")
Back to Journals » International Medical Case Reports Journal » Volume 13
Airway Management with Dexmedetomidine and High-Flow Nasal Cannula in a Patient with Deep Neck Infection
Authors Kim HJ, Lee S, Cho HM , Kim KW , Choi HR , Bang SR
Received 7 August 2020
Accepted for publication 17 November 2020
Published 2 December 2020 Volume 2020:13 Pages 679—683
DOI https://doi.org/10.2147/IMCRJ.S276018
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Hyo Jin Kim, Solyi Lee, Hak Moo Cho, Kyung Woo Kim, Hey Ran Choi, Si Ra Bang
Department of Anesthesiology and Pain Medicine, Inje University Seoul Paik Hospital, Seoul, Korea
Correspondence: Si Ra Bang
Department of Anesthesiology and Pain Medicine, Inje University Seoul Paik Hospital, Seoul, Korea
Tel +82-2-2270-0095
Fax +82-2-2270-0094
Email [email protected]
Abstract: Retropharyngeal deep neck infection sometimes necessitates securing of the airway and surgery for drainage. Airway management in patients with deep neck infection is challenging for anesthesiologists. A 56-year-old woman diagnosed with deep neck infection was admitted for incision and drainage. In the first operation for incision and drainage, indirect videolaryngoscope was utilized to confirm the airway before tracheal intubation, and the patient was intubated successfully. In the second operation for wound closure, dexmedetomidine administration and high-flow nasal cannulation were used during monitored anesthesia care throughout a subsequent procedure. The outcome in the present case suggests that indirect videolaryngoscope, dexmedetomidine, and high-flow nasal cannula can facilitate effective management during surgery in patients with retropharyngeal deep neck space infection.
Keywords: dexmedetomidine, high-flow nasal cannula, indirect laryngoscope, neck infection
Introduction
Deep neck infection refers to infection of the potential spaces and fascial planes of the neck in which abscesses and cellulitis can form.1 It can result in rapid progression associated with serious complications such as edema, distortion, and potentially fatal airway obstruction. It can also involve bilateral communication between the retropharyngeal space and the parapharyngeal spaces, which contain the carotid sheaths and border the “danger” space posteriorly that extends from the skull base to the posterior mediastinum.2
Many cases of severe neck infection require securing of the airway, and surgery for drainage. Because of the numerous potential complexities involved, airway management of patients with deep neck infection can be challenging for anesthesiologists. For a long time, the gold standard of difficult airway management was awake fiberoptic intubation.3 Notably however, it can be technically difficult and cause discomfort and pain. Herein we report the details of a case of deep neck infection in which indirect videolaryngoscope, dexmedetomidine administration, and high-flow nasal cannula were utilized.
Case Report
The patient whose case is described herein provided written informed consent for its publication. This study was approved by the Institutional Review Board of Inje University Seoul Paik Hospital (PAIK 2020-10-003). A 56-year-old woman 150 cm in height and weighing 86 kg was admitted with a diagnosis of deep neck infection for incision and drainage. She reported that she had experienced neck swelling and tenderness for the past 6 days. She had been diagnosed with hypertension 6 years prior, and her blood pressure was well controlled via medication.
Preoperative airway evaluation revealed Mallampatti class IV with mouth opening of less than three finger widths.4 Neck computed tomography (CT) findings included right side retropharyngeal abscess extending to the anterior and posterior cervical space and carotid space (Figure 1). She was not premedicated. In the operating theater, her initial vital signs were blood pressure 140/83 mmHg, heart rate 110 beats/min, and saturation of percutaneous oxygen (SpO2) 97%. Her arterial blood gas analysis results included mild respiratory alkalosis due to tachypnea with a respiration rate of 25 breaths/min, pH 7.50, partial pressure of CO2 34.1 mmHg, partial pressure of O2 124.6 mmHg, and O2 saturation 99%. Oxygen saturation was maintained above 97% throughout the procedure.
