")
Back to Journals » International Journal of Women's Health » Volume 12
Adverse Obstetrical and Perinatal Outcomes Among Advanced Age Pregnant Mothers in Northeast Ethiopia: A Comparative Cross-Sectional Study
Authors Asefa U, Melese Ayele W
Received 29 September 2020
Accepted for publication 25 November 2020
Published 8 December 2020 Volume 2020:12 Pages 1161—1169
DOI https://doi.org/10.2147/IJWH.S284124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Ukba Asefa,1 Wolde Melese Ayele2
1Department of Gynecology and Obstetrics, Dessie Specialized Referral Hospital, Dessie, Amhara Regional State, Ethiopia; 2Department of Epidemiology and Biostatistics, Wollo University, Dessie, Amhara Regional State, Ethiopia
Correspondence: Wolde Melese Ayele
Department of Epidemiology and Biostatistics, Wollo University, Dessie 1145, Ethiopia
Tel +251921885231
Email [email protected]
Purpose: It is known that being pregnant at any reproductive age is not risk-free. Aside from this, older gravidity usually ends up with adverse outcomes both to the mother and newborn. Hence, the aim of this study was to investigate the association of adverse maternal and perinatal outcomes with advanced maternal age pregnancy in Northeastern Ethiopia.
Methods: A hospital-based comparative cross-sectional study was employed among pregnant mothers. The study was conducted among advanced age (≥ 35 years, n= 398) mothers and adult age (20– 34 years, n=398) mothers. Socio-demographic, obstetrics, and pregnancy outcomes were checked from patient records. Descriptive statistics were used to describe parameters collected from patient records and comparing the two groups. Bivariable and multivariable logistic regressions were done to determine factors associated with maternal and perinatal outcomes. The magnitude of the association was measured using odds ratio at 95% confidence level and statistical significance was declared at a P-value of < 0.05.
Results: Advanced age mothers had significantly higher adverse pregnancy outcomes (64.6% vs 37.8%) compared with adult age mothers. This study shows that advanced maternal age is statistically associated with pregnancy-induced hypertension (AOR=3.14, 95% CI: 1.931– 5.089), antepartum hemorrhage (AOR=2.22, 95% CI: 1.245– 3.942), a cesarean delivery (AOR=2.59, 95% CI: 1.775– 3.790), and postpartum hemorrhage (AOR=2.01, 95% CI: 1.445– 2.819). Moreover, advanced maternal age pregnancy was also a risk factor for preterm delivery (AOR=3.01, 95% CI: 1.441– 6.297), low birth weight (AOR=3.08, 95% CI: 1.735– 5.492), low fifth minute Apgar score (AOR=3.99, 95% CI: 2.099– 7.618), and perinatal death (AOR= 2.46, 95% CI: 1.360– 4.42).
Conclusion: In this study, adverse pregnancy and perinatal outcomes among advanced aged mothers were high in a specialized hospital where emergency obstetric and newborn care is set and quality obstetric care is expected. Therefore, healthcare providers, the specialized hospital, and policymakers should give due emphasis to the effective intervention of advanced age pregnant mothers.
Keywords: advanced maternal age, pregnancy, adverse obstetric outcome, adverse perinatal outcomes, Ethiopia
Introduction
Advanced Maternal Age (AMA) is being 35 or older years age believed that the age of the occurrence of adverse pregnancy outcomes by many researchers.1,2 This is because older mothers are more prone to develop chronic illnesses such as obesity, hypertension, and diabetes mellitus.3,4
In general, the overall risk of having a child with a birth-defect is small. However, these are increasing in older women.5 According to a society of obstetrics and gynecology of the Canada committee, every pregnant mother exceeding 35 years of age should be offered a test for fetal aneuploidy and screened with ultrasound as their offspring are at a higher risk of having birth defects.6,7 The incidence of preterm labor, preeclampsia, chronic hypertension, gestational diabetes mellitus, increased maternal and fetal mortality, and the cesarean birth rates are observed increasingly in advanced age pregnant mothers.8–12
Pregnancy-related adverse outcomes in advanced maternal age are a result of various salient factors. Among those, an increasing rate of divorce and remarriage, utilization of effective birth control methods, the advent of artificial reproductive technologies (ART), and women's involvement in higher education and better career opportunity could be listed.10,13,14 In contrast to developed countries, where most of the advanced maternal age women are usually primiparous, they are multiparous in developing countries owing to factors such as ineffective family planning utilization and has the interest of having a bigger family size as a result of socio-economic and cultural influence.15,16
Globally, the researchers have extensively explored the association of AMA with adverse obstetrical and perinatal outcomes. However, no researches are conducted to identify the association of advanced maternal age with these outcomes in the study area and even a few in Ethiopia. Therefore, this study aimed to determine the magnitude of obstetrical and perinatal outcomes and its association with AMA. The findings will have a vital input to the policymakers and planners in updating and designing interventions to improve pregnancy outcomes among advanced age mothers. Moreover, identifying the response of AMA pregnancy will be useful in developing an effective sensitization program for couples and enabling them about informed choices for pregnancies during advanced maternal age. To the lowest, Dessie Specialized Hospital will use the finding in the application of delivery procedures. The result will also have vital importance for clinicians, public health specialist, non-governmental initiatives, and future researchers in the related problems.
