")
Back to Journals » OncoTargets and Therapy » Volume 11
Alternative treatment strategies to sorafenib in patients with advanced hepatocellular carcinoma: a meta-analysis of randomized Phase III trials
Authors Wang H , Wang HF, Yu ZC, Liu HH
Received 22 April 2018
Accepted for publication 15 June 2018
Published 27 August 2018 Volume 2018:11 Pages 5195—5201
DOI https://doi.org/10.2147/OTT.S171918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Federico Perche
Hui Wang, Hefang Wang, Zhichong Yu, Honghao Liu
Department of Radiation Oncology, Yancheng First People’s Hospital, Yancheng, Jiangsu 224005, China
Introduction: This meta-analysis was conducted to evaluate efficacy and safety in patients treated with sorafenib vs other tyrosine-kinase inhibitors (TKIs) or selective internal radiotherapy (SIRT) for advanced hepatocellular carcinoma (HCC).
Methods: Electronic databases were systematically reviewed for randomized Phase III trials comparing sorafenib with other TKIs or SIRT in advanced HCC. Sorafenib was defined as the control arm. Other TKIs or SIRT was defined as the experimental arm. Overall survival (OS), time to progression (TTP), objective response rate (ORR), disease-control rate (DCR), and adverse events (AEs) were reviewed. Four trials in the other-TKI group (n=4,218) and two in the SIRT group (n=819) were eligible.
Results: Compared with sorafenib, other TKIs showed similar benefit on OS (HR 1.08, 95% CI 0.93–1.24; P=0.31) and TTP (HR 0.86, 95% CI 0.66–1.12; P=0.26) for advanced HCC. A significant increase in ORR (RR 1.67, 95% CI 1.15–2.43; P=0.008) was found with other TKIs, but no increase in DCR (RR 1.11, 95% CI 0.98–1.26; P=0.11) was observed. Other TKIs were associated with more frequent grade 3/4 AEs than sorafenib, including hypertension (P<0.00001), thrombocytopenia (P=0.002), fatigue (P<0.00001), decreased appetite (P<0.00001), and vomiting (P<0.0001). For locally advanced HCC, neither OS (HR 1.14, 95% CI 0.98–1.32; P=0.09) nor TTP (HR 0.87, 95% CI 0.74–1.02; P=0.10) differed significantly in SIRT and sorafenib. There was an increase in ORR (RR 2.60, 95% CI 1.69–4.00; P<0.0001), but no improvement in DCR (RR 0.91, 95% CI 0.81–1.02; P=0.11) in the SIRT group. Fewer patients treated with SIRT had grade 3/4 AEs than those treated with sorafenib, including diarrhea (P<0.0001), fatigue (P=0.0006), and hand–foot syndrome (P=0.0002). Other TKIs were noninferior to sorafenib in OS and TTP in advanced HCC, but with increased risk of toxicities.
Conclusion: Patients with locally advanced HCC treated with SIRT got similar efficacy with less toxicity to those treated with sorafenib.
Keywords: sorafenib, tyrosine-kinase inhibitors, selective internal radiotherapy, hepatocellular carcinoma, meta-analysis
Introduction
Hepatocellular carcinoma (HCC) is the fifth-most common cancer in males and the seventh in females worldwide. Patients in developing countries account for about 85% of victims globally.1 Hepatitis B virus (HBV) infection is the leading cause of HCC in Asia, while hepatitis C virus (HCV) infection is the main pathogen in Europe and North America.2 Over the past few decades, the incidence of HCC has been increasing in Western countries, particularly in the population infected with HCV.3 Surgery or liver transplantation are regarded as optimal treatment options, but only about 20% of HCC patients are suitable for potentially curative resection. Patients with intermediate stage HCC may obtain limited survival benefit from locoregional treatment.4 Although early- and intermediate-stage HCC can be controlled temporarily, most patients may progress to an advanced stage after the initial therapy.
