")
Back to Journals » Patient Preference and Adherence » Volume 8
Alcohol use, antiretroviral therapy adherence, and preferences regarding an alcohol-focused adherence intervention in patients with human immunodeficiency virus
Authors Kekwaletswe C, Morojele N
Received 8 October 2013
Accepted for publication 13 December 2013
Published 31 March 2014 Volume 2014:8 Pages 401—413
DOI https://doi.org/10.2147/PPA.S55547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Connie T Kekwaletswe,1 Neo K Morojele1,2
1Alcohol and Drug Abuse Research Unit, Medical Research Council, Pretoria, 2School of Public Health, University of the Witwatersrand, Johannesburg, South Africa
Background: The primary objectives of this study were to determine the association between alcohol and antiretroviral therapy (ART) adherence and the perceived appropriateness and acceptability of elements of an adherence counseling program with a focus on alcohol-related ART nonadherence among a sample of ART recipients in human immunodeficiency virus (HIV) clinics in Tshwane, South Africa.
Methods: We conducted a cross-sectional study with purposive sampling. The sample comprised 304 male and female ART recipients at two President's Emergency Plan For AIDS Relief-supported HIV clinics. Using an interview schedule, we assessed patients' alcohol use (Alcohol Use Disorders Identification Test), other drug use, level of adherence to ART, and reasons for missing ART doses (AIDS Clinical Trials Group adherence instrument). Additionally, patients’ views were solicited on: the likely effectiveness of potential facilitators; the preferred quantity, duration, format, and setting of the sessions; the usefulness of having family members/friends attend sessions along with the patient; and potential skill sets to be imparted.
Results: About half of the male drinkers’ and three quarters of the female drinkers’ Alcohol Use Disorders Identification Test scores were suggestive of hazardous or harmful drinking. Average self-reported ART adherence was 89.7%. There was a significant association between level of alcohol use and degree of ART adherence. Overall, participants perceived two clinic-based sessions, each of one hour’s duration, in a group format, and facilitated by a peer or adherence counselor, as most appropriate and acceptable. Participants also had a favorable attitude towards family and friends accompanying them to the sessions. They also favored an alcohol-focused adherence counseling program that employs motivational interviewing and cognitive behavioral therapy-type approaches.
Conclusion: The association between alcohol use and ART nonadherence points to a need for alcohol-focused ART adherence interventions. Patients’ perceptions suggest their amenability to clinic-based brief motivational interviewing and cognitive behavioral therapy-type adherence interventions delivered by lay persons in group settings. Further research should investigate how best to implement such interventions in the existing health system.
Keywords: alcohol, adherence, antiretroviral therapy, patient perception, South Africa
Introduction
Parallel to the expansion of antiretroviral therapy (ART) programs in sub-Saharan Africa has been an evident decrease in human immunodeficiency virus (HIV)-related mortality and morbidity.1,2 To date, South Africa has had one of the largest ART programs globally, with over 1.7 million treatment recipients between 2004 and 2011.3 More recently, Shisana4 estimated the total number of ART recipients to be over 2 million as of mid 2012. Nonetheless, the positive clinical outcomes of the ART program are dependent on, among other factors, high levels of adherence among those enrolled on ART regimens.5–8
Despite some research showing levels of adherence to ART in resource-limited settings to be similar or superior to those of patients in resource-rich settings,9 a recent commentary from the USA10 has cautioned that optimal adherence to sustain viral suppression over a lifetime is often a challenge. Thus, it is imperative to further investigate modifiable factors that could compromise optimal ART adherence, which in turn could be intervention targets, eg, hazardous alcohol consumption.
An increasing body of research attests to the association between alcohol consumption and suboptimal adherence to ART.11–17 For instance, in a meta-analysis by Hendershot et al,15 drinkers were 50%–60% as likely to be adherent as nondrinkers (odds ratio 0.55, 95% confidence interval 0.49–0.61). This effect was more evident for problem drinkers than for nonproblem drinkers. Another study18 found nonadherence to be approximately nine times more likely to occur (odds ratio 8.78, 95% confidence interval 7.17–10.77) on days when alcohol was consumed. Moreover, a temporal and dose-response relationship19 between alcohol consumption and missed ART doses has been reported, with the highest frequency of missed ART doses occurring on drinking days, followed by post-drinking days, and then nondrinking days. In our recent study in South Africa,20 alcohol use was independently associated with ART adherence, over and above demographic, structural, and psychosocial factors. Given the role of alcohol in compromising ART adherence, it is evident that alcohol-focused ART interventions are needed, particularly in settings such as South Africa, which have numerous persons enrolled on ART and very high levels of per capita alcohol consumption.21
A number of ART adherence interventions have been developed and evaluated in substance-using and nonsubstance-using HIV populations.22–24 These interventions have been very diverse and include the following types of approaches: directly administered ART, medication-assisted therapy, scripted telephone calls, strengthening of family support for adherence, enhanced interactive computer intervention, psychoeducation by a health professional, motivational interviewing (MI), cognitive behavioral therapy (CBT), MI plus CBT, CBT for adherence and depression, self-management, and contingency management. A meta-analytic review of 19 randomized controlled trials revealed that interventions using cognitive-behavioral types of approaches coupled with a core set of psychoeducation elements (eg, improving problem-solving, teaching self-monitoring skills) were among the most effective.24 Overall, the effect of adherence interventions in substance-using and nonsubstance-using populations has been modest, and tends not to persist over time.22,24 Based on their review, Mathes et al23 have conjectured that patients most likely to benefit from an adherence counseling program are those who are at particularly high risk for nonadherence, such as substance abusers. Indeed, only one of the 21 trials they evaluated showed statistically significant results for adherence rates as well as viral loads. This one intervention involved MI for alcohol-dependent patients.
To our knowledge, an alcohol-focused ART adherence intervention has not been implemented in South Africa, so we sought to close this gap by examining the need for such an intervention and its most appropriate content and approach(es). Specifically, we conducted a study to determine the extent to which alcohol is associated with suboptimal ART adherence. We also examined the preferences of members of the target population regarding a prospective alcohol-focused ART adherence intervention, given their unique knowledge of their own health status, and their preferences for treatment and health outcomes.25,26 Eliciting the preferences of the target population may enhance the feasibility and acceptability of the intervention and reduce attrition, while improving the effectiveness of the intervention.27
We conducted a study among HIV patients in ART clinics, all of whom would have attended the regular mandated pre-ART initiation preparatory adherence counseling program according to the South African treatment guidelines.28 This program typically involves 3–4 counseling sessions (each 30–50 minutes in duration) which are delivered by lay adherence counselors to the patient alone or with a treatment supporter, and include topics such as HIV, the benefits of good adherence, costs of poor adherence, potential barriers to ART adherence, and how to seek adherence support.
We conducted formative research to design and develop an intervention to address alcohol-related nonadherence to ART, which comprised both a qualitative and a quantitative substudy. This paper describes the quantitative substudy, which had three aims. The first was to evaluate whether there is a relationship between levels of alcohol use (nondrinking, nonproblem drinking, and problem drinking) and ART adherence. The hypothesis related to this aim was that the higher the level of alcohol use the lower the degree of ART adherence. The second aim was to determine the extent of perceived appropriateness, acceptability, and utility of elements of a proposed alcohol-focused adherence counseling program among ART recipients. The third aim was to assess whether sex, drinking levels, and adherence levels are associated with preference of elements of an alcohol-focused adherence counseling program.