Materials and Methods
A chart review comparative cross-sectional study was conducted from March 2020 to July 2020 to assess the magnitude of adverse outcomes of advanced maternal age pregnancy in Dessie Specialized Hospital, Ethiopia. Dessie is 401 km far from Addis Ababa, the capital of the country. The city is located at an altitude of 2216 meters above sea level. According to the 2007 national census conducted by the central statistics agency of Ethiopia, Dessie has a total population of 151,174, of whom 78,242 (51.8%) are female. Dessie specialized Hospital is serving a total of eight million people surrounding it. Currently, the Hospital is serving as a teaching hospital for Wollo University.
Pregnant mothers whose age is ≥35 years were considered as a study group and mothers whose age is between 20 and 34 years old were taken as a reference group. Low birth weight (LBW) was defined as an infant weight less than 2500 g at birth. Similarly, infants’ fifth minutes Apgar score of 3 and less was considered as low fifth minutes Apgar score. The detailed operational/standard definitions of terms are presented in supplement 1. Mothers with the pre-existed medical disease, twin/triple/quadruple pregnancy, Rh-negative mothers, and incomplete records were excluded from the study.
The sample size was determined using Epi Info by assuming a one to one ratio of study to reference groups, 95% confidence level, and 80% power of the study. The proportion of mal-presentation of the fetus among AMA and the reference group 9.6 and 4.3%17 was taken to compute the sample size. Finally, it yields a total sample of 796 (398 charts of AMA and 398 charts of 20–34 age mothers).
Charts of mothers who delivered from 30 April 2019 to 01 April 2020 were retrieved using a systematic sampling technique. Two K values, K1 and K2, were computed for both study and reference groups, respectively. The values are calculated as K1 (N1/n1), where ‘N1ʹ is total mothers ≥35 years old and ‘n1ʹ is calculated sample size for study groups, and K2 (N2/n2) where ‘N2ʹ is total mothers 20–34 years old admitted in the ward during one year and ‘n2ʹ is calculated sample size for reference groups. Accordingly, K1 was 3 and K2 was 2. Charts of the study population were selected at every Kth interval of each study group. The first study mother’s chart was selected by a simple random sampling technique from each K.
Data were retrieved from the sampled pregnant mothers’ chart using a structured questionnaire which was devised by reviewing various literature. As shown in supplement 2, the questionnaire was constituted of five parts which include the socio-demographic characteristics, obstetric history of the mothers, pregnancy complications, maternal effects and mode of delivery, and adverse perinatal outcomes. Data were collected by eight graduate midwives who have experience in data collection.
The collected data were checked for its completeness, coded, and entered into SPSS version 21. The data were presented with texts and tables. Descriptive statistics was undergone to compute frequency, percentile, and mean of different variables. The binary logistic regression model was used to test the association between dependent and independent variables. Dependent variables are adverse obstetrical outcomes such as Pregnancy-Induced Hypertension (PIH), Antepartum Hemorrhage (APH), cesarean delivery, amniotic fluid disorders, Premature Rupture of Membranes (PROM), Gestational Diabetes Mellitus (GDM), and Postpartum Hemorrhage (PPH). Likewise, perinatal outcomes such as preterm delivery, low birth weight, low fifth minute Apgar score, post-term pregnancy, and perinatal death are dependent variables. Maternal age was the key independent variable of this study. Likewise, residency, Anti-natal Care (ANC), and gravidity of mothers were considered as independent variables. All variables with
P-value ≤0.2 were included in the multivariable analysis. The magnitude of the association was measured using odds ratio at 95% confidence interval and statistical significance was declared at P-value of <0.05.
