")
Back to Journals » Journal of Pain Research » Volume 13
An Observational Study of Intraoperative Neuromonitoring as a Safety Mechanism in Placement of Percutaneous Dorsal Root Ganglion Stimulation and Spinal Cord Stimulation Systems
Authors Hagedorn JM , Deer TR , Falowski SM , Yadav A , Comer A, Al-Asadi Z, Engle AM
Received 29 October 2020
Accepted for publication 26 November 2020
Published 8 December 2020 Volume 2020:13 Pages 3349—3353
DOI https://doi.org/10.2147/JPR.S289416
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Jonathan M Hagedorn,1 Timothy R Deer,2 Steven M Falowski,3 Abhishek Yadav,4 Ashley Comer,2 Zayd Al-Asadi,5 Alyson M Engle2
1Department of Anesthesiology and Perioperative Medicine, Division of Pain Medicine, Mayo Clinic, Rochester, MN, USA; 2The Spine and Nerve Center of the Virginias, Charleston, WV, USA; 3Argires-Marotti Neurosurgical Associates of Lancaster, Lancaster, PA, USA; 4Department of Anesthesiology and Perioperative Medicine, Brown University, Providence, RI, USA; 5University of South Florida, Tampa, FL, USA
Correspondence: Timothy R Deer Email [email protected]
Introduction: Percutaneous neurostimulator device placement, specifically dorsal root ganglion (DRG) stimulation and spinal cord stimulation (SCS), involves the placement of thin wires within the spinal canal at specific locations, the DRG or dorsal column of the spinal cord, respectively, to provide an electrical current that modifies the pain signal as it enters the central nervous system from the periphery. Placement of neurostimulator devices is generally safe overall, but not without risk of major and minor complications. In this study, we assess the use of intraoperative neuromonitoring (IONM) as a tool to improve the safety of placing neurostimulator devices and subsequently minimizing postoperative complications.
Methods: After IRB approval, an observational study was performed in 115 procedures to evaluate safety during placement of both temporary and permanent DRG and SCS systems and to document retrospectively any long-standing adverse events.
Results: The rate of intraoperative neuromonitoring abnormal activity was 1.7% (n = 2), which allowed prompt recognition of nerve irritation and lead repositioning. Of the 115 consecutive implant cases performed with IONM, the postoperative minor adverse event rate was 1.7% (n = 2), which were transient and corrected with reprogramming. There were no long-standing neurological complications.
Conclusion: In the largest observational study to date, we show that IONM creates a safe environment for patients undergoing SCS and DRG neurostimulator placement with the potential to decrease neurological complication rates. The use of IONM may be an alternative method to improve patient safety and outcomes as compared to monitor anesthesia care.
Keywords: dorsal root ganglion, spinal cord stimulation, intraoperative neuromonitoring, safety, complications
Introduction
Neurostimulation is an established therapy for chronic, refractory neuropathic pain.1 Two types of neurostimulator systems for treating pain include dorsal root ganglion (DRG) stimulation and spinal cord stimulation (SCS). These devices provide analgesia by modulating pain pathways through the delivery of electrical current. Electrical current is supplied by electrodes located on thin wires, called electrode leads, which are placed near target nerve structures. DRG neurostimulator leads are positioned near the target DRG. SCS leads are positioned dorsomedially in the epidural space at the optimal target level. Electrode leads can be placed surgically or percutaneously.2 Both techniques require proper anatomic positioning of the lead(s) to achieve therapeutic efficacy and to avoid complications and unwanted patient complaints. For example, thoracic electrodes positioned laterally rather than dorsomedially are more likely to result in unwanted painful stimulation of the thoracic nerve roots.2 Placement of neurostimulator devices is generally safe overall with proper technique and expertise, but it is not without risks of major and minor complications.3–7 Neurological injury is a rare but potentially devastating complication of this procedure that can have serious permanent neurologic sequalae including paralysis, hypesthesia, and incontinence. Neurological injury can result from direct needle trauma, infection, or bleeding that causes compression of nerve structures and potentially decreased blood flow to the spinal cord. Detection of neurological injury during placement is critical for both patient safety and proper lead placement. Guidelines have suggested that placement of a lead in the spinal canal or at the DRG should be performed in the awake and conversant patient, or if performed in the anesthetized patient, intraoperative neurophysiologic monitoring (IONM) should be performed during the surgical procedure.4 IONM can reduce the risk of neurological deficits by early detection of changes in motor-evoked potentials (MEP) and somatosensory-evoked potentials (SSEP) during SCS placement, as well as electromyography (EMG) and SSEP during DRG stimulator lead placement. In the past, IONM has been widely limited to placement of a surgical paddle lead requiring laminectomy.8–11 Increased utilization of IONM led to its additional availability. The use of IONM for patient safety is becoming more accepted for any patient requiring a general anesthetic or deep sedation for spinal interventions. Although there is sufficient data for the application of IONM during surgical lead placement, there is limited evidence supporting its use for percutaneous lead placement. This study provides additional evidence to the existing body of literature supporting the use of IONM for enhanced patient safety during percutaneous lead placement.
