")
Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
Analysis of Patients with Focal Epilepsy and Drug-Resistant Epilepsy in Italy: Evaluation of Their Characteristics, Therapeutic Pathway and the Consumption of Healthcare Resources
Authors Perrone V, Veronesi C, Dovizio M, Ancona DD, Andretta M, Bartolini F, Cavaliere A, Chinellato A, Ciaccia A, Cillo M, De Francesco A, Enieri N, Ferrante F, Gentile S, Procacci C , Ubertazzo L, Vercellone A, Lucatelli D, Procaccini M, Degli Esposti L
Received 9 February 2022
Accepted for publication 7 July 2022
Published 28 July 2022 Volume 2022:14 Pages 513—521
DOI https://doi.org/10.2147/CEOR.S361692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Giorgio Colombo
Valentina Perrone,1 Chiara Veronesi,1 Melania Dovizio,1 Domenica Daniela Ancona,2 Margherita Andretta,3 Fausto Bartolini,4 Arturo Cavaliere,5 Alessandro Chinellato,6 Andrea Ciaccia,7 Mariarosaria Cillo,8 Adele De Francesco,9 Nicola Enieri,6 Fulvio Ferrante,10 Simona Gentile,11 Cataldo Procacci,2 Loredana Ubertazzo,12 Adriano Vercellone,13 Domenico Lucatelli,14 Michela Procaccini,14 Luca Degli Esposti1
1CliCon S.r.l., Società Benefit-Health, Economics & Outcomes Research, Bologna, Italy; 2Dipartimento Farmaceutico, ASL BAT, Andria, Italy; 3UOC Assistenza Farmaceutica Territoriale, Azienda ULSS 8 Berica, Vicenza, Italy; 4Dipartimento Farmaceutico, USL Umbria 2, Terni, Italy; 5Farmaceutica Aziendale, ASL Viterbo, Viterbo, Italy; 6Unità Operativa Farmacia Ospedaliera, ULSS 3 Serenissima, Mestre, Italy; 7ASL Foggia, Foggia, Italy; 8Dipartimento Farmaceutico, ASL Salerno, Salerno, Italy; 9Azienda Ospedaliero-Universitaria “Mater Domini”, Catanzaro, Italy; 10ASL Frosinone, Frosinone, Italy; 11Direzione Generale per la Salute, Campobasso, Italy; 12ASL Roma 4, Civitavecchia, Roma, Italy; 13ASL Napoli 3 sud, Napoli, Italy; 14Angelini Pharma, Roma, Italy
Correspondence: Valentina Perrone, CliCon S.r.l., Società Benefit-Health, Economics & Outcomes Research, Via Murri 9, Bologna, 40137, Italy, Tel +39 3450316494, Email [email protected]
Purpose: A retrospective analysis was conducted to estimate the number of patients with focal epilepsy and drug-resistant epilepsy (DRE) and their characteristics, the therapeutic patterns, the consumption of health resources in a real-world Italian setting.
Patients and Methods: A retrospective study was carried out on the administrative databases of a sample of Italian Health Departments, covering approximately 8.7 million health-assisted individuals. All adult patients with at least one hospitalization for focal epilepsy and an electroencephalogram (between 01/2010 and 12/2019), and at least one prescription of antiseizure medication (ASM) (between 01/2011 and 12/2018) were included in the study. Patients with at least two treatment failures and treated with a subsequent ASM were considered DRE.
Results: Overall, 1897 patients with focal epilepsy (mean age 56 years, 47% male) were identified, of which 485 (25.6%) with DRE (mean age 53 years, 43% male). Among patients with focal epilepsy and DRE, respectively, 48% and 54% had essential hypertension, 23.4% and 26.6% had cardiovascular disease, and 46.3% and 62.1% had peptic ulcer/prescription of gastric secretion inhibitors. During follow-up, patients with focal epilepsy maintained first-line treatment for 53.9 months; among these, 52% passed to the second-line, and 485 (25.6% of the total) began third-line treatment. In patients with focal epilepsy, the mean cost was € 4448 (of which € 1410 were epilepsy-related), and in DRE patients total expenditures averages € 5825 (of which € 2165 were epilepsy-related). In both patients with focal epilepsy and DRE, hospitalizations represented the most impacting item of expenditure.
Conclusion: The present analysis conducted in a setting of Italian clinical practice has shown that 25% of patients with focal epilepsy were resistant to antiepileptic treatments. Furthermore, these results showed that health-care costs for the management of epileptic patients were mainly accountable for the costs related to the disease-management and to hospitalizations.
