")
Back to Journals » Drug Design, Development and Therapy » Volume 15
An Overview of Lenalidomide in Combination with Rituximab for the Treatment of Adult Patients with Follicular Lymphoma: The Evidence to Date
Authors Yilmaz U , Salihoglu A, Soysal T
Received 25 June 2021
Accepted for publication 25 August 2021
Published 7 September 2021 Volume 2021:15 Pages 3809—3820
DOI https://doi.org/10.2147/DDDT.S281614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qiongyu Guo
Umut Yilmaz, Ayse Salihoglu, Teoman Soysal
Division of Hematology, Department of Internal Medicine, Cerrahpasa Faculty of Medicine, Istanbul University-Cerrahpasa, Istanbul, Turkey
Correspondence: Umut Yilmaz
Istanbul University-Cerrahpasa, Cerrahpasa Medical Faculty, Department of Internal Medicine, Division of Hematology, Fatih, Istanbul, Turkey
Tel +90 541 797 76 47
Email [email protected]
Abstract: Follicular lymphoma (FL) is an indolent (low-grade) malignancy of B cells and is among the most common hematological cancers affecting adults. Its clinical presentation, natural course, and severity are highly variable. Management of FL depends on the clinical setting; most patients require multiple lines of treatment. Chemoimmunotherapy is the standard of care for FL patients needing treatment; however, alternative treatments are limited for refractory patients or those unfit for chemoimmunotherapy. Multiple alternatives to chemoimmunotherapy for FL are being developed, with some showing significant promise. Lenalidomide combination with rituximab (LR) is among the most successful and extensively studied novel approaches. LR has been compared head-to-head in clinical trials with rituximab monotherapy and chemoimmunotherapy in the frontline and to lenalidomide or rituximab monotherapy in the relapsed or refractory setting for the treatment of FL. Initial reports of these nine trials have been published in the last decade, and their long-term data will be available in the coming years. LR offered superior efficacy to either lenalidomide or rituximab monotherapy alone. The RELEVANCE trial compared the efficacy of LR with chemoimmunotherapy among 1030 FL patients and demonstrated similar efficacy with a different side effect profile. Myelosuppression, rash, and fatigue were among the significant adverse events. Most patients treated with LR received thromboprophylaxis. This paper aims to summarize and comment on the published evidence regarding LR treatment for FL through a literature review. The clinical trials will be presented in detail, and methodological differences complicating their comparisons will be discussed.
Keywords: rituximab, lenalidomide, follicular lymphoma, chemo-free, R2
Introduction
Follicular lymphoma (FL) is the most common subtype of indolent B-cell malignancies and accounts for 20 to 30% of non-Hodgkin lymphomas (NHL), with an incidence of 2–3 cases per 100.000 persons per year. The median age of FL diagnosis is between 59 and 65 years across different studies.1,2
Indolent B-cell malignancies, also called low-grade non-Hodgkin lymphomas have distinct clinical courses from most other cancers making their management principles unique. The relentless tumor progression and need for immediate therapy widely associated with cancer do not necessarily follow the diagnosis of indolent lymphoma. Along with other indolent lymphomas, FL is expected to run a chronic course with a preserved quality of life, interrupted by periods of increased tumor activity that may entail antineoplastic therapy. Indolent B-cell malignancies’ response to treatment is usually satisfactory and durable; however, they are expected to relapse or progress following a variable period of tumor inactivity. Allogeneic hematopoietic stem cell transplantation (HCT) has curative potential in FL; however, it is rarely employed as many patients are transplantation-ineligible due to old age or donor unavailability by the time it may be indicated.3 Thus, indolent lymphomas are practically considered incurable. Another exceptional feature of low-grade lymphomas is the risk of transformation to high-grade lymphomas, which may occur any time from the diagnosis. There are no prospective studies showing that large-cell transformation is avoidable with therapy; however, a retrospective analysis suggests this risk was lower in patients who received rituximab.4 In this context, the natural course of the patient inflicted by FL may range from minimally symptomatic, stable disease for many years; to life-threatening tumor progression within weeks.
Local therapy options are limited to rare patients with early-stage FL. Most patients have advanced disease at the time of the diagnosis, but not all need treatment. The Groupe d’Etude des Lymphomes Folliculaires (GELF)5 or British National Lymphoma Investigation (BNLI)6 criteria can guide assessing a patient’s need for systemic therapy; however, this is a highly individualized measure and will be discussed later.
Chemoimmunotherapy with an anti-CD20 monoclonal antibody (rituximab) added to a cytotoxic chemotherapy backbone (cyclophosphamide, doxorubicin, vincristine, prednisone (CHOP) combination or bendamustine) has become a worldwide recommendation for the medically fit patients with advanced FL at the first-line or in the late-relapse settings. However, chemoimmunotherapy may not be efficient in patients with chemo-resistant disease, early relapse after chemoimmunotherapy, and those heavily pretreated due to multiple relapses. Cytotoxic treatments may also be unsuitable due to patients’ old age, comorbidities, prior toxicities, and personal expectations from medical care. Considering the chronic nature of the disease, preservation of the quality of life is also a priority, making practical administration routes and favorable side effect profiles other attractive features for FL treatments. Thus, the availability of therapeutic options with different mechanisms of action and different profiles of toxicity are invaluable to FL patients.
Until the last decade, the alternatives of chemoimmunotherapy were limited to more intensive cytotoxic therapies or less efficient approaches such as rituximab monotherapy and palliative treatments. Recent advances are expanding the armamentarium for FL management with novel agents belonging to the classes of immunomodulatory agents, third-generation monoclonal antibodies, phosphoinositide 3ʹ-kinase (PI3K), enhancer of zeste homolog 2 (EZH2), Bruton tyrosine kinase inhibitors, bispecific antibodies, and epigenetic modifiers.7 Standing out among these novel treatment approaches is the rituximab combination with the second-generation immunomodulatory agent lenalidomide (LR).
