")
Back to Archived Journals » Core Evidence » Volume 14
Anabolics in the management of glucocorticoid-induced osteoporosis: an evidence-based review of long-term safety, efficacy and place in therapy
Received 6 April 2019
Accepted for publication 17 July 2019
Published 23 August 2019 Volume 2019:14 Pages 41—50
DOI https://doi.org/10.2147/CE.S172820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Adam D Taylor, Kenneth G Saag
Division of Clinical Immunology and Rheumatology, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Kenneth G Saag
Division of Clinical Immunology and Rheumatology, Department of Medicine, University of Alabama at Birmingham, 820 Faculty Office Tower, 510 20 th Street South, Birmingham, AL 35294-3408, USA
Tel +1 205 996 9784
Fax +1 205 975 6859
Email [email protected]
Introduction: Glucocorticoid-induced osteoporosis is an underrecognized complication of chronic glucocorticoid therapy characterized by a decrease in new bone formation. Anabolic therapies, such as teriparatide, a recombinant human parathyroid hormone, combat the disease by promoting new bone growth.
Aims: This article outlines the pathophysiology of glucocorticoid-induced osteoporosis and details the evidence of efficacy, safety, and patterns of use of teriparatide and other future anabolic therapies.
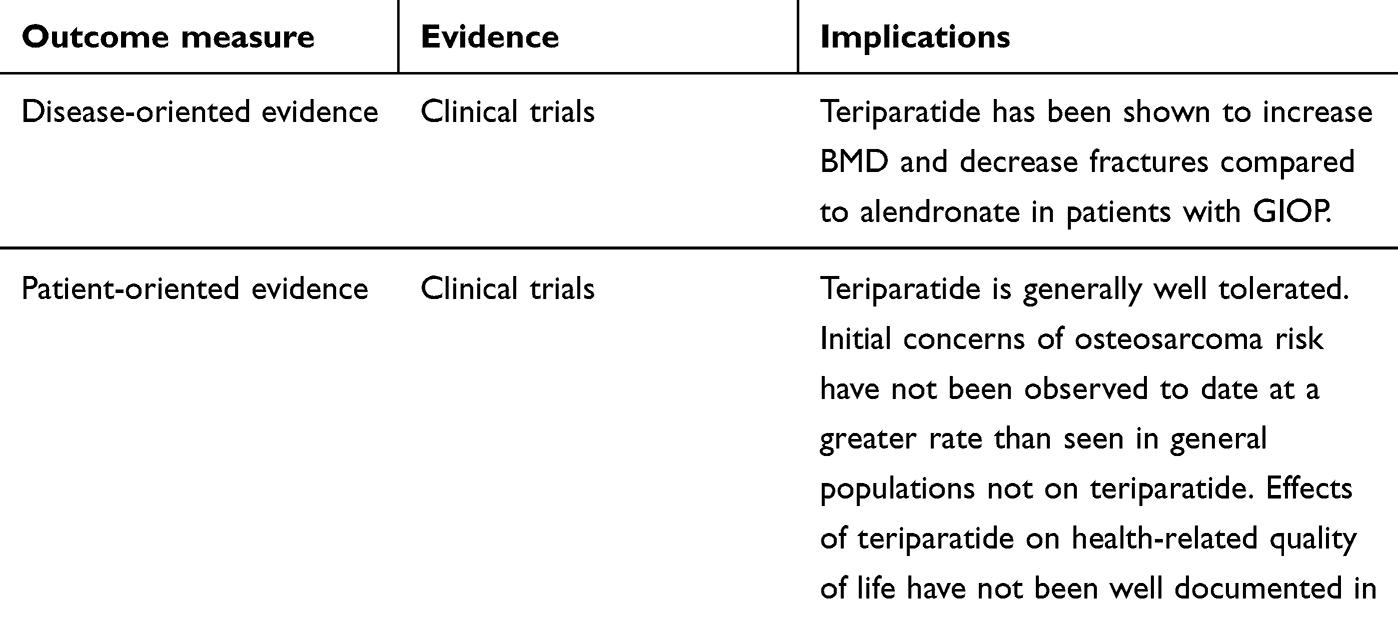
Evidence review: In multiple clinical trials, teriparatide has been shown to significantly increase lumbar spine bone mineral density (BMD) in patients with glucocorticoid-induced osteoporosis when compared with placebo, alendronate, and risedronate. When compared with alendronate, significantly fewer vertebral fractures were noted in the teriparatide group. Adverse effects noted in clinical trials include nausea, insomnia, flushing, myalgias, and mild hypercalcemia/hyperuricemia. Early studies in rats noted an increased incidence of osteosarcoma; however, an increased rate beyond levels seen in general populations has not been noted in human studies or with long-term pharmacovigilance. Abaloparatide and romosozumab are newer anabolic therapies that have shown some benefit in postmenopausal osteoporosis but have not yet been studied in the chronic glucocorticoid population.
Place in therapy: Major specialty organizations continue to recommend bisphosphonates as first-line therapy in glucocorticoid-induced osteoporosis due to the proven benefit and relative affordability. However, the use of anabolics shows promise to improve outcomes by increasing BMD and reducing fracture-associated morbidity and mortality and has a role for selected populations at high fracture risk.
