")
Back to Journals » International Journal of General Medicine » Volume 14
Airway Clearance Therapy in Cystic Fibrosis Patients Insights from a Clinician Providing Cystic Fibrosis Care
Authors Chaudary N , Balasa G
Received 15 April 2021
Accepted for publication 25 May 2021
Published 14 June 2021 Volume 2021:14 Pages 2513—2521
DOI https://doi.org/10.2147/IJGM.S274196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nauman Chaudary, Gabriella Balasa
Division of Pulmonary Disease and Critical Care Medicine, Department of Internal Medicine, Virginia Commonwealth University School of Medicine, Richmond, VA, USA
Correspondence: Nauman Chaudary
VCU Adult Cystic Fibrosis Center, Division of Pulmonary Disease and Critical Care Medicine, 1200 East Broad Street, Box 980050, Richmond, VA, 23298, USA
Tel +1 804 828-1579
Fax +1 804 828-2578
Email [email protected]
Abstract: Cystic fibrosis (CF) is a genetic disease characterized by an accumulation of thick layers of mucus, leading to airway obstruction and air trapping. Poorly cleared mucus leads to frequent respiratory infections that produce chronic cough and dyspnea. The presence of infected mucus induces progressive inflammation. The resulting damage anatomically distorts airways leading to development of bronchiectasis. Bronchiectasis is irreversible and results in progressive respiratory function decline over time. Impaired mucociliary clearance together with tenacious mucus makes expectoration with cough alone problematic. Clinicians providing effective care for CF patients must have knowledge of the wide variety of treatment options currently available. Knowledge of these techniques will enable clinicians to prescribe airway clearance therapy (ACT) where necessary and provide treating physicians the ability to adapt to changing patient treatments as necessary. Training programs frequently do not provide in-depth knowledge of ACT technologies in CF patients resulting in knowledge gaps once physicians are in practice. This paper reviews strategies for ACT. It is specifically targeted for clinicians who frequently provide care for patients with CF.
Keywords: cystic fibrosis, airway clearance
Introduction
Patients with CF frequently present with cough and mucus clearance problems. The lungs of CF patients are responsible for the majority of morbidity and mortality this patient population undergoes. To keep lungs clear of infection and inflammation, the average CF patient must devote over 100 min focused on airway clearance each day. Most ACT studies are focused on sputum clearance and less on changes in lung function or exercise capacity.
Physiology of Mucus Secretion and Cough