Keywords: epilepsy, real-world evidence, clinical practice, pharmacoutilization, healthcare resource consumption
Introduction
Epilepsy is one of the most common chronic severe neurological disorders, affecting approximately 68 million people worldwide.1 It usually manifests as infantile (epileptic) spasms or focal seizures during the first year of life. Focal epilepsy remains the most frequent form after the first year of life.2 Many patients with epilepsy have significant disabilities and severe physical, neuropsychological complications.3 Since epilepsy is a fairly common clinical condition affecting all ages and requiring long-term treatment, thus it is associated with high health-care costs for health systems.4 Conventional treatment for epilepsy is based on the long-term administration of antiseizure medications (ASM).5 Today, the pharmacological armamentarium against epilepsy is very complex and includes several drugs.6 Although polytherapy with antiepileptic drugs results in long-term seizure remission in most patients, about 30% of patients do not achieve remission with currently available ASM and are defined as patients with refractory or refractory drug-resistant epilepsy (DRE).7,8 These individuals sustained the physical and psychological consequences of uncontrolled seizures with a heavy drug burden and an increased mortality.9 In addition, the management of DRE patients in some cases required non-pharmacological treatment, especially surgery.10
It has been well recognized that epilepsy is a disease with a pronounced societal and healthcare impact.11 The high health-care costs are related to assessment and treatment, surgery and hospitalization for seizures, lost employment, income, and household work.12 These costs vary according to the severity of the condition, response to treatment, length of time since diagnosis.11 However, the economic impact of epilepsy and the real impact of drug-resistant epilepsy have been poorly quantified, and few studies are available up to now, particularly in Italy.
Thus, the present retrospective analysis aimed to estimate the number of patients with focal epilepsy and drug-resistant epilepsy, their therapeutic pathway, and the economic burden of the disease, in terms of the consumption of health resources and the related direct costs, in a real-world Italian setting.
Materials and Methods
Data Source
This is an observational study based on data extracted from the administrative databases from different Italian Entities, distributed among the Italian territory, covering approximately 8.7 million inhabitants. Within the administrative flows, the anonymous univocal numeric code assigned to each patient allowed the electronic linkage of all subjects’ records across the databases. Specifically, data-linkage was performed among the following databases: demographic database (to collect data on patients’ demographic), pharmaceutical database [to collect data on prescription drugs reimbursed by the Italian National Health System (NHS), in terms of related Anatomical-Therapeutic Chemical (ATC) code, and prescription date], hospitalization database [to give information on discharge diagnoses at any level classified according to the International Classification of Diseases, 9-th Revision, Clinical Modification (ICD-9-CM) and date of diagnosis], outpatient diagnostic tests and specialist visits database (contains the date of prescription, type, description of diagnostic tests and procedure for patients in analysis), and exemption database [to collect data on date and type of exemption code]. For the current study, Italian entities databases were selected by their geographical distribution, by data completeness, and by the high-quality linked datasets. The anonymous univocal numeric code ensured total compliance with the European General Data Protection Regulation (GDPR) (2016/679). No identifiers related to patients were provided to the authors. All the results of the analyses were produced as aggregated summaries, and thus data cannot be assigned, either directly or indirectly, to a single institution, department, doctor, individual, or individual prescribing behaviors. Based on the Privacy Guarantor Authority general authorization for personal data treatment for scientific research purposes– n.9/2014, informed consent was not required, as its collection would be impossible for organizational reasons. According to the Italian law on the conduction of observational analyses, the ethics committee of each participating entity was notified and approved the study (Supplementary Table 1).
Study Design
Among the study population, all adult patients with a diagnosis of focal epilepsy were enrolled. Focal epilepsy was identified by the presence of all the following criteria (the applied methodology was previously reported and validated):13,14 i) the presence of at least one hospitalization discharge diagnosis at primary or secondary level for focal epilepsy (ICD-9-CM codes are listed in the Supplementary Table 2) evaluated during all study period from January 2010 to December 2019; ii) the presence of at least one prescription for an ASMs (ATC codes: N03A, N05BA09), with the first ASM prescribed as a monotherapy with at least 60 days’ supply (evaluated during the inclusion period, ie, from January 2011 to December 2018); and iii) the presence of at least one electroencephalogram (EEG) (ICD-9-CM procedure code 89.14) evaluated during all study period from January 2010 to December 2019. Among patients with focal epilepsy, those with at least two failed ASM treatment lines and in third-line treatment at the inclusion time were defined as patients with DRE. For focal epileptic patients, the index date was the date of first ASM prescription during the inclusion period; while for DRE patients the date of prescription of third-line ASM was defined as the index-date. All patients were followed-up for all available period (at least one year) after the index-date.
