")
Back to Journals » Journal of Pain Research » Volume 13
An Experimental Analogue Study on the “Dose-Response Relationship” of Different Therapeutic Instructions for Pain Exposures: The More, The Better?
Authors Körfer K, Schemer L, Kube T, Glombiewski JA
Received 3 June 2020
Accepted for publication 20 August 2020
Published 1 December 2020 Volume 2020:13 Pages 3181—3193
DOI https://doi.org/10.2147/JPR.S265709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Karoline Körfer,1 Lea Schemer,2 Tobias Kube,2 Julia A Glombiewski2
1Department of Clinical Psychology and Psychotherapy, Philipps-University Marburg, Marburg, Germany; 2Department of Clinical Psychology and Psychotherapy, University of Koblenz – Landau, Landau, Germany
Correspondence: Karoline Körfer
Department of Clinical Psychology and Psychotherapy, Philipps-University Marburg, Marburg, Germany
Email [email protected]
Objective: Novel suggestions derived from the inhibitory learning model on how to optimize exposure therapy have been debated with enthusiasm in the last few years, particularly with respect to the focus on expectancy violations. However, little is known about how this new approach directly compares to the traditional habituation rationale of exposure therapy. In the present study, we examined these two competing therapeutic instructions among healthy female participants in an experimental heat pain paradigm.
Design and Methods: Participants (N= 116) received a therapeutic instruction derived from either a habituation-based approach or the inhibitory learning model (expectation violation). Participants were repeatedly exposed to painful thermal stimulations until a predefined exposure goal was reached.
Results: The expectation violation instruction led to faster goal attainment and higher response rates than the habituation instruction. Both instructions led to increased pain tolerance in the short and long term (one-week follow-up).
Conclusion: Our results suggest that exposure treatments using an expectation violation instruction are especially time-effective. Although the findings from this analogue design cannot be directly generalized to populations with clinically relevant levels of chronic pain, they do point to some important theoretical and clinical implications for the treatment of pain.
Keywords: exposure therapy, inhibitory learning model, expectation violation, dose-response relationship
Introduction
For decades of research, exposure therapy has been shown to be a highly effective intervention for various mental health problems, such as anxiety,1–3 obsessive compulsive disorder,4 and post-traumatic stress disorder.5 More recently, Vlaeyen and colleagues have adapted exposure therapy to chronic low back pain.6 Such exposure-based treatment approaches expose patients to situations they normally avoid, eg, exhibiting certain movements that are perceived as threatening.7 Several randomized controlled trials as well as single-case studies have demonstrated that exposure therapy is effective in reducing disability by targeting pain-related fear in back pain6,8–12 and chronic regional pain syndromes.13,14
Notwithstanding the indisputable effectiveness of exposure therapy, a debate about the central underlying mechanisms has emerged in the last decade. In particular, the long-standing assumption that habituation (ie, experiencing that a certain unpleasant emotional state subsides over time) is the underlying mechanism has recently been challenged.15–19 Supposedly, not habituation, but a violation of an individual’s expectations leads to successful and long-lasting extinction.16,20,21 That is, it is assumed that making the experience that a feared outcome does not occur results in more sustained symptom reduction. These two rationales can be translated into different therapeutic instructions when delivering exposure treatment: Following the habituation rationale, people suffering from pain, for instance, could be guided to rate their emotional response during the exposure to a certain (feared) movement (eg, distress on a scale from 0 to 10); in this case, exposure is continued until the patients’ distress significantly declines (ie, habituation is reached). Alternatively, they could be guided to test their expectation (eg, “exhibiting this movement will damage my spinal cord”) by performing the respective movement and iteratively rate the subjective probability of harmful consequences (eg, likelihood of spine damage). When doing these exercises, patients normally experience that their expectation of physical harm is disconfirmed, thus leading to enhanced activity and reduced impairment.22,23 Yet, despite widespread enthusiasm for such an “inhibitory learning model”,15,24,25 little is known about how it compares directly to habituation-based approaches.25–28
Some recent studies have compared habituation- and inhibitory learning-based (expectation violation) approaches. The evidence attained from studies that examined exposures for different mental disorders (eg, anxiety) points to either no differences between the two instructions29 or slightly superior effects of the inhibitory learning approach.21,30,31 The first direct comparison in an experimental study on pain31 revealed that, in comparison to a control instruction, both instructions improved cognitive pain coping, but only the expectation violation instruction increased pain tolerance.
Besides the mere effectiveness of a specific treatment, its efficacy might also be taken into account when considering its implementation into routine care, which is characterized by high case load and efficient time scheduling.32,33 Thus, if one has two treatment options at hand, which are similarly effective, but one outperforms the other in terms of the time required to achieve the predefined outcome, the more efficacious treatment ought to be preferred. Following this reasoning, it has been suggested that one advantage of expectation violation-based exposure therapy might be the lower number of repetitions needed, that is, the treatment “dose” to achieve a therapeutic goal (“response”).34 This might be because habituation is not deemed crucial to defining a single session and an entire exposure-based treatment as successful.35 Indeed, a recent randomized controlled trial comparing a short-term and a long-term version of exposure therapy for patients with chronic back pain revealed faster improvement when fewer sessions were offered.36 This means that exposure therapy for pain has the potential to bring about significant improvement very quickly; yet, it is not clear whether this can be best achieved by focusing on habituation-based or expectation violation-based instructions.
Therefore, the aim of the current study was to investigate the efficacy and the “dose-response relationship” of different instructions for pain exposure. We compared a habituation-based instruction and an expectation violation-based instruction in pain-free female participants who were exposed to painful thermal stimulations after inducing fear of bodily harm. In doing so, we aimed to replicate the previous study mentioned above,31 and extended its design by adding a one-week follow-up assessment and tailoring the number of exposure trials. For reasons of feasibility, we decided to use an analogue sample to investigate differences in the efficacy of two exposure instructions deriving from distinct theoretical approaches.37 Although the generalization of results from analogue samples to a clinical population is questionable, Craske and colleagues suggested that examining fear extinction in healthy individuals and analogue samples may be promising to understand the underlying processes, which, ultimately, may also inspire subsequent research in clinical samples.19
We hypothesized that participants in the expectation violation condition would require fewer exposure trials than those in the habituation condition to reach a predefined exposure goal (hypothesis 1: “dose-response relationship”). Drawing on previous findings,31 we expected no differences in relevant pain outcomes between the conditions (hypothesis 2: “changes in cognitive pain coping and pain perception: pain tolerance, pain intensity and pain unpleasantness”). In addition, we were interested in potential predictors of the response, because although exposure has proven effective for treating patients with chronic pain in multidisciplinary settings with limited time and resources, high dropout rates have been reported compared to (non-exposure-based) cognitive-behavioral therapy treatments.36 Hence, it might be important to identify baseline patient characteristics that bear predictive value for treatment outcomes or relapse.33,38,39 Accordingly, we examined pain anxiety and pain catastrophizing as two potential predictors of the treatment response. These variables were chosen as exposure has been found especially effective for patients with elevated levels of fear,36 while high catastrophizers did not improve from exposure treatments.40 Catastrophizing is one of the best predictors not only for clinical pain, but also for experimental pain (eg,41,42). That is, participants who endorse catastrophizing thoughts in relation to experimentally induced pain, show higher pain ratings and greater temporal summation of thermal pain.41 Moreover, healthy participants have been found to differ in terms of their cognitive and emotional response to pain (eg,43).
