")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 11
Alemtuzumab for the treatment of multiple sclerosis
Authors Willis M, Robertson N
Received 31 December 2014
Accepted for publication 16 January 2015
Published 31 March 2015 Volume 2015:11 Pages 525—534
DOI https://doi.org/10.2147/TCRM.S80112
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Mark D Willis, Neil P Robertson
Institute of Psychological Medicine and Clinical Neuroscience, Cardiff University, University Hospital of Wales, Heath Park, Cardiff, UK
Abstract: Alemtuzumab is an anti-CD52 monoclonal antibody, recently approved for the treatment of active, relapsing multiple sclerosis (MS). Administration of alemtuzumab causes a rapid and dramatic reduction in circulating lymphocytes, with a predictable subsequent pattern of immune reconstitution. Although the precise mode of action remains unclear, treatment results in a marked reduction in annualized relapse rates, slowing of disability progression compared with an active comparator, and may even cause disability reversal. Although conferring clear clinical benefits, alemtuzumab carries a significant long-term risk of autoimmune disease (AID), which has a particular predilection for the thyroid gland, although a wide range of other disorders have also been reported. However, risks of AID can usually be anticipated and treated successfully, provided rigorous monitoring and surveillance protocols are followed by clinicians and patients alike. Despite its immunosuppressive mechanism of action serious infections are rare and malignancies commonly associated with immunodeficiency have not been observed to date. Alemtuzumab’s unique mode of administration, as well as it’s durability of effect, provides an important addition to currently available therapeutic interventions for MS, and in particular is a valuable treatment option in recent onset and highly active relapsing disease.
Keywords: multiple sclerosis, alemtuzumab, autoimmune disease
Introduction
Multiple sclerosis (MS) is a common inflammatory, demyelinating disease of the central nervous system (CNS)1 with a worldwide prevalence of approximately 2.5 million2 and an estimated lifetime cost per individual of $2.2 million.3 Reported disease prevalence is gradually increasing4 and there is an urgent need for treatments which are both safe and efficacious. Genome wide association studies have implicated genes involved in T-lymphocyte function and cell-mediated immunity in disease pathogenesis.5,6 The mode of action of currently available drugs has generally been targeted at these aspects of the immune system by modulating lymphocyte function,7,8 affecting lymphocyte trafficking,9 or depleting lymphocyte numbers.10 The main impact of these drugs has been directed toward markers of inflammation during the earlier relapsing phase of disease by reducing frequency of clinical relapse as well as surrogate radiological markers of inflammation. However, the long-term aspiration is that this strategy will also eventually result in the prevention of long-term disability progression. There is a now a steady stream of new drugs being licensed and approved for use in MS, but despite their demonstrable efficacy in reducing relapse rates and radiological indicators of disease, their effect on disease progression and disability has been less striking.
Alemtuzumab is an anti-CD52 humanized monoclonal antibody recently licensed for the treatment of active MS in the European Union,11 Canada,12 Australia,13 Brazil,14 Mexico,15 the UK,16 and was also approved for use in the US in November 2014 after a controversial initial rejection.17,18 Clinical trials have demonstrated superior efficacy against an active comparator (interferon beta-1a) and uniquely for drugs used in the treatment of MS, some data have shown a pattern of disability reversal.10,19,20 In this review, we aim to summarize the mechanism of action of alemtuzumab, its clinical efficacy and side effect profile and speculate on its role in the ever-expanding landscape of MS therapeutics.
Overview of pharmacology
Approximately 5% of the cell surface of lymphocytes is covered with CD52, a 12 amino acid glycosylated glycosylphosphatidylinositol-linked protein. Monocytes, macrophages, eosinophils, and NK cells also express CD52, albeit at lower levels, as well as epithelial cells lining the epididymis, vas deferens, and seminal vesicle.21–23 The function of CD52 is largely unknown but is thought to contribute to T-cell activation,24 migration,25 and the induction of regulatory T-cells.25 Hematopoietic precursors lack CD52, which is an important factor in allowing lymphocyte reconstitution following treatment.26
Alemtuzumab was initially developed to treat fludarabine-resistant chronic lymphocytic leukemia but has also been utilized in other autoimmune disorders and transplantation.27 Alemtuzumab has complex pharmacokinetics but appears to undergo rapid initial clearance, which is dependent on peripheral lymphocyte load.28 Clearance of the drug is reduced with repeated administrations29 and antibodies can develop, which may become problematic after multiple doses.28,29 The use of SM3, a non-cell-binding variant given prior to treatment with alemtuzumab has been suggested as a potential solution to the problem of neutralizing antibodies but its use has yet to reach standard clinical practice.28
Treatment with alemtuzumab results in a rapid and dramatic reduction in circulating lymphocytes, with a subsequent preferential reconstitution of the immune system.30 This is thought to occur as a result of antibody dependent cell-mediated cytotoxicity.31 The rate of lymphocyte reconstitution varies amongst individuals but accelerated lymphocyte recovery is not thought to reliably predict disease activity.32–34 In particular, B-cells recover quickest (due to B-cell activating factor [BAFF]),35 followed by CD8+ and CD4+ T-lymphocytes.32,35,36 Interestingly, for a few months following treatment, regulatory CD4+ T-cells dominate the T-cell repertoire37–39 and it is thought this alteration to the inflammatory milieu is likely to be responsible for the improved long-term outcomes in patients treated with alemtuzumab, rather than the shorter term immunodeficiency. The paucity of opportunistic infections seen in treated patients would also appear to support this observation.10,19,20
Clinical application
When used in the context of MS, alemtuzumab is administered intravenously at a dose of 12 mg/day (d) for 5 consecutive days, with a further 3-day course 12 months later. In order to negate the cytokine release effect of monoclonal antibody treatment, patients are preadministered with 1 g of intravenous methylprednisolone for the first 3 days of each treatment course. Within clinical trials, patients were retreated with a subsequent 3-day course of alemtuzumab if they experienced ≥1 protocol-defined relapse or ≥2 new or enlarging brain or spinal cord lesions.40 In clinical practice, retreatment with a further 3-day course is often applied if a clinical relapse or new radiological disease activity is observed, although the precise boundaries of relapse characteristics or other markers of disease activity which may prompt retreatment have yet to be defined.