Results
Socio-Demographic Characteristics of the Participants
A total of 752 mothers’ charts were reviewed, making a response rate of 94.5%. The mean age of the advanced age mothers was 38 years old with a standard deviation of 3.12, while the adult mothers were 26.56 years old with a standard deviation of 3.49. Sixty-eight (18.1%) of advanced aged mothers and 51 (13.5%) of adult mothers had less than four times anti-natal (ANC) follow up. Two hundred fourteen (57%) and 196 (52.1%) of advanced age mothers and adult age mothers were multigravidas, respectively. The socio-demographic descriptive table is shown in Table 1.
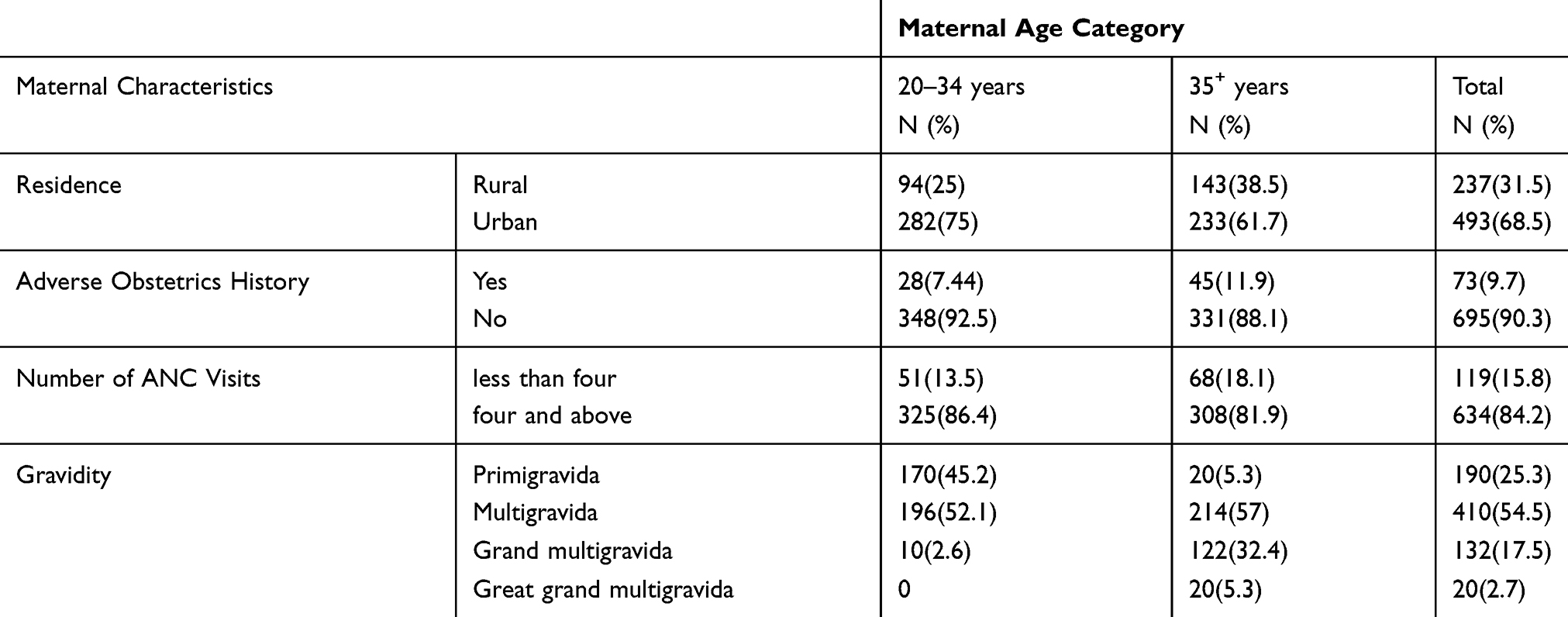 |
Table 1 Obstetrics Characteristics and Residence of Advanced and Adult Mothers, Dessie Referral Hospital, Northeast Ethiopia (n=752) |
Magnitude of Maternal Related Characteristics
This study revealed that the magnitude of pregnancy-induced hypertension and antepartum hemorrhage among advanced age mothers were 70 (18.6%) and 60 (16%), respectively. However, these were 26 (6.9) and 20 (5.3%) in adult age mothers. Slightly higher advanced mothers had GDM (1.6% Vs 2.4%) compared to adult pregnant mothers. Almost one-third of 129 (34.7%) advanced age mothers and 82 (21.8%) adult mothers underwent cesarean section. Roughly higher 20 (5.4%) of advanced age mothers had postpartum hemorrhage than adult mothers 5 (1.3%). The overall obstetrical outcomes are presented in Table 2.
