")
Back to Journals » Journal of Inflammation Research » Volume 15
An inflammatory Signature of Glucose Impairment in Cystic Fibrosis
Authors Montemari AL , Manco M , Fiocchi AG, Bartoli M, Facchiano F, Tabolacci C, Scatigna M , Ciciriello F, Alghisi F, Montemitro E, Carsetti R, Lucidi V, Fiscarelli EV
Received 16 March 2022
Accepted for publication 9 August 2022
Published 10 October 2022 Volume 2022:15 Pages 5677—5685
DOI https://doi.org/10.2147/JIR.S365772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Adam D Bachstetter
Anna Lisa Montemari,1 Melania Manco,2 Alessandro Giovanni Fiocchi,3 Manuela Bartoli,4 Francesco Facchiano,5 Claudio Tabolacci,5 Maria Scatigna,6 Fabiana Ciciriello,3 Federico Alghisi,3 Enza Montemitro,3 Rita Carsetti,7 Vincenzina Lucidi,3 Ersilia Vita Fiscarelli1
1UOS Cystic Fibrosis Diagnostic, UOC Microbiology and Immunology Diagnostic, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy; 2Research Area for Multifactorial Diseases, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy; 3Cystic Fibrosis Unit, Department of Pediatrics Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy; 4Department of Ophthalmology, Medical College of Georgia, Augusta University, Augusta, GA, USA; 5Department of Oncology and Molecular Medicine, Istituto Superiore Di Sanità, Rome, Italy; 6Department of Life, Health and Environmental Sciences, University of L’Aquila, L’Aquila, Italy; 7Diagnostic Immunology Unit, Department of Laboratories, B Cell Pathophysiology Unit, Immunology Research Area, Bambino Gesù Children’s Hospital, IRCCS, Rome, Italy
Correspondence: Melania Manco, Bambino Gesù Children’s Hospital, IRCCS, piazza Sant’Onofrio 4, Rome, Italy, Tel +39 06 6859 2649, Fax +39 06 6859 2904, Email [email protected]
Objective and Design: Cystic fibrosis-related diabetes (CFRD) is a severe complication associated with increased morbidity and mortality in cystic fibrosis (CF) patients. Extensive inflammatory state in CF leads to pancreas damage and insulin resistance with consequent altered glucose tolerance and CFRD development. The aim of the present study was to identify circulating levels of inflammatory markers specifically associated with impaired glucose tolerance (IGT) and overt CFRD in a sample of young adults with CF.
Materials and Methods: Sixty-four CF outpatients, without evident active pulmonary exacerbation, infectious and autoimmune diseases, were enrolled in the study and the levels of 45 inflammatory serum mediators were measured through x magnetic bead panel multiplex technology.
Results: Serum levels of PDGF-AA, CCL20/MIP3α, IFNα, CCL11/eotaxin, CXCL1/GROα, GMCSF, B7H1/PDL1, IL13, IL7, VEGF, and TGFα were all significantly (p< 0.05) elevated in patients according to glycemic status and directly correlated with glycated hemoglobin and C-reactive protein levels.
Conclusion: Our findings suggest that increased levels of specific circulating inflammatory mediators are directly associated with impaired glucose tolerance in CF patients, thus, potentially implicating them in CFRD pathogenesis and warranting larger longitudinal studies to validate their monitoring as predictor of CFRD onset.
Keywords: cystic fibrosis-related diabetes, cytokines, growth factors, immune mediators, impaired glucose tolerance, inflammation
Introduction
Cystic fibrosis (CF) is a genetic disease affecting more than 30,000 people in the US and 48,000 in Europe, of which 5531 are in Italy.1 CF is caused by over 2000 different single mutations of the cystic fibrosis transmembrane conductance regulator (CFTR) gene,2 which results in disruption of normal ion transport across the epithelial cell surface and leads to sticky mucus accumulation in the respiratory, reproductive, and digestive tracts including the pancreas.3
Persistent inflammation in CF patients promotes tissue injury, thus significantly contributing to the diffuse organ damage and failure seen in these patients.4
Lungs and pancreas are among the most affected organs and deterioration of their function highly affects CF morbidity and mortality.4 In the pancreas, endocrine dysfunction may occur in parallel with exocrine insufficiency (pancreatic insufficiency, PI) leading to cystic fibrosis-related diabetes (CFRD), a unique form of diabetes, associated with worse clinical outcomes including faster deterioration of lung function evidenced by a decline of the FEV1% (forced expiratory volume in the first second).5
CFRD incidence increases with age. About 20% of adolescents present with overt diabetes and, by their forties, about half of the patients having PI will develop CFRD.5 Interestingly, 10–15% of the CF patients maintain preserved exocrine pancreatic function (pancreatic sufficiency, PS) and most likely will not develop CFRD. Early diagnosis and treatment of diabetes improves overall prognosis and an annual screening with an oral glucose tolerance test (OGTT) is recommended starting at least by the age of 10.