Airway mucus production and water secretion are tightly regulated events and carry key physiological functions. Further, airway mucous possesses important antibacterial and protective properties. Airway glands typically produce less than 10 mL of mucus per day. Excess mucus production, a manifestation in CF, results in loss of its protective effects. Excessive mucus leads to cough that induces airway constriction the result of which expels mucus from the lungs. However, excessive cough, a characteristic of CF, leads to airway collapse with a failure to adequately clear mucus.1 See Table 1.
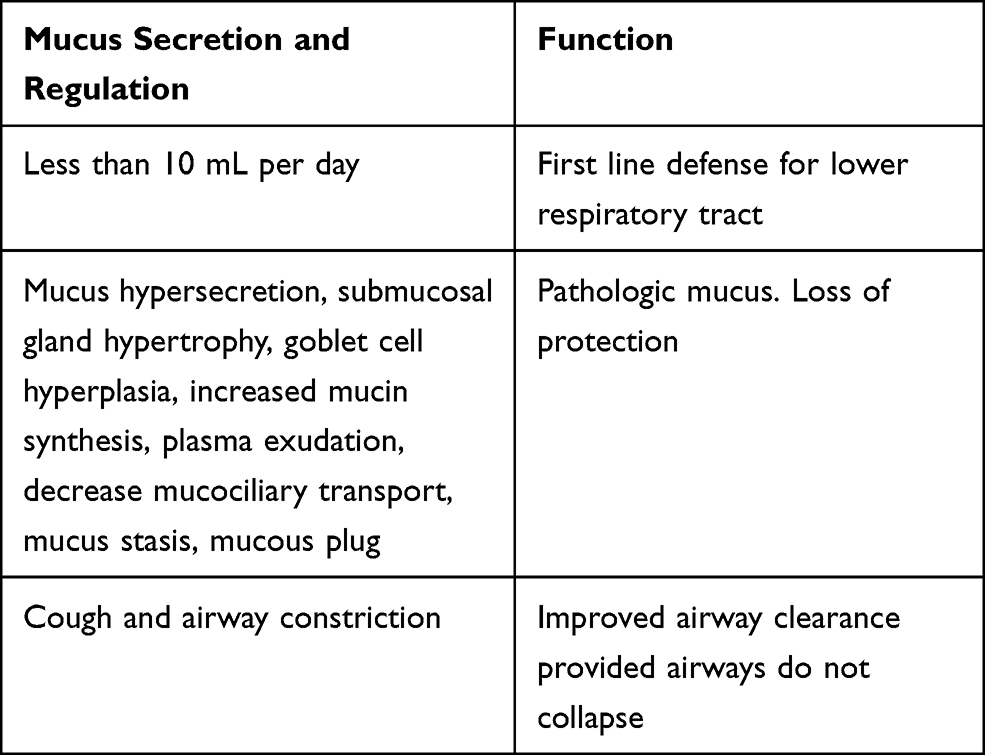 |
Table 1 Physiology of Mucus, Cough, and Airway Clearance |
Drugs That Play a Role in Airway Clearance
Pharmacotherapies have targeted airway bronchodilation, mucolytic, sympathomimetic, anticholinergic, and anti-inflammatory categories. Most pharmacological studies focused on airway clearance are inconclusive. A recent Cochrane review of mucolytic agents in chronic obstructive lung disease suggests this agent class may be of benefit.2 See Table 2
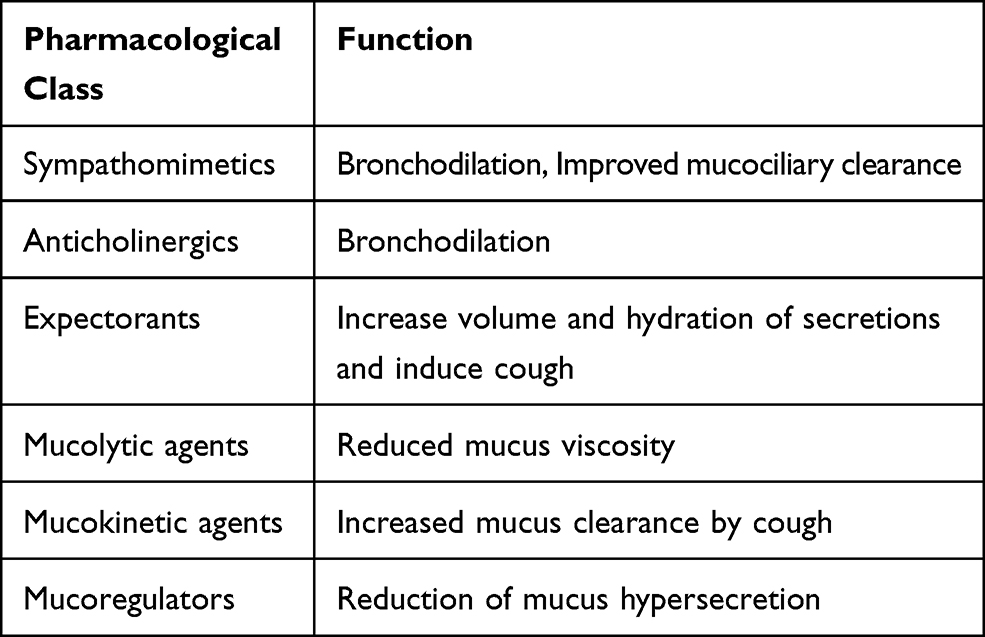 |
Table 2 Role of Pharmacologic Categories in Airway Clearance |
Airway Clearance Techniques That Do Not Require Devices
Airway Clearance Techniques (ACT)
For many decades airway clearance techniques have been used that require patient participation and changes in body posture to enhance clearance and to produce effective coughs that ultimately help recruit poorly ventilated lung zones. Generally, these techniques help restore mucociliary escalator function and mucus production which ultimately improves gas-liquid interface interaction in airways. See Table 3
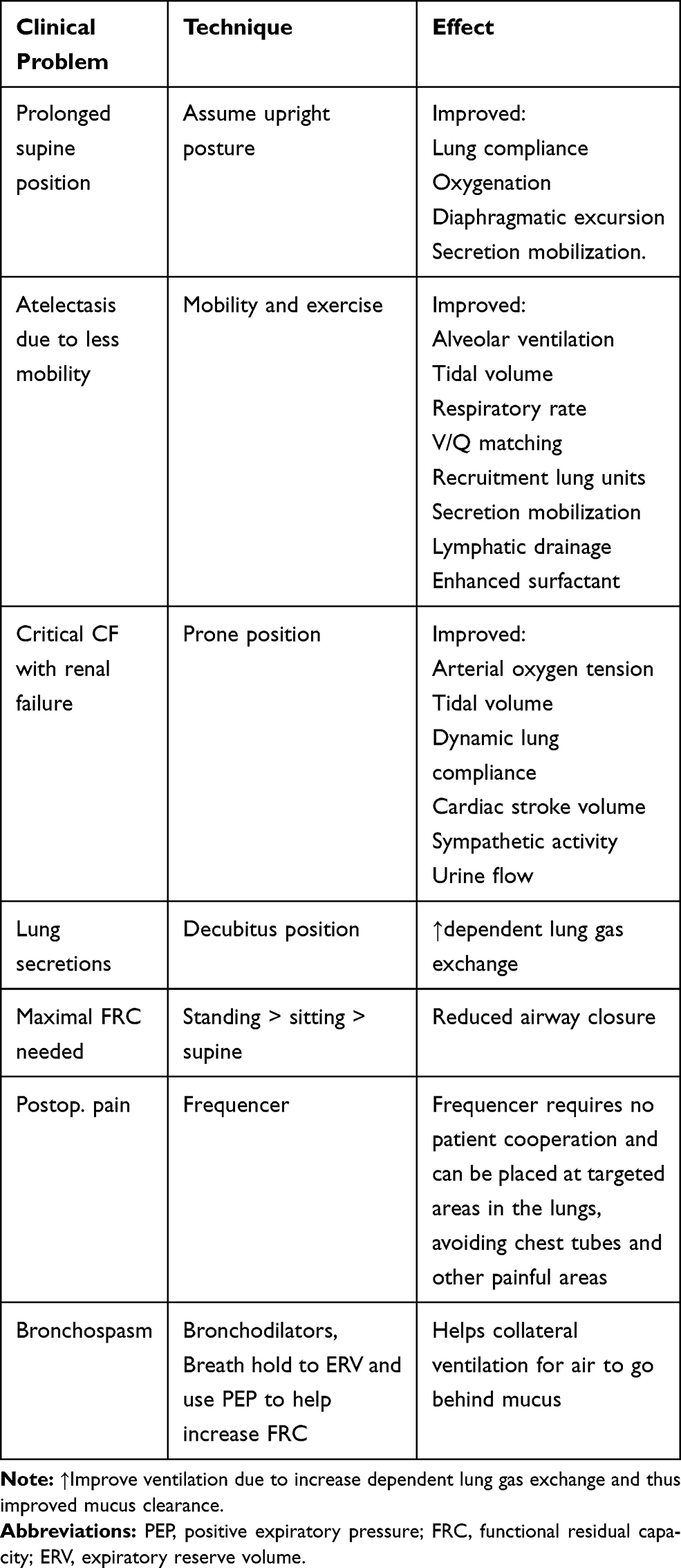 |
Table 3 Role of Optimal Position and Ventilation in CF ACT |
Clinical trials for ACT techniques without devices (eg, vibratory vests) are difficult due to significant variability of primary outcomes due often to patients employing more than one technique for airway clearance.3 Use of “breathing techniques” with associated devices is extremely important for airway secretion clearance in treatment of CF. Use of active breathing exercises to enhance airway mucus clearance strengthens lung capacity lung over time.4 Breathing techniques, mentioned above, are often underutilized by CF patients and frequently not recommended by physicians and respiratory therapists engaged in CF care. Patient education involving breathing technique demonstrations associated with the use of devices to further enhance mucus clearance are essential for establishing daily airway clearance regimens that the educated CF patient must use. Further, use of paper handouts in clinics with repetitive reinforcement of proper technique is crucial for establishing adherence to a daily regimen.
