")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
An Evaluation of the Use and Effectiveness of Case Management in Clinical Nursing Education
Authors Liang YM, Xie JY, Chen XH
Received 25 February 2021
Accepted for publication 26 July 2021
Published 27 August 2021 Volume 2021:14 Pages 3597—3603
DOI https://doi.org/10.2147/RMHP.S308144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Yu-Mei Liang,1 Jing-Yu Xie,1 Xiao-Hong Chen2
1Department of Nursing, Maoming People’s Hospital, Maoming, Guangdong Province, 525000, People’s Republic of China; 2Department of Neurosurgery, Maoming People’s Hospital, Maoming, Guangdong Province, 525000, People’s Republic of China
Correspondence: Yu-Mei Liang
Department of Nursing, Maoming People’s Hospital, No. 101 of Weimin Road, Maoming, Guangdong, 525000, People’s Republic of China
Tel +86-0668-2922648
Email [email protected]
Background: This study aims to evaluate the use and effectiveness of case management in clinical nursing education.
Methods: A sample of 181 nurses at the N3–N5 level were selected for clinical nursing education and divided into two groups using the random number method. The control group (n = 90) received traditional training, and the observation group (n = 91) received a case management model of training. The theoretical knowledge, nursing skills, training satisfaction, job stress, workplace mindfulness, career satisfaction, and job happiness of the two groups were compared. In addition, 50 patients were selected as subjects for each group, and their satisfaction with the nursing care that they received was also measured and compared.
Results: Theoretical knowledge and nursing skills scored higher in the observation group than in the control group (p < 0.05), and overall training satisfaction was higher in the observation group than in the control group (p < 0.05). After training, job stress in the observation group was lower than in the control group (p < 0.05), while workplace mindfulness, career satisfaction, and job happiness were higher in the observation group than in the control group (p < 0.05). In terms of nursing quality, on all indicators, the observation group scored higher than the control group (p < 0.05), and the patients’ nursing satisfaction scores were higher in the observation group than in the control group (p < 0.05).
Conclusion: Case management can improve the professionalism and overall skills of nurses at the N3–N5 levels. It is conducive to reducing job stress, enhancing workplace mindfulness, improving career satisfaction and job happiness, and improving the quality of nursing, thereby providing patients with better nursing care.
Keywords: clinical nursing, nursing education, case management, nursing quality management, application evaluation
Introduction
Clinical nursing competence refers to the ability of nurses to provide holistic care to their patients by mastering nursing techniques. Clinical nursing education is considered one of the important ways to improve the level of professionalism of nurses, and it has a significant impact on their preparation for the nursing profession.1,2 An important issue that needs to be addressed in current nursing training programs is how to provide a good clinical education. The decentralization of treatment and the increase in the complexity of cases and available services led to the birth of the case management model in 1960.3 The American Academy of Nursing defined case management as a dynamic, systematic, and collaborative approach to the provision and coordination of health resources for specific populations.4 There is a link between the role of case management and care management, so while they have different taxonomies, both of them are connected with the same model, which goes by the name of case care management,5 and in the context of this study, they will go by the name “case care.” Case care explores the individual characteristics and common patterns of disease in healthcare. Various guidelines show that in order to improve case care, it is important for nurses to gather information concerning their nursing cases and not just use the information collected by doctors.6 In other words, nurses play a central role in taking charge of patients as they act as a link between the hospital and the territory.7
The basic functions of a nursing case manager include identifying target populations, carrying out individual assessment and evaluation, engaging in health resource assessment and planning, providing health services, coordinating health resources, acting as a supervisor, and advocating for case management to ensure the effective implementation of the entire process.8 Therefore, proper training in case management in clinical education can contribute to improving the integrative, clinical-thinking, and evidence-based skills of the nursing staff. The case management system was officially adopted into clinical nursing education in our hospital in July 2019 and has achieved good results, which are reported on in this paper.