Sorafenib is an oral multitarget tyrosine-kinase inhibitor (TKI), which acts by blocking the activities of Raf kinase and VEGFR and inhibiting tumor angiogenesis and proliferation.5 Sorafenib has been recognized as a standard therapy for advanced HCC, resulting from the approval of it for a modest overall survival (OS) benefit.6,7 The successful approval of sorafenib has greatly stimulated the development of other TKIs in advanced HCC. There have been six randomized controlled trials to evaluate efficacy and safety of other TKIs, including sunitinib, brivanib, linifanib, dovitinib, lenvatinib, and nintedanib, and all demonstrated noninferiority to sorafenib in OS in patients with advanced HCC.8–13 However, linifanib and lenvatinib showed significant improvement in time to progression (TTP) and objective response rate (ORR) to sorafenib.10,12
Although sorafenib is the reference treatment in advanced HCC, dose reduction or discontinuation of sorafenib are frequently necessary, due to such adverse events (AEs) as diarrhea, fatigue and hand–foot syndrome.6,7,14 Selective internal radiation (SIRT) might be an alternative therapy to sorafenib with less toxicity in locally advanced HCC patients.15,16 SIRT with yttrium 90 (90Y) microspheres is a therapeutic procedure applied via the hepatic artery, delivering brachytherapy directly to liver tumors. In the SARAH and SIRVENIB trials, OS and TTP in the SIRT group were similar to the sorafenib group among patients with locally advanced HCC. However, ORR and AE frequency were improved with SIRT over sorafenib.15,16
As mentioned, other TKIs and SIRT might be alternative treatments to sorafenib for advanced HCC. We conducted this meta-analysis with only large prospective randomized trials included to examine efficacy and safety of other TKIs and SIRT vs sorafenib comprehensively. The main end points were OS and TTP. Secondary end points were ORR, disease-control rate (DCR) and AEs.
Methods
Literature-search strategy
Databases were searched systematically, including PubMed, Embase, Chinese National Knowledge Infrastructure, and Wanfang, for titles including “sorafenib” for identification of sorafenib, “tyrosine kinase inhibitor” or “TKI” for identification of TKIs, “selective internal radiotherapy” or “selective internal radiation” for identification of SIRT, and “(hepatocellular or liver) and (cancer or carcinoma)” or “hepatoma” or “HCC” for identification of HCC.
Inclusion and exclusion criteria
We included studies based on the following inclusion criteria: randomized Phase III trials, OS or TTP reported, one treatment group receiving sorafenib and the other receiving other TKIs or SIRT, and HCC patients with Child–Pugh A or B liver-function status, performance status (PS) 0–1, and Barcelona Clinic Liver Cancer B or C enrolled. Reviews, retrospective studies, studies unrelated to the topics, or studies without outcomes of interest were excluded. Publication language was not limited.
Data extraction and quality assessment
We reviewed trials and abstracts of potentially eligible studies and extracted information from studies that met the inclusion criteria, including authors, publication year, sample size, patient characteristics, treatment regimens, and treatment efficacy, such as OS, TTP, ORR, and DCR. The Jadad scoring system was used to assess study quality, graded 0–5 depending on randomization, blinding, and dropout.
Statistical analysis
The main end points were OS and TTP. OS was defined as time from random assignment to death from any cause. TTP was defined as time from randomization until disease progression. Secondary end points were ORR and DCR. Results for OS and TTP were expressed as HRs with 95% CIs. HRs and 95% CIs were used directly if reported in the trial. Otherwise, we worked out HR and 95% CI values by a method previously reported.17 Results for ORR and DCR are expressed as relative risk. Results of grade 3/4 AEs are also expressed as relative risk. The meta-analysis was performed using RevMan 5.3. To evaluate statistical heterogeneity across the studies, χ2 and I2 statistics were used, with predefined significance for χ2 P-value <0.1 or I2>50%. HR and ORR were calculated with a fixed-effect model if heterogeneity was not observed. Otherwise, a random-effect model was used. P<0.05 (two-sided) was considered statistically significant.
Results
Study characteristics
After exclusion of 156 studies, a total of four trials in the other-TKI group and two trials in the SIRT group were eligible (selection process in Figure 1; detailed information listed in Table 1). Based on the data available for all eligible trials, patients were mostly male, median age 56 and 66 years, with good PS (0–1), good liver function (Child–Pugh A and B) and advanced HCC (Barcelona Clinic Liver Cancer B and C). The results of assessing the quality of all eligible studies are also shown in Table 1.