Keywords: teriparatide, steroid, osteoporosis, GIOP
Core evidence clinical impact summary for teriparatide
 |
|
Scope of the problem
Glucocorticoid-induced osteoporosis remains an underrecognized problem in patients receiving long-term glucocorticoid therapy. Despite the emerging number of glucocorticoid-sparing therapies, physicians and patients still rely on glucocorticoids in the management of many acute and chronic illnesses.1 A study of patients registered with a general practitioner in England noted that glucocorticoids are used chronically by 0.5% of the population, including 1.4% of patients older than 55 years.2 A more recent analysis placed the prevalence of glucocorticoid use in 1 year at 3%, which was stable to slightly increased from a prior study in 1999.3 A third study noted a 34% increase in long-term glucocorticoid use from 1989 to 2008.4 While the risks of long-term glucocorticoid use on bones are well known, they remain underrecognized and undertreated.5 One study looking at new glucocorticoid prescriptions found that only 41% of women older than 50 were prescribed concurrent antiosteoporotic therapies and only 16% had a bone mass measurement.6
Mechanism of glucocorticoid effects on bone
The pathophysiology of glucocorticoid-induced osteoporosis arises primarily from the direct effects of glucocorticoids on bone and is characterized by two distinct phases: an early rapid and transient phase followed by a slower, progressive phase.7 The early phase is primarily characterized by an increase in osteoclastogenesis that leads to an increase in bone resorption. This effect is mediated by an upregulation of receptor activator of nuclear factor kappa-Β ligand (RANKL) and macrophage colony-stimulating factor (M-CSF) along with a decrease in osteoprotegerin (OPG).8,9 However, this effect is only temporary; the primary driver of glucocorticoid-induced osteoporosis is mediated by a reduction in the number of circulating osteoblasts. This is accomplished by several different pathways. Glucocorticoids upregulate the expression of peroxisome proliferator-activated receptor-gamma (PPAR-γ), which subsequently increases the differentiation of precursor cells to adipocytes rather than osteoblasts, thereby decreasing the number of circulating osteoblasts.10 Next, osteoblastogenesis is mediated by the Wnt/β-catenin signaling pathway. However, glucocorticoids inhibit Wnt binding via increased expression of Dickkopfl (Dkk1), subsequently inducing destabilization of β-catenin by glycogen-synthase kinase-3β and a resulting decrease in osteoblastogenesis.11–17 Finally, activation of caspase 3 leads to increased apoptosis of circulating osteoblasts.18,19
Epidemiology of glucocorticoid effects on bone
It is well established from epidemiologic studies that long-term glucocorticoid use has a negative effect on bone health. Several studies have noted an increased risk of fractures among patients on chronic steroid therapy.20–25 This risk appears to be dose dependent, both with the daily dose and with cumulative dose, and at least partially reversible upon cessation of steroid use.20,23,26 However, many patients with rheumatoid arthritis, the most common glucocorticoid-requiring disease, still use small doses to control disease despite being on steroid-sparing therapy, and increased fracture risk has been seen even at small daily doses.1,23
As discussed above, glucocorticoid use causes a rapid increase in bone resorption followed by decreased formation of new bone that has a significant effect on overall bone health. A study of a Norwegian cohort found that current glucocorticoid usage was associated with a 2.6-fold decrease in bone mineral density (BMD) when followed over 2 years.27 Steroid use also has negative consequences on bone health independent of BMD; a study in postmenopausal women noted an increased risk of fracture at similar BMD in patients on chronic steroid therapy.28 The effect of steroids on bone health seems to be a least partially reversible on discontinuation of the drug, but this is not an option for all patients, necessitating adequate antiosteoporotic therapy.29
Antiresorptive therapies in glucocorticoid-induced osteoporosis
Bisphosphonates are the best-studied drug class in the treatment of postmenopausal osteoporosis, and this has largely carried over to glucocorticoid-induced osteoporosis as well. Alendronate, risedronate, raloxifene, and ibandronate have all been shown in randomized controlled trials to increase BMD over placebo in glucocorticoid-induced osteoporosis.30–35 Zoledronic acid and denosumab have been shown to be superior to risedronate in BMD increase.36,37 Finally, risedronate and alendronate have been shown to decrease vertebral fracture rate compared to placebo, based on extensions to clinical trials or post hoc analyses of the original trials.38,39
Anabolic therapies in glucocorticoid-induced osteoporosis – mechanism and overview
Despite the proven efficacy of the antiresorptive therapies above, bisphosphonates may not be the ideal treatment for osteoporosis caused by long-term steroids, particularly within the low-turnover state of the disease. The chronic long-term effects of steroids on the bones are mediated by a decrease in bone formation, due to the decrease in osteoblast production and activity. Thus, strictly antiresorptive therapy may not be as beneficial in this low-turnover state as in osteoporosis secondary to estrogen deficiency, a high turnover state mediated by a relative increase in osteoclast activity.40 Anabolic therapies protect against bone degradation by promoting new bone growth rather than by a reduction in remodeling. This is accomplished by reversal of many of the pathways, leading to glucocorticoid-induced osteoporosis as noted above, including enhancement of the Wnt signaling pathway and inhibition of PPAR-gamma, ultimately leading to increase in circulating osteoblasts.41 The concept of an “anabolic window” has been described in which direct action on osteoblasts leads to a rapid but short-lived period of increased bone growth. This is then followed by a second, less rapid phase of bone growth.
Teriparatide in glucocorticoid-induced osteoporosis
BMD and fracture data
Teriparatide, a subcutaneous recombinant human parathyroid hormone (1–34), was the first anabolic agent approved for the treatment of osteoporosis and the only one that has been studied specifically in glucocorticoid-induced osteoporosis. Before being approved for patients on chronic glucocorticoid therapy, PTH and teriparatide were tested in postmenopausal women and men with osteoporosis prior to receiving FDA approval for these indications in 2002. A randomized controlled trial conducted in 2001 on postmenopausal women with osteoporosis noted a decreased fracture risk and increased BMD in the lumbar spine and femoral neck in patients on teriparatide when compared with placebo.42 A smaller RCT in 2002 conducted in postmenopausal women showed a significant increase in BMD at the lumbar spine, femoral neck, and total body, as well as a reduced nonvertebral fracture rate, in patients treated with teriparatide compared to those treated with alendronate.43 A third RCT conducted in 2003 in men with osteoporosis noted an increase in femoral neck, spine, and total body BMD in the teriparatide group compared to the placebo group.44
The first study of PTH in glucocorticoid-induced osteoporosis was a randomized controlled trial in 1998.45 The study was conducted in 51 postmenopausal women with 12 months of previous steroid use and compared hormone replacement therapy with hormone replacement therapy plus PTH. The primary endpoint of the study was BMD at the lumbar spine, which, after 12 months of therapy, was significantly higher in the PTH group (35% and 11% by quantitative CT and dual-energy X-ray absorptiometry [DXA], respectively) than in the estrogen-only group (1.7% and 0%, respectively). No significant differences were seen in BMD at the total hip or femoral neck between the two groups, and the study was not powered to detect differences in fracture rates.
