")
Back to Journals » Open Access Journal of Sports Medicine » Volume 14
All-Arthroscopic Refixation of an Osteochondral Femoral Avulsion of the Anterior Cruciate Ligament with a Laxity-Minimizing Suture
Authors Horstmann H , Karkosch R, Plagge J, Smith T, Petri M
Received 28 December 2022
Accepted for publication 14 April 2023
Published 3 May 2023 Volume 2023:14 Pages 21—27
DOI https://doi.org/10.2147/OAJSM.S397512
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Hauke Horstmann, Roman Karkosch, Jochen Plagge, Tomas Smith, Maximilian Petri
Department of Orthopedic Surgery, Hannover Medical School, Hannover, Germany
Correspondence: Hauke Horstmann, Anna-von-Borries-Straße 1-7, Hannover, 30625, Germany, Tel +49 511 5354 568, Fax +49 511 5354 685, Email [email protected]
Purpose: Torn anterior cruciate ligaments in children are rare injuries. The incidence of concomitant avulsion fracture in the skeletally immature patient is high. Reports of arthroscopic reconstruction in the literature are sparse.
Case Presentation: We present the case of a femoral avulsion fracture of the anterior cruciate ligament in a seven-year-old girl. The patient underwent arthroscopic refixation with DynacordTM Suture and Suture Button. At a follow-up of 8 weeks, the patient had free range of motion and a stable knee, with a negative Lachman- and Pivot-Shift-test in particular.
Conclusion: Refixation of femoral avulsion fracture can lead to good results. Open physes and size of the knee should be taken into account. Anatomic reconstruction is compulsory to receive bone on bone healing.
Keywords: anterior cruciate ligament, femoral avulsion, arthroscopy, refixation
Introduction
Insufficient anterior cruciate ligaments (ACL) in skeletally immature patients are rare. The incidence of this injury is 1–3.4%.1 Whereas the literature presents a number of studies on tibial insertional avulsions, reports on the uncommon femoral fracture site are seldom.2–5 Operative techniques vary from arthrotomy with suture refixation6 to arthroscopic retrograde K-wire fixation.7 Furthermore, some of these case reports lack in precise illustration of surgical technique options.
This case report presents an all-arthroscopic refixation of an osteochondral femoral avulsion of the anterior cruciate ligament with a laxity-minimizing suture to prevent secondary elongation.
Case Presentation
A seven-year-old girl had a trauma with twisting her left knee. She had pain, swelling and instability. The patient used crutches. The knee had an extension deficit of 15° with flexion up to 70°. Knee examination revealed a grade two Lachman and anterior drawer test with a soft endpoint. No valgus- or varus-instability was examined. Initial anteroposterior and lateral radiographs were inconspicuous. Magnetic resonance imaging (MRI) revealed a displaced femoral avulsion fracture of the ACL (Figure 1). The physes presented unfused.
 |
Figure 1 MRI, coronal (a) and sagittal (b) plane; the black arrow marks the femoral avulsion. |
The patient and parents were consented for an arthroscopic procedure with refixation of the avulsion with or without meniscal repair. Surgery was performed 18 days after trauma.
Examination under anesthesia confirmed a grade two positive Lachman and anterior drawer test with a soft endpoint as well.
Setup: The patient was positioned supine with the leg placed in a static leg holder flexed to 90°. A tourniquet of 150 mm Hg was used after exsanguinating the leg.
Portals: An anterolateral viewing portal, an anteromedial working portal and a far medial drilling portal were created in vertical direction.
Diagnostic arthroscopy: Diagnostic arthroscopy was performed. An unstable vertical longitudinal tear of the lateral meniscus in the posterior horn was detected. The ACL was proved to be lax with the expected femoral avulsion (Figures 2 and 3). The medial meniscus as well as the posterior cruciate ligament (PCL) was intact. No cartilage defect was observed.