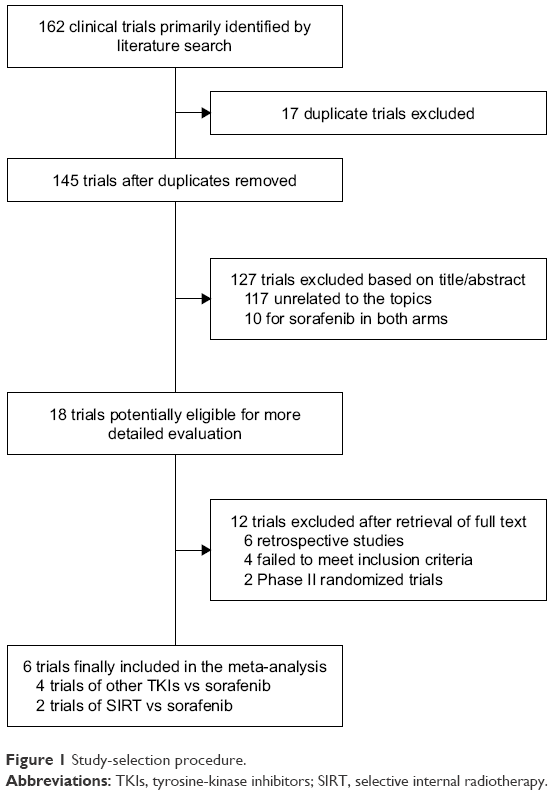 | Figure 1 Study-selection procedure. |
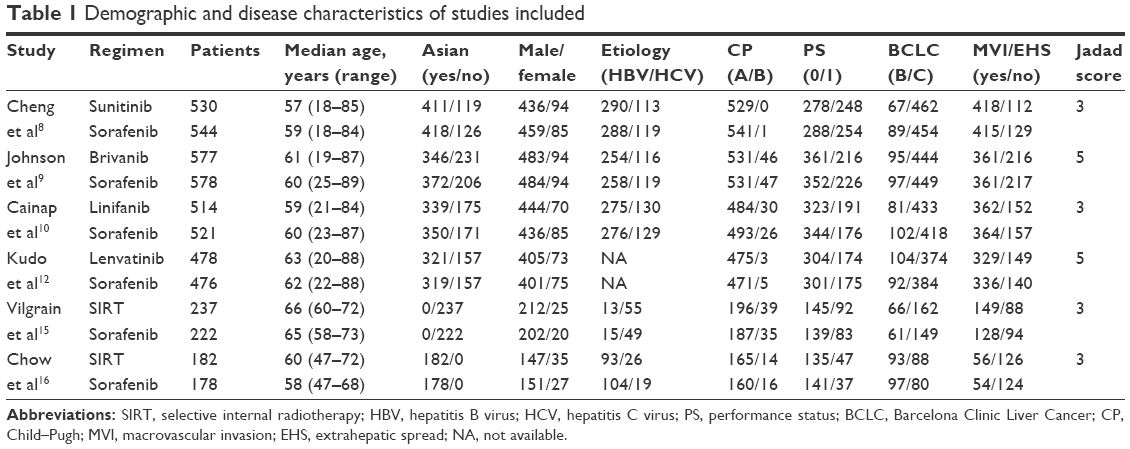 | Table 1 Demographic and disease characteristics of studies included |
Other TKIs vs sorafenib
Main analyses of OS and TTP
Survival analyses were based on 4,218 patients from four trials. Other TKIs showed similar benefit on OS to sorafenib for advanced HCC (HR 1.08, 95% CI 0.93–1.24; P=0.31) (Figure 2). There was heterogeneity among the trials (P=0.008, I2=74%), so a random-effect model was used. The pooled HR of TTP was 0.86 (95% CI 0.66–1.12, P=0.26) with significantly high heterogeneity (I2=92%, P<0.00001) using a random-effect model, as shown in Figure 3.