Analysis of Baseline Characteristics
For all patients included in the study, baseline characteristics in terms of age, sex, previous hospitalizations and treatments, during the characterization period (12 months prior index-date) were evaluated. Comorbidities and clinical manifestations were identified by hospital discharge diagnosis, the exemption code and/or the prescription of specific medications. In line with the recent literature,15 the presence of the following diagnoses/treatments were evaluated: use of anti-dementia medications (by at least one prescription of drugs with ATC code N06D); use of antimigraine preparations (at least of one prescription of drugs with ATC code N02C); hypertension [identified by at least one hospitalization with a discharge diagnosis for essential hypertension (ICD-9-CM code 401) or at least one prescription of antihypertensive drugs (ATC codes: C02, C03; C07; C08; C09)]; previous cardiovascular disease [identified by at least one hospitalization with a discharge diagnosis for ischemic heart disease (ICD-9-CM codes: 410, 411, 413, 414), cardiac dysrhythmias ICD-9-CM code: (ICD-9-CM code: 427), heart failure (ICD-9-CM code: 428), cerebrovascular disease (ICD-9-CM codes: 430, 431, 432, 433, 434, 435, 436, 437, 438), atherosclerosis and aneurysm (ICD-9-CM code: 440–442), and other peripheral vascular disease (ICD-9-CM codes: 443)]; tumors [identified by at least one hospitalization with a discharge diagnosis for malignant neoplasms, stated or presumed to be primary, of specified sites, except of lymphatic and hematopoietic tissue (ICD-9-CM codes: 140–195), malignant neoplasms, stated or presumed to be secondary, of specified sites (ICD-9-CM codes: 196–198), malignant neoplasms, without specification of site (ICD-9-CM code: 199), malignant neoplasms, stated or presumed to be primary, of lymphatic and hematopoietic tissue (ICD-9-CM codes: 200–208), neuroendocrine tumors (ICD-9-CM code: 209)]; peptic ulcer/use of gastric secretion inhibitors [identified by at least one hospitalization with a discharge diagnosis for gastric, duodenal, peptic (site unspecified), or gastrojejunal ulcer (ICD-9-CM codes: 531–534), or at least one hospitalization with a procedure for control of hemorrhage and suture of ulcer of stomach or duodenum (ICD-9-CM codes: 44.4), or at least one prescription of drugs for peptic ulcer and gastro-esophageal reflux disease (ATC code A02B)]; arthritis (identified by at least one hospitalization with a discharge diagnosis for diffuse diseases of connective tissue (ICD-9-CM codes: 710–719)).
Pharmaco-Utilization Analysis and Treatment Sequences
Treatment sequences were evaluated in terms of ASM treatment lines. ASM treatment lines were identified based on the prescription of a different ASM (respect to the index medication) as by the replacement of the current ASM (switch) or as a drug addition to the current ASM (add-on). The switch, the add-on or the prescription of a new ASM with respect to the existing therapy, marked the beginning of a new treatment line; discontinuation of treatment and elimination of ASM from the combination therapy did not mark the beginning of a new line.
Analysis of Healthcare Resources Consumptions and Related Direct Costs
In all alive patients during the first year of follow-up, the healthcare resource consumption (per patients) was evaluated in terms of drug treatments, hospitalizations admissions, and outpatient specialized services (laboratory tests, specialistic visits, diagnostic procedures). Overall direct medical costs in Euros (€) were related to the following resource consumption: hospitalizations (determined by using the DRGs tariffs) and epilepsy-related hospitalizations (considering ICD-9-CM codes: 345.90; 345.91), drug costs (evaluated for those drugs reimbursed by the Italian NHS and using the NHS purchase price) and ASM-related costs, and the outpatient specialist service costs (accordingly to Regional tariffs) and EEG-costs. Data were reported as the mean annual healthcare cost per patient.
Statistical Analysis
All analyses were descriptive. Continuous variables were reported as mean±standard deviation (SD); categorical variables were expressed as numbers and percentages. All analyses have been performed using STATA SE version 17.0 (StataCorp LLC, College Station, TX, USA).
Results
During the study period and among the study population of 8.7 million of health-assisted individuals, 11,562 (0.1%) patients with at least one hospitalization discharge diagnosis for focal epilepsy were identified (Figure 1). Among them, 9204 (79.6%) had at least one ASM prescription. Overall, 1897 adult patients (which represents 0.02% of the study population) affected by focal epilepsy were included. Among them, 485 (25.6%) were identified as DRE patients (Figure 1). The baseline characteristics of patients are reported in Table 1. In focal epilepsy and DRE patients, respectively, the age at the inclusion averaged 56 and 53 years, and 47% and 43%, respectively, were males. 48% of focal epilepsy patients and 54% of DRE patients had hypertension, 46% of focal epilepsy patients and 62% of DRE patients had peptic ulcer/prescription of gastric secretion inhibitors, and 23% and 26% of focal epileptic and DRE patients, respectively, had previous cardiovascular events (Table 1). Almost 4% and 7% of focal epileptic and DRE patients had a diagnosis of cancer, respectively (Table 1).
