")
Back to Journals » Clinical Ophthalmology » Volume 12
Age, sex, and type of medication predict the effect of anti-VEGF treatment on central retinal thickness in wet age-related macular degeneration
Received 3 December 2017
Accepted for publication 18 January 2018
Published 8 March 2018 Volume 2018:12 Pages 473—479
DOI https://doi.org/10.2147/OPTH.S158760
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Toke Bek, Sidsel Ehlers Klug
Department of Ophthalmology, Aarhus University Hospital, Aarhus, Denmark
Purpose: Randomized clinical trials studying the effects of VEGF inhibition on wet age-related macular degeneration (wAMD) are designed so that the effects of individually varying risk factors on the treatment response are eliminated. The influence of these risk factors can be studied in large data sets from real-life experience.
Patients and methods: All 2,255 patients diagnosed with wAMD requiring anti-VEGF treatment in at least one eye over more than 9 years in a defined Danish population with 0.9 million inhabitants were studied. The predictive value of eye laterality, sex, current smoking status, type of anti-VEGF compound, membrane position, membrane type, leakage area, number of injections, number of visits, age, time to follow-up, visual acuity, and central retinal thickness (CRT) at baseline on change in CRT after three monthly injections with anti-VEGF compound followed by treatment pro re nata for up to 12 months was assessed.
Results: After 12 months, 67 patients had died, 903 had had stable CRT for at least 6 months, and 1,285 patients had not achieved stable CRT. The reduction in CRT was -84.8±118.3 µm, whereas the increase in visual acuity was 2.2±14.7 Early Treatment Diabetic Retinopathy Study letters. The risk factors included contributed to 64% of the variation in CRT reduction. High age and high CRT at baseline predicted high CRT reduction, whereas more injections, treatment with ranibizumab, and male sex predicted a low CRT reduction.
Conclusion: Age, sex, and type of anti-VEGF medication can be used to plan treatment and inform patients about the expected response of anti-VEGF treatment in wAMD.
Keywords: wet AMD, anti-VEGF treatment, risk factors, real-life experience
Plain-language summary
The introduction of intraocular drugs to antagonize the neovascular effects of VEGF has improved the visual prognosis for patients with wet age-related macular degeneration (wAMD) considerably. In real life, results may be influenced by individual factors that can be elucidated in large data sets from daily clinical practice. As such, 2,255 patients diagnosed with wAMD requiring anti-VEGF treatment over more than 9 years in a defined Danish population with 0.9 million inhabitants were studied. The predictive value of eye laterality, sex, current smoking status, type of anti-VEGF compound, anatomical characteristics of the new vessel, number of injections, number of visits, age, time to follow-up, visual acuity, and central retinal thickness (CRT) at baseline on change in CRT after three monthly injections with anti-VEGF compound followed by treatment as needed for up to 12 months was assessed. High age and high CRT at baseline predicted high CRT reduction, whereas more injections, treatment with ranibizumab, and male sex predicted low CRT reduction after 12 months. This implies that age, sex, and type of anti-VEGF medication can be used to plan treatment and inform patients about the expected response of anti-VEGF treatment in wAMD.
Introduction
The introduction of intraocular drugs to antagonize the neovascular effects of VEGF has improved the visual prognosis for patients with wet age-related macular degeneration (wAMD) considerably.1 The effect of the treatment has been documented in randomized clinical trials (RCTs) comparing anti-VEGF treatment with other treatment modalities,2–4 comparing different anti-VEGF compounds with each other,5 and in comparisons of alternative treatment strategies with the same anti-VEGF compound.6 In the translation of this evidence to daily clinical practice, the strict inclusion criteria of RCTs are not followed. Therefore, results may be influenced by individual factors, such as comorbidity, treatment preferences, loss of follow-up due to death or migration, and lack of standardization of follow-up intervals due to organizational challenges. However, with access to large data sets, this lack of homogeneity gives the opportunity to study the contribution of individual risk factors to the outcome of the treatment. A recent study of real-life experience with anti-VEGF treatment in wAMD had a long follow-up,7 but the study was retrospective, patient selection due to death or discontinuation of follow-up was not accounted for, and the study was powered only for the study of a few variables.