Methods
Participants
A power analysis for MANOVAs (α = 0.05; power = 0.80) indicated that a sample of 111 participants was needed to detect significant effects. Based on the results of Schemer and colleagues,31 we expected medium to large effects. Participants were recruited through flyers and advertisements. They received either course credit or financial compensation for their participation. Inclusion criteria were: female sex; 18–65 years; sufficient German language knowledge; absence of any medical illness (eg, acute/chronic pain; Raynaud’s disease; hypertension; neuropathy; coronary diseases; diabetes). Of note, males were excluded because we aimed to reduce potential sources of confounding effects, given previous research pointing to sex differences in pain sensitivity,44 habituation,45,46 and reported pain.47 The local ethics committee at the Psychology department at the Philipps-University Marburg approved this study’s protocol (AZ: 2017–41k).
Study Design
The procedure (similar to;31 for further details, see Supplementary Materials, Table A1) consisted of three parts, each about one week apart (see Figure 1). Participants were randomly assigned to either a habituation instruction (n = 58) or an expectation violation instruction (n = 58). A computer-generated randomization schedule guaranteed an equal number of participants in each condition and the same number of trials per condition for each experimenter. To investigate whether the therapeutic instructions differentially affected pain perception (pain tolerance, intensity, and unpleasantness) as well as cognitive coping with pain, all measures were conducted immediately after the exposure trials (post-test) and one week later (follow-up).
 |
Figure 1 Study design and procedure. After completing a battery of questionnaires online, the participants signed in for a laboratory assessment consisting of three parts: (a) baseline (t0); the manipulation of threat expectations was followed by the baseline of pain tolerance, intensity, and unpleasantness; (b) following the presentation of the therapeutic instruction (randomized allocation to either habituation or expectation violation), the participants underwent several exposure trials until a predefined exposure goal was reached. During these exposure trials, the participants were exposed to nociceptive thermal stimuli; (c) a post-test (pain tolerance, intensity, unpleasantness) and a post-assessment of questionnaires was followed by a manipulation check. In a one-week follow-up, pain tolerance, intensity, unpleasantness, and the questionnaires were conducted again before the aims of the study were disclosed to the participants. |
Demographic data were assessed by brief self-report items and further outcome variables (Cognitive Pain Coping, Pain Catastrophizing, and Pain Anxiety) online prior to the laboratory appointment. After giving their informed consent in accordance with the Declaration of Helsinki, participants’ threat beliefs were manipulated as described in Threat Induction. First, in the baseline phase, we tested the participants’ individual pain tolerance (see Pain Tolerance, Pain Intensity, and Pain Unpleasantness). Then, depending on the experimental condition and thus the therapeutic instruction, the exposure-based treatment was explained. Next, participants were asked to apply the strategy they had just learned (habituation vs expectation violation) when being provided with the painful thermal stimulations. Participants then rated the credibility of the instructions they had been given, respectively. In the post-test phase, they were instructed to reflect on what they had learned. Subsequently, the post-training assessment of pain tolerance was conducted and participants completed the same additional questionnaires from the baseline assessment (Cognitive Pain Coping, Pain Catastrophizing, and Pain Anxiety) again. At follow-up, pain tolerance was assessed again and participants completed the questionnaires (Cognitive Pain Coping, Pain Catastrophizing, and Pain Anxiety) one more time. Finally, participants rated the credibility of the threat manipulation, and they were debriefed about the manipulation and its real purpose (see below).
Threat Induction
As exposure therapy is designed to target extended fear of pain levels and threat beliefs, we experimentally induced threat in healthy participants. To this end, we referred to previous studies using similar manipulations.48,49 The specific threat induction used in the present study was derived from a previous study.31 To examine the suitability of this manipulation, the authors tested it in a small pilot study (N = 18). To evoke fear of pain, participants were asked to sign a declaration of alleged side effects (eg, skin redness, fainting). To enhance the personal relevance of these adverse effects, the experimenter claimed that due to appearing skin redness, she was required to measure the skin thickness, as it would correlate with the likelihood of side effects. The experimenter (falsely) described a sham measure as an indicator to evaluate an individual’s vulnerability to the occurrence of side effects. First, every participant was informed that her value was allegedly a “borderline higher risk” for side-effects to occur. Second, fear was enhanced by claiming that the temperature during the following trials would become more intense, with participants being unable to stop it by themselves, in contrast to the baseline assessment of pain tolerance. Participants were not informed that the temperature would not rise above their previously measured pain tolerance (≤ 52°C).
Intervention: Exposure Instructions and Determination of an Exposure Goal
The exposure instructions consisted of two parts: First, participants listened to standardized instructions via loudspeaker, in which the exposure rationale was explained, based on the respective theory. These instructions were used in other studies before.31,50 Second, participants were guided to either focus on their emotional or to their cognitive appraisal of the painful stimulations via standardized questions. These questions were based on a detailed manual, which was developed in a previous study.31 The contents of the two instructions are presented in detail below.
The habituation instruction focused on changes in the emotional response to the feared stimulus. The exposure rationale was explained as a process of fear habituation each time someone faces a feared situation. The experimenter then encouraged participants to verbalize their emotional response (eg, fear, distress, anxiety, discomfort) prior to the exposure trials. Before and after each trial, participants were asked to indicate and rate their momentary emotional response (eg, “How distressed do you feel before the next trial?”) on an 11-point scale (0 = neutral; 100 = very high). The individual exposure goal was reached when the level of the emotional response was reduced by half of its initial score (eg, from “80” to “40”).
The expectation violation instruction focused on the cognitive response to the feared stimulus. The exposure rationale was explained as a systematic testing of individual predictions about negative outcomes through exposure experience. The experimenter encouraged participants to formulate their central concerns about the exposure trials with the thermode. The concerns being mentioned by the participants (eg, “My skin will burn and blister”) at this point were those expectations that were supposed to be disconfirmed subsequently. Specifically, prior to each trial, participants were asked to estimate the expected likelihood of experiencing their feared outcome (eg, “How likely do you think your skin will burn and blister during the next trial?”) on an 11-point scale (0 = not likely; 100 =very likely). The individual exposure goal was reached as soon as the likelihood of the concern’s occurrence fell to at least half of its initial score (eg, from “80” to “40”).
Further details regarding the instructions and the standardized questions used can be found in the Supplementary Materials, B. Experimenters were trained in adhering to the standardized protocol.
Measures
“Dose”
The dependent variable was the number of trials that participants needed to reach their exposure goal, which reflects the treatment “dose”. Specifically, training continued until participants had demonstrated sufficient progress in reaching the a priori defined exposure goal (as described in Intervention: Exposure Instructions and Determination of an Exposure Goal), with a minimum of three trials and a maximum of 10 trials. The minimum of three trials was set based on the observation in a previous study that only 50% of the participants reported a decrease in distress within three trials.31 The maximum of ten trials was chosen primarily for reasons of feasibility, see also36 in this respect. Of note, we used different methods to determine the exposure goal for the two conditions for the following reason: As we hypothesized the instruction to differ in terms of efficacy, we put effort into explaining and implementing each rationale precisely while not confusing it with key terms of the other condition, respectively. Accordingly, the predefined exposure goals differed between the two conditions, since the underlying rationales were significantly different. Thus, the stop criterion (that is, the point where the experimenter finished the exposure session) differed between the two experimental conditions, but the dependent variable was identical in both conditions (“number of trials needed”). Worthy of note, all participants were not previously informed about a specific number of trials to avoid this being interpreted as a safety signal.
Pain Tolerance, Pain Intensity, and Pain Unpleasantness
Participants were applied heat stimulations on the non-dominant forearm using a thermode (Thermal Sensory Analyzer: TSA II; Medoc Ltd, Ramat Yishai, Israel), a commonly used device to study pain experimentally in the laboratory. The procedure has been found reliable and valid for assessing pain tolerance (eg,51–53). Starting with a temperature of 32°C, temperature continuously increased with a slope of 0.5°C per second (while not exceeding the maximum of 52°C). Pain tolerance was assessed by asking participants to tolerate the thermal stimulations for as long as possible, and to terminate the measurement when they were no longer willing to bear it. Thus, the participants’ pain tolerance is the point (temperature in °C) where they stopped the increasingly painful thermal stimulation. The maximum temperature of 52°C was reached after 40 seconds, unless participants stopped the measure prior to that. When the measurement was stopped, the software automatically initiated a temperature decline to the initial temperature of 32°C (slope 10°C/second).