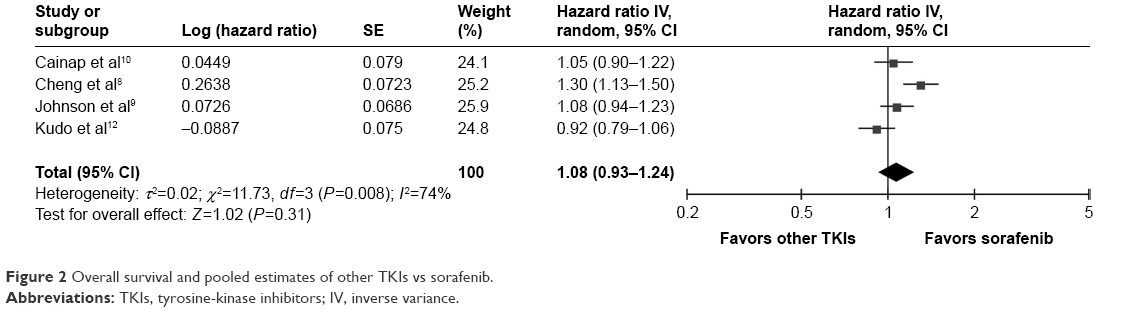 | Figure 2 Overall survival and pooled estimates of other TKIs vs sorafenib. |
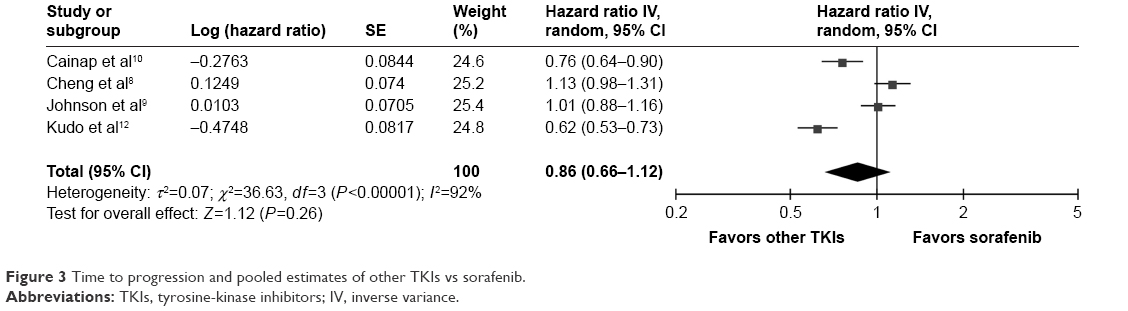 | Figure 3 Time to progression and pooled estimates of other TKIs vs sorafenib. |
Subgroup analyses of OS
Subgroup analyses identified baseline factors as prognostic of OS: region, AFP level, PS, etiology, and tumor burden. There were no significant differences in OS benefit between sorafenib and other TKIs in subgroups (Table 2).
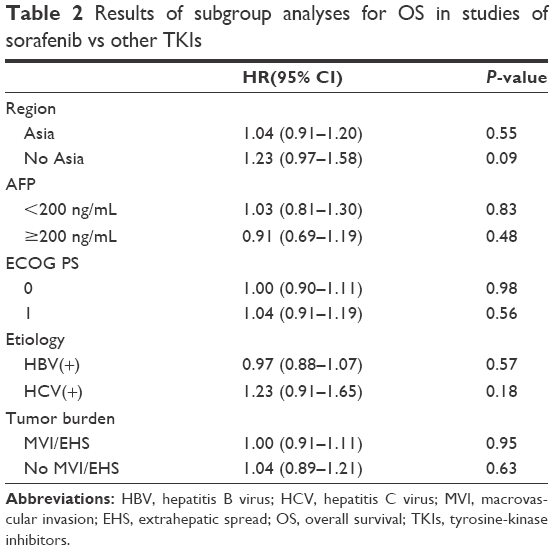 | Table 2 Results of subgroup analyses for OS in studies of sorafenib vs other TKIs |
Analyses of ORR and DCR
Other TKIs showed greater ORR than sorafenib (RR 1.67, 95% CI 1.15–2.43; P=0.008); however, other TKIs failed to show improvement compared with sorafenib for DCR (RR 1.11, 95% CI 0.98–1.26; P=0.11; Table 3).
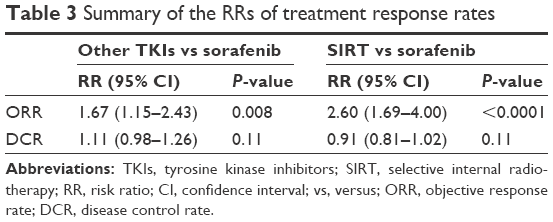 | Table 3 Summary of the RRs of treatment response rates |
AEs
Compared with sorafenib, other TKIs were associated with higher incidence of hypertension (RR 1.99, 95% CI 1.67–2.39; P<0.00001), fatigue (RR 1.79, 95% CI 1.42–2.26; P<0.00001), thrombocytopenia (RR 4.18, 95% CI 1.66–10.56; P=0.002), decreased appetite (RR 2.21, 95% CI 1.62–3.01; P<0.00001), and vomiting (RR 3.15, 95% CI 1.88–5.26; P<0.0001). However, hand–foot syndrome (RR 0.39, 95% CI 0.19–0.82; P=0.01) and rash (RR 0.34, 95% CI 0.17–0.68; P=0.002) occurred less frequently in the other-TKI group than the sorafenib group (Table 4).
