")
Back to Journals » Journal of Inflammation Research » Volume 13
Alteration of Liver Biomarkers in Patients with SARS-CoV-2 (COVID-19)
Authors Gholizadeh P , Safari R, Marofi P, Zeinalzadeh E, Pagliano P, Ganbarov K , Esposito S, Khodadadi E, Yousefi M, Samadi Kafil H
Received 14 April 2020
Accepted for publication 16 June 2020
Published 1 July 2020 Volume 2020:13 Pages 285—292
DOI https://doi.org/10.2147/JIR.S257078
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Pourya Gholizadeh,1,2 Rohollah Safari,3 Parham Marofi,4 Elham Zeinalzadeh,4 Pasquale Pagliano,5 Khudaverdi Ganbarov,6 Silvano Esposito,5 Ehsaneh Khodadadi,7 Mehdi Yousefi,8 Hossein Samadi Kafil7
1Student Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran; 2Biotechnology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 3Department of Microbiology, Imam Reza Hospital, Tabriz University of Medical Sciences, Tabriz, Iran; 4Hematology and Oncology Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 5Department of Medicine, University of Salerno, Salerno, Italy; 6Department of Microbiology, Baku State University, Baku, Republic of Azerbaijan; 7Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran; 8Stem Cell Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
Correspondence: Hossein Samadi Kafil Tel +98-9127184735
Fax +98-4133364661
Email [email protected]
Introduction: Coronavirus disease 2019 (COVID-19) emerged in China and spread worldwide. In this study, we assessed the characteristics of markers of the liver in patients with COVID-19 to provide new insights in improving clinical treatment.
Patients and Methods: We recruited 279 patients who confirmed COVID-19 and the data of liver biomarkers and complete blood count of patients were defined as the day onset when the patients admitted to the hospital.
Results: The average of LDH value was 621.29 U/L in all patients with COVID-19, and CPK was 286.90 U/L. The average AST was 44.03 U/L in all patients, and ALT was 31.14 U/L. The AST/ALT ratio was 1.64 in all patients. The measurement of CRP was increased by 79.93% in all patients. Average ALT and AST values of patients with elevated ALT were significantly increased in comparison to patients with normal ALT (P-value = 0.001), while AST/ALT ratio was significantly decreased compared to patients with normal ALT (P-value= 0.014). In addition, the average LDH of patients with elevated ALT was significantly increased compared to patients with normal ALT (P-value = 0.014).
Conclusion: Hepatic injury and abnormal liver enzymes related to COVID-19 infection is an acute non-specific inflammation alteration.
Keywords: SARS-CoV-2, COVID-19, hepatic injury, liver enzymes, aminotransferases
Introduction
Since December 2019, coronavirus disease 2019 (COVID-19) was first reported in China and has led to a major concern of health problems worldwide.1 COVID-19 is caused by a novel coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).2,3 SARS-CoV-2 is classified as a single-stranded and positive-sense RNA virus, which belongs to the genus Betacoronavirus.4 This virus is closely related to two bat-derived SARS-like coronaviruses (88–99% similarity) including bat-SL-CoVZXL21 and bat-SL-CovZC45, while it is more distant from Middle East respiratory syndrome coronavirus (MERS-CoV, approximately 50% similarity) and SARS-CoV (approximately 79% similarity).4 The outstanding symptoms of COVID-19 are acute atypical pneumonia and pulmonary damage, which can progress to multiple organ failureleading to death in patients with underlying co-morbidities.2,3,5 However, ordinary symptoms of respiratory system infection were found in non-severe cases.2,3,5 The most common underlying diseases are cardiovascular disease and hypertension among adult patients followed by diabetes mellitus.5,6 Adults older than 18 years of age are the most common patients infected with SARS-CoV-195 and there are some cases of children aged between 2 and 15 years.7 In some cases, liver dysfunction followed by COVID-19 has also been observed, which could indicate a possibility for hepatic injury caused by COVID-19. The liver is constantly exposed to viruses, antigens, bacteria, and their products with inflammatory potential, which leads to hepatic injury. Several factors such as excessive alcohol consumption, exposure to toxins, viral infections and bile duct obstruction could cause hepatic injury.8 Viral agents such as hepatitis B virus (HBV), hepatitis C virus (HCV) and hepatitis E virus (HEV) are common causes of varying degrees of hepatic injury.9–11 Furthermore, some reports demonstrated that SARS-infected patients and MERS-infected patients had an increased value of liver enzyme and various degrees of hepatic injury.12,13 Li et al14 reported that C-reactive protein (CRP) index in patients with elevated alanine aminotransferase (ALT) level was significantly higher. They suggested that cytokine storm syndrome may cause COVID-19-related hepatic injury.14 However, the mechanism and reason for COVID-19-related hepatic injury is still unclear. At this time, COVID-19-related hepatic injury remains controversial and there is no more research regarding this issue. It is required to find the relationship between COVID-19 and its related hepatic injury, which could solve and decrease the practical clinical problems, and improve clinical treatment. Therefore, in this study, we assessed the characteristics of markers of liver function in patients with COVID-19 to provide new insights to better follow these patients.