After each pain tolerance assessment, participants rated their pain intensity on a Numeric Rating Scale, ranging from 0 = no pain to 10 = worst imaginable pain and the pain unpleasantness on the same scale with the extrema (0 = bearable to 10 = unbearable). The distinction between pain intensity and unpleasantness is based on the commonly used differentiation between rather can be considered as measuring of the cognitive/“appraised” aspects of pain (intensity) and a more affective the (“felt”)/affective dimension of pain (unpleasantness).54
For the subsequent exposure trials, the temperature corresponding to the individual pain tolerance was applied for a maximum of 4 seconds, before it automatically declined (slope of 10°C/second).
Cognitive Pain Coping
Participants were asked to complete the cognitive pain-coping subscale of the German Coping Questionnaire (FESV),55 which addressed their heat-pain experience. The scale was developed to assess the repertory of strategies to cope with pain and psychological distress among individuals suffering from chronic pain. Further, it aims to assess cognitive processes resulting from pain experiences rather than pain experience itself and the questionnaire is intended to be used in process examination for evaluating treatment success. The instructions were adapted according to the experimental setting31 with good internal consistency (Cronbach’s α = 0.80). Of note, we assessed cognitive pain coping three times (baseline; post-training; and follow-up) to examine whether it changed through the exposure treatment, and whether the two experimental conditions differed herein.
Pain Catastrophizing
We applied the Pain Catastrophizing Scale (PCS)56,57 to measure the participants’ propensity to engage in catastrophizing thoughts in relation to painful sensations. Participants are instructed to reflect on previous painful experiences and to rate the degree to which they experience each of 13 feelings or thoughts when feeling or expecting pain on a 5-point scale (0 = not at all; 4 = all the time). The internal consistency of the adapted questionnaire was good (Cronbach’s α = 0.90).
Pain Anxiety
The 20-item short version of the Pain Anxiety Symptoms Scale (PASS)58 was used to measure fear of pain. Participants rated the frequency of their experiences of fear and anxiety in relation to pain on a 5-point scale (0 = never, 4 = always). At t1 and t2 in our study, participants were asked to refer to the heat pain they had experienced. The escape/avoidance subscale of the PASS was adapted for this purpose. For example, the item “As soon as pain comes on, I take medication to reduce it” was changed to “As soon as pain begins, I try to reduce it somehow.” Given that we adapted the questionnaire used during the experiment, we evaluated its internal consistency based on the present sample. The internal consistency of the adapted questionnaire was good (Cronbach’s α = 0.89).
Confounding Baseline Variables
Moreover, we assessed the following questionnaires at baseline to control for relevant confounding factors: Beck’s Depression Inventory,59 Pain Sensitivity Questionnaire,60 Pain Vigilance and Awareness Questionnaire.61
Statistical Analyses
Data analyses were conducted using IBM SPSS® (Windows v.22: SPSS Inc, Chicago, IL). Participants’ data were excluded if data of an entire session was missing systematically.
To check for baseline differences between the conditions in pain-relevant variables (intensity, unpleasantness, pain sensitivity, and pain vigilance and awareness), depressive symptoms, and demographic data, T- and chi-square tests were carried out.
First, the differential effects of the instruction on the number of exposure trials needed were tested with a t-test for independent samples. Differences between the experimental groups in exposure trials needed were examined in a chi-square test (hypothesis 1). Second, we performed a repeated 2 (Time: post vs follow-up) x 2 (Condition: expectation violation vs habituation) mixed ANOVA with pain tolerance, intensity, unpleasantness, and cognitive pain coping as the dependent variables (hypothesis 2). Differences between the conditions regarding their efficacy should result in a significant Time by Condition interaction in that 2 by 2 ANOVA. In addition, we calculated the effect sizes (Cohen’s d and partial η2). Baseline pain tolerance was included as a covariate as the temperature applied during the exposure trials varied across individuals based on their individual pain tolerance from the baseline pain assessment. Further, in case of baseline differences in demographic or pain-related variables, the respective variable will be included as a covariate in the analysis. Third, predictions of the number of trials needed based on pain anxiety and pain catastrophizing were assessed via a hierarchical multiple regression analysis.
