")
Back to Journals » Infection and Drug Resistance » Volume 15
Analysis of Risk Factors for Sternal Wound Infection After Off-Pump Coronary Artery Bypass Grafting
Authors Yang J, Zhang B, Qu C, Liu L, Song Y
Received 6 July 2022
Accepted for publication 19 August 2022
Published 6 September 2022 Volume 2022:15 Pages 5249—5256
DOI https://doi.org/10.2147/IDR.S381422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Jian Yang,* Bin Zhang,* Chengliang Qu,* Li Liu,* Yanyan Song
Department of Cardiovascular Surgery, General Hospital of Ningxia Medical University, Yinchuan, 750004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanyan Song, Department of Cardiovascular Surgery, General Hospital of Ningxia Medical University, No. 804 Shengli South Street, Xingqing District, Yinchuan, 750004, People’s Republic of China, Tel +86 951-6743014, Fax +86 951-6744302, Email [email protected]
Objective: To investigate the risk factors of deep sternal wound infection (DSWI) after off-pump coronary artery bypass grafting and its prevention and treatment strategy.
Methods: The clinical data of 465 patients who underwent OPCABG with a median chest incision were retrospectively analyzed. The patients were divided into the observation group (with DSWI, 32 cases) and the control group (without DSWI, 433 cases) according to the occurrence of DSWI. The preoperative, intraoperative, and postoperative clinical data relevant to DSWI were collected in both groups. The univariate and multivariate logistic regression analyses were adopted to analyze the risk factors for DSWI after OPCABG and investigateand its prevention and treatment strategy.
Results: DSWI occurred in 32 cases with an incidence of infection of 6.89%. There were 5 cases died in the observation group (with DSWI), the overall mortality rate was 1.07% and the intra-group mortality rate was 15.6%. There were 16 cases died in the control group (without DSWI) because of low cardiac output syndrome and multiple organ failure, the overall and intra-group mortality rates were 3.44% and 3.69% respectively. By analyzing the risk factors of DSWI between the two groups, the differences in age, body mass index (BMI), history of diabetes mellitus (DM), operation time, tracheal intubation time, time of stay in thecardiac care unit, blood transfusion (blood plasma)> 800mL, blood transfusion (erythrocyte suspension)> 6um, secondary thoracotomy were statistically significant between the observation and control groups (P < 0.05 in all).
Conclusion: Obesity, history of DM, prolonged operation time and tracheal intubation time, time of stay in CCU, utilization of blood product and secondary thoracotomy were DSWI independent risk factors after OPCABG.Some preventive measure should been implemented to reduce the incidence of DSWI, such as shorter operation time and tracheal intubation time, reducing the utilization of blood product.
Keywords: off-pump coronary artery bypass grafting, sternal wound infection, risk factor
Introduction
Off-pump coronary artery bypass grafting (OPCABG) is an effective treatment for coronary heart disease (CHD), but deep sternal wound infection (DSWI) after OPCABG is a serious complication after cardiac surgery, accounting for 1% of the complications of cardiac surgery via median incision, with high mortality of up to 20%.1–5 The natural prognosis of DSWI is poor and patients might often die due to multi-organ failure. Early intervention and active treatment of the high-risk factors for infection could reduce the length of the ICU stay and mechanical ventilation duration, improve the short- and long-term outcomes, and improve the quality of life for patients.
DSWI lead to liquefaction and necrosis of the subcutaneous tissues without untreatment, resulting in prolonged illness and death in severe cases. A number of studies have demonstrated some risk factors of DSWI, such as diabetes, obesity, prolonged operative time, use of blood products and others.6–8 However, some predictive value of risk factors are not identified, including tracheal intubation time and beating heart procedures. Therefore, this study aimed to investigate the risk factors for the occurrence of DSWI after surgery and the therapeutic methods for the improvement of prognosis.
