")
Back to Journals » Patient Preference and Adherence » Volume 16
An Assessment of the Knowledge and Practices of Adults in Jazan, Saudi Arabia, Concerning Routine Medical Checkups
Authors Gosadi IM , Ayoub RA, Albrahim HT, Alhakami MS, Ageely EH, Alwadani RS, Shayani HM, Shteafi SA
Received 26 May 2022
Accepted for publication 29 July 2022
Published 5 August 2022 Volume 2022:16 Pages 1955—1969
DOI https://doi.org/10.2147/PPA.S376345
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ibrahim M Gosadi,1 Raum A Ayoub,2 Hakemah T Albrahim,2 Manar S Alhakami,2 Eilaf H Ageely,2 Rawiyah S Alwadani,2 Halah M Shayani,2 Salma A Shteafi2
1Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Faculty of Medicine, Jazan University, Jazan, Saudi Arabia
Correspondence: Ibrahim M Gosadi, Department of Family and Community Medicine, Faculty of Medicine, Jazan University, P.O. Box: 2349, Jazan, 82621, Saudi Arabia, Tel +966 562137711, Email [email protected]
Purpose: This study aims to measure the knowledge and practices of adults in the Jazan region of Saudi Arabia concerning routine medical checkups.
Methods: This study used a cross-sectional design that targeted adults in the Jazan region of Saudi Arabia. The data was collected via self-administered questionnaires, with participants being approached in online settings. The questionnaires measured participant demographics, knowledge, and practice of routine medical checkups as well as their response to the Know Your Numbers campaign services initiative from the Saudi Ministry of Health. A chi-square test was used to detect statistically significant differences between the levels of knowledge and practice according to the measured demographic characteristics.
Results: A total of 516 persons participated in this study. The mean age of the participants was 25 years; 54.7% were female. The median level of knowledge was 3 (out of 9), varying between 0 and 9. The recruited sample exhibited average knowledge of parameters used to classify levels of blood glucose, blood pressure, body mass index, and blood lipids, but low knowledge regarding the recommended age to begin screening for several chronic diseases. Factors associated with levels of knowledge were gender, age, education level, and employment (p value < 0.05). However, a history of chronic disease was the only factor associated with the practice of routine medical checkups (p value 0.023). Finally, less than 5% of this sample reported their participation in the Know Your Numbers campaign.
Conclusion: Attending routine medical checkups is uncommon and only motivated by the existence of a diagnosed medical condition. Furthermore, this study found low utilization of the Know Your Numbers campaign services. This suggests a need for greater emphasis on increasing awareness of routine medical checkups among adults in the Jazan region.
Keywords: medical knowledge, practice, routine, checkup, chronic diseases, screening, Jazan, Saudi Arabia
Introduction
Routine medical checkups have primary, secondary, and tertiary preventive potential, aiming to promote health and detect chronic diseases early in life. Chronic diseases can have a negative impact on the well-being of individuals and influence their overall quality of life if the symptoms are not controlled. Routine medical checkups, including clinical and laboratory indicators, are performed in order to identify those at risk or in early stages of the disease, as well as to ensure appropriate application of primary or secondary prevention measures towards reducing the morbidity and mortality of chronic conditions.1
Saudi Arabia is among the developing countries witnessing a rise of chronic non-communicable diseases—particularly metabolic syndrome, a combination of obesity, diabetes, hypertension, and hypercholesterolemia.2 It has been suggested that the increasing rate of metabolic syndrome in Saudi Arabia is due to the high prevalence of contributing environmental and genetic factors.3 Also of note are the most frequently reported types of cancer in Saudi Arabia: breast cancer among females and colon cancer among males.4 Furthermore, there is low utilization of screening services for early detection of cancer, including breast and colon cancer, in Saudi Arabia.5
The increase in chronic conditions in Saudi Arabia can be associated with a high disease burden. According to the Saudi Arabia 1999–2017 report, which is based on the Global Burden of Disease Study 2017, cardiovascular diseases ranked first as a cause of disability-adjusted life years in 2017. Furthermore, neoplasm was reported as one of the conditions that increased years lived with disability in the period between 1990 and 2017. Although the influence of transport-related injuries on disability-adjusted life years has decreased in Saudi Arabia, the influence of metabolic and behavioral risk factors remains a constant contributor to years lived with disability.6
The incidence of chronic conditions in Saudi Arabia is influenced by several non-modifiable and behavioral risk factors identified in the Saudi community. The World Health Survey—Saudi Arabia, which was carried out in 2019 and involved a sample of 9339 participants from all governmental regions of the country, reported a high prevalence of physical inactivity and unhealthy diet habits. Of the respondents, 80% reported insufficient physical activity levels and 93% reported insufficient consumption of fruits and vegetables.7 This suggests a high prevalence of behavioral risk factors for chronic diseases, especially with aging adults in the country. The increasing incidence of chronic diseases and their contributing factors demonstrate the importance of routine medical checkups among the Saudi population.