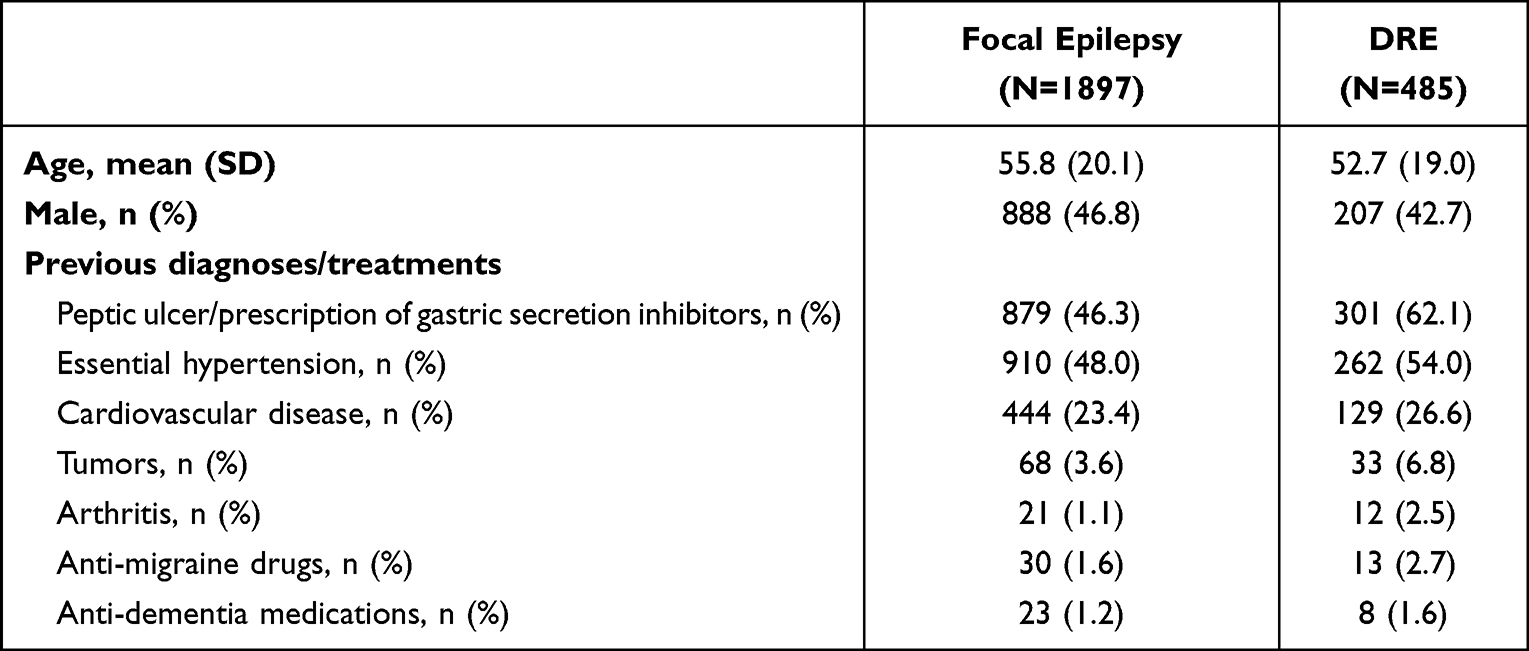 |
Table 1 Baseline Demographic and Clinical Characteristics of Patients with Focal Epilepsy and DRE |
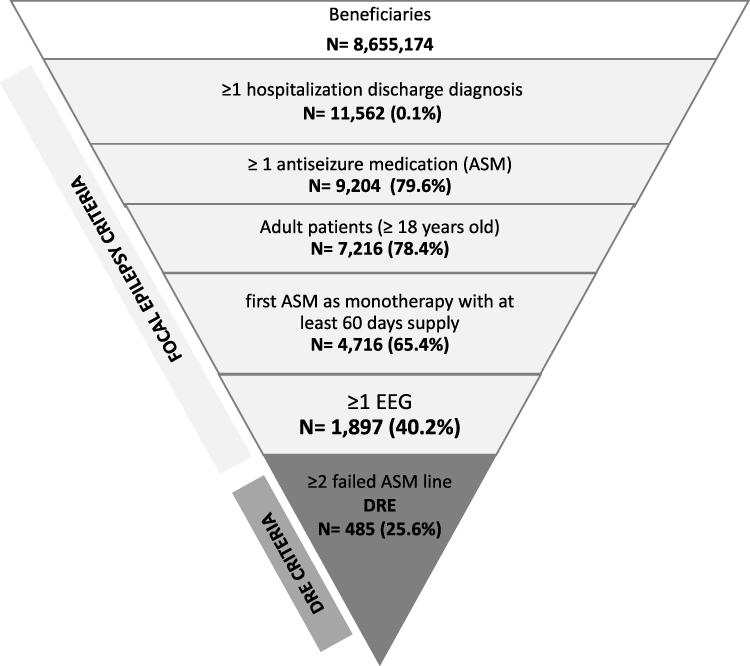 |
Figure 1 Flow-chart for the identification patients with focal epilepsy and DRE. |
The evaluation of treatment sequences in focal epileptic patients is reported in Table 2. During the follow-up, overall 1897 of focal epileptic patients were in first-line treatment and remained in first-line for a mean period of 54 months, and the most prescribed medications were levetiracetam (42.8% of patients), carbamazepine (13.8%), valproic acid (11.0%) (Supplementary Figure 1). Among patients starting the first-line, 988 patients (52%) started a second-line treatment [specifically 759 patients had an add-on treatment, while 229 switched therapy]; patients remained in the second line with a mean duration of 29 months. In the group of patients in second-line therapy, during the follow-up, 485 patients (25.6 of overall focal epilepsy patients) passed to third-line treatment [301 patients had an add-on treatment and 184 switched the therapy]; these patients were defined as DRE and remained in the third line for an average period of 25 months (Table 2). During the first year of follow-up, the mean/annual consumption of health-care resources for patients with focal epilepsy was (mean ± SD): 20.1 ± 11.8 of drug prescriptions, 7.4±7.6 outpatient specialized services prescriptions, and 0.7±1.1 hospitalizations. In DRE patients, the mean/annual consumption of health-care resources was 26.7±15.1 of drug prescriptions, 8.5±7.9 outpatient specialized services