Materials and methods
The study was cross-sectional and sampled 304 HIV patients at two President’s Emergency Plan For AIDS Relief-funded HIV clinics based at district (level 1) hospitals in the Tshwane Metropolitan Municipality, Gauteng Province, South Africa. Trained fieldworkers recruited participants from each of the two ART clinics. Prospective participants were approached by fieldworkers, informed of the aims and purposes of the study, and then invited to participate. Inclusion criteria for study participation were: age 18 years or older; HIV-positive status; on ART for at least 4 months; speaker of English, Setswana/Sesotho, or isiZulu; and cognitively intact to ensure patients could give informed consent. There was no formal assessment of intact cognition; the fieldworkers were trained to assess this via their subjective judgments of patients in terms of domains like level of consciousness (alertness, drowsiness), attention, orientation (person, place, and situation), use of language, and ability to comprehend while the purpose of the study was being explained.
Those who consented to taking part in the study then signed informed consent forms prior to being interviewed. The interview was conducted at a time that did not interfere with the patients’ medical visit and in the interviewees’ language of choice. The participants were given an appreciation voucher worth ZAR30 (approximately US$4) at the end of the interview.
Interviews were conducted using a semistructured interview schedule that, among other factors (not relevant to this paper), consisted of measures of demographic factors, HIV-related factors, structural factors (eg, stigma), ART adherence, alcohol use, other drug use, and Likert scale items assessing participants’ perceptions of the appropriateness and acceptability of elements of an adherence counseling program for alcohol-related ART nonadherence.
This research was approved by the ethics committee of the University of Pretoria (protocol number 98/2009) and by the Centers for Disease Control and Prevention.
Measures
Demographics and HIV-related factors
Survey questions (based on South African studies29 or designed by the authors) assessed participant age, sex, level of education, marital status, employment, food insecurity, HIV disclosure, perceived HIV stigma (worry about maltreatment due to HIV status), enacted HIV stigma (loss of friends and being treated differently post HIV disclosure), and length of time on ART.
Alcohol use
Alcohol use was measured using the 10-item Alcohol Use Disorders Identification Test (AUDIT), which screens for excessive drinking and related risks,30 and has high levels of validity and reliability.31 The maximum score on the AUDIT is 40, and the cutoff score for harmful/hazardous drinking is 8 for men and 6 for women.30,32,33 The alcohol drinker types were: nondrinkers; nonproblem drinkers (AUDIT scores 1–7 for men and 1–5 for women); and problem drinkers (AUDIT scores 8–40 for men and 6–40 for women). Alcohol consumption was based on the AUDIT question asking about the number of drinks one has on a typical drinking day. The alcohol consumption groups were: light drinking (1–2 drinks), moderate drinking (3–4 drinks), and binge drinking (≥5 drinks). Cronbach’s alpha for the AUDIT in this study was 0.78.
Other drug use
We assessed participants’ lifetime and current use of cannabis (dagga), methaqualone, heroin, and other drugs.
Adherence to ART and reasons for missing doses
The AIDS Clinical Trials Group adherence instrument (ACTG)34 is a structured interview which uses timeline follow-back questioning to recall, day-by-day, all the medication doses missed. We employed the standard 4-day recall period of the ACTG to assess adherence to ART. As in Beyene et al,35 self-reported ART adherence was computed using the formula: percent adherence = (number of doses patient should have taken minus number of doses missed)/number of doses patient should have taken ×100%. Optimal adherence to ART was based on the commonly used cutoff of ≥95% adherence.36–38
We retained nine of the ACTG reasons for missing doses items (Table S1) and added nine questions to reflect additional context-relevant barriers to ART adherence based on the literature39–43 and/or our prior qualitative research. The reasons for missing doses were measured on a 4-point Likert scale with responses ranging from “never” (scored 0) to “often” (scored 3).
Appropriateness and acceptability of elements of an alcohol-focused adherence counseling program
Of the ten questions developed by the authors for purposes of this study, eight specifically elicited participants’ views on the appropriateness and acceptability of elements of a proposed alcohol-focused adherence counseling program. The first two questions required patients to answer yes or no: whether the clinic’s mandated pre-ART initiation adherence counseling program or the on an as-needed basis ART adherence counseling ever focus on patients with alcohol-related ART nonadherence; and whether there was a specific need for an additional counseling program to address alcohol-related nonadherence. Patients’ views regarding the proposed alcohol-focused adherence counseling program were sought on: a) the likely effectiveness of the intervention if delivered by each of five different types of potential facilitators; responses were indicated on a 4-point Likert scale and ranged from “not well at all” (1) to “very well” (4); b) the number of sessions (session quantity); responses were indicated on a 4-point Likert scale and ranged from “one” (1) to “more than three” (4); c) the preferred duration of each session; responses were indicated on a 4-point Likert scale that ranged from “30 minutes” (1) to “over 1 hour and 30 minutes” (4); d) potential session formats; responses were indicated on a binary scale (yes/no) regarding five formats: group sessions, individual sessions, two-person sessions (ART client and other chosen person, eg, “treatment supporter”), watching videotapes, and reading written material/brochures; e) appropriate settings (ie, clinic, school, community, and an option of “other” which participants specified; session setting); responses were indicated on a binary scale (yes/no); f) the usefulness of having family members/friends attend sessions along with the patient; responses were indicated on a binary scale (yes/no); and g) the perceived utility of each of four types of content/potential skill sets to be imparted (session content): i) “share ideas on how to drink less often”, ii) “share ideas on drinking fewer quantities of alcohol each time one drinks”, iii) “share strategies for coping that do not involve alcohol”, and iv) “discuss the advantages and disadvantages of not drinking”; responses were indicated on a 4-point Likert scale ranging from “very useful” (1) to “don’t know” (4). Finally, patients’ supplementary views regarding the proposed additional adherence counseling program were solicited via a single open-ended question: “Do you have any other comments about this additional program?” Participants’ responses to this one open-ended question were not audio-recorded, but the fieldworkers wrote notes to reflect the responses in the space provided at the end of the questionnaire.
Analyses
The data regarding demographic factors, HIV-related factors, extent of other drug use, reasons for missing ART doses, average adherence, and patient preferences regarding the various elements of an alcohol-focused ART adherence counseling program were analyzed using descriptive statistics (ie, frequencies, means). The Pearson’s chi-square (χ2) test and Fisher’s exact test were used to evaluate whether there was a statistically significant difference between males and females on demographic and HIV-related factors. Two-way contingency table analysis with cross-tabulations (with Pearson’s chi-square test and Fisher’s exact test where relevant) were used to evaluate the relationships between the quantity of alcohol consumed and ART adherence and between elements of an adherence counseling program and the following: sex, drinking levels/drinker types (nondrinker, problem drinker, nonproblem drinker), and adherence (low or high). The Kruskal–Wallis test was used to evaluate associations between ART adherence and alcohol use, with the Mann–Whitney U test for post hoc comparisons. Quantitative analyses were conducted using IBM® SPSS® Statistics for Windows version 21.0 software (IBM Corp, Armonk, NY, USA).
The responses to the one open-ended question regarding participants’ additional comments about the proposed alcohol-focused adherence program were analyzed inductively and thematically.44 The first author and two coders independently read and reread the comments, and identified initial codes by making notes of salient issues within the comments.44,45 The coders then discussed and compared the initial codes, identified similarities and discrepancies, and compiled a refined list of codes. Discrepancies were resolved through discussion, and decisions to retain a code were based on consensus that there were adequate quotes from the text to support the code. Each coder was then assigned half of the codes and allocated a code from her list to each comment, where applicable. The coders then exchanged their coded comments and assessed whether they agreed with the assignment of codes.45 The first author and the coders then met to discuss similarities and links between the codes and to derive overall categories and then themes.