Methods and Materials
Patient Selection
In this retrospective study, we recruited 279 patients with confirmed COVID-19 from 23 February to 19 March 2020 at Imam-Reza teaching and treatment hospital, Tabriz, Iran. This hospital was isolated and all wards of the hospital admitted patients with COVID-19 infection. All the patients were hospitalized and COVID-19 infection had been confirmed with real-time PCR and chest CT scan. All patients had no history of liver diseases and chronic hepatitis viral infection and their liver disease was due to COVID-19 disease. Samples of throat and nasopharyngeal swabs were collected from patients suspicious for COVID-19 for RT-PCR diagnosis. Pneumonia was diagnosed based on the Infectious Diseases Society of America/American Thoracic Society (IDSA/ATS) guidelines.15 Briefly, patients with pneumonia were diagnosed as having pneumonia who had at least one of the clinical symptoms of fever, cough, pleuritic chest pain, and dyspnea, as well as a finding of coarse crackles or elevated inflammatory biomarkers or auscultation and a new inflammation on chest CT. Pulmonary radiology showed that the lesions of COVID-19 in all patients progressed more than 50% within 24–48 hours. Treatment was done based on a combination of azithromycin and hydroxychloroquine and supportive therapy.
Baseline Data Collection
All laboratory reports were retrospectively extracted from the hospital information system (HIS). The data of liver function biomarkers and complete blood count (CBC) was defined as the day of onset when the patients were admitted to the hospital. The liver function tests included ALT, AST, lactate dehydrogenase (LDH).
Statistical Analysis
Microsoft Excel version 2016 was used for statistical analysis. All quantitative analyses were represented by the mean and standard deviation (STDEV). t-Student, Mann–Whitney U, and Chi-square tests were used to compare the differences between COVID-19 patients with elevated ALT group and normal ALT group. In addition, Spearman correlation coefficients were used to describe the strength and direction analysis of the linear relationship between ALT, AST, CPK and LDH variables. Significance was set as a P-value < 0.05.
Results
The average age of all patients with COVID-19 was almost 59 years old and 164 (58.78%) patients were male and 115 (41.22%) were female. The average LDH value was 621.29 U/L in all patients with COVID-19, and creatine phosphokinase (CPK) was 286.90 U/L. The average AST was 44.03 U/L in all patients and ALT was 31.14 U/L. The AST/ALT ratio was 1.64 in all patients. The measurement of CRP was increased by 79.93% in all patients. Patients' red blood cell values, platelet values and their indexes were normal. Furthermore, patients' white blood cell values were normal. The results are shown in Table 1.