prescriptions, and 0.8±1.1 hospitalizations (Table 3). For the management of focal epileptic patients, the average annual total cost amounted to € 4448, of which € 1410 were epilepsy-related; specifically, 1237 € were related to drugs (540 € for ASM consumptions), 740€ to outpatient specialized services (and 17€ to EEG specifically), and 2470 € to hospitalizations (with 853 € for epilepsy-related hospitalizations) (Figure 2A). Regarding the management of DRE patients, a tendency of increase of annual total cost was found: € 5825, of which € 2165 were epilepsy-related; specifically, 1837 € were related to drugs (1144 € for ASM consumptions), 1017 € to outpatient specialized services (and 13€ to EEG specifically), and 2971 € to hospitalizations (with 1009 € for epilepsy-related hospitalizations) (Figure 2B).
 |
Table 2 Evaluation of Treatment Sequences During the Follow-Up Among Included Patients |
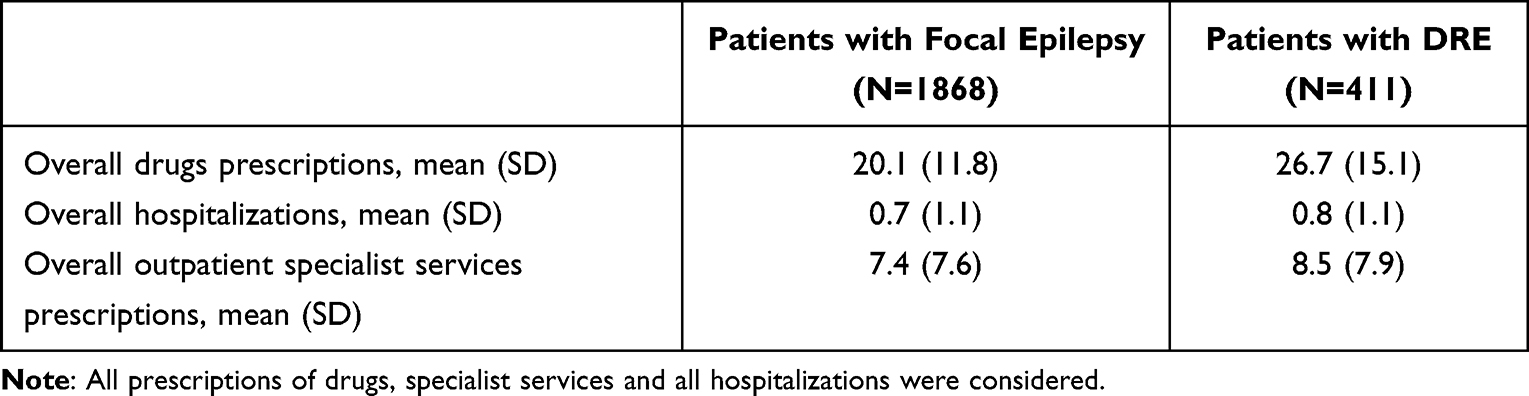 |
Table 3 Healthcare Resource Consumptions in Alive Patients During the First Year of Follow Up |
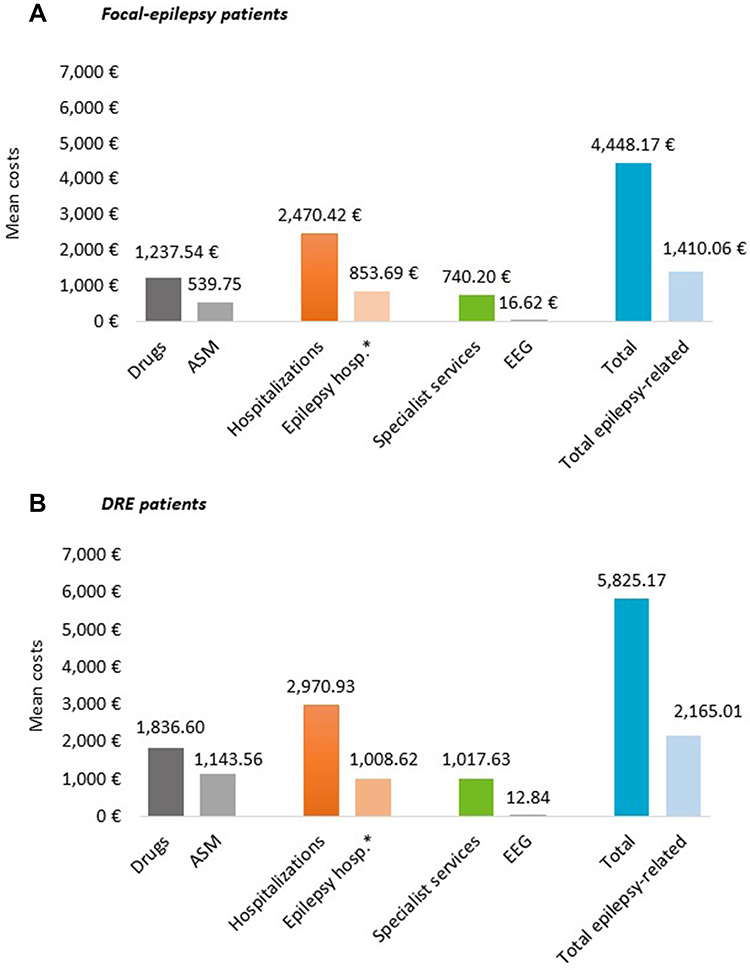 |
Figure 2 Overall and epilepsy-related direct healthcare costs during first year of follow up, in patients with focal epilepsy (A) and DRE (B). Abbreviations: ASM, antiseizure medication; EEG, electroencephalogram. Notes: Patients with at least 1 year of follow-up (deaths excluded). *ICD-9-CM codes: 345.90; 345.91 included. |
Discussion
The present analysis of real-world data among the Italian population estimated the number of patients affected by focal epilepsy and by DRE, their therapeutic pathway, and the economic burden associated with the disease management.