The landmark trial in teriparatide use in glucocorticoid-induced osteoporosis was published in 2007.46 The study was a large, multicenter, randomized controlled trial testing teriparatide against alendronate in patients with glucocorticoid-induced osteoporosis. Participants in the trial were patients 21 years of age or older with a history of sustained glucocorticoid therapy (defined as the mean daily dose of prednisone 5 mg or more for at least three consecutive months) with a T score of −2.0 or −1.0 and a history of a fragility fracture while on steroids. Participants were divided into groups of daily 20 mcg teriparatide or daily 10 mg oral alendronate for 18 months. The primary endpoint of the trial was BMD of the lumbar spine and total hip, assessed by DXA. Additional endpoints included fractures, divided into vertebral and nonvertebral, and markers of bone remodeling. After 18 months of therapy, the teriparatide group had a 7.2% increase in lumbar spine BMD vs 3.4% in the alendronate group (p<0.001) and the teriparatide group had a 3.8% increase in total hip BMD vs 2.4% in the alendronate group (p=0.005). Vertebral fractures were significantly decreased in the teriparatide group; there were no significant differences in nonvertebral fractures between the two groups. Adverse events were minor and relatively similar between the two groups. The trial was continued through 36 months with similar results with a significant increase in lumbar spine, total hip, and femoral neck BMD in the teriparatide group as compared to the alendronate group. The teriparatide group had fewer vertebral fractures; there was no difference in nonvertebral fractures.47 Results from the trial are summarized in Figure 1.
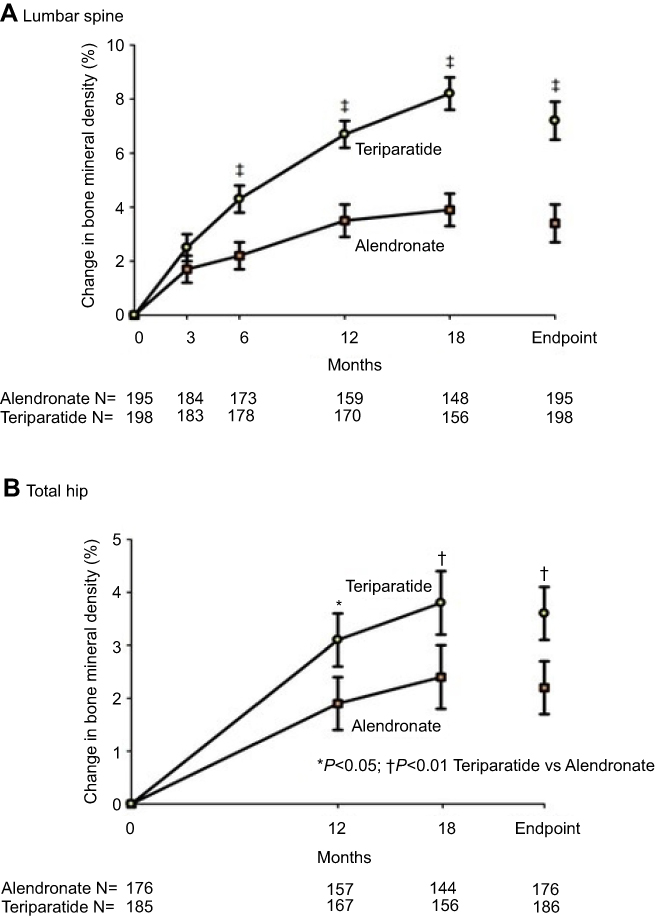 |
Figure 1 Results of a randomized-controlled trial comparing teriparatide with alendronate in patients with glucocorticoid-induced osteoporosis.Note: From the New England Journal of Medicine, Saag KG, Shane E, Boonen S, et al, Teriparatide or Alendronate in Glucocorticoid-Induced Osteoporosis, 357(20), 2028–2039, Copyright © 2007 Massachusetts Medical Society. Reprinted with permission.46 |
A third large randomized controlled trial, the EuroGIOPs trial published in 2013, pitted teriparatide vs risedronate in men with glucocorticoid-induced osteoporosis.48 In the primary outcome of this trial, after 18 months, lumbar spine BMD, as measured by quantitative computed tomography (QCT), demonstrated a 16.3% increase in the teriparatide group vs a 3.8% increase in the risedronate group (p=0.004). New clinical fractures were fewer in the teriparatide group (zero as compared to five in the risedronate group), but the difference was not statistically significant (p=0.056).
Bone turnover markers and alternative endpoints
Bone turnover markers (BTMs) provide a convenient way to analyze the different mechanistic effects of anabolic therapies compared to antiresorptive therapies and are another surrogate measure for a biologic response. An increase in bone formation markers has been consistently noted in studies with teriparatide, in opposition to the decrease in bone formation markers seen in bisphosphonates such as alendronate/risedronate.45–50 Changes in procollagen type I N propeptide (PINP), a protein formed during the synthesis of new type I collagen in the osteoblast, have been noted to correlate with increases in BMD as well as changes in finite element strength in patients on teriparatide.50,51
As imaging techniques improve, more sensitive techniques to quantify bone strength have been developed and used in the study of teriparatide. High-resolution computed tomography (HRCT) is one such emerging alternative method to measure BMD.52 While BMD is most widely measured using DXA, HRCT uses three-dimensional imaging to permit greater sensitivity in diagnosis as well as the ability to measure both cortical and trabecular bone integrity. As noted above, this technique was applied in the EuroGIOPs trial where teriparatide was compared with risedronate in men with glucocorticoid-induced osteoporosis.48 Teriparatide was noted to have greater BMD at the lumbar spine, as measured by QCT as well as improved bone strength and stiffness, calculated by HRQCT-based finite element analysis, a model used to simulate the properties of bone.53
Reference point indentation is a technique in which the mechanical properties of a bone can be analyzed at a level of detail finer than exclusively imaging-based tests. As previously noted, patients on long-term glucocorticoids are at increased risk of fractures compared to controls with similar BMD measurements, indicating that glucocorticoid use causes a deterioration in bone quality not adequately measured by BMD. A study evaluating reference point indentation in patients recently starting glucocorticoids noted a significant decrease in bone material strength index (BMSi) in patients on calcium/vitamin D only, no significant change in patients on risedronate, and an improved BMSi in denosumab and teriparatide after 7 weeks of therapy. No BMD changes were noted over this period, indicating that reference point indentation provides the sensitivity necessary to detect early changes in bone integrity not seen on traditional imaging measures.54
The trabecular bone score (TBS) is a technique to assess the bone texture and provide information about bone quality from DXA images. TBS has been positively correlated with bone microarchitecture and is a better predictor of fracture risk than BMD.55,56 A subpopulation analysis of the original teriparatide vs alendronate trial used archived DXA scans to calculate TBSs in order to compare the effects of teriparatide and alendronate on TBS as well as assess for differences between BMD and TBS. As noted above, the BMD increased in both groups from baseline; however, only the teriparatide group noted a significant increase in TBS from baseline, while the alendronate group noted no significant difference in TBS.57 This finding indicates that the TBS may be another sensitive measure that can detect differences and effects of treatment better than BMD alone.