Materials and Methods
General Data and Study Setting
A total of 465 patients undergoing OPCABG via a median thoracic incision in our department from January 2016 to December 2020 were consecutively enrolled in this study.Among them the observation group (with DSWI, 32 cases) and the control group (without DSWI, 433 cases) according to the occurrence of SWI after surgery (Figure 1). The inclusion criteria:The diagnosis of CHD was confirmed in all cases through coronary angiography, and all patients undergoing OPCABG via a median thoracic incision in. Exclusion criteria: 1. Other cardiac operations were performed at the same time. 2. Preoperative complicated infectious diseases. The study was approved by the institutional review committee ofGeneral Hospital of Ningxia Medical University and the informed written consents were signed by all patients.
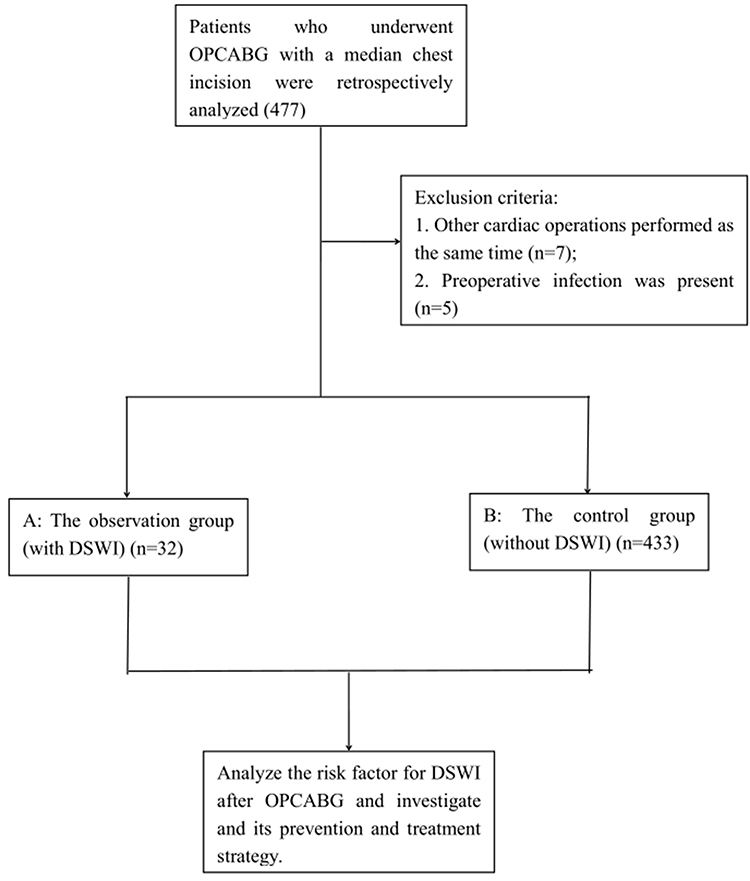 |
Figure 1 Flow chart. |
Methods
Surgical Methods and Postoperative Treatment: Patients in both groups underwent OPCABG via the median thoracic incision under general anesthesia. Postoperatively, the patients were treated in the cardiac care unit (CCU) with ventilator-assisted ventilation in the cardiac surgery department. Low-dose dobutamine, dopamine were administered to assist circulation as well as continuous monitoring of the hemodynamic parameters. Treatments for the secondary prevention of CHD, such as dual antiplatelet aggregation drugs, lipid regulation and plaque stabilization, control of ventricular rate, and coronary dilation, were conducted. Antibiotics were given 24 hours after surgery for the prevention of infection. The occurrence of SWI should be noted in case of postoperative fever, skin redness at the incision site, increased skin temperature, and exudates from the wound. Chest CT scanning can detect insidious SWI, but needle aspiration should be conducted for those with high suspicion.
The Definition and Diagnostic Criteria for DSWI
The definition of DSWI: DSWI, also known as mediastinal infection, is defined as infection related to surgical incision and involving muscle and bone, with or without infection in the posterior sternal space.1,9,10
The Diagnostic Criteria for SWI:11 SWI after cardiac surgery can be divided into the superficial SWI (SSWI) and deep SWI (DSWI).12 SSWI is an infection limited to the skin and subcutaneous tissues without the involvement of the sternum or mediastinum. DSWI is an infection that involves the sternum or mediastinum. DSWI can be diagnosed when the patient has one of the following manifestations: (1) microbial growth in the culture of mediastinal tissue or secretion; (2) evidence of mediastinal inflammation during surgery or histopathological examination; (3) persistent postoperative chest pain, sternal instability, or fever (with a temperature greater than 38°C), accompanied by purulent mediastinal drainage or isolation of pathogenic microorganisms from the culture of blood or mediastinal area secretions.