Overall, about 1900 patients with a diagnosis of focal epilepsy during the study period were identified, and among them almost 490 patients were affected by the drug-resistant form. The proportion of patients with DRE was found to be 25% of overall patients with focal epilepsy, in line with previously published evidence.7–9 The analysis of clinical characteristics of patients enlightened a significant portion of epileptic patients being affected by numerous comorbidities, such as hypertension, cardiovascular disease, and using several co-medications, ie, inhibitors of gastric secretion, anti-dementia drugs, and anti-migraine agents. Large-population studies report that several diseases, including depression, anxiety, dementia, migraine, heart disease, peptic ulcers, and arthritis, are up to eight times more common in people with epilepsy than in the general population,15–17 thus defining a high comorbidity burden in these patients.15 In particular, in the present analysis, diagnoses of hypertension and of cardiovascular disease were found in almost 50% and 23% of focal epilepsy patients, respectively. Data from an observational study among US population has reported that hypertension accounted in almost 12% of epileptic patients,18 while in survey-based analysis 24–34% of patients with focal epilepsy were also affected by hypertension, 15% by stroke and 10–18% by heart disease.15 The higher prevalence of hypertension and cardiovascular disease found in the present analysis could be attributable by the fact that late-onset patients were enrolled based on hospitalization for focal-epilepsy and ASM prescription.