Lenalidomide is an orally active drug with a variety of proposed mechanisms of antineoplastic activity. Lenalidomide’s molecular target is thought to be the cereblon part of the E3 ubiquitin ligase complex. Lenalidomide binding to this complex brings about the degradation of transcription factors IKAROS and AIOLOS. These molecular changes are thought to have antiproliferative, antiangiogenic, and immunomodulatory effects against B-cell neoplasms.8 The most significant adverse events associated with lenalidomide use are myelosuppression and increased tendency to thrombotic complications often necessitating dose-modifications and thromboprophylaxis, respectively. Fatigue and rash are among the common non-specific adverse events; although often mild in nature, they may be frustrating and potentially result in interruption or cessation of lenalidomide treatment.9
The initial studies with LR are showing clinical efficacy rates in alignment with those of chemoimmunotherapy. The promising data with LR were met with great enthusiasm, and extensive studies have been designed in the last decade to understand its benefits better, assess its hypothesized practicality, and identify related prognostic biomarkers for the treatment of FL. In this paper, we will attempt to study the published clinical evidence regarding LR use for FL, focusing mainly on its efficacy and safety. We will also discuss its place among alternative regimens and comment on its potential to influence the general approach for managing FL.
We performed a review of the literature using the PubMed database and searched with the keyword combination “((follicular lymphoma) AND (lenalidomide)) AND (rituximab)”; articles written in languages other than English were excluded. The search resulted in 78 articles, 22 excluded due to irrelevant content after reviewing the abstracts. Articles contributing data regarding LR treatment for FL were designated for full-text analysis. Three additional articles were discovered through the hand search of the references of one of the retrieved articles. Thus, the full text of 59 articles was evaluated, mainly focusing on the data from the clinical grounds. We planned to pool the data from different publications under the trials that these articles retrieved their data. Articles not constructed of the data from clinical trials were studied separately and noted when considered significant.
The literature review from the PubMed database revealed a total number of thirteen articles directly reporting on the nine clinical trials that studied the use of LR for FL. Seven articles reported on trials that studied the combination of LR with other drugs for FL. We also found several reviews, commentaries, case reports, and biomarker studies regarding the topic; these studies will be mentioned later in this section. We summarized the treatment schedules of the initially mentioned nine clinical trials in Table 1 and compared the selected findings in Table 2.
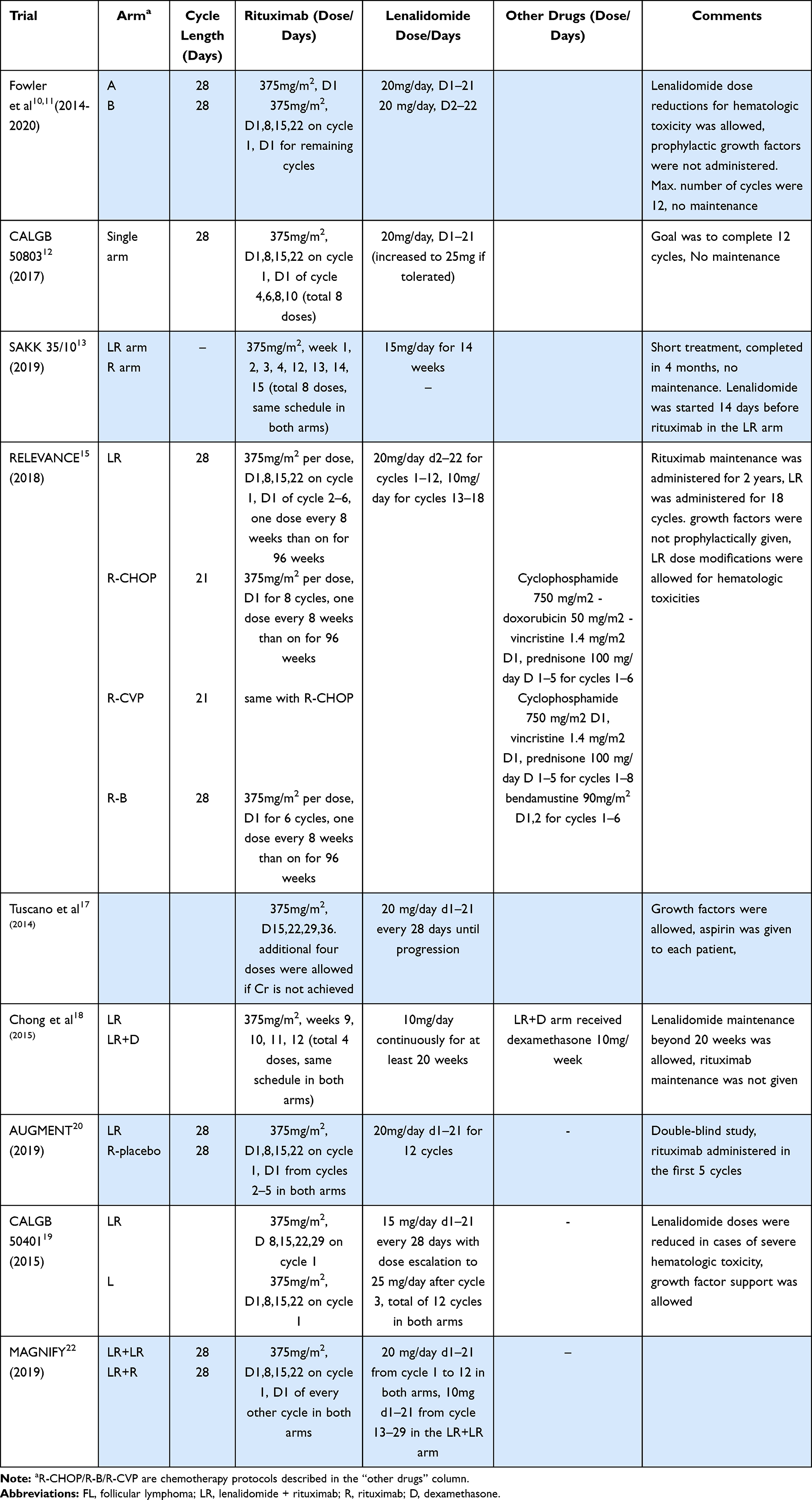 |
Table 1 Treatment Schedules of the Nine Clinical Trials Studying LR Treatment for FL |
 |
Table 2 Selected Results from the Clinical Trials Studying LR for FL |
LR Treatment for FL - Trials for the Frontline Therapy
Fowler et al conducted a single-arm, open-label, phase-2 trial evaluating the safety and efficacy of LR as a first-line treatment for advanced-stage indolent lymphoma patients. The primary objective was to determine the rates of responses. A total of 156 patients were enrolled between the years 2008 and 2012 at a single institution. Early results were published in 2014,10 and the results for the FL subpopulation of 79 patients were updated in 2021.11 Patients with grade 3 FL were not included in the trial, and the indications for treatment were not standardized (only half of the patients met the GELF criteria for high tumor burden). Thirty-six patients (46%) were older than age 60. Lugano 2014 criteria using the Positron emission tomography (PET) data were used to define responses in the 2021 follow-up analysis. The treatment duration in this trial was six to twelve months, and no maintenance therapy was administered. Three patients discontinued treatment before the first response assessment. In the intention-to-treat analysis, 75 of 79 (95%) patients responded to LR, and 68 of 79 (86%) achieved complete remission (CR) as the best response. Twenty-four of 79 patients needed dose reduction, while 51% of patients experienced a grade ≥ 3 toxicity. Overall, seven patients discontinued LR treatment prematurely, three due to progression, and two due to arterial thrombosis. Interestingly, achievement of CR was more likely in female patients; however, it was independent of traditional risk factors (FLIPI, PRIMA-PI) and the SUV values of the involved lymph nodes. Dose-reduced patients did not have a lower incidence of CR. The Median follow-up was 103 months. Four patients had died, eight had developed secondary malignancies, and one was lost to follow-up. Progression-free survival (PFS) at eight years was 65%. 8-year PFS was closely associated with CR as the best response. PFS was shorter in non-Caucasian patients. Progression of disease at 24 months was only 7% in those who achieved CR.
