")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Analysis of Factors Influencing Depression in Elderly People Living with HIV/AIDS Based on Structural Equation Model: A Cross-Sectional Study in Guangxi, China
Authors He K , Zhang X, Yang D, Fu X, Chen Y, Chen Z , Mo J, Zhou L, Xu F, Jiang X, Shi W, Cao L, Li Y
Received 16 March 2023
Accepted for publication 22 May 2023
Published 29 May 2023 Volume 2023:16 Pages 1491—1501
DOI https://doi.org/10.2147/JMDH.S410538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Kailian He,1,2,* Xiashuang Zhang,1,2,* Dong Yang,3 Xiaofeng Fu,3 Yulu Chen,1,2 Ziqi Chen,1,2 Jinglin Mo,3 Lingmi Zhou,3 Fang Xu,3 Xiuli Jiang,3 Wuxiang Shi,4 Liang Cao,1,5 You Li1,2
1Department of Environmental Health and Occupational Medicine, School of Public Health, Guilin Medical University, Guilin, Guangxi, 541199, People’s Republic of China; 2Guangxi Health Commission Key Laboratory of Entire Lifecycle Health and Care (Guilin Medical University), Guilin, Guangxi, 541199, People’s Republic of China; 3Department of AIDS Control and Prevention, Guilin Center for Disease Control and Prevention, Guilin, Guangxi, 541000, People’s Republic of China; 4Health Management Unit, Faculty of Humanities and Management, Guilin Medical University, Guilin, Guangxi, 541199, People’s Republic of China; 5Department of Experimental Teaching Center, School of Public Health, Guilin Medical University, Guilin, Guangxi, 541199, People’s Republic of China
*These authors contributed equally to this work
Correspondence: You Li; Liang Cao, Email [email protected]; [email protected]
Purpose: The purpose of our study is to understand the current status of depression and medical social support in elderly HIV/AIDS, as well as the role of social support on depression, so as to provide a certain reference for reducing the occurrence of depression in the population.
Methods: A total of 115 participants with PLWHA (people living with HIV/AIDS) aged 50 years or older were collected in Guilin from December 2021 to July 2022. Depression and medical social support were assessed using the Center for Streaming Depression Scale (CES-D) and the Medical Social Support Scale (MOS-SSS). The structural equation model was used to examine the relationship between medical social support and depression.
Results: Sixty-one of 115 participants developed depressive symptoms with a prevalence of 53.0%. The results of univariate analysis showed that ethnicity, health status, mean monthly income, antiviral treatment status, and medical social support influenced PLWHA depression (P< 0.05). Simple linear regression showed that health status (95% CI: − 9.901~-2.635), and antiviral treatment status (95% CI: − 12.969~-3.394) influent depression (P< 0.05). There were associations between total medical social support, practical support dimension, message and emotional support dimension, social interactive cooperation dimension, emotional support dimension and depression (unadjusted and adjusted for contextual factors) (P < 0.05). Using multiple linear regression analyses, we found that medical-social support was negatively associated with depression with a standardized effect value of − 0.223. PLWHA with higher medical social support had lower prevalence of depression.
Conclusion: The results indicate that the prevalence of depression among HIV/AIDS patients in Guilin is high. So the joint efforts of individuals, families, and society are needed to improve the physical and mental health of the PLWHA.
Keywords: older people living with HIV/AIDS, medical social support, depression, structural equation model, SEM
Introduction
Acquired immune deficiency syndrome (AIDS) is a pervasive chronic infectious disease caused by the human immunodeficiency virus (HIV) that is emerged as a pressing global public health concern. According to the Joint United Nations Programme on HIV/AIDS (UNAIDS), there were 1.5 million new HIV infections and 650,000 AIDS-related deaths globally in 2021, with an estimated 38.4 million people living with HIV by the end of 2021.1 Data from the Chinese Health Care Commission showed that 60,154 cases including 19,623 deaths of AIDS were reported nationwide in 2021.2 The vast body of scholarship on HIV/AIDS focuses on diverse facets ranging from epidemiology, clinical management, prevention to mental health.3 Depression is the second most prevalent psychiatric disorder in the world and is prevalent among people living with HIV. The global prevalence of depression among HIV-infected patients was 31% (28%~34%), with the highest 44% (35%~53%) in South America and lowest 22% (17%~27%) in Europe.4 The prevalence of depression among HIV/AIDS patients is 48.8% in China.5 Depression not only impairs the social function of the patients6,7 and reduces the quality of life8 but also decreases medication adherence in HIV/AIDS patients.9 This behavior eventually leads to the worsening of the disease. Studies have found that age, gender, economic income, and medical social support all can influence the depression.10,11
Medical social support influences people’s social lives and constitutes as an effective coping mechanism. Some scholars found that medical social support for AIDS patients was at an intermediate level, with an average score of 53.63.12 High levels of medical social support can alleviate the psychological stress of patients. In particular, the elderly PLWHA, an isolated and marginalized group with a low level of medical social support, was more prone to psychological problems as they bear pressure alone.13 Giving patients appropriate care and support can reduce their psychological burden.14 Therefore, understanding the medical social support of elderly HIV/AIDS patients and the relationship between medical social support and depression is of great importance to reduce the occurrence of depression.
In this study, we used the Medical Social Support Scale (MOS-SSS) and the Center for Streaming Depression Scale (CES-D) to investigate the current status of medical social support and depression in older adults with HIV/AIDS. The results help us to understand the current status of depression and medical social support in older adults and the effect of medical social support on depression. These findings will provide the theoretical basis for reducing the occurrence of depression in PLWHA and improving their mental health.