Observation Indicators
The preoperative, intraoperative, and postoperative clinical data relevant to SWI were collected in both groups. The preoperative clinical data were age, gender, BMI, histories of hypertension, DM, COPD, smoking, and triglyceride levels. Primary endpoint: Sternal incision infection occurred after surgery. Secondary endpoint: operation duration, mechanical ventilation duration, length of stay in the CCU in the cardiac surgery department, drainage volume on the operation day, volume of postoperative blood transfusion, secondary median incision debridement, postoperative pulmonary infection, and postoperative hypoxemia, Infection rate, death rate.
Statistical Methods
The statistical analysis was performed by another blinded statistician using SPSS 19.0 software. The measurement data were expressed as mean ± standard deviation ( ), and the t-test was used for statistical analysis. The countable data were expressed as percentages or rates. The X2-test was used for statistical analysis, and the Fisher’s exact probability method was adopted for those that did not meet the condition. The unconditional multivariate logistic regression analysis was used for the analysis of the risk factors for SWI that had statistical significance. P < 0.05 was considered statistically significant.
), and the t-test was used for statistical analysis. The countable data were expressed as percentages or rates. The X2-test was used for statistical analysis, and the Fisher’s exact probability method was adopted for those that did not meet the condition. The unconditional multivariate logistic regression analysis was used for the analysis of the risk factors for SWI that had statistical significance. P < 0.05 was considered statistically significant.
Results
Comparison of Clinical Results Between the Two Groups of Patients
A total of 465 patients undergoing OPCABG via a median thoracic incision were enrolled and DSWI occurred in 32 cases with an incidence of infection of 6.89%. There were 5 cases died in the observation group (with DSWI), the overall mortality rate was 1.07% and the intra-group mortality rate was 15.6%. There were 16 cases died in the control group (without DSWI) because of low cardiac output syndrome and multiple organ failure, the overall and intra-group mortality rates were 3.44% and 3.69% respectively.
The Description of the Population
A total of 465 patients undergoing OPCABG via a median thoracic incision were enrolled and DSWI occurred in 32 cases with an incidence of infection of 6.89%. In the observation group, there were 20 males and 12 females, with an average age of 66.1 ± 10.5 years and an average body mass index (BMI) of 26.78 ± 4.56 kg/m2. There were 11 cases combined with hypertension, 13 cases with diabetes mellitus (DM), 9 cases with chronic obstructive pulmonary disease (COPD), and 12 cases with a smoking history. In the control group, there were 262 males and 171 females, with an average age of 58.7 ± 13.6 years and an average BMI of 20.34 ± 3.21 kg/m2. There were 102 cases combined with hypertension, 98 cases with DM, 84 cases with COPD, and 202 cases with a smoking history. The details are illustrated in Table 1.