Results
Baseline Characteristics
In total, 180 participants completed the online survey, and 121 of them participated in the subsequent experimental session. One person withdrew her participation due to the threat manipulation. Four participants were excluded from the analyses because data from an entire session (t0, t1, or t2) was missing for these participants. Thus, we analyzed data from 116 participants whose ages ranged from 18 to 41 years (M = 22.6, SD = 3.2). The demographic data are shown in Table 1, and the means and standard deviations of the baseline measures are reported in Table 2.
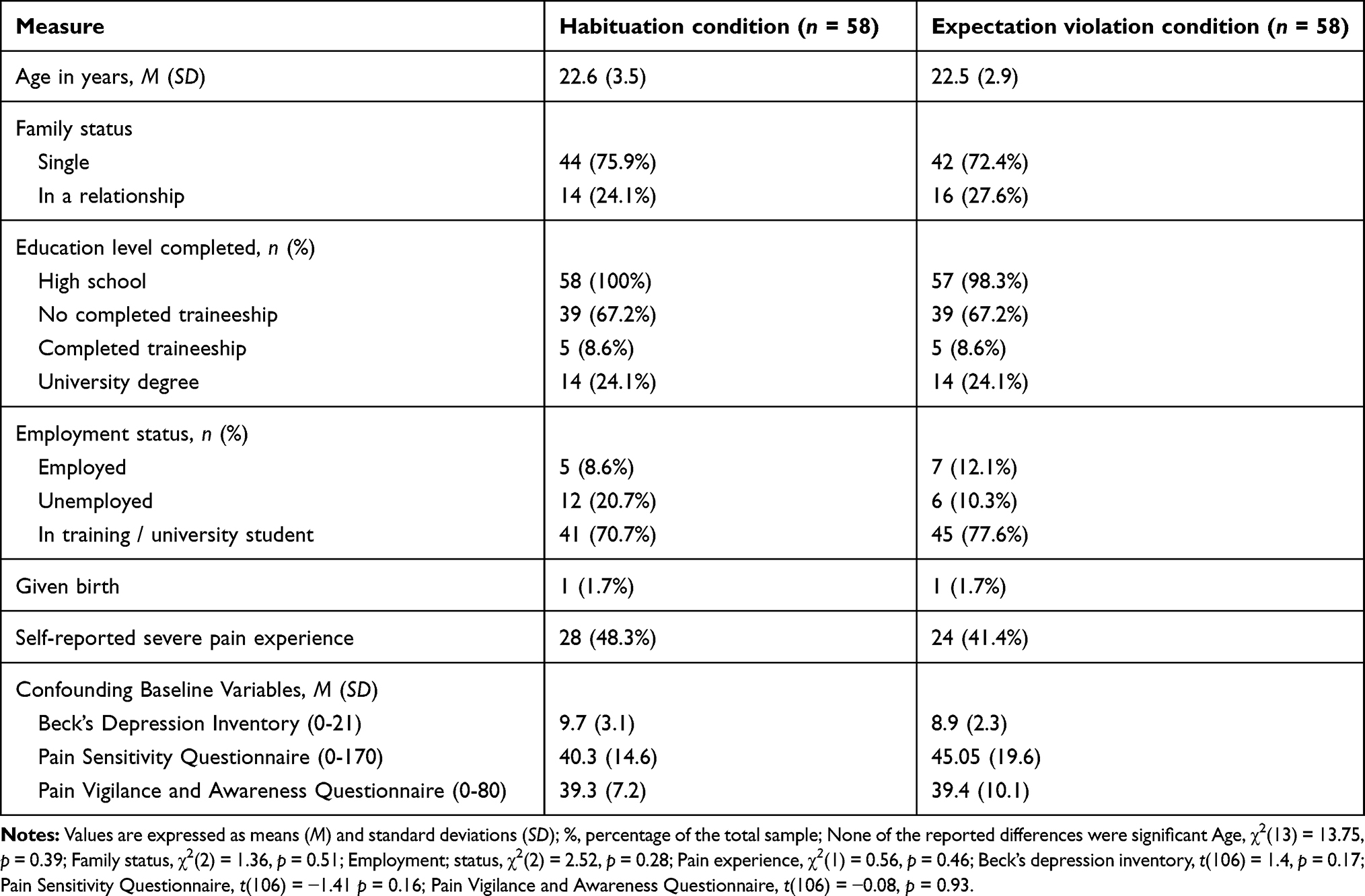 |
Table 1 Participants’ Demographic Characteristics and Baseline Scores for Both Conditions |
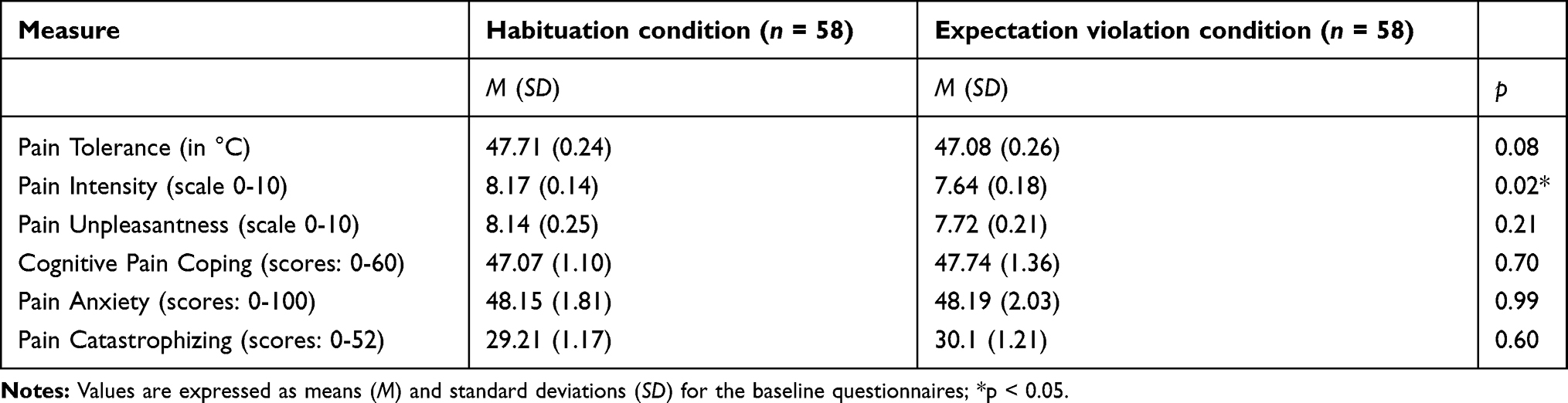 |
Table 2 Baseline Values of Variables of Interest for Both Groups |
The multivariate analyses indicated no significant differences between the conditions on any baseline questionnaire (depressive symptoms, pain sensitivity, pain vigilance), Pillai’s trace = 0.99, F(6,109) = 1.44, p = 0.208. A multivariate ANOVA revealed no significant baseline differences between the conditions for pain unpleasantness, pain anxiety, pain catastrophizing, and cognitive pain coping. However, for pain intensity, we did note significant differences between the two conditions, F(1, 114) = 5.26, p = 0.024, showing greater pain intensity in the habituation condition.
Hypothesis Tests
Hypothesis 1: “Dose-Response Relationship”
A t-test for independent groups revealed a significant group difference in the number of exposure trials needed, t(114) = 4.98, p < 0.001, Cohen’s d = 0.93, with an average of ~3 trials in the expectation violation condition (M = 3.41, SD = 1.57) and an average of ~5 trials in the habituation condition (M = 5.43, SD = 2.66). In line with our main hypothesis, the number of necessary exposure trials differed between conditions, χ2(6) = 39.79, p < 0.001. A histogram of the detailed proportion of trials needed for each condition is shown in Figure 2.
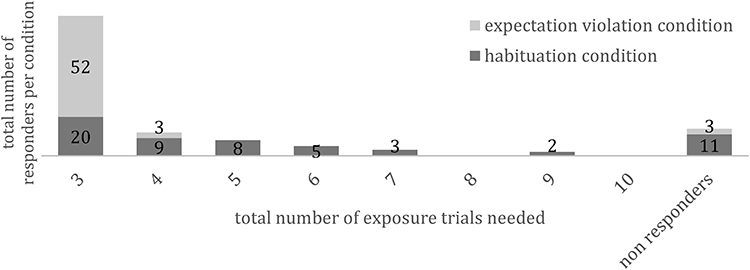 |
Figure 2 Number of exposure trials (dose) needed to achieve the predefined exposure goal (responder) by instruction condition. |
Hypothesis 2: “Changes in Cognitive Pain Coping and Pain Perception: Pain Tolerance, Pain Intensity and Pain Unpleasantness”
To test whether the conditions differed in relevant pain outcomes after treatment, we conducted a multivariate Time by Condition ANOVA. The assumptions of this test (normal distribution, homogeneity of covariance matrices) were fulfilled adequately. Due to baseline differences in pain intensity, the baseline pain intensity was included as a covariate in addition to the baseline pain tolerance (see 2.4.2). Neither the main effect of Time, Pillai trace = 0.12, F(4, 109) = 0.86, p = 0.488, partial η 2 = 0.03, nor Condition, Pillai trace = 0.06, F(4, 109) = 1.84, p = 0.126, partial η 2 = 0.06, nor the Time by Condition interaction, Pillai trace = 0.03, F(4, 109) = 0.93, p = 0.450, partial η2 = 0.03, was significant. These results indicated that the two experimental conditions did not differ in any of these outcomes (ie, cognitive pain coping, pain tolerance, intensity, unpleasantness), neither at post- nor at follow-up assessment.
Research Questions: “Predictors”
As shown in Table 3, pain anxiety negatively predicted the number of trials across experimental groups, whereas pain catastrophizing was a positive predictor. Higher pain anxiety levels predicted a lower number of trials needed, and higher pain catastrophizing levels predicted a higher number of trials needed. Taken together, these predictors accounted for 24% of the variance in the model. Including the interaction terms “Pain anxiety/Condition” and “Pain catastrophizing/Condition”, did not explain additional variance.
