")
Back to Journals » Patient Preference and Adherence » Volume 16
Analysis of Related Factors of Coping Styles in Infertile Patients in Central China
Authors Mao J, Guo H, Wang J, Li Y, Xu M
Received 16 March 2022
Accepted for publication 14 June 2022
Published 2 July 2022 Volume 2022:16 Pages 1605—1612
DOI https://doi.org/10.2147/PPA.S364345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Jing Mao,1 Huiping Guo,2 Juan Wang,1 Ying Li,1 Meng Xu1
1Department of Reproductive Medicine, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China; 2Nursing College, Henan University of Chinese Medicine, Zhengzhou, People’s Republic of China
Correspondence: Jing Mao, Department of Reproductive Medicine, the First Affiliated Hospital of Henan University of Chinese Medicine, No. 19 Renmin Road, Jinshui District, Zhengzhou, 450000, People’s Republic of China, Tel +86-18703657086, Email [email protected]
Objective: To investigate the psychosocial factors, including personality characteristics, coping style, social support and alexithymia of infertile patients, and explore the relevant factors regarding the medical coping style choice of infertile patients in central China.
Methods: Sixty infertile patients in the reproductive medicine centre in our hospital were investigated using a self-made general situation questionnaire; internal control, powerful others and opportunities scale; social support rating scale; and medical coping questionnaire, and the data was analysed.
Results: Of the 60 infertile patients, 57 (95%) were female, with an average age of 27.85 ± 14.52 years old, and 42 (70%) had secondary infertility. The score of the face dimension was lower than the norm (19.17 ± 2.18 vs 19.43 ± 3.82, P = 0.012), and those of the avoidance (15.98 ± 2.43 vs 14.41 ± 2. 94, P = 0.030) and yield (9.48 ± 3.19 vs 8.83 ± 3.19, P = 0.012) dimensions were higher than the norm. The multiple linear regression analysis showed that internal control and the utilisation of support were influencing factors for the coping style (R2 = 0.271, adjusted R2 = 0.144, F = 9.827, P < 0.001), and internal control was the influencing factor for the avoidance coping style (R2 = 0.024, adjusted R2 = 0.021, F = 3.363, P = 0.014). The education level, opportunity and utilisation of support factors influenced the yield dimension (R2 = 0.087, adjusted R2 = 0.076, F = 7.749, P < 0.001).
Conclusion: Considering the association between the coping styles and psychosocial factors, it was recommended to formulate targeted intervention strategies based on these influencing factors to guide patients to adopt positive coping styles and achieve good outcomes.
Keywords: infertility, coping style, psychosocial factors, relevance
Introduction
Infertility refers to the situation when couples who have had sex for at least 12 months without contraception do not become pregnant. It is a group of fertility disorders with various causes and is an adverse reproductive health event for couples of childbearing age.1 Infertility refers to fertility problems of couples of childbearing age in various countries and regions across the world. Recently, the prevalence of infertility has increased significantly due to environmental pollution.2 It is reported that an average of 15% of couples are infertile.3 The incidence rate of infertility is 8–33% in the United States, 13.2% in Iran4 and approximately 7–10% in China.1 Previous studies have shown that the age of Chinese infertile patients is between 25 to 30 years old, which shows a younger trend.5
Infertility is a reproductive health defect, and more than 80% of infertile couples bear great psychological pressure, especially infertile women.6,7 Infertile women in China often feel inferior and crowded due to the influence of China’s traditional culture.4 In addition, the heavy economic burden of infertility, complex treatment process and uncertainty of treatment lead to poor mental health. Continuous psychological stress leads to not only a series of psychological problems, such as long-term depression, anxiety, paranoia and interpersonal sensitivity8,9 but also the decline of marital life quality, changes in sexual life and reduced pregnancy and childbirth rates.1 Therefore, increasing scholars suggest that medical workers should pay attention to the psychological pressure and emotional response of infertile women.10
Therefore, the purpose of this study is to investigate the current situation regarding the medical coping style choice of infertile patients and explore whether the psychological locus of control and social support have an impact on the choice of coping style. This will provide a theoretical basis for improving patients’ psychological elasticity and guiding them to adopt a positive coping style.