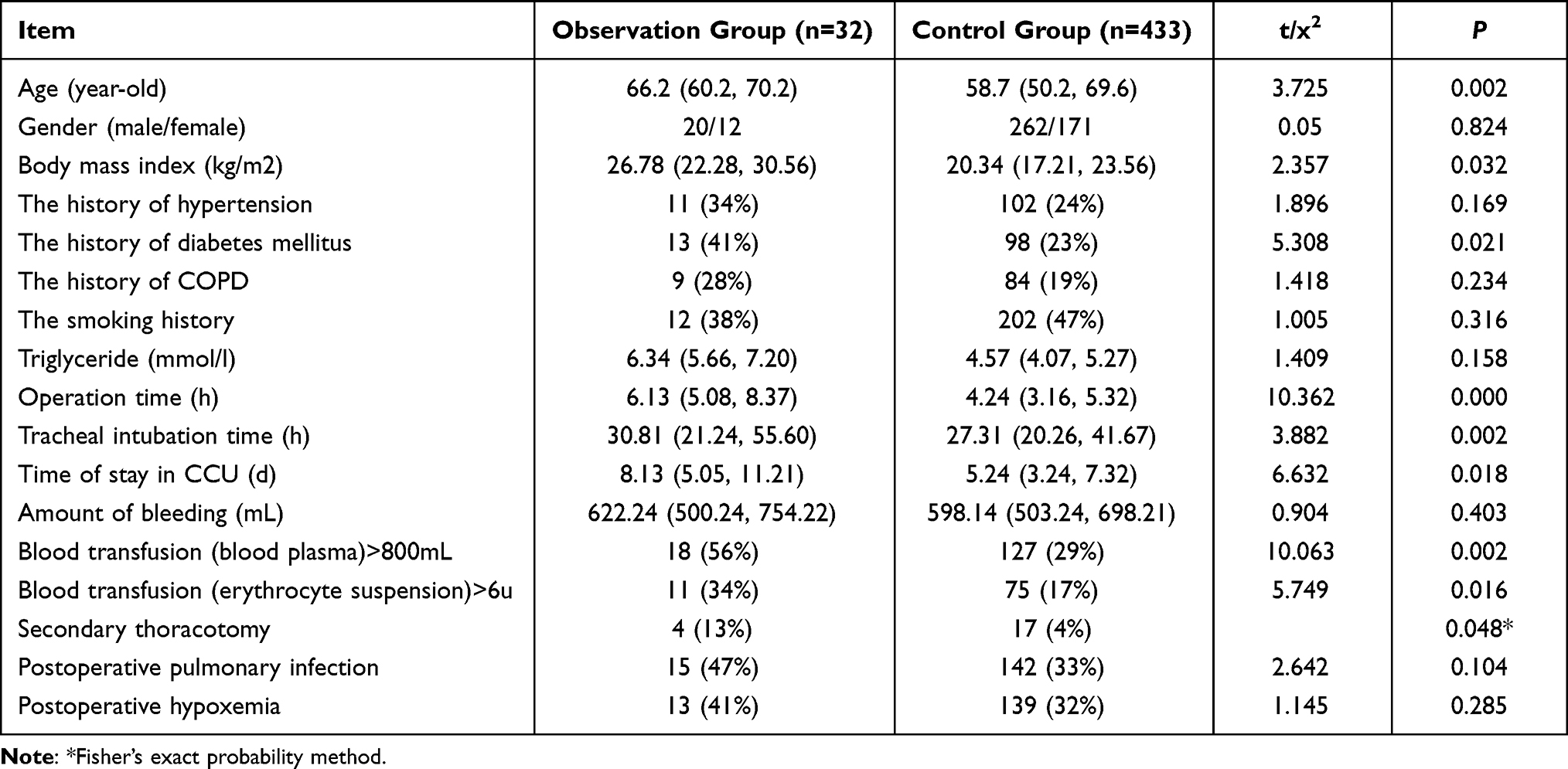 |
Table 1 The Comparison of the Risk Factors for Sternal Wound Infection Between the Two Groups of Patients [M (P25, P75)], n(%)] |
The Comparison of Preoperative, Intraoperative, and Postoperative Risk Factors for SWI Between the Two Groups of Patients
By analyzing the risk factors of DSWI between the two groups, the differences in age, body mass index (BMI), history of diabetes mellitus (DM), operation time, tracheal intubation time, time of stay in CCU, blood transfusion (blood plasma)>800mL, blood transfusion (erythrocyte suspension)>6u, secondary thoracotomy were statistically significant between the observation and control groups (P < 0.05 in all).The details are demonstrated in Table 1. Further multi-factor Logistic regression analysis showed that BMI >28 kg/m2, history of diabetes mellitus, operation time >6h, tracheal intubation time >30h, time of stay in CCU>8d, blood transfusion (blood plasma) >800mL, blood transfusion (erythrocyte suspension)>6u. Secondary thoracotomy were statistically significant between the observation and control groups (P < 0.05 in all).The details are demonstrated in Table 2.