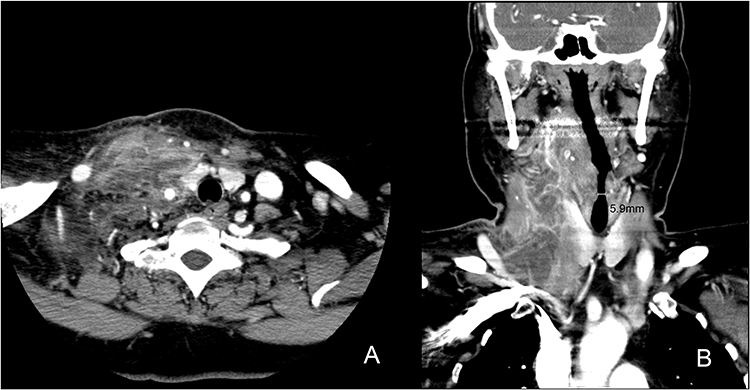 |
Figure 1 (A) An axial view computed tomography image depicting right side retropharyngeal abscess extending to the carotid space. (B) A coronal view computed tomography image. The narrowest part of the airway was approximately 5.9 mm in diameter. |
Preoxygenation was administered via a facial mask with 100% oxygen for more than 5 min. Potentially difficult intubation was anticipated, and accordingly, an indirect videolaryngoscope (UEScope®, UE Medical Devices, MA, USA) was prepared, as were endotracheal tubes (ETTs) of various diameters. Prior to anesthesia, we planned to confirm the airway via videolaryngoscope and then decide whether awake intubation should be performed or not. After applying lidocaine spray, indirect videolaryngoscopic airway examination was performed. To topicalize the airway near the epiglottis 60 mg of 10% lidocaine spray (10 mg/puff) was administered via the patient’s oral cavity, followed by gargling. Upon inspection the epiglottis was visible, but the glottis was not (Cormack and Lehane grade 3).5 After confirming visualization of the epiglottis via indirect videolaryngoscope, intubation using indirect videolaryngoscope was performed under general anesthesia. Sugammadex 400 mg was prepared in case of failed intubation. General anesthesia was induced via propofol 120 mg and rocuronium 60 mg prior to tracheal intubation. Mask ventilation was feasible with a two-handed technique, and a tidal volume of 300 mL was achieved at approximately 20 cmH2O of peak airway pressure. Intubation was initially attempted with an ETT with an internal diameter (ID) of 7.0 mm, but that tube was subsequently changed to a 6.5-mm ID ETT due to difficulty passing the vocal cord, then the patient was successfully intubated. Oxygen saturation was maintained above 97% throughout the procedure.
Anesthesia was maintained with 1.7 volume % of sevoflurane and remifentanil, 2 L/min of air, and 2 L/min of O2. Pressure-controlled ventilation mode was used. During the procedure end-tidal CO2 was maintained at 28–30 mmHg and pulse oximetry was 100%. The surgery consisted of incision and retropharyngeal abscess drainage via a transcervical approach, and the surgeon decided to delay wound closure.
At the end of the operation, the patient was transferred directly to the intensive care unit (ICU) and breathing was maintained via a mechanical ventilator due to the risk of airway obstruction after extubation. In the ICU, saturation was evidently well controlled at above 95% via pressure-controlled ventilation, as evidenced by tidal volume 450 mL, respiration rate 12 breaths/min, and PEEP 5 cmH2O under FiO2 0.4.
The next day, while still in the ICU, the patient recommenced spontaneous breathing and was subsequently successfully extubated. The surgeon decided to perform wound closure and packing gauze removal the following day. Monitored anesthesia care was planned to avoid repeated intubation.
The patient was not premedicated. On arrival in the operating room noninvasive blood pressure monitoring, electrocardiography, pulse oximetry, and end-tidal CO2 measurement via a nasal cannula with 100% O2 at 3 L/min were instigated. Sedation was established via continuous infusion of dexmedetomidine at 6 µg/kg/hr. After dexmedetomidine administration, SpO2 decreased to 95%, and therefore the patient was changed to a reservoir mask with 100% O2 administered at 6 L/min. SpO2 then dropped to 94%, prompting a decision to use high-flow nasal cannula (Optiflow™; Fisher and Paykel Healthcare, Auckland, New Zealand) oxygen delivery set to 30 L/min of humidified oxygen flow (fractional inspired oxygen 1.0).
SpO2 was maintained at 100%. After a loading dose of dexmedetomidine 6 µg/kg/hr for 10 min, the dose was reduced to 0.6 µg/kg/hr. Prior to the incision, 50 µg of fentanyl was administered. After approximately 20 min, fentanyl 50 µg and midazolam 1 mg were administered and dexmedetomidine was increased to 0.7–1.0 µg/kg/hr because the patient complained of ongoing discomfort. During the procedure, her vital signs were stable and there were no signs of bradycardia. She did not report any discomfort during subsequent operations. The level of consciousness was monitored using the Observer’s Assessment of Alertness and Sedation (OAA/S) score. An OAA/S score of 2 was maintained throughout the operation.6
In the recovery room, 100% O2 at 3 L/min was supplied via a nasal cannula, and O2 saturation was maintained at 96–100%. She was then transported to a general hospital room. On the 12th postoperative day, she was discharged without any sequelae.