Materials and Methods
Study Population
Form December 2021 to July 2022, a convenience sampling method was utilized to procure a sample of 115 HIV/AIDS patients aged 50 years and above in Guilin, Guangxi. The survey was conducted by staffs from the CDC AIDS Section. The recruitment of participants was restricted to those who were undergoing follow-up at the AIDS unit, and the confidentiality of all information pertaining to the subjects was ensured criteria for the study subjects were as follows. Inclusion criteria were including 1) the HIV antibody test being positive, 2) age ≥50 years, 3) voluntarily participating in the study, 4) having some reading comprehension and completing the questionnaire independently. Exclusion criteria for the study subjects were as follows: 1) those with severe visual and hearing impairment or low reading ability who could not correctly understand the purpose and content of the research project. 2) those with severe acute or chronic physical illnesses that resulted in functional impairment and could not participate in the interview. 3) those who were unwilling to participate in our study.
Research Tools
We collected the information on sociodemographic characteristics, including age, gender, ethnicity, marital status, education level, occupation, personal health status, average monthly personal income, household registration (living in rural or urban areas), BMI (kg/m2), antiviral treatment status, duration of infection, CD4+cell count (cells/mm3), whether to get tested for HIV, sexual behavior, chronic disease conditions with the questionnaire.15,16
Depression was measured using the Center for Streaming Depression Scale (CES-D), which was designed by the Center for Research on the Epidemiology of Aging at the National Institute of Mental Health (Chinese version),17 with a total of 20 items. The scale contains four dimensions: depressed mood (1st, 3rd, 6th, 9th, 10th, 14th, 17th, and 18th items), positive emotions (4th, 8th, 12th, and 16th items), somatic symptoms and activity delay (2nd, 5th, 7th, 11th, 13th, and 20th items) and interpersonal dimension (15th and 19th items). The CES-D scale is scored on a 4-point Likert scale from 0 (never) to 3 (always), in which 4 items are scored inversely from 0 (always) to 3 (never). The sum of the individual item scores is the total depression score, which ranges from 0 to 60. There is no specific depression score, and the score of ≥16 is generally considered to indicate the risk of depression, the magnitude of the score directly correlates with the likelihood and severity of depression.
The Medical Outcomes Study Social Support Survey, or MOS-SSS scale, was designed by Sherburne & Stewart.18 Our study used the Chinese version, which improved by the Chinese scholar Li Huan in 2012,12 and the validity reached 0.95. The questionnaire consists of four dimensions with 20 items: tangible support (2nd, 5th, 12th, and 15th items), informational and emotional support (3rd, 4th, 8th, 9th, 13th, 16th, 17th, and 19th items), positive social interaction (7th, 11th, 14th, and 18th items), and affectionate support (6th, 10th, and 20th items). The first item is a subjective question that measures the size of the patient’s support network, and the 2nd to 20th items are objective questions which are scored from 1 to 5 depending on the degree of occurrence, with a score of 1 indicating not at all, 2 indicating a little, 3 indicating some, 4 indicating most, and 5 indicating all. The total score ranges from 19 to 95, with higher scores indicating higher levels of medical social support.
Statistical Analysis of the Data
The data were double inputted in parallel with Epidata v3.1. Continuous variables were expressed as the mean±standard deviation ( ). The Kolmogorov‒Smirnov test was used to assess the normality continuous variables. Data conforming to a normal distribution was compared between the two groups with t-test, and categorical variables were expressed as frequencies (percentages) and were analyzed by chi-square test. Following the univariate analysis, simple linear regression was used to further investigate the relationship with each of the background variables that was significant in the univariate analysis and depressive symptoms. The relationship between medical social support and depressive symptoms in patients with HIV/AIDS were examined using a set of simple and multivariate linear regressions. Then, the relationship between medical social support and depression was briefly analyzed with Pearson correlation analysis. Finally, we analyzed the relationship between medical social support and depression using structural equation modeling (SEM). SEM is a statistical analysis method combined with matrix modeling, mainly applies in the fields of economics, psychology. It attempts to use the empirical information collected by the researcher to confirm the relationship among the hypothesized latent variables. The statistical analyses were performed using SPSS26.0 and AMOS24.0 statistical packages, and a two-sided test p value ≤ 0.05 was considered statistically significant.
). The Kolmogorov‒Smirnov test was used to assess the normality continuous variables. Data conforming to a normal distribution was compared between the two groups with t-test, and categorical variables were expressed as frequencies (percentages) and were analyzed by chi-square test. Following the univariate analysis, simple linear regression was used to further investigate the relationship with each of the background variables that was significant in the univariate analysis and depressive symptoms. The relationship between medical social support and depressive symptoms in patients with HIV/AIDS were examined using a set of simple and multivariate linear regressions. Then, the relationship between medical social support and depression was briefly analyzed with Pearson correlation analysis. Finally, we analyzed the relationship between medical social support and depression using structural equation modeling (SEM). SEM is a statistical analysis method combined with matrix modeling, mainly applies in the fields of economics, psychology. It attempts to use the empirical information collected by the researcher to confirm the relationship among the hypothesized latent variables. The statistical analyses were performed using SPSS26.0 and AMOS24.0 statistical packages, and a two-sided test p value ≤ 0.05 was considered statistically significant.
Ethics Review
All study subjects signed an informed consent form before the survey, and the subjects voluntarily accepted the questionnaire. This study conformed to the principles of the Declaration of Helsinki and was approved by the Ethics Committee of Guilin Medical University (GYLL2021078).
