")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
An Investigation of Organizational Correlates of Distress in Non-Clinician Biomedical Researchers in the United States
Authors Boitet LM , Meese KA , Colón-López A , Schwiebert LM , Rogers DA
Received 3 December 2022
Accepted for publication 24 January 2023
Published 5 February 2023 Volume 2023:16 Pages 333—343
DOI https://doi.org/10.2147/JMDH.S399517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Laurence M Boitet,1 Katherine A Meese,2 Alejandra Colón-López,3 Lisa M Schwiebert,4 David A Rogers5
1Department of Health Services Administration and University of Alabama at Birmingham (UAB) Medicine Office of Wellness, University of Alabama at Birmingham, Birmingham, AL, USA; 2Department of Health Services Administration and Director of Wellness Research, UAB Medicine Office of Wellness, University of Alabama at Birmingham, Birmingham, AL, USA; 3Department of Medical Education, University of Alabama at Birmingham, Birmingham, AL, USA; 4Department of Cell, Integrative, and Developmental Biology, University of Alabama at Birmingham, Birmingham, AL, USA; 5Department of Surgery and UAB Medicine Office of Wellness, University of Alabama at Birmingham, Birmingham, AL, USA
Correspondence: Laurence M Boitet, UAB Medicine Office of Wellness, 1720 2nd Ave. S, Birmingham, AL, 35294-2129, Tel +1 404 702 9301, Email [email protected]
Purpose: Challenges ushered by the COVID-19 pandemic led to an increased focus on the mental well-being of the healthcare workforce. Despite the important contribution non-clinician biomedical researchers make to the mission of academic medical centers, the well-being of this unique population remains understudied in the United States. The purpose of this study was to examine the individual and organizational correlates of distress among non-clinician biomedical researchers.
Methods: A survey was delivered to employees of a large academic medical center in the southeastern United States, including non-clinician biomedical researchers. Participants were asked to assess their own well-being using the validated Well-Being Index (WBI) tool, resilience, work and nonwork-related stressors and demographic descriptors. Descriptive statistics and bivariate analyses were conducted, and binary logistic regression was used to examine predictors of increased odds of overall distress.
Results: Nearly 44% of surveyed non-clinician biomedical researchers met the threshold for high distress which indicates an increased risk of suicidal ideation, turnover intention, and burnout. The major correlates of distress were at the organizational level, including perceived organizational support (OR 0.79, 95% CI 0.70– 0.90), heavy workload and long hours (OR 3.25, 95% CI 1.53– 6.88), inability or lack of support to take time off (OR 2.80, 95% CI 1.03– 7.66) and conflict with supervisor (OR 5.03, 95% CI 1.13– 22.1). While lower individual resilience (OR 0.69, 95% CI 0.54– 0.88) was statistically significantly associated with greater distress, it accounted for less than 10% of the overall variance when controlling for other work-related factors.
Conclusion: These findings suggest that developing organizational interventions that address institutional support for non-clinician biomedical researchers within academic medical centers represents an important opportunity to reduce distress within this population. While emphasizing individual resiliency as an important in the pursuit of well-being, it is also the responsibility of the organization to create and foster an environment in which employees can access their own resilience.
Keywords: burnout, job satisfaction, well-being, academic medical center
Introduction
Numerous studies examine physician and physician scientist burnout and well-being, with a substantial increase in investigations prompted by the stress posed by the COVID-19 pandemic.1–12 While there have been a few pre-COVID perspectives and commentaries about well-being and burnout amongst non-clinician biomedical scientists,13–19 this topic remains sparsely explored through original, empirical investigation. Furthermore, the experiences of distress and burnout for researchers are likely to have been altered by the conditions of the pandemic, as noted across arrange of disciplines within healthcare.20
For the purposes of this study, we adopted the definition of biomedical researchers as those who conduct research with the potential to improve human health within any field related or adjacent to medicine and biology.21,22 This research has built the foundation for modern medicine and is closely intertwined with education and clinical care to produce the highest quality patient care possible.23 Although non-clinician biomedical researchers traditionally play little to no role in direct patient interaction, reports indicate a considerable beneficial and measurable impact of research activity on patient care and healthcare performance in medical centers.24–26 Though integral to the academic medical center, these researchers are largely absent in current research and discussion about the well-being of healthcare employees, attributed at least in part due to their unique role in this setting and within the mission of the academic medical center.2
Prior to the COVID-19 pandemic, the literature pointed to numerous factors that were suggested to drive stress and burnout in biomedical researchers. One such study from the United Kingdom (UK) captured a wide array of researchers at all training levels, both in and outside of academia. Results indicated grim perspectives on the sustainability of well-being in the work environment, citing long working hours, insufficient career flexibility, and job insecurity.27 A similar UK study of academic researchers indicated unsupportive environments and negative work culture as additional factors contributing to high levels of stress in this population, which ultimately contribute to burnout and depression.17,27 Concerningly, researcher burnout has been found to be comparable to that of healthcare workers, with considerable risk of already experiencing or acquiring a mental health disorder.28 Similar results were demonstrated in trainees28 indicating impacts throughout the research pipeline. This was corroborated by a recent global study of doctoral students, where themes of stress, long working hours, anxiety, and depression were found.19
The pressures research-intensive academic medical centers have faced during the pandemic are likely to have resulted in increased stress throughout the organization, highlighting the need to understand the correlates and predictors of distress in non-clinician biomedical researchers. Consideration must be given to the organizational, team, and individual factors that ultimately contribute to well-being of these individuals in research-intensive medical centers. Understanding the unique correlates and degree of distress in biomedical researchers is important for organizations to comprehend. The status of research output is critical to medical center reputation and biomedical research faculty, trainees, and lab personnel are important contributors to this aim.29,30 Therefore, the well-being of those individuals is a critical consideration for the security of institutional research reputation and prestige, as well as the advancement of science to improve human health.
The minimal extant literature on the well-being of biomedical researchers in the United States (US) fails to address organizational drivers of distress among US biomedical scientists as they have been done in other geographic locations or focuses solely on trainees. Therefore, the aim of this study was to address this knowledge gap by assessing the correlates of distress using validated instruments in non-clinician biomedical researchers, a vastly understudied population of individuals, within an academic medical center in the US.