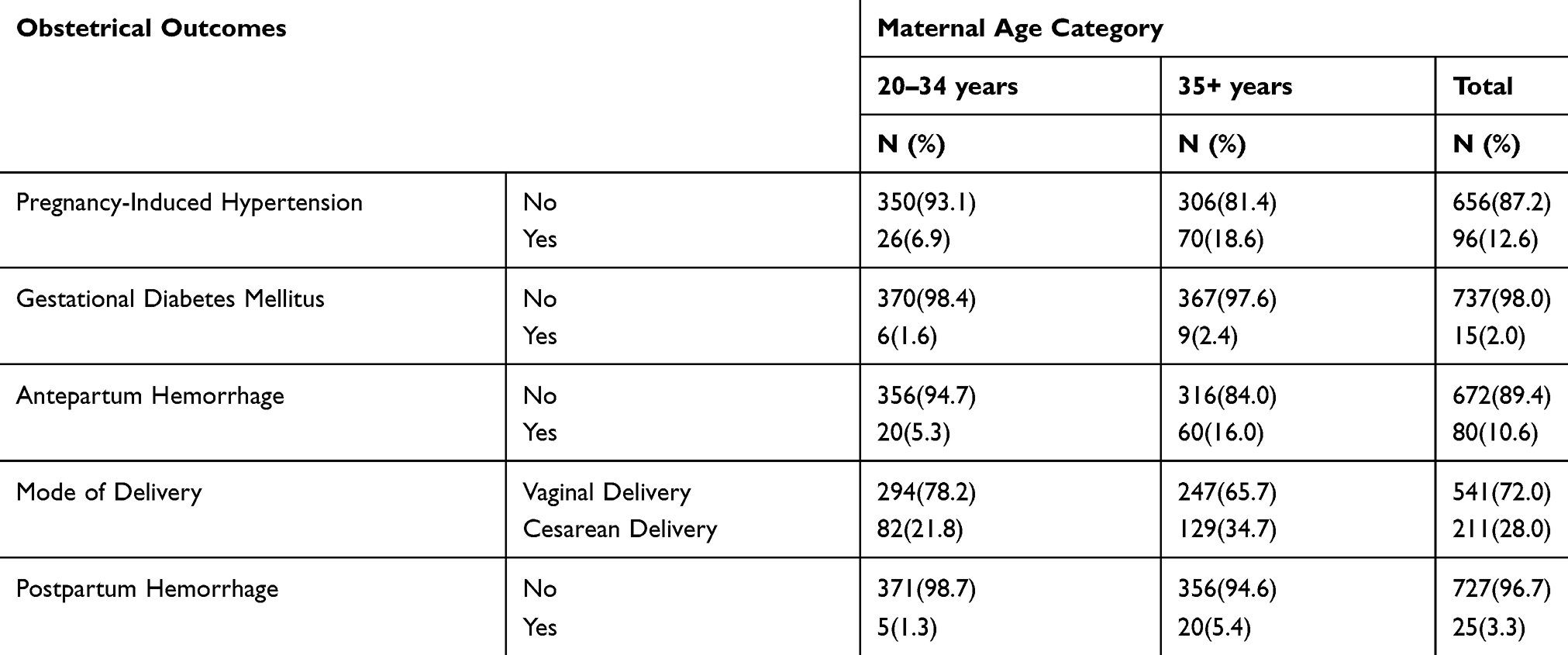 |
Table 2 Magnitude of Adverse Obstetrical Outcomes of Advanced and Adult Mothers, Dessie Referral Hospital, Northeast Ethiopia (n=752) |
Magnitude of Adverse Neonatal Outcomes
The overall adverse neonatal outcome among advanced aged mothers was 281 (74.7%), while among adult age mother was 96 (25.3%). The mean gestation week was 37.9±2.3 (mean ± SD) among advanced aged mothers and 38.19±2.0 (mean ± SD) among adult mothers. Similarly, the mean birth weight of babies born from advanced age mothers was 3187.3 grams ± 543.1 (mean ± SD), whereas babies born from adult mothers had a mean birth weight of 3259 grams ± 500.2 (mean ± SD). The descriptive table is shown in Table 3.