Clinical efficacy
Early experience
The early experience of using alemtuzumab in MS not only led to its eventual availability as a therapeutic agent, but also provided useful information concerning overall disease pathogenesis. Its first use as a treatment in MS was in patients with progressive disease and despite an observed reduction in magnetic resonance imaging (MRI) lesion load,41,42 these patients continued to accumulate disability, with increasing cerebral atrophy noted 7 years after treatment induction.27,43 Conversely, patients with relapsing disease were noted to have had a reduction in annualized relapse rates and improved disability.27,43 These observations led to the now well established theory that MS is characterized by an early, inflammatory demyelinating phase manifesting clinically as relapses, with a subsequent axonal, degenerative phase which is largely responsible for accumulation of longer term disability. It was therefore hypothesized that, in order to prevent or slow the inevitable migration from inflammation to neurodegeneration, patients would need early, effective and prompt treatment in order to suppress an otherwise perpetuating aberrant immune response.42,43 Two open-label studies based on this principle subsequently confirmed its beneficial effect on relapse rates and disability outcomes in relapsing MS patients who were treatment naïve or who had failed beta-interferon treatment.44,45
Clinical trials (CAMMS223, CARE-MSI, and CARE-MSII)
Following the encouraging results of the early experience with alemtuzumab, one Phase II trial (CAMMS223)10 and two Phase III trials (CARE-MSI and CARE-MSII) were undertaken.19,20 CAMMS223 compared low- and high-dose alemtuzumab against an active comparator (high dose interferon beta-1a) in patients with early, active, relapsing-remitting MS (RRMS)10 – the first time in MS drug trials that an active comparator had been employed. The subsequent Phase III trials investigated the use of alemtuzumab with relapsing MS in treatment naïve patients (CARE-MSI)20 and in those patients who had previously been treated with alternative disease modifying therapies (DMTs) (CARE-MSII).19 The main clinical outcomes and adverse events from these trials are summarized in Table 1.
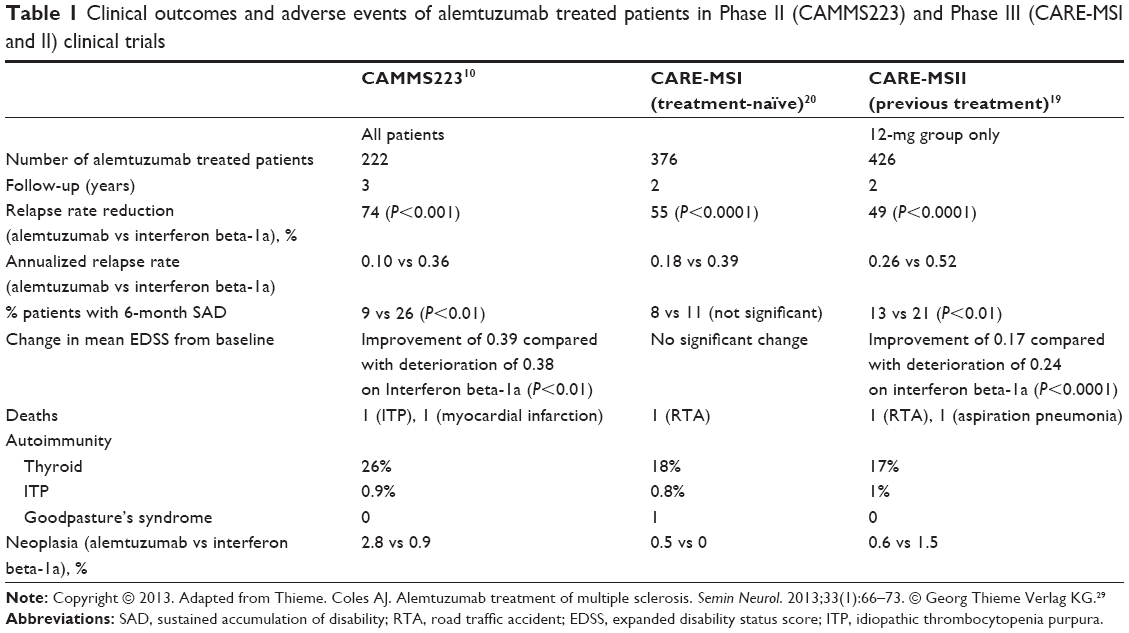 | Table 1 Clinical outcomes and adverse events of alemtuzumab treated patients in Phase II (CAMMS223) and Phase III (CARE-MSI and II) clinical trials |
CAMMS223
In CAMMS223, 334 patients with a diagnosis of RRMS according to the 2001 McDonald criteria,46 disease onset less than 36 months before screening, at least two clinical episodes during the previous 2 years, an expanded disability status score (EDSS)47 of 3.0 or less, and one or more enhancing lesions on MRI10 were included. Patients were randomized to either alemtuzumab 12 mg/d, alemtuzumab 24 mg/d, or high dose (44 μg) subcutaneous interferon beta-1a three times weekly.10
Outcomes
The results from CAMMS223 were striking and showed alemtuzumab to be superior to interferon beta-1a in all outcome measures. In particular, pooling of the 12 and 24 mg alemtuzumab treatment groups, demonstrated a reduction in annualized relapse rates (ARR) of 74%, a reduction in the risk of sustained accumulation of disability (SAD; a ≥1-point increase in EDSS from baseline if baseline EDSS >0, or ≥1.5-point increase if baseline EDSS=0, persistent over a 6-month period) of 71%, and an improvement in mean EDSS score of 0.39 points at 36 months. This was in contrast to those patients receiving interferon beta-1a in whom the EDSS score worsened by 0.38 points over the same time period. Radiological outcomes were similarly impressive. Although all patients demonstrated a reduction in the volume of lesions on T2-weighted MRI, the reduction was more marked in the alemtuzumab groups, achieving significance at 12 and 24 months. However, no significant difference was observed at 36 months. Reduction in brain volume was also significantly less in the pooled alemtuzumab treatment group.10 Further analysis of this cohort of patients over 5 years of follow-up has demonstrated that the improvements seen in EDSS persist up to this point, although this is largely achieved within the first 36 months.48 Additional post-hoc analysis exploring a new measure of disability; sustained reduction of disability (SRD; a reduction from baseline of at least 1 EDSS point confirmed over 6 months for patients with a baseline EDSS ≥2.0) demonstrated significantly more patients achieving this outcome in the alemtuzumab-treated group compared with patients given interferon beta-1a.49
CARE-MSI and CARE-MSII