Results
Sociodemographic Characteristics of HIV/AIDS Patients Over 50 Years of Age
The study included 115 individuals aged 50 years or above. Sixty-one participants (accounting for 53.0%) exhibited symptoms of depression. The mean depression score for all participants was 18.0±10.3, with the depression-free group scoring 9.6±3.0 and the probable depression group scoring 25.4±8.9. The male and female ratio was 63.5% and 36.5%, respectively, and the mean age of the participants was 61.2±7.1 years. Of the total sample, 80.9% of participants were Han, while the remaining 19.1% belonged to ethnic minorities. This difference was statistically significant between the probable depression group and normal group (P<0.05). A total of 53% of participants reported poor physical health, whereas 47% reported their physical health to be relatively good, with the difference being statistically significant (P<0.05). The participants exhibited relatively low income, with 28.7% earning more than $2000 per month, 45.2% earning less than $1000, and 26.1% earning between $1000 and $2000, and the differences were statistically significant (P<0.05). The majority of PLWHA (82.6%) were receiving antiviral therapy, while only 17.4% had never received antiviral therapy (P<0.05). The study participants exhibited a mean body mass index of 21.5±2.8 kg/m2. In addition, 23.5% of the participants had chronic diseases. No significant difference was discovered between the two groups on different infective time and diverse CD4+ cell counts (P>0.05). The mean medical social support score was 55.2±16.3, with the depression-free group scoring 59.6±16.0 and the probable depression group scoring 51.4±16.0.There were statistically significant differences (P<0.05) in the scores for practical support dimension, social interactive cooperative support dimension, and emotional support dimension of the medical social support. However, no statistically significant difference was found in the message and emotional support dimensions (P > 0.05). (See Table 1).
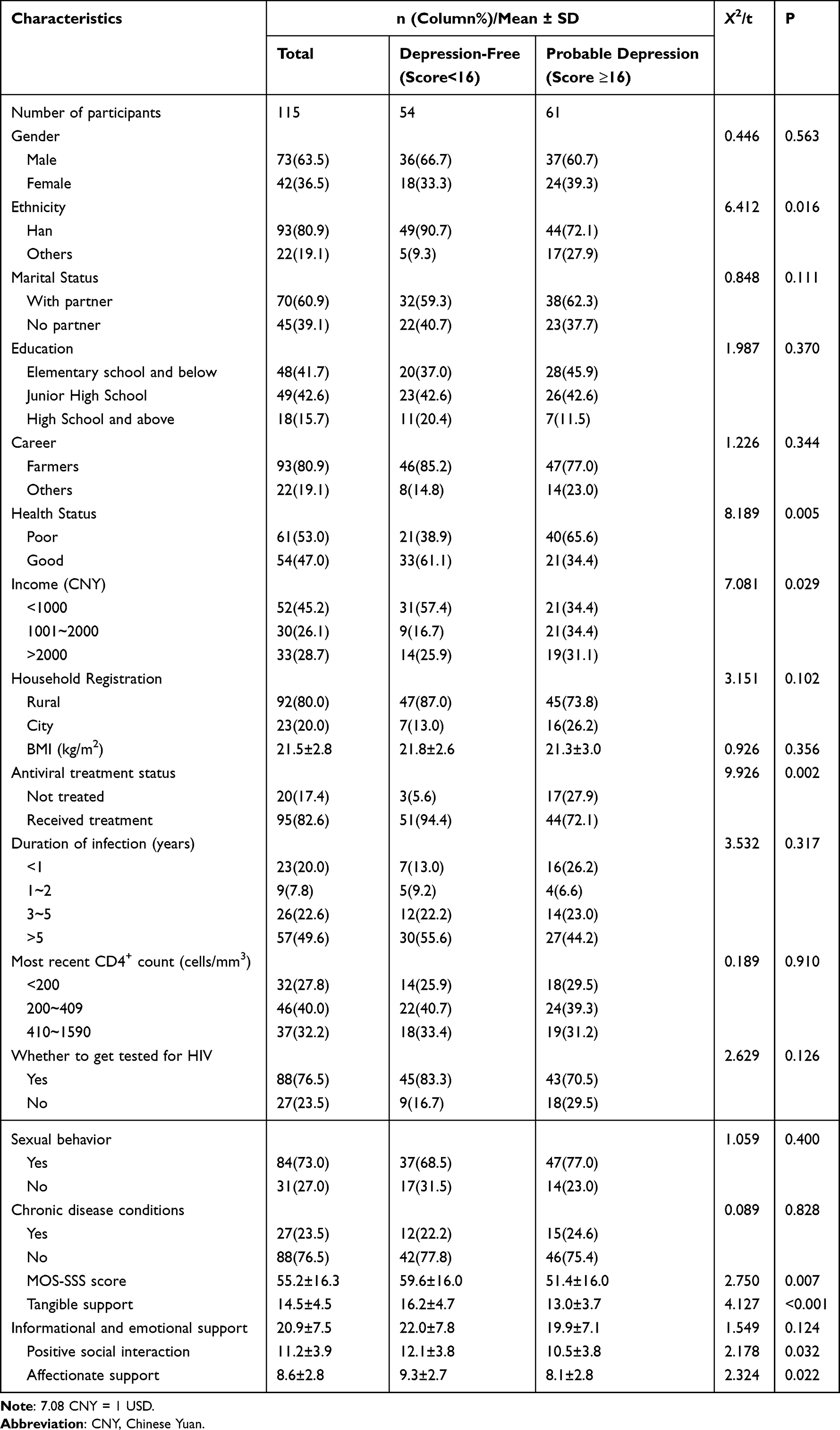 |
Table 1 The Socio-Demographic Characteristics of HIV/AIDS Patients Over 50 Years of Age (n=115) |
Associations Between Variables and Depressive Symptoms
There were negative associations between the CES-D scores and good health status (unstandardized b = −6.268, standardized b = −0.306, P<0.05), and receiving antiviral treatment (unstandardized b = −8.182, standardized b = −0.303, P<0.05). (See Table 2).