At the Department of Ophthalmology, Aarhus University Hospital, all patient records from patients receiving anti-VEGF treatment for wAMD have been collected prospectively and registered in a database since March 1, 2007. The present study reports the predictive value of baseline age, sex, central retinal thickness (CRT), visual acuity (VA), angiographic appearance, number of visits and injections, and type of anti-VEGF medication to the change in CRT within 12 months in the first or only treated eye of 2,255 patients with wAMD receiving three monthly anti-VEGF injections followed by treatment pro re nata.
Patients and methods
Population
The Department of Ophthalmology, Aarhus University Hospital receives all patients for evaluation and treatment of wAMD from a population of approximately 0.9 million inhabitants in the eastern part of the Central Denmark Region. The patients are referred from practicing ophthalmologists to whom the population has free access within a few days, when visual symptoms occur. When the ophthalmologist suspects treatment is required for wAMD, the patient is referred for further diagnosis and treatment at the eye department. During the period from March 1, 2007 to April 1, 2016 (9 years and 1 month), 5,487 patients had been referred for evaluation of suspected wAMD.
Eye examination
At the primary examination, patients were interviewed about the duration and nature of visual symptoms, previous history of systemic and ocular disease, medication, and smoking habits. Subsequently, VA was measured on each eye using ETDRS (Early Treatment Diabetic Retinopathy Study) VA charts (Polaphor; Block Optic, Dortmund, Germany), followed by instillation of tropicamide 1% (Alcon, Copenhagen, Denmark) and phenylephrine 10% (Region Midtjylland Hospital Pharmacy, Aarhus, Denmark) eyedrops.
Optical coherence tomography (OCT) was performed using Topcon equipment (DRI OCT or 3-D OCT 2000 Triton; Topcon, Tokyo, Japan) to detect retinal thickening that might suggest the presence of a subretinal neovascularization. The average retinal thickness of the central circular area with a diameter of approximately 1 mm around the point of fixation8 was noted as CRT.
When a choroidal neovascularization was suspected, fluorescein angiography (FA) was performed with the filling phase on the most affected eye using a CF-1 angiography system (Canon, Amstelveen, Netherlands) until August 31, 2016, after which the DRI OCT Triton was used. In cases with overt or suspected subretinal neovascularization, the location of the lesion was assessed as being subfoveal, parafoveal, peripapillary, or extrafoveal, the type of lesion defined to be either classic, predominantly classic, minimally classic, or occult, and the largest diameter of the area showing hyperfluorescence that increased through the angiographic phases was assessed in micrometers, with the horizontal diameter of the optic disk set to a reference of 1,000 μm.
Exclusion
Patients with the following characteristics were excluded from the analysis: residence outside the defined geographical area of the region, age below 50 years, previous or later treatment in other regions, migration during the treatment period, other diseases that might cause subretinal neovascularization, such as pathological myopia, pseudoxanthoma elasticum, choroiditis or known chorioretinal scarring, and previous treatment of AMD with retinal photocoagulation or photodynamic therapy. This resulted in the inclusion of 2,740 eyes from 2,269 patients (41.3% of the referred patients) to receive anti-VEGF treatment for wAMD in the department during the period.
Inclusion for treatment followed Danish national guidelines that implied the presence of: choroidal neovascularization documented by FA, retina edema, a history of visual impairment during the preceding 6 months, and VA of more than 20 ETDRS letters. Treatment was planned as three monthly injections with anti-VEGF compound followed by monthly controls with measurement of VA and OCT scanning, with treatment pro re nata until central retinal edema had disappeared or remained stable for 6 months. Due to individual preferences or other intercurrent disease, the first three injections were not completed within the first year in 22 eyes from 14 patients, leaving 2,718 eyes from 2,255 patients to follow the recommended treatment plan. For the following analyses, the first treated eye was chosen to represent the patient, and patient selection is shown in Table 1.