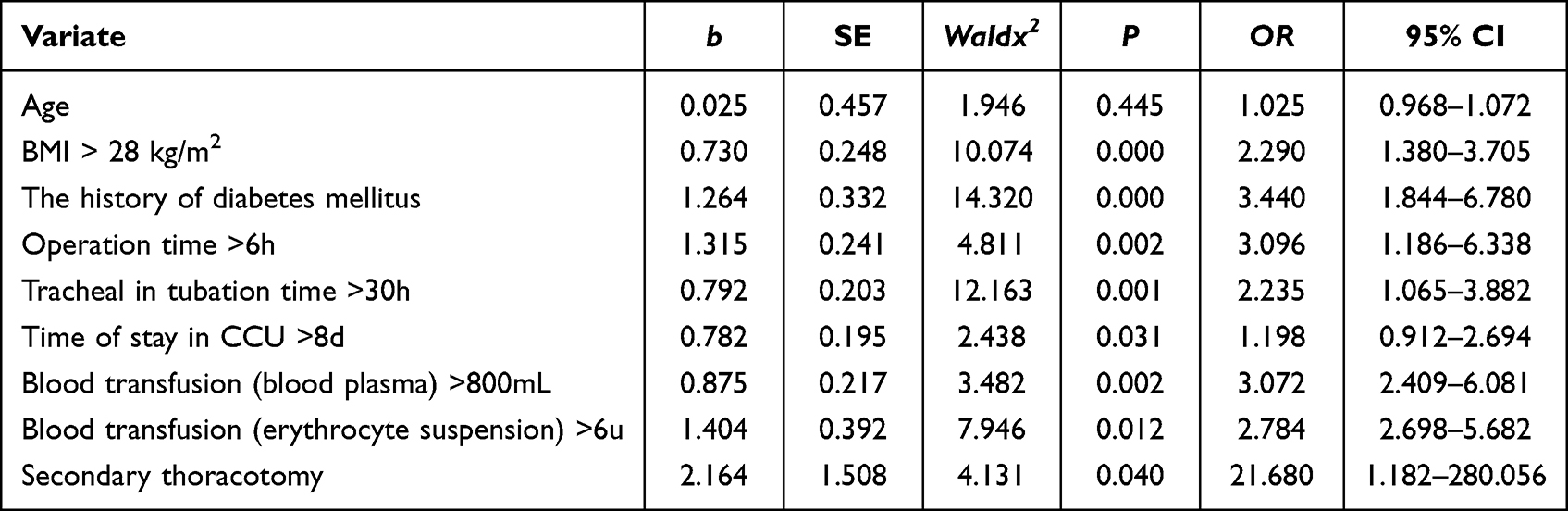 |
Table 2 The Logistic Regression Analysis of the Risk Factors for Sternal Wound Infection in the Two Groups of Patients |
Discussion
DSWI is a serious complication after cardiac surgery, accounting for 1% of the complications of cardiac surgery via median incision, with high mortality of up to 20%.4,5 In the present study, the risk factors for SWI after OPCABG were analyzed. The therapeutic methods to effectively reduce the occurrence of SWI after OPCABG were discussed to improve the prognosis in patients.
The results of this study showed that patients’ age, body mass index, history of diabetes, duration of surgery, duration of mechanical ventilation, duration of postoperative intensive care, amount of postoperative blood transfusion, and second chest opening were risk factors for sternotomy infection after OPCABG (P<0.05), and further multifactorial logistic regression analysis showed that body mass index greater than 28 kg/m2, history of diabetes, duration of surgery > 6h, duration of mechanical ventilation >30h, time of stay in CCU >8d, blood transfusion (blood plasma) > 800mL, blood transfusion erythrocytesuspension) > 6u, and secondary thoracotomy was an independent risk factor for sternotomy infection after OPCABG. The reasons are discussed as follows.