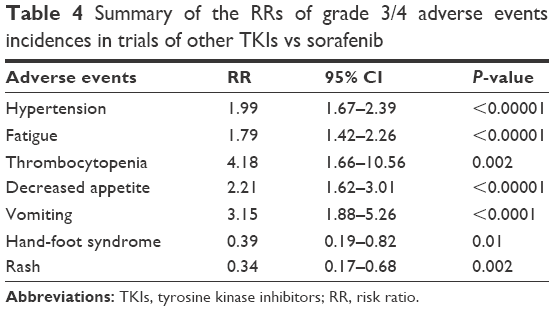 | Table 4 Summary of the RRs of grade 3/4 adverse events incidences in trials of other TKIs vs sorafenib |
SIRT vs sorafenib
Main analyses of OS and TTP
Two trials of SIRT vs sorafenib involving 819 patients reported HRs with 95% CIs of OS and TTP. Pooled HRs for OS and TTP were 1.14 (95% CI 0.98–1.32, P=0.09; Figure 4) and 0.87 (95% CI 0.74–1.02, P=0.10; Figure 5) and showed similar efficacy in the SIRT and sorafenib groups. There was no heterogeneity between the trials for OS (I2=0, P=0.87; Figure 4) or TTP (I2=0; P=0.94; Figure 5), so a fixed-effect model was used.
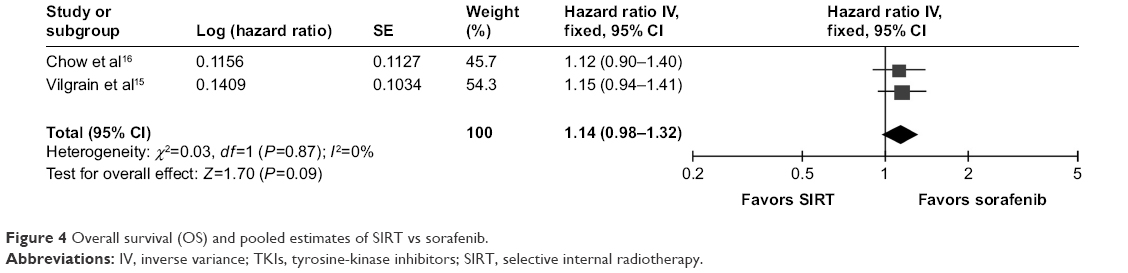 | Figure 4 Overall survival (OS) and pooled estimates of SIRT vs sorafenib. |
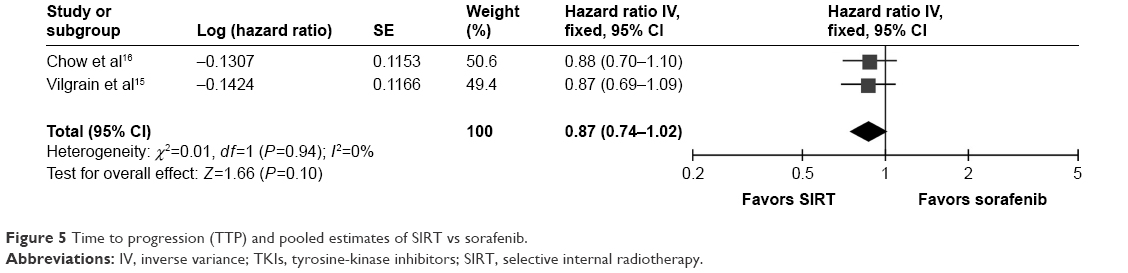 | Figure 5 Time to progression (TTP) and pooled estimates of SIRT vs sorafenib. |
Analyses of ORR and DCR
The ORR was significantly greater (RR 2.60, 95% CI 1.69–4.00; P<0.0001) in the SIRT group than the sorafenib group, but no improvement in DCR (RR 0.91, 95% CI 0.81–1.02; P=0.11) was identified in the SIRT group (Table 3).