CALGB 50803 was an open-label, single-arm, multicenter phase-2 trial to study LR at frontline treatment for FL. The primary objectives were to determine the response rates and to measure the time to progression. Patients with grade 3b FL or high-risk FLIPI scores were excluded. The study inclusion criteria did not obligate treatment need for enrollment. The trial took place from the year 2010 to 2012 and recruited 65 patients with advanced-stage FL. The results were published in 2017.12 Fifty-one of 65 patients completed the treatment protocol—two patients discontinued due to progression, six due to intolerance. Fourteen patients went through grade 3 or 4 neutropenia; however, only one episode of febrile neutropenia was detected during the trial. Among other noteworthy adverse events, grade 3 rash developed in five patients, and four patients reported severe fatigue. ITT analysis revealed an overall response rate of 95%, CR was achieved in 47 patients (72%). Per-protocol analysis revealed a CR rate of 92%. Five-year PFS was 72%, there were no cases of secondary malignancies, and all patients were alive after a median follow-up of five years.
SAKK 35/10 was a randomized, open-label, phase-2 clinical trial designed to compare the outcomes of rituximab monotherapy (R arm) with LR (LR arm) for the frontline therapy of FL. The primary endpoint was to compare the CR rates at six months. Grade 3b FL patients were excluded. Random assignment was stratified according to the FLIPI score, grade, and the presence of bulky disease. Only the FL patients considered to need systemic therapy were included. The duration of treatment was four months. The trial recruited 77 patients for each arm, and 79% of patients were aged 60 or above. The results were published in 2019 after a median follow-up of four years.13 Twenty-two patients in the R arm discontinued treatment; 18 due to lack of efficacy, and one due to toxicity. Nineteen patients in the LR arm discontinued treatment, 13 due to toxicity (most due to rash, one due to thrombosis), and three due to lack of efficacy. In the ITT analysis, the LR arm had significantly higher CR rates than the R arm (CR: 61% vs 36% P < 0.001, by independent response review of computed tomography (CT) imaging, 1999 IWG criteria). PFS and time to next treatment (TTNT) were also significantly longer in the LR arm (median PFS: 5 years vs 2.3 years/TTNT: unreached vs 2.1 years). Patients in the LR arm experienced Grade ≥ 3 toxicity at a higher rate (56% vs 22%). Severe neutropenia was observed in 23% of patients in the LR arm; however, no episode of febrile neutropenia was detected. Five patients developed secondary cancers in the LR arm compared to three in the R arm. A total of 14 deaths were observed, seven in both arms. No death was judged to be related to treatment. A sub-study analyzed the mRNA expression levels of Th17 axis-related genes from the tumor tissues of 71 patients from this trial. High Th17 signature was a poor prognostic factor in the R arm with significantly shorter PFS. This effect was not observed in the LR arm, suggesting that the addition of lenalidomide neutralized the negative prognostic impact of this potential biomarker.14
Conducted between 2011 and 2014, the RELEVANCE trial is the first Phase III trial and the most extensive study concerning LR treatment in FL. It was a randomized, open-label study conducted in 137 centers designed to demonstrate superiority comparing LR with chemoimmunotherapy for the frontline treatment of FL. The primary endpoints were the CR rate at 120 weeks and PFS. Previously untreated grade 1–3a FL patients who fulfilled the GELF criteria or had either elevated LDH or B2-microglobulin levels were randomly assigned to two arms. Randomization was stratified according to age, FLIPI score, and the presence of bulky disease. LR arm was planned to receive 18 cycles of treatment followed by two years of rituximab maintenance. Chemoimmunotherapy arm was designed to receive rituximab with either bendamustine or CHOP or cyclophosphamide, vincristine, prednisone (CVP) combination followed by rituximab maintenance for two years. The study results were published in 201815 after a median follow-up of 37 months, and it is expected to be updated in 2024. The median age was 59 in both arms, and the β-2 microglobulin levels were elevated in 51% of the patients. A total of 1030 patients were enrolled in the trial, and response rates were studied in the ITT population. Only 5% of patients in the chemoimmunotherapy group received R-CVP. Overall, 69% of patients in the LR arm and 71% of patients in the chemoimmunotherapy arm completed the planned treatment and maintenance. The dose modifications were more common, and relative dose intensity was lower in the LR arm. The rates of severe neutropenia and neutropenic fever were higher in the chemoimmunotherapy arm than the LR arm, suggesting that LR may be safer against infectious complications. Severe cutaneous reactions were more common in the LR arm than the chemoimmunotherapy arm (4% vs <1%). Thrombotic complications were seen only in 2% of patients for both arms; however, most patients in the LR arm received thromboprophylaxis. The second primary malignancy rates were 7% for the LR arm and 10% for the chemoimmunotherapy arm. Responses were assessed according to the 