The occurrence of PI and CFRD has been attributed to diverse causes including fibrosis and fatty infiltration in the pancreatic tissue followed by “beta cells strangulation”.6 However, morphological study of pancreatic tissues from neonates, infants and very young children with CF found that in children with CF under four years of age, the relative beta-cell areas and percentage of beta cells were reduced to about 50% of controls, but this reduction was not associated with the severity of exocrine damage and fibrosis. Proliferating insulin-positive cells were scarce or absent in young CF pancreata whose islets were infiltrated with dispersed inflammatory cells suggesting smaller-sized beta-cell population present at birth and impaired beta-cell growth in CF children.7 The more recent work by Hart et al8 confirmed that PI and CFRD are characterized by beta cell loss and intra-islet inflammation in the setting of a complex pleiotropic disease and not by any intrinsic islet dysfunction from CFTR mutation. However, the incidence of diabetes and its severity does not even correlate with the residual beta cells. Glucose tolerance balance fails over time and patients may move in and out through stages of indeterminate glycemia, impaired glucose tolerance (IGT) and CFRD. The occurrence of pulmonary infections and the use of glucocorticoid therapy can also contribute to precipitate the IGT trend toward diabetes.5
Sterile inflammation in combination with recurrent infections contributes to loss of insulin production through beta-cell destruction, also by altering insulin sensitivity, making CFRD a unique form of diabetes.9 While there is a clear association between pathogen-induced and sterile inflammation with IGT and development of CFRD, little is known on the inflammatory mediators directly involved in this process and whether their levels could be associated with the progression of glucose intolerance and diabetes onset in CF patients.
Here, we have performed a high throughput screening assessing circulating levels of different inflammatory mediators (cytokines, chemokines and growth factors) in a sample of CF young adults to investigate whether their expression profiles correlated with IGT and CFRD.
Materials and Methods
CF Patients
Sixty-four CF outpatients were enrolled at the CF Center of the Bambino Gesù Children’s Hospital of Rome, Italy, from July to September 2019. The CF center evaluates patients along childhood-adulthood transition for all disease comorbidities, including diabetes. The study was performed in accordance with the revised Declaration of Helsinki of 2000 and with the ethical standards of the Bambino Gesù Children’s Hospital Review Board that approved the study (approval no. 201802P004364). All the participants provided a written informed consent.
CF diagnosis was based on two positive sweat tests (≥60 mmol/L) and/or genotyping. Pancreatic functionality was established on clinical observations (ie the presence of steatorrhea and malabsorption), clinical tests (determination of fecal elastase-1 and chymotrypsin and/or lipase) and pancreatic enzyme replacement treatment.
Inclusion criteria were age older than 18 and absence of evident active pulmonary exacerbations. Exclusion criteria were occurrence of infection (ie human Immunodeficiency Virus, Viral Hepatitis) and autoimmune diseases.
As routine investigation, patients underwent a standard OGTT for the diagnosis of IGT and diabetes; induced sputum or deep oropharyngeal swab to detect microbial infections and colonization and blood collection; spirometry with forced expiratory volume in the first second (FEV1%) quantification. In addition to routine exams, fasting sera from study participants were collected and stored at −20°C in Eppendorf tubes until analysis. Patient’s history, genotype and follow-up data, including biochemistry and microbiology were retrieved from the electronic health records.
CFRD was diagnosed as 2 h blood glucose at T120′ of OGTT >200 mg/dL (>11.1 mmol/L), fasting blood glucose >126 mg/dL (>7 mmol/L) on two or more occasions, glycated hemoglobin (HbA1c) ≥48 mmol/mol; indeterminate hyperglicemia as random blood glucose >200 mg/dL on two or more occasions with symptoms; and IGT as 2 h blood glucose at T120′ of OGTT >140 and <199 mg/dL during periods of stable health conditions.
Patients were grouped as follows: pancreatic sufficient patients with normal glucose tolerance (PS-NGT), exocrine pancreatic insufficient patients with normal glucose tolerance (PI-NGT) and exocrine pancreatic insufficient CF patients with impaired glucose tolerance or diabetes (PI-IGT/CFRD).
No patient had exocrine sufficiency and IGT/CFRD in our sample, being these patients very rare in the CF population.
Luminex Assay
The levels of 45 mediators involved in inflammation and immune response (listed in Table S1) were measured through xMAP multiplex technology by a customized human magnetic luminex assay, (#FCSTM18-45, R&D Systems, Minneapolis, MN, USA). The analysis was carried out according to the manufacturer’s instructions and quantification performed with a Bio-Plex® 200 System (Bio-Rad Laboratories, Hercules, CA, USA) equipped with magnetic workstation and Bio-Plex Manager Software version 6.1. All samples were run in duplicate (average % CV <10% for all analytes).
Statistical Analysis
Data are expressed as mean and standard deviation or number and percentage, unless differently stated. Comparisons among groups was done by ANOVA. Log mean was adopted to stabilize the variance. A nonparametric Dunn test was applied and the obtained p-values adjusted using the Benjamini–Hochberg false discovery rate (FDR) method. The F-tests were significant when p<0.05. Spearman rank correlation was used to investigate relationships among HbA1c as estimate of average glucose control, CRP as estimate of systemic inflammation, c-peptide as index of residual beta cell function, FEV1 and the investigated serum mediators that resulted differently expressed among groups. Then, stepwise forward and backward regression models were run to identify molecules predicting values of HbA1c, CRP, c-peptide and FEV1 values; ordinal regression model to identify predictors of PS and PI phenotypes; an exploratory factor analysis (with principal components approach) to identify inflammatory patterns associated with the abovementioned outcomes. Age, sex, BMI, use of drug were covariates in the analyses.
