")
Back to Journals » Journal of Inflammation Research » Volume 15
Age Related Cognitive Function Was Positively Associated with Diastolic Pressure and Negatively Associated with Antibody Expression in Chinese Oldest-Old and Centenarian Adults
Authors Feng L, Wu D, Ping P, Lin J, Zhao Y, Yao Y , Zhang P , Fu S
Received 20 October 2021
Accepted for publication 16 May 2022
Published 10 December 2022 Volume 2022:15 Pages 6675—6682
DOI https://doi.org/10.2147/JIR.S344105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Monika Sharma
Long Feng,1,* Di Wu,2,* Ping Ping,3,* Jieqiong Lin,4,* Yali Zhao,5 Yao Yao,6,7 Pei Zhang,8 Shihui Fu2,9
1Department of Anesthesiology, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, People’s Republic of China; 2Department of Cardiology, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, People’s Republic of China; 3General Station for Drug and Instrument Supervision and Control, Joint Logistic Support Force of Chinese People’s Liberation Army, Beijing, People’s Republic of China; 4Department of Pathology, Fujian Medical University Cancer Hospital, Fujian Cancer Hospital, Fuzhou, People’s Republic of China; 5Central Laboratory, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, People’s Republic of China; 6Center for the Study of Aging and Human Development and Geriatrics Division, Medical School of Duke University, Durham, NC, USA; 7Center for Healthy Aging and Development Studies, National School of Development, Peking University, Beijing, People’s Republic of China; 8School of Life Science, Beijing Institute of Technology, Beijing, People’s Republic of China; 9Department of Geriatric Cardiology, Chinese People’s Liberation Army General Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shihui Fu, Department of Cardiology, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, People’s Republic of China, Email [email protected] Yali Zhao, Central Laboratory, Hainan Hospital of Chinese People’s Liberation Army General Hospital, Sanya, People’s Republic of China, Email [email protected]
Purpose: Age related cognitive function (ARCF) is of increasing concern in an aging population. Few studies have examined the relationships between ARCF and antibody expression or blood pressure, particularly in older populations. Large sample sizes are needed to elucidate these relationships to inform better strategies for identification and prevention of cognitive decline. The present study was designed to investigate these relationships in Chinese oldest-old and centenarian adults.
Patients and Methods: A household survey was performed that included 436 centenarians and 520 oldest-old adults (80– 99 years) residing in 16 cities and counties of Hainan province, China. ARCF was assessed using the mini-mental state examination.
Results: The median age of participants in this study was 92 years, with a range of 80 to 116 years. Females accounted for 68.5% (655) of the participant pool. Multivariate linear regression analysis showed that age [Exp(B): − 0.220, 95% confidence interval (CI): − 0.270–-0.169], female gender [Exp(B): − 3.459, 95% CI:-4.458–-2.460], Han ethnicity [Exp(B): − 1.732, 95% CI: − 2.693–-0.772], serum creatinine [Exp(B): − 0.019, 95% CI: − 0.037–-0.001], immunoglobulin light chain KAP [Exp(B): − 0.008, 95% CI: − 0.015– 0.000], and anti-ribonucleoprotein antibody [Exp(B): − 6.393, 95% CI: − 10.898–-1.887] were negatively associated with ARCF (P < 0.05). Coronary artery disease [Exp(B): 1.957, 95% CI: 0.170– 3.744] and diastolic pressure [Exp(B): 0.041, 95% CI: 0.002– 0.079] were positively associated with ARCF (P < 0.05).
Conclusion: ARCF was positively associated with diastolic pressure and negatively associated with antibody expression in Chinese oldest-old and centenarian adults.