A study by Al-Kahil et al conducted on 414 participants of both genders aged 36 and over in Riyadh reported that most participants (67.5%) did not perform routine medical checkups despite being aware of their importance. Health concerns were the most common factor influencing this practice, the second being lack of time and laziness.8 A similar study conducted by Eke et al aimed to record knowledge and attitudes to routine medical checkups in southeastern Nigeria. The study included 323 participants of both genders, aged 15–65. The majority of respondents (74.9%) were aware of the importance of regular medical checkups. General examination was the most prevalent type of medical checkup (60.7%), followed by blood pressure measurement (55.4%). The use of routine medical checkups differed between genders: 39.4% of females performed routine medical checkups, in comparison to 29.4% of males. The practice of periodic medical checkups among their sample was unaffected by age, gender, or educational background.9 Furthermore, in another Nigerian study that targeted the use of routine medical checkups among healthcare workers, it was noted that although 295 participants (92.8%) had high levels of knowledge, only 147 (46%) practiced routine medical checkups.10
The current literature suggests that local and international communities have an appropriate level of knowledge concerning the importance of routine medical checkups, but a low practice of such. This demonstrates the importance of raising awareness and providing the necessary infrastructure to encourage adult individuals to perform routine medical checkups. One of the recent efforts by the Saudi Ministry of Health (MoH) was the establishment of the Know Your Numbers campaign. This nation-wide campaign was established in November 2021 and encourages adults to measure their blood sugar, blood pressure, waist circumference, and body mass index (BMI) using official Ministry of Health applications such as the Sehhaty app.11
Studies measuring awareness and practice of routine medical checkups in Saudi Arabia are limited, and the number of people using the health services provided by the Know Your Numbers campaign is currently unknown. The main objectives of this study are to measure the awareness and practice of routine medical checkups of adults in Jazan, to investigate factors associated with knowledge and practice of routine medical checkups of adults in Jazan, and to assess the utilization of health services provided by the Know Your Numbers campaign in Jazan, Saudi Arabia.
Methods
Study Setting and Context
This study was a cross-sectional investigation conducted from March to April 2022. The data was collected in online settings from targeted adult individuals living in the Jazan region of Saudi Arabia. Ethical approval to conduct the study was granted by the Standing Research Committee of Jazan University (approval number REC-43/05/093, dated December 2021). Subjects were recruited after securing their informed consent, and the study was performed in accordance with the Declaration of Helsinki.