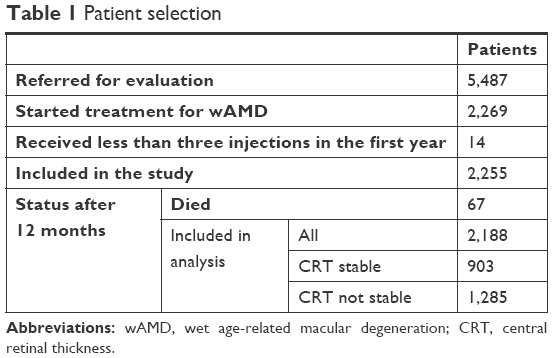 | Table 1 Patient selection |
In practice, the control period was shorter when treatment was performed on the two eyes on different days and VA and CRT measured on both eyes at each visit, and longer during holiday seasons and periods when staffing levels had not been adjusted to accommodate increasing activity. When retinal thickness had become stable, the patient was transferred to the practicing ophthalmologist for regular follow-up with measurement of VA and OCT, on the basis of which the patient was referred for retreatment if CRT had increased. The electronic patient record automatically received information from the national death register about deceased persons. Among the 2,255 patients entering treatment, 67 had died during the first 12 months, leaving the remaining 2,188 patients to be included in the analysis. The background data of the two groups are shown in Table 2. In 903 patients where treatment had stabilized retinal thickness such that injections had not been necessary for at least 6 months, the effect was evaluated from data obtained at the first examination after the last injection, which was 186±88 days after enrollment. In the remaining 1,285 patients who had not achieved stable CRT, the effect was evaluated at the first examination after 12 months, which was 391±17 days after enrollment.
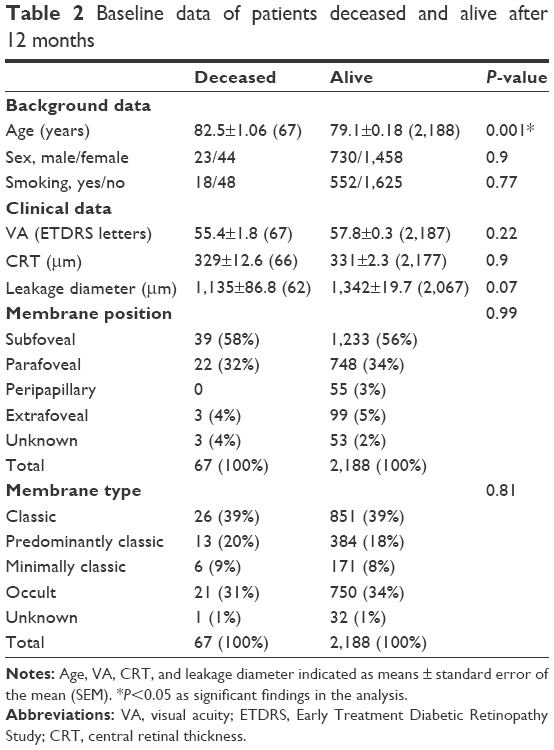 | Table 2 Baseline data of patients deceased and alive after 12 months |
From March 1, 2007, treatment was performed using only ranibizumab 10 mg/mL (Lucentis; Novartis, Basel, Switzerland), with the possibility of changing to aflibercept 4 mg/mL (Eylea; Bayer, Leverkusen, Germany) in nonresponders, from 2013. From 2015, national guidelines changed such that the first-choice treatment was aflibercept in all cases, with the possibility to change to ranibizumab in nonresponders. Therefore, 1 year after commencement of treatment, 1,731 had received only ranibizumab and 372 patients had received only aflibercept. The remaining 85 patients had received both compounds, and were not included with a value for treatment type in the analysis.
All clinical data were entered continuously into a structured patient record, from which the data were transferred to a database for surveillance of activity and quality of treatment. According to Danish rules, the reporting of anonymized data documenting results of routine clinical practice is regarded as quality assessment, and does not require permission from an ethical committee.