1999 International Working Group criteria reviewed by independent researchers; PET imaging was not utilized. The best overall response rates for the chemoimmunotherapy arm and the LR arm were 89% and 84%, respectively. The rates of achievement of CR for the chemoimmunotherapy arm were 67% versus 59% in the LR arm. The statistical analysis of best treatment responses during the RELEVANCE trial was not presented in the paper, and treatment efficacies were compared through the response states at week 120 and by PFS analysis. The 120th-week response assessments demonstrated no statistically significant difference between the efficacy of the chemoimmunotherapy arm and the LR arm. The CR rate at week 120 was 53% for the chemoimmunotherapy arm and 48% for the LR arm (p=0.13), proposing that LR is not inferior to chemoimmunotherapy for the frontline treatment of FL. However, it should be noted that 15.3% of the patients were not included for response evaluation at week 120 due to various reasons. The 3-year PFS was similar between the two arms (78% vs 77%). The subgroup analysis of patients treated with R-Bendamustine hinted towards a lower hazard ratio for progression at 3-years than LR (3-years PFS for R-Bendamustine appears to be 88%); however, authors concluded that the study was not powered to address the comparison of LR to different chemoimmunotherapy protocols. FLIPI score was a useful prognostic marker in the chemoimmunotherapy arm but not in the LR arm. OS was 94% in both arms. A sub-study proposed that more patients in the LR arm achieved a complete molecular response, and the depth of response using minimal residual disease analysis from peripheral blood or bone marrow was correlated with longer PFS.16
LR Treatment for FL - Trials on Previously Treated Patients
Tuscano et al conducted a phase-2 trial, studying the effects of LR on patients with R/R indolent lymphoma in need of therapy guided by the GELF criteria. The primary objective was to determine the response rates. The results were published in 2014 after a median follow-up of 43 months.17 Thirty patients were enrolled, 22 had FL, and half of the patients were heavily pretreated. All patients had received rituximab, and half were refractory to rituximab. Four to eight doses of rituximab were scheduled, and lenalidomide was to be continued until progression. Three patients discontinued treatment before response assessments (two due to toxicity, one due to transformation). Among the FL patients, 17 had an overall response, while nine achieved complete remission. After a median follow-up of 43 months, the median PFS for the nine patients who achieved CR was not reached. Of note, two cases of tumor lysis syndrome with 25mg/day lenalidomide were observed. Also, the responses showed a trend towards improvement with continued lenalidomide treatment, as 34% of patients achieved their best responses only in the maintenance phase.
Chong et al studied the outcomes of LR treatment in indolent lymphoma patients, refractory to rituximab or rituximab-chemotherapy combinations. A total of 50 patients were enrolled in this single-center, open-label, phase-2 trial. Lenalidomide maintenance was permitted. The primary endpoint was the overall response rate. A subset of the patients also received 10mg dexamethasone once every week. The initial results were published in 2015 after a median follow-up of 39 months.18 Only five of 26 FL patients responded after the initial 8-week lenalidomide; however, the number of responding patients rose to 17 after the four rituximab doses. The increment in response following rituximab in these patients who were known to be rituximab-irresponsive suggested that rituximab and lenalidomide may have a synergistic action in FL. The authors proposed that regulatory T cell suppression induced by lenalidomide enhanced the antibody-directed cellular cytotoxicity response following the administration of rituximab. The researchers also studied the effect of the FcγRIIIa-158 phenylalanine associated with inadequate response to rituximab and found better efficacy compared to the historical controls with LR. The outcomes for the subgroup that received dexamethasone were not significantly different. The median PFS for FL patients was 16.5 months in this trial that did not include rituximab maintenance.
The CALGB 50401 trial was a multicenter, randomized, phase-2 trial designed to study the outcomes of LR versus lenalidomide in patients with relapsed or refractory FL, with the primary objective being the determination of response rates. The early results were published in 2015.19 Patients with grade 3b FL and those who progressed within six months of last rituximab therapy were excluded, and randomization was not stratified. The need for treatment for the recruited patients was not discussed. The trial recruited 91 patients randomized to two arms. Early treatment discontinuation was frequent in the L arm, mostly due to lymphoma progression. ORR was higher in the LR arm than the L arm (76.1% vs 53.3% P = 0.029), median PFS was longer in the LR arm (2 vs 1.1 years). An interesting note in this study was the trend towards fewer thrombotic events in the LR arm over the L arm (4% vs 16% P=0.157) thought to be due to better lymphoma control in the LR arm.