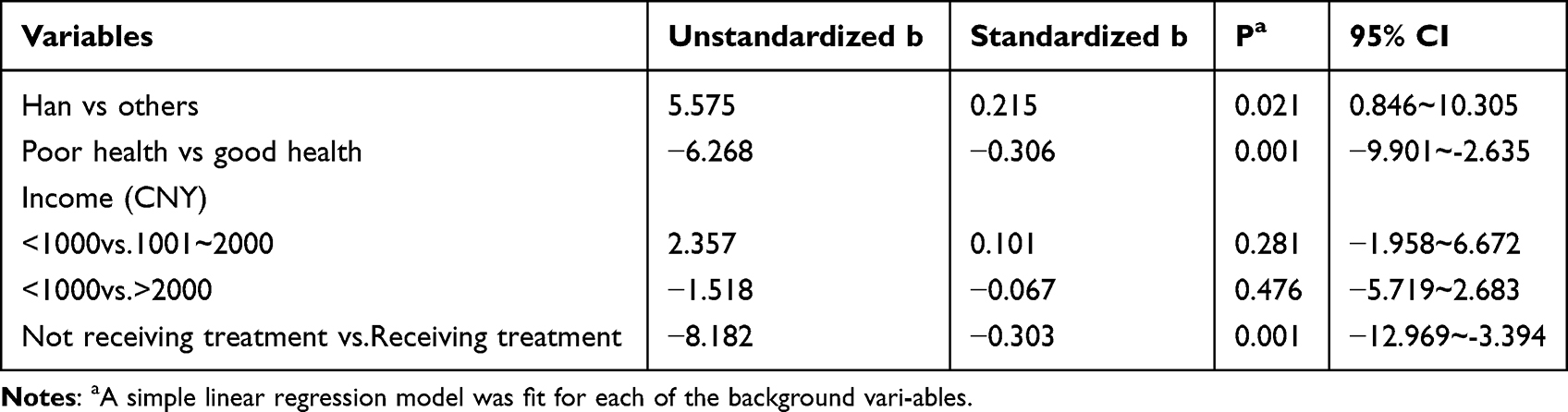 |
Table 2 Simple Linear Regression Analysis for the Associations Between Each Background Variable and Depressive Symptoms (n = 115) |
The higher the scores obtained by participants on the total medical social support (standardized b=−0.309), tangible support dimension (standardized b=−0.342), information and emotional support dimension (standardized b=−0.229), social interaction cooperation dimension (standardized b=−0.229), emotional support dimension (standardized b=−0.284), and the lower the scores obtained on the depression scale (P<0.05) after controlling for contextual factors. (See Table 3).
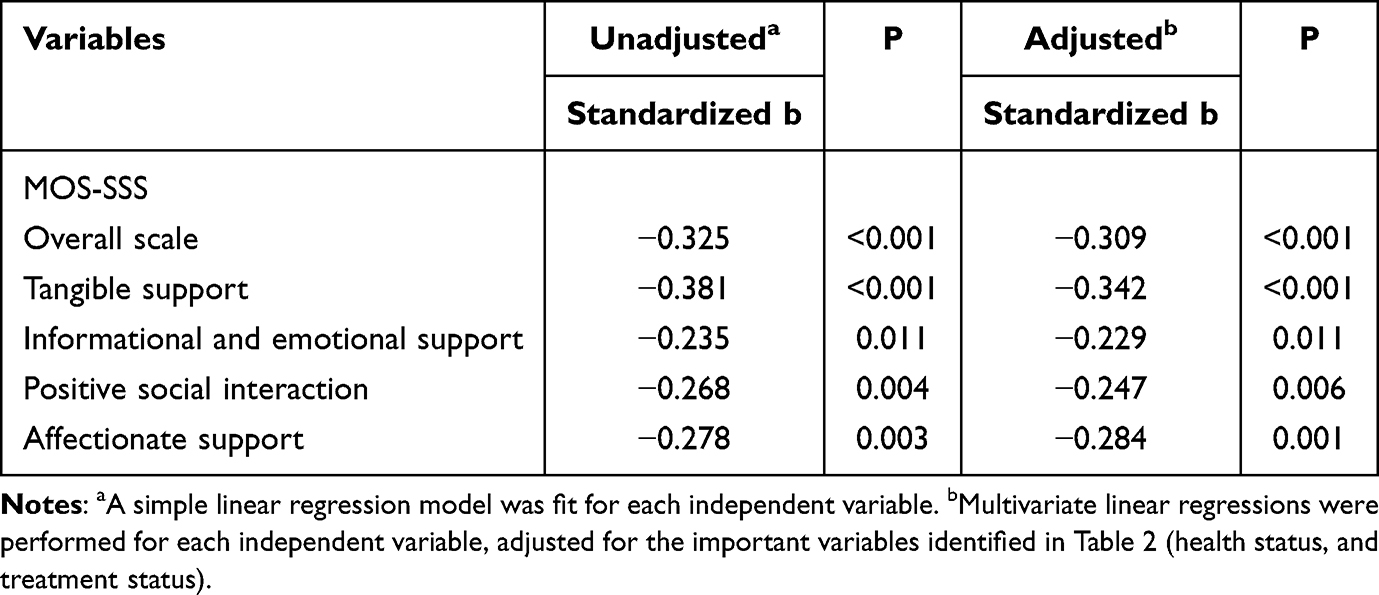 |
Table 3 After Controlling for Contextual Factors Associated with Higher CES-D Scores (n = 115) |
Correlation Between Medical Social Support and Depression
A Pearson correlation analysis of medical social support and depression in older PLWHA showed that practical support was negatively correlated with depressed mood, somatic symptoms, activity retardation, interpersonal score, and total depression score. There were negative correlations between total depression scores and message, emotional support. The negative correlations were found between social interactive cooperative support and positive mood, and total depression scores, and between emotional support and positive mood, and total depression scores. Medical social support was negatively correlated with depressed mood, positive mood, and total depression scores. All the differences were statistically significant (P < 0.05). (See Table 4).