Analyses were performed with Stata IC/15.1 (StataCorp LLC, College Station, TX, USA). A p-value <0.05 was considered statistically significant.
Results
Study Sample
Out of the 64 CF patients enrolled in the study, four were excluded: (Supplementary Figure 1; one patient with type 1 diabetes (T1D), one patient with a paresthesia of unidentified nature, one with leukocytosis and one with mononucleosis).
The final sample population included 60 patients, (40 females, 66.7%). Median age was 27.9±8.3 years. We stratified patients in three subgroups, according to pancreatic functionality and glycemic status as it follows: pancreatic sufficient patients with normoglycemia (PS-NGT, N=10), pancreatic insufficient patients with normoglycaemia (PI-NGT, N=26) and pancreatic insufficient patients with glucose impairment or overt diabetes (PI-IGT/CFRD, N=24). One patient had isolated IFG and two patients has indeterminate glycemia, all three were included in the PI-IGT/CFRD group. In this latter group, three patients presented with IGT and 18 had CFRD (Supplementary Figure 1). All the patients were Caucasian.
Table 1 summarizes patients’ anthropometric and metabolic characteristics. There were no significant differences in body weight, height and BMI among groups. The CF genotype distribution displayed the absence of the homozygosis for the F508del in the PS-NGT group and the highest percentage of patients carrying the allele F508del (either homozygosis or heterozygosis) in the PI-IGT/CFRD group. In Table S2 the genotype of each patient is reported.
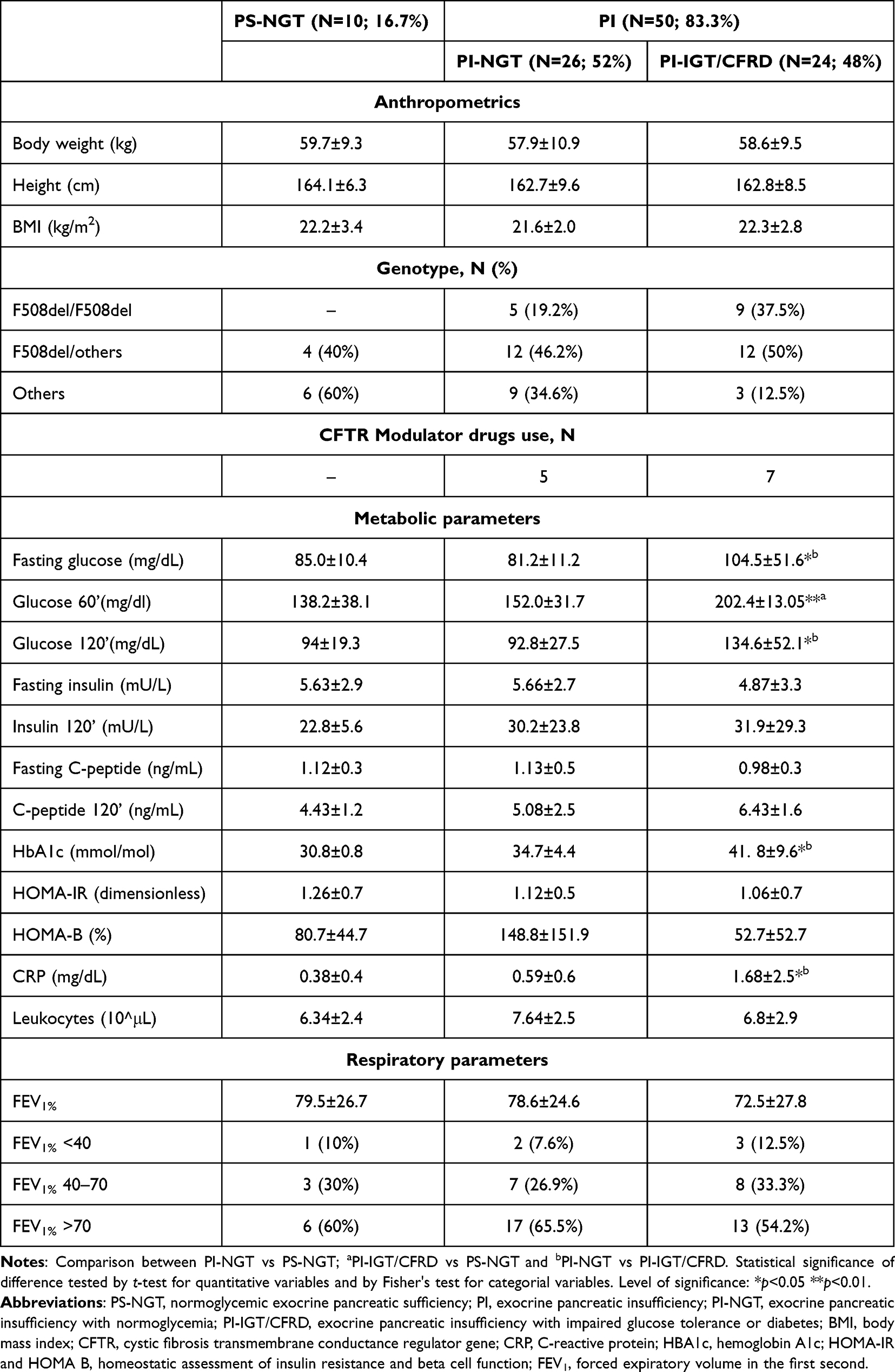 |
Table 1 Demographic and Metabolic Characteristics of the CF Patients Recruited in the Study |
None of the patients of the PS-NGT group were using modulator drugs while five patients in the PI-NGT group and seven in the PI-IGT/CFRD group were following a medical treatment with modulator drugs (Table 1). As expected, glucose parameters were significantly different among groups with the PI-IGT/CFRD group displaying higher levels of glycemia at the different OGTT time-points and HbA1c. This group showed the highest value of CRP (p<0.05).