The incidence of incisional infection was higher in obese patients (P<0.05), which may be due to the following reasons. ① Obese patients have more adipose tissue at the incision site and less blood supply, which increases the incidence of postoperative incision infection due to poor incision healing ability. ② Surgical impact. In order to expose well, it is inevitable to move the pull hook back and forth, sometimes pulling hard, making the tissue compression injury more serious. The tissue compression injury itself can lead to slow healing or incisional infection. ③ Fat liquefaction. ④ Patient’s own factors. Obese patients have a higher incision liquefaction rate due to the thick skin fat layer of the incision, and the lack of nutrition is more obvious after the injury. Secondly, obese patients are prone to sweating and the incision is not easily kept dry, which may also lead to incision infection or delayed healing.4
Diabetes can lead to microvascular lesions, resulting in impaired microcirculation, tissue ischemia and hypoxia at the incision site, and slow healing, which can predispose to infection.13–15 Second, postoperative stress, during surgery and the postoperative period, elevated blood glucose is usually observed, leading to increased secretion of catabolic hormones (eg catecholamines or cortisol) and decreased insulin secretion, and related studies have shown that hyperglycemia is associated with an increased risk of DSWI in diabetic patients. However, hypoglycemia should be avoided in patients.
Direct cardiac surgery is generally a long and extensive operation, and there is a correlation between the duration of cardiac surgery and postoperative incisional infections. During surgery, the number of bacteria landing in the surgical area can be 35,000 to 60,000 per hour. The longer the surgery, the longer the exposure time, and also increases the chance of contact between bacteria and the incision on medical devices and elsewhere. Some domestic studies have reported that the longer the operation time, the more serious the incision is stretched and compressed by the instruments for a long time, which will cause local ischemia and hypoxia in the surrounding tissues, resulting in tissue damage and eventually a decrease in tissue resistance. Once postoperative infection occurs, the morbidity and mortality rate is high.
The duration of mechanical ventilation is also an independent risk factor for sternotomy infection after OPCABG. In patients with prolonged tracheal intubation, sputum is not easily and adequately eliminated, which is conducive to bacterial growth, and the use of ventilators also increases sternal instability, which affects healing.After cardiac surgery, the patient needs to be monitored in the intensive care unit and transferred to the general ward for treatment only after the tracheal intubation is removed and the condition is stabilized. Due to the seriousness of the patient’s primary disease, coupled with many invasive operations in the intensive care unit and the massive application of broad-spectrum antibacterial drugs, sternotomy infection is likely to occur and worsen the condition. Therefore, the indications for invasive operations should be strictly mastered, the aseptic operation protocols should be carefully implemented, and the necessity of continued indwelling should be assessed and recorded daily for patients using ventilators, central venous placement and indwelling catheters to minimize the indwelling time.
The amount of perioperative blood transfusion is associated with the incidence of postoperative infection,16,17 and the mechanism of post-transfusion infection may be due to the negative regulation of host immune defenses. The bacterial killing effect of macrophages and NK cells is diminished by homologous blood transfusion, and the total antimicrobial defense is impaired despite positive regulation in some aspects of humoral immunity. Therefore, blood transfusion suppresses the function of immune cells in the patient’s organism and reduces the patient’s immune function.Therefore, the pros and cons of whether blood transfusion is needed in the perioperative period should be weighed, and no or less blood transfusion should be done as much as possible without affecting the patient’s treatment.
Therefore, blood glucose should be controlled during the perioperative period and maintained below 180–200 mg/dl during the intraoperative and early postoperative period.18 Several approaches could be taken preoperatively to reduce the risk of infection: detection and management of opportunistic infections (pneumonia, urinary tract, and skin) and prophylactic administration of adequate antibiotics before skin incision, with 1 g of cefazolin being commonly administered (up to 2 g for those with sizable body weight).During the operation, strict aseptic procedures, gentle treatment of tissues, and careful and adequate hemostasis should be conducted to minimize mediastinal hemorrhage, avoid secondary thoracotomy, and control operation duration. Postoperatively, multiple measures should be conducted to reduce the occurrence of postoperative SWI, including minimizing mechanical ventilation duration, avoiding unnecessary blood transfusions, trying to achieve zero blood transfusions, etc.