Data Collection Tool
A questionnaire was developed to measure the levels of knowledge of and adherence to recommended routine medical checkups. The contents of the questionnaire were retrieved from the guidelines of several health education resources related to the prevention and management of chronic non-communicable diseases. These guidelines include Health Tools by the Saudi MoH for BMI12 and waist circumference,13 the Saudi Hypertension Management Guidelines,14 the Saudi Diabetes Clinical Practice Guidelines,15 and Saudi MoH projects for the screening of breast cancer,16 colon cancer,17 and osteoporosis.18 Sections pertaining to the assessment of cardiac risk, anxiety, and depression were adopted from the Saudi Guide to the Promotion of Family Medicine Curriculum in Primary Healthcare Centers.19
The questionnaire consists of three main components: demographics of the participants, measurement of knowledge of routine medical checkups, and practice of routine medical checkups, including the Know Your Numbers campaign. The content of the questionnaire was reviewed by a consultant in public health and trialed on a sample of ten participants to test its validity and comprehensiveness in measuring knowledge and practices. Detailed descriptions of items used to measure the demographics, history of chronic diseases, knowledge and practices of the participants are provided in Tables 1-4. Finally, the last section of the questionnaire measured variables related to participants’ awareness and utilization of the Know Your Numbers campaign, including being aware of the campaign, where they learned about the campaign, and performing the measurements.
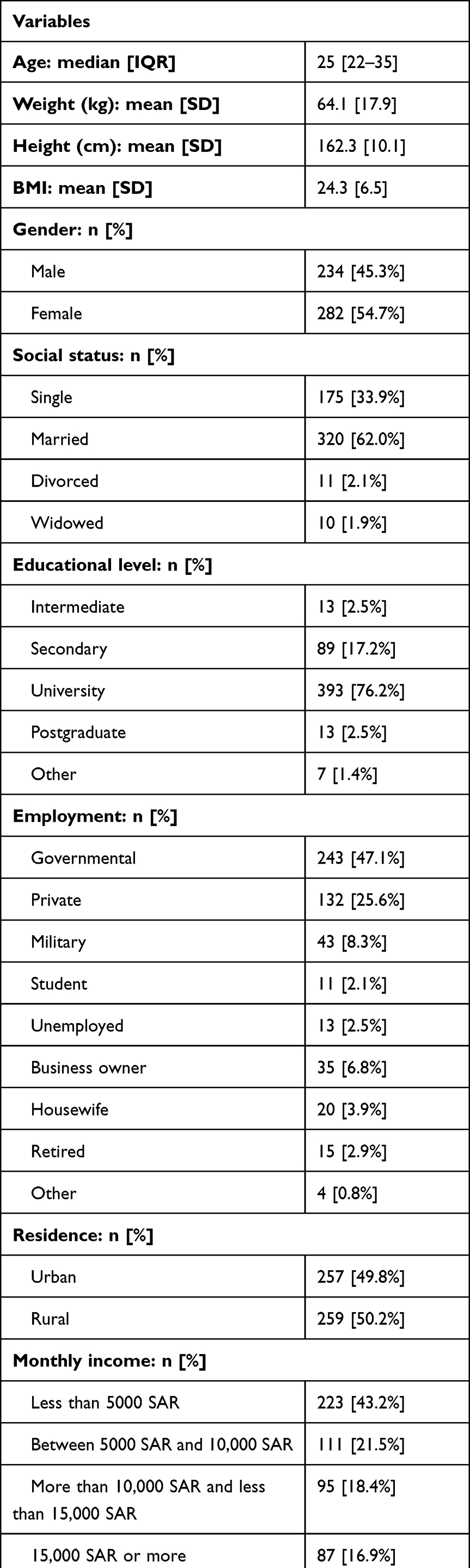 |
Table 1 Sociodemographic Characteristics of a Sample of 516 Participants from Jazan, Saudi Arabia |
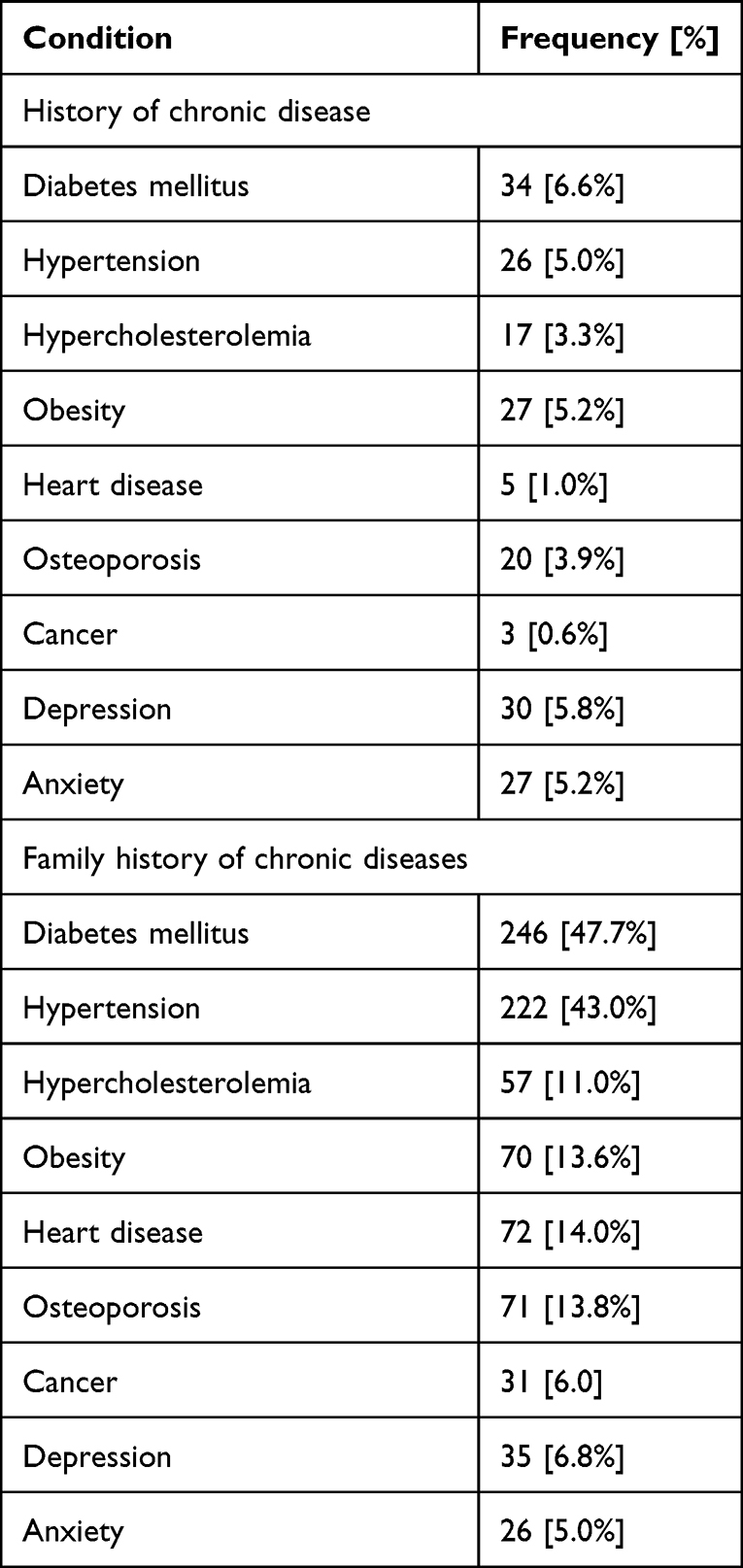 |
Table 2 Personal and Family History of Chronic Disease Among a Sample of 516 Subjects from Jazan, Saudi Arabia, and Family Chronic Disease History |
 |
Table 3 Knowledge Levels of 516 Adults from Jazan, Saudi Arabia, Concerning Routine Medical Checkups |
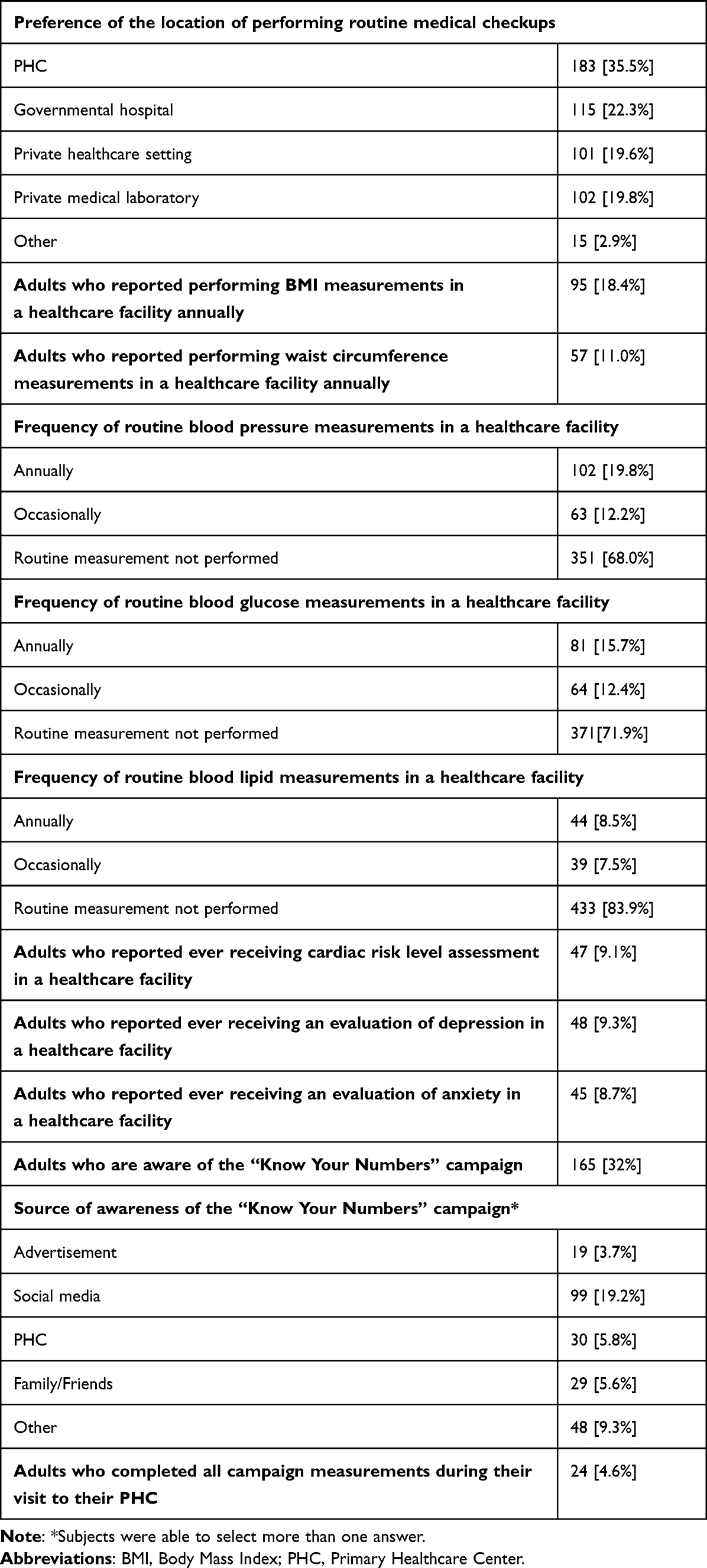 |
Table 4 The Practices of 516 Adults from Jazan, Saudi Arabia, Concerning Routine Medical Checkups and Awareness and Utilization of the “Know Your Numbers” Campaign |
Data Collection Process