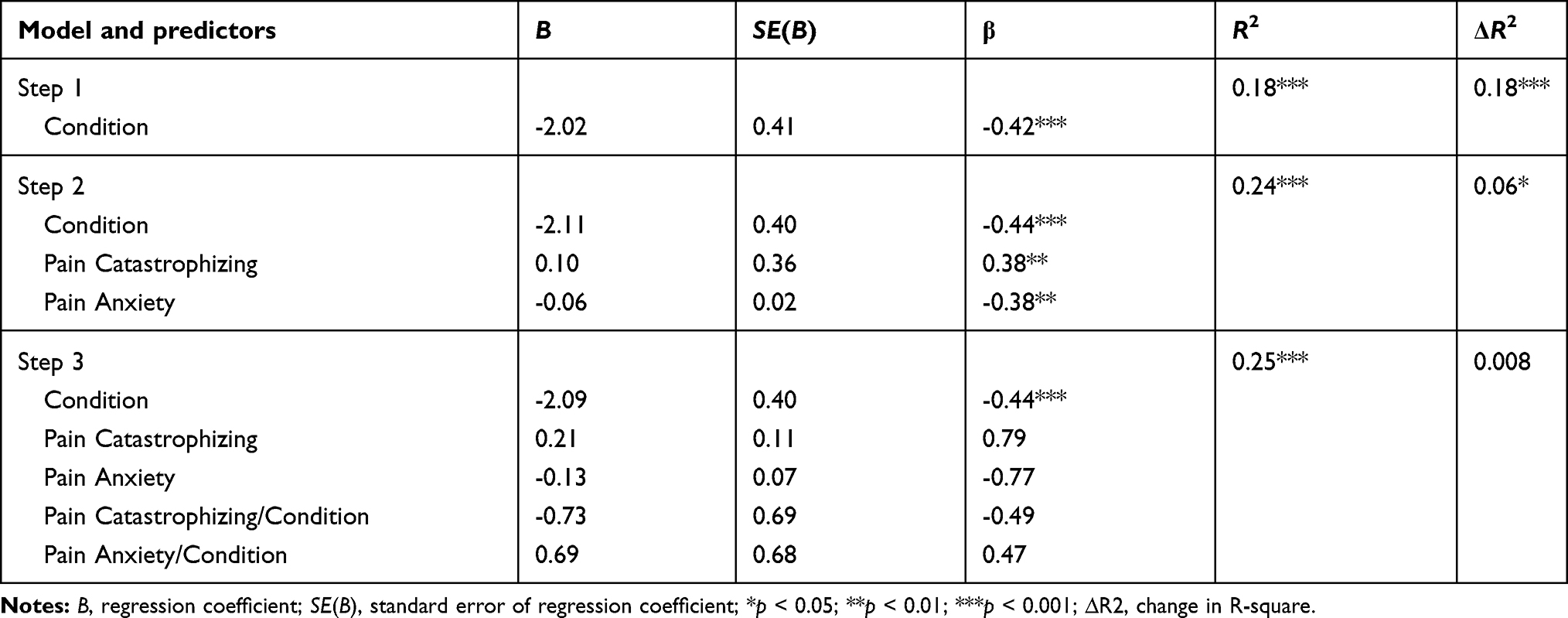 |
Table 3 Hierarchical Multiple Regression Analysis for Prediction of Number of Exposure Trials Needed |
Discussion
In this study, we compared the effects of a habituation-based and an expectation violation-based instruction – representing different therapeutic strategies in exposure treatment – when healthy participants where provided with painful thermal stimulations. A novel feature of this study was the investigation of the “dose-response relationship”, that is, the number of exposure trials needed for each exposure instruction to reach a predefined exposure goal. In line with our main hypothesis, the number of exposure trials needed to achieve the predefined exposure goal differed between instructions: Participants in the expectation violation condition needed a lower “dose” (ie, fewer exposure trials) to reach their predefined goal than participants in the habituation condition. Specifically, almost 90% of the participants from the expectation violation condition needed only the minimum number of trials (3 trials = fast responders). The remaining participants did not reach the exposure goal within 10 sessions, though (= nonresponders). Participants from the habituation condition, on the other hand, needed significantly more trials to reach their goal: Only a third of all participants from this group reached the exposure goal within the minimum number of trials (= fast responders) and a fifth failed to reach it at all (= nonresponders). The other participants reached their goal between four to nine sessions (= normal to late responders). Across both conditions, participants’ pain tolerance (including the corresponding intensity and unpleasantness measures) increased from baseline to post-treatment. This effect also held at the one-week follow-up. Thus, both instructions were similarly effective in increasing participants’ pain tolerance. However, as we did not implement a control group receiving no instructions, we cannot be sure that the increase can indeed be attributed to the therapeutic instructions. Cognitive pain coping did not change during the training course. We found that habituation and expectation violation did not differ in terms of pain-related outcomes. Thus, our results suggest that while habituation and expectation violation may be similarly effective in terms of pain perception, expectancy violation might be the more time-effective approach in view of the lower number of trials required to reach the exposure goal.
Our finding that participants in the expectation violation condition required fewer trials to achieve similar effects as participants in the habituation condition is consistent with the inhibitory learning approach.15,16 In this approach, it is assumed that extinction learning can be enhanced by maximizing the discrepancy between prediction and experience (ie, expectancy violation). Thus, since individuals are aware of their concrete expectations, they can reevaluate them in light of the new learning experience (eg, harmful consequences do not occur). Accordingly, focusing on cognitive change during exposure, that is, the disconfirmation of fear-related expectations, has been discussed in terms of having the potential to maximize the effects of exposure therapy.21,62 With the habituation instruction, on the other hand, the individual has no concrete task other than to observe his or her physical and emotional reaction without engaging in any avoidance behavior.63 Our results suggest that learning in this approach takes longer, presumably because the disconfirmation of fear-related beliefs requires more time as compared to the more “straightforward” expectation violation approach.
Similar to a previous study,31 we failed to detect any differences between the two exposure instructions in terms of their effects on pain coping. Nevertheless, in that previous study, the expectation violation but not the habituation instruction increased pain tolerance in comparison to a control group. Similarly, only the expectation violation instruction led to distinct changes in physiological activation. We could not replicate this finding in the present study. This discrepancy might be the result of the omission of a control condition in the present study. Our results are in line with other experimental studies comparing the two exposure approaches.29 Although aiming at expectation violation was no more effective than aiming at habituation, both instructions were more effective than a no-treatment control group in that study.
One might interpret our results as an indication that both instructions are effective, but that expectation violation may be considered a “shortcut”. It might possess an advantage thanks to its context of cognitive preparation, as the individual has been given precise instructions as to what they should focus on. Taking into account that chronic pain is often treated in multidisciplinary (inpatient) settings with restricted schedules, rapid responses seem highly relevant.36,64
Higher levels of pain anxiety and lower levels of pain catastrophizing in our healthy sample were predicted fewer trials needed, independently of the instruction type. Considering this finding in a broader context with regard to findings from clinical samples, this may appear contradictory at first glance: while higher pain anxiety was associated with fewer trials needed, higher pain catastrophizing was related to more trials needed. Yet, it should be noted that the conclusions that can be drawn in relation to pain anxiety and catastrophizing are limited due to the use of a healthy sample, since variance in these variables is limited in healthy volunteers. This apparently contradictory pattern might be resolved by considering the following: Exposure therapy is especially pertinent for highly fear-avoidant chronic pain patients7,65 and has recently been found effective only for patients with elevated levels of fear-avoidance beliefs.36 A faster response in persons with higher anxiety scores is therefore in line with this finding. Furthermore, there is empirical evidence suggesting that patients who manifest high levels of catastrophizing and fear benefit less from therapy,15,40,66 and its reduction predicts and mediates the outcomes of both physical and psychological treatments.5,67,68 Catastrophizing was identified as a moderator of treatment outcome, particularly for exposure treatment; indeed, exposure was effective only for patients with low or moderate levels of catastrophizing, whereas high catastrophizers did not improve from the treatment.40 Catastrophizing may impede exposure therapy, as individuals with high levels are less willing to confront themselves. Thus, they may avoid situations that violate their threat expectations and exposure-based treatments alike.
Limitations and Strengths
The most notable limitation of the present study is the clinically unrepresentative sample. Our participants were healthy and not seeking pain treatment. In order to enhance the internal validity of our study, we used strict eligibility criteria and self-selection processes, which, however, further restricted the generalizability of our findings. Our study cohort was characterized by a restricted age range, overrepresented students or academics, and included only females. The generalizability of the current findings to males may also be limited with regard to gender-specific differences in pain perception and reporting. Moreover, concerning age range, educational levels, and motivational state, our sample was not representative for patients with chronic pain (see eg,69). Nevertheless, our approach of an experimental analogue study offers some insights into the underlying mechanisms of change in fear of pain. By this view, the examination of a clinical sample may have been problematic in terms of internal validity, since patients suffering from chronic pain differ greatly in their individual learning histories, thereby posing confounding influences on the parameters of interest. Participants in our sample, however, did not significantly differ in how they experienced pain; thus, the group differences regarding the number of exposure sessions needed can more safely be attributed to the different therapeutic instructions.