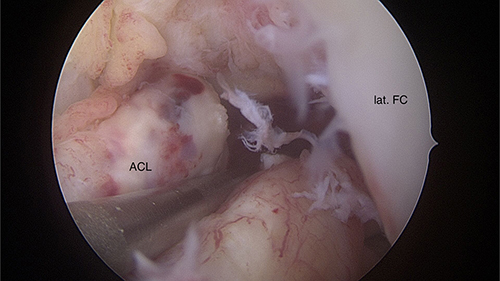 |
Figure 2 Arthroscopy, notch; ACL tear. |
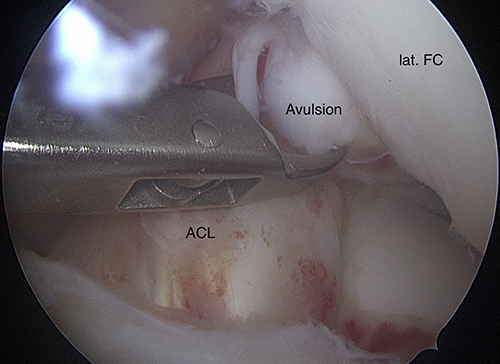 |
Figure 3 Arthroscopy, notch; ACL avulsion. |
Lateral meniscus repair: An all-inside meniscal repair system (TruespanTM, DePuy Mitek Inc., Raynham, USA) was used for fixation of the lateral meniscus.
ACL avulsion refixation: The femoral ACL insertion site was debrided using a 4.0 curved shaver (Arthrex, Naples, FL, USA). Using a 5.5 mm offset drilling guide, a beath pin was inserted at the anatomic femoral insertion site of the ACL via the anteromedial portal (Figure 4). Fluoroscopy was used to ensure appropriate positioning of the transphyseal pin.8 Using an arthroscopic lasso, 2 strands of No. 2 DynacordTM (DePuy Mitek, Raynham, MA, USA) non-absorbable sutures were shuttled through the proximal part of the ACL stump (Figure 5). The strands were passed through the beath pin tunnel. A 3 cm longitudinal incision was performed at the distal lateral femur, the iliotibial band was split longitudinally, and the suture strands were retrieved. The knee was placed into 20° of flexion, and the sutures were then tied over a suture button (Arthrex, Naples, FL, USA) under direct arthroscopic visualization of the ACL stump. At this point, subtle manipulation of the avulsed osteochondral fragment was performed with a probe and arthroscopic forceps to ensure anatomic reduction of the fragment into its original site (Figures 6 and 7). No redon drainage was used.
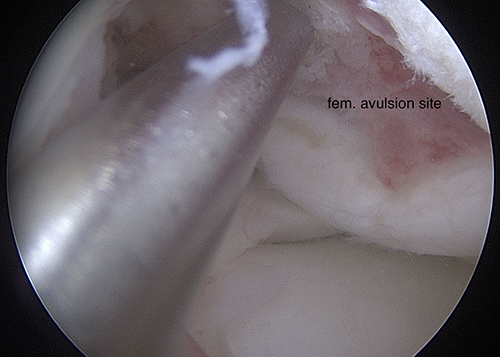 |
Figure 4 Arthroscopy, notch; femoral avulsion site. |
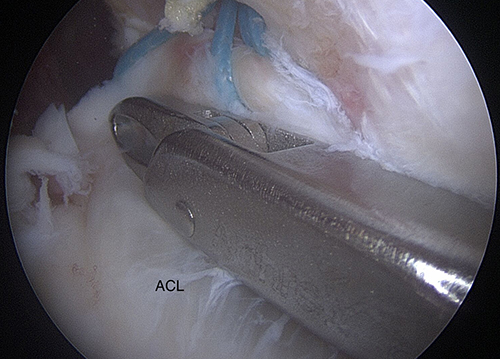 |
Figure 5 Arthroscopy, notch; ACL avulsion looped with DynacordTM suture. |
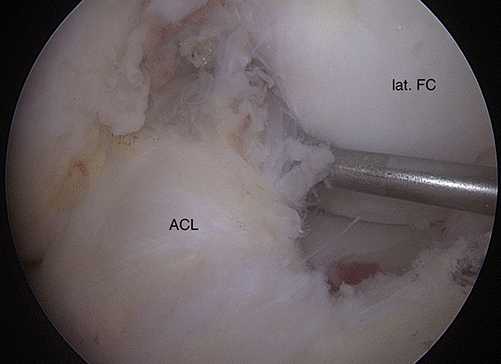 |
Figure 6 Arthroscopy, notch; anatomically reducted ACL. |
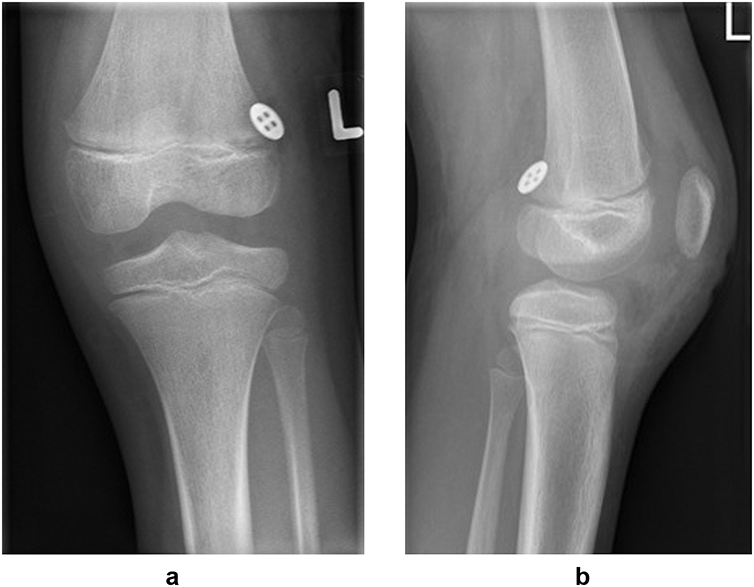 |
Figure 7 Postoperative x-ray, coronal (a) and sagittal (b) plane. |