Safety
The safety of teriparatide has been a topic of potential concern since the initial study and development of the drug. In the large RCTs referenced above, teriparatide tended to be well tolerated, with only minor side effects such as nausea, insomnia, flushing, myalgias, and mild hypercalcemia/hyperuricemia.46,48 However, early rat studies indicating an increased risk of osteosarcoma and other bone tumors have necessitated further study on the safety of the drug.58 Due to these findings, the FDA mandated a postmarketing study to further study this association. In 2012, the 7-year findings of this 15-year study were published, and it was noted that no patients had developed osteosarcoma with a prior history of teriparatide use.59 Data presented from the 12-year follow-up noted two patients who had developed osteosarcoma following teriparatide treatment. This rate was deemed to be within the expected range assuming no increased risk.60 The difference in findings in rat and human studies may be due to different patterns of use, since rat studies noting increased osteosarcoma risk have either been at much higher doses or for a much longer relative duration than are typically used in humans.61–63
Furthermore, bisphosphonates are not without safety risk either. Long-term use of bisphosphonates can impair the bone quality and has been associated with osteonecrosis of the jaw and atypical fractures, among others.64,65 Like any medication, caution should be taken when long-term use of a medication is anticipated.
Cost
A final concern that may potentially limit the widespread use of teriparatide in glucocorticoid-induced osteoporosis is the cost of the medication. Indeed, teriparatide is significantly more expensive than bisphosphonates, and patients with glucocorticoid-induced osteoporosis typically have an underlying medical condition that would make affordability even more of a concern. However, given the decrease in vertebral fractures associated with teriparatide, leading to direct cost savings, as well as improvement in the quality of life, a justification could be made for the long-term cost-effectiveness of teriparatide. One economic analysis found that when the additional mortality from osteoporosis-related fractures was considered, teriparatide could be economically justified as first line for glucocorticoid-induced osteoporosis.66
Patterns of use
Because teriparatide currently has a limited time course, the question of whether bisphosphonates are beneficial following a course of teriparatide therapy was an important topic of study. Although not done specifically in glucocorticoid-induced osteoporosis, the PaTH study published in 2005 randomly assigned patients who previously underwent 1 year of PTH to placebo or alendronate.67 After 1 year, the patients in the alendronate group noted a significant increase in gains in BMD at both the spine and hip. Based on these findings and other studies, nearly all patients who receive anabolic agents should follow these drugs with antiresorptive therapy to maximize the benefits and to “fill-in” the new remodeling space collected. Simultaneous bisphosphonates with PTH, tested earlier in the same trial, appeared to blunt the effect of PTH rather than the enhancement seen by sequential therapy.68
The optimal duration of teriparatide treatment is not completely clear. Currently, due to concerns about safety, a maximum of 24 months of therapy is recommended. Teriparatide appears to provide benefit beyond this timeframe; the 36-month follow-up of the original teriparatide-alendronate trial noted a significant increase in BMD between months 24 and 36 with minimal difference in adverse events; however, further study is needed.47
Similarly, the benefit of a second course of therapy after a discrete break has mixed results. Two studies published in 2009 measured the effects of retreatment with teriparatide. The first enrolled patients who had previously completed 1 year of teriparatide and then 1 year of alendronate and treated them with an additional year of teriparatide.69 Similar BMD increases were seen after each course of teriparatide, drawing the conclusion that retreatment may be a viable option. However, a separate study in which teriparatide was taken for a year, stopped for a year, and then taken for an additional year found an attenuated effect in BMD increase on the second course of teriparatide.70 Additional study is needed to determine the benefit of a second course of medication.
Other anabolic therapies in glucocorticoid-induced osteoporosis
Anabolic sex steroids
Prior to the discovery of PTH and teriparatide, anabolic sex steroids and hormone replacement therapy were a topic of study in glucocorticoid-induced osteoporosis. Sex steroids were an appealing target for therapy; the rationale being that long-term glucocorticoids led to a sex corticosteroid deficiency, which then resulted in increased bone reabsorption, and HRT was familiar from its popularity at the time in treatment of postmenopausal osteoporosis.71 In women on long-term glucocorticoids, hormone replacement therapy demonstrated significant increases in BMD and decreased bone resorption.72–74 Enthusiasm for the use of HRT in glucocorticoid-induced osteoporosis diminished after the publication of the Women's Health Initiative (WHI) trial exposed the risks of long-term HRT.75 Androgen supplementation with nandrolone decanoate in women with glucocorticoid-induced osteoporosis was showed to increase forearm bone density.76 Finally, testosterone supplementation in men on chronic glucocorticoid therapy was associated with increase in BMD at the lumbar spine and hip.77,78 No benefit was seen with nandrolone decanoate in men.78
Abaloparatide
Although teriparatide is the only anabolic antiosteoporotic therapy that has been specifically studied in a long-term glucocorticoid population, there is emerging evidence supporting the study of additional medications with similar mechanisms of action. Use of abaloparatide, a daily subcutaneous parathyroid hormone-related protein analog, in postmenopausal women has demonstrated significantly increased BMD at the lumbar spine, femoral neck, and total hip when compared to placebo as well as a significantly reduced incidence of both vertebral and nonvertebral fractures at a wide range of baseline fracture risks.79–83 Efficacy was mostly comparable to teriparatide in limited trials, although abaloparatide was associated with a significant increase in total hip BMD compared to teriparatide.79 The mechanism behind this difference is unclear but may be due to a decreased bone resorption period, leading to a larger increase in bone growth.84
Romozosumab
Romosozumab is a monoclonal antibody against sclerostin, a protein secreted by osteocytes that inhibits bone formation through regulation of osteoblasts. Like abaloparatide, sclerostin antibodies have not been studied in patients on chronic steroids; however, they have shown benefit when administered subcutaneously in postmenopausal women and men. In postmenopausal women specifically, romosozumab increased BMD when compared to placebo and teriparatide and decreased the incidence of fractures when compared to placebo and alendronate.85–89 Fewer data exist in men, but a Phase III trial noted an increased spine and hip BMD in romosozumab when compared to placebo.90
Organizational glucocorticoid-induced osteoporosis guidelines
Different major specialty organizations have published guidelines regarding the use of teriparatide in the treatment of glucocorticoid-induced osteoporosis. The International Osteoporosis Foundation and the European Calcified Tissue Society (IOF-ECTS) published a set of guidelines in 2012, where they mentioned teriparatide as a frontline option, along with alendronate, etidronate, risedronate, and zoledronic acid.91 They reviewed the data included above but did not differentiate among the medications listed as frontline. The UK National Osteoporosis Guideline Group (NOGG) and the American College of Rheumatology (ACR) both published guidelines in 2017.92,93 The NOGG gave teriparatide an A-grade recommendation based on proven benefit in spine BMD, hip BMD, and vertebral fracture but recommend alendronate and risedronate as first line due to lower cost, mentioning that teriparatide can be considered if these are not tolerated or contraindicated. The ACR took a similar stance, recommending oral bisphosphonates over teriparatide in adults at moderate and high risk of major fracture due to the cost and burden of therapy with daily injections. In patients who have a new fracture or significant worsening of BMD on oral bisphosphonates, the ACR recommended consideration of teriparatide at that time.