The AUGMENT was a phase-3, double-blind, randomized, multicenter trial to compare the outcomes of LR therapy with R-placebo in patients with relapsed or refractory indolent lymphomas. The primary endpoint was PFS. Grade 3b FL patients were not included. Patients either refractory to rituximab or had progressed within six months of the last rituximab dose were excluded. The initial results were published in 2019 after a median follow-up of 28.3 months.20 The need for treatment was judged by the investigators; no strict criteria were used. Eight doses of rituximab and twelve cycles of lenalidomide or placebo were scheduled. The treatment responses and follow-up data were assessed through CT or MRI imaging reviewed by independent researchers; PET imaging was not used. A total number of 358 patients were recruited; 295 of these had the diagnosis of FL. The randomization was stratified according to previous rituximab therapy, time from last treatment, and histology. Overall, 51% of the patients fulfilled the GELF criteria for high tumor burden, and 49% of patients were either refractory to or had progressed within two years of their last anti-lymphoma treatment. The rate of treatment completion and grade ≥3 adverse events were higher in the LR arm. Eighty-eight patients in the LR arm developed severe neutropenia; however, only five of these cases were complicated by neutropenic fever. Nearly 70% of patients in both arms received thromboprophylaxis, and thrombotic complications were rare in this trial (2% in the LR arm, 1% in the R arm). ORR, CR rates and median PFS were significantly better in the LR arm over the R-placebo arm (80% vs 55%, 35% vs 20%, and 39.4 months vs 13.9 months, respectively). Patient-reported outcomes from the trial were analyzed for health-related quality of life, showing no clinically meaningful changes from baseline across the post-baseline assessments for either arm.21 Among FL patients, the LR arm had higher two-year overall survival (OS) rates than the R-placebo arm (95% vs 86%, p=0.02). LR appeared to be superior to R-placebo in all FL patient subgroups analyzed, including the elderly and those judged to be unfit for cytotoxic chemotherapy.
MAGNIFY trial started recruiting patients in 2014, and the early results were updated in 2020 after a median follow-up of 23.7 months.22 The trial is designed to determine the optimal duration of lenalidomide in R/R indolent lymphoma and compare the outcomes of maintenance therapy with LR to rituximab. Three-hundred and seventy patients were enrolled (80% had FL grade 1–3a). All patients were scheduled for 12 cycles of LR (9 doses of rituximab), and those without progression were randomized to either LR or rituximab maintenance. Overall, 35% of patients prematurely discontinued LR therapy (13% due to adverse events, 11% due to progression). Although 36% experienced grade ≥3 neutropenia, only 3% of patients had an episode of febrile neutropenia. ORR for the FL patients was 70%, with 41% achieving CR. Median PFS was 39.4 months for FL patients, and outcomes were more favorable in patients without a history of rituximab failure and in those with less prior treatment exposure. We expect the comparison of LR maintenance with rituximab maintenance to be reported soon.
Other Clinical Studies with LR or LR Combinations in FL
A retrospective analysis of 356 untreated FL patients compared the efficacy of LR to R-chemotherapy.23 Fifty of the 94 patients who had received LR in this report were patients from the NCT00695786 trial (Fowler et al), and overall, 39 patients received LR for more than six cycles. The chemoimmunotherapy groups had a higher frequency of patients with high FLIPI scores and high tumor burden by GELF criteria. The three-year PFS for LR, BR, R-CHOP, R-CHOP + maintenance, BR + maintenance was 87%, 63%, 60%, 72%, 97% respectively. The study concluded that the efficacy of LR in untreated grade 1,2 FL was comparable to that of chemoimmunotherapy.
Tilly et al studied the outcomes of lenalidomide in combination with R-CHOP (R2-CHOP for untreated FL in a single-arm Phase 2 trial. The study was encouraged by the promising data in the FL subgroup of patients from the phase one trial (NCT00901615) conducted by the same group. The results were published in 2018.24 Eighty patients were enrolled, 59 patients achieved CR (74%), and three-year PFS was 79%. The study concluded that this combination was tolerable; however, the study did not achieve the primary objective of an 80% CR rate.
The HOVON110/ReBeL study is examining the use of bendamustine combination with LR for R/R FL. The initial Phase 1 part of the study has been published25 with the main finding that this combination is tolerable. The results of the phase-2 part are awaited.
The NCT00784927 trial studied LR combined with cyclophosphamide and dexamethasone (LR-CD) in untreated indolent lymphomas. This was a single-arm phase 2 trial that recruited 33 patients. Only eight patients in this trial had the diagnosis of FL. Among the eight FL patients, six achieved CR. The study concluded that LR-CD was a tolerable and potentially efficient option that could be studied further in larger patient populations.26
The combination of ibrutinib with LR and idelalisib with LR were studied in two single-arm phase two trials.27,28 Ibrutinib+LR and idelalisib+LR were judged to be excessively toxic without additional clinical benefit to LR for the frontline setting.
The NCT00294632 trial studied dexamethasone combination with LR for high-grade lymphomas. There were four patients with FL in this study, all four had grade 3 tumors, were heavily pretreated, and none achieved CR.29
Safety Profile of LR
Secondary Malignancies and Large Cell Transformation
Among the many fears with any newly developed antineoplastic therapy is the possibility that it may carry an excess risk of secondary malignancies, especially when compared to other treatment alternatives. The trials mentioned above have reported secondary malignancy rates of 3%, 7%, 6.5%, 10% and 0% within median follow up periods of 28,20 38,15 48,13 5911 and 6012 months respectively. AUGMENT and RELEVANCE trials had higher numbers of patients in their non-lenalidomide arms that developed secondary cancers than their LR arms. Overall, secondary cancers have not complicated FL patients treated with LR at an alarming rate in the initial studies; however, data with longer follow-up periods will be more informative in the coming years. Large cell transformation was not a common event in any of the trials concerning LR for FL, with the rates not exceeding 3% in any study.
Myelosuppression
Neutropenia developed nearly in half of the patients receiving LR when all the trials mentioned above are considered. Most researchers paid close attention to neutropenia and studied these events in detail. Although neutropenia was graded as a severe adverse event in most cases, its implications did not appear to be proportionately severe for patients receiving LR. Febrile neutropenia, the main clinical consequence of neutropenia, was rare with LR (<3% in all the trials). Neutropenia was judged to be predictable in most cases. In the RELEVANCE trial, febrile neutropenia complicated 34 of 503 patients in the chemoimmunotherapy arm compared to the eleven of 507 patients in the LR arm.15 These data support the view that patients receiving LR may be at lower risk for neutropenic complications, provided that appropriate dose modifications are employed.