The reported incidence of complications from DRG stimulation ranges from reports of 32% to 43%.12 A large retrospective safety analysis reported overall safety event rate of SCS and DRG at 3.1% (n > 2000) and 3.2% (n > 500) respectively.13 The most common complication was infection at 1% for both SCS and DRG. Neurological safety events accounted for 0.6%, lower than the reported 8% from the ACCURATE trial.14 Another large retrospective review of 5458 percutaneous SCS implants reported an incidence of spinal cord injury at 2.35% (n=128) and spinal hematoma at 0.75% (n=41).10 The incidence of cerebrospinal fluid leak was estimated around 0.3% for SCS and 2.7% for DRG percutaneous lead placement.4,13 The adverse event rate of neurostimulation was around 10.5% (n=8) in patients with DRG and 13.2% (n=10) in the SCS group.14
Correct lead placement is essential for therapeutic efficacy and patient safety to minimize adverse events. Fluoroscopic imaging in the anterior-posterior and lateral projections is commonly used to confirm lead placement. However, in certain lead placements, quality imaging cannot be obtained.15 IONM has been proposed as an alternative method for confirmation of lead placement under general anesthesia.8,9,11,16–18 Falowski et al conducted a prospective, multicenter open-label trial evaluating SCS implantation in patients awake and conversive versus asleep with neuromonitoring. The study reported a lower adverse event rate in the asleep group 10.5% (n=2) compared with the awake group 54.5% (n=6).9 Data also suggest that neurostimulator leads placement with IONM use may result in improved therapeutic efficacy.9,19
The aim of this study was to evaluate the intraoperative and postoperative adverse event rates of percutaneous DRG and SCS lead placement under general anesthesia with IONM.
Materials and Methods
Permission to conduct this study was granted by the Saint Francis Hospital Institutional Review Board, who deemed it an exempt protocol and waived the need for consent given the retrospective design and lack of patient identifiers. The study was conducted in accordance with the Declaration of Helsinki. This was an observational study at the time of the implant and a retrospective case-series at the time of follow-up, in which 115 DRG and SCS cases performed at a single private practice institution between August 2017 and March 2020 were reviewed. Patients older than 14 years of age whose records contained a history of DRG stimulation or SCS with neuromonitoring were identified. Patients were included if they had undergone general anesthesia with IONM during DRG stimulation or SCS trial or implantation surgery. Patients were selected for general anesthesia during SCS placement because of the inability to be positioned in the prone position while awake due to discomfort (n=23) or difficulty breathing (n=3). A patient could appear multiple times in the study if they had a trial followed by a permanent implant and if IONM was utilized during each individual case. Documentation was reviewed for a single board-certified pain medicine physician who performed all DRG and SCS procedures. IONM was performed by a single neuromonitoring technologist with consistent equipment across all patients (Nuvasive, West Carrollton, Ohio). All DRG stimulation and SCS devices used in this study were manufactured by the same manufacturer (Abbott Neurological, Austin, Texas).