Autogenic Drainage
This was developed over six decades ago and helps move tenacious mucus in patients with defective mucus clearance. Multiple airway clearance techniques that utilize only the breath are teachable to CF patients. A highly effective form entitled autogenic drainage involves controlled breathing to transport mucus from smaller to larger airways for improved expectoration. It incorporates three breathing exercises: The first phase is designed to “unstick” small airway mucus predominately by respiratory movements targeted to lung bases. The next phase termed the “collecting” phase involves movement from mid-airways through breathing at low to mid-lung levels. The third or the “evacuating” phase raises mucus to central airways by breathing at mid to high lung ventilatory levels. This is accomplished by first taking an extremely large breath followed by a breath hold for several seconds. Following the breath hold, virtually all air is exhaled to a very low lung volume. From that point the patient takes small breaths followed by exhalation to force air out to maintain a low lung volume. This maneuver is repeated until patients begin to audibly perceive chest rattling on exhalation. At this point a larger breath is taken and moderate exhalation maneuver is performed. This is repeated several times. The patient then takes deep inhalations followed by small exhalations targeting maintenance of larger lung volumes. In the final step, patients take very deep inhalations followed by large forced expiratory “huffs” to expel mucus. In this final phase patients should avoid straining of cervical musculature which may cause premature airway closure which will retard clearance.
As guidance for all airway techniques, avoiding strain on the airways and throat muscles is important to avoid airway collapse which can cause wheezing and temporary narrowing of the airways. This will prevent the mucus from moving from the airway.
Active Cycle Breathing (ACBT)
This technique involves chest expansion followed by forced expiratory breaths cycled several times. This maneuver achieves adequate sputum clearance. Specifically, patients hold shoulders as motionless as possible while employing chest wall musculature to inflate the lungs. Patient then breath holds for several seconds. This maneuver is repeated several times until secretions are audible in upper airways. Then using the same technique as the final step in autogenic drainage, a large forced expiratory huff is used to expel mucus from the lungs. In a Cochrane review, Warnock and Gates examined the effectiveness and acceptability of chest physiotherapy (CPT) compared to no treatment or simply to spontaneous cough alone for improvement in sputum clearance in patients with CF.5 One hundred and fifty-seven studies were identified. This review showed that patients employing ACT experienced short‐term effects for increased mucus transport. The authors found no evidence that patients who employed these techniques experienced long‐term effects in chest clearance, quality of life, or survival with CPT.5 Main et al compared CPT with other ACTs in terms of their impact on respiratory function, individual preference, adherence, and quality of life and were unable to demonstrate any meaningful advantage of CPT over other methods. They suggested that the lack of meaningful evidence may have resulted in differences in clinical trial design. The authors discovered a trend for participants preferring “self‐administered airway clearance techniques.” Limitations of this review included a paucity of well‐designed, adequately powered, long‐term trials.6
McKoy et al compared the clinical effectiveness of the active cycle breathing technique with other airway clearance techniques in patients with CF. Importantly, the authors found no significant difference in: (1) quality of life, (2) sputum weight, (3) exercise tolerance, (4) lung function, or (5) oxygen saturation between the ACBT and AD or between the ACBT and airway oscillating devices. They found no significant difference in lung function or the number of yearly pulmonary exacerbations between the ACBT alone or in conjunction with conventional CPT. In this report, they concluded that there is insufficient evidence for supporting or rejecting the use of the ACBT over any other ACT. The limitations stated again included lack of similar comparisons in groups; also, lack of data and long-term studies.7
ACT independent of a device (eg, high-frequency chest wall oscillator) requires that a caretaker be available to provide patient therapies, a limitation for many patients. In 2005, the Cystic Fibrosis Foundation (CFF) recommended that airway clearance therapy should be performed by all patients with cystic fibrosis. In this communique, they noted no one ACT method to be superior over other forms, implying that one form of airway therapy may prove more useful at different stages of a CF patient’s life. Expert clinician recommendations at VCU are that CF patients should have the option to choose the ACT based on the trajectory of their CF disease. Further, the CFF recommended aerobic exercise to be beneficial in CF patient care.8
Nixon et al reported that CF patients who habitually pursue frequent exercise exhibit enhanced physical fitness and were three times more likely to survive than patients with poor exercise regimens. They concluded that higher level of fitness reduces risk of dying, but that it remains unknown whether joining an exercise program will improve prognosis in patients with CF.9
Mortensen et al examined the effects of postural drainage (PD) or positive expiratory pressure (PEP) regimens on whole lung and regional tracheobronchial clearance (TBC) in 10 patients with CF. They concluded that PD or PEP, when combined with forced exhalation techniques (FET), exert similar effects on short-term whole lung and regional TBC in patients with CF.10 In other important work, Button examined the effects of body positions on ventilation, mucus distribution, lung volume changes, huff and cough strength, expiratory flow and gastroesophageal function in CF across the lifespan. They concluded that clinicians should consider the effects of body position on regional ventilation in clinical reasoning and decision making in patients with CF in the application of optimal ACT.11 Manual applied techniques such as external chest percussion and postural drainage are effective but are dependent on the presence of a caretaker for assistance, and are frequently inconvenient for the patient.