Results
Demographics
As shown in Table 1, the sample comprised mostly females (67.4%). The mean age for males and females was 37.29±7.77 years and 35.19±8.14 years, respectively. Most participants were in the age groups 30–34 and 35–39 years, and most were single, unemployed, and minimally educated. Just under two thirds (64.5%) of the participants indicated that their “household goes hungry/has no food” either “sometimes” or “often”. Participants’ overall duration on ART ranged from 4 months to 10.5 years (mean 23.7±15.7 months for males and mean 25.5±20.0 months for females).
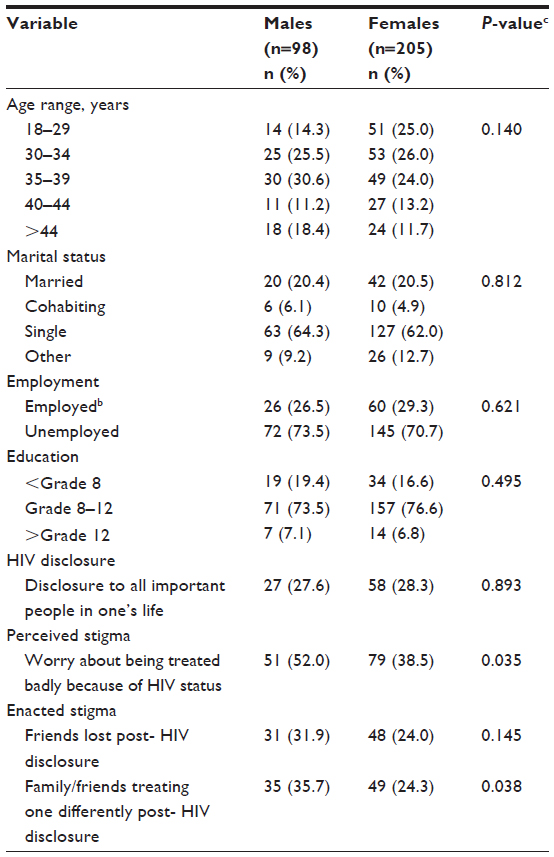 | Table 1 Demographic and HIV-related characteristics of ART recipients (n=304a) |
Just over a quarter of participants had disclosed their HIV status to all important people in their lives (Table 1). Participants indicated more perceived than enacted HIV stigma. Males reported significantly more perceived stigma than females (P<0.05; two-tailed Fisher’s exact test) and were more likely to report that their family/friends treated them differently after their HIV disclosure (P<0.05, two-tailed Fisher’s exact test).
Alcohol use
Of the 304 participants, only 123 reported having ever consumed alcohol. Those who reported having ever consumed alcohol constituted 52.0% of the men and 34.6% of the women. Most of the participants (91.0%) who were lifetime drinkers had consumed alcohol in the previous month, with the figures for men and women being 98.0% and 86.1%, respectively. Men drank alcohol significantly more frequently than women (χ2 [3, n=302]=19.52; P<0.001). The mean AUDIT score for male drinkers was 13.25±7.33 (range 2–27) while the mean AUDIT score for female drinkers was 7.38±5.60 (range 1–25). Using the AUDIT cutoff score of ≥8 for men and ≥6 for women, about three quarters of the male drinkers (74.5%) and slightly more than half of the female drinkers (54.9%) drank in a hazardous/harmful fashion.
Other drug use
Overall, most of the participants reported not having used other drugs. In total, 5.7%, 1.6%, 1.6%, and 17.9% of the participants who had consumed alcohol reported having used cannabis, methaqualone, and heroin, respectively.
ACTG adherence
Average self-reported ART adherence in the previous 4 days was 89.7%±19.90%, and 61.8% of the sample (n=188) reported 100% adherence. Based on the most commonly used cutoff of ≥95% adherence as indicative of good adherence, only 67.8% of the sample were adherent to their prescribed ART regimen. The Kruskal–Wallis test showed significant differences between the participants within the three drinking levels (nondrinking, nonproblem drinking and problem drinking) on median ART adherence scores (χ2 [2, n=286]=14.48; P=0.001). Mean rank adherence ranged from highest to lowest in the following order: nondrinker (155.73), nonproblem drinker (132.90), and problem drinker (119.84). The results of cross-tabulation of alcohol consumption with ART adherence did not yield a significant result (χ2 [2, n=108]=1.68; P>0.05). Nonetheless, there was a general trend of a lower proportion of high ART adherence with increasing quantity of alcohol use, ie, light drinking (62.5%), moderate drinking (54.7%), and binge drinking (45.2%).
Reasons for missing ART doses
Of the 18 possible reasons for missing ART doses (Table S1) “simply forgot” was the most commonly reported reason (49.7% of the sample). Taking alcohol/drugs was reported by only 12.8% of the whole sample as a reason for missing ART doses. In contrast, 30.1% of lifetime drinkers indicated taking alcohol/drugs as a reason for missing ART doses, 25.2% of whom indicated either “sometimes” or “often”.
Perceived appropriateness and acceptability of elements of an adherence counseling program for reducing alcohol-related ART nonadherence
Need for an additional adherence counseling program
Seventy-one percent of the participants affirmed that the clinic’s existing ART counseling program did periodically focus on those with alcohol-related ART nonadherence. Nevertheless, about 95% of the participants felt that there was still a need for an additional adherence counseling program that would address alcohol-related ART nonadherence.
Preferred facilitators
As shown in Figure 1, the most preferred facilitator for the proposed alcohol-focused adherence intervention was a fellow patient on ART, followed by an adherence counselor. Outside health care professionals were preferred over the clinic’s health care providers. A person from the community was the least preferred facilitator. No significant sex differences emerged in regards to preferred facilitators. There was no evidence of a difference in preference of facilitators by drinker group. The cross-tabulations for the three drinker types yielded no valid results; analyses for four of five potential facilitators had ≥20% of cells with expected frequencies less than five, while the one with acceptable frequencies (clinic’s health care provider) yielded no significant differences regarding preferred facilitators. Finally, participants with reported high adherence (≥95%) were more in favor of health care professionals (from the clinic and from outside the clinic) as intervention facilitators (χ2 [3, n=286]=28.17, P<0.001; and χ2 [3, n=286]=31.00; P<0.001, respectively) than were those with low adherence. There were no other significant differences between the responses of those with high and low adherence on these items.
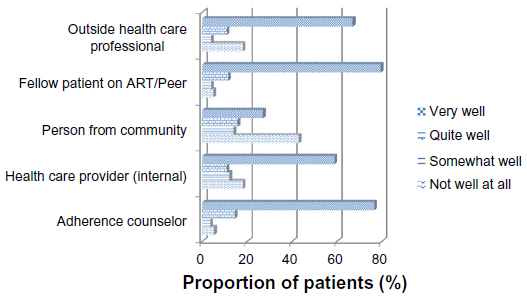 | Figure 1 Perceptions regarding how well the program would work if delivered by various interventionists. |
Session quantity and session duration
In terms of the number of sessions the alcohol-focused adherence counseling program should have, two sessions were preferred by the largest group of participants (40.3%); 18.7% preferred one session, 21.7% preferred three sessions, and 19.3% preferred more than three sessions. Further, one hour was the most preferred session duration (40.8% chose this option) of the proposed alcohol-focused intervention; in contrast, 21.4% of the participants preferred 30 minutes, 19.7% preferred one hour and 30 minutes, and 18.1% preferred over one hour and 30 minutes. No significant sex differences emerged in regards to preferred session quantity or session duration (Table 2). However, there were significant differences in the responses of the three drinker types regarding session duration (χ2 [6, n=299]=13.33; P<0.05), but not session quantity. No significant differences in session quantity and session duration emerged in the responses of those with high and low adherence.