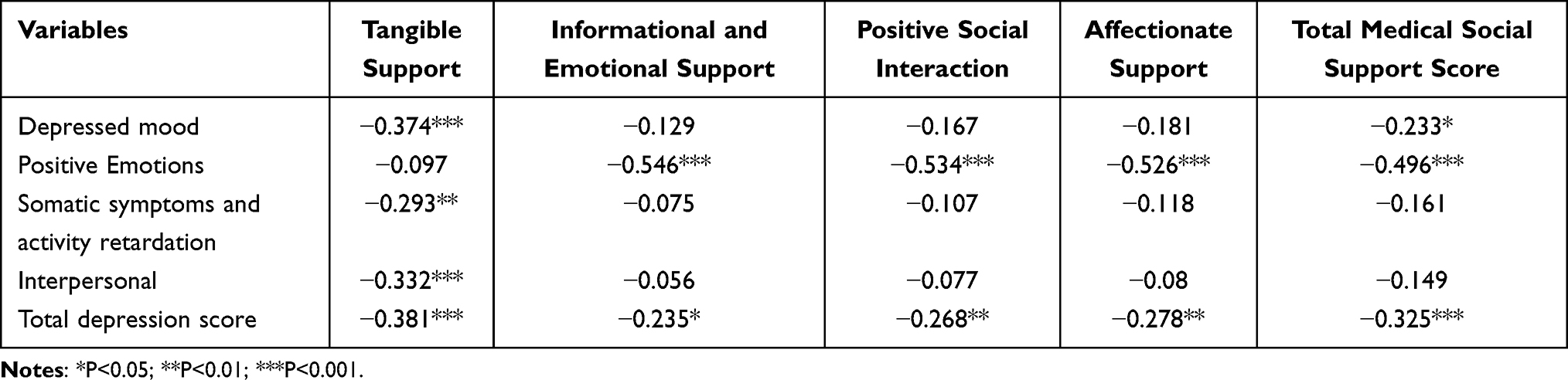 |
Table 4 Analysis of the Correlation Between Medical Social Support and Depression in Patients with HIV/AIDS Over 50 Years of Age |
Structural Equation Modeling of Medical Social Support and Depression
The structural equation model theoretical model was shown in Figure 1: A theoretical model of the effect of medical social support on depression. The model parameters were estimated by the great likelihood method, and the model after importing the data operation was shown in Figure 2: A knotted equation model of the effect of medical social support on depression. The fit index of the model was χ2/df=9.266, RMSEA=0.269, GFI=0.876. The model fit was poorly matched, and the factor loading of positive emotion on depression was not statistically significant (P>0.05). After modification based on Model 2 (Figure 3: A modified knot equation model of the effect of medical social support on depression), χ2/df=0.854 (<3), RMSEA=0.000 (<0.08), GFI=0.993 (>0.9), AGFI=0.963 (>0.9), TLI=1.003 (>0.9), the modified model fit was good, and the path coefficient and other factor loadings of the structural model were statistically significant (P<0.05). This finding showed that medical social support had a direct effect on depression with a standardized effect value of −0.223, and the factor loadings for depression were depressed mood, somatic symptoms, activity delay, and interpersonal in descending order, 0.968, 0.902, and 0.750, respectively.
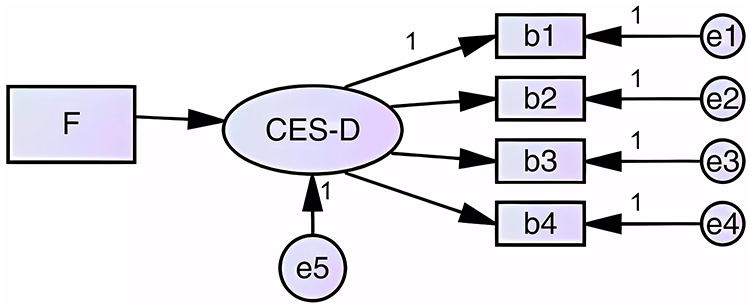 |
Figure 1 A theoretical model of the effect of medical social support on depression. F indicates medical social support; b1 indicates depressed mood; b2 indicates positive mood; b3 indicates somatic symptoms and delayed activity; and b4 indicates interpersonal. |
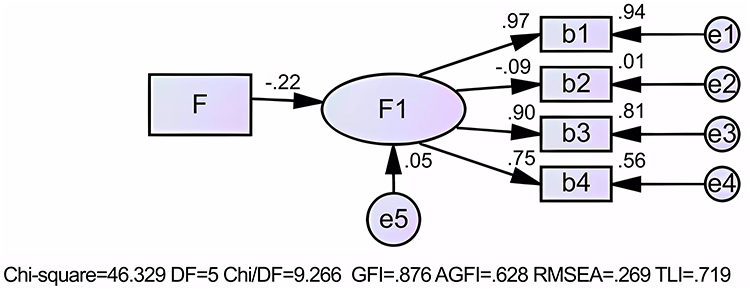 |
Figure 2 A knotted equation model of the effect of medical social support on depression. F indicates medical social support; F1 indicates depressive symptoms. b1 indicates depressed mood; b2 indicates positive mood; b3 indicates somatic symptoms and delayed activity; and b4 indicates interpersonal. |
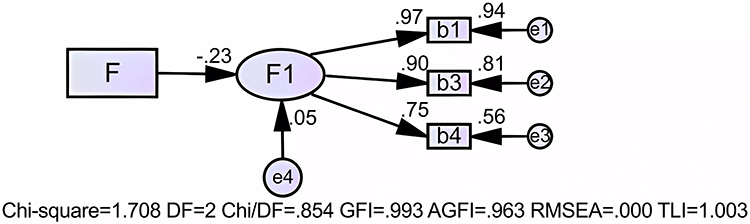 |
Figure 3 A modified knot equation model of the effect of medical social support on depression. F indicates medical social support; F1 indicates depressive symptoms. b1 indicates depressed mood; b3 indicates somatic symptoms and delayed activity; and b4 indicates interpersonal. |
Discussion
Our survey found that the prevalence of depressive symptoms in elderly HIV/AIDS ≥50 years old was 53.0% in Guilin. This prevalence was higher than the global prevalence of depression among PLWHA (31%).4 This difference may have arisen because we selected a population of older adults who were facing both the challenges of aging and HIV disease. Our study was higher than the prevalence of depression in Asian older PLWHA.19 The prevalence of depression in older PLWHA identified herein was also higher than that reported by Ciesla et al7 (44.8%), and Yu et al20 (39.86%) in China. The depression rate of HIV/AIDS patients is two to three times higher than that of the general population, probably because a treatment method for AIDS is lacking, social discrimination and stigma against AIDS persist, and antiretroviral treatment is associated with side effects.21,22 However, the prevalence of depression was lower than the other studies by Bhatia et al23 (58.75%), Liu et al24 (74.2%) and Wang et al25 (62%) in China. The differences may be mainly due to the sample sizes, international social environment, cultural background, medical conditions, and knowledge of the disease.26,27 The differences were probably due to the successful psychological interventions taken by the government and society for HIV/AIDS patients in recent years.Therefore, the mental health burden of elderly HIV/AIDS was serious in Guilin, and the mental health status of PLWHA warrant our attention.