Materials and Methods
Research Subjects
The theoretical basis of the American hierarchical management system was put forward by Dr. Patricia Benner, from the University of California, San Francisco School of Nursing, in 1984. She described a “novice to expert” nursing career development model, divided into 5 developmental stages, namely novice, advanced beginner, competent, proficient, and expert nurse. This model was widely recognized by nurses and nursing scholars and eventually became the theoretical basis of most hospital-level management systems.9
China’s “Guidelines for the Construction of Professional Nurses’ Core Competence” were put forward in 2009. This competence was based on the ability to master a ward setting and implement its management, the ability to care for critically ill patients, the ability to master and use specialized technology, and the acquisition of educational training and scientific research capabilities. Professional nursing was classified into 6 levels, N0, N1, N2, N3, N4, and N5, representing individual positions, ranks, and abilities, and their progressive relationships. In this study, N3 level nurses refer to junior nurses with more than 5 years’ experience or senior nurses with less than 5 years’ experience. N4 level nurses refer to supervisor nurses who have been working for more than 5 years and hold a bachelor’s degree or professional nurses who have a bachelor’s degree and have been working for more than 5 years. N5 nurses refer to chief nurses or co-chief nurses, head nurses, or specialist nurses with a bachelor’s degree. It can be seen that the level increases gradually from N3–N5 with professional maturity and the development of their nursing skills.10
The present study was approved by the Medical Ethics Committee. This study was conducted in accordance with the Declaration of Helsinki and the nurses and patients gave informed consent. Since there were 181 N3–N5 nurses in Maoming People’s Hospital in Guangdong in 2019, all of them were included in the study cohort. Ninety nurses at the N3–N5 levels were selected as subjects in the control stage of the study (the control group) between January and June 2019. Another 91 nurses at the N3–N5 levels were selected between July and December 2019 as subjects in the observation stage of the study (the observation group). As for the patients, 10 of them were selected in the pre-experiment stage, 5 in the control group and 5 in the observed group, to obtain the following parameters: μ1 = 85.88, μ2 = 90.6, and б = 6.19. Based on α = 0.5 and actual power = 0.95, a sample size of 90 patients was calculated using Pass 15 software. Taking the 10% shedding rate into account, the final sample size was 100 patients, who were equally divided into two groups. Thus, a total of 50 patients were selected as the nursing subjects for each of the two stages. The random process was performed in the following way: random numbers were generated by a dedicated person using SPSS software, and the patients were randomly divided into two groups, the experimental group and the control group, in a ratio of 1:1.
The inclusion and exclusion criteria for nurses and patients were as follows: (1) The nurses were recruited from Maoming People’s Hospital, based on the following criteria: they were at N3, N4, or N5 level; they had passed basic theory and practical examinations; they had college level degrees or above; and they were willing to participate in the clinical studies and promised not to drop out. The participants were assigned to the control or observation group by the investigators using the random numbers method. (2) Of the patients who were interested in participating in the study, only those that met the following criteria were recruited: they were 18 years of age or older; they received care from two groups of nurses; they had no serious underlying disease, such as advanced cancer or severe cardiopulmonary failure; they had no history of long-term use of psychotropic drugs; and they were able to perform activities of daily living unaided.
Methods
The traditional training method was used for the clinical nursing education of the control group and involved lectures, working in different hospital departments, and self-study.
The observation group received training interventions five times in total, lasting twenty-two minutes each time, and the case management model was used for clinical nursing education, with the establishment of an information platform for the whole-process case management practice. This allowed for the sharing of information centered on risk factors, complications, rehabilitation, discharge preparation plans, and nurse–patient communication. The characteristics of case management are that each case involves the overall diagnosis and treatment, nursing coordination, and quality supervision. The nurses were able to participate in case management learning, which meant they increased their knowledge, enhanced their team collaboration capabilities, and clarified the role of a nurse at each level. With the identification of the case management target, the nurses could conduct a comprehensive assessment of the patient and establish a health file and case assessment sheet. The medical and nursing team worked together to develop a nursing treatment plan, then formed a nursing plan for case management, and followed up on the case management target throughout the process by querying and collecting information and organizing data. This was followed by an evaluation of the teaching effect and feedback. Nursing reports were compiled monthly, with a wide range of data being uploaded to the information platform to enable resource sharing. Nurses at each level were able to improve on and optimize the practical tools and processes of case management, and active learning and thinking was encouraged.