This investigation targeted adults in the Jazan region in southwestern Saudi Arabia. The data was collected through self-administered, semi-structured questionnaires. The questionnaires were anonymous and did not require the names or personal information of the participants. A web link was generated to facilitate distribution of the questionnaire to the targeted population. The generated link enabled the targeted participants to access and complete the questionnaire. Social media was used to promote the existence of the link in order to reach the target population. For example, the researcher promoted the generated link via the WhatsApp status function and WhatsApp groups. Participants who completed their survey were asked to share the link with acquaintances to facilitate reaching the required sample size.
Sample Size Calculation and Targeted Population
Convenient, non-random snowball sampling was used to reach the required sample size. The number of subjects required for an adequate sample was estimated using the StatCalc component of the Epi Info software. A study by Al-Kahil et al investigated the knowledge and practice of routine medical checkups in Riyadh,8 finding that 69.57% of the participants had appropriate knowledge of routine medical checkups. With a prevalence of 69.57%, a confidence level of 95%, and a 5% margin of error, the required sample size was estimated to be 325 participants.
Data Analysis
The Statistical Package for the Social Sciences software (version 21) was used to analyze the data. Proportions and frequencies were used to summarize binary and categorical variables. Means and standard deviations were used to summarize normally distributed continuous variables, and medians and the interquartile range were used to summarize skewed data. A chi-square test was used to test the differences between levels of knowledge or practice concerning routine medical checkups according to the sample’s demographics. To enable comparison between demographic characteristics, personal and family history of chronic diseases were grouped into having a personal or family history of a disease or not; age was grouped using the median as a cutoff point, into being over 25 or 25 and under; BMI was grouped with 25 as a cutoff point; marital status was grouped as being either married or not; education level was grouped as having university education or lower; employment was grouped as having governmental, private, or military employment or other employment status (including student, housewife, business owner, retiree, unemployed); monthly income was grouped using 10,000 SAR as a cutoff point.
Knowledge was scored by giving one point for each correct answer. Knowledge of routine medical checkups was grouped into higher and lower levels of knowledge, using median knowledge as a cutoff point. Finally, practice of routine medical checkups was grouped into having performed a minimum of one measurement or assessment in the previous three years or not having performed any. A p value of less than 0.05 was presumed to be statistically significant for the applied statistical test.