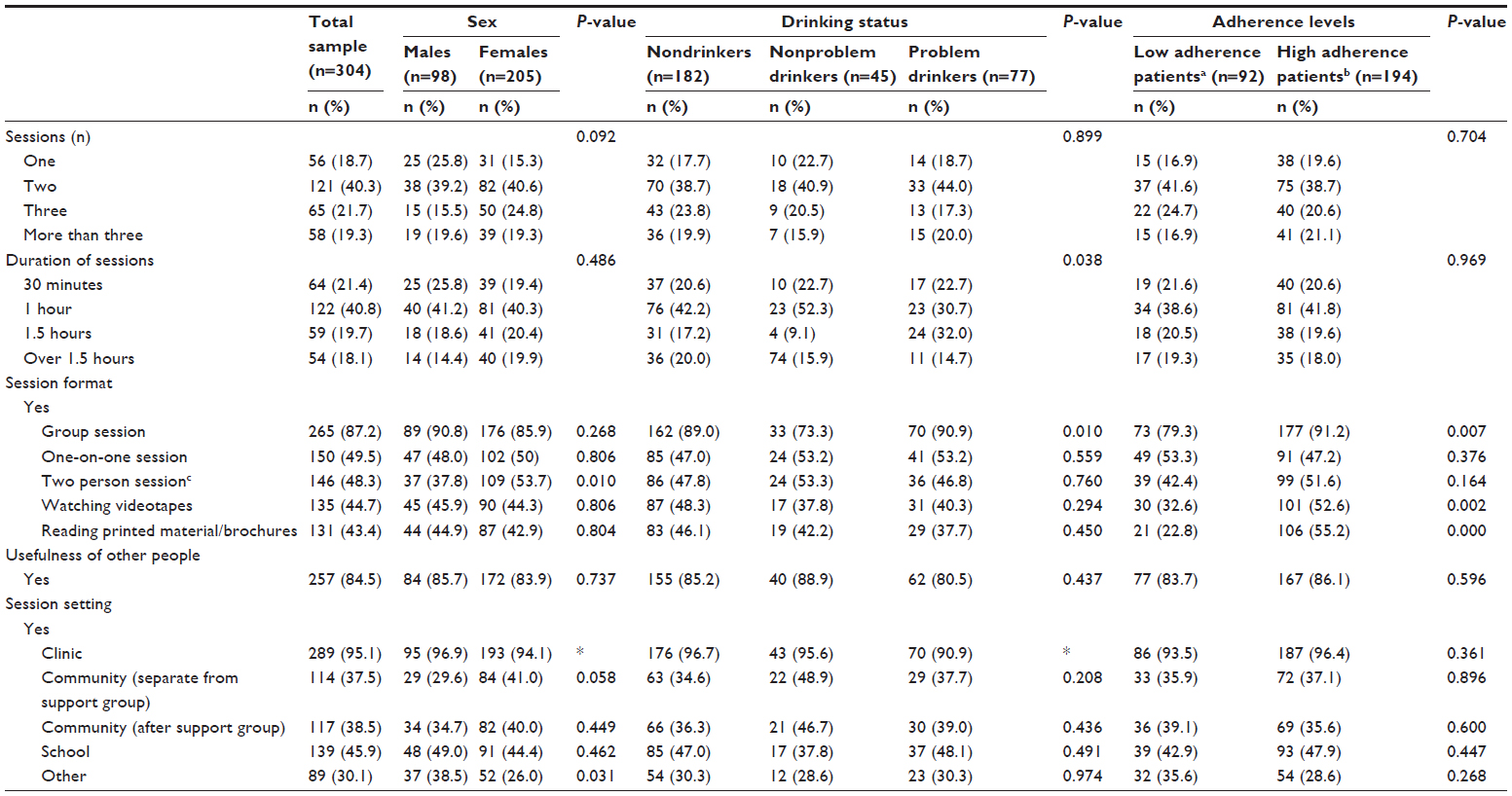 | Table 2 Patient preferences regarding elements of an alcohol-focused adherence intervention for total sample, by sex, drinking status, and adherence status |
Format of the sessions
The most preferred format was the group session format (chosen by 87.2% of participants), followed by individual sessions (49.5%). The two-person session, video watching approach, and reading materials approaches were considered to be acceptable by 48.3%, 44.7%, and 43.4% of the respondents, respectively. There was a significant sex difference in preference of a two-person session (P=0.01; two-tailed Fisher’s exact test), with men being more opposed to a two-person session than women. In addition, nonproblem drinkers were less likely to be in favor of the group session (73.3%) than problem drinkers (90.9%) and nondrinkers (89.0%, χ2 [2, n=304]=9.21; P≤0.01). Furthermore, three significant differences emerged in preferred session formats as they relate to high (≥95%) and low (<95%) adherence levels. Those with high adherence levels had higher preference than those with low adherence in terms of group sessions (P<0.01; two-tailed Fisher’s exact test), watching videotapes by themselves (P<0.01; two-tailed Fisher’s exact test), and reading printed materials/brochures by themselves (P<0.001; two-tailed Fisher’s exact test).
Session setting
Most participants (95.1%) chose “clinic” as an appropriate setting for the proposed alcohol-focused intervention. A school was acceptable to 45.9% of the participants. Apart from the “other” option (eg, shebeens, workplace), the two community settings that were inquired about (ie, the same setting as one where a community-based support group was held, and a setting different from where a community-based support group was held) were the least preferred settings. In this regard, there was a marginally significant sex difference (P=0.058; two-tailed Fisher’s exact test), with men being more opposed than women to the community setting separate from where a community-based support group is held. Males preferred “other” session settings (eg, workplace) more than females (P<0.05; two-tailed Fisher’s exact test). However, there were no significant differences between the nondrinkers, nonproblem drinkers, and problem drinkers and those with low and high adherence on the variables regarding session setting.
Participation by family members/friends
Most participants (84.5%) favored having family members or friends attending the additional adherence counseling program along with the ART recipient. No significant differences by sex, drinking type or adherence level emerged in regards to participants’ preferences for the presence of family members/friends during sessions.
Content of proposed adherence counseling program
As shown in Figure 2, “sharing coping strategies that do not involve alcohol” and “discussing the advantages and disadvantages of not drinking” were perceived as likely to be “very useful” programmatic approaches by 84.8% and 82.2% of participants, respectively. The “sharing of ideas on how to drink less often” and “how to drink fewer quantities per drinking occasion” were considered likely to be effective by fewer participants (62.6% and 58.9%, respectively). No significant sex differences emerged regarding the perceived utility of the different types of content of the proposed adherence counseling program. All the cross-tabulations for the three drinker types yielded no valid results; there were ≥20% of cells with expected frequencies less than five. The cross-tabulations for adherence levels yielded valid results for two of four intervention approaches, namely “share ideas on how to drink less often” and “share ideas on drinking fewer quantities”. Those with high adherence levels were more in favor of these intervention approaches than those with low adherence levels (χ2 [3, n=285]=30.09, P<0.001; and χ2 [3, n=285]=25.06, P<0.001, respectively).