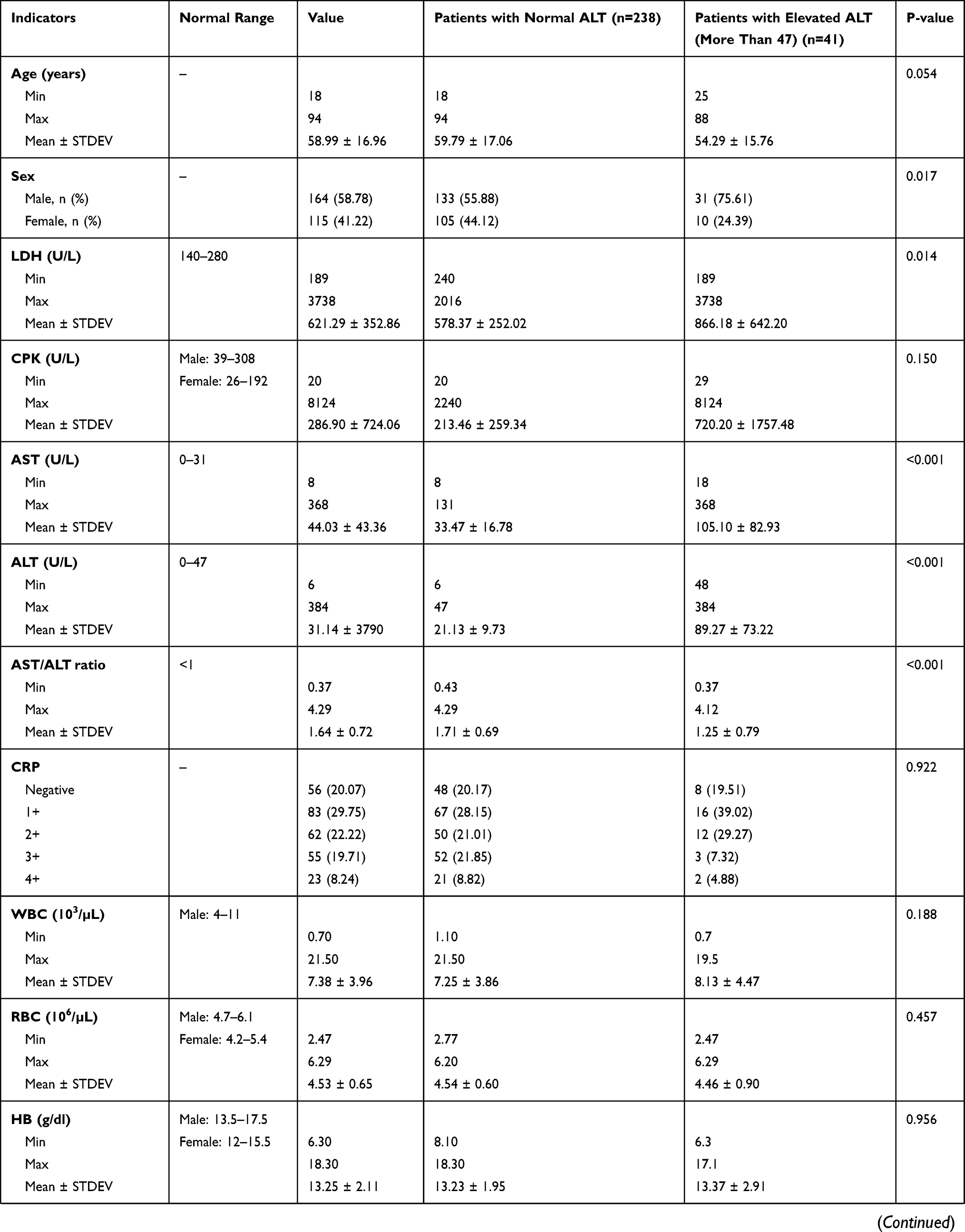 | 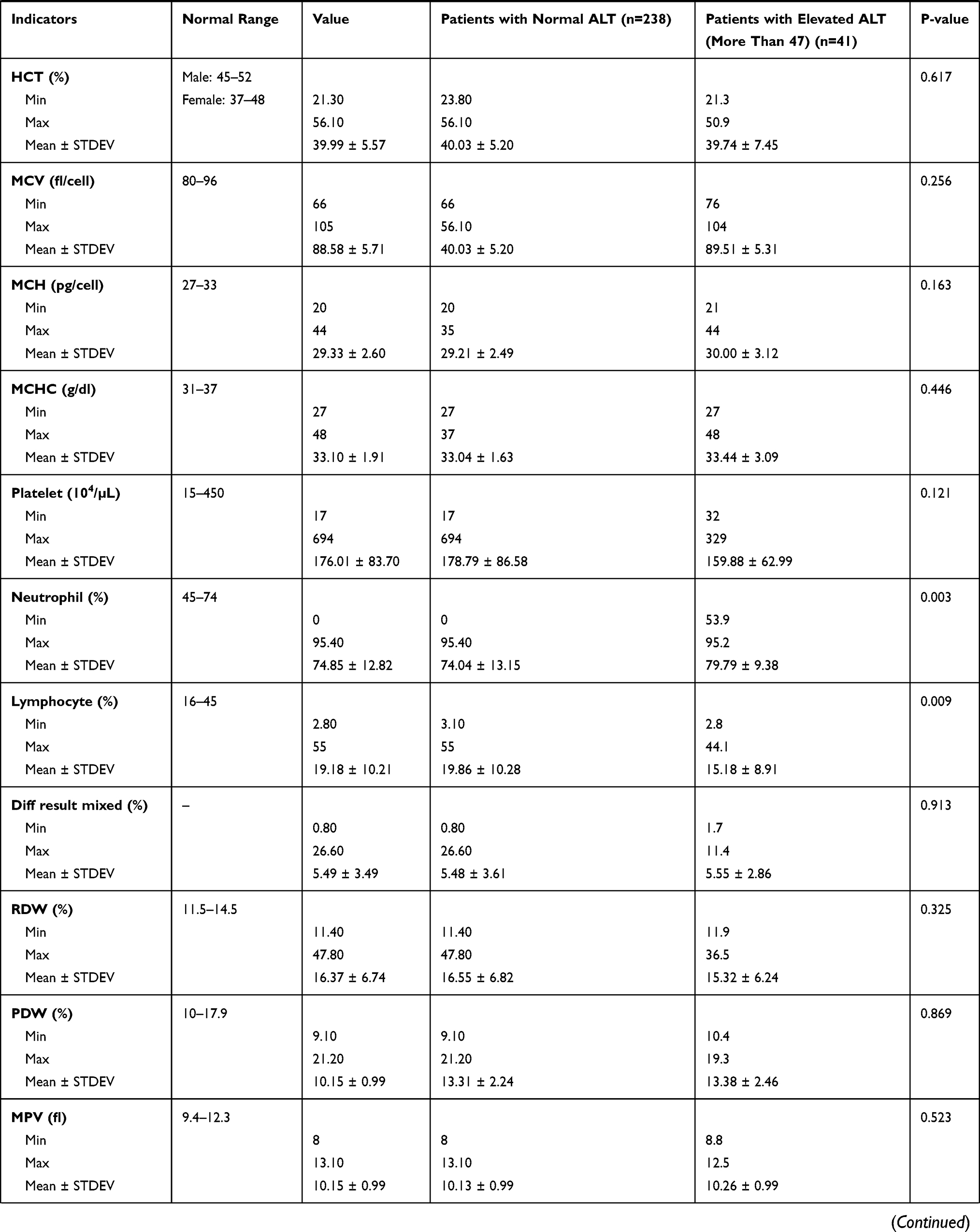 | 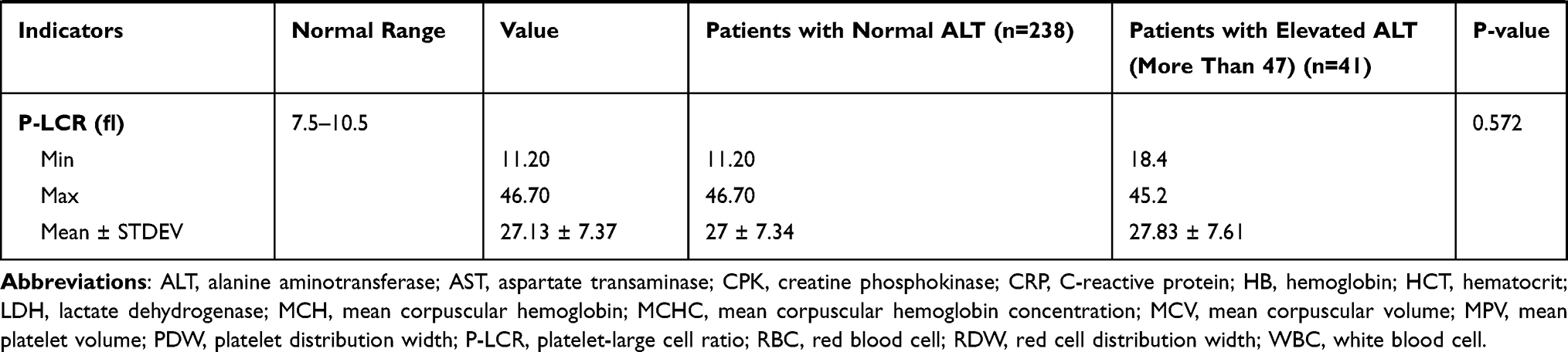 |
Table 1 Characteristics of Patients with COVID-19 and Characteristics of the ALT Elevated Group in Comparison to the Normal Group of Patients with COVID-19 |
In total, for 279 patients, laboratory results showed that 41 (14.70%) patients had an elevated ALT value, while only 9.75% (4 of 41) of those with elevated ALT had a normal AST value. Seven patients (17.07%) with elevated ALT were recruited from the intensive care unit (ICU), while 22 patients (9.24%) with normal ALT were recruited from the ICU. There were more male patients with elevated ALT in comparison to normal patients (P-value = 0.017). Furthermore, the average age of patients with elevated ALT was almost lower than patients with normal ALT (P-value = 0.054). The average ALT and AST values of patients with elevated ALT were significantly increased in comparison with patients with normal ALT (approximately 89 U/L and 105 U/L vs 21 U/L and 33 U/L, respectively; P-value < 0.001), while the AST/ALT ratio was significantly decreased in comparison to patients with normal ALT (1.25 vs 1.71, P-value= 0.014). Also, the average LDH of patients with elevated ALT was significantly increased compared to patients with normal ALT (approximately 866 U/L vs 578 U/L, P-value = 0.014; Figure 1). In addition, the ALT values were positively correlated with the AST values in patients with elevated ALT (P< 0.001). Also, there was a positive correlation in values of AST with CPK and LDH (P < 0.05) and CPK values with AST and LDH values (P< 0.05) in patients with elevated ALT (Figure 2), while all values were positively correlated with each other in patients with normal ALT (P< 0.05). Furthermore, we classified the patients by degree of ALT evaluation (1X ALT, 1.5X ALT, 2X ALT, 3X ALT and more than 3X ALT) and found that AST values were significantly different between groups (P < 0.001) and increased AST values were significantly increased in 3X ALT and more than 3X ALT groups (P = 0.033 and P < 0.001, respectively).