Results
A total of 516 people participated in this investigation. The total number of participants exceeded the estimated number due to snowballing sampling and promotion of the questionnaire via social media. Table 1 describes the demographic characteristics of the included sample. The median age of the participants was 25, and the mean BMI was 24.3. More than half of the participants were female (282). The majority of respondents had a university education (76.2%), were government employees (47.1%), reported a monthly income of less than 5000 SAR (43.2%), and had never smoked (54.3%). Participants’ areas of residency were equally distributed across rural and urban areas.
Table 2 presents the participants’ personal and family histories of chronic diseases. The most frequently diagnosed condition among the study sample was diabetes (6.6%), followed by depression (5.8%). The least frequently diagnosed chronic condition was cancer (3 participants). The most frequently reported conditions in participants’ family histories were diabetes (47.7%) and hypertension (43.0%), while the least frequently reported was anxiety (5%).
Table 3 illustrates participants’ knowledge regarding periodical checkups. The median level of knowledge was 3 (out of 9), varying between 0 and 9. The proportion of respondents who correctly answered items measuring knowledge of BMI was relatively higher than those who correctly answered items measuring knowledge of waist circumference. The frequency of adults who reported correct answers to items measuring knowledge of blood glucose was higher compared to items measuring knowledge of blood pressure (44.0% vs 32.6%). Finally, when participants were asked about the recommended age to begin screening for chronic conditions, nearly 40% knew the recommended age to begin measuring blood glucose, while a low proportion knew the correct ages to begin colon cancer and breast cancer screening.
Table 4 describes participants’ practices concerning routine medical checkups and awareness and utilization of the Know Your Numbers campaign. There were 183 (35.5%) participants who preferred to perform routine medical examinations in primary healthcare, while 115 (22.3%) preferred to perform them in government hospitals. When the participants were asked whether they perform BMI and waist circumference measurements on an annual basis, only 18.4% and 11.0% reported measurements of BMI and waist circumference, respectively. When asked how frequently they perform routine measurements of blood pressure, blood glucose, and blood lipids, the majority reported not performing any routine measurements for all three parameters. Less than 10% of the participants reported ever receiving cardiac risk level, depression, or anxiety assessments.
The findings concerning the Know Your Numbers campaign suggest low awareness and participation levels in the Jazan region. Nearly one third of the sample reported being aware of the Know Your Numbers campaign, with the main source of awareness being social media. Only 5.8% of the participants reported having heard of the campaign from their primary healthcare center (PHC), and only 24 (less than 5%) adults reported taking measurements as part of the campaign.
Table 5 displays levels of knowledge and practices concerning routine medical checkups according to the measured characteristics. The differences of knowledge levels were statistically significant according to gender, age, education level, and employment (p value > 0.05). The proportions of participants with higher levels of knowledge about routine medical checkups were higher among males in comparison to females, those who are younger than 25 in comparison to those who are older, those with university education in comparison to those with lower education levels, and those who are employed in the governmental, private, or military sector in comparison to those with other employment conditions. However, assessment of the distribution of levels of practice according to the measured factors revealed that a history of a diagnosed chronic condition was the only factor associated with performing a minimum or one measurement or assessment. (p value 0.023).
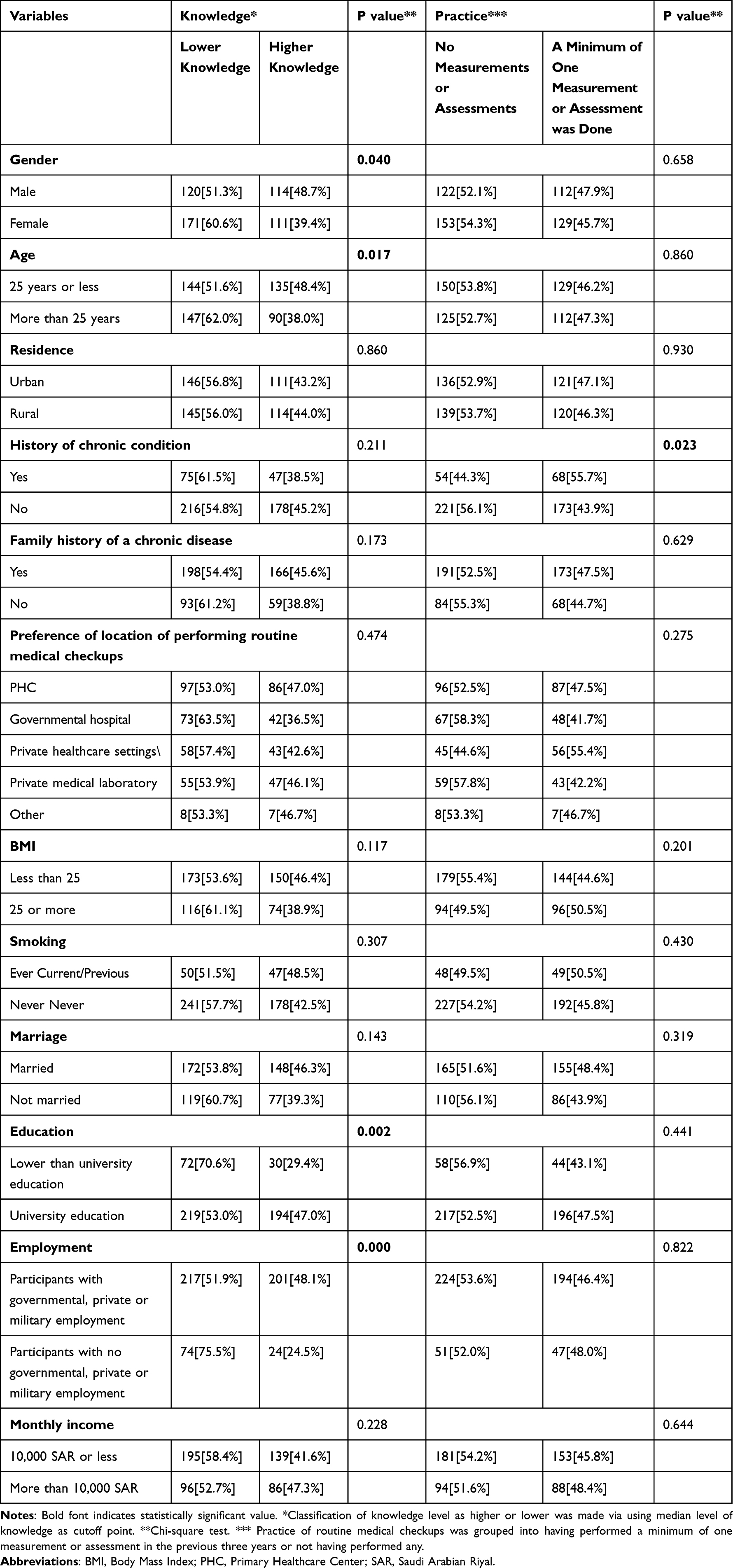 |
Table 5 Demographic Factor Distribution According to Levels of Knowledge of Routine Medical Checkups and Frequency of Routine Medical Checkups Among 516 Adults from Jazan, Saudi Arabia |
Discussion