The results of univariate analysis showed statistically significant differences in ethnicity, personal health status, mean monthly income, antiviral treatment status, and medical social support between the depression-free and the probable depression in older PLWHA. Ethnicity influenced depression in PLWHA, probably because ethnic minorities faced numerous life difficulties and had limited access to information and help compared with elderly Han due to differences in culture, socioeconomic status, language, and geographical location.28,29 The analysis of relevant factors influencing depression in HIV/AIDS patients showed that possible influencing factors included economic income level, household registration, CD4+ cell count level and medical social support.30–32 Among these factors, economic income and medical social support were consistent with the results of our study, and the differences were statistically significant. However, no significant differences were detected in CD4+ cell count level and household registration. The 72.2% of patients with CD4+ cell count levels >200 cells/mm3 in this investigation may have received antiviral treatment, and most of them were not severely affected. Thus, the univariate analysis did not show significant differences in the depression rate by CD4+ cell count level. For household registration, lifestyle differences between rural and urban households did not show significant differences in depression symptoms due to the continuous development of urbanization and the implementation of new rural construction.
The results of the simple linear regression analysis indicated that the variables of personal health status, and antiviral treatment status had significant associations with the depression. Studies have shown that improved health in elderly individuals corresponds with a better psychological state.33 Self-rated health, a subjective evaluation of older people’s health status, reflects the strengths and weaknesses of older people’s mental health to a certain extent. Self-rated health better indicates that older people are more satisfied with their current state, while a good state of mind can also reduce the influence of negative emotions, so strengthening physical health guidance for older PLWHA can reduce the occurrence of psychological problems, such as depression. Worldwide, people with HIV/AIDS commonly experience financial problems.34 Economic factors play a large role in the treatment of patients with HIV/AIDS. PLWHA require long-term medication to maintain their survival status. After HIV infection, participants’ working ability, reduced income, and concerns about costs will affect their antiviral treatment effect.35 HIV/AIDS with high economic pressure from family and society may be more likely to have psychological problems, whereas having an appropriate economic income will alleviate psychological burdens. Depression can have many negative effects on HIV/AIDS patients. For example, depression is an important influence on ART adherence.36 HIV/AIDS patients with depression were 40% less likely to adhere to antiretroviral therapy than those without depression. International studies have shown that antiviral therapy and CD4+ cell count levels at initiation of therapy are strongly associated with morbidity and mortality.37 The number of CD4+ cells is an important indicator of the degree of damage to the immune system of the infected person. Antiviral therapy reduces the destruction of human CD4+ cells by inhibiting the replication of HIV in the body, allowing the body’s immune function to be rebuilt. A lower CD4+ cell count indicated a poor prognosis, which was associated with subsequent depression.28 Participants receive early antiviral therapy to increase CD4+ cell levels, prolong their life expectancy and improve their quality of life, which can effectively relieve depression.
In adjusted and unadjusted multiple linear regression and correlation analysis of depression and medical social support, medical social support and its dimensions remained negatively associated with the occurrence of depression in older PLWHA. The study found that medical social support was associated with risk factors for the development of depression in HIV/AIDS, with the risk of developing depression being 7.09 times higher in moderate medical social support than in strong medical social support. Moreover, the risk of developing depression was 2.53 times higher in low medical social support than in strong medical social support.38 When patients face difficulties, the lack of medical social support may exacerbate the panic and anxiety felt by the patient. When patients cannot rely on their own ability to solve the problem, they will feel helpless to the extent that they become depressed and unable to self-regulate. Medical social support is a spiritual pillar for patients, buffering the impact and pressure brought by the surrounding environment, improving their mindset and reducing the occurrence of depression.
In structural equation modeling, medical social support was shown to have a direct effect on depression, and many studies have confirmed a negative association between medical social support and depression.39,40 The stigma and discrimination faced by individuals living with HIV/AIDS are a well-known phenomenon, and this social discrimination can have serious implications for their mental health. Individuals with HIV/AIDS may experience depression due to the societal prejudice they encounter, which can lead to feelings of isolation and hopelessness. Furthermore, the necessity of lifelong medication and regular follow-up appointments can disrupt patients’ daily lives, adding to their worries and stress levels. HIV/AIDS patients often feel reluctant to seek outside help due to the risk of privacy breaches, particularly among vulnerable populations such as elderly PLWHA. These individuals may face additional hardships such as divorce, widowhood, and the absence of children, leading to feelings of emptiness and monotony in their lives. In such circumstances, a lack of spiritual culture can exacerbate depression symptoms. Therefore, patients with HIV/AIDS require comprehensive support, including material, emotional, and informational assistance, to cope with the multifaceted challenges of their condition. However, it is important to acknowledge the limitations of our study, such as the cross-sectional study design, self-reported data, and the use of a convenience sampling approach, which may restrict the generalizability of our findings. Better medical social support can decrease patients’ bad moods and allow them to actively cope with the physical and psychological stresses caused by the disease. Therefore, we encourage HIV/AIDS patients to actively participate in social activities while informing trustworthy people, especially family members, about their condition and give full play to medical social support, especially family support, which can not only improve the mental health of HIV/AIDS patients but also reduce the occurrence of depression. At the same time, medical social support can improve individuals’ social adaptability and ability to cope with adversity, and adequate social and family support can provide PLWHA with more care and emotional support, which can improve their ability to cope with psychological stress41 and can make them feel cared for and needed as a way to buffer stress and reduce or even prevent depression.