Keywords: age related cognitive function, antibody expression, centenarian, diastolic pressure, oldest-old
Introduction
Age related cognitive function (ARCF) is of increasing concern in an aging population. The brain is an immune privileged organ, and many immune factors expressed in the brain are essential for removing pathogens, misfolded proteins, and dead cells.1 Recent studies have suggested that immune factors are closely related to neurodegenerative disease, and can be directly activated by fibrillar Aβ and neurofibrillary tangles.2,3 Understanding the role of immune factors such as expressed antibodies in modulation of ARCF in older populations is critical.3,4 Recent studies have shown that abnormal blood pressure may also contribute to ARCF, and patients with abnormal blood pressure were at significantly higher risk of cognitive decline.5,6
Few studies have evaluated the relationships between ARCF and antibody expression or blood pressure, particularly in older populations. Moreover, these studies primarily included adults that would not be considered “oldest-old” or centenarians, or included older adults in Western countries.3–7 Age and region may be associated with ARCF, and the factors that contribute to ARCF remain unclear.8 Therefore, large sample sizes are needed to elucidate these relationships in Chinese oldest-old and centenarian adults to aid in development of strategies to identify and prevent cognitive decline. Hainan has the highest density of oldest-old and centenarian adults in China, and the China Hainan Centenarian Cohort Study (CHCCS) is a data source for a large population-based sample of oldest-old and centenarian adults. The present study was designed to investigate the relationships between ARCF and antibody expression or blood pressure in Chinese oldest-old and centenarian adults. In other words, the hypothesis of the present study was that ARCF may be related to antibody expression and blood pressure in Chinese oldest-old and centenarian adults.
Materials and Methods
Using the list of oldest-old and centenarian adults provided by the Department of Civil Affairs of Hainan Province, China, a household survey was conducted on all centenarians (100 years or older) and oldest-old adults (80–99 years) residing in 16 cities and counties of Hainan province from June 2014 to June 2016 (Figure 1).9,10 The survey sample of 1863 cases included 966 centenarians and 897 oldest-old adults. The inclusion criteria were: 1) aged ≥ 80 years; 2) residing in Hainan province. The exclusion criteria were: 1) missing data; 2) autoimmune diseases. Following application of the inclusion and exclusion criteria, 436 centenarians and 520 oldest-old adults were included in this study. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Chinese People’s Liberation Army General Hospital (301HNLL-2016-01). All participants provided written informed consent before participating in the study.
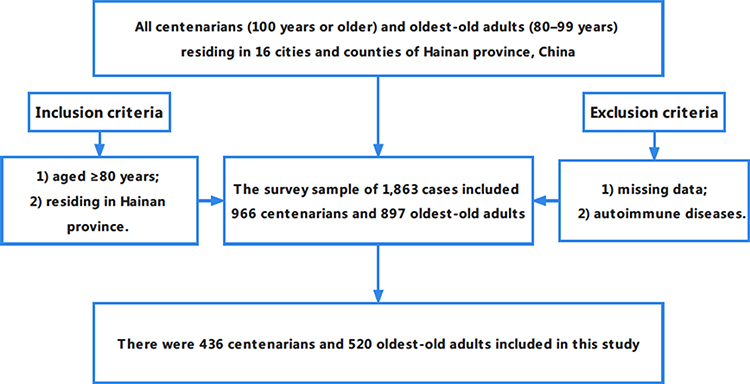 |
Figure 1 Flow chart of the participant selection process. |
A household survey method was used to collect basic information using interview questionnaires, physical examinations, and blood tests conducted by systematically trained local doctors and nurses who could communicate in the local language. Data collected in this study included age, sex, ethnicity, education level (illiteracy, elementary school level, and junior high school level), stroke, diabetes, coronary artery disease (CAD), body mass index (BMI), systolic pressure, diastolic pressure, alanine aminotransferase (ALT), aspartate aminotransferase, serum creatinine (Scr), urea nitrogen, uric acid (UA), triglyceride, high density lipid cholesterol and low density lipid cholesterol, immunoglobulin A, immunoglobulin G, immunoglobulin M, immunoglobulin E, complement C3, complement C4, immunoglobulin light chain KAP, immunoglobulin light chain LAM, anti-cardiolipin antibody, anti-β2 glycoprotein I antibody, anti-ribonucleoprotein antibody, anti-Sm antibody, anti-Sjogren syndrome antigen A antibody, anti-Sjogren syndrome antigen B antibody, anti-scleroderma-70 antibody, anti-mitochondrial antibody, proliferating-cell nuclear antigen antibody, anti-Jo-1 antibody, anti-centromere antibody, anti-double-stranded deoxyribonucleic acid antibody, anti-nucleosome antibody, anti-histone antibody, anti-ribosomal P-protein antibody, and anti-pm-scl antibody.