Each patient had to have a postoperative follow-up visit to be included in the study. All patient charts, operative notes, and follow-up visits were reviewed retrospectively. The primary diagnosis was identified for each patient. Patient charts were interrogated for demographics such as age and sex. The number of leads and location of lead placement during the DRG and SCS procedures were also recorded. Any change in SSEP, MEP, or EMG during the procedure were identified. Any changes made by the physician due to an abnormality were noted in the results section.
Postoperative follow-up notes were interrogated for any postoperative complication, such as numbness, paresthesia, infection, general discomfort, and tenderness. If any abnormalities arose and the procedure had to be revised, the reasoning for revision was noted.
Results
A retrospective chart review of 115 consecutive cases was performed. Stratification of case demographics, implant types, and follow-up results are displayed in Table 1. In the overall sample, the mean age was 58.2 ± 14.8 years. Seventy-two cases were females (62.6%) while 43 cases were males (37.4%). Table 2 represents the list of primary diagnoses for the cohort. Cervical radiculitis, herpetic neuralgia, and left ilioinguinal neuralgia represented one case (0.9%) each. This was followed by thoracic radiculopathy (n=3, 2.6%), peripheral neuropathy (n=6, 5.2%), and complex regional pain syndrome type 1 (n=7, 6.1%). The most common diagnoses prior to surgery were lumbar radiculitis (n=15, 13.0%), lumbar radiculopathy (n=24, 20.9%), and complex regional pain syndrome type 2 (n=57, 49.5%).
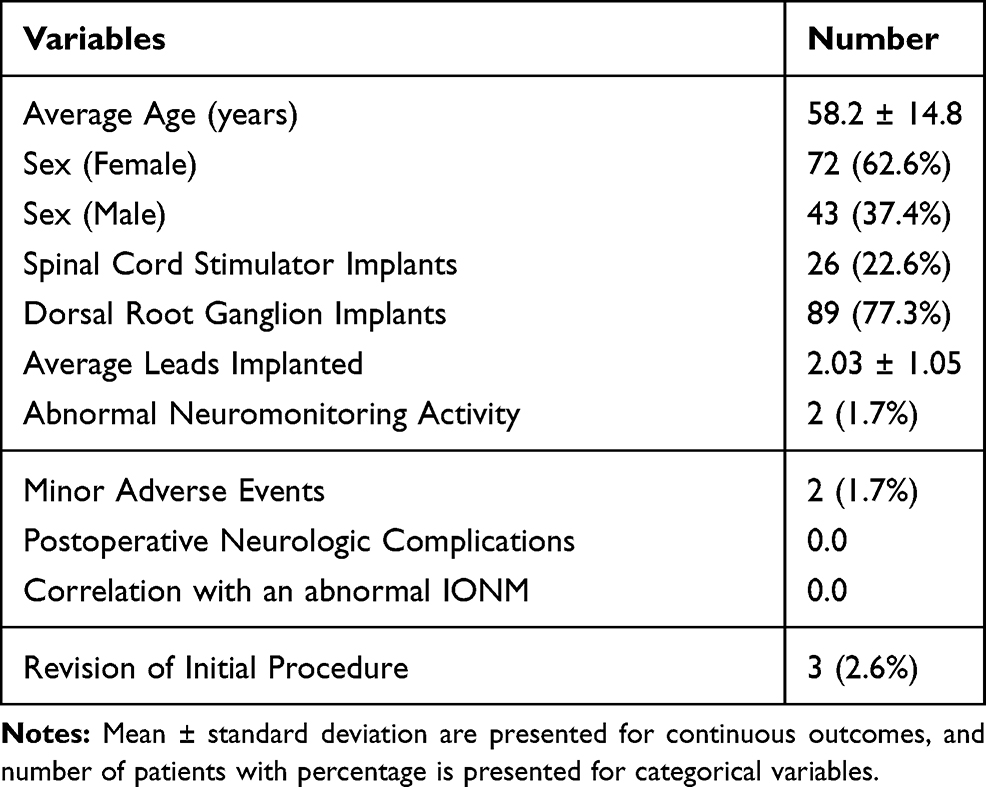 |
Table 1 Stratification of Demographics, Implants and Postoperative Complications |
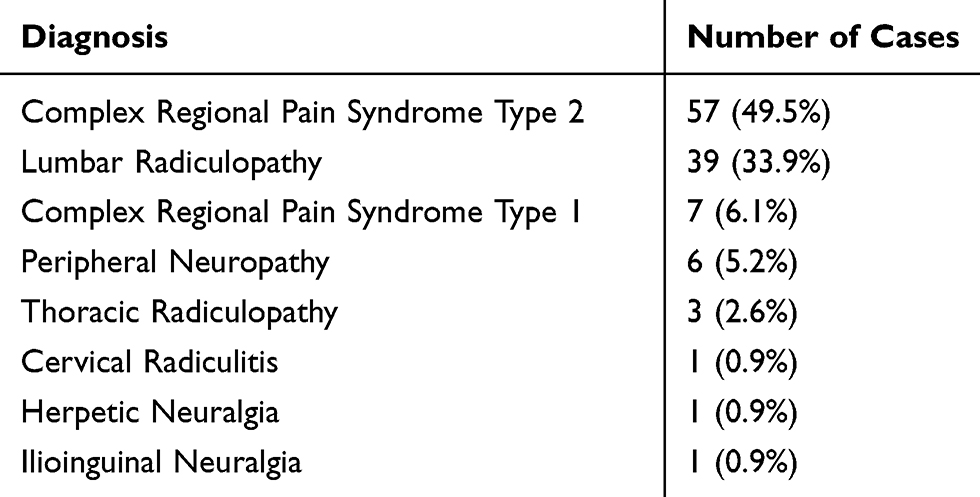 |
Table 2 Stratification of Diagnoses. Diagnoses and Case Numbers for the 115 Cases Performed |
Of the 115 cases performed, there were 26 SCS cases (22.6%) and 89 DRG cases (77.3%). Of the 26 SCS cases, 19 (73.1%) were permanent implants and seven (26.9%) were trials. Of the 89 DRG cases, 55 (61.8%) were permanent implants and 34 (38.2%) were trials. The mean number of leads implanted per case was 2.03 ± 1.05. Postoperative numbness occurred in two (1.7%) cases, which immediately resolved in both cases after device reprogramming by the company representative. There were no serious or major neurologic complications following any of the procedures. Three (2.6%) individuals required revision procedures for lead fracture (n=1) and suboptimal lead placement (n=2). The lead fracture was a DRG case. Suboptimal lead placement occurred in one DRG case and one SCS case. Of all 115 cases performed with IONM, two (1.7%) cases had abnormal neuromonitoring activity and neither of these individuals developed long-term sequelae.