Materials and Methods
Study Design and Data Collection
We collected data using a cross-sectional, anonymous semi-structured survey that was administered to 6276 employees via email at a large medical center in the southeastern US. Data collection was conducted from June 7 to July 30, 2021 through an internet-based design using Qualtrics (Seattle, Washington). The distributed survey collected information from participants on self-reported distress, individual resilience, work and non-work-related stressors, organizational-level factors, and overall well-being. The survey has been validated and previously used to understand well-being across the entire healthcare team.20 Participants were informed about the anonymous, confidential nature of the survey as well as the minimal risks associated therein.
Participants were informed of the minimal risks associated with survey completion, limited to possible psychological distress from questions related to stressors. Participants were informed of the voluntary nature of the survey, as well as survey anonymity and confidentiality. Participants were required to consent to participate before beginning the survey. If they declined, they were automatically exited from the survey. The surveying organization’s Institutional Review Board reviewed and approved the study protocol.
Study Participants
The survey was sent to 6276 employees across various job roles including physician, clinical support staff, administration and management, and nurses. At the surveyed institution, 777 of all employees were classified as non-clinical researcher/scientist or lab personnel at the time of survey. A total of 2890 employees responded (46% response rate), and 325 (41.8% response rate) selected to role of “Non-Clinical Researcher/Scientist” or “Lab personnel.” Of the 325 “Non-Clinical Researcher/Scientist” or “Lab personnel” respondents, 3 participants self-identified as working in Administration/Management and 36 participants self-identified as working in Pathology or Hospital Laboratories. These 39 cases were omitted, as this study aimed to identify stressors in individuals working in traditional research-intensive roles. An additional 41 cases were omitted using list-wise deletion due to missing information resulting in a final analytic sample of non-clinician biomedical researchers of 245 (31.5%).
Dependent Variables
Data were collected concerning work- and nonwork-related stressors, and well-being. Well-being was measured using the 9-item Well-Being Index (WBI) tool that has been previously validated and used to capture levels of distress in the surveyed population.31–34 Scores derived from the WBI range from −2 to 9, with higher scores indicating higher distress. In the general population, scores greater than or equal to 2 are indicative of “high distress.” For the purpose of this study, WBI scores were recoded into a binary outcome. Scores greater than or equal to 2 were given the designation of 1 representing “high distress”, while scores lower than 2 received a value of 0.
Independent Variables
Work-Related Factors
A modified 8-item Perceived Organizational Support measure35 was utilized in this study, as previously described.20 Briefly, a 3-question adaptation of the Perceived Organizational Support scale was used to assess participants’ perception of their organization’s interest in their satisfaction, well-being, and extra efforts and contributions. Scores derived from this scale range from 3 to 15.
Moral distress was evaluated using a single-item measure,36 as previously described.20 Participants were asked the frequency at which they experienced moral distress, such as feeling as though they could not do the right thing or were unsure of what the right thing was on a 5-point Likert scale, with 5 indicating “almost every work day”, 4 “A few times a week”, 3 “Once a week”, 2 “A few times per month”, 1 “A few times or less”, and 0 “None.”
Participants were also asked to identify their major work-related stressors, such as rapid change in workflows or policies, inability or lack of support to take time off, conflict with colleagues, conflict with supervisor/leader, feeling mistreated by other employees at work, and increased responsibilities or job demands. Cases that indicated presence of a major work-related stressor were given the designation of 1, while those that did not receive a value of 0.
Nonwork-Related Factors
Participant resilience was measured using the previously described 2-item Connor-Davidson Resilience Scale (CD-RISC2).37 Scores from this scale range from 0 (not at all resilient) to 8 (highest resilience) and mean CD-RISC2 score for the general US adult population is 6.91. Participants were asked to identify their major nonwork-related stressors, ranging from childcare and social isolation to personal COVID-19 infection and politics.
Surveyed participants were prompted to provide information regarding gender and race. Due to sample size, gender was collapsed into three categories: Male, Female or Sexual Minority (which included those indicating “Non-Binary or Self-Describe”), and Prefer not to answer. Likewise, race was collapsed into three categories: White, Non-white, and Prefer not to answer.
Analytic Strategy
The data were analyzed using State SE 17.0 for Mac (Stata Corp., College Station, Texas). WBI distress, perceived organizational support, and CD-RISC2 scores were calculated and expressed as mean with standard deviation. Work-related stressors were expressed as frequency of indicating presence of the stressor. Moral distress was expressed as mean with standard deviation. Bivariate logistic regression was used to determine the association between the outcome variable (distress) and all numeric predictors. Chi-squared and Fisher’s Exact tests were conducted as appropriate to determine the association between the outcome variable and all categorical predictors. A multivariable binary logistic regression analysis with robust estimators was used to predict the odds of high distress when considering individual and organizational level factors in our sample population. To identify the relative contribution of each variable to the variance in distress in our sample, dominance analysis was performed.
Results
Participant Descriptives
The majority of the sample identified as White (n = 133; 54.3%), whereas 80 (32.7%) identified as other races and 32 (13.1%) preferred not to answer. Due to low numbers in each of the race categories, other races are represented here as “Non-White.” Approximately three-quarters of participants identified as Female or Sexual Minority (n = 150; 62.2%), with 73 (29.8%) identifying as Male and 22 (9%) who preferred not to answer.
Descriptive Analysis
Table 1 describes each variable by mean, standard deviation, percentage, and whether the variation in the selected predictors was significantly associated with distress in this sample of non-clinician biomedical researchers. Nearly half (43.67%) of the sample exhibited high distress scores (WBI ≥ 2) at the time of survey collection. In the bivariate analysis, heavy workload or long hours (30.6%, p < 0.001), inability or lack of support to take time off (14.7%, p < 0.001), conflict with colleagues (11.4%, p< 0.05), and conflict with supervisor (10.2%, p < 0.001) as major stressors were significantly associated with high WBI distress. Additionally, lower perceived organizational support scores were significantly associated with distress (p < 0.001). On an individual level, resiliency (p = 0.001) and moral distress frequency at work (p < 0.001) were significantly associated with high WBI distress.