Thromboembolic Complications
Among the most worrisome adverse events associated with lenalidomide is thromboembolism. Lymphoma patients treated with lenalidomide combined with a biologic agent have been reported to have a tendency towards less thrombosis risk when compared to other patients using lenalidomide.30 The thrombotic events were observed in approximately 5% of the patients receiving LR treatment in most trials.10,12,19,20 The thrombotic event rates in the RELEVANCE trial that studied 1030 patients was 7% for the LR arm and 5–6% for the R-chemotherapy arm; however, 78% of patients in the LR arm were given thromboprophylaxis, whereas this rate was 28% in the R-chemotherapy arm.15
Tumor Lysis Syndrome -Tumor Flare Reactions
Tumor lysis syndrome (TLS) was reported very rarely in LR trials for FL. Only one trial reported a dose reduction of lenalidomide from 25mg/day to 20mg/day for TLS.18 Six of 507 patients were reported to have severe TLS in the RELEVANCE trial. Tumor flare reaction (TFR) is a clinical entity that describes the initial inflammatory enlargement of malignant masses upon initiation of an antineoplastic treatment, frequently an immunomodulatory drug or an immune checkpoint inhibitor. TFR occurred in 5–10% of patients treated with LR across the trials; however, severe forms were rare (1%). One case of tumor flare reaction in a mediastinal lymph node resulting in atelectasis was reported, warning physicians to be aware of this phenomenon in patients receiving LR.31
Discussion
The nine trials conducted to study LR treatment in FL completed their scheduled treatment periods without significant events requiring their premature closure. The inclusion criteria (need of therapy, nuclear grade, prognostic scores) and the treatment schedules (dose and duration of lenalidomide and rituximab administration) were significantly heterogeneous between these nine trials. In the randomized trials, LR was more efficient than rituximab monotherapy. The RELEVANCE trial was conducted as a superiority trial; however, this was not demonstrated, and the results could only support that LR and chemoimmunotherapy had similar efficacy rates. The ORR ranged between 78% and 95% in the frontline and 65% to 80% in the R/R settings in the ITT populations. Strati et al reported an imposing 86% CR/CRi rates for LR in the first-line treatment of FL using PET imaging for response assessment.11 The CR/CRi rates were between 59% and 72% in the frontline and 35% to 41% in the R/R settings in the other trials concerning LR for FL (ITT populations). Historical trials studying rituximab and chemotherapy (R-chemo) combinations in FL reported CR rates around 30–40% and CR/CRi rates near 70% in the frontline settings. The ORR is reported as high as 90% in R/R settings for R-Bendamustine;32,33 however, these trials only recruited rituximab-naive patients. The AUGMENT trial demonstrated better two-year OS probability in R/R FL patients who received LR compared to those who received rituximab monotherapy. However, the AUGMENT trial was not powered to compare OS, and differences in subsequent treatments of these patients were not analyzed. Overall, the response rates with LR in both frontline and R/R settings for FL appear to be comparable with those reported for chemoimmunotherapy.
The PFS, TTNT, and OS for FL require extensive follow-ups to achieve meaningful results due to the unique natural course of indolent lymphomas outlined earlier. These data for LR are yet to reach adequate time for comparison with historical controls. The study with the most extended follow-up for LR11 is impressive, with an 8-year PFS rate of 65% for the frontline treatment that challenges the 69-month median PFS reported after frontline B-R for FL;34 however, the studies had significant methodological differences. In relapsed/refractory patients, median PFS was between 12.4 months to 39.4 months and was superior to rituximab monotherapy. The trials evaluating chemoimmunotherapy in R/R FL recruited patients that had no previous exposure to rituximab. Thus, the comparison of PFS/TTNT/OS of these trials with the data from the trials of LR would be biased. The rates and severity of adverse events were not alarming overall; however, cutaneous reactions and non-specific side effects such as fatigue prevented LR from being adequately administered in up to one-fifth of the patients.
A significant element of heterogeneity between the nine clinical trials was caused by the lack of a standard for assessing the treatment need. Clinicians interested in FL need a clear understanding of treatment indications to interpret the literature appropriately. As the clinical course of an FL patient is governed by complicated dynamics, systemic therapy may be delayed in a significant proportion of patients. Many a multitude of factors, including patient-related factors (performance status, comorbidities, age, medication use, life expectancy, personal preferences, the extent of the social support, accessibility to an isolated environment at times of epidemic/pandemic infections et), lymphoma related factors (FL grade, tumor volume, prior course, treatment responses, relapse times, the speed of progression, severity of the lymphoma-related clinical problems, etc), and the toxicity profiles of efficient treatment alternatives are among the variables that need to be assessed regularly to recognize the ideal time to commit to a treatment. Many researchers studied the outcomes of the initial watchful waiting approach in asymptomatic indolent lymphoma patients and reported median progression times between two to five years.6,35 Among the trials concerning the topic of this review, NCT01316523 used the GELF criteria strictly, RELEVANCE and SAKK 35/10 used their own, well-defined criteria, and others either depended on the judgment of the local investigator or did not assess the need for therapy at all. It is not surprising to find better response rates and longer PFS or TTNT in patients who do not need immediate treatment. Thus, the PFS and TTNT data reported in some of these trials may not be as lengthy in real life, especially at institutions where watchful waiting is methodically employed and systemic treatment is only administered when the physician and the patient are convinced of its need. The heterogeneity in the timing and duration of treatment also makes the results much more difficult to compare between different trials. Clinicians can be advised to approach these comparisons with caution and always note the treatment indications and duration (active treatment was four months in SAKK 35/10, and over two years in RELEVANCE) when evaluating PFS and TTNT data for indolent lymphomas.