The two Phase III trials, CARE-MSI and CARE-MSII were each performed over a study period of 2 years with the primary endpoints of annualized relapse rate and time to 6-month SAD. CARE-MSI and CARE-MSII involved treatment-naïve patients with RRMS and patients who had active disease despite conventional disease-modifying therapy respectively. Treatment-naïve patients in CARE-MSI were randomly assigned either alemtuzumab 12 mg/d for 5 consecutive days followed 12 months later by a further 3-day course, or SC interferon beta-1a 44 μg three times weekly.20 Patients in CARE-MSII received either 12 or 24 mg alemtuzumab or interferon beta-1a.19 One year after CARE-MSII commenced, patients were only randomized to alemtuzumab 12 mg or interferon beta-1a.19
Outcomes
As with the Phase II trial, CAMMS223, patients experienced a reduction in annualized relapse rate compared with the interferon beta-1a group, albeit at a more modest 55% reduction in CARE-MSI and 49% in CARE-MSII.19,20 As with the Phase II study, CARE-MSII also demonstrated a significant improvement in the EDSS score compared with interferon beta-1a (improvement of 0.17 compared with a deterioration of 0.24 in the interferon beta-1a group) and significantly less patients who had SAD (13% vs 21%). In addition, significantly more patients achieved a SRD (22% vs 9%) in the alemtuzumab group.19,20 However, significance was not achieved in the disability outcomes in CARE-MSI with an improvement in EDSS score from baseline observed in both treatment groups.20
Differences were also observed in MRI outcomes between the two groups with gadolinium enhancing lesions, change in brain parenchymal fraction and patients with new or enlarging T2 hyperintense lesions being significantly lower in the alemtuzumab group in both Phase III studies.19,20 Recently presented data suggests that these MRI outcomes have been maintained at 3-year follow-up in both the CARE-MSI and CARE-MSII studies.50
Similarly, in the 3-year follow up extension studies of the CARE-MS cohorts, the majority of patients (CARE-MSI: 64% and CARE-MSII: 55%) have remained free of MS disease activity.50 The 4-year follow-up of CARE-MSI and CARE MS-II has also demonstrated good durability, with the majority of patients not requiring further therapy in the 2-year extension period.51,52 In addition, a reduction in annualized relapse rates was maintained and the majority of patients (CARE-MSI: 83%, CARE-MSII: 76%) did not experience a 6-month SAD.53
Long-term follow-up of open-label patients
More recently further data has been published by the Cambridge group regarding long-term outcomes (median 7-year follow-up) of 87 patients treated with alemtuzumab from two previous open-label studies. This study used the same outcome measures for disability but also utilized an area under the curve (AUC) model. Six-month SAD and SRD were observed in 32.2% and 43.5% of patients respectively. AUC analysis demonstrated 59.8% of patients had experienced an overall improvement or stabilization of disability. Mean EDSS reduction over the course of the study was −0.2 (pre, 3.8; post, 3.6). As in previous studies, mean ARR was drastically reduced by 91%.54 Of note, over a third of this study cohort was considered to have failed previous DMTs although outcomes were the same in treatment-naïve and treatment-experienced patients. Our own regional cohort, with a mean follow-up of 5.5 years has demonstrated a similarly impressive reduction in ARR of 88%. However, in contrast to the Cambridge group, we have thus far been unable to confirm a reversal in disability (Table 2).55
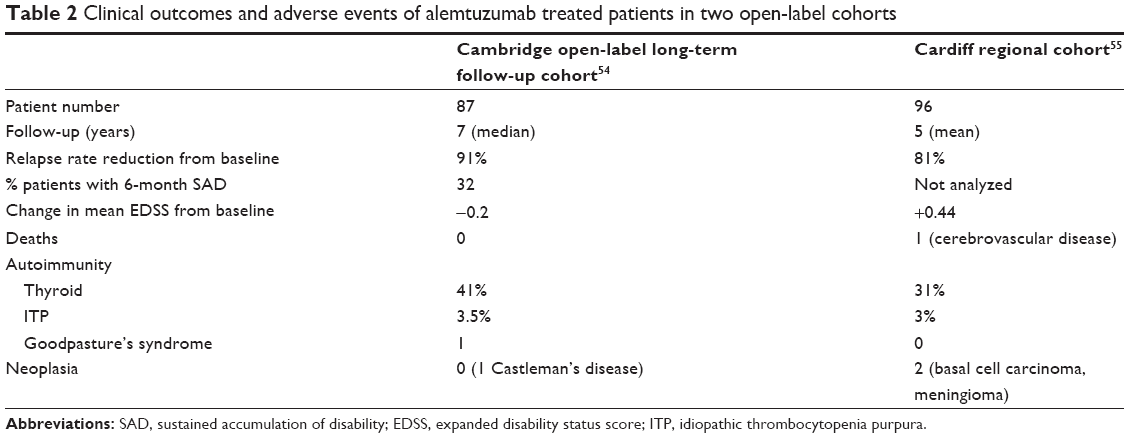 | Table 2 Clinical outcomes and adverse events of alemtuzumab treated patients in two open-label cohorts |
Adverse events
Autoimmune disease
The principal longer term adverse event related to alemtuzumab use in MS patients has been that of novel autoimmune disease (AID). The thyroid gland appears to be the most common target but other conditions such as idiopathic thrombocytopenic purpura (ITP), autoimmune hemolytic anemia, autoimmune neutropenia, and Goodpasture’s syndrome have also been recognized, although at much lower frequencies.10,19,20 It is not entirely understood why AID occurs following alemtuzumab therapy, although it has been suggested that it may be related to homeostatic T-cell proliferation after lymphocyte depletion.56 However, it does appear to be a largely disease-specific phenomenon since an increased frequency of autoimmune thyroid disease is not observed in patients with B-cell chronic lymphocytic leukemia. This would seem to suggest that there are specific factors associated with MS disease pathogenesis that play a role in AID expression in this context,57 and therefore may offer a unique insight into human autoimmunity.