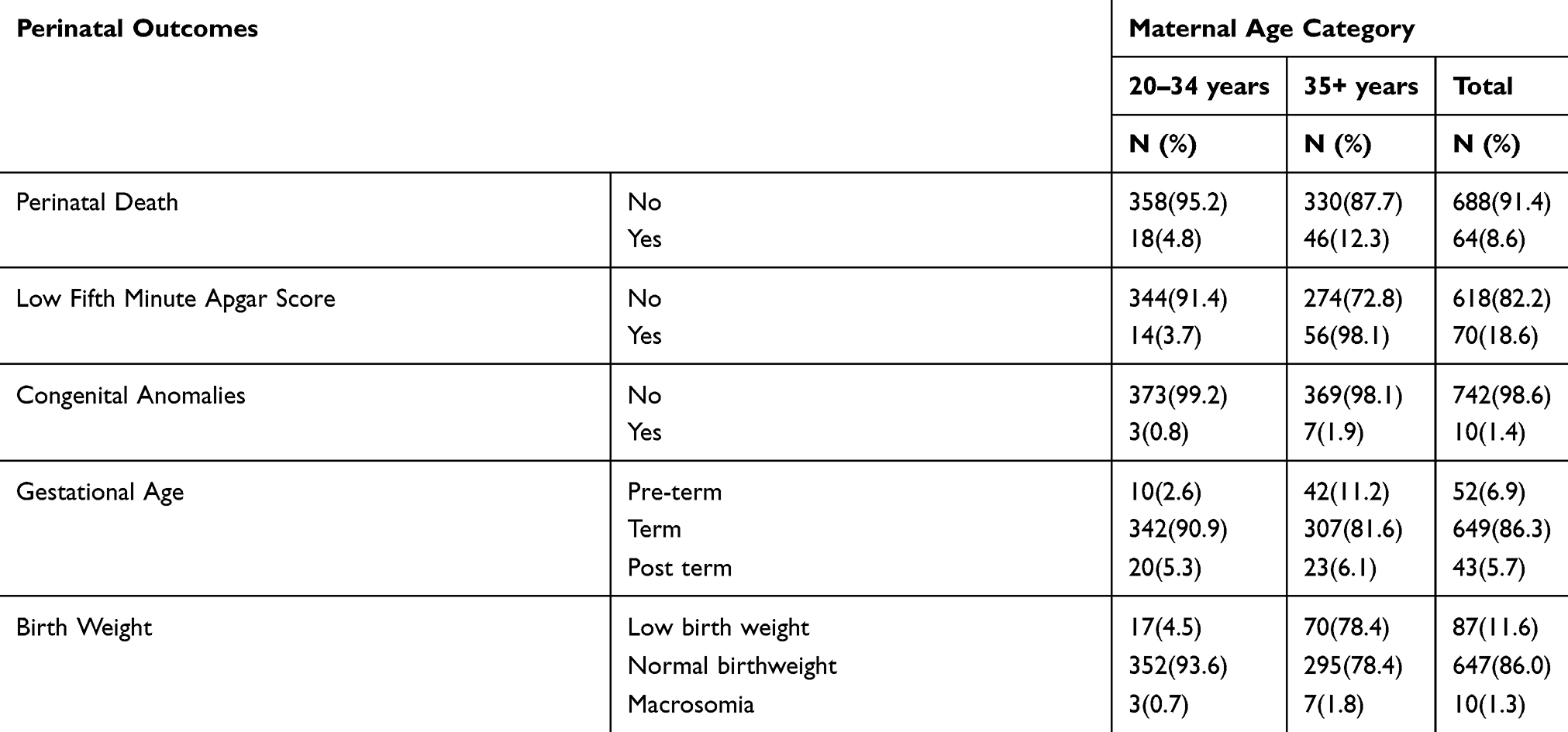 |
Table 3 Magnitude of Adverse Perinatal Outcomes of Advanced and Adult Mothers, Dessie Referral Hospital, Northeast Ethiopia (n=752) |
Association of Maternal Age with Adverse Obstetrical Outcomes
This study comprised five obstetrical outcome variables. Age was statistically significantly associated with four (pregnancy-induced-hypertension, antepartum hemorrhage, postpartum hemorrhage, and mode of delivery) adverse maternal outcome variables encompassed in this study. Advanced age mothers were three times more likely to get pregnancy-induced-hypertension than their reference group [AOR=3.13, 95% CI: 1.931–5.089].