The mini-mental state examination (MMSE) was administered by specialized neurologists to evaluate ARCF during the same visit in which interview questionnaires were investigated, and physical examinations and blood tests were performed.11 The Georgia Centenarian Study has previously showed that age and education could significantly affect performance of MMSE.12 Identification of age related cognitive decline (ARCD) using the MMSE based on education level were as follows: illiteracy, 17 points; elementary school level, 20 points; and junior high school level, 24 points.13,14
Statistical Analysis
Statistical analysis was performed using Statistic Package for Social Science 19.0 software package (Chicago, IL, USA). Data were presented as means and standard deviations (continuous variables with normal distributions), medians and interquartile ranges (continuous variables with skewed distributions), and numbers and percentages (categorical variables). Comparisons were performed between participants with and without ARCD using Student’s t-tests for continuous variables with normal distributions, Mann–Whitney U-tests for continuous variables with skewed distributions, and Chi-squared tests for categorical variables. All variables evaluated in the study were included in the multivariate linear regression analysis, which was used to analyze the variables associated with ARCF. P < 0.05 (two-sided) was considered statistically significant.
Results
The median age of participants in this study was 92 years, with a range of 80 to 116 years. Females accounted for 68.5% (655) of the participant pool. As shown in Table 1, participants with ARCD were older, more likely to be female and classified as “other ethnicity”, had a lower proportion of CAD, had lower levels of BMI, diastolic pressure, ALT, and UA, and higher levels of immunoglobulin light chain KAP and anti-β2 glycoprotein I antibody. In addition, participants with ARCD had a higher proportion of illiteracy, and had anti-scleroderma-70 antibody than those without ARCD (P < 0.05).
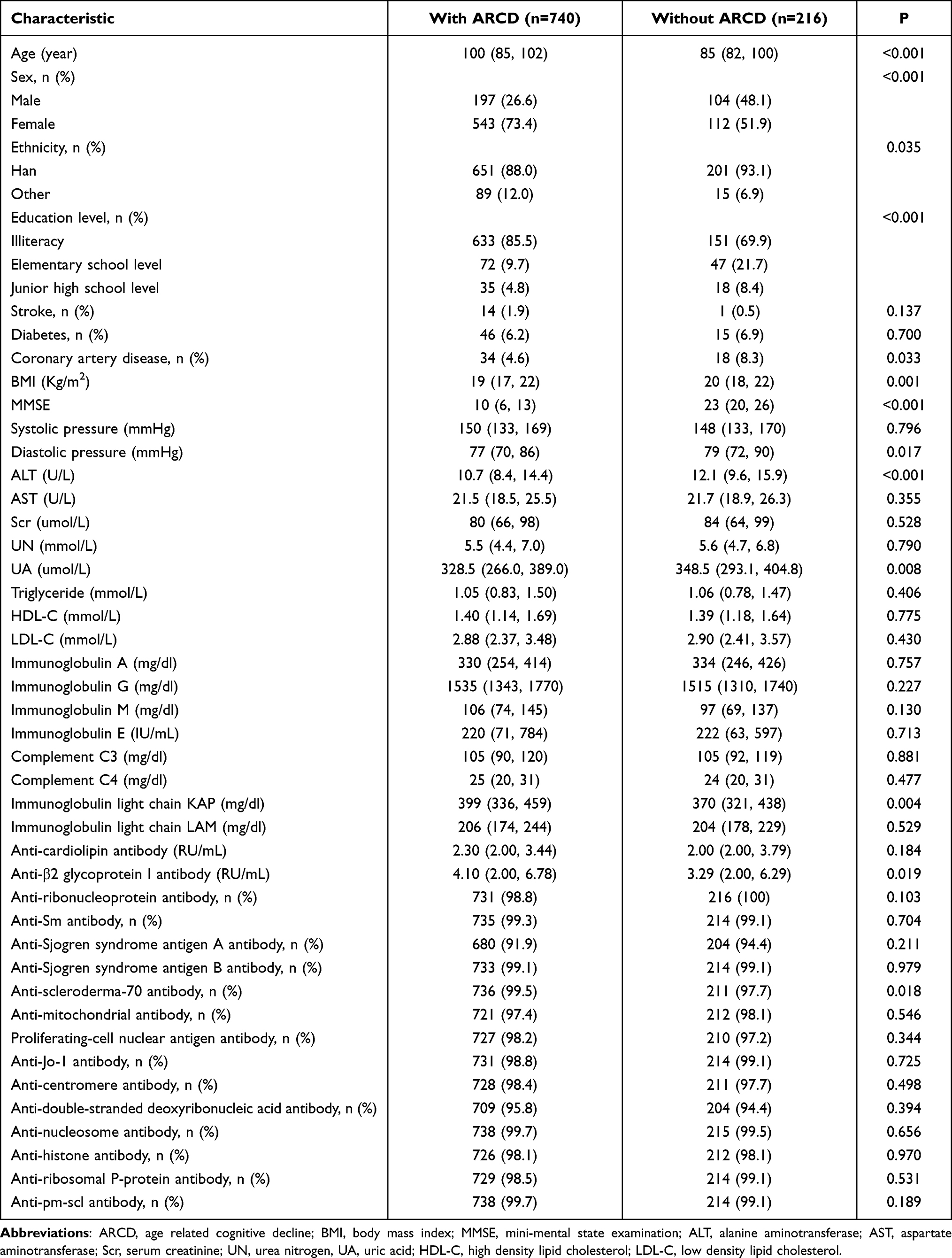 |
Table 1 Demographic and Blood Analysis Data for Individuals with and without ARCD |
Multivariate linear regression analysis showed that age [Exp(B): −0.220, 95% confidence interval (CI): −0.270–-0.169], female gender [Exp(B): −3.459, 95% CI: −4.458–-2.460], other ethnicity [Exp(B): −1.732, 95% CI: −2.693–-0.772], Scr [Exp(B): −0.019, 95% CI: −0.037–-0.001], immunoglobulin light chain KAP [Exp(B): −0.008, 95% CI: −0.015–0.000], and anti-ribonucleoprotein antibody [Exp(B): −6.393, 95% CI: −10.898–-1.887] were negatively associated with ARCF (P < 0.05; Table 2). CAD [Exp(B):1.957, 95% CI: 0.170–3.744] and diastolic pressure [Exp(B): 0.041, 95% CI: 0.002–0.079] were positively associated with ARCF (P < 0.05).