Mucociliary Clearance: mucociliary clearance of the normal human airway is approximately 5 mm/min. From posterior basal segments of lung to trachea is approximately 300 mm. In a head down posture 60–100 min are required for mucus to travel from lung bases to the trachea. Studies of gravitational effects on mucus clearance in CF supports postural drainage as effective means of airway clearance.12 (Table 4).
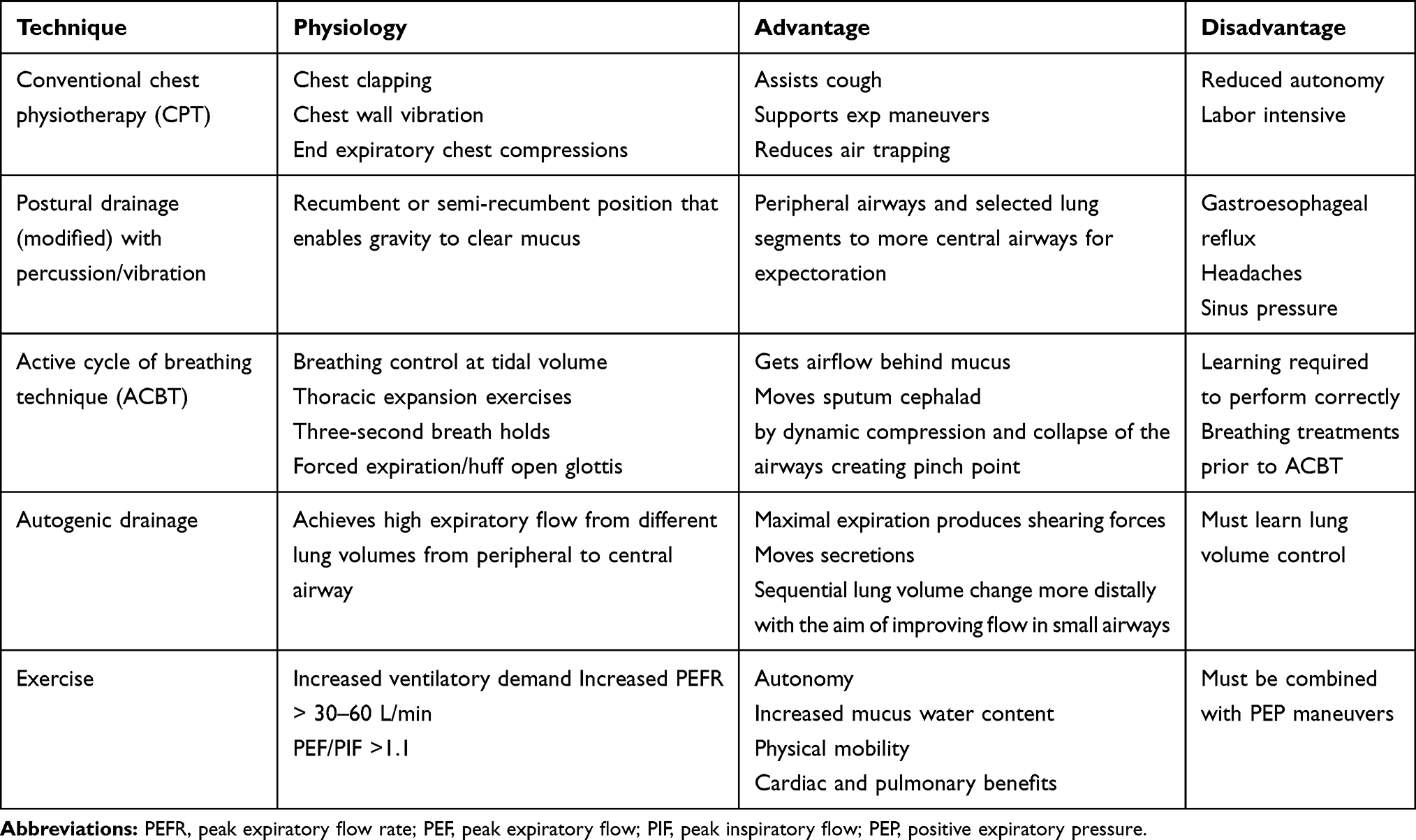 |
Table 4 Various ACT Without Devices |
For manual techniques to be effective, air must be located “behind the mucus.” Clinicians may instruct patients to try a three second breath hold as well to permit deep inspiration to allow use of collateral ventilation to inflate the lungs behind the mucus before forceful exhalation. See Figure 1 for recommended ventilation strategies.