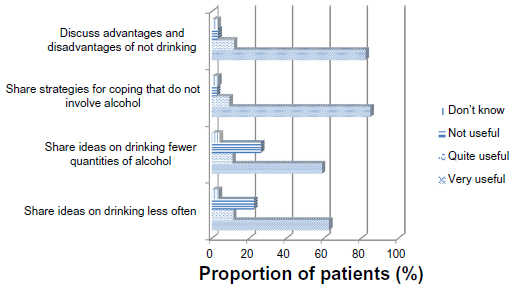 | Figure 2 Perceived usefulness of probable content for the adherence counseling program. |
Responses to open-ended question “Do you have any other comments about this additional program?”
Based on our content analysis, the topics which participants mentioned as they relate to the additional alcohol-focused adherence counseling program were a need for provision of more education regarding drinking alcohol while on ART, a need for emphasis on all dimensions of adherence (eg, time, dose), a need for more social support, and a need to address cigarette use, food insecurity, unemployment, stigma, HIV disclosure, other drugs of abuse, and living positively with HIV. Additional comments that were made related to consistency of condom use, HIV education, long clinic waiting times, and clinic/health care service improvement. Participants also expressed enthusiasm regarding the prospective alcohol-focused adherence counseling program.
Discussion
This study sought to determine whether there is a relationship between levels of alcohol use and ART adherence and the extent of perceived appropriateness, acceptability, and utility of elements of a proposed alcohol-focused adherence counseling program among ART recipients. Further, we assessed whether sex, drinking levels, and adherence levels are associated with preference of elements of an alcohol-focused adherence counseling program.
As in prior research,16 we found support for the hypothesis that a high degree of alcohol use (problem drinking) was associated with the lowest ART adherence levels. On the other hand, potentially due to low sample sizes in each level of alcohol consumption, we did not find a significant relationship between alcohol consumption and ART adherence, although we did find a general trend of a lower proportion of high ART adherence with increasing quantity of alcohol use. The average self-reported ART adherence rate in this sample was 89.7%, which is above the average reported in some African countries.13 However, considering the commonly used cutoff of ≥95% adherence to indicate optimal adherence, just over two thirds (67.8%) of participants were adherent to their prescribed ART regimen.
About 40% of the participants reported lifetime alcohol use, while very few reported lifetime use of other drugs. The prevalence of hazardous or harmful drinking was 74.5% and 54.9% for male and female drinkers, respectively. Just under one third of the drinkers as a group cited taking alcohol/drugs as a reason for missing ART doses; a potentially modifiable barrier to ART adherence via targeted intervention efforts. Consistent with prior research,34,46–48 “simply forgot” was the most common reason for skipping ART doses.
The most preferred facilitator for an alcohol-focused adherence counseling program was a peer (ie, a fellow patient on ART), closely followed by an adherence counselor. The preference for these types of facilitators is not surprising, given that adherence counselors/peer interveners are often ART patients who have excelled at adherence themselves and undergone training in basic counseling and related matters.49–51 Although challenges may arise in training such lay counselors to deliver behavioral interventions (eg, MI and CBT) for alcohol reduction, in a setting of inadequate mental health professionals,41,52 use of lay counselors may be appropriate to ensure sustainability of the intervention. Indeed, Papas et al53,54 demonstrated that lay counselors (paraprofessionals) could deliver a CBT-based alcohol reduction intervention with high fidelity in a non-English language (Kiswahili).
The preference for health care providers as facilitators of the proposed alcohol-focused intervention by those with high ART adherence warrants further investigation, because this potentially is an indicator of the quality of the health care provider-patient relationship; a construct associated with adherence and adherence self-efficacy beliefs in serious medical conditions including HIV.55,56 Nevertheless, it is interesting that, across the sample as a whole, the peer intervener and the adherence counselor were preferred over both clinic and outside health care professionals. This finding could be explained by the common view that individuals having personal experience of a particular problem are best placed to help others overcome the same problem,49,57,58 as with support groups for chronic social and medical problems.59 Patients’ reported negative experiences with HIV clinic staff60 might also account for the latter finding. The least preferred facilitator was a person from the community, which might be attributable to HIV-related stigma,48,61,62 or inability of the participant to fathom why a person lacking a shared HIV experience could be expected to be effective.
Generally, participants mostly preferred a clinic-based one-hour session across two sessions in a group format. Moreover, there was notable preference among problem drinkers for sessions longer than one hour. This may reflect a greater perceived need for alcohol-focused adherence counseling among problem drinkers. Significant preference for group sessions was also notable for nondrinkers and problem drinkers, as well as for those with high adherence. The high preference of those with high adherence for self-directed formats (watching videotapes and reading printed material/brochures) potentially points to unmeasured fundamental differences between those with high and low adherence, such as autonomous regulation, which is thought to contribute to ART adherence via mediators like self-efficacy.63
Men were more opposed than women to a two-person session, and marginally opposed to the community setting (separate from a support group) as a setting for program attendance. Rather, men had a higher preference than women for other settings (eg, workplace) in addition to community-based ones. These findings might be explained by men’s preference to keep their health information private64–66 and their reporting of significantly higher perceived HIV stigma in their communities.
Overall, the patients’ attitudes toward family members/friends attending the sessions was very favorable, which is in line with previous research,37,67 indicating the appeal of patient-nominated “treatment supporters.”