Besides, the advanced age mothers were 2.21 times more likely to develop antepartum hemorrhage compared to adult age mothers during their pregnancy period [AOR=2.21, 95% CI: 1.245–3.942]. Moreover, advanced age mothers were more than two times more likely to undergo a cesarean section than their counterparts [AOR=2.59, 95% CI: 1.775–3.790].
Similarly, advanced age mothers were four-fold at risk of developing postpartum hemorrhage than adult mothers during their pregnancy [AOR=4.16, 95% CI: 1.548–11.227]. The overall regression result is shown in Table 4.
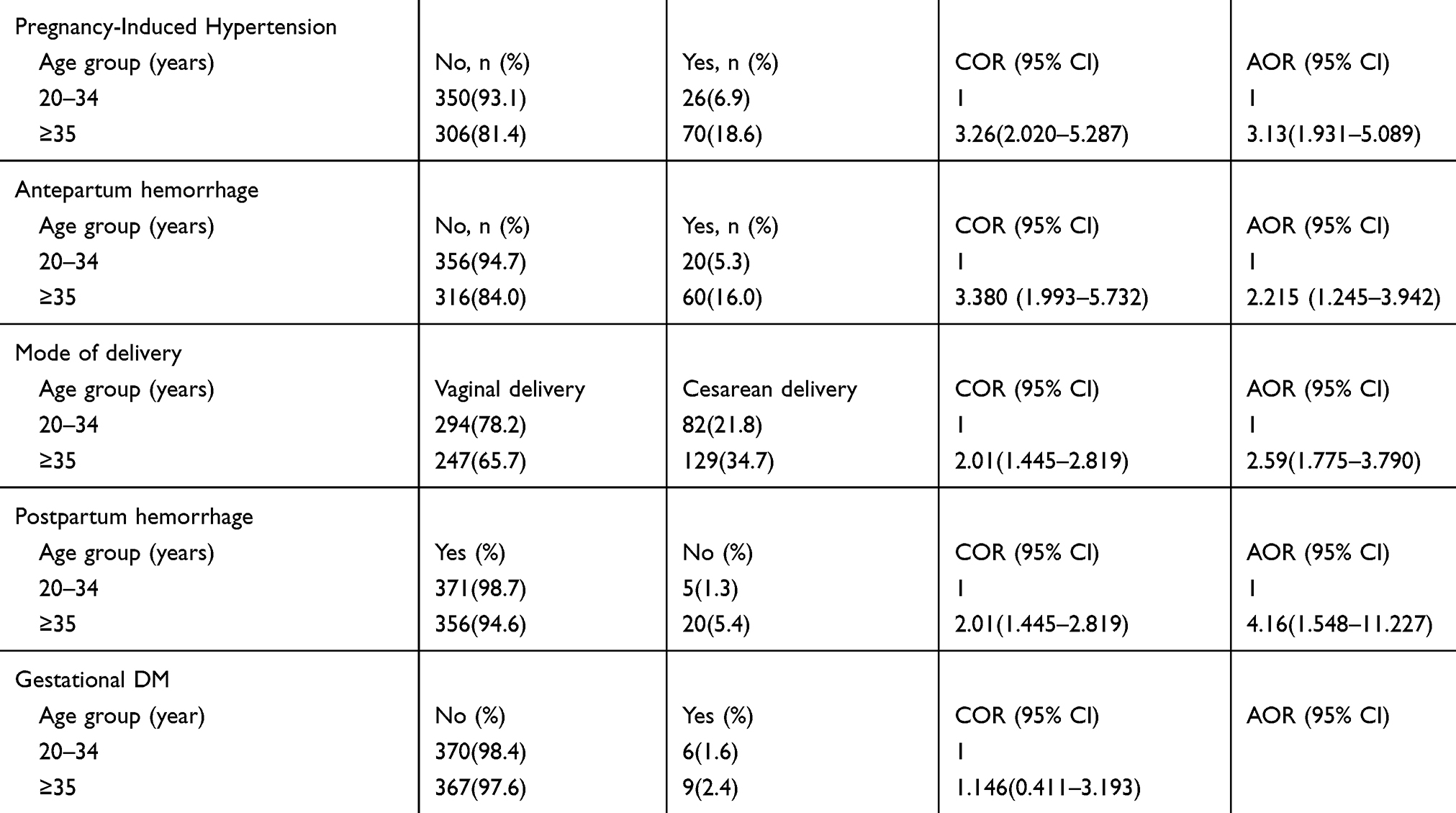 |
Table 4 Bivariate and Multivariate Analyses of Association of Adverse Pregnancy Outcomes with Maternal Age in Dessie Referral Hospital, Northeast Ethiopia (n=752) |
Associated Maternal Age with Perinatal Outcomes
This study revealed that perinatal death is significantly associated with maternal age. Perinatal death was 2.46 times more likely to happen upon in babies born from advanced age mothers than adult pregnancy [AOR=2.46, 95% CI: 1.36–4.42]. Also, pre-term delivery, low birth weight, and low fifth minute Apgar score were found to be significantly associated with maternal age. Babies born from advanced age mothers were 3.01 times more likely to be born prematurely [AOR=3.01, 95% CI: 1.441–6.297].