For those with SWI, the treatment experience from the cases in the present study is summarized as follows. The clinical manifestations of SWI might be obvious or insidious and often depend on the source of infection. Staphylococcus aureus infections tend to be highly pathogenic and appear within 10 days after surgery. Conversely, the onset of coagulase-negative staphylococcal infections was late, painless, and insidious.12
The small/superficial infections usually presented with tenderness, redness, plasma exudation, or localized pus flow from the incision with a fixed sternum. Large/deep incision infections (located in the deep subcutaneous tissue, osteomyelitis, mediastinitis) might have all of the above manifestations but often have significant purulent drainage and sternal instability. Patients often have fever, chills, drowsiness, and chest wall pain, with elevated leukocytes in a routine blood test. The culture of purulent drainage might reveal the existence of pathogenic bacteria and guide the administration of suitable antibiotics. Incision puncture (sternal puncture) might be feasible as an anti-infection diagnosis with no pus drainage.In cases with an unstable sternum, a chest CT might be useful for diagnosis and help detect the presence of deep infections, such as post-sternal soft tissue, loss of fat integrity, or post-sternal gas-containing abscesses without drainage.19 Minor infections could usually be treated effectively with intravenous antibiotics, incision opening, and local dressing changes.Persistent sinus or multiple recurrent dehiscences might suggest the existence of deeper infection, often involving the sternal sutures, and secondary thoracotomy should be conducted instead of dressing changes.Removal of the metallic line, scraping the diseased bone, and six weeks of antibiotic treatment were effective for deep infections. In case of early exposure of the sternal metallic line or bone, the occurrence of SWI should be noted, and deep infection should be ruled out before dealing with the incision problem. Mediastinal exploration should be required for significant infections as well as dilation of infected tissue, removal of foreign bodies, drainage, and reduction of dead space.
For large/deep incision infections, vacuum sealing drainage (VSD) was adopted in our department as a therapeutic method.VSD is a novel and efficient drainage method with the adoption of VSD material (covered with polyethylene ethanol-hydrated seaweed salt foam dressing) and a biological semi-permeable membrane as an intermediary between the trauma and the outside, isolating the trauma or body cavity from the outside, and providing continuous negative pressure suction.The VSD system can increase the microcirculatory blood flow by dilating small arteries, thus promoting the production of granulation tissue and accelerating the incision healing. At the same time, it can reduce incisional edema and bacterial accumulation.20 For those with severe mediastinitis, chronic osteomyelitis, refractory infection, subcutaneous infection spreading to the sternum and contaminating the metallic line, the opening approach should be adopted. After a few days of sternal debridement, daily dressing changes, and cleaning of the incision, the therapeutic method of bilateral pectoralis major flap edge loosening and translation should be applied to eliminate the sternal cavity in time, promote the healing of subcutaneous tissue, and promote the discharge of exudate, with an efficiency of 96%.21
There are some limitations in this study. Due to the relative fragmentation of sternotomy infection cases after OPCABG, there is a lack of evidence from large randomized controlled trial studies. Additionally, the sample size of patients in group with DSWI is too small for comparison with patients without DSWI.
Conclusion
In this study, we found that the morbidity of DSWI undergoing OPCABG was 6.89% with an intra-group mortality rate of 15.6%. Additionally, obesity, history of DM, prolonged operation time and tracheal intubation time, time of stay in CCU, utilization of blood product and secondary thoracotomy were DSWI independent risk factors after OPCABG. We should implement multimodal preventive measure to reduce the incidence of DSWI after OPCABG, such as shorter operation time and tracheal intubation time, reducing the utilization of blood product.
Abbreviations
OPCABG, Off pump coronary artery bypass grafting; COPD, Chronic Obstructive Pulmonary Disease; SSWI, superficial sternal wound infection; DSWI, deep sternal wound infection.
Ethics
This study was conducted with approval from the institutional review committee of General Hospital of Ningxia Medical University. This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Funding
This study was supported by The Ningxia Hui Autonomous Region key research and development plan in the field of social development projects (The general project, No: 2021BEG03070) In 2021.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gummert JF, Barten MJ, Hans C, et al. Mediastinitis and cardiacsurgery-an updated risk factor analysis in 10,373 consecutive adult patients. Thorac Cardiovasc Surg. 2002;50(2):87–91. doi:10.1055/s-2002-26691
2. Floros P, Sawhney R, Vrtik M, et al. Risk factors and management approach for deep sternal wound infection after cardiac surgery at a tertiary medical centre. Heart Lung Circ. 2011;20(11):712–717. doi:10.1016/hlc.2011.08.001
3. Kirmani BH, Mazhar K, Saleh HZ, et al. External validity of the Society of Thoracic Surgeons risk stratification tool for deep sternal wound infection after cardiac surgery in a UK population. Interact Cardiovasc Thorac Surg. 2013;17(3):479–484. doi:10.1093/icvts/ivt222
4. Kubota H, Miyata H, Motomura N, et al. Deep sternal wound infection after cardiac surgery. J Cardiothorac Surg. 2013;8:132. doi:10.1186/1749-8090-8-132
5. Bryan CS, Yarbrough WM. Preventing of deep wound infection after coronary artery bypass grafting: a review. Tex Heart Inst J. 2013;40(2):125–139.