Methods
Participants
Sixty infertile patients who were treated in the reproductive medicine centre of our hospital from September 2021 to November 2021 were selected as the research subjects. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The First Affiliated Hospital of Henan University of Chinese Medicine. All patients agreed to participate in this study. The inclusion criteria are as follows: (1) meet the WHO diagnostic criteria for infertility;11 (2) aged between 20–40 years old; (3) the ability to read and fill in by yourself; and (4) voluntary participation in the survey. The exclusion criteria are as follows: (1) those who refuse to cooperate after the researcher explains the study; (2) cognitive and communication barriers; (3) patients with other severe diseases; and (4) those who have experienced major life events during the past six months. Sixty infertile patients were investigated using a general questionnaire; internal control, powerful others and opportunities scale; social support rating scale (SSRs); and medical coping questionnaire.
Research Methods
The cross-sectional survey method was adopted to select the survey objects using convenient sampling to explain the research purpose, methods and confidentiality principles to them, issue the questionnaire after consent and enable them to fill in it alone and return it after 20 minutes.
(1) General information questionnaire: This was prepared by the researcher and included gender, education level, family residence type, education level, infertility type and treatment time. Due to the uncertainty and complexity of the specific causes of infertility, we divided the patients into primary infertility and secondary infertility groups.
(2) Internal control, powerful others and chance scale (IPC): this scale was compiled by Levenson in 1972 and consists of the following three subscales: the internal control scale (I), which measures the extent to which people can control their own lives; the influential others scale (P), which tests whether individuals believe that others can control events in their lives; and the opportunity scale (C), which measures the individual’s belief that opportunities can affect their own life experiences and things. The IPC scale is widely used in the field of psychology in China and has been proved to have good reliability and validity.12
(3) SSRs: This was designed by Xiao Shuiyuan in 1986 according to China’s national conditions. The scale is comprehensively evaluated from the following three dimensions: subjective support, objective support and utilisation of social support. The score shows the level of individual social support. The scale is widely used in social support-related studies in China, and the scale has been confirmed to have good reliability and validity.13
(4) Medical coping modes questionnaire: This questionnaire was prepared by Feifel et al, and the Chinese version was revised by Jiang Qianjin et al. It includes the following three dimensions: face, avoidance and yield, with a total of 20 items. Each item is scored according to levels 1–4, of which eight items are scored in reverse. The higher the cumulative score of each dimension, the more inclined the dimension is to this coping style. The reliability and validity of the revised Chinese version of the scale are acceptable and suitable for the evaluation of Chinese patients.14
Statistical Analysis
After the questionnaire was collected, the scores of each scale and dimension were calculated, and all the steps were checked by two people. The data was presented as descriptive statistics using SPSS 26.0, and a t-test was used for intergroup comparisons and expressed as mean ± standard deviation (x ± s). A single factor analysis was used for general data; a Pearson correlation analysis was used between the dimensions of the questionnaire; the statistically significant variables of the single factor analysis and correlation analysis were used as independent variables; and the dimensions of the medical coping questionnaire were used as dependent variables for the multiple linear stepwise regression analysis.
Results
After 60 questionnaires were distributed, 60 questionnaires were recovered, and zero invalid questionnaires were excluded. There were 60 valid questionnaires in total, and the effective questionnaire rate was 100%.
Basic Data of 60 Infertile Patients
The basic data of 60 infertile patients are shown in Table 1. Most patients were female (95%) and had a college or undergraduate degree (56.67%). Secondary infertility was the main type of infertility (70%) in the population, with a range of treatment times.