The therapeutic pathway of focal epileptic patients showed that only half of the patients remained in first-line treatment during years, and a half passed to the second-line. Among patients in the second line, almost half passed to the third-line treatment, and these are drug-resistant patients. The progression among lines (second and third line) accounted for the most of patients (60–70%) for the addition of ASM to the current therapeutic plan. This tendency in epilepsy clinical practice could be explained by several findings. In a recent large hospital cohort study over the past two decades, it has been reported that combination therapy was associated with a progressive increase in seizure-free rate than monotherapy in DRE patients.19 The benefits of polytherapy in the management of DRE might be related to the recent introduction of many new ASMs with different and novel mechanisms of action and better pharmacokinetic and tolerability profiles.19 Therefore, polytherapy, including these new ASMs in the regimen, is the approved mode of DRE management, and this has prompted physicians to try various combinations of polytherapy to optimize the clinical outcomes.19
The estimation of the economic burden in focal epilepsy patients and especially in those with DRE has shown that during the one-year follow-up, high healthcare resource consumptions was found, mainly related to the high number of drug prescriptions. These data could be explained by the polytherapy regimen adopted for DRE patients but also by the presence of a high rate of comorbidities/clinical manifestations among epileptic patients. In our cohorts, the management of epilepsy was associated with a high annual cost, especially in patients with DRE, of which a considerable portion was related to medications and hospitalizations and to epilepsy-related health-care resources. These data are in line with a previous observational study that stated that the costs of epilepsy vary significantly according to the time course of the disease and the response to treatment,3,20 with hospital admissions (probably for surgery procedures)10 and drugs (ie, polytherapy) being the major sources of expenditure. In addition, it has been reported that a significant fraction of the drug costs is attributable to the new ASMs, and the spending on ASMs has been estimated to be increasing at a rate of 10% per year in developed countries.21
The limitations of the present analysis were related to its retrospective and observational nature and to the use of anonymized data derived from administrative databases. Although administrative databases have progressively improved data collection, in terms of accuracy and completeness, some information may be missing or incorrectly reported. In case the necessary information is missing for a given patient, that patient has been discarded from the analysis. Our cohorts of patients reflected real clinical practice by evaluating data from a sub-set of health-assisted individuals. Primary care data were not collected for this study; therefore, it was not possible to assess the primary care-based management of the patients in the analysis. In addition, there was a lack or limited clinical information on comorbidities, and other potential confounders that could have influenced the present results. Since the comorbidities herein analyzed were addressed based on any available data before inclusion (using proxy of diagnosis), there might be incomplete capture of these variables among patients. Data on pharmacological treatments were captured from medical prescription and dispensing information, and the reason of treatment switch has not been retrievable from the database. Moreover, since the availability of patients’ clinical data are scarce, thus the assumption of the stay in first-line treatment as a seizure-free state could represent a study limitation. Another limitation could be represented by the fact that among epilepsy-related healthcare resource consumptions, epilepsy surgery and hospitalization for EEG monitoring to presurgical evaluation were not evaluated as outpatient EEGs. Moreover, in the present analysis, patients from the inpatient setting have been included, thus mostly patients with more severe motor onset seizures that require hospitalized care have been identified.
Conclusion
In conclusion, this retrospective observational study among the Italian population describes the characteristic of patients affected by focal epilepsy, their therapeutic management, and the disease economic burden. Among epileptic patients, almost a quarter had the drug-resistant form, being in the third-line of treatment. The healthcare resource consumptions and costs for patient’ management were mainly derived from hospitalizations and drug-related expenditure. Our finding suggested that the management of epilepsy still represents substantial health and economic burden, and improving seizure control and reducing the economic burden, especially in refractory epilepsy, still remain an important unmet medical need.
Acknowledgments
Angelini Pharma purchased the study report that is the basis for this manuscript. This manuscript was developed by CliCon S.r.l. Società Benefit and sponsored by Angelini Pharma. The agreement signed by Clicon S.r.l. Società Benefit and Angelini Pharma S.p.A. does not create any entityship, joint venture or any similar relationship between parties. Clicon S.r.l. Società Benefit is an independent company. Neither CliCon S.r.l. Società Benefit nor any of their representatives are employees of Angelini Pharma for any purpose.
Disclosure
V Perrone, C Veronesi, M Dovizio, DD Ancona, M Andretta, F Bartolini, A Cavaliere, A Chinellato, A Ciaccia, M Cillo, A De Francesco, N Enieri, F Ferrante, S Gentile, C Procacci, L Ubertazzo, A Vercellone, and L Degli Esposti report no conflicts of interest in this work. D Lucatelli and M Procaccini are employees of Angelini Pharma, Italy. The authors report no other conflicts of interest in this work.