In early studies, thyroid AID occurred in approximately 30% of patients.27,58 The subsequent clinical trials confirmed these rates with 23%, 18%, and 16% developing thyroid AID in CAMMS223, CARE-MSI, and CARE-MSII respectively.10,19,20 In a large, open-label, multicenter cohort of 248 patients, 17% of patients developed thyroid AID. In this group of patients 50% of AID occurred within 24 months of initial treatment. The risk of developing AID was unaffected by the cumulative dose, dosage interval, or dosage frequency suggesting that risk was acquired at the time of first treatment course.59 In the Cambridge open label long-term follow-up study, total AID occurred in 48% of treated patients with thyroid autoimmunity observed in 41% of patients. About 63% of these patients had Grave’s disease.54 Once again in this cohort, autoimmunity was not associated with the number of treatment cycles.54 Although these rates are higher than previously reported they probably reflect the longer follow-up time. Data available to date from the open-label extensions of the Phase III clinical trials also suggests that the safety profile does not appear to change with additional treatment courses.60,61
In addition to thyroid AID, other AID has been recognized. The second most common adverse AID, and perhaps the most concerning, has been ITP. CAMMS223 was suspended after three patients were diagnosed with ITP. One of these patients died of an intracerebral hemorrhage before an established diagnosis was made. Three further cases were diagnosed during the period of suspension.10 In the Phase III trials, the risk of developing ITP was approximately 1% within 2 years of treatment.19,20 In the large multicenter UK cohort, ITP was observed in 2% of patients59 and 3.5% in the Cambridge long-term follow-up cohort.54 Other forms of AID are rare but there have been four reported cases of glomerulonephritis secondary to anti-glomerular basement membrane antibodies (Goodpasture’s syndrome).20,43,62 In the future, those at risk of autoimmune adverse events may be able to be identified through the use of biomarkers, such as IL-21, which has been associated with the development of AID in one study, although technical difficulties have so far prevented further validation studies.63
Infections
Despite alemtuzumab having a profound effect on B- and T-cell populations, significant opportunistic infections are rarely seen. The reason for this is likely related to the relative preservation of the innate immune system and hematopoietic precursor cells in the bone marrow and thymus, and due to the fact that B- and T-lymphocyte populations are allowed to reconstitute in the months and years following infusion.26,64 In addition, the function of the remaining T- and B-lymphocytes is unimpaired and central memory, effector memory, and regulatory T-cells are depleted to a lesser extent than naïve T-cells, suggesting memory responses are unaffected by treatment.64
In data available from clinical trials, most infections were mild to moderate and responded to conventional therapies but were observed in 67%–77% patients in the Phase III trials receiving alemtuzumab at the 12 mg dose.19,20 The most common infections included nasopharyngitis, upper respiratory tract infections, urinary tract infections, herpes viral infections, sinusitis, and influenza.19,20 Spirochetal gingivitis, pyogenic granuloma, and listeria meningitis were the only infections observed in the open-label studies that may have been attributable to immunosuppression. All patients are now given dietary advice regarding listeria as the case of listeria meningitis occurred following ingestion of unpasteurized cheese.29 Herpes virus infections were the most commonly observed infections in the Cambridge open-label long-term follow-up cohort with 13% of patients experiencing reactivation of varicella zoster virus.54 However, this infection is now largely avoided by the administration of prophylactic oral aciclovir following infusion and pretreatment vaccination programs.
Malignancy
Once again, despite profound T-lymphocyte depletion, which might have been considered to increase risk of malignancy in patients treated with alemtuzumab, this has so far not been observed. Although some cases of malignancy did occur in alemtuzumab treated patients within the clinical trials, these studies were not powered in such a way as to detect small changes. Overall, in the Phase II trial malignancy was observed in 2.8% of patients taking the 24 mg dose and 0.9% of patients taking interferon beta-1a.10 In CARE-MSI and CARE-MSII (12 mg), malignancy rates for alemtuzumab vs interferon beta-1a treated patients were 0.5% vs 0% and 0.6% vs 1.5% respectively.19,20 Outside of clinical trials, one case of malignant melanoma and one case of Castleman’s disease (a prelymphomatous condition) have been observed.29,65 No further malignancies were observed in the Cambridge long-term open-label follow-up.54 However, because of the theoretical risk of cervical malignancy with T-lymphocyte depletion, it is the practice in our institution to ensure that female patients have had a recent cervical smear examination prior to treatment and to encourage continued engagement in locally available cervical screening programs in the longer term.