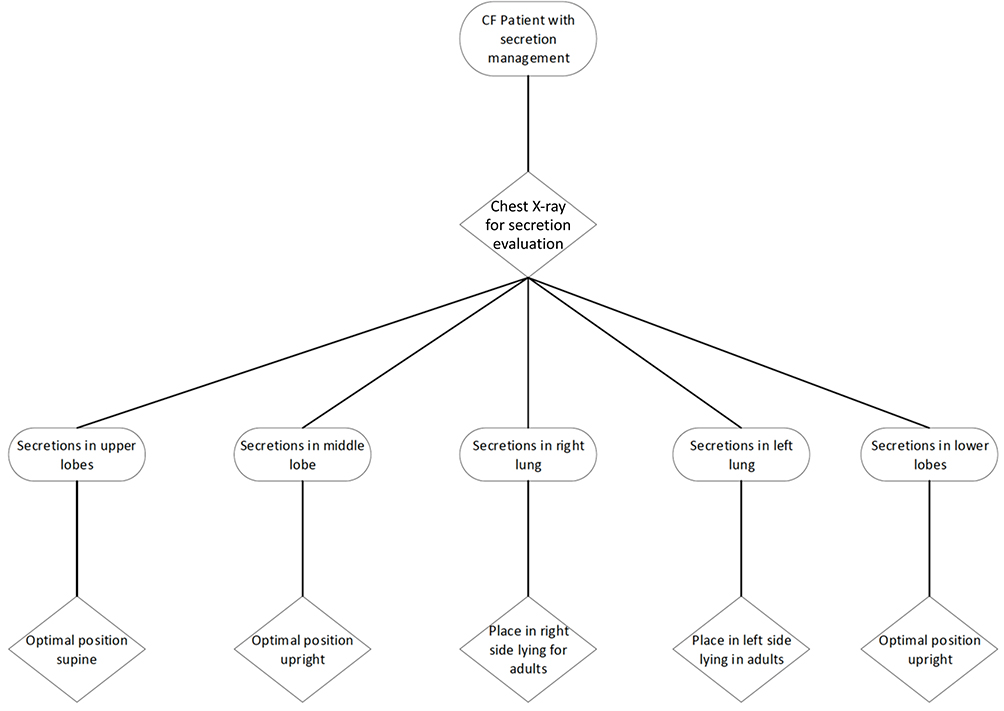 |
Figure 1 ACT positioning recommended in clinical scenarios. |
Dwyer et al compared treadmill and cycle exercise and its effect on sputum production and ventilation for airway clearance. They found that expectoration improved following exercise and ventilation and respiratory flow were significantly higher during treadmill and cycle exercise when compared to controls. Sputum mechanical impedance following treadmill exercise decreased where as it did not have the same effect with cycle exercise. The authors concluded that the reductions in sputum mechanical impedance with treadmill exercise may have been due to thoracic oscillations associated with walking.13
Airway Clearance Device and Techniques
In addition to these techniques, devices can and should be used between breathing technique sets and incorporated into a daily regimen. See Table 5. A common type of device is called a positive expiratory pressure (PEP) therapy device. These devices work by active exhalation against a vibrating expiratory resistance. This resistance can be a flap as with the vibraPEP,™ Acapella,™ or Aerobika™ or by an object pushing against gravity such as the flutter device. This device employs a ball that is pushed up and down by the exhalation of breath. Another less commonly used device is the PEP mask that has different nozzle sizes on the end which restricts the exhalation. Back pressure created by restriction to airflow strengthens the lung capacity and moves mucus. These PEP devices are frequently used in combination with breathing techniques to enhance sputum clearance.
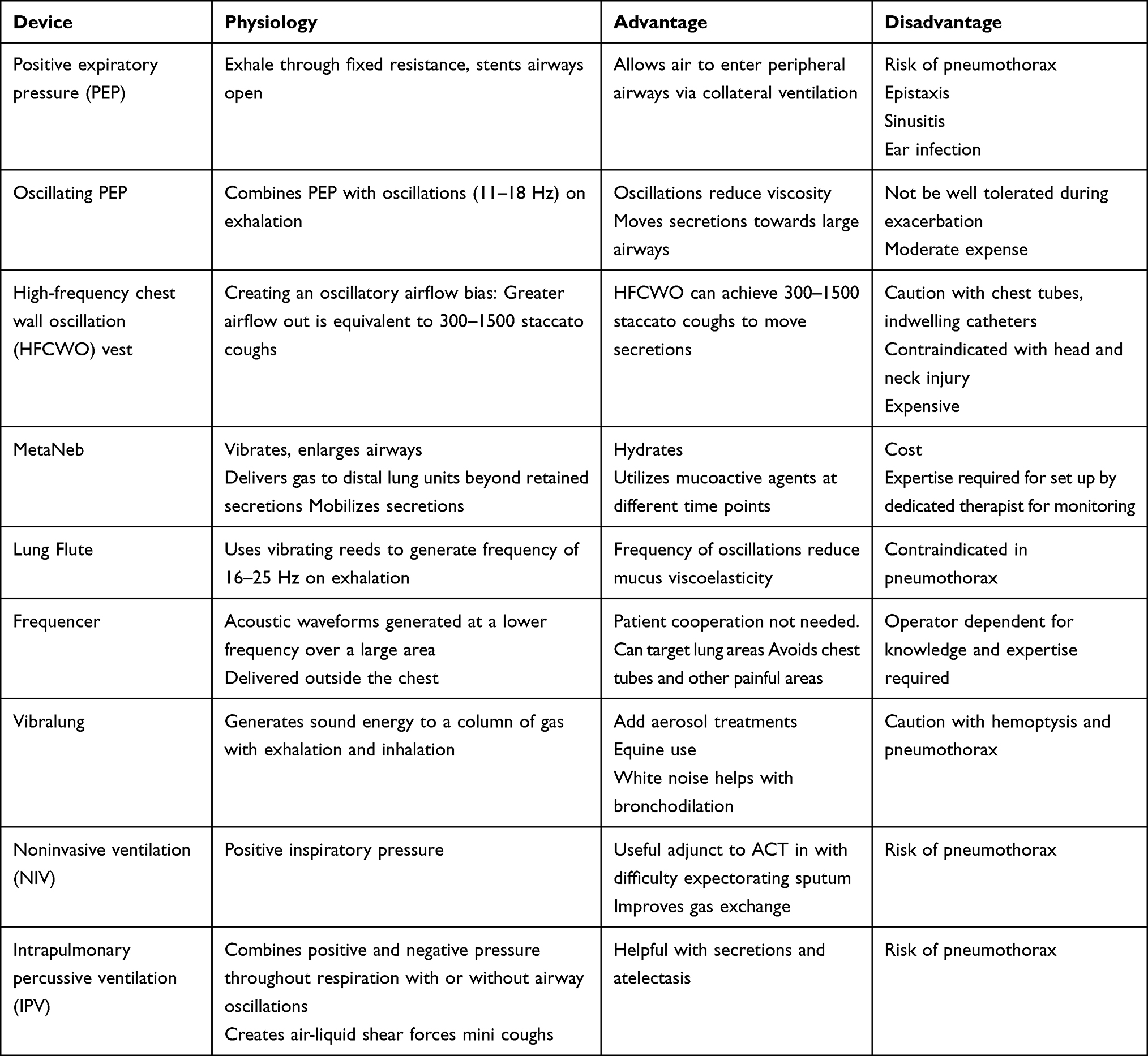 |
Table 5 Airway Clearance Therapy with Devices |
The Hillrom™ Monarch™ vest and respironics vests are more passive forms of airway clearance. These devices are high frequency chest wall oscillating devices (HFCWO) which vibrate the chest enabling the loosening and movement of mucus from airway walls. The device is worn around the chest with holes for the arms. Percussion pods move at different frequencies and pressure settings adjusted to the user’s preferences. A similar more localized hand-held device, called a percussor, vibrates at different frequencies to help mobilize mucus.
Hristara-Papadopoulou et al studied literature supporting various airway clearance devices and concluded that current devices facilitate mucus removal while also improving pulmonary function. They also concluded that evidence is limited to support a specific device. These authors recommended that more studies are required in order to enable specific recommendations for each device.14
App et al compared AD and flutter. Results showed sputum viscoelasticity was significantly lower with the flutter in comparison with AD, predicting improvements in mucociliary and cough of the secretions.15
HFCWO unlike oscillations from PEP therapy, creates oscillations outside of the chest, creating airflow that helps move secretions with greater airflow out than one attains with normal breathing. HFCWO achieves 300–1500 staccato coughs to move secretions with enhanced central and peripheral airway clearance. There is evidence that the oscillations produced by HFCWO break down and thin mucus viscosity acting as a “physical mucolytic” shearing mucus from bronchial walls. Mucus is moved to the central airways to be removed by cough or swallowed. Tracheal mucus clearance is most pronounced in the range of 11–15 Hz vibratory reaching 340% at 13 Hz. For HFCWO to be effective, inflation pressures and frequency are crucial for patient comfort, effectiveness, and adherence. Both the Afflo™ and Monarch™ HFCWO vests are portable systems utilizing discs or pods that vibrate/percuss the lungs, thinning mucus and creating cough-like airflow.16,17