Data analysis
The anatomical characteristics observed on FA were converted to semiquantitative scales – membrane position: subfoveal =1, parafoveal =2, peripapillary =3, extrafoveal =4; membrane type, classic =1, predominantly classic =2, minimally classic =3, occult =4.
Statistical analysis
All analyses were performed in Stata version 14.0 (StataCorp, College Station, TX, USA). Unpaired t-tests (continuous variables) or χ2 tests (contingency values) were used to test for differences at baseline between patients who had died and those who were alive after 12 months. Paired t-tests were used to test for changes in CRT and VA from baseline to the last examination during the follow-up period, and for testing differences in the percentage of different membrane types and positions among the two groups.
Multiple linear regression was performed to study the contribution of individual risk factors to the effect of treatment on the change in CRT. Categorical variables were laterality (right = 1, left = 0), sex (male = 1, female = 0), current smoking status (positive = 1, negative = 0), anti-VEGF treatment (ranibizumab = 1, aflibercept = 0), membrane position (1–4), membrane type (1–4), treatment count (three to 12), and number of visits (three to 13). Continuous variables were age (years), time to follow-up (days), VA (ETDRS number), and CRT (μm) at baseline. The distribution of time to follow-up was skewed, due to the truncation of the follow-up period, and was log-transformed, after which this and all other parameters were normally distributed (Q–Q plots).
Results
Table 2 shows that at baseline, patients who had died after 12 months were significantly older than those who were alive at that time, whereas there were no significant differences between the two groups for the other variables studied. Patients who were alive after 12 months had had a mean of 7.8 (range three to 13) visits, during which they had received 5.1 (three to 12) anti-VEGF injections. This resulted in a reduction of −84.8±118.3 (−869 to 731) μm in CRT and an increase of 2.2±14.7 (−81 to 77) in VA ETDRS letters.
Table 3 shows the results of multiple linear regression. Risk factors included contributed to 64% (adjusted R2) of the variation in CRT change. Since the reduction in CRT was registered as a negative value, coefficients with a negative sign were positive risk factors for CRT reduction and vice versa. It appeared that high age and CRT at baseline predicted a significantly higher CRT reduction, whereas an increasing number of injections, treatment with ranibizumab, and male sex predicted a significantly lower CRT reduction. Number of visits, smoking status, eye laterality, follow-up time, and anatomical parameters related to the neovascular membranes observed by FA and VA at baseline showed no predictive value for the change in CRT.
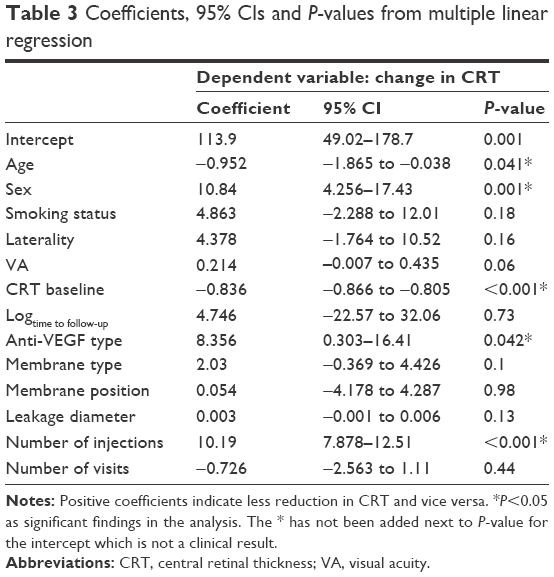 | Table 3 Coefficients, 95% CIs and P-values from multiple linear regression |
Discussion
The present study contributes new evidence on the effect of anti-VEGF treatment on wAMD by documenting a predictive value of age, sex, and type of anti-VEGF compound for the reduction in CRT that can be achieved in 12 months. This adds to a previous study of clinical signs and symptoms that can predict the need for anti-VEGF treatment in newly referred patients with suspected wAMD.9 The study has a number of methodological strengths. It was possible to consider approximately 170 patients per variable studied, which is a strong design for a multiple linear regression analysis.10 Additionally, the data were collected prospectively from a single center that received all patients referred within a defined geographical area. This resulted in the initiation of treatment in approximately 295 new patients per million citizens per year, which corresponds to other real-life data from both the Danish and the British health-care systems.11,12 Furthermore, information from central death registries excluded selection bias from patients who had died during the study period, and mortality during the first 12 months after enrollment was able to be calculated at 3.5%, which corresponds to the mortality in the general population of this age-group.13 Finally, patients in whom treatment had stabilized retinal thickness for at least 6 months were followed in a standardized program with the practicing ophthalmologists, who would refer patients in need of retreatment after initial stabilization. This ensured that the CRT measured after the last injection in patients where CRT had become stable reflected the therapeutic effect of anti-VEGF treatment within 12 months. The truncation of follow-up at this time ensured the inclusion of a sufficient number of patients who had been treated alone with either ranibizumab, which was first-choice treatment during the first few years, or aflibercept, which has been used as first choice for the past few years, but a recalculation of the model with a follow-up of respectively 24 and 60 months showed the same results, except for the difference in the effect of the two anti-VEGF compounds (not shown).