The overall high preference for “share strategies for coping that do not involve alcohol” as part of the content of the intervention suggests that a CBT-type of intervention might be acceptable. This proposition is in line with the fact that skills building (eg, as it relates to emotion regulation, interpersonal, or problem-solving deficits) is one of the core elements of CBT for substance use disorders.68 Indeed, communication and coping skills training are commonly part of CBT for substance use disorders and have yielded positive outcomes in the treatment of substance use disorders.69,70 The overall high preference for “discussing advantages and disadvantages of not drinking” (decisional balance, a useful technique in effecting substance use-related behavior change),71 as part of the intervention’s content seems to suggest that an MI-based approach might also be an acceptable intervention strategy. Consequently, from this local research with ART recipients, we could expect people living with HIV/acquired immune deficiency syndrome to have a favorable attitude to an alcohol-focused adherence counseling program that employs MI/CBT. Our study findings suggest it is plausible that a CBT/MI-based intervention to address alcohol-related nonadherence to ART in the South African context is feasible and could be delivered by lay counselors in group settings. This is a positive finding, given the evidence base supporting MI and CBT for alcohol reduction in general72–75 and among people living with HIV/acquired immune deficiency syndrome.76
The participants in this study thought that it would be important for the additional adherence counseling program to address diverse issues such as cigarette smoking, food insecurity, stigma, low social support, and abuse of other drugs, most of which have been found to be barriers to ART adherence in prior research.39–43,61 The perceived importance of addressing food insecurity in an ART adherence-related intervention is not surprising, given that most of the participants were unemployed and about a third reported having missed ART doses due to a lack of food; and just under two thirds indicated a significant degree of food insecurity. Moreover, food insecurity has been cited as a notable barrier to ART adherence.60,77–79
The study had a number of limitations. First, since relatively few participants reported taking alcohol/drugs as the reason for missing ART doses, the current participants’ views may not be generalizable to those of likely recipients of the proposed intervention, and hence are worth interpreting with some caution. Second, we relied on self-report for assessing adherence levels and alcohol use, both of which may have questionable reliability. Study participants could conceivably under-report their alcohol use in health care settings, given the prevalent communication by health care providers that alcohol use is prohibited while on ART.42,80,81 Under-reporting of nonadherence can also be expected, as individuals may have a need to seem adherent to the prescriptions and behaviors required by their health care providers; thus fitting the “good patient” persona.66,82 Third, the use of closed-ended questions with Likert scale response options and binary response options (yes/no) does not give a full nuanced view of the participants’ perspective, which is best suited to a qualitative study. Fourth, as a result of potential self-selection bias, the prevalence of hazardous drinking (based on the AUDIT score) is high, but might not be representative of patients attending HIV clinics locally. Lastly, the cross-sectional nature of this study does not allow inferences of causality, hence there is a possibility that suboptimal adherence to ART is accounted for by other factors, such as depression. Depression has been found to be comorbid with alcohol use disorders in some studies.83
The results of the study have implications for the design of adherence counseling programs with a focus on decreasing alcohol-related nonadherence to ART as well as for health care workers who provide ART and manage patients on ART. Based on the marked prevalence of hazardous drinking amongst patients who drink alcohol, we propose routine and ongoing screening for harmful use of alcohol and alcohol use disorders among all HIV patients. Provision of on-site advice or brief counseling for those displaying harmful or hazardous use of alcohol and referrals to more intensive alcohol treatment services for those with serious alcohol-related problems are indicated. The study’s findings also suggest that ART patients would be amenable to brief MI/CBT-type interventions to address alcohol-related nonadherence that are delivered by lay persons within the clinic setting. The need for such interventions is not in question, but how they can be integrated into an already overburdened health care system is a question worthy of further investigation.
Acknowledgments
This paper was supported by Cooperative Agreement Number U2G/PS001137-02 from the Centers for Disease Control and Prevention. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention. The authors would like to thank Ms Mantoa Nzeku for managing the study, Ms Naledi Kitleli and Mr Kgalabi Ngako for supervising the field staff, and Ms Sebenzile Nkosi and Ms Naledi Kitleli for helping with analysis of the data. We are indebted to the clinic site managers and health care providers and to the patients who agreed to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
Floyd S, Molesworth A, Dube A, et al. Population-level reduction in adult mortality after extension of free anti-retroviral therapy provision into rural areas in northern Malawi. PLoS One. 2010;5(10):e13499. | |
Herbst AJ, Cooke GS, Bärnighausen T, KanyKany A, Tanser F, Newell ML. Adult mortality and antiretroviral treatment roll-out in rural KwaZulu-Natal, South Africa. Bull World Health Organ. 2009;87(10):754–762. | |
Johnson LF. Access to antiretroviral treatment in South Africa, 2004–2011. South Afr J HIV Med. 2012;13(1):22–27. | |
Shisana O. At last the glass is half full. Plenary presentation at the Sixth South African AIDS Conference, Durban, South Africa, Jun 2013. Available from: http://www.hsrc.ac.za/en/media-briefs/hiv-aids-stis-and-tb/plenary-session-3-20-june-2013-hiv-aids-in-south-africa-at-last-the-glass-is-half-full. Accessed December 9, 2013. | |
Kobin AB, Sheth NU. Levels of adherence required for virologic suppression among newer antiretroviral medications. Ann Pharmacother. 2011;45(3):372–379. | |
Li JZ, Paredes R, Ribaudo HJ, et al. Relationship between minority nonnucleoside reverse transcriptase inhibitor resistance mutations, adherence, and the risk of virologic failure. AIDS. 2012;26(2):185–192. | |
Nachega JB, Hislop M, Dowdy D, Chaisson RE, Regensberg L, Maartens G. Adherence to nonnucleoside reverse transcriptase inhibitor-based HIV therapy and virologic outcomes. Ann Intern Med. 2007;146(8):564–573. | |
Parienti JJ, Das-Douglas M, Massari V, et al. Not all missed doses are the same: sustained NNRTI treatment interruptions predict HIV rebound at low-to-moderate adherence levels. PLoS One. 2008;3(7):e2783. | |
Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;9(6):679–690. | |