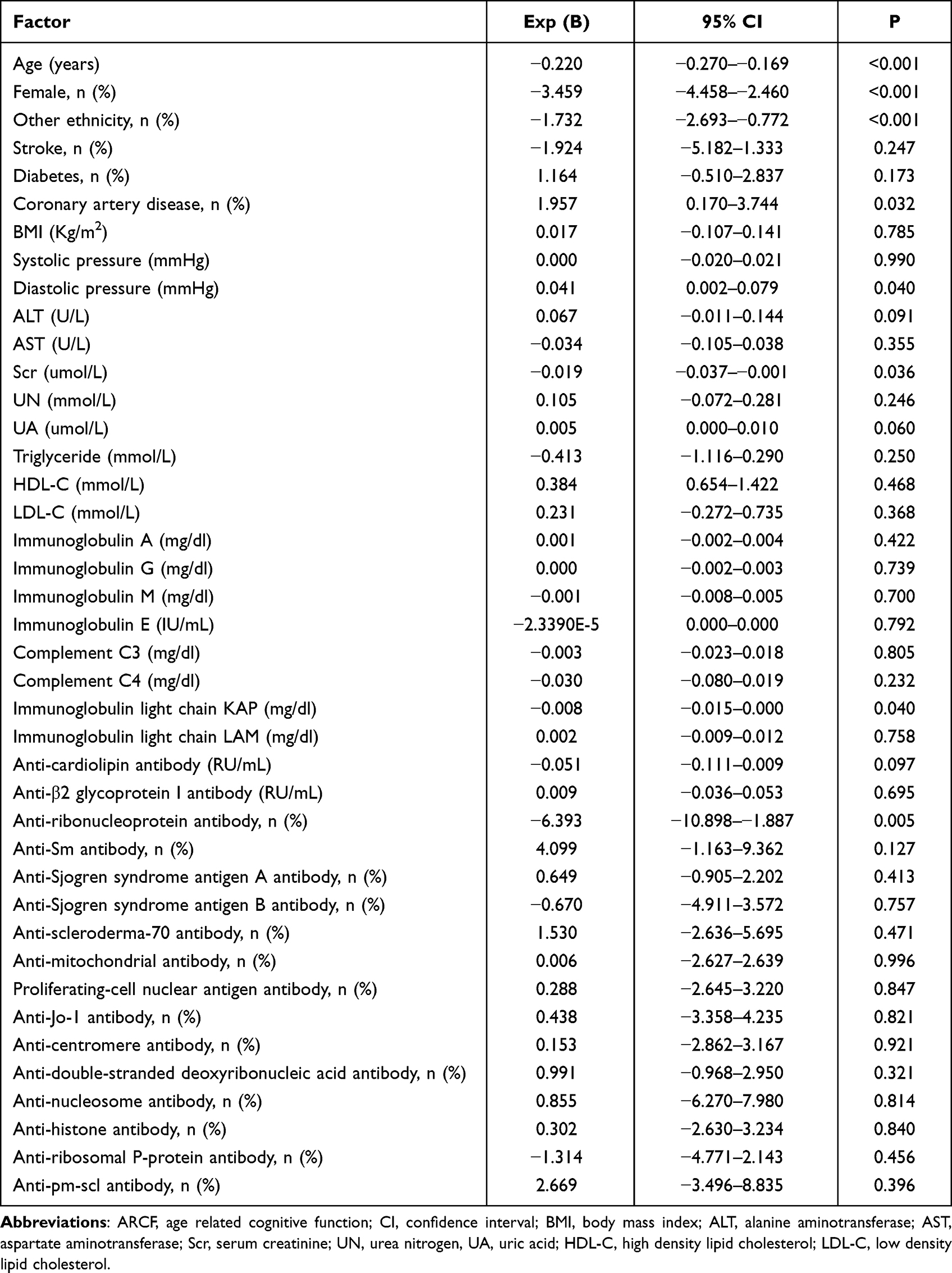 |
Table 2 Factors Associated with ARCF in Multivariate Linear Regression Analysis of Oldest-Old and Centenarian Adults |
Discussion
The present study found a positive association between diastolic pressure and ARCF in Chinese oldest-old and centenarian adults. This result was consistent with that in a study in which the incidence of cognitive decline was associated with reduced blood pressure at follow-up.15 Furthermore, hypotension and stroke are strong risk factors for development of cognitive decline.16 Lower diastolic pressure and orthostatic hypotension in older populations have been shown to be strongly correlated with increased risk of cognitive decline.17 Reduced diastolic pressure can limit blood supply to the brain, resulting in reduced blood perfusion of the brain, and exacerbation of cognitive decline.18 Reduced blood pressure may be related to small vessel disease (lacunar infarction, leukoaraiosis, subcortical white matter lesion, or micro-bleed) or large vessel disease (stroke).19 Older populations can exhibit varying degrees of vascular disease, hypotension, and cognitive decline. In addition to vascular changes, pathological changes in brain regions responsible for blood pressure regulation may promote reduced blood pressure, resulting in cognitive decline.20 Adequate control of blood pressure to prevent hypotension may help to preserve cognitive function in older populations.