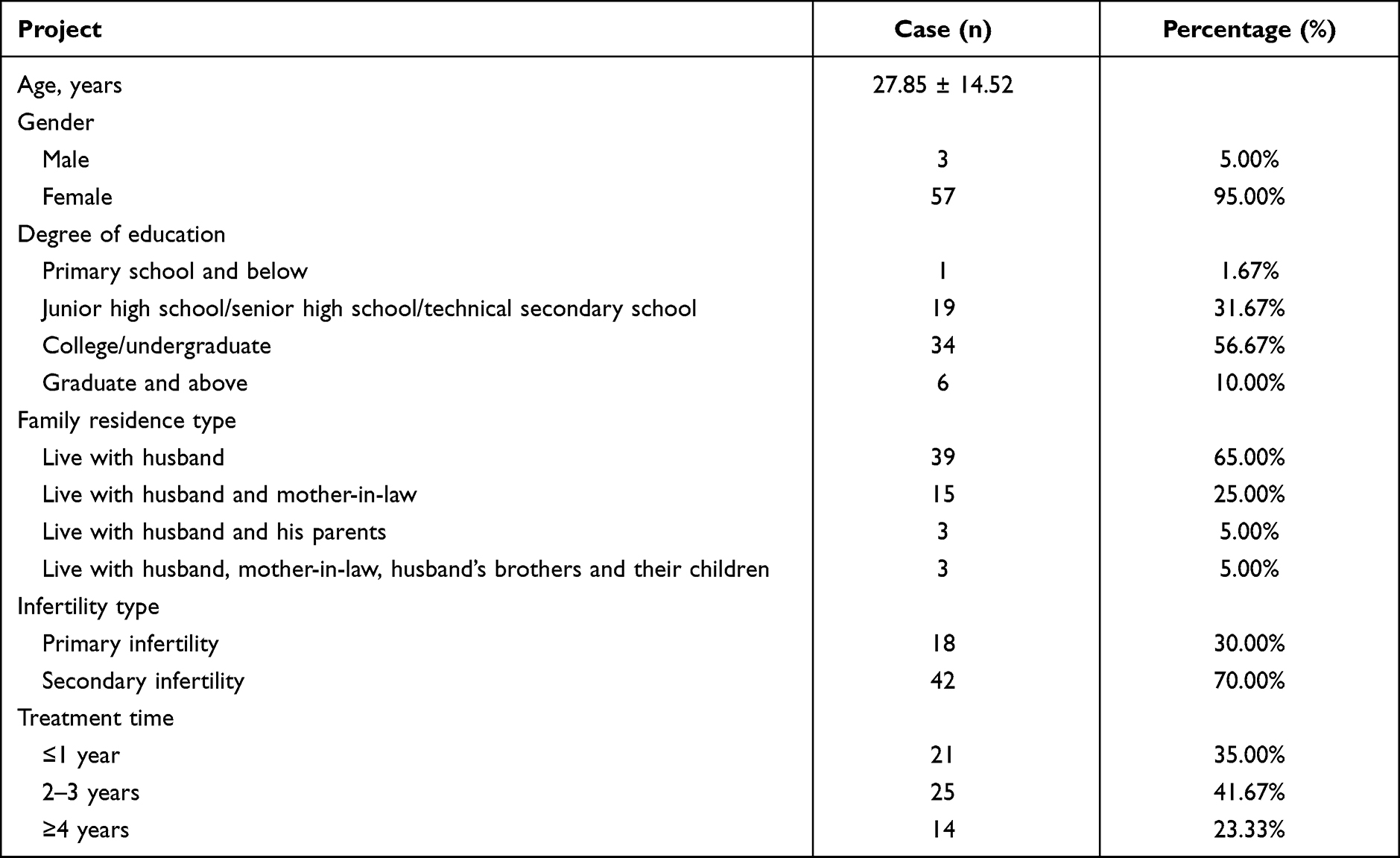 |
Table 1 Basic Data of Infertile Patients |
Scores of Each Dimension of the Medical Coping Scale and Comparison with Norm
Compared to the norm, there was a significant difference in the face (19.17 ± 2.18 vs 19.43 ± 3.82), avoidance (15.98 ± 2.43 vs 14.41 ± 2.94) and yield (9.48 ± 3.19 vs 8.83 ± 3.19) dimensions in the medical coping scale (P < 0.05 for all) (see Table 2 for the specific results).
 |
Table 2 Scores of Each Dimension of Medical Coping Scale and Comparison with the Norm |
Total Score and Each Dimension Score of the Internal Control, Powerful Others and Opportunities Scale and SSRs
For the 60 infertile patients, the overall scores of the internal control, powerful others and opportunities scale, social support assessment scale, each dimension and the items of each dimension are shown in Table 3.