In contrast no difference was found in leukocytes count among the three groups. Finally, lowest mean FEV1% was found in the PI-IGT/CFRD group that also comprised the highest percentage of patients displaying severe pulmonary insufficiency as defined by a FEV1% <40. The majority of the patients showing preserved lung function (FEV1% >70%) were found in the PS-NGT and PI-NGT groups.
Luminex Assay Data Analysis and IGT/CFRD at Baseline
Serum levels of 45 molecules involved in inflammation and immune responses have been assessed using a customized human magnetic luminex assay. The list of the factors included in the assay and mean, minimum, and maximum values for each analyte (cytokines, chemokines, interferons and growth factors) in the three groups are reported in Tables S3–S5. Serum levels of IL17A, IFNβ and basic FGF (FGFb) were undetectable in most of the patients whereas IL17A/IL25 and IL33 were undetectable only in the PS-NGT patients, therefore, these molecules were excluded from the analysis.
Table 2 reports molecules whose geometric means were significantly different among the three groups.
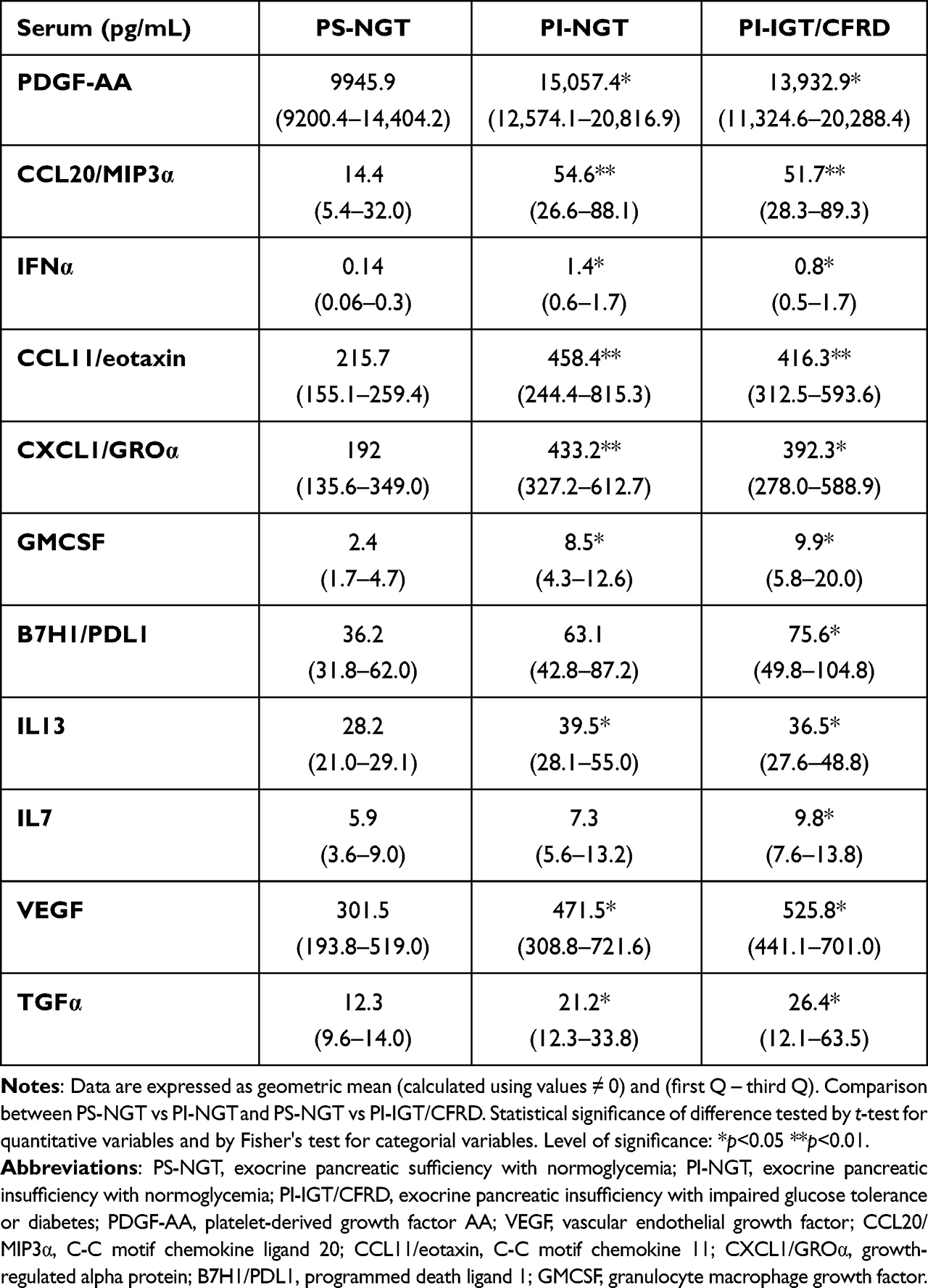 |
Table 2 Molecules Whose Mean Values Were Significantly Different in the Three Groups |
Table 3 reports correlation analysis among HbA1c as an estimate of glucose homeostasis, CRP as a marker of systemic inflammation, and C-peptide as an estimate of residual beta cell mass, FEV1 and the investigated serum mediators.