Observation Indicators
The observation indicators were measured twice and then compared before and after the interventions. A comparison was made of the theoretical knowledge and nursing skills of the two groups of nurses. The content of the assessment included theoretical knowledge, basic nursing skills, and specialized nursing skills, and it took the form of a paper assessment, which was self-produced (made by Xiaohong Chen), with scores of 0–100 on the paper. The higher the score was, the greater the mastery of theoretical knowledge. The practical assessment was conducted by assessing basic and specialized nursing skills performed on a dummy model, which were scored jointly by experts from the nursing department of the hospital. The final score for the individual assessment was calculated as the sum of the scores from each of the scoring experts divided by the number of experts, expressed as a percentage, ie, the final score ranged from 0 to 100; the higher the score, the better the mastery of practical nursing skills. The training satisfaction of the two groups of nurses was evaluated using a self-produced questionnaire. The total score on the questionnaire was 100 points, and the degree of training satisfaction was divided into very satisfied (81–100 points), generally satisfied (60–80 points), and dissatisfied (0–59 points). The overall satisfaction rate was expressed as a percentage of the sums of “very satisfied” and “generally satisfied.” Job stress was compared using a stress response scale, the “Chinese nurse stressor scale”, developed by Jingping Zhang, with a score range of 0–10 points. A high score indicated that the nurse experienced a great deal of stress at work. Workplace mindfulness was assessed and compared using a workplace mindfulness scale developed by Erik Dane in 2013. This tool uses a Likert five-point scale, with the score being positively correlated with workplace mindfulness. The Minnesota Job Satisfaction Questionnaire was used to evaluate career satisfaction, with a total score of 100 points; the higher the score, the more satisfied the nurses were in their job. With regard to job happiness, the SD scale of Happiness was used in the evaluation, with a score range of 37–185 points; the higher the score, the greater the nurse’s happiness at work. Finally, the quality of nursing was measured in terms of service attitude, communication skills, night rounds, health education, and nursing documents, and these were scored by the expert evaluation team organized by the nursing department of the hospital. The score range was 0–100 points. The final score was calculated as the sum of the scores given by each expert divided by the number of experts and expressed as a percentage; the higher the score, the better the quality of nursing. All of the above indicators were measured by the research team.
Patient satisfaction with nursing care in the two stages of the study was scored by the patients and compared with the nursing scores. The scoring was expressed as a percentage, and a higher score indicated greater satisfaction.
Statistical Analysis
SPSS 26.0 software was used to perform the statistical analysis. The countable data were expressed as numbers (n) and tested by the χ2 test. The measurement data were expressed as ( ). Two independent sample t-tests were used for the comparison between the two groups. A p-value < 0.05 was considered statistically significant.
). Two independent sample t-tests were used for the comparison between the two groups. A p-value < 0.05 was considered statistically significant.
Results
General Data
The control group consisted of female nurses aged 28–47 years old, with an average age of (37.15 ± 4.63) years old, and comprised 39 grade N3, 35 grade N4, and 16 grade N5 nurses. The observation group consisted of female nurses aged 28–48 years old, with an average age of (37.39 ± 4.52) years old, and included 41 grade N3, 34 grade N4, and 16 grade N5 nurses.
A total of 50 patients were randomly selected in each of the two stages for satisfaction evaluation. They all received the care of nurses from both groups. The control group patients consisted of 27 males and 23 females aged 27–81 years old, with an average age of (54.18 ± 12.65) years old. The observation group patients consisted of 26 males and 24 females aged 26–82 years old, with an average age of (54.47 ± 12.53) years old. There was no statistically significant difference between the two stages in the general characteristics of the nurses and patients (p > 0.05), and the data were comparable.