Pregnancy
Pregnancy outcomes in patients receiving alemtuzumab have so far been encouraging. In the Cambridge long-term follow-up study, 15 babies were born to 12 women (20% of females in the study). All deliveries and births were uncomplicated. The partner of one male patient suffered a miscarriage with a subsequent live birth diagnosed with a congenital heart defect.54 From our own experience in Cardiff there have been a total of 13 pregnancies in 12 female patients (18%). Two of these pregnancies resulted in miscarriage. No adverse childhood events have been reported to us (unpublished data). Although no consistent effects of alemtuzumab on fetal development have been observed thus far, the parent company recommends effective contraception during treatment and for 4 months following treatment.60
Practical guidelines for use
Infusion related side effects are common, occurring in approximately 90% of patients10,19,20 and should be anticipated by the treating physician. Early use of alemtuzumab demonstrated that patients experience a transient worsening of preexisting symptoms or a recurrence of historical symptoms related to cytokine release, in particular TNF-α, IL-6, and IFN-γ. This was thought to occur by the direct effect of these cytokines on partially demyelinated pathways.66 The concomitant use of corticosteroids prior to infusion of alemtuzumab prevents this cytokine release66 and thus all patients receive intravenous methylprednisolone prior to treatment for the first three days of each treatment course. Other common infusion related side effects include headaches, pyrexia, and rash, which should be treated symptomatically with antihistamines and antipyretics.60,61 In response to the relatively common occurrence of herpetic infections, aciclovir at a dose of 200 mg BID is now given during treatment and for 1-month posttreatment.20,60,61,67 In their recent approval of alemtuzumab, the US Food and Drug Administration (FDA) recommended that patients also receive varicella-zoster vaccination 6 weeks prior to treatment if they do not have anti-varicella antibodies present.68 However, it should also be noted that live vaccines are advised against following treatment, and immunization in the few weeks following alemtuzumab therapy may be ineffective.69
As a result of the high incidence of adverse autoimmune events following infusion, the parent company also recommends rigorous monitoring of patients receiving alemtuzumab (Table 3). In particular, laboratory tests should be conducted at periodic intervals for 48 months following last treatment course. This includes complete blood count with differential (prior to treatment initiation and at monthly intervals thereafter), serum creatinine levels (prior to treatment initiation and at monthly intervals thereafter), urinalysis with microscopy (prior to treatment initiation and at monthly intervals thereafter), and thyroid function tests (prior to treatment initiation and every 3 months thereafter).60 The FDA also recommends skin examination at the start of treatment and yearly thereafter to monitor for melanoma.68 Physician and patient education regarding the identification of clinical features of adverse AID is also crucial in identifying adverse events early.
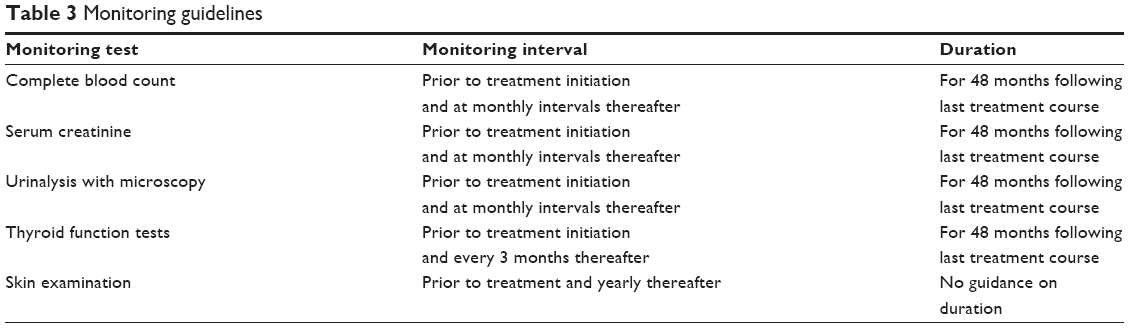 | Table 3 Monitoring guidelines |
Place in therapy
Alemtuzumab has been shown to be effective in reducing relapse rates and to have an effect on disability progression, but its role in a number of therapeutic strategies now available to clinicians is still to be fully established and is reflected in the variance in licensed indications internationally (Table 4). For example, in Europe and Australia, alemtuzumab is available for use in patients with “active disease defined by clinical or imaging features”.11,13 This is in contrast to the recent decision from the FDA who have now approved its use after initial rejection cautioning that it should be “reserved for patients who have had an inadequate response to two or more drugs indicated for the treatment of MS”.17 Although award of a license in the US is encouraging, the trial data suggest that treatment is most efficacious when given early in the disease course. By adopting a strategy which dictates that patients should fail two drugs before commencing alemtuzumab, the “window of therapeutic opportunity”43 for effective control of disease over the longer term as well as future avoidance of fixed disability may be missed.
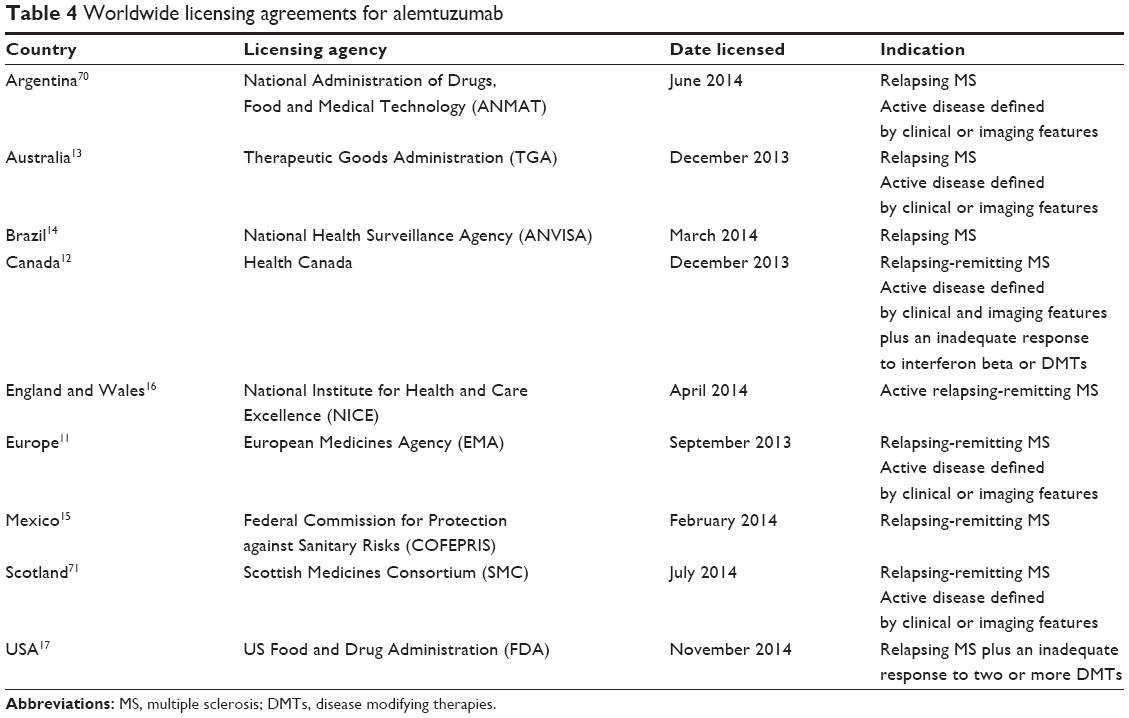 | Table 4 Worldwide licensing agreements for alemtuzumab |