AEs
The incidence of diarrhea (RR 0.10, 95% CI 0.03–0.28; P<0.0001), fatigue (RR 0.42, 95% CI 0.26–0.69; P=0.0006), and hand–foot syndrome (RR 0.04, 95% CI 0.01–0.22; P=0.0002) in patients treated with SIRT was significantly lower than those treated with sorafenib. However, there were no significant differences between SIRT and sorafenib in the occurrence of pyrexia (P=0.15), nausea (P=0.78), abdominal pain (P=0.23), ascites (P=0.62) gastric ulcer (P=0.22), or upper gastrointestinal hemorrhage (P=0.34; Table 5).
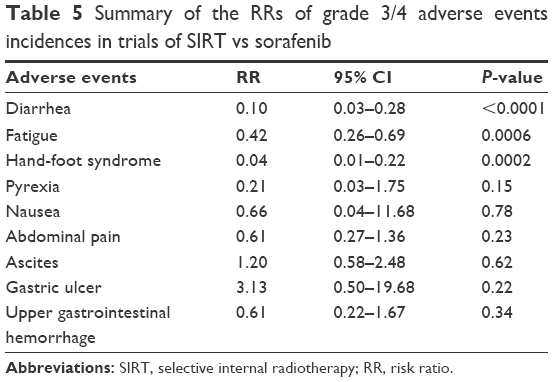 | Table 5 Summary of the RRs of grade 3/4 adverse events incidences in trials of SIRT vs sorafenib |
Discussion
Our meta-analysis included more data than previous meta-analyses, in which recent published clinical trials have not been updated.12,15,16,18–20 In addition, our meta-analysis included randomized Phase III trials only. As such, our findings are more comprehensive and reliable. Based on four trials and 4,218 patients, results demonstrated similar efficacy of other TKIs to sorafenib on both OS and TTP for advanced HCC patients. Subgroup analyses identified AFP level, PS, etiology, and tumor burden as key prognostic indicators. No differences on OS were found in any subgroups. Pooled results of two trials comprising 819 patients did not show a difference in OS and TTP between SIRT and sorafenib among locally advanced HCC patients. Therefore, other TKIs and SIRT might be alternative treatments to sorafenib for advanced HCC.
Broad-spectrum TKIs have been developed and tested in first- and second-line therapy for advanced HCC.8–13,21–23 Four randomized Phase III trials have investigated the use of other TKIs (sunitinib/brivanib/linifanib/lenvatinib) as first-line therapy, all including sorafenib as the control. Our results suggested that other TKIs had similar benefits on OS and TTP when compared with sorafenib. We also conducted subgroup analyses to demonstrate the efficacy of sorafenib vs other TKIs in advanced-HCC patients with various clinical characteristics. Patients from different geographic regions, with different AFP levels, with various PS, and with different tumor burden obtained similar benefits in OS. However, there was a trend of patients treated with sorafenib who were HCV-infected having increased hazard than those treated with other TKIs, although this showed no statistically significant evidence. Consistently, Shao et al and Jackson et al reported improved OS for patients positive for HCV when treated with sorafenib, but no evidence of any improvement in OS attributable to sorafenib for patients positive for HBV and negative for HCV.18,20 Meanwhile, a retrospective study of patients who received sorafenib for advanced HCC found that HCV infection but not ethnicity was associated with OS.24 As for mechanism, HCC development and progression are relevant to Raf1–MAPK pathway activation and HCV proteins activate the Raf1–Mek–ERK pathway.25–27 Moreover, a study has suggested that HCV-related HCC exhibits higher expression of VEGF than HBV-related disease.28 Sorafenib can mediate inhibition of VEGFR and Raf1, and this may explain the efficacy of sorafenib in HCV-related patients. Therefore HCV-related HCC patients may get better efficacy from sorafenib than other etiologic factor-related disease.5
Pooled ORR was significantly higher in advanced-HCC patients treated with other TKIs than those treated with sorafenib, but DCRs were similar between sorafenib and other TKIs. Unfortunately, the improvement in ORR did not translate into a survival advantage. The incidence of grade 3/4 AEs was higher for other TKIs than sorafenib. Notably, differences were seen in the toxicity profile between sorafenib and other TKIs, with higher rates of grade 3/4 hypertension, fatigue, decreased appetite, vomiting, and thrombocytopenia occurring in those treated with other TKIs, whereas patients on sorafenib had higher rates of grade 3/4 rash and hand–foot syndrome. Although other TKIs have similar efficacy compared with sorafenib, other factors, such as toxicity and cost-effectiveness, will determine their roles in the future management of advanced HCC.29