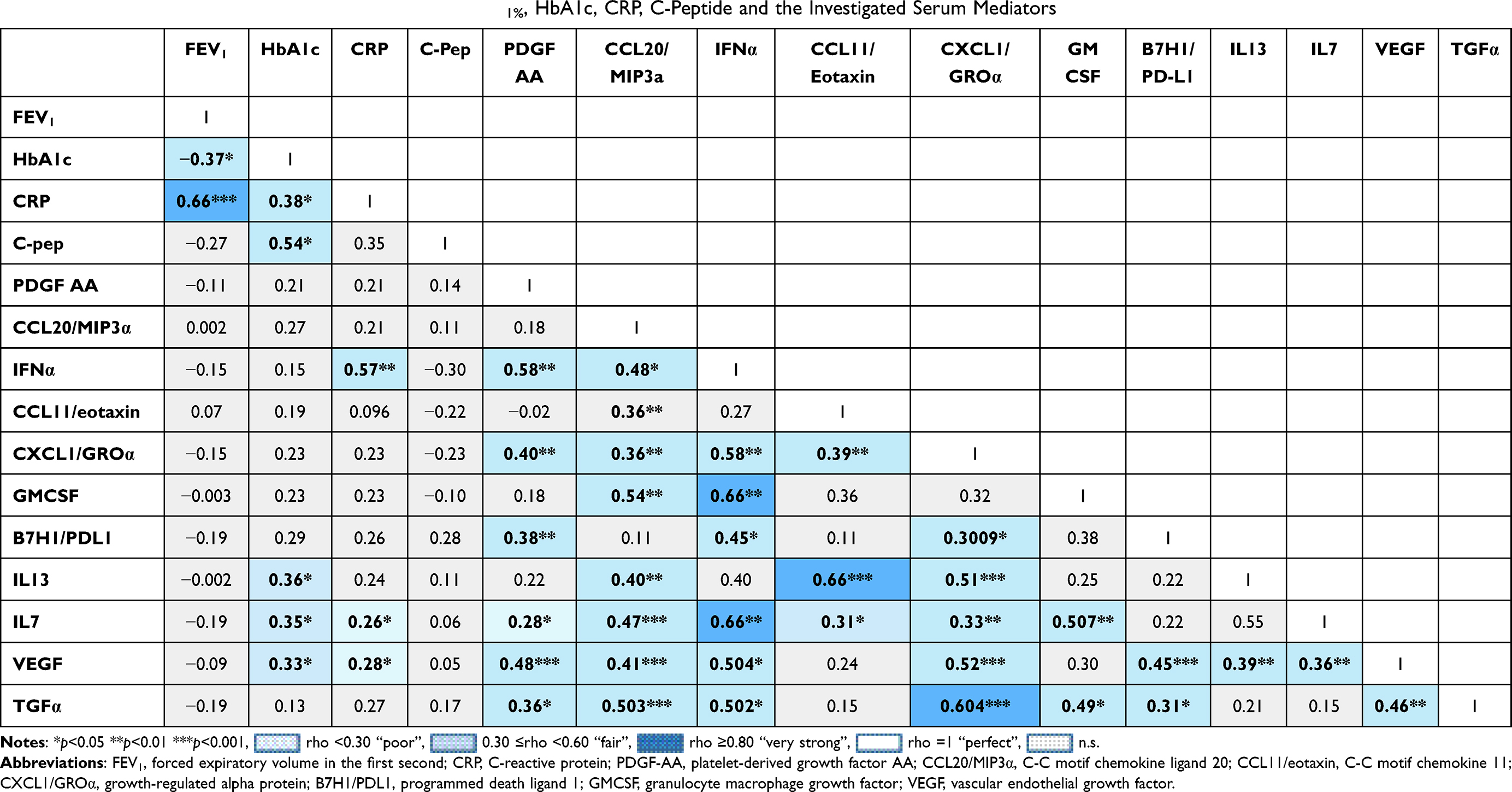 |
Table 3 Correlation Analysis (Spearman's Rho) Among FEV1%, HbA1c, CRP, C-Peptide and the Investigated Serum Mediators |
Regression analyses did not find any molecule from Tables 2 and 3 predicting phenotypes of PS, PI and IGT/CFRD as an ordinal outcome and HBA1c, C-peptide, PCR and FEV1 values as continuous outcomes.