Conclusion
Glucocorticoid-induced osteoporosis is an underrecognized complication of chronic steroid therapy. The underlying mechanism of disease, that of a low-turnover state characterized by a decrease in the formation of new bone, differs from that of postmenopausal disease, and the optimal treatment of the disease may differ as well. Anabolics, such as teriparatide, a recombinant parathyroid hormone, offer a way to increase bone production in a way that traditional antiresorptive therapies do not. The optimal treatment course and long-term effects are still under investigation, but teriparatide therapy appears to improve bone quality and decrease fracture risk when compared to antiresorptive therapy. Future directions include investigations into new anabolic medications, head-to-head comparisons between anabolics, as well as more study on the optimal duration of anabolic therapy and the potential for repeated courses of therapies.
Disclosure
Kenneth G Saag reports personal fees from Abbvie, Amgen, Ironwood/AstraZeneca, Bayer, Gilead, Horizon, Kowa, Radius, Roche/Genetech, SOBI, Takeda, and Teijin; and grants from Amgen, Ironwood/AstraZeneca, Horizon, SOBI, Takeda, Radius, and Mereo, outside the submitted work. Kenneth G Saag has served as a consultant to Amgen, Radius and Roche. The authors report no other conflicts of interest in this work.
References
1. Thiele K, Buttgereit F, Huscher D, Zink A. German collaborative arthritis centres. Current use of glucocorticoids in patients with rheumatoid arthritis in Germany. Arthritis Rheum. 2005;53(5):740–747. doi:10.1002/(ISSN)1529-0131
2. Walsh LJ, Wong CA, Pringle M, Tattersfield AE. Use of oral corticosteroids in the community and the prevention of secondary osteoporosis: a cross sectional study. BMJ. 1996;313(7053):344–346. doi:10.1136/bmj.313.7053.344
3. Laugesen K, Jørgensen JOL, Sørensen HT, Petersen I. Systemic glucocorticoid use in Denmark: a population-based prevalence study. BMJ Open. 2017;7(5):e015237. doi:10.1136/bmjopen-2016-015237
4. Fardet L, Petersen I, Nazareth I. Prevalence of long-term oral glucocorticoid prescriptions in the UK over the past 20 years. Rheumatology (Oxford). 2011;50(11):1982–1990.
5. Curtis JR, Westfall AO, Allison JJ, et al. Longitudinal patterns in the prevention of osteoporosis in glucocorticoid-treated patients. Arthritis Rheum. 2005;52(8):2485–2494.
6. Mudano A, Allison J, Hill J, Rothermel T, Saag K. Variations in glucocorticoid induced osteoporosis prevention in a managed care cohort. J Rheumatol. 2001;28(6):1298–1305.
7. Compston J. Glucocorticoid-induced osteoporosis: an update. Endocrine. 2018;61(1):7–16.
8. Swanson C, Lorentzon M, Conaway HH, Lerner UH. Glucocorticoid regulation of osteoclast differentiation and expression of receptor activator of nuclear factor-kappaB (NF-kappaB) ligand, osteoprotegerin, and receptor activator of NF-kappaB in mouse calvarial bones. Endocrinology. 2006;147(7):3613–3622.
9. Hofbauer LC, Gori F, Riggs BL, et al. Stimulation of osteoprotegerin ligand and inhibition of osteoprotegerin production by glucocorticoids in human osteoblastic lineage cells: potential paracrine mechanisms of glucocorticoid-induced osteoporosis. Endocrinology. 1999;140(10):4382–4389.