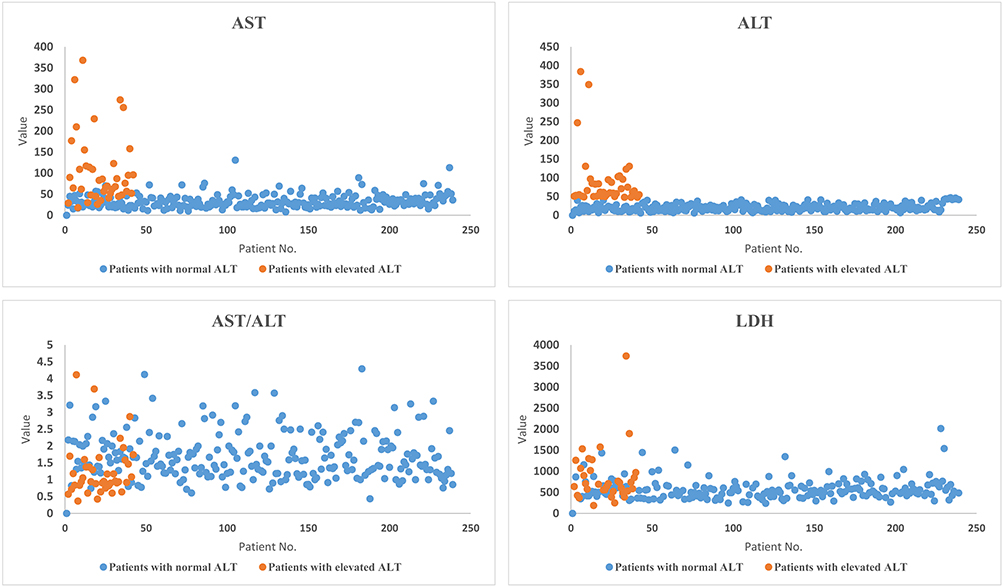 |
Figure 1 Distribution of ALT, AST, AST/ALT ratio, and LDH values among the elevated ALT and normal ALT patients with COVID-19. Each point in the diagrams show the values of the individual patients. Orange points belong to the elevated ALT patients and blue points to the normal ALT patients. The values of ALT, AST, AST/ALT ratio, and LDH of the elevated ALT patients were increased in comparison to the normal ALT patients (P-value < 0.05). |
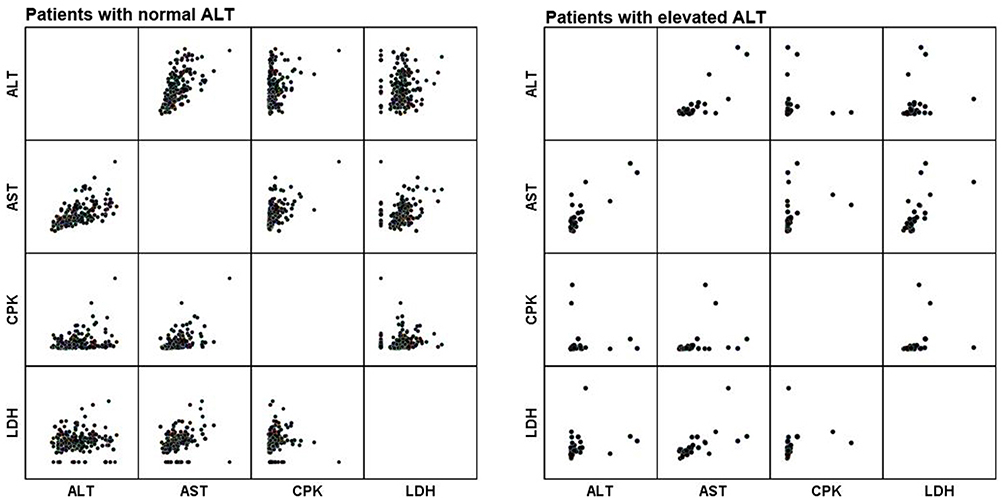 |
Figure 2 Correlation of the ALT, AST, CPK and LDH values with each other in patients with normal ALT and elevated ALT. The positive correlation was shown between the ALT and AST values in patients with elevated ALT, while the positivecorrelation between all values was shown with each other in patients with normal ALT. |
The blood differential cells' results showed that the average neutrophil percentage of patients with elevated ALT was significantly increased in comparison to patients with normal ALT (P-value = 0.003), while the average lymphocyte percentage was significantly decreased compared to patients with normal ALT (P-value = 0.009).
Discussion
COVID-19 infection mainly causes pulmonary symptoms, but this infection may simultaneously lead to other organ injuries such as cardiac muscle, kidneys, and liver.7,16,17 As shown in this study, an increase in factors of hepatic injury has occurred in COVID-19 patients. Liver enzymes including ALT and AST are useful biomarkers of hepatic dysfunction in patients.18–20 Most liver diseases initially cause mild symptoms, but they must be detected early. Liver dysfunction can be crucially important in some diseases. The hepatic injury could be determined by tests that are associated with liver function (e.g. albumin), liver cellular integrity (e.g. ALT and AST), and some are associated with conditions linked to the biliary tract (e.g. alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT)).18–20 The liver is constantly exposed to viruses, antigens, bacteria, and their products with inflammatory potential, which