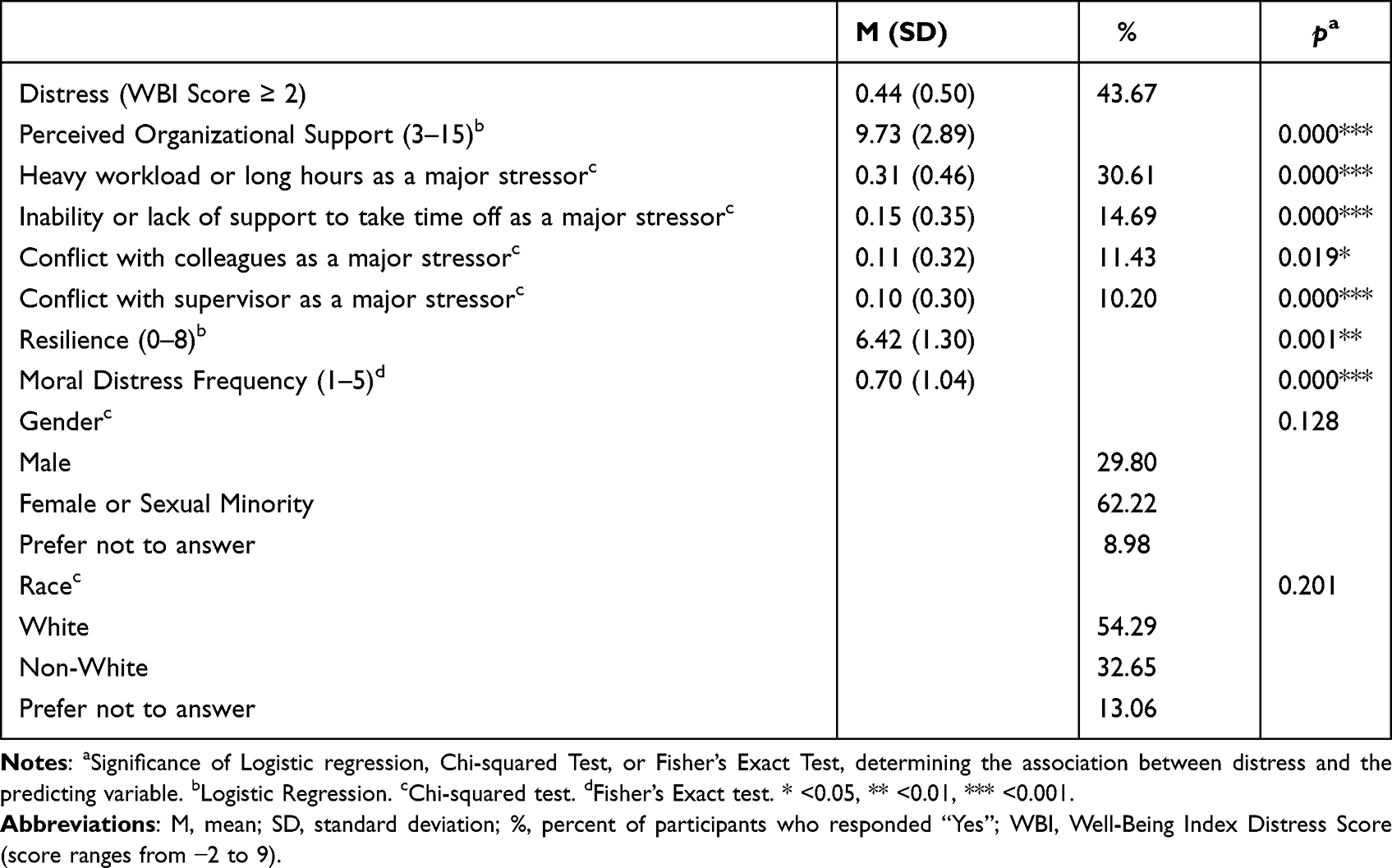 |
Table 1 Sample Characteristics of Non-Clinician Biomedical Researchers from a Southeastern Academic Medical Center from June to July 2021 (n = 245) |
Multivariate Regression
Table 2 presents results from multivariate logistic regression analyses predicting the odds of experiencing high distress in biomedical researchers. Odds ratios (OR) and robust standard errors (SE) are shown. In our sample, work-related stressors that were associated with increased odds of high WBI distress scores included heavy workload or long hours (OR = 3.25, p = 0.002), the inability or lack of support to take time off (OR = 2.80, p = 0.045), and conflict with supervisor (OR = 5.03, p = 0.033). Additionally, non-clinician biomedical researchers who felt more supported by their organization exhibited lower odds of high WBI distress (OR = 0.79, p < 0.001). In terms of nonwork-related variables, biomedical researchers with low resiliency scores had higher odds of distress (OR = 0.69, p = 0.003). No significant findings were observed related to conflict with colleagues as a major stressor, moral distress, gender, or race.