This investigation was a cross-sectional study that targeted adults in Jazan, Saudi Arabia, to assess their knowledge of routine medical checkups, their medical practices, and their participation in the Know Your Numbers campaign. The recruited sample exhibited average knowledge of parameters used to classify levels of blood glucose, blood pressure, BMI, and blood lipids, yet low knowledge about the recommended age to begin screening for a number of chronic diseases. Factors associated with levels of knowledge were gender, age, education level, and employment. However, only being diagnosed with a chronic disease was associated with performing a minimum of one measurement or assessment. Finally, less than 5% of this sample reported their participation in the Know Your Numbers campaign and assessment of their BMI, waist circumference, blood glucose, and blood pressure as part of the campaign.
The findings of our investigation can be compared to similar local and international studies. A study by Al-Kahil et al measured the knowledge and practices of 414 participants with regards to routine medical checkups among middle-aged and elderly people in the Riyadh region of Saudi Arabia in 2019. In their study, it was reported that most participants did not perform routine medical checkups (65.7%). Al-Kahil et al reported relatively high awareness of routine medical checkups in their sample. Furthermore, they reported that factors influencing the practice of routine medical checkups were health concerns, while factors associated with low performance of routine medical checkups were lack of time and laziness.8 Despite the methodological differences between our investigation and theirs, their findings concerning factors associated with levels of knowledge and practices are similar to ours, as several factors were found to be associated with levels of knowledge, but a history of chronic disease was the only factor identified as being associated with performing routine medical checkups in our investigation.
In our study, higher levels of knowledge about routine medical checkups were noted among males compared to females, but there were no gender differences with regards to performing routine medical checkups. In a study by Al Baloushi et al that recruited a sample of 721 adults from the eastern province of Saudi Arabia and measured their practices of performing medical checkups, only 22.5% reported performing routine medical checkups; the practice was influenced by participants’ age, gender, and marital status. Our study identified similar low performance of routine medical checkups, but none of the demographic factors, apart from having a chronic disease, were associated with the practice of performing routine medical checkups.20 Our study did not investigate gender variation in the use of routine medical checkups. However, a study by Hale suggests potential psychological reasons for gender variations in the use of routine medical checkups because men like to be seen as strong, and they neglect to seek help for medical conditions such as prostate cancer. It can be postulated that, unlike men, women may be more concerned about their health and may thus pursue routine medical checkups more frequently in comparison to men.21
This study demonstrates a low level of knowledge regarding medical checkups, especially among those who are older than 25. Our study did not identify differences in practice levels by age group; however, another study done in Saudi Arabia by Maqbul et al showed that individuals aged 41–50 were more likely to perform routine medical checkups in comparison to other younger groups. Although our study did not identify any such differences, it can be postulated that older subjects, who are prone to chronic diseases, are more likely to perform routine medical checkups in comparison to younger, healthy individuals.22
A study by Alzahrani et al targeted Saudi adults living in the US to investigate their utilization of routine medical checkups. Alzahrani et al reported that among the recruited sample of 381 adults, only 25.5% reported performing routine checkups. Similar to our findings, Alzahrani et al reported that the likelihood of performing routine medical checkups was correlated with having a diagnosed chronic disease. Furthermore, Alzahrani et al reported that participants who trusted their primary care providers were more likely to perform routine medical checkups.23 Nonetheless, the association between trusting healthcare providers and the probability of routine medical checkups was not assessed in our study.