Our study describes the current situation of depression and medical social support in elderly HIV/AIDS patients and the role of medical social support on depression. It also reveals the impact of medical social support on depression more objectively through a theoretical construction model, which is different from few previous studies on elderly HIV/AIDS patients. At the same time, it provides a theoretical basis for medical decision makers to carry out targeted psychological interventions and rational allocation of public health resources. Nevertheless, despite the valuable insights offered by our study, some limitations should be taken into account when interpreting the results. First, this is a cross-sectional study and it is not possible to determine the causality. Therefore, the findings should be cautiously interpreted when discussing the relationship between the variables under investigation. Second, relying on self-reported data for some variables may have introduced potential recall bias, which could have affected the accuracy and completeness of the data collected. Third, the use of a convenience sampling method might have resulted in sample selection bias, limiting the generalizability of our findings to other populations. Therefore, future studies should consider using more robust research designs and sampling methods to address these limitations and obtain more reliable and generalizable findings. Subsequently, we could increase the sample size for the study. Finally, we were unable to control for potential confounders such as side effects of antiretroviral therapy and social discrimination. The results of this study need to be further confirmed by a prospective follow-up study with a large sample.
Conclusion
In conclusion, the prevalence of depression among HIV/AIDS patients in Guilin is high, and the individual, family, and society need to work together to pay close attention to elderly patients. Government-funded counseling and monitoring services are being expanded in most provinces, free medical programs have been extended to most hospitals in China, and medical and social workers can provide appropriate medical and psychological support to patients to improve the physical and mental health of elderly PLWHA.
Data Sharing Statement
The datasets used and/or analyzed during the current study were available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to express their gratitude to the Guilin CDC and pay their respects to them. The authors acknowledge the efforts of the study team and extend special thanks to the patients who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas. They took part in drafting, revising or critically reviewing the article. They gave final approval of the version to be published. All authors have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Science research and Technology Development project of Guilin city (20210227-6-1), the Major Science and Technology Projects in Guangxi (GKAA22096026).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global HIV & AIDS statistics. Fact sheet; 2021:37.
2. Available from: http://www.nhc.gov.cn/jkj/s3578/202204/4fd88a291d914abf8f7a91f6333567e1.
3. Benton TD, Kee NW, Leung D, Canetti A, Karnik N. Depression among youth living with HIV/AIDS. Child Adolesc Psychiatr Clin N Am. 2019;28(3):447–459. doi:10.1016/j.chc.2019.02.014
4. Rezaei S, Ahmadi S, Rahmati J, et al. Global prevalence of depression in HIV/AIDS: a systematic review and meta-analysis. BMJ Support Palliat Care. 2019;9(4):404–412. doi:10.1136/bmjspcare-2019-001952
5. Wang T, Fu H, Kaminga AC, et al. Prevalence of depression or depressive symptoms among people living with HIV/AIDS in China: a systematic review and meta-analysis. Bmc Psychiatry. 2018;18(1):160. doi:10.1186/s12888-018-1741-8
6. Chandra PS, Ravi V, Desai A, Subbakrishna DK. Anxiety and depression among HIV-infected heterosexuals--A report from India. J Psychosom Res. 1998;45(5):401–409. doi:10.1016/S0022-3999(98)00028-2
7. Ciesla JA, Roberts JE. Meta-analysis of the relationship between HIV infection and risk for depressive disorders. Am J Psychiatry. 2001;158(5):725–730. doi:10.1176/appi.ajp.158.5.725
8. Zorrilla EP, McKay JR, Luborsky L, Schmidt K. Relation of stressors and depressive symptoms to clinical progression of viral illness. Am J Psychiatry. 1996;153(5):626–635.
9. Horberg MA, Silverberg MJ, Hurley LB, et al. Effects of depression and selective serotonin reuptake inhibitor use on adherence to highly active antiretroviral therapy and on clinical outcomes in HIV-infected patients. J Acquir Immune Defic Syndr. 2008;47(3):384–390. doi:10.1097/QAI.0b013e318160d53e
10. Tan T, Zhou C, Lu R, et al. Depression and associated factors among men living with HIV/AIDS aged 50 years and over in Chongqing, China. J Multidiscip Healthc. 2022;15:2033–2040. doi:10.2147/JMDH.S378956
11. Nyirenda M, Chatterji S, Rochat T, Mutevedzi P, Newell ML. Prevalence and correlates of depression among HIV-infected and -affected older people in rural South Africa. J Affect Disord. 2013;151(1):31–38. doi:10.1016/j.jad.2013.05.005
12. Wu X, Chen J, Huang H, et al. Perceived stigma, medical social support and quality of life among people living with HIV/AIDS in Hunan, China. Appl Nurs Res. 2015;28(2):169–174. doi:10.1016/j.apnr.2014.09.011
13. Zhakipbayeva BT, Nugmanova ZS, Tracy M, et al. Factors influencing the quality of life in persons living with human immunodeficiency virus infection in Almaty, Kazakhstan. Int J Std Aids. 2019;30(13):1318–1328. doi:10.1177/0956462419876484
14. Hershow RB, Gottfredson NC, Ha TV, et al. Longitudinal analysis of depressive symptoms, perceived social support, and alcohol use among HIV-infected men who inject drugs in Northern Vietnam. Subst Use Misuse. 2020;55(8):1237–1245. doi:10.1080/10826084.2020.1732422
15. Mao Y, Qiao S, Li X, et al. Depression, social support, and adherence to antiretroviral therapy among people living with HIV in Guangxi, China: a longitudinal study. Aids Educ Prev. 2019;31(1):38–50. doi:10.1521/aeap.2019.31.1.38
16. Liu L, Pang R, Sun W, et al. Functional social support, psychological capital, and depressive and anxiety symptoms among people living with HIV/AIDS employed full-time. Bmc Psychiatry. 2013;13:324. doi:10.1186/1471-244X-13-324
17. Rooney AS, Moore RC, Paolillo EW, et al. Depression and aging with HIV: associations with health-related quality of life and positive psychological factors. J Affect Disord. 2019;251:1–7. doi:10.1016/j.jad.2019.03.025
18. Sherbourne CD, Stewart AL. The MOS social support survey. Soc Sci Med. 1991;32(6):705–714. doi:10.1016/0277-9536(91)90150-B
19. Thet D, Siritientong T, Sangarlangkarn A, et al. Deterioration of nutritional status and its negative association with depression among older HIV-infected Asian population: a four-year longitudinal study. AIDS Res Hum Retroviruses. 2022;38(7):592–600. doi:10.1089/aid.2021.0087
20. Yu J, Li J, Cuijpers P, Wu S, Wu Z. Prevalence and correlates of depressive symptoms in Chinese older adults: a population-based study. Int J Geriatr Psychiatry. 2012;27(3):305–312. doi:10.1002/gps.2721
21. Rubin LH, Maki. PM. HIV, depression, and cognitive impairment in the era of effective antiretroviral therapy. Curr HIV/AIDS Rep. 2019;16(1):82–95. doi:10.1007/s11904-019-00421-0
22. Perazzo JD, Currie J, Horvat DC, Lambert J, Webel AR. Depression and social capital in people living with HIV. J Psychiatr Ment Health Nurs. 2020;27(1):54–61. doi:10.1111/jpm.12552
23. Bhatia MS, Munjal S. Prevalence of depression in people living with HIV/AIDS undergoing ART and factors associated with it. J Clin Diagn Res. 2014;8(10):C1–C4.