leads to hepatic dysfunction. Multitudinous factors such as excessive alcohol consumption, exposure to toxins, viral infections and bile duct obstruction prevention could cause hepatic injury.8 Viral agents such as HBV, HCV and HEV are common causes of varying degrees of hepatic insufficiency.9–11 Furthermore, some reports demonstrated that SARS-infected patients and MERS-infected patients had an increased value of liver enzyme and various degrees of hepatic injury.12,13 In our study, we found that 41 of 239 COVID-19 patients had higher values of liver enzymes (e.g. ALT and AST). Similarly to our study, in recent studies, researchers revealed that transaminases (e.g. ALT and AST) were increased in patients with COVID-19.14,16 Chen et al16 demonstrated that 43 of 99 COVID-19 patients had various liver enzyme abnormalities (i.e. ALT and AST) and one patient had severe increase hepatic enzyme (ALT 7590 U/L, AST 1445 U/L) leading to hepatic dysfunction. Moreover, our results showed that the LDH value was increased in COVID-19 patients, as well as being significantly increased in patients with elevated ALT in comparison to patients with normal ALT. These results are consistent with other studies7,14,21,22 and this phenomenon may be due to the cell apoptosis induced by COVID-19 infection or to the use of antiviral compounds. Some studies suggested that the increased levels of LDH are an indicator for evaluating anti-influenza activity of antiviral compounds.23,24 Also, Mori et al23 suggested that influenza virus-infected cells are responsible for the LDH leakage due to releasing virus particles from host cells because antiviral drugs such as ribavirin, carbodine, and 3-deazaguanine pyrazofurine inhibited the LDH leakage. Uchide et al25 also suggested that the apoptosis cell degeneration induced by influenza virus infection is associated with increasing LDH value. In addition, LDH is one of the diagnostic markers of lung diseases and liver diseases. Therefore, a significant increase in LDH values in patients with elevated ALT may be due to the simultaneous involvement of lungs and liver.