Discussion
Glucose intolerance and overt diabetes in CF patients are clinically significant conditions associated with functional decline and increased mortality.10 Despite strict monitoring (OGTT testing) required by age 10, progression to overt diabetes in CF patients is still not well predictable or defined. As inflammation, both sterile and pathogen-related, has been identified as a major player in CFRD onset and progression,11,12 a correlation of inflammatory mediators with different levels of glucose tolerance could provide new diagnostic tools and open the path to innovative immunomodulatory therapeutic interventions. The results of our high throughput study identified 11 molecules of which serum levels were significantly augmented in the PI-IGT/CFRD group compared to those with normal endocrine and exocrine pancreatic function (PS-NGT) (Table 2).
These upregulated factors included: CXCL1/GROα, VEGF, CCL11/eotaxin, PDGF/AA, IFNα, CCL20/MIP3α, and B7H1/PDL1, IL7, IL13, TGFα and GMCSF. The PI-IGT/CFRD group displayed higher CRP values that directly correlated with poor metabolic glucose control (HbA1c) and reduced pulmonary function. Increased VEGF, IL7, IL13 expression levels were correlated with HBA1c (Table 3).
CXCL1/GROα is a chemokine known to play a key role in recruitment and activation of neutrophils. In addition, this chemokine is involved in vascular complications and inflammation of pancreatic islets in T2D13,14 and in airways inflammation in non-CF subjects.15 VEGF is known for its ability to promote migration and proliferation of endothelial cells, monocytes/macrophages chemotaxis and vasodilatation through the release of nitric oxide.16 However, increased VEGF levels have been reported in patients affected by prediabetes and T2D17 and are involved in the pathogenesis of diabetic microvascular complications.18 Most importantly, VEGF is also pivotal for lung maturation and surfactant production19 and its levels are increased in pulmonary diseases.20 As to PDL1, a B7 family co-stimulatory protein expressed on antigen presenting cells, its engagement within its receptor inhibits T cell proliferation, induces apoptosis and promotes differentiation of CD4+ T cells into Foxp3+ regulatory T cells. PD1/PDL1 system is a critical immune checkpoint21 that plays a pivotal role in the pathogenesis of type 1 diabetes. In the attempt at counteracting the host immune response, the beta cells of patients with T1D overexpress the molecule on their surface.22 However, elevated concentrations of PD-1 have been also implicated in the pathogenesis and progression of IPF.23 While GROα and VEGF might be involved in pancreatic damage, PDL1 elevation is likely to have a counter-regulatory role and could represent a protective marker.
Increased levels of VEGF, GROα and PDL1, in the PI-IGT/CFRD group are likely associated with the pro-fibrotic lung environment. The fibrocystic lung represents a peculiar microenvironment characterized by severe oxygen depletion. Hypoxia/inflammation could promote activation of transcription factors, such as the signal transducers and activator of transcription 3 (STAT3) that is a known transcriptional inducer of VEGF, GROα and PDL1.24–26 Interestingly, we also found higher levels of IL7, a mediator supporting the proliferation of multiple immune cells and activating a signaling cascade, which also includes the JAK-STAT pathway, further enhancing the signaling mechanisms involved in pulmonary and endocrine pancreas inflammation and impairment.
CCL11/eotaxin, CCL20/MIP3α, PDGF-AA, IFNα were also upregulated in CF patients with altered glucose metabolism and are likely to mediate both lung and pancreas damage owing to their pro-fibrogenic/pro-angiogenic activity and ability to trigger the immune system as found in various lung fibrotic diseases and diabetes conditions (i.e CCL11/eotaxin).27–30
Our every attempt at identifying patterns of molecules predicting phenotypes of interest that considered clinical features such as age, comorbidities, exacerbation rates has failed. An explanation for this might be the small sample size. Supplemental Figure 2 resumes signaling mechanisms potentially involved in pulmonary and endocrine pancreas inflammation and impairment.
Indeed, we are aware of caveats of our study including the sample size that, however, is reasonably large when considering that CF is a rare condition and with different sex severity among groups;31 and the cross-sectional design that does not allow us to draw any causative relationship between inflammatory phenotypes and occurrence of 2conclusion, our high throughput analysis has revealed the existence of a potential signature of inflammation associated with altered glucose homeostasis in CF. Whether these markers can be diagnostic/prognostic of the CFRD risk, hence complementing the OGTT screening, must be further investigated in longitudinal studies of larger cohort. Currently, glucose testing remains an easy, fast, and inexpensive method to track occurrence of altered glucose homeostasis, but patients may fluctuate for a long time between normal and altered glucose metabolism before a diagnosis of IGT or CFRD is made. Identification of early biomarkers of CFRD development in an already compromised patient population might be informative to establish early therapies that, targeting definite inflammatory paths, ie the PD-1/PD-L1, reduce the burden of CFRD-related complications, including more rapid lung deterioration and increased mortality, with a more personalized medicine approach.