Older populations with chronic kidney disease are at increased risk of cognitive decline. The prevalence of cognitive decline in patients undergoing dialysis is particularly high, with a range of 30% to 87%.21,22 Furthermore, chronic kidney disease has been shown to be closely associated with development of dementia and cognitive decline.23–25 Scr is a marker of reduced kidney function and was previously associated with cognitive decline.26 In our study, Scr was negatively associated with ARCF in Chinese oldest-old and centenarian adults. Reduced kidney function results in an inability to eliminate metabolites and toxins, which can accumulate in the body and negatively impact cognitive function.
We also found that anti-ribonucleoprotein antibody and immunoglobulin light chain KAP were negatively correlated with ARCF in Chinese oldest-old and centenarian adults. Immunoglobulin light chains are small protein molecules formed by plasma cells.27–29 Previous studies have shown that accumulation of immunoglobulin light chains in the brain may contribute to reduced cognitive function.30,31 In addition, other studies have shown that older patients positive for anti-ribonucleoprotein antibody had reduced cognitive function, and this reduction was mitigated by steroid treatment.32,33 Therefore, reduction in anti-ribonucleoprotein antibody through steroid treatment may be a strategy to protect cognitive function in older populations.
Our study was subject to several limitations. First, this was a survey of Chinese oldest-old and centenarian adults, and the results may not be generalizable to all populations. Second, this was a cross-sectional study, and the findings need to be confirmed in studies with large sample sizes that include follow-up data collection.
Conclusions
ARCF was positively associated with diastolic pressure and negatively associated with antibody expression in Chinese oldest-old and centenarian adults.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Hainan Hospital of Chinese People’s Liberation Army General Hospital (301HNLL-2016-01). Informed consent was obtained from all participants and/or their legal guardians.
Acknowledgments
We appreciate all those who participated in the present study for their continued cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (81900357, 81941021, 81903392, 81901252, 82001476, 81802804, 81801251), the Military Medical Science and Technology Youth Incubation Program (20QNPY110, 19QNP060), the Excellent Youth Incubation Program of Chinese People’s Liberation Army General Hospital (2020-YQPY-007), the Natural Science Foundation of Hainan Province (821QN389, 821MS112), the Military Medicine Youth Program of Chinese People’s Liberation Army General Hospital (QNF19069, QNF19068), the National Key R&D Program of China (2018YFC2000400), the National S&T Resource Sharing Service Platform Project of China (YCZYPT[2018]07), the Specific Research Fund of The Innovation Platform for Academicians of Hainan Province (YSPTZX202216), the Hainan Major Scientific and Technological Cooperation Project (2016KJHZ0039), the China Postdoctoral Science Foundation funded project (2019M650359, 2020M682816, 2021T140298), the Medical Big Data R&D Project of Chinese People’s Liberation Army General Hospital (MBD2018030), the National Geriatric Disease Clinical Medicine Research Center Project (NCRCG-PLAGH-2017-014), the Central Health Care Scientific Research Project (W2017BJ12), the Hainan Medical and Health Research Project (16A200057), the Sanya Medical and Health Science and Technology Innovation Project (2016YW21, 2017YW22, 2018YW11, 2018YW16), and the Clinical Scientific Research Supporting Fund of Chinese People’s Liberation Army General Hospital (2017FC-CXYY-3009). The sponsors had no role in the design, execution, interpretation, review, approval, or control of this study.