Oral high frequency percussive/vibratory/oscillatory devices create directional “stroking” and percussion which helps move secretions stimulating a cough. These combinations hydrate and utilize mucus regulators at different time points. Devices like MetaNeb™, Clearway™, and ultrasonic nebulizers are examples. Intrapulmonary percussive ventilation (IPV) can be administered via mouthpiece, mask, tracheostomy, or in line with ventilator. IPV, MetaNeb, PercussiveNEB, CoughAssist T70 lung expansion, vibrate and enlarge airways and deliver gas into distal lung units beyond retained secretions which helps to mobilize secretions cephalad. The oral high frequency percussive/vibratory/oscillatory devices provide internal percussion of the lungs to loosen mucus in contra-distinction to the vest, which provides percussion from outside. With the exception of cough assist devices, the vest and others can deliver high density aerosol to hydrate mucus with positive expiratory pressure. Cough assist devices provide insufflation exsufflation that creates airflow which triggers cough aiding airway clearance. With new software, cough assist provides internal oscillation of 5–20 Hz and an amplitude. Oscillations, controlled by the patient, are created both on inhalation or exhalation or both based on comfort.18–20
Acoustic percussors include the Lung Flute,™ Vibralung®, and Frequencer®. The lung flute uses vibrating reeds to generate frequency of 16–25 Hz on exhalation. The frequencer delivers acoustic waveforms generated at a lower frequency but over a large area outside the chest. The frequencer must be moved over the chest to provide the energy to a focused location. This device requires no significant patient cooperation and can be placed to specific target lung areas (eg, right middle lobe, right lower lobe) avoiding lines and chest tubes and painful areas. Vibralung generates sound energy sending in the airways on both exhalation and inhalation with frequencies ranging from 5 to 1200 Hz. Energy is transferred to airways through resonance and can be added to aerosol treatments. The Vibralung was approved for equine use prior to human use approval. According to frequency employed (ie, low to high) vibralung impact different airway calibers. The white noise it creates promotes bronchodilation.4,14
Noninvasive ventilation (NIV) with or without oxygen has been used specifically in advanced CF lung disease. Multiple studies now show that NIV is a useful adjunct to other airway clearance techniques, in CF patients who have difficulty expectorating sputum. NIV improves gas exchange during sleep to a greater extent than oxygen therapy. The impact of NIV on CF pulmonary exacerbations and disease progression remain unclear.21–23
Clinical Applications of Devices
The Frequencer™ requires no patient cooperation and can be placed to targeted areas in the lungs avoiding chest tubes and other painful areas. For mucus plugging of blocked airways and air trapped behind secretions mobilization is assisted by augmentation of collateral ventilation, breath hold and appropriate positioning for ventilation and drainage. Optimization of inspiration to optimize expiratory efforts facilitate clearance. Mobilization of impacted, thick secretions is achieved with the use of mucoactive agents such as HTS/Dornase or by using oscillatory devices or even manual techniques. Techniques that can be helpful include: ACBT, positive pressure NIV, OPEP/HFCWO, and correct body positioning.