Likewise, babies born from advanced age mothers were 3.08 times more likely to be low birth weight [AOR=3.08, 95% CI: 1.735–5.492] and 3.99 times more likely to have low fifth minute Apgar score [AOR=3.99, 95% CI: 2.099–7.618] than babies born from the reference aged mothers. Residency, ANC follow-up, and gravidity of mothers did not show statistically significant association with perinatal outcomes. The regression results are presented in Table 5.
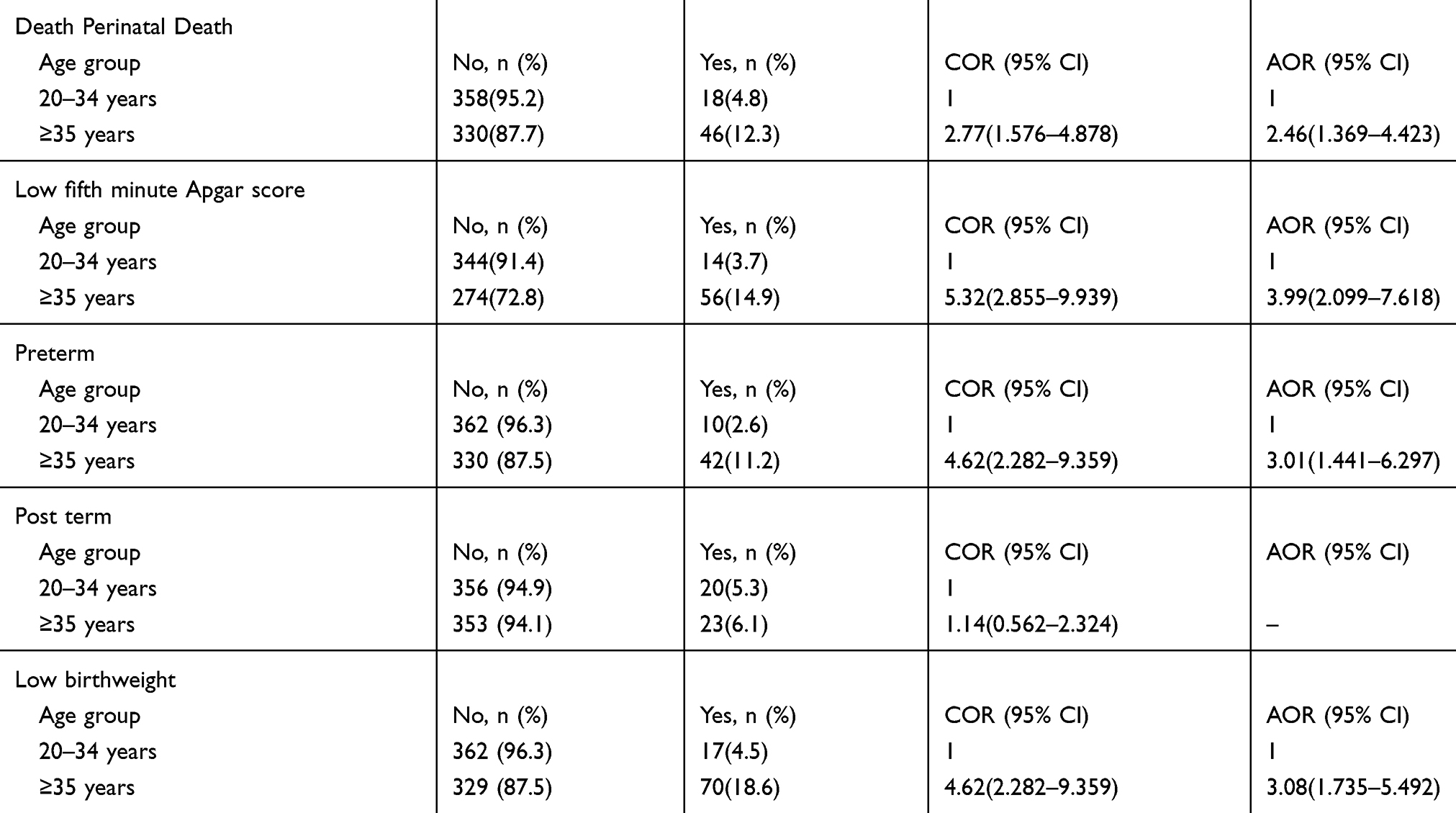 |
Table 5 Bivariate and Multivariate Analyses of Associated Advance Age with Adverse Perinatal Outcomes in Dessie Referral Hospital, Northeast Ethiopia (n=752) |
Discussion
The overall adverse pregnancy outcome among advanced age mothers and adult mothers was 64.6% and 37.8%, respectively, which indicates that there is a significant difference between the two groups. The result is in line with the reports in studies in Ayder Hospital Ethiopia and worldwide multicounty assessment.17,18
This study showed that advanced maternal age was statistically significantly associated with many adverse pregnancy outcomes. One of the main findings of this study was the association of maternal age with pregnancy-induced hypertension (PIH). Advanced age pregnant mothers were three times more likely to happenstance pregnancy-induced hypertension compared with adult mothers. This finding is consistent with the study done in Northern Ethiopia, Malaysia, and the United Kingdom.17,19,20 Likewise, it is congruent with studies in Saudi Arabia and Turkey21,22 in which there is a significant difference among advanced and adult aged pregnant mothers. Science proved that endothelial response to vasodilators diminishes as mothers get older.23 This fact might be the main reason for the similarity of the studies. However, a study conducted in India contradicts this study in which pregnancy-induced hypertension has no significant association with maternal age.24 This variation might be due to the sample size and socio-demographic difference between the two study areas.