Of the abnormalities, one was during a T12 and S1 bilateral DRG implantation. During the procedure, the S1 nerve root showed EMG activity during lead implantation. The lead was promptly removed, and the irritation resolved quickly. This led to a repositioning of the lead. No abnormal IONM activity was present during the remainder of the case. The patient had no postoperative complications. Additionally, no revision procedures have been performed on this individual to date.
The second abnormality was during a T7-T11 spanning SCS placement. After gaining epidural access at T12-L1 the lead was advanced superiorly but favored the right side. Before testing could be performed to confirm lead location, the SSEP signals decreased by 50% on the right side. The lead was quickly retracted with recovery of signals to baseline. It was then repositioned more midline with SSEP remaining stable. After lead placement, collision testing was performed on this individual to confirm proper lead location and SSEP remained stable. The patient had no postoperative complications. No revision procedures have been performed on this individual to date.
Discussion
Neurological Injury
Injury to the spinal cord or dorsal root ganglion is possible during implantation of a neurostimulation device given their close proximity. Anterior misplacement of the lead or needle can result in spinal cord injury sequelae. Dural puncture by the lead or needle can result in CSF leak and post-dural puncture headache. We reported no postoperative neurological complications which is an improvement over previous literature reports that range from 0.6 to 8%.10,13,14,19 The comparative rates of serious neurological complications are from larger retrospective reviews (n > 5458 percutaneous SCS implants and n > 500 DRG cases).4,10,13 Notably, Falowski et al showed improved operating time with the use of IONM possibly accounting for lower overall complication rates, as was seen in our study.9 Since it is difficult to compare retrospective studies due to the absence of selection standards, additional prospective studies are needed to determine the long-term utility of IONM in the DRG implanted patient. Placement without IONM in the patient under general anesthesia is not recommended; therefore, this type of comparative study is not advisable.