Bangsberg DR, Haberer JE. Lifetime HIV antiretroviral therapy adherence intervention: timing is everything: comment on “managed problem solving for antiretroviral therapy adherence”. JAMA Intern Med. 2013;173(4):306–307. | |
Azar MM, Springer SA, Meyer JP, Altice FL. A systematic review of the impact of alcohol use disorders on HIV treatment outcomes, adherence to antiretroviral therapy and health care utilization. Drug Alcohol Depend. 2010;112(3):178–193. | |
Do NT, Phiri K, Bussmann H, Gaolathe T, Marlink RG, Wester CW. Psychosocial factors affecting medication adherence among HIV-1 infected adults receiving combination antiretroviral therapy (cART) in Botswana. AIDS Res Hum Retroviruses. 2010;26(6):685–691. | |
Etienne M, Hossain M, Redfield R, Stafford K, Amoroso A. Indicators of adherence to antiretroviral therapy treatment among HIV/AIDS patients in 5 African countries. J Int Assoc Physicians AIDS Care (Chic). 2010;9(2):98–103. | |
Farley J, Miller E, Zamani A, et al. Screening for hazardous alcohol use and depressive symptomatology among HIV-infected patients in Nigeria: prevalence, predictors, and association with adherence. J Int Assoc Physicians AIDS Care (Chic). 2010;9(4):218–226. | |
Hendershot CS, Stoner SA, Pantalone DW, Simoni JM. Alcohol use and antiretroviral adherence: review and meta-analysis. J Acquir Immune Defic Syndr. 2009;52(2):180–201. | |
Jaquet A, Ekouevi DK, Bashi J, et al. Alcohol use and non-adherence to antiretroviral therapy in HIV-infected patients in West Africa. Addiction. 2010;105(8):1416–1421. | |
Nakimuli-Mpungu E, Bass JK, Alexandre P, et al. Depression, alcohol use and adherence to antiretroviral therapy in sub-Saharan Africa: a systematic review. AIDS Behav. 2012;16(8):2101–2118. | |
Parsons JT, Rosof E. The temporal relationship between alcohol consumption and HIV-medication adherence: a multilevel model of direct and moderating effects. Health Psychol. 2008;27(5):628–637. | |
Braithwaite RS, McGinnis KA, Conigliaro J, et al. A temporal and dose-response association between alcohol consumption and medication adherence among veterans in care. Alcohol Clin Exp Res. 2005;29(7):1190–1197. | |
Morojele NK, Kekwaletswe CT, Nkosi S. Associations between alcohol use, other psychosocial factors, structural factors and antiretroviral therapy (ART) adherence among South African ART recipients. AIDS Behav. August 10, 2013. [Epub ahead of print.] | |
World Health Organisation. Global status report on alcohol and health. Geneva, Switzerland: World Health Organisation; 2011. Available from: http://www.who.int/substance_abuse/publications/global_alcohol_report/msbgsruprofiles.pdf. Accessed December 9, 2013. | |
Binford MC, Kahana SY, Altice FL. A systematic review of antiretroviral adherence interventions for HIV-infected people who use drugs. Curr HIV/AIDS Rep. 2012;9:287–312. | |
Mathes T, Pieper D, Antoine SL, Eikermann M. Adherence-enhancing interventions for highly active antiretroviral therapy in HIV-infected patients – a systematic review. HIV Med. 2013;14(10):583–595. | |
Simoni JM, Pearson CR, Pantalone DW, Marks G, Crepaz N. Efficacy of interventions in improving highly active antiretroviral therapy adherence and HIV-1 RNA viral load. A meta-analytic review of randomized controlled trials. J Acquir Immune Defic Syndr. 2006; 43 Suppl 1:S23–S35. | |
Say RE, Thomson R. The importance of patient preferences in treatment decisions – challenges for doctors. BMJ. 2003;327(7414):542–545. | |
Department of Health. The Expert Patient: A New Approach To Chronic Disease Management for the 21st Century. London, UK: Department of Health; 2001. | |
Weymann N, Härter M, Petrak F, Dirmaier J. Health information, behavior change, and decision support for patients with type 2 diabetes: development of a tailored, preference-sensitive health communication application. Patient Prefer Adherence. 2013;22(7):1091–1099. | |
National Department of Health. Clinical Guidelines for the Management of HIV and AIDS in Adults and Adolescents. Pretoria, South Africa: Republic of South Africa Department of Health; 2010. | |
Medical Research Council. South Africa Demographic and Health Survey: Women’s Questionnaire. Cape Town, South Africa: Medical Research Council; 2008. | |
Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption – II. Addiction. 1993;88(6):791–804. | |
Reinert DF, Allen JP. The Alcohol Use Disorders Identification Test (AUDIT): a review of recent research. Alcohol Clin Exp Res. 2002;26(2):272–279. | |
Pérula-de Torres LA, Fernández-García JA, Arias-Vega R, Muriel-Palomino M, Márquez-Rebollo E, Ruiz-Moral R. [Validity of AUDIT test for detection of disorders related with alcohol consumption in women]. Med Clin (Barc). 2005;125(19):727–730. Spanish. | |
Reinert DF, Allen JP. The alcohol use disorders identification test: an update of research findings. Alcohol Clin Exp Res. 2007;31(2):185–199. | |
Chesney MA, Ickovics JR, Chambers DB, et al. Self-reported adherence to antiretroviral medications among participants in HIV clinical trials: the AACTG adherence instruments. Patient Care Committee and Adherence Working Group of the Outcomes Committee of the Adult AIDS Clinical Trials Group (AACTG). AIDS Care. 2000;12(3):255–266. | |
Beyene KA, Gedif T, Gebre-Mariam T, Engidawork E. Highly active antiretroviral therapy adherence and its determinants in selected hospitals from south and central Ethiopia. Pharmacoepidemiol Drug Saf. 2009;18(11):1007–1015. | |
Bisson GP, Rowh A, Weinstein R, Gaolathe T, Frank I, Gross R. Antiretroviral failure despite high levels of adherence: discordant adherence-response relationship in Botswana. J Acquir Immune Defic Syndr. 2008;49(1):107–110. | |
Kunutsor S, Walley J, Katabira E, et al. Improving clinic attendance and adherence to antiretroviral therapy through a treatment supporter intervention in Uganda: a randomized controlled trial. AIDS Behav. 2011;15(8):1795–1802. | |
Steele KT, Steenhoff AP, Newcomb CW, et al. Early mortality and AIDS progression despite high initial antiretroviral therapy adherence and virologic suppression in Botswana. PLoS One. 2011;6(6):e20010. | |
Coetzee B, Kagee A, Vermeulen N. Structural barriers to adherence to antiretroviral therapy in a resource-constrained setting: the perspectives of health care providers. AIDS Care. 2011;23(2):146–151. | |
Dahab M, Charalambous S, Hamilton R, et al. “That is why I stopped the ART”: patients’ and providers’ perspectives on barriers to and enablers of HIV treatment adherence in a South African workplace programme. BMC Public Health. 2008;8:63. | |
Kagee A, Remien RH, Berkman A, Hoffman S, Campos L, Swartz L. Structural barriers to ART adherence in Southern Africa: challenges and potential ways forward. Glob Public Health. 2011;6(1):83–97. | |
Lyimo RA, de Bruin M, van den Boogaard J, Hospers HJ, van der Ven A, Mushi D. Determinants of antiretroviral therapy adherence in northern Tanzania: a comprehensive picture from the patient perspective. BMC Public Health. 2012;12:716. | |
Mills EJ, Nachega JB, Bangsberg DR, et al. Adherence to HAART: a systematic review of developed and developing nation patient-reported barriers and facilitators. PLoS Med. 2006;3(11):e438. | |
Hennink M, Hutter I, Bailey A. Qualitative Research Methods. London, UK: Sage Publications Ltd; 2011. | |
Saldana J. The Coding Manual for Qualitative Researchers. London, UK: Sage Publications Ltd; 2009. | |