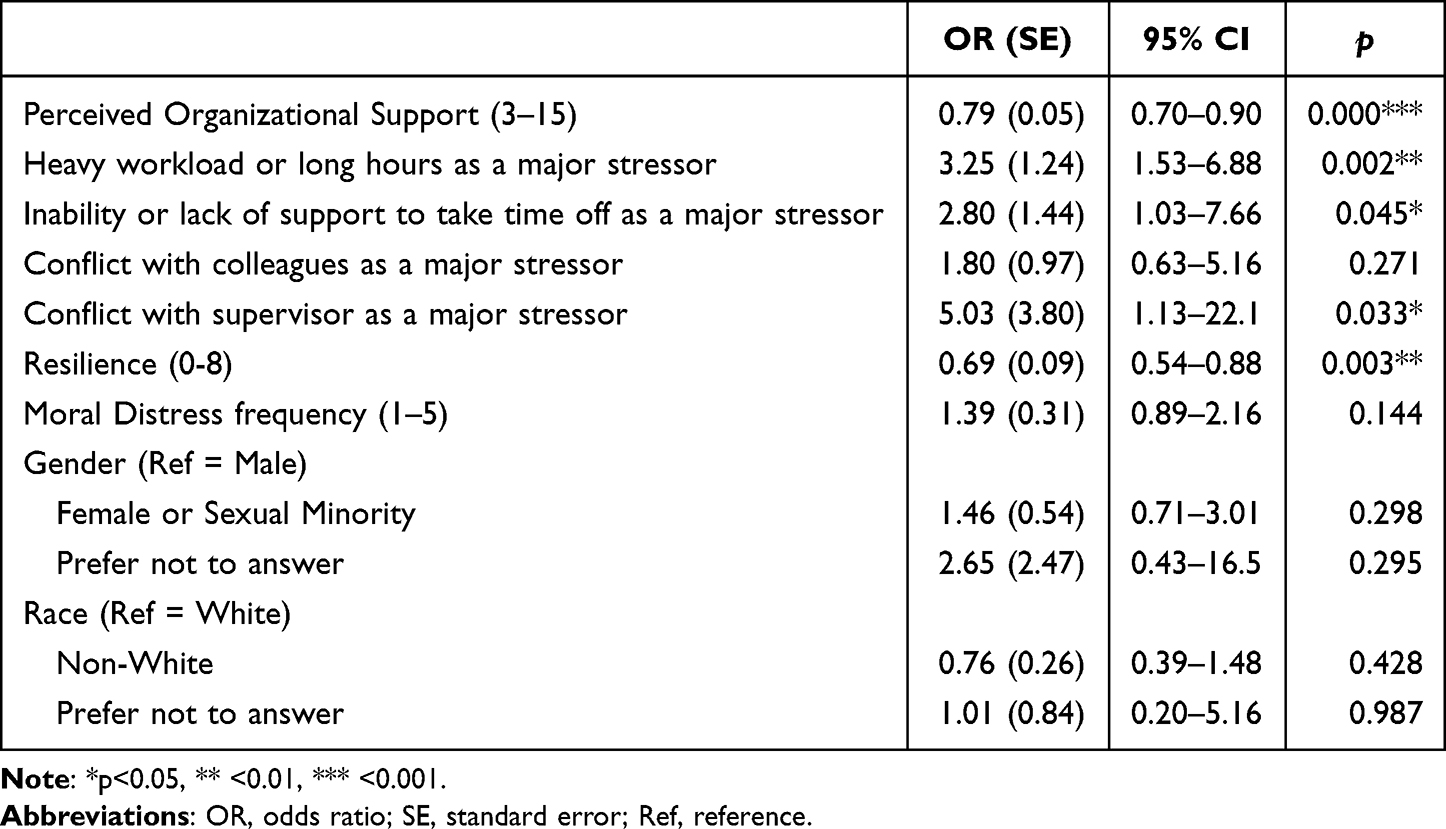 |
Table 2 Logistic Regression Analysis Predicting Odds of High Distress (WBI ≥ 2) for Non-Clinician Biomedical Researchers (n = 245) |
Table 3 presents the results from the dominance analysis. The factors with the greatest level of contribution to the overall variance in distress, ranked high to low, are depicted. Perceived organizational support (27.89%), heavy workload or long hours (18.39%), and conflict with supervisor (13.08%) contributed most to the variance in high distress, accounting for 59.4% of predicted variance, while inability or lack of support to take time off (12.86%) and resilience (9.97%) explained a lesser portion of the variance. Non-significant predictors in our model contributing to overall variance in distress included moral distress (11.11%), conflict with colleagues (3.54%), gender (2.92%), and race (0.24%), non-significant predictors of distress in our sample, accounted for less than 7% of predicted variance.
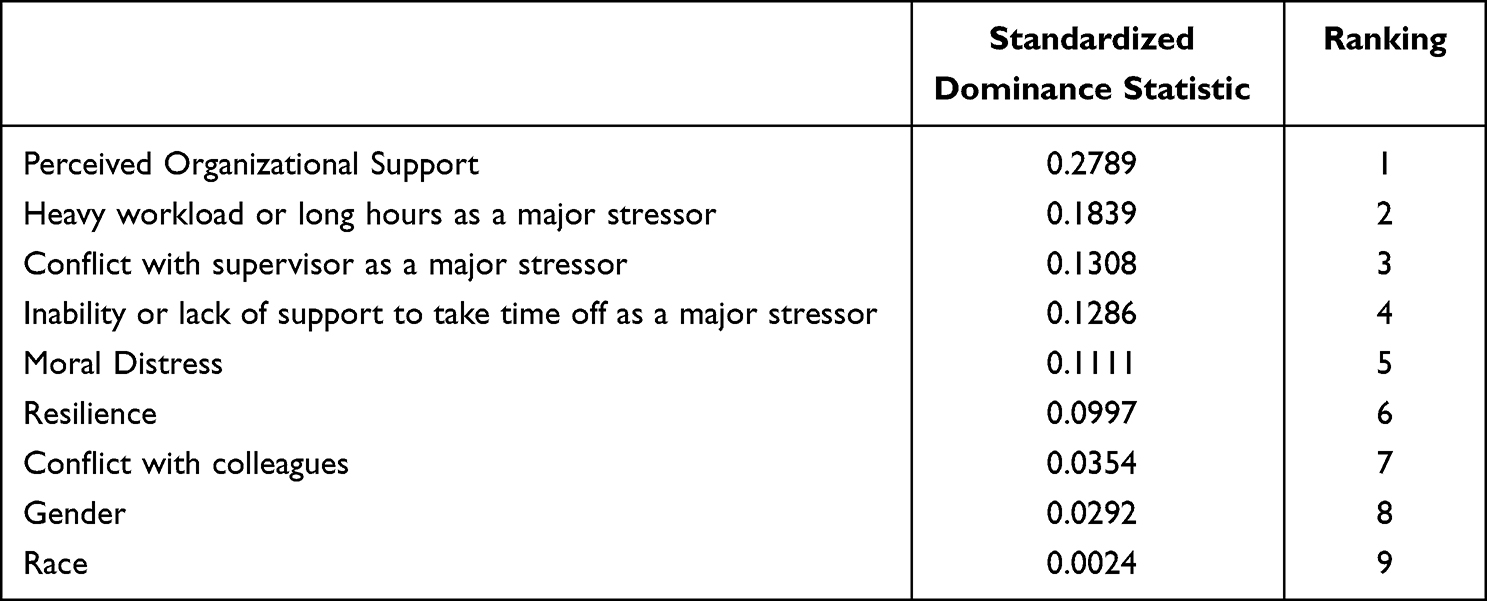 |
Table 3 Contribution of Predictors to Overall Variance in Distress in Non-Clinician Biomedical Researchers (WBI ≥ 2) (n = 245) |
Discussion
The purpose of this study was to evaluate the individual, team, and organizational level stressors of non-clinician biomedical scientists in a US academic medical center. This work extends our previous research that examined similar stressors for all members of the healthcare team.20 The prevalence of burnout between clinicians and biomedical scientists was recently investigated but concluded that biomedical scientist burnout could not be assessed or addressed in the same manner as those who work in clinical environments.2 Therefore, non-clinician biomedical researchers were exclusively investigated in this report. In the present analysis, we found that nearly 44% of non-clinician biomedical researchers reported high distress. Previous literature indicates that high WBI distress scores correlate with poor quality of life, burnout, and suicidality.31,33,38 To be fully understood, stressors that are correlated to distress were divided into those that are work-related and those that originate outside of work for the purposes of the discussion. Interestingly, likely due to the unique job role of the non-clinician biomedical researcher, the correlates of distress were distinct from previously analyzed healthcare workers.20 This elucidates an opportunity for the organization to implement tailored interventions that address correlates of distress in non-clinician biomedical researchers, separate to those that address the entire healthcare team.