24. Liu H, He X, Levy JA, et al. Psychological impacts among older and younger people living with HIV/AIDS in Nanning, China. J Aging Res. 2014;2014:576–592. doi:10.1155/2014/576592
25. Wang H, Zhang C, Ruan Y, et al. Depressive symptoms and social support among people living with HIV in Hunan, China. J Assoc Nurses AIDS Care. 2014;25(6):568–576. doi:10.1016/j.jana.2014.02.001
26. Yu X, Baillargeon J, Berenson AB, et al. Incident depression among Medicare beneficiaries with disabilities and HIV. Aids. 2022;36(9):1295–1304. doi:10.1097/QAD.0000000000003268
27. Drummond KL, Painter JT, Curran GM, et al. HIV patient and provider feedback on a telehealth collaborative care for depression intervention. Aids Care. 2017;29(3):290–298. doi:10.1080/09540121.2016.1255704
28. Olisah VO, Adekeye O, Sheikh TL. Depression and CD4 cell count among patients with HIV in a Nigerian University Teaching Hospital. Int J Psychiatry Med. 2014;48(4):253–261. doi:10.2190/PM.48.4.b
29. Giyeon K, Jamie D, Chao-Hui H. Race/ethnicity and the factor structure of the center for epidemiologic studies depression scale: a meta-analysis. Cult Divers Ethn Min. 2011;17(4):381–396. doi:10.1037/a0025434
30. Song JY, Lee JS, Seo YB, et al. Depression among HIV-infected patients in Korea: assessment of clinical significance and risk factors. Infect Chemother. 2013;45(2):211–216. doi:10.3947/ic.2013.45.2.211
31. Swendeman D, Fehrenbacher AE, Roy S, et al. Gender disparities in depression severity and coping among people living with HIV/AIDS in Kolkata, India. PLoS One. 2018;13(11):e207055. doi:10.1371/journal.pone.0207055
32. Xiao Z, Li X, Qiao S, Zhou Y, Shen Z. Social support, depression, and quality of life among people living with HIV in Guangxi, China. Aids Care. 2017;29(3):319–325. doi:10.1080/09540121.2016.1224298
33. Byeon H. Relationship between physical activity level and depression of elderly people living alone. Int J Environ Res Public Health. 2019;16(20):4051. doi:10.3390/ijerph16204051
34. Djellouli N, Quevedo-Gomez MC. Challenges to successful implementation of HIV and AIDS-related health policies in Cartagena, Colombia. Soc Sci Med. 2015;133:36–44. doi:10.1016/j.socscimed.2015.03.048
35. Peltzer K, Pengpid S. Socioeconomic factors in adherence to HIV therapy in low- and middle-income countries. J Health Popul Nutr. 2013;31(2):150–170. doi:10.3329/jhpn.v31i2.16379
36. Velloza J, Celum C, Haberer JE, et al. Depression and ART initiation among HIV serodiscordant couples in Kenya and Uganda. Aids Behav. 2017;21(8):2509–2518. doi:10.1007/s10461-017-1829-z
37. Zhang F, Dou Z, Ma Y, et al. Effect of earlier initiation of antiretroviral treatment and increased treatment coverage on HIV-related mortality in China: a national observational cohort study. Lancet Infect Dis. 2011;11(7):516–524. doi:10.1016/S1473-3099(11)70097-4
38. Duko B, Geja E, Zewude M, Mekonen S. Prevalence and associated factors of depression among patients with HIV/AIDS in Hawassa, Ethiopia, cross-sectional study. Ann Gen Psychiatry. 2018;17:45. doi:10.1186/s12991-018-0215-1
39. Li L, Lee SJ, Thammawijaya P, Jiraphongsa C, Rotheram-Borus MJ. Stigma, social support, and depression among people living with HIV in Thailand. Aids Care. 2009;21(8):1007–1013. doi:10.1080/09540120802614358
40. Xiaowen W, Guangping G, Ling Z, et al. Depression and anxiety mediate perceived social support to predict health-related quality of life in pregnant women living with HIV. Aids Care. 2018;30(9):1147–1155. doi:10.1080/09540121.2018.1456640
41. Biratu A, Haile D. Prevalence of antenatal depression and associated factors among pregnant women in Addis Ababa, Ethiopia: a cross-sectional study. Reprod Health. 2015;12:99.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.