The Comparison of Theoretical Knowledge and Practical Nursing Skills Assessment
The theoretical knowledge, basic nursing skills, and specialized nursing skills assessment scores were higher in the observation group than in the control group (p < 0.05), as shown in Table 1.
 |
Table 1 Comparison of the Theoretical Knowledge and Nursing Skills Assessment Between Two Groups of Nurses ( |

The Comparison of Training Satisfaction
The overall training satisfaction rate was 100% in the observation group, which was higher than that of the control group (p < 0.05), as shown in Table 2.
 |
Table 2 Comparison of Training Satisfaction Between Two Groups of Nurses [n(%)] |
The Comparison of Job Stress Scores, Workplace Mindfulness Scores, Career Satisfaction Scores, and Job Happiness Indexes
The job stress score, workplace mindfulness score, career satisfaction score, and job happiness index had improved after training for both groups of nurses (p < 0.05). However, after training, the job stress score was lower in the observation group than in the control group (p < 0.05), and the workplace mindfulness score, career satisfaction score, and job happiness index were higher in the observation group than in the control group (p < 0.05), as shown in Table 3.
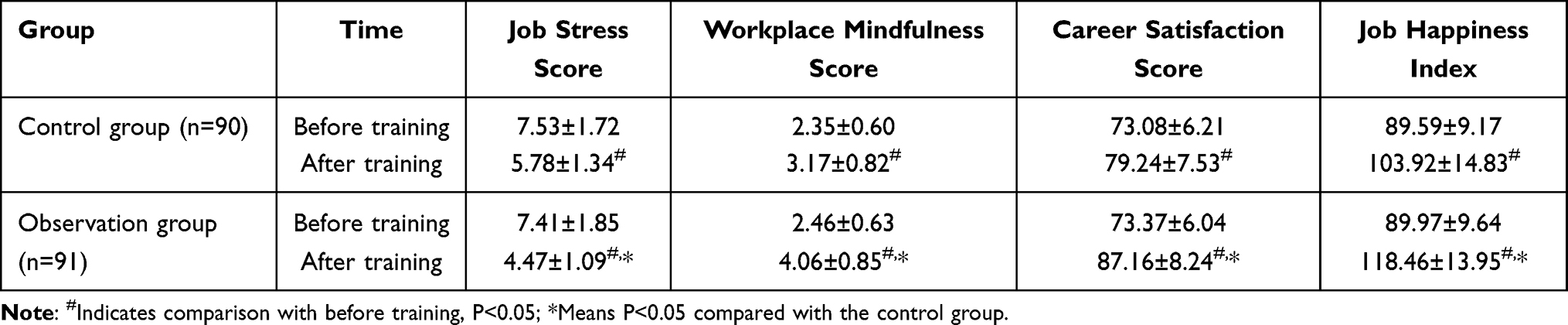 |
Table 3 Comparison of the Job Stress Score, Workplace Mindfulness Score, Career Satisfaction Score, and Job Happiness Index Between the Two Groups of Nurses ( |

The Comparison of Nursing Quality Scores
The observation group had higher nursing quality scores than the control group in terms of service attitude, communication skills, night rounds, health education, and nursing documents (p < 0.05), as shown in Table 4.
 |
Table 4 Comparison of the Nursing Quality Scores Between Two Groups of Nurses ( |

The Comparison of Nursing Satisfaction
The patient satisfaction scores for practical nursing skills, nursing attitude, health education, demand satisfaction, and nursing initiative were higher for the observation group than for the control group (p < 0.05), as shown in Table 5.