With bronchospasm, inspiratory time is reduced, resulting in nonhomogenous filling and emptying lung units. Breath hold during periods of bronchospasm is difficult due to dyspnea. Furthermore, expiratory airflow is limited. Thus, secretion mobilization is limited. However, secretion mobilization will occur in expiratory reserve volume (ERV) of during periods of bronchospasm. An efficient strategy in patients with bronchospasm utilizes bronchodilators followed by breath hold if possible enabling patients to “breathe into ERV.” Importantly, PEP increases functional residual capacity during tidal breathing thus promoting collateral ventilation. Thus, PEP may enhance lung emptying which improves dyspnea. Gentle acceleration of expiratory airflow with autogenic drainage while utilizing control of breathing aids in airway recovery between each cough. Exhaling into ERV in autogenic drainage helps mobilize secretions.
MetaNeb at home device, Volara™ is a fully electronic, intuitive, smart single patient use circuit and has automatic programs so that patients are able to realize the same great clinical outcomes as seen in the hospital in the home setting with a simple start button. It benefits CF, neuromuscular and bronchiectasis patients with the unique triple therapy in one: secretion clearance, lung expansion, and nebulizer treatment. The main benefit of OLE (oscillations and lung expansion) therapy by the Volara is that it is an efficient 10 min therapy that delivers lung expansion (CPEP), secretion clearance (CHFO/oscillations) and aerosol delivery indicated for the treatment and prevention of pulmonary atelectasis and mobilization of airway secretions.24
A variety of techniques can be utilized to improve mucus clearance in CF. Guidelines from the American College of Chest Physicians (ACCP) state, devices allow patients to achieve the same benefits derived from CPT without the assistance of a caregiver appear to be as effective as CPT in increasing sputum production.25
Future Directions
Existing data and routine for ACT for patients with CF is limited and often conflicting for various findings of ACT structure in CF. Paucity of data also exists for treatment approaches for ACT in CF. Medications and devices have been used for ACT in CF but there remains a desperate need to have future studies that can address this deficiency.
Better guidelines for ACT devices as well as treatment protocols for CF are urgently needed.
We report a study in which a routine of structured airway clearance is compared to a nonstructured airway clearance routine. Lung function between the two groups will then be reported. In this study, the goal is to show that structured airway clearance therapy routines improve lung function, reduce exacerbations and improve quality of life.26 The results will be reported some time in 2021.
Conclusion
Airway clearance is a necessity for maintenance of lung health by reducing mucus volume in the lungs. Long-term airway clearance is vital for reduction of bacterial infection-induced exacerbation frequency in CF patients. From a patient perspective, the most effective methods of airway clearance are the active forms of breathing techniques with incorporation of a PEP device into the routine. Many patients however, use only passive forms of airway clearance, primarily the HFCWO vest, because of its ease of use and not requiring undivided attention during its use. Proper breathing techniques should be encouraged and reinforced by intermittent refamiliarization and education of airway clearance techniques with patients. A prescription for ACT must be personalized and must include precision physiotherapy. Currently, no one form is superior to another, but must be acceptable to the patient taking into account an individual patient’s clinical, functional, environmental, and social factors. Together with a sound understanding of airway clearance physiology, key issues to consider for airway clearance prescriptions are a patient’s need to achieve minimum expiratory airflow of 30–60 liters per minute to enable mobilization of secretions. In addition, patients will need methods such as oscillatory PEP, HFCWO to mobilize secretions. Clinicians must be able to assess how technically correct a patient’s current clearance technique actually is. Both a practice and knowledge gap exist in airway clearance by many clinicians due to large variations in training programs in the teaching of various airway clearance techniques. Cystic Fibrosis Foundation guidelines indicate that no one airway clearance is superior to others. The guidelines are of interest both for what can and what cannot be concluded with confidence.
Clinicians caring for CF patients must regularly review and optimize treatment types and techniques. Further, a patient’s individual choice is important for attaining the best airway clearance outcome. Unfortunately, due to multiple different barriers to treatment, adherence by CF patients to airway clearance therapy is approximately 40–47%. However, armed with the knowledge in this document, clinicians can improve patient outcomes. Patients must have important education to successfully change behavior.
Author Information
Dr Chaudary is a Professor of Medicine and Director of the Adult Cystic Fibrosis Center at Virginia Commonwealth University Medical Center.
Gabriella “Ella” Balasa, Director, United States Adult Cystic Fibrosis Association
Funding
There is no funding to report.
Disclosure
(1) No financial disclosure to report. (2) Dr Chaudary serves on advisory boards for Dymedso and PARI corporations, received personal fees from Abbcom Inc. and grants from CFF. The authors report no other conflicts of interest in this work.
References
1. Hess DR. Airway clearance: physiology, pharmacology, techniques, and practice. Respir Care. 2007;52(10):1392–1396.
2. Poole PJ, Black PN. Mucolytic agents for chronic bronchitis or chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2006;3:CD001287. doi:10.1002/14651858.CD001287.pub2
3. Main E, Grillo L, Rand S. Airway clearance strategies in cystic fibrosis and non-cystic fibrosis bronchiectasis. Semin Respir Crit Care Med. 2015;36(2):251–266. doi:10.1055/s-0035-1546820
4. Flume PA, Robinson KA, O’Sullivan BP, et al. Cystic fibrosis pulmonary guidelines: airway clearance therapies. Respir Care. 2009.