Abbreviations
B7H1/PDL1, programmed death ligand 1; CCL2/MCP1, C-C motif chemokine ligand 2; CCL3/MIP1α, macrophage inflammatory protein 1 alpha; CCL4/MIP1b, macrophage inflammatory protein 1-beta; CCL5/RANTES, C-C motif chemokine ligand 5; CCL11/eotaxin, C-C motif chemokine 11; CCL19/MIP3b, macrophage inflammatory protein 3 beta; CCL20/MIP3α, C-C motif chemokine ligand 20; CD40L, CD40 ligand; CFRD, cystic fibrosis-related diabetes; CFTR, cystic fibrosis transmembrane conductance regulator gene; CRP, C-reactive protein; CXCL1/GROα, growth-regulated alpha protein; CXCL2/GROβ, C-X-C motif chemokine ligand 2; CXCL10/IP10, C-X-C motif chemokine ligand 10; CX3CL1/fractalkine, C-X3-C motif chemokine ligand 1; FEV1, forced expiratory volume in the first second; FGF basic, fibroblast growth factor basic; Flt3 L, fms-related tyrosine kinase 3 ligand; GCSF, granulocyte colony stimulating factor; GMCSF, granulocyte macrophage growth factor; IGT, impaired glucose tolerance; Il1ra/IL1F3, interleukin 1 receptor antagonist; PDGF-AA, platelet-derived growth factor AA; PDGF-BB, platelet-derived growth factor BB; PI, exocrine pancreatic insufficiency; PI-IGT/CFRD, exocrine pancreatic insufficiency with impaired glucose tolerance or diabetes; PI-NGT, exocrine pancreatic insufficiency with normoglycemia; PS-NGT, normoglycemic exocrine pancreatic sufficiency; STAT3, signal transducers and activators of transcription 3; TRAIL, TNF-related apoptosis-inducing ligand; VEGF, vascular endothelial growth factor.
Data Sharing Statement
Clinical data are available from the last author upon reasonable request in accordance with the General Data Protection Regulation (EU) 2016/679.
Acknowledgments
We are grateful to Dr Cinzia Leuter, Medicine and Surgery, Campus Bio-Medico, University of Rome, Italy for her advice. Claudio Tabolacci was supported by Fondazione Umberto Veronesi that is gratefully acknowledged. The technological support from the “Complex Protein Mixture (CPM) Analysis” Facility at the Dept. OMM, Istituto Superiore di Sanità, is kindly acknowledged. The authors acknowledge the patients for their enthusiastic participation and dedicate this work to Barbara Bartoli and all deceased patients of our CF center.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded through RC 201802P004364.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cystic Fibrosis Foundation. Cystic fibrosis foundation patient registry, 2019 annual data report and ECFSPR annual report; 2018.
2. Kotnala S, Dhasmana A, Kashyap VK, Chauhan SC, Yallapu MM, Jaggi M. A bird eye view on cystic fibrosis: an underestimated multifaceted chronic disorder. Life Sci. 2021;268:118959. doi:10.1016/j.lfs.2020.118959
3. Morrison CB, Markovetz MR, Ehre C. Mucus, mucins, and cystic fibrosis. Pediatr Pulmonol. 2021;54(S3). doi:10.1002/ppul.24530
4. Turcios NL. Cystic fibrosis lung disease: an overview. Respir Care. 2020;65(2):233–251. doi:10.4187/respcare.06697
5. Moran A, Pillay K, Becker D, Granados A, Hameed S, Acerini CL. ISPAD clinical practice consensus guidelines 2018: management of cystic fibrosis-related diabetes in children and adolescents. Pediatr Diabetes. 2018;19:64–74. doi:10.1111/pedi.12732
6. Davis PB. Cystic Fibrosis. Pediatr Rev. 2001;22(8):257–264. doi:10.1542/pir.22-8-257
7. Bogdani M, Blackman SM, Ridaura C, Bellocq J-P, Powers AC, Aguilar-Bryan L. Structural abnormalities in islets from very young children with cystic fibrosis may contribute to cystic fibrosis-related diabetes. Sci Rep. 2017;7(1):17231. doi:10.1038/s41598-017-17404-z
8. Hart NJ, Aramandla R, Poffenberger G, et al. Cystic fibrosis-related diabetes is caused by islet loss and inflammation. JCI Insight. 2018;3(8):e98240. doi:10.1172/jci.insight.98240
9. Kelsey R, Manderson Koivula FN, McClenaghan NH, Kelly C. Cystic fibrosis–related diabetes: pathophysiology and therapeutic challenges. Clin Med Insights Endocrinol Diabetes. 2019;12:117955141985177. doi:10.1177/1179551419851770
10. Doan LV, Madison LD. Cystic Fibrosis Related Diabetes. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
11. Chen GY, Nuñez G. Sterile inflammation: sensing and reacting to damage. Nat Rev Immunol. 2010;10(12):826–837. doi:10.1038/nri2873
12. Hunt WR, Hansen JM, Stecenko AA. Glucose ingestion in cystic fibrosis induces severe redox imbalance: a potential role in diabetes. J Cyst Fibros. 2020;19(3):476–482. doi:10.1016/j.jcf.2020.02.010