Overstimulation
Unwanted nerve stimulation is an adverse event with general reports around 10.5–13.2%.14
Confirmation of correct lead placement is essential for both therapeutic efficacy and patient safety. Improper lead position can cause nerve irritation leading to unwanted nerve stimulation. In our cohort, we found two instances of separate patients experiencing unwanted paresthesia production (1.7%). Both completely resolved with reprogramming. This study supports previous reports that suggest IONM may be an alternative method for confirmation of lead placement under general anesthesia.8,11,16,17
Overall Adverse Event Rates
Falowski’s prospective, multicenter open-label trial demonstrated lower adverse event rates in the asleep (IONM) group (n=2/19; 10.5%) compared with the awake group (n=6/11, 54.5%).9 Similarly, in the largest retrospective study on SCS and IONM with over 300 surgeries, the authors reported more favorable adverse events and fewer revisions with IONM.15 The results of our study corroborate these findings with a reported lower rate of adverse events with the use of IONM when compared to the adverse event rate reported in the literature when these procedures are performed without IONM.7,9,12,16,19
IONM Protocol
Integrating IONM during the implantation of neurostimulation devices is now a viable option for the interventional pain physician. IONM technique and protocols incorporate EMG and SSEP during cervical and thoracic lead placements.20 General endotracheal anesthesia with a secure airway for the prone patient is required. The preferred anesthetic of choice is total intravenous anesthesia without paralytics, which produces no effect on EMG and minimal effect on SSEP (eg, propofol and benzodiazepine).
Conclusion
The use of IONM may be an alternative method to improve patient safety and outcomes as compared to monitor anesthesia care. Comparative studies of these methods in the future will further determine the utilization of this method.
Disclosure
AY, ZA, and AME report no conflicts of interest in this work. JMH is a consultant for Abbott, Boston Scientific, and Nevro. JMH is on an advisory board for Boston Scientific. TRD is a consultant for Abbott, Axonics, Medtronic (Stimgenics), Vertos, Flowonix, Saluda Medical, SpineThera, Mainstay Medical, Nalu, Nevro Corp, Cornerloc, Paintec, SPR Therapeutics, and Boston Scientific (Vertiflex). TRD is a member of the advisory board for Abbott, Flowonix, Nalu, SPR Therapeutics, and Vertiflex. TRD has equity options in Vertos, SpineThera, Saluda Medical, Nalu, Paintec, and Cornerloc. TRD has funded research from Abbott, Mainstay Medical, Saluda Medical, SPR Therapeutics, and Vertiflex. TRD has a patent pending for the DRG paddle lead with Abbott. SMF is a consultant for Abbott, Medtronic, Vertiflex, Boston Scientific, and Vertos. SMF has equity in Saluda, SPR, AGR, CornerLoc, PainTeq, SpineThera, Neural Integrative Solutions, Thermaquil, Stimgenics, and Celery. SMF has research funding with Abbott, Medtronic, Vertiflex, Boston Scientific, Biotronik, and Stimgenics. AC is a consultant for Abbott, Saluda, SPR, and Vertos. The authors report no other conflicts of interest in this work.