 |
Table 5 Comparison of the Nursing Satisfaction Between Two Groups of Patients ( |

Discussion
The case management model is a new model in use in China that refers to a method of healthcare for certain types of disease. It involves disease assessment, nursing care, and follow-up, for example, and is aimed at providing medical services for a specific patient population that is an extension of in-hospital care services, since it is an integrated method of care that differs from the traditional fragmented care system.11 We have been tracking and commissioning the case management system since April 2019 and officially put the case management system into use in clinical care in July 2019. The application of the present system enables real-time sharing of nursing case resources throughout the hospital and facilitates timely access to information, which helps to ensure barrier-free access to nursing case resources and an understanding of the individualized needs of the patients, thus improving the anticipatory thinking in nurses and enabling them to better engage in nursing care and provide more attentive care for patients, which is consistent with the results of several studies.12–14
With the reform of the medical system and the continuous updating of medical information, nurses can continue to learn and improve their theoretical knowledge and practical nursing skills.15–17 To improve the level of professionalism in nurses, it is also important to organize regular professional training, through which they can constantly update their knowledge reserves and learn new nursing concepts and tools and improve the quality of their nursing care.18 Previous training methods were stereotypical and lacked relevance, resulting in nurses’ professional abilities not being substantially improved after undergoing training.19–21
Training that exploits the case management model is more targeted and can encourage nurses’ interest in learning, stimulate their initiative, and cultivate critical thinking, teamwork skills, writing skills, language communication skills, and computer skills. It enables nurses to carry out their work more efficiently, reduces the pressure they face, and improves the overall quality of nursing. It also allows nurses to gain a sense of professional value from their work, which was absent in the past.
The case management model can also indirectly improve patients’ evaluation of nursing care. Nurses have access to clinically-based and evidence-based medical evidence and can thus provide patients with more considered nursing care. They can assess the individual needs of patients and make diagnoses and nursing intervention plans, which can promote the one-to-one relationship between nurses and patients, so that patient satisfaction is greater. In addition, case management requires nurses to conduct a comprehensive evaluation of patients rather than just deliver a single intervention, ensuring a continuous process of care for patients from hospital to home. In general, effective case management enables patients to understand and obtain high-quality and efficient medical care,22,23 and it also provides an effective, efficient, and economical care strategy for nurses, which has a significant positive impact on the nursing profession.24
Limitations
The application of case management in clinical nursing education is often affected by the case management system and equipment, case design and content, the number of nurses, and the quality of the nurses. The participants in this study were selected from one third-grade class-A hospital, which may have affected the outcomes. Future research should therefore involve a range of hospitals.
Conclusion
The use of case management in clinical nursing education can improve the professionalism and overall abilities of nurses at the N3–N5 level, help to reduce the stress of nursing, and increase workplace mindfulness, career satisfaction, and job happiness. It can also improve the quality of nursing and patient care and help to ensure that patients are more satisfied with the nursing care they receive.
Funding
This study was funded by Science and Technology Plan Project of Maoming City (Maokezi [2019]47 No.190404191701118), and High-level Hospital Construction Research Project of Maoming People's Hospital. The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cho E, Sloane DM, Kim EY, et al. Effects of nurse staffing, work environments, and education on patient mortality: an observational study. Int J Nurs Stud. 2015;52(2):535–542. doi:10.1016/j.ijnurstu.2014.08.006
2. Forber J, DiGiacomo M, Carter B, Davidson P, Philips J, Jackson D. In pursuit of an optimal model of undergraduate nurse clinical education: an integrative review. Nurse Educ Pract. 2016;21:83–92. doi:10.1016/j.nepr.2016.09.007
3. Lukersmith MS, Millington M, Salvador-Carulla L. What is case management? A scoping and mapping review. J Integr Care. 2016;16(4):2. doi:10.5334/ijic.2477
4. Soares LG, Higarashi IH. Case management as a high-risk prenatal care strategy. Rev Bras Enferm. 2019;72(3):692–699. doi:10.1590/0034-7167-2018-0483
5. Bertuol M, Di Niro V, Tagliabue C, et al. The process of developing the professional identity of the nurse case care manager: a grounded theory study. Acta Biomed. 2020 Jun 20;91(6-S):19–27. doi:10.23750/abm.v91i6-S.10019
6. Joo JY, Liu MF. Effectiveness of nurse-led case management in cancer care: systematic review. Clin Nurs Res. 2019;28(8):968–991. doi:10.1177/1054773818773285
7. Foà C, Bertuol M, Deiana L, Rossi S, Sarli L, Artioli G. The Case/Care Manager in Eating Disorders: the nurse's role and responsibilities. Acta Biomed. 2019;90(11-S):17–28. doi:10.23750/abm.v90i11-S.8989
8. Lambert AS, Legrand C, Ces S, Van Durme T, Macq J. Evaluating case management as a complex intervention: lessons for the future. PLoS One. 2019;14(10):e0224286. doi:10.1371/journal.pone.0224286