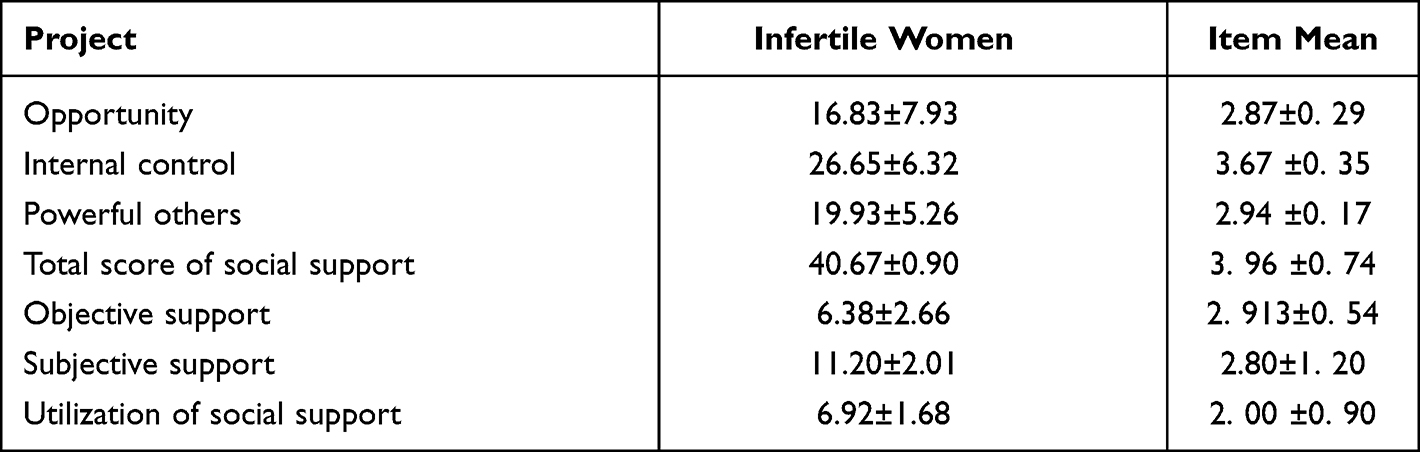 |
Table 3 Total Scores and Dimensions of Internal Control, Powerful Others and Opportunities Scale and Social Support Rating Scale |
Univariate Analysis of the General Data of Each Dimension in the Medical Coping Questionnaire
In the univariate analysis of the general data of each dimension of the medical coping questionnaire, there was a statistically significant difference in the education level of the face dimension (P < 0.05). Additionally, there was a significant difference in the family living environment in the avoidance (P < 0.05) and treatment time (P < 0.05) dimensions (see Table 4 for specific results).