Despite its impressive efficacy, there is still uncertainty concerning retreatment after the initial standard treatment cycle (two treatment courses over 12 months). Should treatment continue indefinitely if the patient continues to relapse or has active radiological disease or should a new agent be introduced, and if so which one? From the Cambridge long-term follow-up study, alemtuzumab appears to have a remarkably durable treatment effect with the majority (52%) only requiring the standard treatment cycle after a median 7-year follow-up, only 36% of patients receiving three, 8% four and 1 patient five cycles.54 It is unknown what effect further immunosuppression with agents such as natalizumab or the newer oral agents may have on efficacy or future adverse events and this will need to be further explored in future studies. With oral disease modifying agents now becoming widely available, patient choice may move away from standard injectable treatments. However, it is likely that alemtuzumab will be a popular choice for selected patients, especially those with aggressive relapsing disease and poor prognostic indicators. In contrast to standard DMTs, and indeed other monoclonal antibody therapies such as natalizumab, the standard two-treatment courses for alemtuzumab is convenient for patients who only need attend hospital for 8 days of treatment in a 12-month period. It may also have a particular role for those patients who are planning to become pregnant since patients are advised to use effective contraception for only 4 months after infusion.
Conclusion
Alemtuzumab is an efficacious treatment for active relapsing MS having been shown in robust clinical trials and against an active comparator to significantly reduce relapse rates, MRI outcomes and, at the very least, achieve some stabilization of disability progression in both treatment-naïve and treatment-experienced patients. Although autoimmune adverse events are common, our experience is that they are largely predictable and can be recognized and treated early with a robust surveillance and monitoring program, which may make practical use of this therapy more suited to the larger specialist MS clinical services.
Author contributions
Both authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in either drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclosure
Neil P Robertson and his institution (University Hospital of Wales) have received funding from a neuroimmunology fellow program supported by Genzyme. The authors report no other conflicts of interest.
References
Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372(9648):1502–1517. | ||
Multiple Sclerosis Trust. Prevalence and incidence of multiple sclerosis. Available from: http://www.mstrust.org.uk/atoz/prevalence_incidence.jsp. Accessed Januray 16, 2015. | ||
Whetten-Goldstein K, Sloan FA, Goldstein LB, Kulas ED. A comprehensive assessment of the cost of multiple sclerosis in the United States. Mult Scler. 1998;4(5):419–425. | ||
Hirst C, Ingram G, Pickersgill T, Swingler R, Compston DA, Robertson NP. Increasing prevalence and incidence of multiple sclerosis in South East Wales. J Neurol Neurosurg Psychiatry. 2009;80(4):386–391. | ||
Sawcer S, Hellenthal G, Pirinen M, et al. Genetic risk and a primary role for cell-mediated immune mechanisms in multiple sclerosis. Nature. 2011;476(7359):214–219. | ||
Patsopoulos NA, Barcellos LF, Hintzen RQ, et al. Fine-mapping the genetic association of the major histocompatibility complex in multiple sclerosis: HLA and non-HLA effects. PLoS Genet. 2013;9(11):e1003926. | ||
Zafranskaya M, Oschmann P, Engel R, et al. Interferon-beta therapy reduces CD4+ and CD8+ T-cell reactivity in multiple sclerosis. Immunology. 2007;121(1):29–39. | ||
Neuhaus O, Farina C, Yassouridis A, et al. Multiple sclerosis: comparison of copolymer-1-reactive T cell lines from treated and untreated subjects reveals cytokine shift from T helper 1 to T helper 2 cells. Proc Natl Acad Sci U S A. 2000;97(13):7452–7457. | ||
Johnson TA, Lapierre Y, Bar-Or A, Antel JP. Distinct properties of circulating CD8+ T cells in FTY720-treated patients with multiple sclerosis. Arch Neurol. 2010;67(12):1449–1455. | ||
Coles AJ, Compston DA, Selmaj KW, et al. Alemtuzumab versus interferon beta-1a in early multiple sclerosis. N Engl J Med. 2008;359(17):1786–1801. | ||
Genzyme. European Commission approves Genzyme’s multiple sclerosis treatment Lemtrada™ (alemtuzumab) [press release]. Cambridge, MA: Genzyme; 2013 [September 17]. Available from: http://news.genzyme.com/press-release/european-commission-approves-genzymes-multiple-sclerosis-treatment-lemtrada-alemtuzuma. Accessed January 12, 2015. | ||
Genzyme. Genzyme’s Lemtrada™ approved in Canada for tratement of multiple sclerosis [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-canada-treatment-multiple-sclerosis. Accessed January 16, 2015. | ||
Genzyme. Genzyme’s Lemtrada™ approved in Australia for treatment of multiple sclerosis [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-australia-treatment-multiple-sclerosis. Accessed January 16, 2015. | ||
Genzyme. Genzyme’s Lemtrada™ approved in Brazil for treatment of multiple sclerosis [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-brazil-treatment-multiple-sclerosis. Accessed January 16, 2015. | ||
Genzyme. Genzyme’s Lemtrada® approved in Mexico for treatment of multiple sclerosis [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-mexico-treatment-multiple-sclerosis. Accessed January 16, 2015. | ||