The effect of anti-VEGF treatment for wAMD has been documented in a number of innovative RCTs. These studies were designed to compare the effect of different therapeutic approaches on groups matched so that the influence of other potential risk factors had been eliminated.2–4 Increasing the number of injections in these studies resulted in improved effects on VA and CRT.14 However, in the real-life setting, from which data are reported here, treatment was adjusted to the response, implying that patients with a more modest treatment effect also received more injections.7 In accordance with this, derived variables, such as the follow-up time and the number of visits, and thereby also the control interval, had no separate influence on the treatment response. The real-life setting implied that all patients were treated,15 and thus the average therapeutic response was more moderate than in RCTs performed on selected patient materials.5,6
The change in CRT was used to monitor treatment, and was thus used as the dependent variable in the multiple linear regression analysis. The relevance of this approach was documented by the fact that the parameters included were able to explain approximately 64% of the variation in CRT. A tentative recalculation of the model with VA as the dependent factor showed that the parameters included could only predict 14% of the variation in this factor after 12 months, and supports the view that VA had not been the primary factor used to monitor treatment.16 The variation in CRT might potentially have been predicted further by the inclusion of the morphology of individual retinal layers or genetic factors that have been shown to predict the outcome of treatment.17,18
It has previously been shown that the prevalence of wAMD may be higher in women than in men.19,20 However, the present study showed that sex was the factor contributing most to the effect on CRT, with male sex reducing the effect of the treatment on CRT. This is supported by a study in which male sex was found to be a risk factor that reduced the visual prognosis 60 months after initiation of anti-VEGF treatment for wAMD.6 The background for this finding is unknown, but may be related to hormonal factors and implies that information to the patient about the expected treatment response should be differentiated between men and women.
The study also showed that increasing age predicted increasing reduction in CRT, although the effect was small, amounting to less than 1 μm per year of extra life. This is opposite to findings of increasing risk of recurrence of subretinal neovascularization with age for patients in a pro re nata regime21 and that visual improvement after anti-VEGF treatment in wAMD may decrease with age.6,22 The finding may reflect the general health status of patients with a better response in those who survive longer. Additionally, although a higher CRT at baseline predicted a potential for more CRT reduction, baseline VA was not predictive for CRT reduction. These observations underline the lack of short-term covariance between VA and CRT in macular diseases,23,24 although the choice of CRT to monitor the effect of interventions on macular disease rests on the assumption that retinal thickness influences VA in the longer term.