Clearly, a single-trial exposure treatment, as performed in the present study, is not representative of the conduction of exposure treatment in therapy, which is usually delivered over weeks or months, accompanied by other interventions such as cognitive restructuring. However, to compare the effects of two different instructions, isolating the sole effect of exposure therapy and reducing it to a specific duration is advantageous. Therein lies the superiority of well-controlled efficacy trials over clinical trials for investigating the effects of single treatment parameters that could enhance clinical practice (see also35). If a parameter is found to be effective in cost-effective analogous samples, its effectiveness should undergo further investigation in clinical trials with representative samples and interventions in a second step.7,37,70 A further limitation of our study was that the main outcome of the study (trials needed to achieve exposure goal) was determined differently for the conditions. Although inevitable due to the different explanations provided to the participants, as noted above, this potentially compromises our findings, as we cannot rule out the possibility that distress decreases slower than expectancy and that this explains the differences between conditions, and not the instructions themselves. This issue might be addressed in future by using physiological measures in addition to self-report measures.
To test for effect stability and to expand comparability to exposure therapy, a one-week follow-up was established. As suggested by Craske and colleagues,71 exposure trials should be conducted at separate occasions with time intervals long enough to enable long-term learning, a factor based on findings from studies with rodents in which the consolidation of extinction learning works best with training sessions spaced apart.72 This is considered especially important as the expectation violation approach derived from the inhibitory learning model is supposed to minimize the return of fear (see15).
In clinical practice, a specific criterion needs to be predefined that indicates when the exposure session can be terminated. As the criterion ought to be derived from the presumed mechanism of change, different exposure criteria for our instruction conditions were inevitable26,28 and explicitly required to analyze the efficacy of different exposure-based approaches.50,73 In the previous study,31 only 50% of participants reported a decrease in their fear levels over the course of three exposure trials. Thus, we extrapolated that three trials are insufficient for habituation to occur in most participants.
Directions for Future Research
While the present research was a laboratory study focusing on heat pain tolerance, future studies examining different exposure instructions might focus on more clinically relevant outcomes such as disability and global functioning.23 In addition, exposure in chronic pain can be optimized in three ways based on future research. First, studies that shed light on the underlying mechanisms of action are likely to help to optimize the treatment (eg, evidence-based criteria for a successful session). Second, research on individual characteristics such as the catastrophizing tendencies that predict treatment response, non-response, or dropout are particularly relevant74,75 to plan individual treatments (eg, prevention of side effects and unnecessary strain) and to minimize direct and indirect financial costs for the healthcare system. Third, in line with the agenda of personalized medicine to administer patients “the right drug at the right dose at the right time”,76 future research should inform psychotherapists about differential indications, such as which therapeutic instruction is most effective for which patient.77
Clinical Implications
Although our study was designed as an experimental analogue study in healthy participants, some cautious conclusions about treating pain in clinical practice might be drawn. As such, our main finding, showing that the respective exposure goal was achieved faster in the expectancy violation approach than in the habituation approach, can be seen as an argument favoring this approach. In doing so, instructing patients to formulate and re-examine their concrete individual concerns prior to exposure treatments and re-examine them during exposure treatments may help reduce patients’ excessive and disabling fear-avoidance beliefs.78 Introducing a re-evaluation of beliefs might be especially helpful in chronic pain patients, as they experience a transition of the informational character of pain experiences (ie, pain loses its useful signal character for harm prevention in chronic conditions). There is recent evidence that shorter exposure outperforms longer versions in chronic pain36 and obsessive-compulsive disorder.79 The impact of specific therapeutic instructions requires further investigation in clinical samples.
Conclusion
While the two therapeutic instructions for exposure treatment (habituation vs expectation violation instruction) did not differ in increasing pain tolerance, the expectation violation instruction proved to be superior in terms of the number of trials needed to achieve the predefined exposure goal. Independently of the therapeutic instruction, high levels of pain anxiety and low levels of pain catastrophizing predicted faster responses. Our results suggest that expectation violation is an effective shortcut for exposure treatments, although replication in samples with chronic pain is clearly warranted.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors like to thank Prof. Dr. Winfried Rief for his overall support. The authors wish to acknowledge Lena Brückner, M. Sc., Julia Hoffmann, M. Sc., and Erika Renner, B. Sc., for their diligent work during the acquisition phase. This study was funded by the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) – project number 290878970-GRK 2271, Projekt 3; grant to Prof. Dr. Julia Glombiewski. The publication was funded by the Open Access Fund of the University of Marburg.
Disclosure
The authors report no potential conflicts of interest for this work.
References
1. Foa EB, Kozak MJ. Emotional processing of fear: exposure to correct information. Psychol Bull. 1986;99(1):20–35. doi:10.1037/0033-2909.99.1.20
2. Hofmann S, Smits J. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621–632. doi:10.4088/JCP.v69n0415
3. Norton PJ, Price EC. A meta-analytic review of adult cognitive-behavioral treatment outcome across the anxiety disorders. J Nerv Ment Dis. 2007;195(6):521–531. doi:10.1097/01.nmd.0000253843.70149.9a
4. Kozak MJ, Foa EB, Steketee G. Process and outcome of exposure treatment with obsessive-compulsives: psychophysiological indicators of emotional processing. Behav Ther. 1988;19:157–169. doi:10.1016/S0005-7894(88)80039-X
5. Powers MB, Halpern JM, Ferenschak MP, Gillihan SJ, Foa EB. A meta-analytic review of prolonged exposure for posttraumatic stress disorder. Clin Psychol Rev. 2010;30(6):635–641. doi:10.1016/j.cpr.2010.04.007
6. Vlaeyen JWS, De Jong J, Geilen M, Heuts PHTG, Van Breukelen G. Graded exposure in vivo in the treatment of pain-related fear: a replicated single-case experimental design in four patients with chronic low back pain. Behav Res Ther. 2001;39(2):151–166. doi:10.1016/S0005-7967(99)00174-6