No intra- or postoperative complications occurred. The patient was mobilized with partial weight bearing using crutches and a hinged knee brace. Range of motion limitation was set to 0° extension for three days postoperatively and then 0°/0°/80° (extension/flexion) until the second postoperative week. Between the third and sixth postoperative week we recommended 0°/0°/90° limitation in the hinged brace. Partial weight-bearing recommendations were: sole contact for the first week, half a body weight for the second week and pain adapted full body weight-bearing for the third and fourth week.
At the first follow-up exam at eight weeks postoperatively, the patient had a stable knee with a negative Lachman and negative anterior drawer test. Range of motion showed 120° of flexion with full extension.
The seven months follow up MRI scan shows complete healing of the avulsion and the meniscal tear. The growth plates proof to be intact. No further bone marrow enhancement is evident.
Discussion
Avulsion fractures of the anterior cruciate ligament are rare injuries, accounting for about 7% in children and adolescents.9 Literature about surgical techniques and outcomes is sparse. A variety of surgical techniques have been proposed, starting from extensive arthrotomy approaches3,4,6,10,11 over to arthroscopic techniques2,7,12,13 (Table 1).
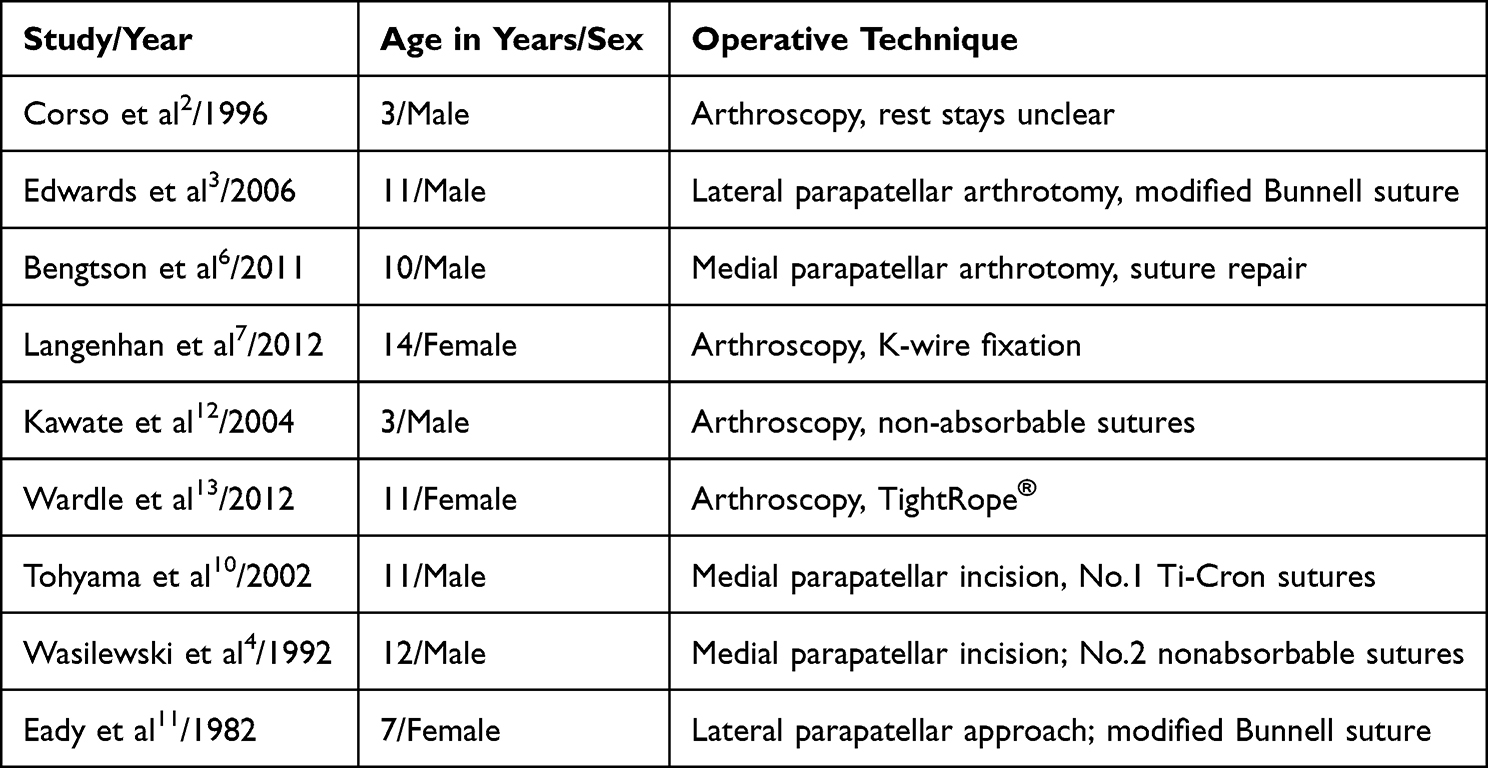 |
Table 1 Literature on Surgical Techniques and Outcomes |
The long-term outcome of the described techniques remains unknown. In particular, secondary elongation due to early loosening of the utilized suture materials persists a matter of concern. In ACL reconstruction, secondary elongation resulting in graft failure is a common problem.14–17 In addition, growth disturbance with the used technique cannot yet be predicted. Nevertheless, our technique including transphyseal drilling is supported by the current literature.8