This study showed that the reduction of CRT induced by aflibercept was significantly higher than the reduction induced by ranibizumab. A recalculation of the multiple regression model with inclusion of the date of first treatment as a variable showed the same result (not shown), which confirms that the use of ranibizumab and aflibercept as first choice during different periods had no influence on the results. The statistical approach also implies that the conclusion of a different effect of the two compounds is independent of the number of treatments and the treatment intervals.25–28 The results confirm previously published evidence that aflibercept is more effective than ranibizumab at reducing macular edema in wAMD,15 and may explain the finding that more injections are needed with ranibizumab than with aflibercept to achieve the same therapeutic response.10
Research on retinal detachment has shown different prevalence of the disease in the two eyes,29 but eye laterality was not found to be a significant factor in the present study. Additionally, although smoking has been shown to be a significant risk factor for the development and progression of wAMD,30 this factor was not found to influence the change in CRT. This finding might be related to the definition of smoking status, but is in accordance with findings that this parameter has no influence on visual prognosis during anti-VEGF treatment.22 Finally, the type and location of neovascular AMD and area of leakage had no predictive value for treatment outcome. The inclusion of peripapillary vessels in the semiquantitative scale in the ranking of the location of subretinal neovascularization may be questionable, but the conclusion was similar in a recalculation of the model where this lesion type had been excluded. Therefore, the collection of clinical data before treatment should not necessarily include smoking habits or type and location of subretinal neovascularization, which underlines the need for improving the classification of retinal lesions in wAMD.31 The finding of a predictive value of age, sex, and type of medication for the therapeutic effect of anti-VEGF treatment in wAMD can be used to plan treatment and inform patients about the expected therapeutic response.
Acknowledgment
The skillful assistance of nurse photographer Helle Hedegaard and IT technician Peter Skaarup is gratefully acknowledged.
Author contributions
TB initiated the writing process, but otherwise the two authors participated equally in all parts of the process, including the conception of the study, acquisition and interpretation of data, drafting of the manuscript, and approval of the result.
Disclosure
The authors report no conflicts of interest in this work.
References
Bloch SB, Larsen M, Munch IC. Incidence of legal blindness from age-related macular degeneration in Denmark: year 2000–2010. Am J Ophthalmol. 2012;153:209–213. | ||
Brown DM, Michels M, Kaiser PK, Heier JS, Sy JP, Ianchulev T. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116:57–65. | ||
Abraham P, Yue H, Wilson L. Randomized, double-masked, sham-controlled trial of ranibizumab for neovascular age-related macular degeneration: PIER study year 2. Am J Ophthalmol. 2010;150:315–324. | ||
Heier JS, Brown DM, Chong V, et al. Intravitral aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119:2537–2548. | ||
Waldstein SM, Simader C, Starurenghi G, et al. Morphology and visual acuity in aflibercept and ranibizumab therapy for neovascular age-related macular degeneration in the VIEW trials. Ophthalmology. 2016;123:1521–1529. | ||
Ho AC, Busbee BG, Regillo CD, et al. Twenty-four month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2014;121:2181–2192. | ||
Pedrosa AC, Sousa T, Pinheiro-Costa J, et al. Treatment of neovascular age-related macular degeneration with anti-VEGF agents: predictive factors of long-term visual outcomes. J Ophthalmol. 2017;2017:4263017. | ||
Ibrahim MA, Sepah YJ, Symons RC, et al. Spectra- and time-domain optical coherence tomography measurements of macular thickness in normal eyes and in eyes with diabetic macular edema. Eye (Lond). 2012;26:454–462. | ||
Hessellund A, Larsen DA, Bek T. The predictive value of subjective symptoms and clinical signs for the presence of treatment-requiring exudative age-related macular degeneration. Acta Ophthalmol. 2012;90:471–475. | ||