Disclosure
The authors declare no conflicts of interest.
References
1. Ricklin D, Lambris JD. Complement in immune and inflammatory disorders: pathophysiological mechanisms. J Immunol. 2013;190:3831–3838. doi:10.4049/jimmunol.1203487
2. Shen Y, Lue L, Yang L, et al. Complement activation by neurofibrillary tangles in Alzheimer’s disease. Neurosci Lett. 2001;305:165–168. doi:10.1016/S0304-3940(01)01842-0
3. Veerhuis R, Nielsen HM, Tenner AJ. Complement in the brain. Mol Immunol. 2011;48(14):1592–1603. doi:10.1016/j.molimm.2011.04.003
4. Fu S, Yao Y, Lv F, Zhang F, Zhao Y, Luan F. Associations of immunological factors with metabolic syndrome and its characteristic elements in Chinese centenarians. J Transl Med. 2018;16(1):315. doi:10.1186/s12967-018-1691-4
5. Drew DA, Weiner DE, Sarnak MJ. Cognitive Impairment in CKD: pathophysiology, management, and prevention. Am J Kidney Dis. 2019;74(6):782–790. doi:10.1053/j.ajkd.2019.05.017
6. Murray AM, Tupper DE, Knopman DS, et al. Cognitive impairment in hemodialysis patients is common. Neurology. 2006;67(2):216–223. doi:10.1212/01.wnl.0000225182.15532.40
7. Nho K, Kueider-Paisley A, Ahmad S, et al. Association of altered liver enzymes with Alzheimer disease diagnosis, cognition, neuroimaging measures, and cerebrospinal fluid biomarkers. JAMA Netw Open. 2019;2(7):e197978. doi:10.1001/jamanetworkopen.2019.7978
8. Murman DL. The Impact of Age on Cognition. Semin Hear. 2015;36(3):111–121. doi:10.1055/s-0035-1555115
9. Fu S, Hu J, Chen X, et al. Mutant single nucleotide polymorphism rs189037 in ataxia-telangiectasia mutated gene is significantly associated with ventricular wall thickness and human lifespan. Front Cardiovasc Med. 2021;8:658908. doi:10.3389/fcvm.2021.658908
10. Fu S, Yu H, Li Y, et al. Multiple measures of mineral metabolism were associated with renal function in Chinese centenarians: a cross-sectional study. Front Med. 2020;7:120. doi:10.3389/fmed.2020.00120
11. Ibrahim NM, Shohaimi S, Chong H-T, et al. Validation study of the mini-mental state examination in a Malay-speaking elderly population in Malaysia. Dement Geriatr Cogn Disord. 2009;27:247e53. doi:10.1159/000203888
12. Xiu S, Zheng Z, Guan S, Zhang J, Ma J, Chan P. Serum uric acid and impaired cognitive function in community-dwelling elderly in Beijing. Neurosci Lett. 2017;637:182e7. doi:10.1016/j.neulet.2016.11.013
13. Rabins P, Schwartz S, Tschanz JA, Corcoran C, Lyketsos C. Risk factors for severe dementia from a population-based sample of incident Alzheimer’s disease: the Cache County Dementia Progression Study. Alzheimers Dement. 2011;7:S356. doi:10.1016/j.jalz.2011.05.1031
14. Kliegel M, Zimprich D, Rott C. Life-long intellectual activities mediate the predictive effect of early education on cognitive impairment in centenarians: a retrospective study. Aging Ment Health. 2004;8:430e7. doi:10.1080/13607860410001725072
15. Molander L, Gustafson Y, Lövheim H. Longitudinal associations between blood pressure and dementia in the very old. Dement Geriatr Cogn Disord. 2010;30(3):269–276. doi:10.1159/000320252
16. Launer LJ, Ross GW, Petrovitch H, et al. Midlife blood pressure and dementia: the Honolulu-Asia Aging Study. Neurobiol Aging. 2000;21:49–55. doi:10.1016/S0197-4580(00)00096-8