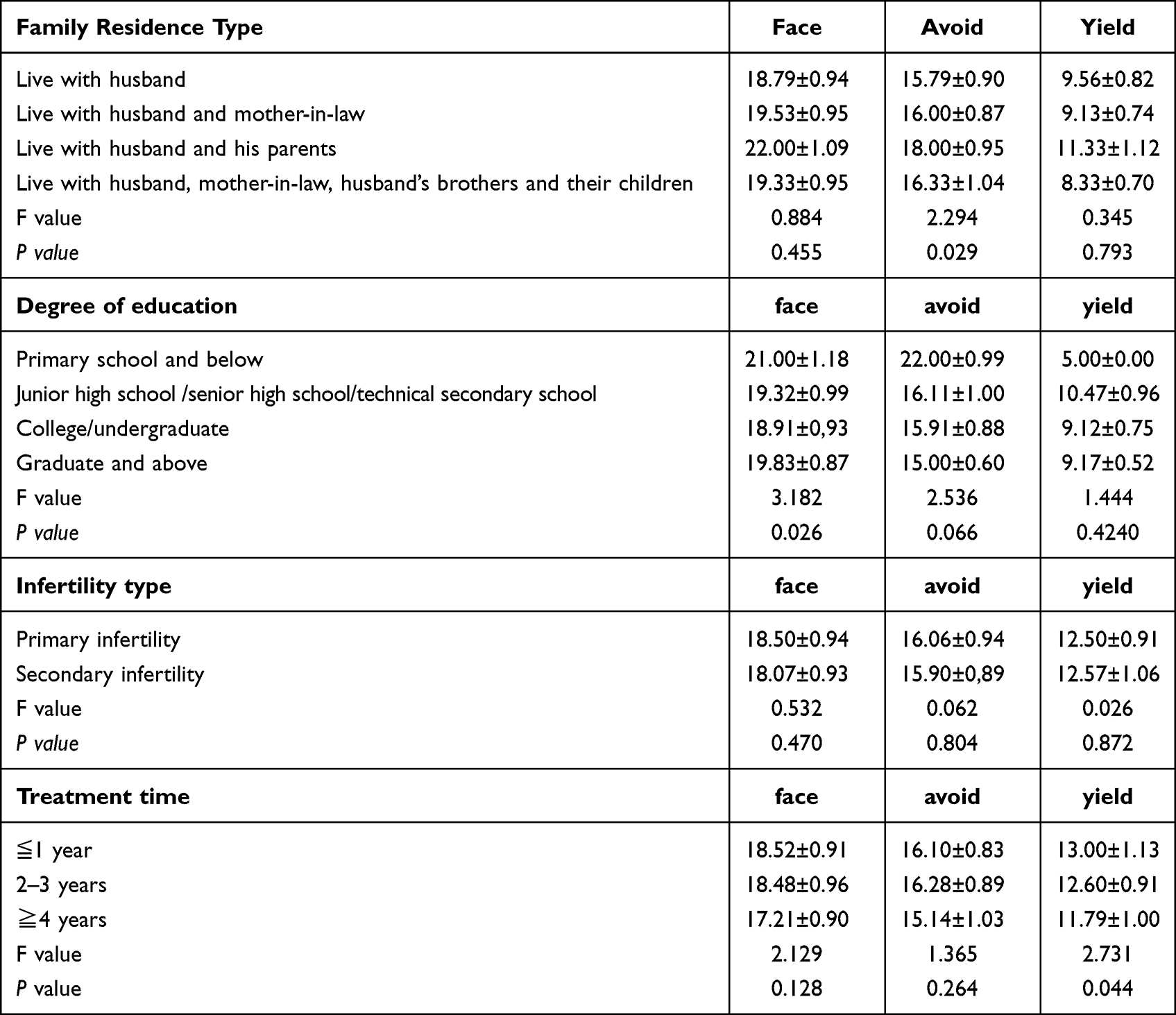 |
Table 4 Univariate Analysis of General Data of Each Dimension in Medical Coping Questionnaire |
Correlation Analysis of the Medical Coping Style, Locus of Control and Social Support
According to the results of the Pearson analysis, the face dimension of the medical coping style is significantly correlated with the internal control and total scores of social support, objective support, subjective support and utilisation of social support. Moreover, the avoidance dimension is significantly correlated with the internal control, and the yield dimension is significantly correlated with opportunity and utilisation of support (see Supplemental Table 1 for specific results).
Multiple Linear Regression Analysis of the Medical Coping Styles of Infertile Women
The multiple linear regression analysis showed that internal control and utilisation of support were the influencing factors of the medical coping style (R2 = 0.271, adjusted R2 = 0.144, F = 9.827, P < 0.001) (see Supplemental Table 2 for specific results), internal control was the influencing factor for the avoidance coping style (R2 = 0.024, adjusted R2 = 0.021, F = 3.363, P = 0.014) (see Supplemental Table 3 for specific results) and age, opportunity and utilisation of support were the influencing factors of the yield coping style (R2 = 0.087, adjusted R2 = 0.076, F = 7.749, P < 0.001) (see Supplemental Table 4 for specific results).