The ideal suture for refixation remains a matter of debate. The DynacordTM suture (DePuy Mitek, Raynham, MA, USA) was launched in 2018 with the initial goal to improve fixation strength in rotator cuff repair. It was developed when a failure of repair was observed in about 20% of the cases due to a loss of suture tension, causing gap formation and precluding the soft tissue from healing to the bony insertion site.18
In an in vivo ovine shoulder model, gap formation with this laxity-minimizing suture was half of the size of the standard suture. In addition, no local tissue damage (cut-through) was observed.19
Arthroscopy provides excellent visualization of the injury, while at the same time allowing for thorough exam of the joint for accompanying injuries. In this particular case, a vertical tear of the posterior horn of the lateral meniscus was detected and repaired with an all-inside suture device (TruespanTM, DePuy Mitek, Raynham, MA, USA).
The technique described here offers the advantages of an all-arthroscopic procedure and a sustainable femoral fixation using high-strength laxity-minimizing sutures.
Conclusion
All-arthroscopic refixation of femoral avulsion injury of the ACL has the potential to restore anatomic joint kinematics and to yield excellent clinical results. Transosseous refixation with extra-epiphyseal button fixation minimizes the risk for growth disturbance. The use of a dynamically shortening suture might be helpful to prevent early gap formation, which might lead to clinical failure.
Clinical Message
This case report illustrates precisely an all-arthroscopic refixation of an osteochondral femoral avulsion of the anterior cruciate ligament with a laxity-minimizing suture to prevent secondary elongation.
Abbreviations
ACL, Anterior cruciate ligament; MRI, Magnetic resonance imaging; Lat. FC, Lateral femur condyle; PCL, Posterior cruciate ligament.