10. Ito S, Suzuki N, Kato S, Takahashi T, Takagi M. Glucocorticoids induce the differentiation of a mesenchymal progenitor cell line, ROB-C26 into adipocytes and osteoblasts, but fail to induce terminal osteoblast differentiation. Bone. 2007;40(1):84–92. doi:10.1016/j.bone.2006.07.012
11. Colditz J, Thiele S, Baschant U, et al. Osteogenic Dkk1 mediates glucocorticoid-induced but not arthritis-induced bone loss. J Bone Miner Res. 2019;19:1314–1325. doi:10.1002/jbmr.3702
12. Beier EE, Sheu TJ, Resseguie EA, et al. Sclerostin activity plays a key role in the negative effect of glucocorticoid signaling on osteoblast function in mice. Bone Res. 2017;9(5):17013. doi:10.1038/boneres.2017.13
13. Sato AY, Cregor M, Delgado-Calle J, et al. Protection from glucocorticoid-induced osteoporosis by anti-catabolic signaling in the absence of sost/sclerostin. J Bone Miner Res. 2016;31(10):1791–1802. doi:10.1002/jbmr.2869
14. Ohnaka K, Tanabe M, Kawate H, Nawata H, Takayanagi R. Glucocorticoid suppresses the canonical Wnt signal in cultured human osteoblasts. Biochem Biophys Res Commun. 2005;329(1):177–181. doi:10.1016/j.bbrc.2005.01.117
15. Wang FS, Lin CL, Chen YJ, et al. Secreted frizzled-related protein 1 modulates glucocorticoid attenuation of osteogenic activities and bone mass. Endocrinology. 2005;146(5):2415–2423. doi:10.1210/en.2004-1050
16. Canalis E, Mazziotti G, Giustina A, Bilezikian JP. Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int. 2007;18(10):1319–1328. doi:10.1007/s00198-007-0394-0
17. Seibel MJ, Cooper MS, Zhou H. Glucocorticoid-induced osteoporosis: mechanisms, management, and future perspectives. Lancet Diabetes Endocrinol. 2013;1(1):59–70. doi:10.1016/S2213-8587(13)70045-7
18. Liu Y, Porta A, Peng X, et al. Prevention of glucocorticoid-induced apoptosis in osteocytes and osteoblasts by calbindin-D28k. J Bone Miner Res. 2004;19(3):479–490. doi:10.1359/JBMR.0301242
19. Weinstein RS, Jilka RL, Parfitt AM, Manolagas SC. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J Clin Invest. 1998;102(2):274–282. doi:10.1172/JCI2799
20. Balasubramanian A, Wade SW, Adler RA, et al. Glucocorticoid exposure and fracture risk in patients with new-onset rheumatoid arthritis. Osteoporos Int. 2016;27(11):3239–3249. doi:10.1007/s00198-016-3646-z
21. Amiche MA, Albaum JM, Tadrous M, et al. Fracture risk in oral glucocorticoid users: a Bayesian meta-regression leveraging control arms of osteoporosis clinical trials. Osteoporos Int. 2016;27(5):1709–1718. doi:10.1007/s00198-015-3455-9
22. van Everdingen AA, Siewertsz van Reesema DR, Jacobs JW, Bijlsma JW. Low-dose glucocorticoids in early rheumatoid arthritis: discordant effects on bone mineral density and fractures? Clin Exp Rheumatol. 2003;21(2):155–160.
23. Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Use of oral corticosteroids and risk of fractures. J Bone Miner Res. 2000;15(6):993–1000. doi:10.1359/jbmr.2000.15.6.993
24. Ramsey-Goldman R, Dunn JE, Huang CF, et al. Frequency of fractures in women with systemic lupus erythematosus: comparison with United States population data. Arthritis Rheum. 1999;42(5):882–890. doi:10.1002/1529-0131(199905)42:5<882::AID-ANR6>3.0.CO;2-C
25. Michel BA, Bloch DA, Fries JF. Predictors of fractures in early rheumatoid arthritis. J Rheumatol. 1991;18(6):804–808.
26. van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Oral corticosteroids and fracture risk: relationship to daily and cumulative doses. Rheumatology (Oxford). 2000;39(12):1383–1389. doi:10.1093/rheumatology/39.12.1383
27. Haugeberg G, Ørstavik RE, Uhlig T, Falch JA, Halse JI, Kvien TK. Bone loss in patients with rheumatoid arthritis: results from a population-based cohort of 366 patients followed up for two years. Arthritis Rheum. 2002;46(7):1720–1728. doi:10.1002/art.10408
28. Van Staa TP, Laan RF, Barton IP, Cohen S, Reid DM, Cooper C. Bone density threshold and other predictors of vertebral fracture in patients receiving oral glucocorticoid therapy. Arthritis Rheum. 2003;48(11):3224–3229. doi:10.1002/art.11283
29. Laan RF, van Riel PL, van de Putte LB, van Erning LJ, van’t Hof MA, Lemmens JA. Low-dose prednisone induces rapid reversible axial bone loss in patients with rheumatoid arthritis. A randomized, controlled study. Ann Intern Med. 1993;119(10):963–968. doi:10.7326/0003-4819-119-10-199311150-00001
30. Saag KG, Emkey R, Schnitzer TJ, et al. Alendronate for the prevention and treatment of glucocorticoid-induced osteoporosis. Glucocorticoid-induced osteoporosis intervention study group. N Engl J Med. 1998;339(5):292–299. doi:10.1056/NEJM199807303390502
31. Emkey R, Delmas PD, Goemaere S, et al. Changes in bone mineral density following discontinuation or continuation of alendronate therapy in glucocorticoid-treated patients: a retrospective, observational study. Arthritis Rheum. 2003;48(4):1102–1108. doi:10.1002/art.10861
32. Reid DM, Hughes RA, Laan RF, et al. Efficacy and safety of daily risedronate in the treatment of corticosteroid-induced osteoporosis in men and women: a randomized trial. European corticosteroid-induced osteoporosis treatment study. J Bone Miner Res. 2000;15(6):1006–1013. doi:10.1359/jbmr.2000.15.6.1006
33. Cohen S, Levy RM, Keller M, et al. Risedronate therapy prevents corticosteroid-induced bone loss: a twelve-month, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum. 1999;42(11):2309–2318. doi:10.1002/1529-0131(199911)42:11<2309::AID-ANR8>3.0.CO;2-K
34. Mok CC, Ying KY, To CH, et al. Raloxifene for prevention of glucocorticoid-induced bone loss: a 12-month randomised double-blinded placebo-controlled trial. Ann Rheum Dis. 2011;70(5):778–784. doi:10.1136/ard.2010.143453
35. Shin K, Park SH, Park W, et al. Monthly oral ibandronate reduces bone loss in korean women with rheumatoid arthritis and osteopenia receiving long-term glucocorticoids: a 48-week double-blinded randomized placebo-controlled investigator-initiated trial. Clin Ther. 2017;39(2):268–278.e2. doi:10.1016/j.clinthera.2017.01.008
36. Reid DM, Devogelaer JP, Saag K, et al. HORIZON investigators. Zoledronic acid and risedronate in the prevention and treatment of glucocorticoid-induced osteoporosis (HORIZON): a multicentre, double-blind,double-dummy, randomised controlled trial. Lancet. 2009;373(9671):1253–1263. doi:10.1016/S0140-6736(09)60250-6
37. Saag KG, Wagman RB, Geusens P, et al. Denosumab versus risedronate in glucocorticoid-induced osteoporosis: a multicentre, randomised, double-blind, active-controlled, double-dummy, non-inferiority study. Lancet Diabetes Endocrinol. 2018;6(6):445–454. doi:10.1016/S2213-8587(18)30075-5
38. Wallach S, Cohen S, Reid DM, et al. Effects of risedronate treatment on bone density and vertebral fracture in patients on corticosteroid therapy. Calcif Tissue Int. 2000;67(4):277–285.