References
1. Taylor RS. Spinal cord stimulation in complex regional pain syndrome and refractory neuropathic back and leg pain/failed back surgery syndrome: results of a systematic review and meta-analysis. J Pain Symptom Manage. 2006;31(4SUPPL):13–19. doi:10.1016/j.jpainsymman.2005.12.010
2. Falowski S, Celii A, Sharan A. Spinal cord stimulation: an update. Neurotherapeutics. 2008;5(1):86–99. doi:10.1016/j.nurt.2007.10.066
3. Van Buyten JP. Neurostimulation for chronic neuropathic back pain in failed back surgery syndrome. J Pain Symptom Manage. 2006;31(4SUPPL):25–29. doi:10.1016/j.jpainsymman.2005.12.012
4. Deer TR, Lamer TJ, Pope JE, et al. The neurostimulation appropriateness consensus committee (NACC) safety guidelines for the reduction of severe neurological injury. Neuromodulation. 2017;20(1):15–30. doi:10.1111/ner.12564
5. Deer TR, Narouze S, Provenzano DA, et al. The neurostimulation appropriateness consensus committee (NACC): recommendations on bleeding and coagulation management in neurostimulation devices. Neuromodulation. 2017;20(1):51–62. doi:10.1111/ner.12542
6. Deer TR, Provenzano DA, Hanes M, et al. The neurostimulation appropriateness consensus committee (NACC) recommendations for infection prevention and management. Neuromodulation. 2017;20(1):31–50. doi:10.1111/ner.12565
7. Deer TR, Pope JE, Lamer TJ, et al. The neuromodulation appropriateness consensus committee on best practices for dorsal root ganglion stimulation. Neuromodulation. 2019;22(1):1–35. doi:10.1111/ner.12845
8. Mammis A, Mogilner AY. The use of intraoperative electrophysiology for the placement of spinal cord stimulator paddle leads under general anesthesia. Oper Neurosurg. 2012;70(suppl_2):ons230–ons236. doi:10.1227/neu.0b013e318232ff29
9. Falowski SM, Sharan A, McInerney J, Jacobs D, Venkatesan L, Agnesi F. Nonawake vs awake placement of spinal cord stimulators: a prospective, multicenter study comparing safety and efficacy. Clin Neurosurg. 2019;84(1):198–205. doi:10.1093/neuros/nyy062
10. Petraglia FW, Farber S, Gramer R, et al. The incidence of spinal cord injury in implantation of percutaneous and paddle electrodes for spinal cord stimulation. Neuromodulation. 2016;19(1):85–90. doi:10.1111/ner.12370
11. Balzer JR, Tomycz ND, Crammond DJ, et al. Localization of cervical and cervicomedullary stimulation leads for pain treatment using median nerve somatosensory evoked potential collision testing. J Neurosurg. 2011;114(1):200–205. doi:10.3171/2010.5.JNS091640
12. Sivanesan E, Bicket MC, Cohen SP. Retrospective analysis of complications associated with dorsal root ganglion stimulation for pain relief in the FDA MAUDE database. Reg Anesth Pain Med. 2019;44(1):100–106. doi:10.1136/rapm-2018-000007
13. Deer T, Pope J, Hunter C, et al. Safety analysis of dorsal root ganglion stimulation in the treatment of chronic pain. Neuromodulation. 2019;2019. doi:10.1111/ner.12941
14. Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669–681. doi:10.1097/j.pain.0000000000000814
15. Shils JL, Arle JE. Intraoperative neurophysiologic methods for spinal cord stimulator placement under general anesthesia. Neuromodulation. 2012;15(6):560–572. doi:10.1111/j.1525-1403.2012.00460.x
16. Falowski SM, Dianna A. A prospective analysis of neuromonitoring for confirmation of lead placement in dorsal root ganglion stimulation. Oper Neurosurg. 2018;14(6):654–659. doi:10.1093/ons/opx172
17. Shils JL, Arle JE. Neuromonitoring for spinal cord stimulation lead placement under general anesthesia. J Clin Neurol. 2018;14(4):444–453. doi:10.3988/jcn.2018.14.4.444
18. Roth SG, Lange S, Haller J, et al. A prospective study of the intra-and postoperative efficacy of intraoperative neuromonitoring in spinal cord stimulation. Stereotact Funct Neurosurg. 2015;93(5):348–354. doi:10.1159/000437388
19. Hwang R, Field N, Kumar V, et al. Intraoperative neuromonitoring in percutaneous spinal cord stimulator placement. Neuromodulation. 2019;22(3):341–346. doi:10.1111/ner.12886
20. Falowski S, Dianna A. Neuromonitoring protocol for spinal cord stimulator cases with case descriptions. Int J Acad Med. 2016;2(2):132–144. doi:10.4103/2455-5568.196863
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.