Another significant topic of discussion might be the divergent definitions of response. When defined by functional imaging (2014 Lugano criteria that rely on PET/CT imaging), a patient’s response depth may differ from those dependent on anatomical assessments (1999 IWG criteria that rely on CT imaging). The two assessment methods were compared in 122 FL patients from the PRIMA trial, where PET/CT after induction therapy was negative in 90 patients. Among these 90 patients, 18 were classified as having a partial response (PR) by the 1999 IWG criteria. PFS rate at 42 months was significantly higher in post-induction PET/CT negative patients than PET/CT positive patients (70.7% vs 32.9%, P < 0.001). The PFS advantage of patients with complete remission over those with partial remission as defined by 1999 IWG criteria was not statistically significant (66.9% vs 55%, P = 0.27) in this study.36 Among the trials studying LR treatment for FL, only NCT-00695786 (Strati et al) evaluated the treatment responses with the 2014 Lugano criteria, and this may have played an important role in the higher CR rates reported in this study. We still need more data on the treatment responses based on PET/CT to emerge and improve our understanding of the clinical implications of PET-derived definitions of response states in indolent lymphomas.
Conclusion
LR treatment produces higher response rates and longer PFS than rituximab monotherapy in both the frontline and R/R settings of FL. The efficacy of LR and chemoimmunotherapy for the first-line treatment of FL has been demonstrated to be similar. Biomarkers predicting responsiveness to LR are urgently needed. Randomized clinical studies directly comparing LR, BR, and RCHOP along with the emergence of long-term data for LR will improve our understanding of the places these treatments have in FL management.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Junlén HR, Peterson S, Kimby E, et al. Follicular lymphoma in Sweden: nationwide improved survival in the rituximab era, particularly in elderly women: a Swedish Lymphoma Registry Study. Leukemia. 2015;29(3):668–676. doi:10.1038/leu.2014.251
2. Link BK, Friedberg JW, Taylor MD, et al. Follicular lymphoma in the United States: first report of the national LymphoCare study. J Clin Oncol. 2009;27(8):1202–1208. doi:10.1200/JCO.2008.18.1495
3. Sureda A, Zhang MJ, Dreger P, et al. Allogeneic hematopoietic stem cell transplantation for relapsed follicular lymphoma: a combined analysis on behalf of the Lymphoma Working Party of the EBMT and the Lymphoma Committee of the CIBMTR. Cancer. 2018;124(8):1733–1742. doi:10.1002/cncr.31264
4. Federico M, Mdc B, Marcheselli L, et al. Rituximab and the risk of transformation of follicular lymphoma: a retrospective pooled analysis. Lancet Haematol. 2018;5(8):e359–e367. doi:10.1016/S2352-3026(18)30090-5
5. Brice P, Bastion Y, Lepage E, et al. Comparison in low-tumor-burden follicular lymphomas between an initial no-treatment policy, prednimustine, or interferon alfa: a randomized study from the Groupe d’Etude des Lymphomes Folliculaires. Groupe d’Etude des Lymphomes de l’Adulte. J Clin Oncol. 2016;15(3):1110–1117. doi:10.1200/JCO.1997.15.3.1110
6. Ardeshna K, Smith P, Norton A, et al. Long-term effect of a watch and wait policy versus immediate systemic treatment for asymptomatic advanced-stage non-Hodgkin lymphoma: a randomised controlled trial. Lancet. 2003;362(9383):516–522. doi:10.1016/S0140-6736(03)14110-4
7. Matasar MJ, Luminari S, Barr PM, et al. Follicular lymphoma: recent and emerging therapies, treatment strategies, and remaining unmet needs. Oncologist. 2019;24(11):e1236. doi:10.1634/theoncologist.2019-0138
8. Gribben JG, Fowler N, Morschhauser F. Mechanisms of action of lenalidomide in B-cell non-Hodgkin lymphoma. J Clin Oncol. 2015;33(25):2803–2811. doi:10.1200/JCO.2014.59.5363
9. Cheson BD, Morschhauser F, Martin P. Management of adverse events from the combination of rituximab and lenalidomide in the treatment of patients with follicular and low-grade non-Hodgkin lymphoma. Clin Lymphoma Myeloma Leuk. 2020;20(9):563–571. doi:10.1016/j.clml.2020.03.009
10. Fowler NH, Davis RE, Rawal S, et al. Safety and activity of lenalidomide and rituximab in untreated indolent lymphoma: an open-label, phase 2 trial. Lancet Oncol. 2014;15(12):1311–1318. doi:10.1016/S1470-2045(14)70455-3
11. Strati P, Jain P, Johnson RJ, et al. Long term follow-up of lenalidomide and rituximab as initial treatment of follicular lymphoma. Blood. 2021;137(8):1124–1129.
12. Martin P, Jung SH, Pitcher B, et al. A Phase II trial of lenalidomide plus rituximab in previously untreated follicular non-Hodgkin’s lymphoma (NHL): CALGB 50803 (Alliance). Ann Oncol. 2017;28(11):2806–2812. doi:10.1093/annonc/mdx496
13. Zucca E, Rondeau S, Vanazzi A, et al. Short regimen of rituximab plus lenalidomide in follicular lymphoma patients in need of first-line therapy. Blood. 2019;134(4):353–362. doi:10.1182/blood-2018-10-879643
14. Menter T, Hayoz S, Zucca E, Kimby E, Dirnhofer S, Tzankov A. Immunomodulatory drugs may overcome the negative prognostic role of active Th17 axis in follicular lymphoma: evidence from the SAKK35/10 trial. Br J Haematol. 2020;190(4):e258–e261. doi:10.1111/bjh.16876
15. Morschhauser F, Fowler NH, Feugier P, et al. Rituximab plus lenalidomide in advanced untreated follicular lymphoma. N Eng J Med. 2018;379(10):934–947. doi:10.1056/nejmoa1805104
16. Delfau-Larue MH, Boulland ML, Beldi-Ferchiou A, et al. Lenalidomide/rituximab induces high molecular response in untreated follicular lymphoma: LYSA ancillary RELEVANCE study. Blood Adv. 2020;4(14):3217–3223. doi:10.1182/bloodadvances.2020001955
17. Tuscano JM, Dutia M, Chee K, et al. Lenalidomide plus rituximab can produce durable clinical responses in patients with relapsed or refractory, indolent non-Hodgkin lymphoma. Br J Haematol. 2014;165(3):375–381. doi:10.1111/bjh.12755
18. Chong EA, Ahmadi T, Aqui NA, et al. Combination of lenalidomide and rituximab overcomes rituximab resistance in patients with indolent B-cell and mantle cell lymphomas. Clin Cancer Res. 2015;21(8):1835–1842. doi:10.1158/1078-0432.CCR-14-2221
19. Leonard JP, Jung SH, Johnson J, et al. Randomized trial of lenalidomide alone versus lenalidomide plus rituximab in patients with recurrent follicular lymphoma: CALGB 50401 (Alliance). J Clin Oncol. 2015;33(31):3635–3640. doi:10.1200/JCO.2014.59.9258
20. Leonard JP, Trneny M, Izutsu K, et al. AUGMENT: a phase III study of lenalidomide plus rituximab versus placebo plus rituximab in relapsed or refractory indolent lymphoma. J Clin Oncol. 2019;37(14):1188.