6. Gardlund B, Bitkover CY, Vaage J. Postoperative mediastinitis in cardiac surgery-microbiology and pathogenesis. Eur J Cardiothorac Surg. 2002;21(5):825–830. doi:10.1016/S1010-7940(02)00084-2
7. Mekontso-Dessap A, Vivier E, Girou E, et al. Effect of timeto onset on clinical features and prognosis of post-sternotomy mediastinitis. Clin Microbiol Infect. 2011;17(2):292–299. doi:10.1111/.1469-0691.2010.03197
8. Chen LF, Arduino JM, Sheng S, et al. Epidemiology and outcome of major postoperative infections following cardiac surgery: risk factors and impact of athogen type. Am J Infect Control. 2012;40(10):963–968. doi:10.1016/j.ajic.2012.01.012
9. Gui Y, Shang Y, Long D, et al. Risk factors for sternal incision infection after cardiac surgery. Chongqing Med. 2019;48(15):2681–2683.
10. Ma J, An J, Wang W, et al. Clinical manifestations and etiological characteristics of deep sternal incision infection after cardiac surgery. J China Med Univ. 2016;45(7):635–640.
11. Sun Z, Zhu Y, Xu G, et al. Regression analysis of the risk factors for post operative nosocomial infection in patients with abdominal tumors: experience from a larger cancer centre in China. Drug Discover. 2015;9(6):411–416.
12. Zhu D, Chen H, Li J, et al. Clinical treatment of mediastinal infection after cardiac surgery with negative pressure sealing drainage combined with sternal fixation system. Guangzhou Med. 2018;52(5):30–34.
13. Kwon S, Thompson R, Dellinger P, Yanez D, Farrohki E, Flum D. Importance of periop-erative glycemic control in general surgery report from the Surgical Care and outcomes Assessment Program. Ann Surg. 2013;257(1):8–14. doi:10.1097/SLA.0b013e31827b6bbc
14. Umpierrez G, Cardona S, Pasquel F, et al. Randomized controlled trial of intensive versus conservative glucose control in patients undergoing coronary artery bypass graft surgery: GLUCOCABG trial. Diabetes Care. 2015;38(9):16651672.
15. Bláha J, Mráz M, Kopecký P. Perioperative tight glucose control reduces postoperative adverse events in nondiabetic cardiac surgery patients. J Clin Endocrinol Metab. 2015;100(8):3081–3089. doi:10.1210/jc.2015-1959
16. Meihui Y, Qingyang Y, Qinghua L. Causal analysis and nursing countermeasures of 45 cases of deep sternal incision infection after cardiac operation. Fujian Med J. 2016;38(5):145–146.
17. Xue W. Analysis of Risk Factors and Pathogens of Wound Infection After Cardiac Surgery and Its Prevention and Control Strategy. Tianjin: Tianjin Medical University; 2018.
18. Bojar RM. Perioperative Management of Adult Cardiac Surgery [M]. Beijing: Science Press; 2007:618–619.
19. Kaspersen AE, Nielsen SJ, Orrason AW, et al. Short and long-term mortality after deep sternal wound infection following cardiac surgery: experiences from SWEDEHEART. Eur J Cardio. 2021;60(2):233–241.
20. Tang P, Li Z, Cen Y, et al. Thoracic wall reconstruction for deep sternal incision infection. Chin J Plastic Surg. 2019;37;(07):810–816.
21. Huo X, Yi L, Wang J, et al. Clinical analysis of unilateral pectoralis major transplantation in the treatment of deep sternal incision infection after early cardiac surgery. Chin J Clin Physicians. 2020;49(07):829–831.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.