Our investigation identified low performance of routine medical checkups among adults in the Jazan region of Saudi Arabia. One of the factors that has been assessed to identify reasons associated with the low performance of routine medical checkups among Saudis was the presence of barriers related to accessing routine medical checkup services. A qualitative study by Alzahrani et al targeted 19 primary healthcare providers in the Makkah region of Saudi Arabia to assess barriers to routine medical checkups among Saudis. Alzahrani et al concluded that some physicians and clinic staff may lack knowledge about routine medical checkups. Furthermore, healthcare system-related barriers were reported by Alzahrani et al, such as limited staffing, crowded healthcare centers, and shortage of required infrastructure to perform routine checkups.24
Comparing our study to similar international investigations revealed several similarities as well as differences. Eke et al conducted a study in southeastern Nigeria to evaluate the perception and practice of periodic medical checkups by traders. The study included 323 participants of both genders aged 15–65 years and reported that 74.9% of the participants were aware of the importance of periodic routine checkups. However, Eke et al also reported low performance of routine checkups (33.3%). The practice of periodic medical checkups was shown to be unaffected by age, gender, or educational background, which is similar to our findings.9 A study conducted by Xi Sun et al in China reported that employees were more likely to perform routine medical checkups,25 which can be explained by the existence of a medical insurance system for employed individuals. This is different to the findings of the current investigation, where employment was not associated with the practice of routine medical checkups. This may be because the healthcare system in Saudi Arabia is freely available for citizens and is not affected by employment status. While expatriates in Saudi Arabia are also covered by health insurance if they are employed, this was not assessed in our investigation.
Similar international campaigns with a similar style to the recent Know Your Numbers campaign provided by the Saudi Ministry of Health were also identified. Nonetheless, a variation in the targeted population or conditions was noted. For example, the Know Your Numbers campaign by the American Health Association targeted women to encourage assessment of blood pressure, cholesterol, blood sugar, and BMI levels.26 Similarly, a Know Your Numbers campaign was conducted in the UK, targeting the assessment of blood pressure only.27 Nonetheless, studies on the utilization and impact of similar international Know Your Numbers campaigns are limited. A community-based Know Your Numbers campaign was conducted via the National Stroke Foundation in Australia between 2008 and 2010 targeting the assessment of blood pressure levels among pharmacy attendees. Among the 59,817 registrants of the campaign, 2044 were followed up with, where improvement in knowledge and engagement with health promotion actions was reported.28
Chronic non-communicable diseases can negatively affect individuals’ quality of life and impose financial burdens on healthcare systems as a whole.22,29–35 Our study identified low utilization of healthcare services for routine medical checkups among adults in the Jazan region. The importance of this finding stems from the fact that non-communicable diseases are mainly a result of genetic and environmental factors, such as family risk, unhealthy food intake, lack of exercise, and unfavorable habits, so early identification and modification of risk factors may influence the outcome of these diseases. It can be argued that performing routine medical checkups and screening for non-communicable diseases—including obesity, hypertension, diabetes, and oncological diseases—is a key factor for early identification, reduction of complications, and modification to a favorable prognosis. Heavier promotion of the importance of routine medical checkups is therefore highly recommended. This notion is further supported by the low utilization of the Know Your Numbers campaign, which is being implemented by the Saudi Ministry of Health at the time of writing this report.
Strengths and Limitations
This study had multiple strengths and weaknesses. The main strength of this investigation is related to its ability to obtain a sample due to social media enabling recruitment of adults who are less likely to attend healthcare facilities for the purpose of performing routine medical checkups. A limitation of this study is inherent in the nature of data collection methods: using a self-administered questionnaire increases the chance of selection bias, as older, illiterate subjects were not able to participate. Additionally, although the questionnaire was self-administered and anonymous, we cannot neglect the possibility of occurrence of social desirability bias among the recruited sample.
Conclusion
Knowledge of routine medical checkups is low among the recruited sample of adults in Jazan, Saudi Arabia. Additionally, performing routine medical checkups is rare and only influenced by the existence of a diagnosed medical condition. Furthermore, we found low utilization of the Know Your Numbers campaign services. This mandates more emphasis on increasing awareness of routine medical checkups among adults in the Jazan region.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from any funding agency.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Herzallah HK, Antonisamy BR, Shafee MH, Al-Otaibi ST. Temporal trends in the incidence and demographics of cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade. Saudi Med J. 2019;40(3):277.
2. Herzallah HK, Antonisamy BR, Shafee MH, Al-Otaibi ST. Temporal trends in the incidence and demographics of cancers, communicable diseases, and non-communicable diseases in Saudi Arabia over the last decade. Saudi Med J. 2019;40(3):277–286.
3. Gosadi IM. Assessment of the environmental and genetic factors influencing prevalence of metabolic syndrome in Saudi Arabia. Saudi Med J. 2016;37(1):594.
4. Saudi Cancer Registry. Cancer Incidence Report, Saudi Arabia 2015. Available from: https://nhic.gov.sa/eServices/Documents/E%20SCR%20final%206%20NOV.pdf.
5. Gosadi IM. National screening programs in Saudi Arabia: overview, outcomes, and effectiveness. J Infect Public Health. 2019;12(5):608–614.
6. Tyrovolas S, El Bcheraoui C, Alghnam SA, et al. The burden of disease in Saudi Arabia 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Planetary Health. 2020;4(5):e195–e208.
7. Saudi Ministry of Health. World Health Survey; 2019. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/Population-Health-Indicators/Documents/World-Health-Survey-Saudi-Arabia.pdf.
8. Al-Kahil AB, Khawaja RA, Kadri AY, et al. Knowledge and practices toward routine medical checkup among middle-aged and elderly people of Riyadh. J Patient Exp. 2020;7(6):1310–1315.
9. Eke C, Eke N, Joe-Ikechebelu N, Okoye S. Perception and practice of periodic medical checkup by traders in South East Nigeria. Afrimedic J. 2012;3(2):24–29.