7. Vlaeyen JWS, Crombez G. Behavioral conceptualization and treatment of chronic pain. Annu Rev Clin Psychol. 2020;16:1. doi:10.1146/annurev-clinpsy-050718-095744
8. Bailey KM, Carleton RN, Vlaeyen JW, Asmundson GJ. Treatments addressing pain-related fear and anxiety in patients with chronic musculoskeletal pain: a preliminary review. Cogn Behav Ther. 2009;39(1):46–63. doi:10.1080/16506070902980711
9. Bliokas VV, Cartmill TK, Nagy BJ. Does systematic graded exposure in vivo enhance outcomes in multidisciplinary chronic pain management groups? Clin J Pain. 2007;23(4):361–374. doi:10.1097/AJP.0b013e31803685dc
10. Leeuw M, Goossens MEJB, van Breukelen GJP, et al. Exposure in vivo versus operant graded activity in chronic low back pain patients: results of a randomized controlled trial. Pain. 2008;138(1):192–207. doi:10.1016/j.pain.2007.12.009
11. Vlaeyen JW, de Jong J, Geilen M, et al. The treatment of fear of movement/(Re) injury in chronic low back pain: further evidence on the effectiveness of exposure in vivo. Clin J Pain. 2002;18:251–261. doi:10.1097/00002508-200207000-00006
12. Woods MP, Asmundson GJG. Evaluating the efficacy of graded in vivo exposure for the treatment of fear in patients with chronic back pain: a randomized controlled clinical trial. Pain. 2008;136(3):271–280. doi:10.1016/j.pain.2007.06.037
13. De Jong JR, Vlaeyen JWS, Onghena P, Cuypers C, Den Hollander M, Ruijgrok J. Reduction of pain-related fear in complex regional pain syndrome type I: the application of graded exposure in vivo. Pain. 2005;116(3):264–275. doi:10.1016/j.pain.2005.04.019
14. den Hollander M, Onghena P, Smeets R, Vlaeyen JWS. Expose or protect? A randomized controlled trial of exposure in vivo vs pain-contingent treatment as usual in patients with complex regional pain syndrome type 1. Pain. 2016;157:2318–2329. doi:10.1097/j.pain.0000000000000651
15. Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. 2014;58:10–23. doi:10.1016/j.brat.2014.04.006
16. Craske MG, Liao B, Brown L, Vervliet B. Role of inhibition in exposure therapy. J Exp Psychopathol. 2012;3(3):322–345. doi:10.5127/jep.026511
17. Treanor M, Craske MG. Exposure therapy. In: Encyclopedia of Mental Health. 2016. doi:10.1016/B978-0-12-397045-9.00024-0
18. Lipp OV, Waters AM, Luck CC, Ryan KM, Craske MG. Novel approaches for strengthening human fear extinction: the roles of novelty, additional USs, and additional GSs. Behav Res Ther. 2020;124(August2019):103529. doi:10.1016/j.brat.2019.103529
19. Craske MG, Hermans D, Vervliet B. State-of-the-art and future directions for extinction as a translational model for fear and anxiety. Philos Trans R Soc B Biol Sci. 2018;373(1742). doi:10.1098/rstb.2017.0025
20. Myers KM, Davis M. Mechanisms of fear extinction. Mol Psychiatry. 2007;12:120–150. doi:10.1038/sj.mp.4001939
21. Salkovskis PM, Hackmann A, Wells A, Gelder MG, Clark DM. Belief disconfirmation versus habituation approaches to situational exposure in panic disorder with agoraphobia: a pilot study. Behav Res Ther. 2007;45(5):877–885. doi:10.1016/j.brat.2006.02.008
22. Vlaeyen JWSS, Kole-Snijders MJ, Rotteveel M, Ruesink R, Heuts P. The role of fear of movement (re)injury in pain disability. J Occup Rehabil. 1995;5(4):235–252. doi:10.1007/BF02109988
23. Boersma K, Linton S, Overmeer T, Jansson M, Vlaeyen J, De Jong J. Lowering fear-avoidance and enhancing function through exposure in vivo: a multiple baseline study across six patients with back pain. Pain. 2004;108(1–2):8–16. doi:10.1016/j.pain.2003.03.001
24. Pittig A, Van Den Berg L, Vervliet B. The key role of extinction learning in anxiety disorders: behavioral strategies to enhance exposure-based treatments. Curr Opin Psychiatry. 2016;29:39–47. doi:10.1097/YCO.0000000000000220
25. Heinig I, Pittig A, Richter J, et al. Optimizing exposure-based CBT for anxiety disorders via enhanced extinction: design and methods of a multicentre randomized clinical trial. Int J Methods Psychiatr Res. 2017;26(2):1–12. doi:10.1002/mpr.1560
26. Benito KG, Walther M. Therapeutic process during exposure: habituation model. J Obsessive Compuls Relat Disord. 2015;6:147–157. doi:10.1016/j.jocrd.2015.01.006
27. Gloster AT, Wittchen HU, Einsle F, et al. Mechanism of action in CBT (MAC): methods of a multi-center randomized controlled trial in 369 patients with panic disorder and agoraphobia. Eur Arch Psychiatry Clin Neurosci. 2009;259(S2):155–166. doi:10.1007/s00406-009-0065-6
28. Himle MB. Let truth be thy aim, not victory: comment on theory-based exposure process. J Obsessive Compuls Relat Disord. 2015;6:183–190. doi:10.1016/j.jocrd.2015.03.001
29. Schyns G, van den Akker K, Roefs A, Hilberath R, Jansen A. What works better? Food cue exposure aiming at the habituation of eating desires or food cue exposure aiming at the violation of overeating expectancies? Behav Res Ther. 2018;102:1–7. doi:10.1016/J.BRAT.2017.12.001
30. Brown LA, Lebeau RT, Chat KY, et al. Associative learning versus fear habituation as predictors of long-term extinction retention. Cogn Emot. 2017;31:687–698. doi:10.1080/02699931.2016.1158695
31. Schemer L, Körfer K, Glombiewski JA. Evaluation of exposure instructions to pain: should therapist focus on fear reduction or expectation violation? Cognit Ther Res. 2019;44(3):697–708. doi:10.1007/s10608-019-10070-7
32. Gunter RW, Whittal ML. Dissemination of cognitive-behavioral treatments for anxiety disorders: overcoming barriers and improving patient access. Clin Psychol Rev. 2010;30(2):194–202. doi:10.1016/j.cpr.2009.11.001
33. Richter J, Pittig A, Hollandt M, Lueken U. Bridging the gaps between basic science and cognitive-behavioral treatments for anxiety disorders in routine care: current status and future demands. Zeitschrift fur Psychol/J Psychol. 2017;225(3):252–267. doi:10.1027/2151-2604/a000309
34. Robinson L, Delgadillo J, Kellett S. The dose-response effect in routinely delivered psychological therapies: a systematic review. Psychother Res. 2019;30(1):79–96. doi:10.1080/10503307.2019.1566676
35. Deacon B, Kemp JJ, Dixon LJ, Sy JT, Farrell NR, Zhang AR. Maximizing the efficacy of interoceptive exposure by optimizing inhibitory learning: a randomized controlled trial. Behav Res Ther. 2013;51(9):588–596. doi:10.1016/j.brat.2013.06.006
36. Glombiewski JA, Holzapfel S, Riecke J, et al. Exposure and CBT for chronic back pain: an RCT on differential efficacy and optimal length of treatment. J Consult Clin Psychol. 2018;86(6):533–545. doi:10.1037/ccp0000298
37. Singal AG, Higgins PDR, Waljee AK. A primer on effectiveness and efficacy trials. Clin Transl Gastroenterol. 2014. doi:10.1038/ctg.2013.13
38. Boston A, Sharpe L. The role of threat-expectancy in acute pain: effects on attentional bias, coping strategy effectiveness and response to pain. Pain. 2005;119(1–3):168–175. doi:10.1016/j.pain.2005.09.032
39. Schemer L, Schroeder A, Ørnbøl E, Glombiewski JA. Exposure and cognitive-behavioural therapy for chronic back pain: an RCT on treatment processes. Eur J Pain. 2019;23(3):526–538. doi:10.1002/ejp.1326
40. Flink IK, Boersma K, Linton SJ. Catastrophizing moderates the effect of exposure in vivo for back pain patients with pain-related fear. Eur J Pain. 2010;14(8):887–892. doi:10.1016/j.ejpain.2010.02.003
41. Edwards RR, Smith MT, Stonerock G, Haythornthwaite JA. Pain-related catastrophizing in healthy women is associated with greater temporal summation of and reduced habituation to thermal pain. Clin J Pain. 2006;22(8):730–737. doi:10.1097/01.ajp.0000210914.72794.bc