CRP, as an inflammatory response to factors released by macrophages and adipocytes, is produced in the liver.26 In the present study, an increase of CRP was found in almost 80% of COVID-19 patients. Similarly to patients with other coronaviruses such as avian flu H7N9 and H1N1 influenza strains,27,28 CRP is increased in COVID-19 patients, and researchers reported that increased CRP is an observed clinical characteristic of most patients with COVID-19 infection.16,29,30 Additionally, we found that there were no differences in CRP values between the elevated ALT group and the normal ALT group. In addition, CRP values were not significantly associated with ALT and AST. This indication was consistent with Guan et al31 and Li et al14 who found the abnormal rate of ALT and AST among COVID-19 patients. While, inconsistent with our results, Li et al14 found that the CRP values were closely associated with hepatic injury in COVID-19 patients, and CRP was significantly higher in the elevated ALT group and the increase of CRP was associated with ALT level. These differences may be the result of a large number of samples or of using a lower-sensitivity diagnostic CRP kit in our study. Furthermore, Zhao et al32 suggested that ACE2 is the putative receptor of SARS-CoV2. Additionally, Chai et al17 demonstrated that specific ACE2 expressed in the liver as well as in the lungs may cause hepatic injury in COVID-19 patients. Some other studies suggested that the systemic inflammatory response to the drug used in the treatment of COVID-19 infection and pneumonia-associated hypoxia may be caused by a hepatic injury in COVID-19 patients.30,33,34 According to the studies of Xu et al33 and Zhang et al,30 distinguishing between the pathological report of hepatic dysfunctions caused by a drug used in the treatment or caused by COVID-19 infection is difficult because some of the patients had a regime of lopinavir/ritonavir and interferon α-2b.
There were some limitations in this study, including some of the patients who died due to COVID-19 infection, owing to overloading of patients with COVID-19, assessment of other risk factors and conditions that may be changed in following up was not possible. Therefore, we focused on risk factors that are presented in the early identification of hepatic injuries. We expect these results could help medical settings to manage hepatic injury caused by COVID-19 infection.
Conclusion
These results suggested that hepatic injury and abnormal values of liver enzymes related to COVID-19 infection is an acute non-specific inflammation alteration. In addition, elevation of liver enzymes may be related to general immune activation and cytokine storming.
Abbreviations
CBC, complete blood count; COVID-19, coronavirus disease 2019; CPK, creatine phosphokinase; CRP, C-reactive protein; HBV, hepatitis B virus; HCV, hepatitis C virus; HEV, hepatitis E virus; HIS, hospital information system; LDH, lactate dehydrogenase; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; STDEV, standard deviation.
Acknowledgments
This study was supported by Tabriz University of Medical Sciences with grant number 65174. Study was approved by the National Ethic Committee of the Ministry of Health, Islamic Republic of Iran with reference number IR.TBZMED.REC.1398.1277 and this study was conducted in accordance with the Declaration of Helsinki. All participants filled informed consent and forms are available from all participants. We thank all staff of Imam Reza Hospital for all they did during the COVID-19 pandemic and in memorial of all our colleagues who lost their lives during this pandemic.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fathizadeh H, Maroufi P, Momen-Heravi M, et al. Protection and disinfection policies against SARS-CoV-2 (COVID-19). Infez Med. 2020;28(2):185–191.
2. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
3. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet. 2020;395(10223):470–473. doi:10.1016/S0140-6736(20)30185-9
4. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574. doi:10.1016/S0140-6736(20)30251-8
5. Lai -C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
6. Ozma MA, Maroufi P, Khodadadi E, et al. Clinical manifestation, diagnosis, prevention and control of SARS-CoV-2 (Covid-19) during the outbreak period. Infez Med. 2020;28(2).
7. Chang D, Lin M, Wei L, et al. Epidemiologic and clinical characteristics of novel coronavirus infections involving 13 patients outside Wuhan, China. JAMA. 2020;323(11):1092. doi:10.1001/jama.2020.1623
8. Guicciardi M, Gores GJ. Apoptosis: a mechanism of acute and chronic liver injury. Gut. 2005;54(7):1024–1033. doi:10.1136/gut.2004.053850
9. Tang LS, Covert E, Wilson E, Kottilil S. Chronic hepatitis B infection: a review. JAMA. 2018;319(17):1802–1813. doi:10.1001/jama.2018.3795
10. Tseng T-C, Liu C-J, Chang CT, et al. HEV superinfection accelerates disease progression in patients with chronic HBV infection and increases mortality in those with cirrhosis. J Hepatol. 2020;72(6):1105–1111. doi:10.1016/j.jhep.2020.01.012
11. Nguyen L, Nguyen M. Systematic review: asian patients with chronic hepatitis C infection. Aliment Pharmacol Ther. 2013;37(10):921–936. doi:10.1111/apt.12300
12. Chau TN, Lee KC, Yao H, et al. SARS‐associated viral hepatitis caused by a novel coronavirus: report of three cases. Hepatology. 2004;39(2):302–310. doi:10.1002/hep.20111
13. Lee JY, Kim Y-J, Chung EH, et al. The clinical and virological features of the first imported case causing MERS-CoV outbreak in South Korea, 2015. BMC Infect Dis. 2017;17(1):498. doi:10.1186/s12879-017-2576-5
14. Li L, Li S, Xu M, et al. The level of plasma C-reactive protein is closely related to the liver injury in patients with COVID-19. medRxiv. 2020.
15. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious diseases society of America/American thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Supplement_2):S27–S72.
16. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
17. Chai X, Hu L, Zhang Y, et al. Specific ACE2 expression in cholangiocytes may cause liver damage after 2019-nCoV infection. bioRxiv. 2020.
18. Johnston DE. Special considerations in interpreting liver function tests. Am Fam Physician. 1999;59(8):2223.
19. Yap CY, Aw TC. Liver function tests (LFTs). Proc Singapore Healthc. 2010;19(1):80–82. doi:10.1177/201010581001900113
20. Dufour DR, Lott JA, Nolte FS, Gretch DR, Koff RS, Seeff LB. Diagnosis and monitoring of hepatic injury. II. Recommendations for use of laboratory tests in screening, diagnosis, and monitoring. Clin Chem. 2000;46(12):2050–2068. doi:10.1093/clinchem/46.12.2050
21. Yang W, Cao Q, Qin L, et al. Clinical characteristics and imaging manifestations of the 2019 novel coronavirus disease (COVID-19): a multi-center study in Wenzhou city, Zhejiang, China. J Infect. 2020;80(4):388–393. doi:10.1016/j.jinf.2020.02.016
22. Ju C-R, Lian Q-Y, Zhang J-H, et al. Recommended prophylactic and management strategies for severe acute respiratory syndrome coronavirus 2 infection in transplant recipients. Chronic Dis Transl Med. 2020. doi:10.1016/j.cdtm.2020.02.003
23. Mori S, Watanabe W, Shigeta S. A colorimetric LDH assay for the titration of infectivity and the evaluation of anti-viral activity against ortho-and paramyxoviruses. Tohoku J Exp Med. 1995;177(4):315–325. doi:10.1620/tjem.177.315
24. Watanabe W, Sudo K, Asawa S, Konno K, Yokota T, Shigeta S. Use of lactate dehydrogenase to evaluate the anti-viral activity against influenza A virus. J Virol Methods. 1995;51(2–3):185–191. doi:10.1016/0166-0934(94)00103-N
25. Uchide N, Ohyama K, Bessho T, Toyoda H. Lactate dehydrogenase leakage as a marker for apoptotic cell degradation induced by influenza virus infection in human fetal membrane cells. Intervirology. 2009;52(3):164–173. doi:10.1159/000224644
26. Lau DC, Dhillon B, Yan H, Szmitko PE, Verma S. Adipokines: molecular links between obesity and atherosclerosis. Am J Physiol Heart Circ Physiol. 2005;288(5):H2031–H2041. doi:10.1152/ajpheart.01058.2004
27. Wu W, Shi D, Fang D, et al. A new perspective on C-reactive protein in H7N9 infections. Int J Infect Dis. 2016;44:31–36. doi:10.1016/j.ijid.2016.01.009
28. Vasileva D, Badawi A. C-reactive protein as a biomarker of severe H1N1 influenza. Inflamm Res. 2019;68(1):39–46. doi:10.1007/s00011-018-1188-x
29. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061. doi:10.1001/jama.2020.1585
30. Zhang J, Zhou L, Yang Y, Peng W, Wang W, Chen X. Therapeutic and triage strategies for 2019 novel coronavirus disease in fever clinics. Lancet Res Med. 2020;8(3):e11–e12. doi:10.1016/S2213-2600(20)30071-0
31. Guan W-J, Ni Z-Y, Hu Y, et al. Clinical characteristics of 2019 novel coronavirus infection in China. MedRxiv. 2020.
32. Zhao Y, Zhao Z, Wang Y, Zhou Y, Ma Y, Zuo W. Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov. BioRxiv. 2020.
33. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
34. Zhang C, Shi L, Wang F-S. Liver injury in COVID-19: management and challenges. Lancet Gastroenterol Hepatol. 2020;5(5):428–430. doi:10.1016/S2468-1253(20)30057-1
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.