Discussion
In this study, we explored the relationship between various psychosocial factors and coping styles in patients with infertility in central China using questionnaires with IPC scales. The main findings were as follows: 1) internal control and the utilisation of support were the influencing factors of the coping style; 2) internal control was associated with the avoidance coping style; and 3) education level, opportunity and utilisation of support were the influencing factors of yield. When patients believe that their infertility is the result of luck and fate, they feel that their condition is uncontrollable and struggle to believe that treatment will bring positive results. Therefore, they showed minimal cooperation in the treatment of infertility stress, depression and anxiety. Previous studies have shown that coping styles may have adverse effects on the quality of life and well-being of patients and the outcomes of fertility treatment.15–17 The present study further emphasised the importance of psychosocial factors in coping styles, and personalised treatment was recommended for infertile patients to achieve better pregnancy outcomes.
Current Situation of Infertile Patients
In this study, the patients’ ages ranged from 20 to 40 years, with an average age of 27.85 ± 14.52 years. The minimum age was 20 years, and the maximum age was 40 years. Moreover, 76.2% of them were under 30 years old, which is consistent with the data in the survey report on the current situation of infertility that was issued by China Population Association in 2012,18 which verifies that infertility patients in China tend to be younger. With the release of the second-child policy, the number of elderly female patients with infertility is gradually increasing. Regarding the type of family residence, 65.0% of nuclear families only live with their husbands. Most women are influenced by China’s traditional fertility ideas and place great psychological pressure on themselves. It is worth noting that self-esteem, depression, guilt, anxiety, emotional distress and communication problems are common in infertile couples.19,20 In a previous study on infertile individuals, although 50.5% of participants had no anxiety, 19%, 17.5%, 11% and 2% of participants had mild, moderate, severe and very severe anxiety, respectively.21 In addition, infertile women are more likely to have severe physical and mental disabilities and a worse quality of life.22
Disease Characteristics
In this study, there are 18 cases of primary infertility (30.0%) and 42 cases of secondary infertility (70.0%). The proportion of unexplained causes in primary infertility is the highest, and the fallopian tube factor is the primary cause of secondary infertility. The fallopian tube loses its normal physiological function due to chronic pelvic inflammation.23 Uterine cavity operation and the neglect of reproductive health are the main causes of chronic pelvic inflammatory disease. Most infertility years are two to three years (41.67%), which could reflect the strong medical awareness of female infertility patients, timely and early treatment and the urgent requirement of fertility.
Multivariate Analysis of the Coping Styles of Infertile Patients
Education Level
In this study, female infertility patients with high education levels had better adaptability. Patients with a high education level usually have a wide range of knowledge, are understanding and can accept new knowledge, understand more infertility-related knowledge, seek medical treatment formally and confirm that the problem of infertility is not completely caused by women. Moreover, such patients generally have relatively stable work, fixed incomes and light economic burdens. Generally, for patients with a low education level, their families have a limited understanding of new knowledge and infertility diseases. Additionally, the low family status will increase pressure, produce negative emotions and affect the intimacy and adaptability of family relations.24
Type of Family Residence
The type of family residence means that the patients who live with their husband and parents have better family intimacy, which may be due to the patients who live with more relatives and friends of their parents in law and men. The conflict that is caused by the different treatment opinions that are provided by different family members will affect the family’s emotional status, and the long-term energy consumption will reduce the patient’s family intimacy.25 Therefore, when intervening with these patients’ families, we should actively communicate with them, carry out relevant publicity and education, and help them to understand that they should care more about their patients in real life, respect their choices and form a good atmosphere for the whole family.