5. Warnock L, Gates A. Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis. Cochrane Database Syst Rev. 2015;12. doi:10.1002/14651858.CD001401.pub3.
6. Main E, Prasad A, van der Schans C. Conventional chest physiotherapy compared to other airway clearance techniques for cystic fibrosis. Cochrane Database Syst Rev. 2005;1. doi:10.1002/14651858.CD002011.pub2.
7. Mckoy N, Wilson L, Saldanha I, Odelola O, Robinson K. Active cycle of breathing technique for cystic fibrosis. Cochrane Database Syst Rev. 2016;7. doi:10.1002/14651858.CD007862.pub4.
8. Lester MK, Flume PA. Airway-clearance therapy guidelines and implementation. Respir Care. 2009;54(6):733–753. doi:10.4187/002013209790983205
9. Nixon PA, Orenstein DM, Kelsey SF, Doershuk CF. The prognostic value of exercise testing in patients with cystic fibrosis. N Engl J Med. 1992;327(25):1785–1788. doi:10.1056/NEJM199212173272504
10. Mortensen J, Falk M, Groth S, Jensen C. The effects of postural drainage and positive expiratory pressure physiotherapy on tracheobronchial clearance in cystic fibrosis. Chest. 1991;100(5):1350–1357. doi:10.1378/chest.100.5.1350
11. Button BM. The effects of body positioning on ventilation: implications for airway clearance therapy. Pediatr Pulmonol. 2010.
12. Wong JW, Keens TG, Wannamaker EM, Crozier DN, Levison H, Aspin N. Effects of gravity on tracheal mucus transport rates in normal subjects and in patients with cystic fibrosis. Pediatrics. 1977;60(2):146–152.
13. Dwyer TJ, Alison JA, McKeough ZJ, Daviskas E, Bye PTP. Effects of exercise on respiratory flow and sputum properties in patients with cystic fibrosis. Chest. 2011;139(4):870–877. doi:10.1378/chest.10-1158
14. Hristara-Papadopoulou A, Tsanakas J, Diomou G, Papadopoulou O. Current devices of respiratory physiotherapy. Hippokratia. 2008;12(4):211–220.
15. App EM, Kieselmann R, Reinhardt D, et al. Sputum rheology changes in cystic fibrosis lung disease following two different types of physiotherapy: flutter vs autogenic drainage. Chest. 1998;114(1):171–177. doi:10.1378/chest.114.1.171
16. Warwick WJ, Hansen LG. The long-term effect of high-frequency chest compression therapy on pulmonary complications of cystic fibrosis. Pediatr Pulmonol. 1991;11(3):265–271. doi:10.1002/ppul.1950110314
17. Osman LP, Roughton M, Hodson ME, Pryor JA. Short-term comparative study of high frequency chest wall oscillation and European airway clearance techniques in patients with cystic fibrosis. Thorax. 2010;65(3):196–200. doi:10.1136/thx.2008.111492
18. McIlwaine M, Button B, Nevitt SJ. Positive expiratory pressure physiotherapy for airway clearance in people with cystic fibrosis. Cochrane Database Syst Rev. 2019;2019(11). doi:10.1002/14651858.CD003147.pub5
19. McIlwaine PM, Wong LT, Peacock D, Davidson AG. Long-term comparative trial of conventional postural drainage and percussion versus positive expiratory pressure physiotherapy in the treatment of cystic fibrosis. J Pediatr. 1997;131(4):570–574. doi:10.1016/s0022-3476(97)70064-7
20. McIlwaine PM, Wong LT, Peacock D, Davidson AG. Long-term comparative trial of positive expiratory pressure versus oscillating positive expiratory pressure (flutter) physiotherapy in the treatment of cystic fibrosis. J Pediatr. 2001;138(6):845–850. doi:10.1067/mpd.2001.114017
21. Moran F, Bradley JM, Piper AJ. Non-invasive ventilation for cystic fibrosis. Cochrane Database Syst Rev. 2009;1:CD002769. doi:10.1002/14651858.CD002769.pub3
22. Young AC, Wilson JW, Kotsimbos TC, Naughton MT. Randomised placebo controlled trial of non-invasive ventilation for hypercapnia in cystic fibrosis. Thorax. 2008;63(1):72–77. doi:10.1136/thx.2007.082602
23. Flight WG, Shaw J, Johnson S, et al. Long-term non-invasive ventilation in cystic fibrosis – experience over two decades. J Cyst Fibros off J Eur Cyst Fibros Soc. 2012;11(3):187–192. doi:10.1016/j.jcf.2011.11.006
24. Huynh TT, Liesching TN, Cereda M, et al. Efficacy of oscillation and lung expansion in reducing postoperative pulmonary complication. J Am Coll Surg. 2019;229(5):458–466.e1. doi:10.1016/j.jamcollsurg.2019.06.004
25. McCool FD, Rosen MJ. Nonpharmacologic airway clearance therapies: ACCP evidence-based clinical practice guidelines. Chest. 2006;129(1Suppl):250S–259S. doi:10.1378/chest.129.1_suppl.250S
26. Rose, Rachel, ”A Structured Airway Clearance and Exercise Program to Improve Clinical Outcomes in Cystic Fibrosis” (2020). Yale School of Medicine Physician Associate Program Theses. 29. Available from: https://elischolar.library.yale.edu/ysmpa_theses/29.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.