9. Benner P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice. Menlo Park, CA: Addison-Wesley; 1984:30–58.
10. Jian B. Study on Constructing a Hierarchical Training System for Nurses in a Third Class a Hospital in Inner Mongolia Based on GROW Model. Hohhot: Inner Mongolia Medical University; 2019.
11. Klein NJ, Evans-Agnew R. Flying by the seat of their pants: a grounded theory of school nurse case management. J Adv Nurs. 2019;75(12):3677–3688. doi:10.1111/jan.14204
12. Joo JY, Liu MF. Experiences of case management with chronic illnesses: a qualitative systematic review. Int Nurs Rev. 2018;65(1):102–113. doi:10.1111/inr.12429
13. Joo JY, Liu MF. Case management effectiveness for managing chronic illnesses in Korea: a systematic review. Int Nurs Rev. 2019;66(1):30–42. doi:10.1111/inr.12472
14. Chastonay OJ, Lemoine M, Grazioli VS, et al. Health care providers’ perception of the frequent emergency department user issue and of targeted case management interventions: a cross-sectional national survey in Switzerland. BMC Emerg Med. 2021;21(1):4. doi:10.1186/s12873-020-00397-w
15. Visser A, Bos WC, Prins JB, Hoogerbrugge N, van Laarhoven HW. Breast self-examination education for BRCA mutation carriers by clinical nurse specialists. Clin Nurse Spec. 2015;29(3):E1–E7. doi:10.1097/NUR.0000000000000118
16. Bjerkvik LK, Hilli Y. Reflective writing in undergraduate clinical nursing education: a literature review. Nurse Educ Pract. 2019;35:32–41. doi:10.1016/j.nepr.2018.11.013
17. Chen B, Wang Y, Xiao L, et al. Effects of mobile learning for nursing students in clinical education: a meta-analysis. Nurse Educ Today. 2020;97:104706. doi:10.1016/j.nedt.2020.104706
18. Taylor V, Ashelford S, Fell P, Goacher PJ. Biosciences in nurse education: is the curriculum fit for practice? Lecturers’ views and recommendations from across the UK. J Clin Nurs. 2015;24(19–20):2797–2806. doi:10.1111/jocn.12880
19. McCutcheon K, Lohan M, Traynor M, Martin D. A systematic review evaluating the impact of online or blended learning vs. face-to-face learning of clinical skills in undergraduate nurse education. J Adv Nurs. 2015;71(2):255–270. doi:10.1111/jan.12509
20. Jensen KT, Knutstad U, Fawcett TN. The challenge of the biosciences in nurse education: a literature review. J Clin Nurs. 2018;27(9–10):1793–1802. doi:10.1111/jocn.14358
21. Shen H, Wang H, Yan L, et al. Incivility in nursing practice education in the operating room. Nurse Educ Today. 2020;88:104366. doi:10.1016/j.nedt.2020.104366
22. Gray L, Klein N, Meuret C, Nelson L, Stahlnecker L. Care coordination: a principle of 21st century school nursing practice with a focus on case management. NASN Sch Nurse. 2020;35(4):219–223. doi:10.1177/1942602X20928345
23. Joo JY, Huber DL. Scoping review of nursing case management in the United States. Clin Nurs Res. 2018;27(8):1002–1016. doi:10.1177/1054773817717861
24. Stark P. Advancing complex case management competencies in a health care system. Prof Case Manag. 2020;25(1):19–25. doi:10.1097/NCM.0000000000000361
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.