Current Situation Regarding the Medical Coping Styles of Female Infertility Patients
Research shows that female infertility patients use avoidance coping strategies more than the domestic norm. Avoidance refers to indifference and a dilution attitude towards stress events, which is a negative coping method. This shows that as infertility still causes psychological problems for many women, they adopt the avoidance coping method to reduce and avoid adverse psychological emotions. Research shows that female infertility patients tend to adopt the avoidance coping style. The positive coping style, which is conducive to the physical and mental health of patients and the treatment and rehabilitation of diseases, can alleviate anxiety, depression and other adverse emotions.26
Psychological Intervention Measures for Infertile Patients
Provide Sufficient Information About Support
Nursing staff should design targeted information on support according to the different health knowledge needs and levels of infertile patients, such as general knowledge about reproduction, common causes of infertility, assisted reproductive technology and possible adverse reactions. It should also be noted that in work, we should pay attention to emotional communication with patients. Instead of mechanically explaining and guiding the patients, one should listen to the patient, show sympathy and understanding for the patient’s condition and provide gentle and appropriate suggestions so that the patient feels emotional care. Then, one should take the initiative to obtain disease-related knowledge and reduce the patient’s level of disease uncertainty.
Have a Positive Response
When communicating with infertile patients, nurses should encourage patients to adopt positive coping styles, such as talking with the surrounding people, participating in collective activities and listening to others’ suggestions, to help patients gain more social support and reduce patients’ negative emotions, such as anxiety and fear. Moreover, patients should be reminded to avoid waiting, dependence and other negative avoidance methods, as these may hinder patients’ access to social support, worsen their physical and mental health and increase the level of disease uncertainty. Relevant domestic research results show that through the intermediary protection of social support, a positive coping style can effectively reduce patients’ bad psychological stress and level of disease uncertainty, improve their overall marriage and life quality and increase their pregnancy rate.27
Provide Sufficient Social Support
Studies have shown that there are many sources of social support, such as their spouse, children, relatives, friends, colleagues, medical personnel and sick friends. Among them, their family provides basic social support, and their spouse, children, other relatives and friends provide social support. By working together, they can effectively reduce the level of disease uncertainty of infertile patients. In addition, social support nursing can expand the social support network of patients to a certain extent. Moreover, medical staff can impart health knowledge to patients, which is conducive to obtaining more support and encouragement through other ways. Social support nursing not only meets the spiritual needs of patients but also gives patients positive support through their emotional experience.
Limitations
The sample size of this study is small, and it did not conduct a more in-depth study on the proposed interventions, which is a limitation of this paper.
Conclusion
To summarise, different locus of control and social support dimensions will lead to different coping styles of infertile patients during medical treatment. Considering the association between coping styles and psychosocial factors, targeted treatment was recommended for these infertile patients to improve their compliance and achieve better outcomes.
Implications
Appropriate intervention methods can guide patients to adopt positive coping methods during diagnosis and treatment and help them to obtain satisfactory pregnancy outcomes.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of The First Affiliated Hospital of Henan University of Chinese Medicine. All participants were informed about the purpose of the study. Written informed consent was obtained from all participants.
Funding
1. Special Project of Chinese Medicine Scientific Research in Henan Province No.20-21ZY2178. 2. The ninth key discipline of Henan province- Nursing of Henan University of Chinese Medicine.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Fan X, Liu LH, Ai H. Current situation and analysis of medical humanities education for postgraduates majoring in obstetrics and Gynecology. J Jinzhou Med Univ. 2021;19(05):63–65.
2. Chiang C, Mahalingam S, Flaws JA. Environmental Contaminants Affecting Fertility and Somatic Health. Semin Reprod Med. 2017;35(3):241–249.
3. Stevenson TL, Lashen H. Empty follicle syndrome: the reality of a controversial syndrome, a systematic review. Fertil Steril. 2008;90(3):691–698.
4. Frederiksen Y, Farver-Vestergaard I, Skovgård NG, Ingerslev HJ, Zachariae R. Efficacy of psychosocial interventions for psychological and pregnancy outcomes in infertile women and men: a systematic review and meta-analysis. BMJ Open. 2015;5(1):e006592.
5. Li XY, Gu XY. Fertility status and challenges in China [J]. China Family Planning Obstetrics Gynecol. 2020;12(1):97–98.
6. Malina A, Błaszkiewicz A, Owczarz U. Psychosocial aspects of infertility and its treatment. Ginekol Pol. 2016;87(7):527–531.
7. Iris A, Aydogan Kirmizi D, Taner CE. Effects of infertility and infertility duration on female sexual functions. Arch Gynecol Obstet. 2013;287(4):809–812.