National Institute for Health and Care Excellence. Alemtuzumab for Treating Relapsing-Remitting Multiple Sclerosis. London, UK: NICE; 2014. Available from: http://www.nice.org.uk/guidance/ta312/resources/guidance-alemtuzumab-for-treating-relapsingremitting-multiple-sclerosis-pdf. Accessed January 16, 2014. | ||
Genzyme. Genzyme’s Lemtrada approved by the FDA [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-fda. Accessed January 16, 2015. | ||
Coles AJ, Compston A. Product licences for alemtuzumab and multiple sclerosis. Lancet. 2014;383(9920):867–868. | ||
Coles AJ, Twyman CL, Arnold DL, et al. Alemtuzumab for patients with relapsing multiple sclerosis after disease-modifying therapy: a randomised controlled phase 3 trial. Lancet. 2012;380(9856):1829–1839. | ||
Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial. Lancet. 2012;380(9856):1819–1828. | ||
Hale G, Rye PD, Warford A, Lauder I, Brito-Babapulle A. The glycosylphosphatidylinositol-anchored lymphocyte antigen CDw52 is associated with the epididymal maturation of human spermatozoa. J Reprod Immunol. 1993;23(2):189–205. | ||
Hale G. The CD52 antigen and development of the CAMPATH antibodies. Cytotherapy. 2001;3(3):137–143. | ||
Rao SP, Sancho J, Campos-Rivera J, et al. Human peripheral blood mononuclear cells exhibit heterogeneous CD52 expression levels and show differential sensitivity to alemtuzumab mediated cytolysis. PLoS One. 2012;7(6):e39416. | ||
Rowan WC, Hale G, Tite JP, Brett SJ. Cross-linking of the CAMPATH-1 antigen (CD52) triggers activation of normal human T lymphocytes. Int Immunol. 1995;7(1):69–77. | ||
Watanabe T, Masuyama J, Sohma Y, et al. CD52 is a novel costimulatory molecule for induction of CD4+ regulatory T cells. Clin Immunol. 2006;120(3):247–259. | ||
Klotz L, Meuth SG, Wiendl H. Immune mechanisms of new therapeutic strategies in multiple sclerosis-A focus on alemtuzumab. Clin Immunol. 2012;142(1):25–30. | ||
Coles A, Deans J, Compston A. Campath-1H treatment of multiple sclerosis: lessons from the bedside for the bench. Clin Neurol Neurosurg. 2004;106(3):270–274. | ||
Somerfield J, Hill-Cawthorne GA, Lin A, et al. A novel strategy to reduce the immunogenicity of biological therapies. J Immunol. 2010;185(1):763–768. | ||
Coles AJ. Alemtuzumab treatment of multiple sclerosis. Semin Neurol. 2013;33(1):66–73. | ||
Fox EJ. Alemtuzumab in the treatment of relapsing-remitting multiple sclerosis. Expert Rev Neurother. 2010;10(12):1789–1797. | ||
Hu Y, Turner MJ, Shields J, et al. Investigation of the mechanism of action of alemtuzumab in a human CD52 transgenic mouse model. Immunology. 2009;128(2):260–270. | ||
Kousin-Ezewu O, Azzopardi L, Parker RA, et al. Accelerated lymphocyte recovery after alemtuzumab does not predict multiple sclerosis activity. Neurology. 2014;82(24):2158–2164. | ||
Cossburn MD, Harding K, Ingram G, et al. Clinical relevance of differential lymphocyte recovery after alemtuzumab therapy for multiple sclerosis. Neurology. 2013;80(1):55–61. | ||
Robertson N, Scolding N. Immune reconstitution and treatment response in multiple sclerosis following alemtuzumab. Neurology. 2014:2150–2151. | ||
Thompson SA, Jones JL, Cox AL, Compston DA, Coles AJ. B-cell reconstitution and BAFF after alemtuzumab (Campath-1H) treatment of multiple sclerosis. J Clin Immunol. 2010;30(1):99–105. | ||
Hill-Cawthorne GA, Button T, Tuohy O, et al. Long term lymphocyte reconstitution after alemtuzumab treatment of multiple sclerosis. J Neurol Neurosurg Psychiatry. 2012;83(3):298–304. | ||
Cox AL, Thompson SA, Jones JL, et al. Lymphocyte homeostasis following therapeutic lymphocyte depletion in multiple sclerosis. Eur J Immunol. 2005;35(11):3332–3342. | ||
Zhang X, Tao Y, Chopra M, et al. Differential reconstitution of T cell subsets following immunodepleting treatment with Alemtuzumab (Anti-CD52 monoclonal antibody) in patients with relapsing-remitting multiple sclerosis. J Immunol. 2013;191(12):5867–5874. | ||
Havari E, Turner MJ, Campos-Rivera J, et al. Impact of alemtuzumab treatment on the survival and function of human regulatory T cells in vitro. Immunology. 2014;141(1):123–131. | ||
Fox E, Arnold DL, Cohen J, et al. Durable efficacy of alemtuzumab in relapsing-remitting multiple sclerosis patients who participated in the CARE-MS studies: three-year follow-up. Neurology. 2013;80 (Meeting abstracts 1):S41.001. | ||
Moreau T, Thorpe J, Miller D, et al. Preliminary evidence from magnetic resonance imaging for reduction in disease activity after lymphocyte depletion in multiple sclerosis. Lancet. 1994;344(8918):298–301. | ||
Coles a J, Wing MG, Molyneux P, et al. Monoclonal antibody treatment exposes three mechanisms underlying the clinical course of multiple sclerosis. Ann Neurol. 1999;46(3):296–304. | ||
Coles AJ, Cox A, Le Page E, et al. The window of therapeutic opportunity in multiple sclerosis: evidence from monoclonal antibody therapy. J Neurol. 2006;253(1):98–108. | ||
Hirst CL, Pace A, Pickersgill TP, et al. Campath 1-H treatment in patients with aggressive relapsing remitting multiple sclerosis. J Neurol. 2008;255(2):231–238. | ||