Work-Related Factors
Multivariate analysis identified perceived organizational support as significantly associated with high distress after controlling for other factors. This important indicator also accounted for the greatest portion of the variance in distress in our sample. We found that individuals who have a higher sense of organizational support were less likely to be distressed, emphasizing the need to consider the unique needs and experiences of non-clinician researchers within the academic medical center setting. It is imperative that organizations consider the impact of biomedical research in the academic medical center, especially when approaching communication, inclusion in decision-making, and operational decisions. In fact, Girod et al cited that attrition of non-clinical faculty from academic medical centers was driven by lack of support, alongside not feeling valued or recognized in the work setting, lack of infrastructural support for scientific work, and lack of opportunity for advancement to leadership positions.39 Another study similarly reported that low institutional support was one of the main drivers of intent to leave academia.40 Importantly, perceived organizational support is positively correlated with employee well-being and includes support from leaders and the extent to which the organization values employee contribution.41,42
Heavy workload or long work hours as a major stressor accounted the second greatest portion of variance in distress and were significantly associated with this outcome. The perception of heavy workload and the obligation to work long hours have long existed in academic research. This perception is historically driven by the pressure to produce high impact research, acquire funding to support research, and require administrative and teaching duties. Another factor driving a culture that celebrates heavy workloads and long working hours is acquisition of a faculty position or tenure.16,18,19 One study showed that biomedical researchers, trained to design and conduct rigorous experiments, were only spending 30% of their time on research-related activities, with the remaining 70% of tasks revolving around supervision, administration, teaching, and funding.18 Of importance, the COVID-19 pandemic likely exacerbated the perceived requirement to shoulder a heavy workload and work long hours due to disruptions in supply chain, access to facilities and equipment, and research productivity. These factors in turn adversely affected the tenure clock, acquisition of faculty positions, and research funding.43,44
While there is pressure from society and organizations to practice self-care and work–life balance, the reality of a hypercompetitive work environment does not support such ideals.14,45,46 This may also influence the significant association of the inability or lack of support to take time off as a major stressor and distress, as researchers may not feel they are able to take time away from their workload due to a productivity-oriented culture. A recent survey indicated that nearly 60% of American workers did not take advantage of their time off47 and since 2020, the average workday nearly extended by an hour,48 despite evidence highlighting the benefits of time away from work.49,50 The specific reasons behind why nearly 15% of our sampled biomedical researchers cited inability to take time off as a major stressor remain to be explored.
Conflict with supervisor as a major stressor was also identified as a significant contributor to distress in biomedical researchers and accounted for the third greatest portion of variance in this outcome. We hypothesize that this stressor could originate from researcher interaction with administrative as well as research-oriented supervisors. Though studies that focus on inter-workplace conflict within biomedical research are scant, previous reports have acknowledged the contribution of conflict between researchers and administration to stress and low morale15 and negative effect on work culture.27 It has been suggested that there exists tension within academic centers, in which administration is prioritized over faculty. This was described by data that showed that though professorial growth had expanded by 51%, the number of administrators and staff had grown by 181%, creating the perception that organizational investment and priority was taken away from teaching and research.51,52 Studies also point to issues regarding perception of decision-making from leadership and lack of transparency and communication therein.27 Within the research work setting, extant evidence within the literature further suggests that power imbalances and top-down power dynamics exist and are associated with discrimination, harassment, bullying, and isolation, especially when considering those in more junior positions.27,28 In fact, it has been suggested that the “publish or perish” reality may in part drive these negative power imbalances throughout different roles within biomedical research, from trainees to senior faculty.53–55 Though conflict with supervisor was identified as a major correlate of distress within this dataset, more investigation is required to fully understand the precise nature of this major stressor within biomedical researchers in the academic medical center setting.