13. Sajadi S, Khoramdelazad H, Hassanshahi G, et al. Plasma Levels of CXCL1 (GRO-α) and CXCL10 (IP-10) are elevated in type 2 diabetic patients: evidence for the involvement of inflammation and angiogenesis/angiostasis in this disease state. Clin Lab. 2013;59. doi:10.7754/Clin.Lab.2012.120225
14. Omatsu T, Cepinskas G, Clarson C, et al. CXCL1/CXCL8 (GROα/IL-8) in human diabetic ketoacidosis plasma facilitates leukocyte recruitment to cerebrovascular endothelium in vitro. Am J Physiol. 2014;306(9):E1077–84. doi:10.1152/ajpendo.00659.2013
15. Meyer N, Nuss SJ, Siebenhüner A, Akdis CA, Menz G, Rothe T. Differential serum protein markers and the clinical severity of asthma. JAA. 2014;67. doi:10.2147/JAA.S53920
16. Wheeler KC, Jena MK, Pradhan BS, et al. VEGF may contribute to macrophage recruitment and M2 polarization in the decidua. PLoS One. 2018;13(1):e0191040. doi:10.1371/journal.pone.0191040
17. Sun X, Zhang H, Liu J, Wang G. Serum vascular endothelial growth factor level is elevated in patients with impaired glucose tolerance and type 2 diabetes mellitus. J Int Med Res. 2019;47(11):5584–5592. doi:10.1177/0300060519872033
18. Lamoke F, Labazi M, Montemari A, Parisi G, Varano M, Bartoli M. Trans-Chalcone prevents VEGF expression and retinal neovascularization in the ischemic retina. Exp Eye Res. 2011;93(4):350–354. doi:10.1016/j.exer.2011.02.007
19. Compernolle V, Brusselmans K, Acker T, et al. Loss of HIF-2α and inhibition of VEGF impair fetal lung maturation, whereas treatment with VEGF prevents fatal respiratory distress in premature mice. Nat Med. 2002;8(7):702–710. doi:10.1038/nm721
20. Al-Husseini A, Kraskauskas D, Mezzaroma E, et al. Vascular endothelial growth factor receptor 3 signaling contributes to angioobliterative pulmonary hypertension. Pulm Circ. 2015;5(1):101–116. doi:10.1086/679704
21. Akturk HK, Kahramangil D, Sarwal A, Hoffecker L, Murad MH, Michels AW. Immune checkpoint inhibitor‐induced Type 1 diabetes: a systematic review and meta‐analysis. Diabet Med. 2019;36(9):1075–1081. doi:10.1111/dme.14050
22. Colli ML, Hill JLE, Marroquí L, et al. PDL1 is expressed in the islets of people with type 1 diabetes and is up-regulated by interferons-α and-γ via IRF1 induction. EBioMedicine. 2018;36:367–375. doi:10.1016/j.ebiom.2018.09.040
23. Geng Y, Liu X, Liang J, et al. PD-L1 on invasive fibroblasts drives fibrosis in a humanized model of idiopathic pulmonary fibrosis. JCI Insight. 2019. doi:10.1172/jci.insight.125326
24. Yuan S, Zhang S, Zhuang Y, Zhang H, Bai J, Hou Q. Interleukin-17 stimulates STAT3-mediated endothelial cell activation for neutrophil recruitment. Cell Physiol Biochem. 2015;36(6):2340–2356. doi:10.1159/000430197
25. Song TL, Nairismägi M-L, Laurensia Y, et al. Oncogenic activation of the STAT3 pathway drives PD-L1 expression in natural killer/T-cell lymphoma. Blood. 2018;132(11):1146–1158. doi:10.1182/blood-2018-01-829424
26. Hwang S, Seong H, Ryu J, et al. Phosphorylation of STAT3 and ERBB2 mediates hypoxia‑induced VEGF release in ARPE‑19 cells. Mol Med Rep. 2020. doi:10.3892/mmr.2020.11344
27. Kohan M, Puxeddu I, Reich R, Levi-Schaffer F, Berkman N. Eotaxin-2/CCL24 and eotaxin-3/CCL26 exert differential profibrogenic effects on human lung fibroblasts. Ann Allergy Asthma Immunol. 2010;104(1):66–72. doi:10.1016/j.anai.2009.11.003
28. Van Dyke AL, Lang Kuhs KA, Shiels MS, et al. Associations between self-reported diabetes and 78 circulating markers of inflammation, immunity, and metabolism among adults in the United States. PLoS One. 2017;12(7):e0182359. doi:10.1371/journal.pone.0182359
29. Coomans de Brachène A, Dos Santos RS, Marroqui L, et al. IFN-α induces a preferential long-lasting expression of MHC class I in human pancreatic beta cells. Diabetologia. 2018;61(3):636–640. doi:10.1007/s00125-017-4536-4
30. Shan Z, Xu C, Wang W, Li W. Enhanced PDGF signaling in gestational diabetes mellitus is involved in pancreatic β-cell dysfunction. Biochem Biophys Res Commun. 2019;516(2):402–407. doi:10.1016/j.bbrc.2019.06.048
31. Lam GY, Goodwin J, Wilcox PG, Quon BS. Sex disparities in cystic fibrosis: review on the effect of female sex hormones on lung pathophysiology and outcomes. ERJ Open Res. 2021;7(1):00475–2020. doi:10.1183/23120541.00475-2020
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.