Fox EJ, Sullivan HC, Gazda SK, et al. A single-arm, open-label study of alemtuzumab in treatment-refractory patients with multiple sclerosis. Eur J Neurol. 2012;19(2):307–311. | ||
McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol. 2001;50(1):121–127. | ||
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. | ||
Coles AJ, Fox E, Vladic A, et al. Alemtuzumab more effective than interferon β-1a at 5-year follow-up of CAMMS223 clinical trial. Neurology. 2012;78(14):1069–1078. | ||
Coles AJ, Fox E, Vladic A, et al. Alemtuzumab versus interferon β-1a in early relapsing-remitting multiple sclerosis: post-hoc and subset analyses of clinical efficacy outcomes. Lancet Neurol. 2011;10(4):338–348. | ||
Havrdova E, Arnold DL, Palmer J, Margolin DH. FC1.4 Disease-free outcomes with alemtuzumab: 3-year followup of the CARE-MS studies. In: 2014 Joint ACTRIMS-ECTRIMS Meeting (MSBoston 2014): oral presentations. Mult Scler. 2014;20(1 suppl):14–66. | ||
Coles AJ, Arnold DL, Cohen JA, et al. P090 Efficacy and safety of alemtuzumab in treatment-naive patients with relapsing-remitting MS: four-year followup of the CARE-MS I study. Poster presented at 2014 Joint ACTRIMS-ECTRIMS Meeting (MSBoston 2014). Mult Scler. 2014;20(1 suppl):67–284. | ||
Hartung HP, Arnold DL, Cohen JA, et al. P043 Efficacy and safety of alemtuzumab in patients with relapsing-remitting MS who relapsed on prior therapy: four-year follow-up of the CARE-MS II study. Poster presented at 2014 Joint ACTRIMS-ECTRIMS Meeting (MSBoston 2014). Mult Scler. 2014;20(1 Suppl):67–284. | ||
Genzyme. At four years, treatment effect maintained in more than two-thirds of patients who received Genzymes’ Lemtrada in pivotal studies [press release]. Available from: http://news.genzyme.com/press-release/four-years-treatment-effect-maintained-more-two-thirds-patients-who-received-genzymes-. Accessed January 16, 2015. | ||
Tuohy O, Costelloe L, Hill-Cawthorne G, et al. Alemtuzumab treatment of multiple sclerosis: long-term safety and efficacy. J Neurol Neurosurg Psychiatry. 2015;86(2):208–215. | ||
Willis MD, Harding KE, Wardle M, Pickersgill T, Tomassini V, Robertson NP. Alemtuzumab: long term follow-up in a single centre cohort. J Neurol Neurosurg Psychiatry. 2014;85(10):e4. doi:10.1136/jnnp-2014-309236.7. | ||
Jones JL, Thompson SA, Loh P, et al. Human autoimmunity after lymphocyte depletion is caused by homeostatic T-cell proliferation. Proc Natl Acad Sci U S A. 2013;110(50):20200–20205. | ||
Daniels GH, Vladic A, Brinar V, et al. Alemtuzumab-related thyroid dysfunction in a phase 2 trial of patients with relapsing-remitting multiple sclerosis. J Clin Endocrinol Metab. 2014;99(1):80–89. | ||
Coles AJ, Wing M, Smith S, et al. Pulsed monoclonal antibody treatment and autoimmune thyroid disease in multiple sclerosis. Lancet. 1999;354(9191):1691–1695. | ||
Cossburn M, Pace AA, Jones J, et al. Autoimmune disease after alemtuzumab treatment for multiple sclerosis in a multicenter cohort. Neurology. 2011;77(6):573–579. | ||
Lemtrada (alemtuzumab). Summary of Product Characteristics. Genzyme Therapeutics Ltd., 2013. | ||
Lemtrada (alemtuzumab). Product Information. Sanofi-Aventis Australia Pty Ltd., 2014. | ||
Clatworthy MR, Wallin EF, Jayne DR. Anti-glomerular basement membrane disease after alemtuzumab. N Engl J Med. 2008;359(7):768–769. | ||
Jones JL, Phuah C, Cox AL, et al. IL-21 drives secondary autoimmunity in patients with multiple sclerosis, following therapeutic lymphocyte depletion with alemtuzumab (Campath-1H). J Clin Invest.2009;119(7):2052–2061. | ||
Turner MJ, Lamorte MJ, Chretien N, et al. Immune status following alemtuzumab treatment in human CD52 transgenic mice. J Neuroimmunol. 2013;261(1–2):29–36. | ||
Pace AA, Zajicek JP. Melanoma following treatment with alemtuzumab for multiple sclerosis. Eur J Neurol. 2009;16(4):e70–e71. | ||
Moreau T, Coles A, Wing M, et al. Transient increase in symptoms associated with cytokine release in patients with multiple sclerosis. Brain. 1996;119:225–237. | ||
Lemtrada (alemtuzumab). Product Monograph. Genzyme Canada, 2013. | ||
National Multiple Sclerosis Society. FDA approves Lemtrada™ (alemtuzumab) for relapsing MS-update. Available from: http://www.nationalmssociety.org/About-the-Society/News/FDA-Approves-Lemtrada%E2%84%A2-%28alemtuzumab%29-for-Relapsing. Accessed January 16, 2015. | ||
McCarthy CL, Tuohy O, Compston DA, Kumararatne DS, Coles AJ, Jones JL. Immune competence after alemtuzumab treatment of multiple sclerosis. Neurology. 2013;81(10):872–876. | ||
Genzyme. Genzyme’s Lemtrada approved in Argentina for treatment of multiple sclerosis [press release]. Available from: http://news.genzyme.com/press-release/genzymes-lemtrada-approved-argentina-treatment-multiple-sclerosis. Accessed January 16, 2015. | ||
Genzyme. Genzyme in the UK: UK news. Available from: http://www.genzyme.co.uk/corp-info/news/local.aspx?id=070714. Accessed January 16, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.