Nonwork-Related Factors
Our study identified a significant association between resiliency and distress in biomedical researchers, wherein researchers with low resiliency scores have higher odds of distress. While the two variables were significantly associated, resiliency accounted for less than 10% of the variance. This suggests that, while individual resiliency building practices are important, organizational factors are more prevalent drivers of distress in non-clinician researchers. While mental health is gaining traction in organizations as a priority for maintaining wellness in employees, the emphasis has mainly been on providing resources for employees to manage their own well-being by way of self-assessments, meditation, yoga, and training.56 Though being resilient is undeniably important in stressful work environments, recent articles note that the push for employees to refine resiliency skills disregards organizational issues that contribute to employee stress.57 Furthermore, these skills are shown to treat symptoms of distress and burnout instead of resolving the cause.58,59 In fact, employee burnout serves as a significant indicator that the organization requires systematic change.60 Individual-level solutions for employee health and satisfaction are less likely to be sustainable compared to those on an organizational level61 and result in costly consequences, such as resignation and employee attrition.62 Importantly, studies suggest that building resilience is not only an individual-level responsibility but also the responsibility of the organization.58,59,63,64
There has been success in the recruitment of underrepresented minorities into biomedical research training programs in recent years; however, these increased numbers are not reflected in the number of underrepresented minorities who hold faculty positions or NIH-funding.65–68 One explanation for this is increased workplace stress and burnout in this population of researchers.69,70 In our study, we did not identify any significant differences in gender or race as they relate to distress. While these findings do not necessarily suggest that no differences exist in the general population, it could be postulated that the organizational factors driving distress have significant impact on all individuals.
There are several limitations to note in this study. The cross-sectional nature of this study limits our ability to investigate cause-and-effect between the outcome and predictors. It also remains unclear whether individuals who are more or less distressed are more likely to participate in an optional survey on well-being. Of note, in our initial data exploration, we investigated the inclusion of physician-scientists within this analysis due to their participation in research as part of their job role. We determined that, due to their dual role in patient care and research, it was best to investigate biomedical researchers and physician scientists separately. Therefore, physician-scientists were excluded from this analysis and will be subjects of future studies. Specific job roles within the non-clinician biomedical researcher category, such as faculty or trainee, were not captured and we were also limited in our sample size, though robust estimators were utilized in our analysis. We postulate that a portion of this small sample size may be attributed to observed levels of perceived organizational support of non-clinician biomedical researchers within the academic medical center. Though some variables did not reach statistical significance, we must not discount their importance in creating sustainable work environments for non-clinician researchers. We also note the limitations associated with the surveyed population originating from a single institution, nonresponse bias, and their effects on the generalizability of the results. However, empirical studies of distress in biomedical researchers within single organizations should not be overlooked or discredited, as they provide important insights into correlates of distress and reduce the confounding variables when measuring across organizations such as macroenvironmental differences. Despite the listed limitations, these findings contribute to a large evidence-based knowledge gap in the drivers of distress in this vastly understudied population that exists within academic medical centers in the US.
Conclusion
The findings presented here indicate that nearly half of non-clinician biomedical researchers were in high distress at the time of survey, indicating an increased risk of suicidal ideation, turnover intention, and burnout. Failure to address organizational drivers of distress could also further weaken employee perceived organizational support, challenging the notion that the organization cares about employee well-being and satisfaction at work.
The major correlates of distress in this population were at the organizational level, including perceived organizational support, heavy workload, long hours, inability or lack of support to take time off, and conflict with supervisor. While lower individual resilience was associated with greater distress, it accounted for less than 10% of the overall variance when controlling for work-related factors. These findings demonstrate that greater emphasis should be placed on developing organizational interventions that address institutional support for non-clinician biomedical researchers within academic medical centers that take into consideration the nuances of the job role and unique dynamics that exist within this population. While emphasizing resiliency as an important factor for success in research, it is also the responsibility of the organization to create and foster an environment in which employees are able to access their own resilience.
Data Sharing Statement
De-identified data are available upon request.
Ethical Approval
This study received approval from the University of Alabama at Birmingham Institutional Review Board (300006629). This study was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki.
Acknowledgments
Authors would like to thank the non-clinician biomedical researchers who took the time to participate in this survey.
Author Contributions
All authors significantly contributed to the study design, acquisition of data, data analysis, article drafting, and article revision. All authors have agreed on the journal placement, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This study was funded by a grant from the ProAssurance Corporation to David A. Rogers. We also thank the NIH/NIGMS Institutional Research and Academic Career Development Award (K12 GM088010 to LMB).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Melnikow J, Padovani A, Miller M. Frontline physician burnout during the COVID-19 pandemic: national survey findings. BMC Health Serv Res. 2022;22(1):365. doi:10.1186/s12913-022-07728-6
2. Messias E, Flynn V. The tired, retired, and recovered physician: professional burnout versus major depressive disorder. Am J Psychiatry. 2018;175(8):716–719. doi:10.1176/appi.ajp.2018.17121325
3. Panagioti M, Geraghty K, Johnson J, et al. Association between physician burnout and patient safety, professionalism, and patient satisfaction: a systematic review and meta-analysis. JAMA Intern Med. 2018;178(10):1317–1331. doi:10.1001/jamainternmed.2018.3713
4. Amanullah S, Ramesh Shankar R. The impact of COVID-19 on physician burnout globally: a review. Healthcare. 2020;8(4):421. doi:10.3390/healthcare8040421
5. Garcia LC, Shanafelt TD, West CP, et al. Burnout, depression, career satisfaction, and work-life integration by physician race/ethnicity. JAMA Netw Open. 2020;3(8):e2012762–e2012762. doi:10.1001/jamanetworkopen.2020.12762
6. Tawfik DS, Profit J, Webber S, Shanafelt TD. Organizational factors affecting physician well-being. Curr Treat Options Pediatr. 2019;5(1):11–25. doi:10.1007/s40746-019-00147-6
7. Harry E, Sinsky C, Dyrbye LN, et al. Physician task load and the risk of burnout among US physicians in a national survey. Jt Comm J Qual Patient Saf. 2021;47(2):76–85. doi:10.1016/j.jcjq.2020.09.011
8. Lou SS, Liu H, Warner BC, Harford D, Lu C, Kannampallil T. Predicting physician burnout using clinical activity logs: model performance and lessons learned. J Biomed Inform. 2022;127:104015. doi:10.1016/j.jbi.2022.104015
9. Shanafelt TD, Boone S, Tan L, et al. Burnout and satisfaction with work-life balance among US physicians relative to the general us population. Arch Intern Med. 2012;172(18):1377–1385. doi:10.1001/archinternmed.2012.3199
10. Perumalswami CR, Griffith KA, Jones RD, Stewart A, Ubel PA, Jagsi R. Patterns of work-related burnout in physician-scientists receiving career development awards from the National Institutes of Health. JAMA Intern Med. 2020;180(1):150–153. doi:10.1001/jamainternmed.2019.4317
11. Rao RC, Dlouhy BJ, Capell BC, Akeju O. The endangered physician-scientist and COVID-19. Cell Rep Med. 2021;2(2):100190. doi:10.1016/j.xcrm.2021.100190
12. Feldman AM. The national institutes of health physician-scientist workforce working group report: a roadmap for preserving the physician-scientist. Clin Transl Sci. 2014;7(4):289–290. doi:10.1111/cts.12209
13. Alberts B, Kirschner MW, Tilghman S, Varmus H. Rescuing US biomedical research from its systemic flaws. Proc Natl Acad Sci. 2014;111(16):5773–5777. doi:10.1073/pnas.1404402111
14. Bleasdale B. Researchers pay the cost of research. Nat Mater. 2019;18(8):772. doi:10.1038/s41563-019-0443-z
15. Holleman WL, Cofta-Woerpel LM, Gritz ER. Stress and morale of academic biomedical scientists. Acad Med. 2015;90:5. doi:10.1097/ACM.0000000000000533
16. Riddiford N. A survey of working conditions within biomedical research in the United Kingdom. F1000Research. 2017;6:229. doi:10.12688/f1000research.11029.2
17. Sang K, Powell A, Finkel R, Richards J. ‘Being an academic is not a 9–5 job’: long working hours and the ‘ideal worker’in UK academia. Labour Ind. 2015;25(3):235–249. doi:10.1080/10301763.2015.1081723
18. Susi T, Shalvi S, Srinivas M. I’ll work on it over the weekend’: high workload and other pressures faced by early-career researchers. Nature. 2019;2019:197735355.