8. Romeiro J, Caldeira S, Brady V, Timmins F, Hall J. Spiritual aspects of living with infertility: a synthesis of qualitative studies. J Clin Nurs. 2017;26(23–24):3917–3935.
9. Klonoff-Cohen H, Natarajan L. The concerns during assisted reproductive technologies (CART) scale and pregnancy outcomes. Fertil Steril. 2004;81(4):982–988.
10. Gdańska P, Drozdowicz-Jastrzębska E, Grzechocińska B, Radziwon-Zaleska M, Węgrzyn P, Wielgoś M. Anxiety and depression in women undergoing infertility treatment. Ginekol Pol. 2017;88(2):109–112.
11. Qian K. Study on stigma and its influencing factors of infertile women [D]. Wannan Med College. 2019;1:548.
12. Xiao L, Chen ZG. A preliminary analysis of College Students’ locus of control structure and IPC scale [J]. Appl Psych. 1989;02:22–27.
13. Xiao SY. Theoretical basis and research application of social support rating scale [J]. J of Clin Psychiatry. 1994;02:98–100.
14. Shen XH, Jiang QJ. Test report of 701 cases of medical coping style questionnaire Chinese version [J]. Chin J of Behav Med. 2000;1:22–24.
15. Ghaheri A, Shahrokhabadi MS, Zayeri F, et al. Relationship among life satisfaction, anxiety and fertility quality of life in women[J]. Koomesh. 2016;17(4):957–965.
16. Maroufizadeh S, Ghaheri A, Samani RO, et al. Psychometric properties of the satisfaction with life scale (SWLS) in Iranian infertile women[J]. Int J Reprod Biomed. 2016;14(1):57–62.
17. Csemiczky G, Landgren BM, Collins A. The influence of stress and state anxiety on the outcome of IVF-treatment: psychological and endocrinological assessment of Swedish women entering IVF-treatment[J]. Acta Obstet Gynecol Scand. 2015;79(2):113–118.
18. Huang M, Huang MY. Research progress on the correlation between anxiety, depression and quality of life of infertile patients. General Nursing. 2017;15(33):4125–4126.
19. Vitale SG, La Rosa VL, Rapisarda AM, et al. Psychology of infertility and assisted reproductive treatment: the Italian situation. J Psychosom Obstet Gynecol. 2017;38:1–3.
20. Maroufizadeh S, Karimi E, Vesali S, et al. Anxiety and depression after failure of assisted reproductive treatment among patients experiencing infertility. Int J Gynaecol Obstet. 2015;130:253–256.
21. Peyvandi S, Hosseini SH, Daneshpour MM, et al. The prevalence of depression, anxiety and marital satisfaction and related factors in infertile women referred to infertility clinics of Sari city in 2008. J Mazandaran Univ Med Sci. 2011;20:26–32.
22. Sezgini H, Hocaoglu C, Guvendag-Gven ES. Disability, psychiatric symptoms, and quality of life in infertile women: a cross-sectional study in Turkey. Shanghai Arch Psychiatr. 2016;28:86–94.
23. Hodgson RM, Lee HL, Wang R, Mol BW, Johnson N. Interventions for endometriosis-related infertility: a systematic review and network meta-analysis. Fertil Steril. 2020;113(2):374–382.e2.
24. Patel A, Sharma PSVN, Kumar P, Binu VS. Sociocultural Determinants of Infertility Stress in Patients Undergoing Fertility Treatments. J Hum Reprod Sci. 2018;11(2):172–179.
25. Rooney KL, Domar AD. The relationship between stress and infertility. Dialogues Clin Neurosci. 2018;20(1):41–47.
26. Li D. Study on the interaction between fertility pressure and its influencing factors in infertile couples [D]. Hubei Medical College. 2020;1:15.
27. Kitchen H, Aldhouse N, Trigg A, Palencia R, Mitchell S. A review of patient-reported outcome measures to assess female infertility-related quality of life. Health Qual Life Outcomes. 2017;15(1):86.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.