21. Witlox WJA, Grimm SE, Riemsma R, et al. Lenalidomide with rituximab for previously treated follicular lymphoma and marginal zone lymphoma: an evidence review group perspective of a NICE single technology appraisal. PharmacoEconomics. 2021;39(2):171–180. doi:10.1007/s40273-020-00971-x
22. Andorsky DJ, Coleman M, Yacoub A, et al. MAGNIFY: phase IIIb interim analysis of induction R 2 followed by maintenance in relapsed/refractory indolent non-Hodgkin lymphoma. J Clin Oncol. 2019;37(15_suppl):7513. doi:10.1200/jco.2019.37.15_suppl.7513
23. Cheah CY, Chihara D, Ahmed M, et al. Factors influencing outcome in advanced stage, low-grade follicular lymphoma treated at MD Anderson Cancer Center in the rituximab era. Ann Oncol. 2016;27(5):895–901. doi:10.1093/annonc/mdw026
24. Tilly H, Morschhauser F, Casasnovas O, et al. Lenalidomide in combination with R-CHOP (R2-CHOP) as first-line treatment of patients with high tumour burden follicular lymphoma: a single-arm, open-label, phase 2 study. Lancet Haematol. 2018;5(9):e403–e410. doi:10.1016/S2352-3026(18)30131-5
25. Stevens WBC, Bakunina K, Cuijpers M, et al. HOVON110/ReBeL Study: results of the Phase I part of a randomized phase I/II study of lenalidomide, rituximab with or without bendamustine in patients with relapsed/refractory follicular lymphoma. HemaSphere. 2020;4(1):e325. doi:10.1097/HS9.0000000000000325
26. Rosenthal A, Dueck AC, Ansell S, et al. A phase 2 study of lenalidomide, rituximab, cyclophosphamide, and dexamethasone (LR-CD) for untreated low-grade non-Hodgkin lymphoma requiring therapy. Am J Hematol. 2017;92(5):467–472. doi:10.1002/ajh.24693
27. Smith SM, Pitcher BN, Jung SH, et al. Safety and tolerability of idelalisib, lenalidomide, and rituximab in relapsed and refractory lymphoma: the Alliance for Clinical Trials in Oncology A051201 and A051202 phase 1 trials. Lancet Haematol. 2017;4(4):e176–e182. doi:10.1016/S2352-3026(17)30028-5
28. Ujjani CS, Jung SH, Pitcher B, et al. Phase 1 trial of rituximab, lenalidomide, and ibrutinib in previously untreated follicular lymphoma: alliance A051103. Blood. 2016;128(21):2510–2516. doi:10.1182/blood-2016-06-718106
29. Wang M, Fowler N, Wagner-Bartak N, et al. Oral lenalidomide with rituximab in relapsed or refractory diffuse large cell, follicular and transformed lymphoma: a phase II clinical trial. Leukemia. 2013;27(9):1902–1909. doi:10.1038/leu.2013.95
30. Yamshon S, Christos PJ, Demetres M, Hammad H, Leonard JP, Ruan J. Venous thromboembolism in patients with B-cell non-Hodgkin lymphoma treated with lenalidomide: a systematic review and meta-analysis. Blood Adv. 2018;2(12):1429–1438. doi:10.1182/bloodadvances.2018016683
31. Suyama T, Yui T, Horiuchi A, Irie R, Osamura Y, Miyao N. Transient atelectasis due to hilar lymph node swelling affected by lenalidomide-induced tumor flare reaction. J Clin Exp Hematopathol. 2021;61(1):48–52. doi:10.3960/jslrt.20045
32. Rummel MJ, Al-Batran SE, Kim SZ, et al. Bendamustine plus rituximab is effective and has a favorable toxicity profile in the treatment of mantle cell and low-grade non-Hodgkin’s lymphoma. J Clin Oncol. 2005;23(15):3383–3389. doi:10.1200/JCO.2005.08.100
33. Robinson KS, Williams ME, van der Jagt RH, et al. Phase II multicenter study of bendamustine plus rituximab in patients with relapsed indolent B-cell and mantle cell non-Hodgkin’s lymphoma. J Clin Oncol. 2008;26(27):4473–4479. doi:10.1200/JCO.2008.17.0001
34. Rummel MJ, Niederle N, Maschmeyer G, et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: an open-label, multicentre, randomised, Phase 3 non-inferiority trial. Lancet. 2013;381(9873):1203–1210. doi:10.1016/S0140-6736(12)61763-2
35. Solal-Ceĺigny P, Bellei M, Marcheselli L, et al. Watchful waiting in low-tumor burden follicular lymphoma in the rituximab era: results of an F2-study database. J Clin Oncol. 2012;30(31):3848–3853. doi:10.1200/JCO.2010.33.4474
36. Trotman J, Fournier M, Lamy T, et al. Positron emission tomography-computed tomography (PET-CT) after induction therapy is highly predictive of patient outcome in follicular lymphoma: analysis of PET-CT in a subset of PRIMA trial participants. J Clin Oncol. 2011;29(23):3194–3200. doi:10.1200/JCO.2011.35.0736
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.