19. Woolston C. PhDs: the tortuous truth. Nature. 2019;575(7782):403–407. doi:10.1038/d41586-019-03459-7
20. Meese KA, Colón-López A, Singh JA, Burkholder GA, Rogers DA. Healthcare is a team sport: stress, resilience, and correlates of well-being among health system employees in a crisis. J Healthc Manag. 2021;66(4):304–322. doi:10.1097/JHM-D-20-00288
21. Rush University. Why pursue a career in biomedical research?; 2018. Available from: https://www.rushu.rush.edu/news/why-pursue-career-biomedical-research.
22. Bureau of Labor Statistics. Occupational outlook handbook, medical scientists; 2022. Available from: https://www.bls.gov/ooh/life-physical-and-social-science/medical-scientists.htm.
23. Penn Medicine. What it means to be an academic medical center. Available from: https://www.pennmedicine.org/about/benefits-of-an-academic-medical-center.
24. Lichten CA, Marsden G, Pollitt A, Kiparoglou V, Channon KM, Sussex J. Does a biomedical research centre affect patient care in local hospitals? Health Res Policy Syst. 2017;15(1):2. doi:10.1186/s12961-016-0163-7
25. Nabel EG. Linking biomedical research to health care. J Clin Invest. 2009;119(10):2858. doi:10.1172/jci41035
26. Hanney S, Boaz A, Soper B, Jones T. Engagement in research: an innovative three-stage review of the benefits for health-care performance. HSDR. 2013;1:8. doi:10.3310/hsdr01080
27. Moran H, Karlin L, Lauchlan E, et al. Understanding Research Culture: what researchers think about the culture they work in. Wellcome Open Res. 2020;5:201. doi:10.12688/wellcomeopenres.15832.1
28. Guthrie S, Lichten CA, Van Belle J, Ball S, Knack A, Hofman J. Understanding mental health in the research environment: a rapid evidence assessment. Rand Health Q. 2018;7:3.
29. Tapper T, Filippakou O. The world‐class league tables and the sustaining of international reputations in higher education. J High Educ Policy Manag. 2009;31(1):55–66. doi:10.1080/13600800802383091
30. Kumar V. The role of university research centers in promoting research. J Acad Mark Sci. 2017;45(4):453–458. doi:10.1007/s11747-016-0496-3
31. Dyrbye LN, Satele D, Shanafelt T. Ability of a 9-item well-being index to identify distress and stratify quality of life in US workers. J Occup Environ Med. 2016;58(8):810–817. doi:10.1097/jom.0000000000000798
32. Dyrbye LN, Shanafelt TD, Johnson PO, Johnson LA, Satele D, West CP. A cross-sectional study exploring the relationship between burnout, absenteeism, and job performance among American nurses. BMC Nurs. 2019;18(1):57. doi:10.1186/s12912-019-0382-7
33. Tawfik DS, Profit J, Morgenthaler TI, et al. Physician burnout, well-being, and work unit safety grades in relationship to reported medical errors. Mayo Clin Proc. 2018;93(11):1571–1580. doi:10.1016/j.mayocp.2018.05.014
34. Dyrbye LN, Satele D, Sloan J, Shanafelt TD. Utility of a brief screening tool to identify physicians in distress. J Gen Intern Med. 2013;28(3):421–427. doi:10.1007/s11606-012-2252-9
35. Eisenberger R, Huntington R, Hutchison S, Sowa D. Perceived organizational support. J Appl Psychol. 1986;71(3):500–507. doi:10.1037/0021-9010.71.3.500
36. National Center for Organization Development. VA All Employee Survey; 2018. Available from: https://www.va.gov/NCOD/VAworkforcesurveys.asp.