Discussion
The retropharyngeal space ascends from the skull base to the tracheal bifurcation and lies anterior to the prevertebral fascia.7 In adults, retropharyngeal abscesses of the neck tend to develop via direct extension from adjacent structures, or compression. The condition can constitute a life-threatening emergency involving airway compromise and other potentially fatal complications.8 Factors associated with the high mortality rate include airway obstruction, mediastinitis, aspiration pneumonia, epidural abscess, jugular venous thrombosis, necrotizing fasciitis, sepsis, and erosion into the carotid artery.9 The condition may require prompt surgical drainage. In the present case, the patient reported suffering from neck swelling, and CT scanning depicted severe narrowing of the airway that required urgent surgery.
It has been recommended that awake fiberoptic intubation should be used for airway management in patients with an airway obstruction in difficult airway situations.3 Awake fiberoptic intubation can be a painful procedure however, and it requires a specific level of technical training.10 Videolaryngoscope provides a wider field of vision, facilitates imaging of laryngeal structures beyond the scope of conventional direct laryngoscopy, and is now considered by some anesthesiologists to be a first-line intubation technique for routine, difficult, and rescue intubations.11 In the present case, videolaryngoscope was conducted to assess laryngeal structure before intubation, in an effort to facilitate more accurate estimation of the likelihood of successful intubation. The final decision on whether to induce general anesthesia was made after confirming the airway via videolaryngoscope just before anesthesia induction. Even with local anesthesia, awake intubation can cause discomfort and anxiety to the patient. In the present case, we could not attempt topicalization via methods such as superior laryngeal blockade or transtracheal injection of lidocaine, due to the distorted airway. Videolaryngoscope was helpful for evaluating the airway immediately prior to general anesthesia induction, to determine whether awake intubation could be performed.
According to the labeled dosage recommendation, 16 mg/kg sugammadex induces immediate recovery of neuromuscular blockade after an intubating dose of 1.2 mg/kg of rocuronium. Sugammadex 4 mg/kg is recommended for the reversal of deep neuromuscular blockade.12 In the current case, 0.8 mg/kg rocuronium was administered to induce general anesthesia; therefore, we prepared 400 mg sugammadex in a syringe as an initial shot. We were also prepared for the injection of additional sugammadex, should that have been required.
The second operation was more challenging because the trachea was not secured via intubation. In view of this, dexmedetomidine and high-flow nasal cannula for oxygenation were utilized in an effort to achieve sedation without respiratory difficulty.
Dexmedetomidine is a lipophilic imidazole derivative and a highly selective α-2 adrenergic receptor agonist that exerts sedative and analgesic effects, with minimal effects on ventilation.13 The administration of high doses (10 µg/kg/hr) to patients undergoing airway surgery can reportedly maintain ventilatory drive, but may cause obstructive apnea and increased blood pressure via increased peripheral vascular resistance.13 Given the potential for sudden exogenous catecholamine release, rapid administration may lead to tachycardia, bradycardia, and hypertension.14 In this case, the loading dose of dexmedetomidine used was only 6 µg/kg/hr, and vital signs remained stable during the procedure.
High-flow nasal cannula provides oxygen at a high-flow rate and surpasses low-flow and intermediate-flow devices by delivering up to 60 L/min of heated humidified gas via the patient’s nasal opening.15 High-flow nasal cannulas are able to titrate fractional inspired oxygen up to 1.0 and consistently deliver highly oxygenated flow to the alveoli because they can provide higher flow rates than conventional inspiratory flow, and can decrease entrapment of room air.16 High-flow nasal cannula generates a low-level PEEP effect, washout of the pharyngeal dead space, reduction of the “work of breathing”, increased alveolar recruitment, and improved mucociliary clearance and patient comfort.17 It is reportedly superior to conventional oxygenation techniques in specific groups of patients who need tracheal intubation in the operating room such as obese patients and pregnant patients, or patients requiring rapid-sequence induction of anesthesia, and in such cases, it may be an effective technique for delaying hypoxemia during anesthesia management.16
Mortality from failure of airway management still occurs in patients with severe deep neck infection.18 Securing the airway remains an ongoing challenge for anesthesiologists. In the present case, indirect laryngoscopy, dexmedetomidine administration, and high-flow nasal cannula were affective for the management of retropharyngeal deep neck space infection.