SIRT with 90Y resin microspheres is an effective treatment for advanced unresectable HCC.30 Several retrospective trials have indicated that SIRT can offer similar OS for patients with locally advanced HCC compared with sorafenib, but with fewer AEs and better quality of life.31–33 Consistently, our meta-analysis, including two randomized Phase III trials, suggested that OS and TTP in the SIRT group was similar to that in the sorafenib group. It can be seen that SIRT is an alternative treatment to sorafenib in patients with locally advanced HCC. Besides, the ORR was significantly higher on SIRT compared with sorafenib for patients with locally advanced HCC, while no increase in DCR was observed. Importantly, tolerability was significantly better in the SIRT than the sorafenib arm. Common grade 3/4 AEs, including hand–foot syndrome, diarrhea, and fatigue, occurred more frequently in patients treated with sorafenib than those treated with SIRT, which is consistent with treatment discontinuation that has previously been observed.6,7 SIRT-related AEs were as expected.
Conclusively, other TKIs and sorafenib resulted in similar OS and TTP in advanced HCC. ORR favored other TKIs, whereas safety results favored sorafenib. For patients with locally advanced HCC, OS did not differ significantly between SIRT and sorafenib. Moreover, SIRT was associated with higher ORR and fewer AEs than sorafenib.
Acknowledgment
This work was supported by the Innovation and Entrepreneurship Program of Jiangsu Province (2017).
Disclosure
The authors report no conflicts of interest in this work.
References
El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011;365(12):1118–1127. | ||
Bosch FX, Ribes J, Borràs J. Epidemiology of primary liver cancer. Semin Liver Dis. 1999;19(3):271–285. | ||
El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med. 1999;340(10):745–750. | ||
Lencioni R. Management of hepatocellular carcinoma with transarterial chemoembolization in the era of systemic targeted therapy. Crit Rev Oncol Hematol. 2012;83(2):216–224. | ||
Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64(19):7099–7109. | ||
Cheng AL, Kang YK, Chen Z, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009;10(1):25–34. | ||
Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. | ||
Cheng AL, Kang YK, Lin DY, et al. Sunitinib versus sorafenib in advanced hepatocellular cancer: results of a randomized phase III trial. J Clin Oncol. 2013;31(32):4067–4075. | ||
Johnson PJ, Qin S, Park JW, et al. Brivanib versus sorafenib as first-line therapy in patients with unresectable, advanced hepatocellular carcinoma: results from the randomized phase III BRISK-FL study. J Clin Oncol. 2013;31(28):3517–3524. | ||
Cainap C, Qin S, Huang WT, et al. Linifanib versus sorafenib in patients with advanced hepatocellular carcinoma: results of a randomized phase III trial. J Clin Oncol. 2015;33(2):172–179. | ||
Cheng AL, Thongprasert S, Lim HY, et al. Randomized, open-label phase 2 study comparing frontline dovitinib versus sorafenib in patients with advanced hepatocellular carcinoma. Hepatology. 2016;64(3):774–784. | ||
Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. | ||
Palmer DH, Ma YT, Peck-Radosavljevic M, et al. A multicentre, open-label, phase-I/randomised phase-II study to evaluate safety, pharmacokinetics, and efficacy of nintedanib vs. sorafenib in European patients with advanced hepatocellular carcinoma. Br J Cancer. 2018;118(9):1162–1168. | ||
Pinter M, Sieghart W, Graziadei I, et al. Sorafenib in unresectable hepatocellular carcinoma from mild to advanced stage liver cirrhosis. Oncologist. 2009;14(1):70–76. | ||
Vilgrain V, Pereira H, Assenat E, et al. Efficacy and safety of selective internal radiotherapy with yttrium-90 resin microspheres compared with sorafenib in locally advanced and inoperable hepatocellular carcinoma (SARAH): an open-label randomised controlled phase 3 trial. Lancet Oncol. 2017;18(12):1624–1636. | ||