Barfod TS, Sørensen HT, Nielsen H, Rodkjær L, Obel N. ‘Simply forgot’ is the most frequently stated reason for missed doses of HAART irrespective of degree of adherence. HIV Med. 2006;7(5):285–290. | |
Tadios Y, Davey G. Antiretroviral treatment adherence and its correlates in Addis Ababa, Ethiopia. Ethiop Med J. 2006;44(3):237–244. | |
Vyankandondera J, Mitchell K, Asiimwe-Kateera B, et al. Antiretroviral therapy drug adherence in Rwanda: perspectives from patients and healthcare workers using a mixed-methods approach. AIDS Care. 2013;25(12):1504–1512. | |
Simoni JM, Franks JC, Lehavot K, Yard SS. Peer interventions to promote health: conceptual considerations. Am J Orthopsychiatry. 2011;81(3):351–359. | |
Gusdal AK, Obua C, Andualem T; for INRUD-IAA project. Peer counselors’ role in supporting patients’ adherence to ART in Ethiopia and Uganda. AIDS Care. 2011;23(6):657–662. | |
Simoni JM, Huh D, Frick PA, et al. An RCT of peer support and pager messaging to promote antiretroviral therapy adherence and clinical outcomes among adults initiating or modifying therapy in Seattle, WA, USA. J Acquir Immune Defic Syndr. 2009;52(4):465–473. | |
Kagee A. Training lay counsellors to provide psychosocial support to ART users: successes and failures. AIDS Care. 2013;25(4):496–502. | |
Papas RK, Sidle JE, Martino S, et al. Systematic cultural adaptation of cognitive-behavioral therapy to reduce alcohol use among HIV-infected outpatients in western Kenya. AIDS Behav. 2010;14(3):669–678. | |
Papas RK, Sidle JE, Gakinya BN, et al. Treatment outcomes of a stage 1 cognitive-behavioral trial to reduce alcohol use among human immunodeficiency virus-infected out-patients in western Kenya. Addiction. 2011;106(12):2156–2166. | |
Fuertes JN, Boylan LS, Fontanella JA. Behavioral indices in medical care outcome: the working alliance, adherence, and related factors. J Gen Intern Med. 2009;24(1):80–85. | |
Fuertes JN, Mislowack A, Bennett J, et al. The physician-patient working alliance. Patient Educ Couns. 2007;66(1):29–36. | |
Robinson D. Self-help groups in primary health care. World Health Forum. 1981;(2):185–191. | |
Nayar KR, Kyobutungi C, Razum O. Self-help: what future role in health care for low and middle-income countries? Int J Equity Health. 2004;3(1):1. | |
Martin CM, Peterson C, Robinson R, Sturmberg JP. Care for chronic illness in Australian general practice – focus groups of chronic disease self-help groups over 10 years: implications for chronic care systems reforms. Asia Pac Fam Med. 2009;8(1):1. | |
Kagee A, Delport TJ. Barriers to adherence to antiretroviral treatment: the perspectives of patient advocates. Health Psychol. 2010;15(7):1001–1011. | |
Dlamini PS, Wantland D, Makoae LN, et al. HIV stigma and missed medications in HIV-positive people in five African countries. AIDS Patient Care STDS. 2009;23(5):1–11. | |
Gilbert L, Walker L. ‘My biggest fear was that people would reject me once they knew my status...’: stigma as experienced by patients in an HIV/AIDS clinic in Johannesburg, South Africa. Health Soc Care Community. 2010;18(2):139–146. | |
Lynam I, Catley D, Goggin K, et al. Autonomous regulation and locus of control as predictors of antiretroviral medication adherence. J Health Psychol. 2009;14(4):578–586. | |
Fitzgerald M, Collumbien M, Hosegood V. “No one can ask me ‘Why do you take that stuff?’”: men’s experiences of antiretroviral treatment in South Africa. AIDS Care. 2010;22(3):355–360. | |
Madiba S, Canti-Sigaqa V. Barriers to participate in support groups for people living with HIV: a qualitative study with men receiving antiretroviral treatment in a HIV clinic in Mthatha, South Africa. Glob J Health Sci. 2012;4(6):119–128. | |
Skovdal M, Campbell C, Madanhire C, Mupambireyi Z, Nyamukapa C, Gregson S. Masculinity as a barrier to men’s use of HIV services in Zimbabwe. Global Health. 2011;7:13. | |
Nachega JB, Knowlton AR, Deluca A, et al. Treatment supporter to improve adherence to antiretroviral therapy in HIV-infected South African adults. a qualitative study. J Acquir Immune Defic Syndr. 2006;43 Suppl 1:S127–S133. | |
McHugh RK, Hearon BA, Otto MW. Cognitive-behavioral therapy for substance use disorders. Psychiatr Clin North Am. 2010;33(3):511–525. | |
Monti PM, Rohsenow DJ, Swift RM, et al. Naltrexone and cue exposure with coping and communication skills training for alcoholics: treatment process and 1-year outcomes. Alcohol Clin Exp Res. 2001;25:1634–1647. | |
Rohsenow DJ, Monti PM, Rubonis AV, et al. Cue exposure with coping skills training and communication skills training for alcohol dependence: 6-and 12-month outcomes. Addiction. 2001;96:1161–1174. | |
Apodaca TR, Longabaugh R. Mechanisms of change in motivational interviewing: a review and preliminary evaluation of the evidence. Addiction. 2009;104(5):705–715. | |
Berglund M, Thelander S, Jonsson E, editors. Treating Alcohol and Drug Abuse: An Evidenced Based Review. New York, NY, USA: Wiley-VCH; 2003. | |
Magill M, Ray LA. Cognitive-behavioral treatment with adult alcohol and illicit drug users: a meta-analysis of randomized controlled trials. J Stud Alcohol Drugs. 2009;70(4):516–527. | |
Martin G, Rehm J. The effectiveness of psychosocial modalities in the treatment of alcohol problems in adults: a review of the evidence. Can J Psychiatry. 2012;57(6):350–358. | |
Smedslund G, Berg RC, Hammerstrom KT, et al. Motivational interviewing for substance abuse. Cochrane Database Syst Rev. 2011;5:CD008063. | |
Parsons JT, Golub SA, Rosof E, Holder C. Motivational interviewing and cognitive-behavioral intervention to improve HIV medication adherence among hazardous drinkers: a randomized controlled trial. J Acquir Immune Defic Syndr. 2007;46(4):443–450. | |
Goudge J, Ngoma B. Exploring antiretroviral treatment adherence in an urban setting in South Africa. J Public Health Policy. 2011;32 Suppl 1:S52–S64. | |
Young S, Wheeler AC, McCoy SI, Weiser SD. A review of the role of food insecurity in adherence to care and treatment among adult and pediatric populations living with HIV and AIDS. AIDS Behav. July 11, 2013. [Epub ahead of print.] | |
Weiser SD, Palar K, Frongillo EA, et al. Longitudinal assessment of associations between food insecurity, antiretroviral adherence and HIV treatment outcomes in rural Uganda. AIDS. August 9, 2013. [Epub ahead of print.] | |
Kalichman SC, Amaral, CM, White D, et al. Alcohol and adherence to antiretroviral medications: interactive toxicity beliefs among people living with HIV. J Assoc Nurses AIDS Care. 2012;23(6):511–520. | |
Kalichman SC, Grebler T, Amaral CM, et al. Intentional non-adherence to medications among HIV positive alcohol drinkers: prospective study of interactive toxicity beliefs. J Gen Intern Med. 2013;28(3):399–405. | |
McCreaddie M, Wiggins S. Reconciling the good patient persona with problematic and non-problematic humour: a grounded theory. Int J Nurs Stud. 2009;46(8):1079–1091. | |
Riper H, Andersson G, Hunter SB, de Wit J, Berking M, Cuijpers P. Treatment of comorbid alcohol use disorders and depression with cognitive-behavioural therapy and motivational interviewing: a meta-analysis. Addiction. December 4, 2013. [Epub ahead of print.] |
Supplementary material
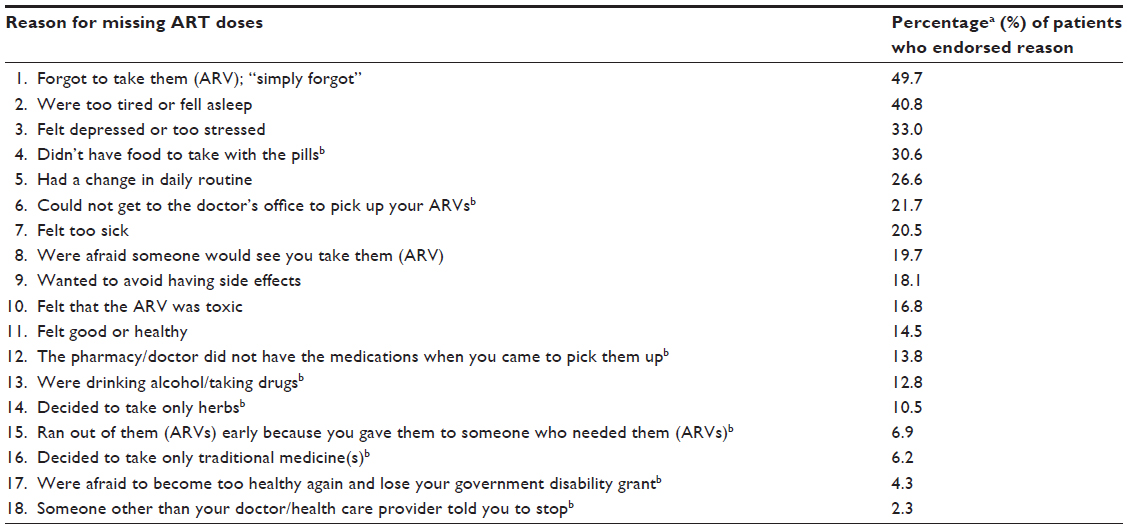 | Table S1 Reasons endorsed by patients for missing doses of ART |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.