39. Adachi JD, Saag KG, Delmas PD, et al. Two-year effects of alendronate on bone mineral density and vertebral fracture in patients receiving glucocorticoids: a randomized, double-blind, placebo-controlled extension trial. Arthritis Rheum. 2001;44(1):202–211. doi:10.1002/1529-0131(200101)44:1<202::AID-ANR27>3.0.CO;2-W
40. Teitelbaum SL, Seton MP, Saag KG. Should bisphosphonates be used for long-term treatment of glucocorticoid-induced osteoporosis? Arthritis Rheum. 2011;63(2):325–328.
41. Carpinteri R, Porcelli T, Mejia C, et al. Glucocorticoid-induced osteoporosis and parathyroid hormone. J Endocrinol Invest. 2010;33(7 suppl):16–21.
42. Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):1434–1441.
43. Body JJ, Gaich GA, Scheele WH, et al. A randomized double-blind trial to compare the efficacy of teriparatide [recombinant human parathyroid hormone (1-34)] with alendronate in postmenopausal women with osteoporosis. J Clin Endocrinol Metab. 2002;87(10):4528–4535.
44. Orwoll ES, Scheele WH, Paul S, et al. The effect of teriparatide [human parathyroid hormone (1-34)] therapy on bone density in men with osteoporosis. J Bone Miner Res. 2003;18(1):9–17.
45. Lane NE, Sanchez S, Modin GW, Genant HK, Pierini E, Arnaud CD. Parathyroid hormone treatment can reverse corticosteroid-induced osteoporosis. Results of a randomized controlled clinical trial. Journal of Clinical Investigation. 1998;102(8):1627–1633.
46. Saag KG, Shane E, Boonen S, et al. Teriparatide or alendronate in glucocorticoid-induced osteoporosis. N Engl J Med. 2007;357(20):2028–2039.
47. Saag KG, Zanchetta JR, Devogelaer JP, et al. Effects of teriparatide versus alendronate for treating glucocorticoid-induced osteoporosis: thirty-six-month results of a randomized, double-blind, controlled trial. Arthritis Rheum. 2009;60(11):3346–3355.
48. Glüer CC, Marin F, Ringe JD, et al. Comparative effects of teriparatide and risedronate in glucocorticoid-induced osteoporosis in men: 18-month results of the EuroGIOPs trial. J Bone Miner Res. 2013;28(6):1355–1368.
49. Eastell R, Chen P, Saag KG, et al. Bone formation markers in patients with glucocorticoid-induced osteoporosis treated with teriparatide or alendronate. Bone. 2010;46(4):929–934.
50. Farahmand P, Marin F, Hawkins F, et al. Early changes in biochemical markers of bone formation during teriparatide therapy correlate with improvements in vertebral strength in men with glucocorticoid-induced osteoporosis. Osteoporos Int. 2013;24(12):2971–2981.
51. Burshell AL, Möricke R, Correa-Rotter R, et al. Correlations between biochemical markers of bone turnover and bone density responses in patients with glucocorticoid-induced osteoporosis treated with teriparatide or alendronate. Bone. 2010;46(4):935–939.
52. Burghardt AJ, Link TM, Majumdar S. High-resolution computed tomography for clinical imaging of bone microarchitecture. Clin Orthop Relat Res. 2011;469(8):2179–2193.
53. Zysset PK, Dall’Ara E, Varga P, Pahr DH. Finite element analysis for prediction of bone strength. Bonekey Rep. 2013;2:386.
54. Mellibovsky L, Prieto-Alhambra D, Mellibovsky F, et al. Bone tissue properties measurement by reference point indentation in glucocorticoid-induced osteoporosis. J Bone Miner Res. 2015;30(9):1651–1656.
55. Pothuaud L, Carceller P, Hans D. Correlations between grey-level variations in 2D projection images (TBS) and 3D microarchitecture: applications in the study of human trabecular bone microarchitecture. Bone. 2008;42(4):775–787.
56. Bousson V, Bergot C, Sutter B, Levitz P, Cortet B. Scientific committee of the groupe de recherche et d’Information sur les ostéoporoses. Trabecular bone score (TBS): available knowledge, clinical relevance, and future prospects. Osteoporos Int. 2012;23(5):1489–1501.
57. Saag KG, Agnusdei D, Hans D, et al. Trabecular bone score in patients with chronic glucocorticoid therapy-induced osteoporosis treated with alendronate or Teriparatide. Arthritis Rheumatol. 2016;68(9):2122–2128.
58. Vahle JL, Sato M, Long GG, et al. Skeletal changes in rats given daily subcutaneous injections of recombinant human parathyroid hormone (1-34) for 2 years and relevance to human safety. Toxicol Pathol. 2002;30(3):312–321.
59. Andrews EB, Gilsenan AW, Midkiff K, et al. The US postmarketing surveillance study of adult osteosarcoma and teriparatide: study design and findings from the first 7 years. J Bone Miner Res. 2012;27(12):2429–2437.
60. Harris D, Midkiff K, Gilsenan A, Andrews E Twelve-year study update for a postmarketing case series study of adult osteosarcoma and teriparatide in the U.S.
61. Vahle JL, Long GG, Sandusky G, Westmore M, Ma YL, Sato M. Bone neoplasms in F344 rats given teriparatide [rhPTH(1-34)] are dependent on duration of treatment and dose. Toxicol Pathol. 2004;32(4):426–438.
62. Gold DT, Pantos BS, Masica DN, Misurski DA, Marcus R. Initial experience with teriparatide in the United States. Curr Med Res Opin. 2006;22(4):703–708.
63. Jolette J, Wilker CE, Smith SY, et al. Defining a noncarcinogenic dose of recombinant human parathyroid hormone 1-84 in a 2-year study in Fischer 344 rats. Toxicol Pathol. 2006;34(7):929–940.
64. O’Ryan FS, Khoury S, Liao W, et al. Intravenous bisphosphonate-related osteonecrosis of the jaw: bone scintigraphy as an early indicator. J Oral Maxillofac Surg. 2009;67(7):1363–1372.
65. Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med. 2008;358(12):1304–1306.