42. Edwards RR, Haythornthwaite JA, Sullivan MJ, Fillingim RB. Catastrophizing as a mediator of sex differences in pain: differential effects for daily pain versus laboratory-induced pain. Pain. 2004;111(3):335–341. doi:10.1016/j.pain.2004.07.012
43. Ruscheweyh R, Nees F, Marziniak M, Evers S, Flor H, Knecht S. Pain catastrophizing and pain-related emotions: influence of age and type of pain. Clin J Pain. 2011;27(7):578–586. doi:10.1097/AJP.0b013e31820fde1b
44. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
45. Hashmi JA, Davis KD. Women experience greater heat pain adaptation and habituation than men. Pain. 2009;145(3):350–357. doi:10.1016/j.pain.2009.07.002
46. Hashmi JA, Davis KD. Effects of temperature on heat pain adaptation and habituation in men and women. Pain. 2010;151(3):737–743. doi:10.1016/j.pain.2010.08.046
47. Robinson ME, Riley JL, Myers CD, et al. Gender role expectations of pain: relationship to sex differences in pain. J Pain. 2001;2(5):251–257. doi:10.1054/jpai.2001.24551
48. Van Damme S, Crombez G, Van Nieuwenborgh-de Wever K, Goubert L. Is distraction less effective when pain is threatening? An experimental investigation with the cold pressor task. Eur J Pain. 2008;12(1):60–67. doi:10.1016/j.ejpain.2007.03.001
49. Jackson T, Pope L, Nagasaka T, Fritch A, Iezzi T, Chen H. The impact of threatening information about pain on coping and pain tolerance. Br J Health Psychol. 2005;10(3):441–451. doi:10.1348/135910705X27587
50. Arch JJ, Twohig MP, Deacon BJ, Landy LN, Bluett EJ. The credibility of exposure therapy: does the theoretical rationale matter? Behav Res Ther. 2015;72:81–92. doi:10.1016/j.brat.2015.05.008
51. Lautenbacher S, Peters JH, Heesen M, Scheel J, Kunz M. Age changes in pain perception: a systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci Biobehav Rev. 2017;75:104–113. doi:10.1016/j.neubiorev.2017.01.039
52. Neziri AY, Scaramozzino P, Andersen OK, Dickenson AH, Arendt-Nielsen L, Curatolo M. Reference values of mechanical and thermal pain tests in a pain-free population. Eur J Pain. 2011. doi:10.1016/j.ejpain.2010.08.011
53. Rolke R, Baron R, Maier C, et al. Quantitative sensory testing in the German research network on neuropathic pain (DFNS): standardized protocol and reference values. Pain. 2006. doi:10.1016/j.pain.2006.01.041
54. Price DD. Psychological and neural mechanisms of the affective dimension of pain. Science (80-). 2000;288(5472):1769–1772. doi:10.1126/science.288.5472.1769
55. Geissner E. Verarbeitung chronischer Schmerzen - Skalen zur Erfassung der Schmerzbewältigung und der schmerzbedingten psychischen Beeinträchtigung. Z Klin Psychol Psychother. 1999;28:280–290. doi:10.1026//0084-5345.28.4.280
56. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037//1040-3590.7.4.524
57. Meyer K, Sprott H, Mannion AF. Cross-cultural adaptation, reliability, and validity of the German version of the pain catastrophizing scale. J Psychosom Res. 2008;64(5):469–478. doi:10.1016/j.jpsychores.2007.12.004
58. McCracken LM, Dhingra L. A short version of the pain anxiety symptom scale (PASS-20): preliminary development and validity. Pain Res Manag. 2002;7(1):45–50. doi:10.1155/2002/517163
59. Beck AT, Steer RA, Brown GK. BDI-Fast Screen for Medical Patients: Manual. San Antonia: Psychological Corporation; 2000.
60. Ruscheweyh R, Marziniak M, Stumpenhorst F, Reinholz J, Knecht S. Pain sensitivity can be assessed by self-rating: development and validation of the pain sensitivity questionnaire. Pain. 2009;146(1–2):65–74. doi:10.1016/j.pain.2009.06.020
61. McCracken LM. “Attention” to pain in persons with chronic pain: a behavioral approach. Behav Ther. 1997;28(2):271–284. doi:10.1016/S0005-7894(97)80047-0
62. Kircanski K, Mortazavi A, Castriotta N, et al. Challenges to the traditional exposure paradigm: variability in exposure therapy for contamination fears. J Behav Ther Exp Psychiatry. 2012;43(2):745–751. doi:10.1016/j.jbtep.2011.10.010
63. Rauch S, Foa E. Emotional processing theory (EPT) and exposure therapy for PTSD. J Contemp Psychother. 2006;36(2):61–65. doi:10.1007/s10879-006-9008-y
64. Goossens MEJB, de Kinderen RJA, Leeuw M, et al. Is exposure in vivo cost-effective for chronic low back pain? A trial-based economic evaluation. BMC Health Serv Res. 2015;15(1):549. doi:10.1186/s12913-015-1212-6
65. Crombez G, Eccleston C, Vlaeyen JWS, Vansteenwegen D, Lysens R, Eelen P. Exposure to physical movement in low back pain patients: restricted effects of generalization. Heal Psychol. 2002;21(6):573–578. doi:10.1037/0278-6133.21.6.573
66. Leeuw M, Goossens MEJBJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWSS. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94. doi:10.1007/s10865-006-9085-0
67. Doménech J, Sanchis-Alfonso V, Espejo B. Changes in catastrophizing and kinesiophobia are predictive of changes in disability and pain after treatment in patients with anterior knee pain. Knee Surgery, Sport Traumatol Arthrosc. 2014;22(10):2295–2300. doi:10.1007/s00167-014-2968-7
68. Smeets RJEM, Vlaeyen JWS, Kester ADM, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7(4):261–271. doi:10.1016/j.jpain.2005.10.011
69. Jacobi F, Höfler M, Siegert J, et al. Twelve-month prevalence, comorbidity and correlates of mental disorders in Germany: the mental health module of the german health interview and examination survey for adults (DEGS1-MH). Int J Methods Psychiatr Res. 2014;23(3):304–319. doi:10.1002/mpr.1439
70. Chambless DL, Hollon SD. Defining empirically supported therapies. J Consult Clin Psychol. 1998;66(1):7–18. doi:10.1037/0022-006X.66.1.7
71. Craske MG, Kircanski K, Zelikowsky M, Mystkowski J, Chowdhury N, Baker A. Optimizing inhibitory learning during exposure therapy. Behav Res Ther. 2008;46(1):5–27. doi:10.1016/j.brat.2007.10.003
72. Cain CK, Blouin AM, Barad M. Adrenergic transmission facilitates extinction of conditional fear in mice. Learn Mem. 2004;11(2):179–187. doi:10.1101/lm.71504
73. Bjork R, Bjork E. Optimizing treatment and instruction: implications of a new theory of disuse. Mem Soc Psychol Perspect. 2006;109–133. doi:10.4324/9780203086254
74. Hasenbring MI, Verbunt JA. Fear-avoidance and endurance-related responses to pain: new models of behavior and their consequences for clinical practice. Clin J Pain. 2010;26(9):747–753. doi:10.1097/AJP.0b013e3181e104f2
75. Vlaeyen JWS, Morley S. Cognitive-behavioral treatments for chronic pain: what works for whom? Clin J Pain. 2005;21(1):1–8. doi:10.1097/00002508-200501000-00001
76. Hamburg MA, Collins FS. The path to personalized medicine. N Engl J Med. 2010;363(4):301–304. doi:10.1056/NEJMp1006304
77. Schneider RL, Arch JJ, Wolitzky-Taylor KB. The state of personalized treatment for anxiety disorders: a systematic review of treatment moderators. Clin Psychol Rev. 2015;38:39–54. doi:10.1016/j.cpr.2015.02.004
78. De Jong JR, Vlaeyen JWS, Onghena P, Goossens MEJB, Geilen M, Mulder H. Fear of movement/(re)injury in chronic low back pain: education or exposure in vivo as mediator to fear reduction? Clin J Pain. 2005;21(1):
79. Van de Griendt JMTM, Verdellen CWJ, van Dijk MK, Verbraak MJPM. Behavioural treatment of tics: habit reversal and exposure with response prevention. Neurosci Biobehav Rev. 2013;37(6):1172–1177. doi:10.1016/j.neubiorev.2012.10.007
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.