References
1. Ngugi AK, Bottomley C, Kleinschmidt I, et al. Estimation of the burden of active and life-time epilepsy: a meta-analytic approach. Epilepsia. 2010;51:883–890. doi:10.1111/j.1528-1167.2009.02481.x
2. Chu-Shore CJ, Major P, Camposano S, et al. The natural history of epilepsy in tuberous sclerosis complex. Epilepsia. 2010;51:1236–1241. doi:10.1111/j.1528-1167.2009.02474.x
3. Beghi E, Garattini L, Ricci E, et al. Direct cost of medical management of epilepsy among adults in Italy: a prospective cost-of-illness study (EPICOS). Epilepsia. 2004;45:171–178. doi:10.1111/j.0013-9580.2004.14103.x
4. Beghi E. Addressing the burden of epilepsy: many unmet needs. Pharmacol Res. 2016;107:79–84. doi:10.1016/j.phrs.2016.03.003
5. Bialer M, White HS. Key factors in the discovery and development of new antiepileptic drugs. Nat Rev Drug Discov. 2010;9:68–82. doi:10.1038/nrd2997
6. Perucca E. The pharmacological treatment of epilepsy: recent advances and future perspectives. Acta Epileptologica. 2021;3:22. doi:10.1186/s42494-021-00055-z
7. Kwan P, Schachter SC, Brodie MJ. Drug-resistant epilepsy. N Engl J Med. 2011;365:919–926. doi:10.1056/NEJMra1004418
8. Kwan P, Brodie MJ. Early identification of refractory epilepsy. N Engl J Med. 2000;342:314–319. doi:10.1056/NEJM200002033420503
9. Kwan P, Brodie MJ. Refractory epilepsy: a progressive, intractable but preventable condition? Seizure. 2002;11:77–84. doi:10.1053/seiz.2002.0593
10. Engel J, Wiebe S, French J, et al. Practice parameter: temporal lobe and localized neocortical resections for epilepsy: report of the Quality Standards Subcommittee of the American Academy of Neurology in Association with the American Epilepsy Society and the American Association of Neurological Surgeons. Neurology. 2003;60:538–547. doi:10.1212/01.wnl.0000055086.35806.2d
11. Allers K, Essue BM, Hackett ML, et al. The economic impact of epilepsy: a systematic review. BMC Neurol. 2015;15:245. doi:10.1186/s12883-015-0494-y
12. Cockerell OC, Hart YM, Sander JW, et al. The cost of epilepsy in the United Kingdom: an estimation based on the results of two population-based studies. Epilepsy Res. 1994;18:249–260. doi:10.1016/0920-1211(94)90045-0
13. An S, Malhotra K, Dilley C, et al. Predicting drug-resistant epilepsy - a machine learning approach based on administrative claims data. Epilepsy Behav. 2018;89:118–125. doi:10.1016/j.yebeh.2018.10.013
14. Franchi C, Giussani G, Messina P, et al. Validation of healthcare administrative data for the diagnosis of epilepsy. J Epidemiol Community Health. 2013;67:1019–1024. doi:10.1136/jech-2013-202528
15. Keezer MR, Sisodiya SM, Sander JW, et al. Comorbidities of epilepsy: current concepts and future perspectives. Lancet. 2016;15:106–115. doi:10.1016/S1474-4422(15)00225-2
16. Gaitatzis A, Sisodiya SM, Sander JW. The somatic comorbidity of epilepsy: a weighty but often unrecognized burden. Epilepsia. 2012;53:1282–1293. doi:10.1111/j.1528-1167.2012.03528.x
17. LaFrance WC, Kanner AM, Hermann B. Psychiatric comorbidities in epilepsy. Int Rev Neurobiol. 2008;83:347–383.
18. Wilner AN, Sharma BK, Soucy A, Thompson A, Krueger A. Common comorbidities in women and men with epilepsy and the relationship between number of comorbidities and health plan paid costs in 2010. Epilepsy Behav. 2014;32:15–20. doi:10.1016/j.yebeh.2013.12.032
19. Park KM, Kim SE, Lee BI. Antiepileptic drug therapy in patients with drug-resistant epilepsy. J Epilepsy Res. 2019;9:14–26. doi:10.14581/jer.19002
20. Owczarek K, Jedrzejczak J. Ekonomiczne aspekty padaczek opornych na leczenie [Economic aspects of drug-resistant epilepsy]. Neurol Neurochir Pol. 2001;35:309–318.
21. Porter R. Economic factors in the development of new antiepileptic drugs. Adv Neurol. 1998;76:239–244.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.