37. Vaishnavi S, Connor K, Davidson JR. An abbreviated version of the Connor-Davidson Resilience Scale (CD-RISC), the CD-RISC2: psychometric properties and applications in psychopharmacological trials. Psychiatry Res. 2007;152(2–3):293–297. doi:10.1016/j.psychres.2007.01.006
38. Hall LH, Johnson J, Watt I, Tsipa A, O’Connor DB. Healthcare Staff wellbeing, burnout, and patient safety: a systematic review. PLoS One. 2016;11(7):e0159015. doi:10.1371/journal.pone.0159015
39. Girod SC, Fassiotto M, Menorca R, Etzkowitz H, Wren SM. Reasons for faculty departures from an academic medical center: a survey and comparison across faculty lines. BMC Med Educ. 2017;17(1):8. doi:10.1186/s12909-016-0830-y
40. Pololi LH, Krupat E, Civian JT, Ash AS, Brennan RT. Why are a quarter of faculty considering leaving academic medicine? A study of their perceptions of institutional culture and intentions to leave at 26 representative U.S. medical schools. Acad Med. 2012;87(7):859–869. doi:10.1097/ACM.0b013e3182582b18
41. Eisenberger R, Rhoades Shanock L, Wen X. Perceived organizational support: why caring about employees counts. Annu Rev Organ Psychol Organ Behav. 2020;7(1):101–124. doi:10.1146/annurev-orgpsych-012119-044917
42. Panaccio A, Vandenberghe C. Perceived organizational support, organizational commitment and psychological well-being: a longitudinal study. J Vocat Behav. 2009;75(2):224–236. doi:10.1016/j.jvb.2009.06.002
43. Chan C, Oey NE, Tan E-K. Mental health of scientists in the time of COVID-19. Brain Behav Immun. 2020;88:956. doi:10.1016/j.bbi.2020.05.039
44. Lauer M. Continued impact of COVID-19 on biomedical research; 2020. https://nexus.od.nih.gov/all/2020/11/04/continued-impact-of-covid-19-on-biomedical-research/.
45. You D. Work-Life balance: can you actually make that happen? Front Pediatr. 2016;3:117. doi:10.3389/fped.2015.00117
46. Woolston C. Postdocs under pressure: ‘Can I even do this any more?’. Nature. 2020;587(7835):689–692. doi:10.1038/d41586-020-03235-y
47. Study: a record 768 million US vacation days went unused in’18, opportunity cost in the billions; 2019. Available from: https://www.ustravel.org/press/study-record-768-million-us-vacation-days-went-unused-18-opportunity-cost-billions.
48. DeFilippis E, Impink SM, Singell M, Polzer JT, Sadun R. Collaborating during coronavirus: the impact of COVID-19 on the nature of work; 2020.
49. Anchor S, Gielan M. The data-driven case for vacation; 2016. Available from: https://hbr.org/2016/07/the-data-driven-case-for-vacation?registration=success.
50. Hruska B, Pressman SD, Bendinskas K, Gump BB. Vacation frequency is associated with metabolic syndrome and symptoms. Psychol Health. 2020;35(1):1–15. doi:10.1080/08870446.2019.1628962
51. Connell R. The Good University: What Universities Actually Do and Why It’s Time for Radical Change. Bloomsbury Publishing; 2019.
52. Ginsberg B. The Fall of the Faculty: The Rise of the All-Administrative University and Why It Matters. Oxford University Press; 2011.
53. Khalifa AA. Losing young researchers in the authorship battle, under-reported casualties. Ethics Med Public Health. 2022;20:100735. doi:10.1016/j.jemep.2021.100735
54. Cortegiani A, Crimi C. No more bullying in medical research. Pulmonology. 2022. doi:10.1016/j.pulmoe.2022.03.007
55. Evans TM, Bira L, Gastelum JB, Weiss LT, Vanderford NL. Evidence for a mental health crisis in graduate education. Nat Biotechnol. 2018;36(3):282–284. doi:10.1038/nbt.4089
56. Lieberman C. What wellness programs don’t do for workers; 2019. Available from: https://hbr.org/2019/08/what-wellness-programs-dont-do-for-workers.
57. Fosslein L, Duffy M. Stop telling employees to be resilient; 2022. Available from: https://sloanreview.mit.edu/article/stop-telling-employees-to-be-resilient/.
58. Pieper C, Schröer S, Eilerts AL. Evidence of workplace interventions-a systematic review of systematic reviews. Int J Environ Res Public Health. 2019;16(19). doi:10.3390/ijerph16193553
59. Panagioti M, Panagopoulou E, Bower P, et al. Controlled interventions to reduce burnout in physicians: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(2):195–205. doi:10.1001/jamainternmed.2016.7674
60. McKinsey Health Institute. Addressing employee burnout: are you solving the right problem?; 2022. Available from: https://www.mckinsey.com/mhi/our-insights/addressing-employee-burnout-are-you-solving-The-right-problem.
61. Montano D, Hoven H, Siegrist J. Effects of organisational-level interventions at work on employees’ health: a systematic review. BMC Public Health. 2014;14(1):135. doi:10.1186/1471-2458-14-135
62. Sull D, Sull C, Cipolli W, Brighenti C. Why every leader needs to worry about toxic culture; 2022. Available from: https://sloanreview.mit.edu/article/why-every-leader-needs-to-worry-about-toxic-culture/.
63. Ovans A. What resilience means, and why it matters; 2015. Available from: https://hbr.org/2015/01/what-resilience-means-and-why-it-matters.
64. Cooper K. Resilience should not be a solitary pursuit; 2022. Available from: https://www.forbes.com/sites/katecooper/2022/05/27/resilience-should-not-be-a-solitary-pursuit/?sh=3912ec801f8b.
65. Gibbs KD
66. Valantine HA, Lund PK, Gammie AE. From the NIH: a systems approach to increasing the diversity of the biomedical research workforce. CBE Life Sci Educ. 2016;15(3):fe4. doi:10.1187/cbe.16-03-0138
67. Hoppe TA, Litovitz A, Willis KA, et al. Topic choice contributes to the lower rate of NIH awards to African-American/black scientists. Sci Adv. 2019;5(10):eaaw7238. doi:10.1126/sciadv.aaw7238
68. Taffe MA, Gilpin NW. Racial inequity in grant funding from the US National Institutes of Health. eLife. 2021;10:e65697. doi:10.7554/eLife.65697
69. Zambrana RE, Valdez RB, Pittman CT, Bartko T, Weber L, Parra‐Medina D. Workplace stress and discrimination effects on the physical and depressive symptoms of underrepresented minority faculty. Stress Health. 2021;37(1):175–185. doi:10.1002/smi.2983
70. Lawrence JA, Davis BA, Corbette T, Hill EV, Williams DR, Reede JY. Racial/ethnic differences in burnout: a systematic review. J Racial Ethn Health Disparities. 2022;9(1):257–269. doi:10.1007/s40615-020-00950-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.