66. Murphy DR, Smolen LJ, Klein TM, Klein RW. The cost effectiveness of teriparatide as a first-line treatment for glucocorticoid-induced and postmenopausal osteoporosis patients in Sweden. BMC Musculoskelet Disord. 2012;13:213.
67. Black DM, Bilezikian JP, Ensrud KE, et al. PaTH study investigators. One year of alendronate after one year of parathyroid hormone (1-84) for osteoporosis. N Engl J Med. 2005;353(6):555–565.
68. Black DM, Greenspan SL, Ensrud KE, et al. PaTH study investigators. The effects of parathyroid hormone and alendronate alone or in combination in postmenopausal osteoporosis. N Engl J Med. 2003;349(13):1207–1215.
69. Cosman F, Nieves JW, Zion M, Barbuto N, Lindsay R. Retreatment with teriparatide one year after the first teriparatide course in patients on continued long-term alendronate. J Bone Miner Res. 2009;24(6):1110–1115.
70. Finkelstein JS, Wyland JJ, Leder BZ, et al. Effects of teriparatide retreatment in osteoporotic men and women. J Clin Endocrinol Metab. 2009;94(7):2495–2501.
71. Odell WD. Testosterone treatment of men treated with glucocorticoids. Arch Intern Med. 1996;156(11):1133–1134.
72. Hall GM, Daniels M, Doyle DV, Spector TD. Effect of hormone replacement therapy on bone mass in rheumatoid arthritis patients treated with and without steroids. Arthritis Rheum. 1994;37(10):1499–1505.
73. Kung AW, Chan TM, Lau CS, Wong RW, Yeung SS. Osteopenia in young hypogonadal women with systemic lupus erythematosus receiving chronic steroid therapy: a randomized controlled trial comparing calcitriol and hormonal replacement therapy. Rheumatology (Oxford). 1999;38(12):1239–1244.
74. Hall GM, Spector TD, Delmas PD. Markers of bone metabolism in postmenopausal women with rheumatoid arthritis. Effects of corticosteroids and hormone replacement therapy. Arthritis Rheum. 1995;38(7):902–906.
75. Rossouw JE, Anderson GL, Prentice RL, et al. Writing Group for the women’s health initiative investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the women’s health initiative randomized controlled trial. JAMA. 2002;288(3):321–333.
76. Adami S, Fossaluzza V, Rossini M, et al. The prevention of corticosteroid-induced osteoporosis with nandrolone decanoate. Bone Miner. 1991;15(1):73–81.
77. Reid IR, Wattie DJ, Evans MC, Stapleton JP. Testosterone therapy in glucocorticoid-treated men. Arch Intern Med. 1996;156(11):1173–1177.
78. Crawford BA, Liu PY, Kean MT, Bleasel JF, Handelsman DJ. Randomized placebo-controlled trial of androgen effects on muscle and bone in men requiring long-term systemic glucocorticoid treatment. J Clin Endocrinol Metab. 2003;88(7):3167–3176.
79. Leder BZ, O’Dea LS, Zanchetta JR, et al. Effects of abaloparatide, a human parathyroid hormone-related peptide analog, on bone mineral density in postmenopausal women with osteoporosis. J Clin Endocrinol Metab. 2015;100(2):697–706.
80. Cosman F, Miller PD, Williams GC, et al. Eighteen months of treatment with subcutaneous abaloparatide followed by 6 months of treatment with alendronate in postmenopausal women with osteoporosis: results of the ACTIVExtend trial. Mayo Clin Proc. 2017;92(2):200–210.
81. Miller PD, Hattersley G, Riis BJ, et al. ACTIVE study investigators. Effect of abaloparatide vs placebo on new vertebral fractures in postmenopausal women with osteoporosis: a randomized clinical trial. JAMA. 2016;316(7):722–733.
82. Bone HG, Cosman F, Miller PD, et al. ACTIVExtend: 24 months of alendronate after 18 months of abaloparatide or placebo for postmenopausal osteoporosis. J Clin Endocrinol Metab. 2018;103(8):2949–2957.
83. McCloskey EV, Johansson H, Oden A, et al. The effect of abaloparatide-SC on fracture risk is independent of baseline FRAX fracture probability: a post hoc analysis of the ACTIVE study. J Bone Miner Res. 2017;32(8):1625–1631.
84. Tella SH, Kommalapati A, Correa R. Profile of abaloparatide and its potential in the treatment of postmenopausal osteoporosis. Cureus. 2017;9(5):e1300.
85. Cosman F, Crittenden DB, Ferrari S, et al. FRAME study: the foundation effect of building bone with 1 year of romosozumab leads to continued lower fracture risk after transition to denosumab. J Bone Miner Res. 2018;33(7):1219–1226.
86. Genant HK, Engelke K, Bolognese MA, et al. Effects of romosozumab compared with teriparatide on bone density and mass at the spine and hip in postmenopausal women with low bone mass. J Bone Miner Res. 2017;32(1):181–187.
87. Langdahl BL, Libanati C, Crittenden DB, et al. Romosozumab (sclerostin monoclonal antibody) versus teriparatide in postmenopausal women with osteoporosis transitioning from oral bisphosphonate therapy: a randomised, open-label, phase 3 trial. Lancet. 2017;390(10102):1585–1594.
88. Cosman F, Crittenden DB, Adachi JD, et al. Romosozumab treatment in postmenopausal women with osteoporosis. N Engl J Med. 2016;375(16):1532–1543.
89. Saag KG, Petersen J, Brandi ML, et al. Romosozumab or alendronate for fracture prevention in women with osteoporosis. N Engl J Med. 2017;377(15):1417–1427.
90. Lewiecki EM, Blicharski T, Goemaere S, et al. A phase 3 randomized placebo-controlled trial to evaluate efficacy and safety of romosozumab in men with osteoporosis. J Clin Endocrinol Metab. 2018;103(9):3183–3193.
91. Lekamwasam S, Adachi JD, Agnusdei D, et al. A framework for the development of guidelines for the management of glucocorticoid-induced osteoporosis. Osteoporos Int. 2012;23(9):2257–2276.
92. Buckley L, Guyatt G, Fink HA, et al. American college of rheumatology guideline for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res (Hoboken). 2017;69(8):1095–1110.
93. Compston J, Cooper A, Cooper C, et al. National Osteoporosis Guideline Group (NOGG). UK clinical guideline for the prevention and treatment of osteoporosis. Arch Osteoporos. 2017;12(1):43.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.