17. Ou YN, Tan CC, Shen XN, et al. Blood pressure and risks of cognitive impairment and dementia: a systematic review and meta-analysis of 209 prospective studies. Hypertension. 2020;76(1):217–225. doi:10.1161/HYPERTENSIONAHA.120.14993
18. Mossello E. Hypertension, hypotension, longevity and dementia. Monaldi Arch Chest Dis. 2020;90(4). doi:10.4081/monaldi.2020.1674
19. Moss MB, Jonak E. Cerebrovascular disease and dementia: a primate model of hypertension and cognition. Alzheimers Dement. 2007;3(2 Suppl):S6–S15. doi:10.1016/j.jalz.2007.01.002
20. Novak V, Hajjar I. The relationship between blood pressure and cognitive function. Nat Rev Cardiol. 2010;7(12):686–698. doi:10.1038/nrcardio.2010.161
21. Sarnak MJ, Tighiouart H, Scott TM, et al. Frequency of and risk factors for poor cognitive performance in hemodialysis patients. Neurology. 2013;80(5):471–480. doi:10.1212/WNL.0b013e31827f0f7f
22. Griva K, Stygall J, Hankins M, Davenport A, Harrison M, Newman SP. Cognitive impairment and 7-year mortality in dialysis patients. Am J Kidney Dis. 2010;56(4):693–703. doi:10.1053/j.ajkd.2010.07.003
23. Madero M, Gul A, Sarnak MJ. Cognitive function in chronic kidney disease. Semin Dial. 2008;21:29–37. doi:10.1111/j.1525-139X.2007.00384.x
24. Murray AM. Cognitive impairment in the aging and chronic kidney disease populations: an occult burden. Adv Chronic Kidney Dis. 2008;15:123–132. doi:10.1053/j.ackd.2008.01.010
25. Murray AM, Knopman DS. Cognitive impairment in CKD: no longer an occult burden. Am J Kidney Dis. 2010;56:615–618. doi:10.1053/j.ajkd.2010.08.003
26. Elias MF, Dore GA, Davey A. Kidney disease and cognitive function. Contrib Nephrol. 2013;179:42–57.
27. Richard EL, McEvoy LK, Oren E, et al. Markers of kidney function and longitudinal cognitive ability among older community-dwelling adults: the Rancho Bernardo Study. J Alzheimers Dis. 2021;83(1):319–331. doi:10.3233/JAD-201605
28. Bai K, Pan Y, Lu F, Zhao Y, Wang J, Zhang L. Kidney function and cognitive decline in an oldest-old Chinese population. Clin Interv Aging. 2017;12:1049–1054. doi:10.2147/CIA.S134205
29. Stratta P, Gravellone L, Cena T, et al. Renal outcome and monoclonal immunoglobulin deposition disease in 289 old patients with blood cell dyscrasias: a single center experience. Crit Rev Oncol Hematol. 2011;79(1):31–42. doi:10.1016/j.critrevonc.2010.05.001
30. Popović M, Tavćar R, Glavac D, et al. Light chain deposition disease restricted to the brain: the first case report. Hum Pathol. 2007;38(1):179–184. doi:10.1016/j.humpath.2006.07.010
31. Nadeau SE. Neurologic manifestations of connective tissue disease. Neurol Clin. 2002;20:151–178. doi:10.1016/S0733-8619(03)00057-4
32. Matsui H, Udaka F, Oda M, et al. Encephalopathy and severe neuropathy due to probable systemic vasculitis as an initial manifestation of mixed connective tissue disease. Neurol India. 2006;54(1):83–85. doi:10.4103/0028-3886.24716
33. Ortega-Hernandez OD, Shoenfeld Y. Mixed connective tissue disease: an overview of clinical manifestations, diagnosis and treatment. Best Pract Res Clin Rheumatol. 2012;26(1):61–72. doi:10.1016/j.berh.2012.01.009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.