Consent to Publish
The patient and caregiver gave written informed consent to publish the case details and any accompanying images. No further institutional approval was required to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Fehnel DJ, Johnson R. Anterior cruciate injuries in the skeletally immature athlete: a review of treatment outcomes. Sports Med. 2000;29(1):51–63. doi:10.2165/00007256-200029010-00005
2. Corso SJ, Whipple TL. Avulsion of the femoral attachment of the anterior cruciate ligament in a 3-year-old boy. Arthroscopy. 1996;12(1):95–98. doi:10.1016/S0749-8063(96)90227-3
3. Edwards MR, Terry J, Gibbs J, Bridle S. Proximal anterior cruciate ligament avulsion fracture in a skeletally immature athlete: a case report and method of physeal sparing repair. Knee Surg Sports Traumatol Arthrosc. 2007;15(2):150–152. doi:10.1007/s00167-006-0154-2
4. Wasilewski SA, Frankl U. Osteochondral avulsion fracture of femoral insertion of anterior cruciate ligament. case report and review of literature. Am J Sports Med. 1992;20(2):224–226. doi:10.1177/036354659202000224
5. Mhaskar VA, Mahehswari J, Sansanwal M. Femoral avulsion of the anterior cruciate ligament in a multiligament setting: a unique case. Knee Surg Relat Res. 2019;31(2):137–142. doi:10.5792/ksrr.18.065
6. Bengtson H, Giangarra C. Osteochondral avulsion fracture of the anterior cruciate ligament femoral origin in a 10-year-old child: a case report. J Athl Train. 2011;46(4):451–455. doi:10.4085/1062-6050-46.4.451
7. Langenhan R, Baumann M, Hohendorff B, Probst A, Trobisch P. Arthroscopically assisted reduction and internal fixation of a femoral anterior cruciate ligament osteochondral avulsion fracture in a 14-year-old girl via transphyseal inside-out technique. Strategies Trauma Limb Reconstr. 2013;8(3):193–197. doi:10.1007/s11751-013-0175-6
8. Pierce TP, Issa K, Festa A, Scillia AJ, McInerney VK. Pediatric anterior cruciate ligament reconstruction: a systematic review of transphyseal versus physeal-sparing techniques. Am J Sports Med. 2017;45(2):488–494. doi:10.1177/0363546516638079
9. Angel KR, Hall DJ. Anterior cruciate ligament injury in children and adolescents. Arthroscopy. 1989;5(3):197–200. doi:10.1016/0749-8063(89)90171-0
10. Tohyama H, Kui K, Yasuda K. Avulsion fracture at the femoral attachment of the anterior cruciate ligament after intercondylar eminence fracture of the tibia. Am J Sports Med. 2002;30(2):279–282. doi:10.1177/03635465020300022201
11. Eady JL, Cardenas CD, Sopa D. Avulsion of the femoral attachment of the anterior cruciate ligament in a seven-year-old child. A case report. J Bone Joint Surg Am. 1982;64(9):1376–1378. doi:10.2106/00004623-198264090-00017
12. Kawate K, Fujisawa Y, Yajima H, Sugimoto K, Tomita Y, Takakura Y. Avulsion of the cartilaginous femoral origin of the anterior cruciate ligament in a three-year-old child. A case report with a thirteen-year follow-up. J Bone Joint Surg Am. 2004;86(8):1787–1792. doi:10.2106/00004623-200408000-00026
13. Wardle NS, Haddad FS. Proximal anterior cruciate ligament avulsion treated with TightRope(R) fixation device. Ann R Coll Surg Engl. 2012;94(2):e96–8. doi:10.1308/003588412X13171221589216
14. Ettinger M, Karkosch R, Horstmann H, et al. Biomechanical properties of adjustable extracortical graft fixations in ACL reconstruction. J Exp Orthop. 2018;5(1):41. doi:10.1186/s40634-018-0154-4
15. Boyle MJ, Vovos TJ, Walker CG, Stabile KJ, Roth JM, Garrett WE. Does adjustable-loop femoral cortical suspension loosen after anterior cruciate ligament reconstruction? A retrospective comparative study. Knee. 2015;22(4):304–308. doi:10.1016/j.knee.2015.04.016
16. Petre BM, Smith SD, Jansson KS, et al. Femoral cortical suspension devices for soft tissue anterior cruciate ligament reconstruction: a comparative biomechanical study. Am J Sports Med. 2013;41(2):416–422. doi:10.1177/0363546512469875
17. Barrow AE, Pilia M, Guda T, Kadrmas WR, Burns TC. Femoral suspension devices for anterior cruciate ligament reconstruction: do adjustable loops lengthen? Am J Sports Med. 2014;42(2):343–349. doi:10.1177/0363546513507769
18. Ladermann A, Denard PJ, Burkhart SS. Management of failed rotator cuff repair: a systematic review. J ISAKOS. 2016;1(1):32–37. doi:10.1136/jisakos-2015-000027
19. Favorito PJ, Spenciner DB, Muench TR, Bartrom J, Ryu RK. Safety evaluation of a laxity-minimizing suture at 5 days and 6 weeks after repair of a sheep infraspinatus tendon. J Shoulder Elbow Surg. 2019;28(1):164–169. doi:10.1016/j.jse.2018.05.043
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.