Kelley K, Maxwell SE. Sample size for multiple regression: obtaining regression coefficients that are accurate, not simply significant. Psychol Methods. 2003;8:305–321. | ||
Rasmussen A, Sander B, Larsen M, et al. Neovascular age-related macular degeneration treated with ranibizumab or aflibercept in the same large clinical setting: visual outcome and number of injections. Acta Ophthalmol. 2017:95;128–132. | ||
Keenan TD, Wotton CJ, Goldacre MJ. Trends over time and geographical variation in rates of intravitreal injections in England. Br J Ophthalmol. 2012;96:413–418. | ||
Juel K. [Mortality in Denmark during 100 years: Danes live longer, but why 3–4 years shorter than Swedish men and French women?] Copenhagen: National Institute for Public Health; 2004. Danish. | ||
Holz FG, Tadayoni R, Beaty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2015;99:220–226. | ||
Ziemssen F, Feltgen N, Holz FG, et al. Demographics of patients receiving intravitreal anti-VEGF treatment in real-world practice: healthcare research data versus randomized controlled trials. BMC Ophthalmol. 2017;17:7. | ||
Block SB, la Cour M, Sander B, et al. Predictors of 1-year visual outcome in neovascular age-related macular degeneration following intravitreal ranibizumab treatment. Acta Ophthalmol. 2013;91:42–47. | ||
Chhablani J, Kim JS, Freeman WR, Kozak I, Wang HY, Cheng L. Predictors of visual outcome in eyes with choroidal neovascularization secondary to age-related macular degeneration treated with intravitreal bevacizumab monotherapy. Int J Ophthalmol. 2013;6:62–66. | ||
Fauser S, Lambrou GN. Genetic predictive biomarkers of anti-VEGF treatment response in patients with neovascular age-related macular degeneration. Surv Ophthalmol. 2015;60:138–152. | ||
Javitt JC, Zhou Z, Maguire MG, Fine SL, Willke RJ. Incidence of exudative age-related macular degeneration among elderly Americans. Ophthalmology. 2003;110:1534–1539. | ||
Rudnicka AR, Jarrar Z, Wormald R, Cook DG, Fletcher A, Owen CT. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology. 2012;119:571–580. | ||
Kuroda Y, Yamashiro K, Miyake M, et al. Factors associated with recurrence of age-related macular degeneration after anti-vascular endothelial growth factor treatment: a retrospective cohort study. Ophthalmology. 2015;122:2303–2310. | ||
Finger RP, Wickremasinghe SS, Baird PN, Guymer RH. Predictors of anti-VEGF treatment response in neovascular age-related macular degeneration. Surv Ophthalmol. 2014;59:1–18. | ||
Bek T, Jørgensen CM. The systemic blood pressure and oxygen saturation in retinal arterioles predict the effect of intravitreal anti-VEGF treatment on diabetic maculopathy. Invest Ophthalmol Vis Sci. 2016;57:5429–5434. | ||
Bressler SB, Ayala AR, Bressler NM, et al. Persistent macular thickening after ranibizumab treatment for diabetic macular edema with vision impairment. JAMA Ophthalmol. 2016;134:278–285. | ||
Böhni SC, Bittner M, Howell JP, Bachmann LM, Faes L, Schmid MK. Comparison of Eylea with Lucentis as first-line therapy in patients with treatment-naïve neovascular age-related macular degeneration in real-life clinical practice: retrospective case-series analysis. BMC Ophthalmol. 2015;15:109. | ||
Lee AY, Lee CS, Egan CA, et al. UC AMD/DR EMR Report IX: comparative effectiveness of predominantly as needed (PRN) ranibizumab versus continuous aflibercept in UK clinical practice. Br J Ophthalmol. 2017;101:1683–1688. | ||
Garweg JG, Gerhardt C, Kodjikian L, Pfister IB. Real-life experience with aflibercept and ranibizumab in the treatment of newly diagnosed neovascular age-related macular degeneration over 24 months. J Ocul Pharmacol Ther. 2017:33:567–572. | ||
Subhi Y, Sørensen TL. Neovascular age-related macular degeneration in the very old (≥90 years): epidemiology, adherence to treatment, and comparison of efficacy. J Ophthalmol. 2017;2017:7194927. | ||
Hajari JN, Bjerrum SS, Christensen U, Kiilgaard JF, Bek T, la Cour M. A nationwide study on the incidence of rhegmatogenous retinal detachment in Denmark, with emphasis on the risk of the fellow eye. Retina. 2014;34:1658–1665. | ||
Chakravarthy U, Wong TY, Fletcher A, et al. Clinical risk factors for age-related macular degeneration: a systematic review and meta-analysis. BMC Ophthalmol. 2010;10:31. | ||
Spaide R. Improving the age-related macular degeneration construct: a new classification system. Retina. Epub 2017 May 26. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.