Chow PK, Gandhi M, Tan SB, et al. SIRVENIB: selective internal radiation therapy versus sorafenib in Asia-Pacific patients with hepatocellular carcinoma. J Clin Oncol. 2018;36(19):1913–1921. | ||
Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta-analyses of the published literature for survival endpoints. Stat Med. 1998;17(24):2815–2834. | ||
Shao YY, Shau WY, Chan SY, Lu LC, Hsu CH, Cheng AL. Treatment efficacy differences of sorafenib for advanced hepatocellular carcinoma: a meta-analysis of randomized clinical trials. Oncology. 2015;88(6):345–352. | ||
Gebski V, Gibbs E, Gandhi M, et al. VESPRO: an individual patient data prospective meta-analysis of selective internal radiation therapy versus sorafenib for advanced, locally advanced, or recurrent hepatocellular carcinoma of the SARAH and SIRVENIB Trials. JMIR Res Protoc. 2017;6(2):e17. | ||
Jackson R, Psarelli EE, Berhane S, Khan H, Johnson P. Impact of viral status on survival in patients receiving sorafenib for advanced hepatocellular cancer: a meta-analysis of randomized phase III trials. J Clin Oncol. 2017;35(6):622–628. | ||
Kudo M, Han G, Finn RS, et al. Brivanib as adjuvant therapy to transarterial chemoembolization in patients with hepatocellular carcinoma: a randomized phase III trial. Hepatology. 2014;60(5):1697–1707. | ||
Llovet JM, Decaens T, Raoul JL, et al. Brivanib in patients with advanced hepatocellular carcinoma who were intolerant to sorafenib or for whom sorafenib failed: results from the randomized phase III BRISK-PS study. J Clin Oncol. 2013;31(28):3509–3516. | ||
Rimassa L, Santoro A, Daniele B, et al. Tivantinib, a new option for second-line treatment of advanced hepatocellular carcinoma? The experience of Italian centers. Tumori. 2015;101(2):139–143. | ||
Peixoto RD, Renouf DJ, Gill S, Cheung WY, Lim HJ. Relationship of ethnicity and overall survival in patients treated with sorafenib for advanced hepatocellular carcinoma. J Gastrointest Oncol. 2014;5(4):259–264. | ||
Aoki H, Hayashi J, Moriyama M, Arakawa Y, Hino O. Hepatitis C virus core protein interacts with 14-3-3 protein and activates the kinase Raf-1. J Virol. 2000;74(4):1736–1741. | ||
Bürckstümmer T, Kriegs M, Lupberger J, Pauli EK, Schmittel S, Hildt E. Raf-1 kinase associates with hepatitis C virus NS5A and regulates viral replication. FEBS Lett. 2006;580(2):575–580. | ||
Giambartolomei S, Covone F, Levrero M, Balsano C. Sustained activation of the Raf/MEK/Erk pathway in response to EGF in stable cell lines expressing the hepatitis C virus (HCV) core protein. Oncogene. 2001;20(20):2606–2610. | ||
Schmitz KJ, Wohlschlaeger J, Lang H, et al. Activation of the ERK and Akt signalling pathway predicts poor prognosis in hepatocellular carcinoma and ERK activation in cancer tissue is associated with hepatitis C virus infection. J Hepatol. 2008;48(1):83–90. | ||
Meyer T. Treatment of advanced hepatocellular carcinoma: beyond sorafenib. Lancet Gastroenterol Hepatol. 2018;3(4):218–220. | ||
Lee EW, Khan S. Recent advances in transarterial embolotherapies in the treatment of hepatocellular carcinoma. Clin Mol Hepatol. 2017;23(4):265–272. | ||
Cho YY, Lee M, Kim HC, et al. Radioembolization is a safe and effective treatment for hepatocellular carcinoma with portal vein thrombosis: a propensity score analysis. PLoS One. 2016;11(5):e154986. | ||
de la Torre MA, Buades-Mateu J, de La Rosa PA, et al. A comparison of survival in patients with hepatocellular carcinoma and portal vein invasion treated by radioembolization or sorafenib. Liver Int. 2016;36(8):1206–1212. | ||
Gramenzi A, Golfieri R, Mosconi C, et al. Yttrium-90 radioembolization vs sorafenib for intermediate-locally advanced hepatocellular carcinoma: a cohort study with propensity score analysis. Liver Int. 2015;35(3):1036–1047. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.