10. Ojong IN, Nsemo AD, Aji P. Routine Medical Checkup Knowledge, Attitude and Practice among Health Care Workers in a Tertiary Health Facility in Calabar, Cross River State, Nigeria. Glob J Health Sci. 2020;12(8):27.
11. Saudi Ministry of Health. MOH Launches “Know Your Numbers” Campaign; 2021. Available from: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-11-15-001.aspx.
12. Saudi Ministry of Health. Body Mass Index (BMI) Calculator; 2021. Available from: https://www.moh.gov.sa/HealthAwareness/MedicalTools/Pages/BodyMassIndex.aspx.
13. Saudi ministry of Health. Saudi guidelines on the prevention and management of obesity 2016. Available from: https://www.moh.gov.sa/Ministry/About/Health%20Policies/008.pdf.
14. Saudi Hypertension Management Society. Saudi Hypertension Management Guidelines. SHMS; 2018.
15. Center SND. Saudi Diabetes Clinical Practice Guidelines 2021. Available from: https://shc.gov.sa/Arabic/Documents/SDCP%20Guidelines.pdf.
16. Saudi Ministry of Health. Clinical Practice Guideline on the Use of Screening Strategies for the Detection of Breast Cancer 2014. Available from: https://www.moh.gov.sa/en/Ministry/Structure/Programs/TCP/Documents/8.%20Breast%20Cancer%20-%20Use%20of%20Screening%20Strategies%20for%20the%20Detection%20of%20Breast%20Cancer.pdf.
17. Saudi Ministry of Health. Colorectal Cancer Early Detection; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Projects/Colorectal-Cancer-Awareness/Pages/default.aspx.
18. Saudi Ministry of Health. Orthopedic Diseases; 2019. Available from: https://www.moh.gov.sa/en/HealthAwareness/EducationalContent/Diseases/OrthopedicDiseases/Pages/001.aspx.
19. Saudi Ministry of Health. Training Guide of Family Medicine Promotion Curriculum in Primary Healthcare Centers; 2019. Available from: https://www.moh.gov.sa/Ministry/About/Health%20Policies/024.pdf.
20. ALBaloushi NN, Alomair SA, Sayed IA. Attitude Toward Performance of Medical Checkups: a Survey from Eastern Profince of Saudi Arabia. Int J Tech Res Applications. 2015;1:27.
21. Hale S, Grogan S, Willott S. Patterns of self‐referral in men with symptoms of prostate disease. Br J Health Psychol. 2007;12(3):403–419.
22. Maqbul MS, Alghamdi RD, Bakhsh LW, Almashjari NA, Alanazi SH. A Cross Section Survey Assessment Study on the Knowledge and Practice of Periodic Medical Check up among the Saudi population. J N Dev Chem. 2021;3(3):40–49.
23. Alzahrani AMA, Felix HC, Stewart MK, Selig JP, Swindle T, Abdeldayem M. Utilization of Routine Medical Checkup and Factors Influencing Use of Routine Medical Checkup among Saudi Students Studying in the USA in 2019. Saudi J Health Sys Res. 2021;1(1):16–25.
24. Alzahrani AM, Quronfulah BS, Felix HC, Khogeer AA. Barriers to routine checkups use among Saudis from the perspective of primary care providers: a qualitative study. Saudi Med J. 2022;43(6):618–625.
25. Sun X, Chen Y, Tong X, et al. The use of annual physical examinations among the elderly in rural China: a cross-sectional study. BMC Health Serv Res. 2014;14(1):1–8.
26. American Heart Association. Know Your Numbers. Available from: https://www.goredforwomen.org/en/know-your-risk/know-your-numbers.
27. Blood Pressure UK. Know Your Numbers; 2021. Available from: https://www.bloodpressureuk.org/know-your-numbers/.
28. Cadilhac DA, Kilkenny MF, Johnson R, Wilkinson B, Amatya B, Lalor E. The Know Your Numbers (KYN) program 2008 to 2010: impact on knowledge and health promotion behavior among participants. Int J Stroke. 2015;10(1):110–116.
29. Alhowaish AK. Economic costs of diabetes in Saudi Arabia. J Family Community Med. 2013;20(1):1–7.
30. Elliott WJ. The economic impact of hypertension. J Clin Hypertension. 2003;5(3):3–13.
31. Czepczor-Bernat K, Brytek-Matera A, Staniszewska A. The effect of a web-based psychoeducation on emotional functioning, eating behaviors, and body image among premenopausal women with excess body weight. Arch Women’s Mental Health. 2021;24(3):423–435.
32. Sharp L, O’Leary E, O’Ceilleachair A, Skally M, Hanly P. Financial impact of colorectal cancer and its consequences: associations between cancer-related financial stress and strain and health-related quality of life. Dis Colon Rectum. 2018;61(1):27–35.
33. Abusanad A, Alghamdi M, Bakkar M, Jazieh AR. General Oncology Care in the Kingdom of Saudi Arabia. In: Cancer in the Arab World. Springer, Singapore; 2022:215–233.
34. Lopes JV, Bergerot CD, Barbosa LR, et al. Impact of breast cancer and quality of life of women survivors. Rev Bras Enferm. 2018;71:2916–2921.
35. Cotrim H, Pereira G. Impact of colorectal cancer on patient and family: implications for care. Eur J Oncol Nurs. 2008;12(3):217–226.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.