
36. Yuki M, Emoto Y, Yoshizawa K, et al. Intestinal bacterial infection diagnosed by histological examination of endoscopic biopsy specimens. Gastroenterology. 2016;10(3):629–638. doi:10.1159/000452212
37. Xie YH, Chongsuvivatwong V, Tang Z, et al. Spatio-temporal clustering of hand, foot, and mouth disease at the county level in Guangxi, China. PLoS One. 2014;9(2):e88065. doi:10.1371/journal.pone.0088065
38. Williams BC, Fries BE, Foley WJ, et al. Activities of daily living and costs in nursing homes. Health Care Financ Rev. 1994;15(4):117–135.
39. Green J, Gordon R, Blanchard M, et al. Development of the Australian NationalSubacute and Non-acute Patient Classification version 4: final report. Wollongong: Centre for Health Service Development, University of Wollongong; 2015. Available from: https://www.ihpa.gov.au/sites/default/files/Documents/an-snap_classification_version_4_final_report.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.