Conclusions
Indirect laryngoscopy, dexmedetomidine, and high-flow nasal cannulation may facilitate effective management during surgery in patients with retropharyngeal deep neck space infection.
Acknowledgment
We thank Dr Owen Proudfoot from Editage (www.editage.co.kr) for English language editing.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Wang LF, Kuo WR, Tsai SM, Huang KJ. Characterizations of life-threatening deep cervical space infections: a review of one hundred ninety-six cases. Am J Otolaryngol. 2003;24(2):111–117. doi:10.1053/ajot.2003.31.
2. Argintaru N, Carr D. Retropharyngeal abscess: a subtle presentation of a deep space neck infection. J Emerg Med. 2017;53(4):568–569. doi:10.1016/j.jemermed.2017.06.004
3. Law JA, Broemling N, Cooper RM, et al. The difficult airway with recommendations for management–part 2–the anticipated difficult airway. Can J Anaesth. 2013;60(11):1119–1138. doi:10.1007/s12630-013-0020-x
4. Mallampati SR, Gatt SP, Gugino LD, et al. A clinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985;32(4):429–434. doi:10.1007/bf03011357
5. Cormack RS, Lehane J. Difficult tracheal intubation in obstetrics. Anaesthesia. 1984;39(11):1105–1111. doi:10.1111/j.1365-2044.1984.tb08932.x
6. Kasuya Y, Govinda R, Rauch S, Mascha EJ, Sessler DI, Turan A. The correlation between bispectral index and observational sedation scale in volunteers sedated with dexmedetomidine and propofol. Anesth Analg. 2009;109(6):1811–1815. doi:10.1213/ANE.0b013e3181c04e58
7. Li RM, Kiemeney M. Infections of the neck. Emerg Med Clin North Am. 2019;37(1):95–107. doi:10.1016/j.emc.2018.09.003
8. Harkani A, Hassani R, Ziad T, et al. Retropharyngeal abscess in adults: five case reports and review of the literature. Sci World J. 2011;11:1623–1629. doi:10.1100/2011/915163
9. Herzon FS, Martin AD. Medical and surgical treatment of peritonsillar, retropharyngeal, and parapharyngeal abscesses. Curr Infect Dis Rep. 2006;8(3):196–202. doi:10.1007/s11908-006-0059-8
10. Collins SR, Blank RS. Fiberoptic intubation: an overview and update. Respir Care. 2014;59(6):
11. Berkow LC, Morey TE, Urdaneta F. The technology of video laryngoscopy. Anesth Analg. 2018;126(5):1527–1534. doi:10.1213/ane.0000000000002490
12. Herring WJ, Woo T, Assaid CA, et al. Sugammadex efficacy for reversal of rocuronium- and vecuronium-induced neuromuscular blockade: a pooled analysis of 26 studies. J Clin Anesth. 2017;41:84–91. doi:10.1016/j.jclinane.2017.06.006
13. Boyd BC, Sutter SJ. Dexmedetomidine sedation for awake fiberoptic intubation of patients with difficult airways due to severe odontogenic cervicofacial infections. J Oral Maxillofac Surg. 2011;69(6):1608–1612. doi:10.1016/j.joms.2010.11.004
14. Grant SA, Breslin DS, MacLeod DB, Gleason D, Martin G. Dexmedetomidine infusion for sedation during fiberoptic intubation: a report of three cases. J Clin Anesth. 2004;16(2):124–126. doi:10.1016/j.jclinane.2003.05.010
15. Drake MG. High-flow nasal cannula oxygen in adults: an evidence-based assessment. Ann Am Thorac Soc. 2018;15(2):145–155. doi:10.1513/AnnalsATS.201707-548FR
16. Asai T, Kim HJ. High-flow nasal oxygenation for anesthetic management. Korean J Anesthesiol. 2019. doi:10.4097/kja.19174
17. Renda T, Corrado A, Iskandar G, Pelaia G, Abdalla K, Navalesi P. High-flow nasal oxygen therapy in intensive care and anaesthesia. Br J Anaesth. 2018;120(1):18–27. doi:10.1016/j.bja.2017.11.010
18. Ovassapian A, Tuncbilek M, Weitzel EK, Joshi CW. Airway management in adult patients with deep neck infections: a case series and review of the literature. Anesth Analg. 2005;100(2):585–589. doi:10.1213/01.Ane.0000141526.32741.Cf
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.