This study also revealed that maternal age was found to be a statistically associated risk factor of APH. This finding is consistent with studies done in Northern Ethiopia and Amman Jordan.17,25 Increased gravidity in advanced age mothers makes them at greater risk of having abnormal placentation.23,26 This fact might be the cause of the similarities of the findings. However, according to the report in the studies from Turkey and India, maternal age and APH have no statistically significant association.21,24 This distinction could be secondary to the difference in the setup of the study areas. Studies conducted in a tertiary hospital that mainly provides services to referral cases from the periphery health institutions.
This study also shows that advanced age mothers were 2.5 times more likely to have their baby born through cesarean section than their adult counterparts. This finding is harmonious with the studies in literature in which an increased risk of cesarean delivery in advanced age pregnancies.8,27–29 Likewise, it is similar to studies done in India, Malaysia, and the UK.19,20,24 This can be secondary to bad obstetric history is common in advanced aged mothers so that mothers with bad obstetric history would choose anonymously to undergo cesarean section because it is assumed safer than vaginal delivery, and pregnancy complications like PIH and APH saw in advanced age mothers and cesarean section could be contemplated for maternal reasons.
Moreover, maternal age was statistically significantly associated with postpartum hemorrhage. Advance aged mothers were roughly fourfold risk of experiencing PPH when compared to adult counterparts. This result is similar to the studies done in Malaysia, Saudi Arabia, the UK, and South Korea concluded that advanced maternal age was a major risk factor for PPH.19,20,30,31 However, studies in Northern Ethiopia and Jordan show that maternal age has no significant association with PPH.17,25 This difference might be due to the former studies are conducted in tertiary hospitals in which more obstetricians are deployed.
The findings of this study showed that maternal age had association with perinatal death, low fifth minute Apgar score, preterm, post-term, and low birth weight perinatal outcomes.
Babies born from advanced age mothers were almost 2.5 times more likely to die within the first week of life than babies of the reference group. This finding is compatible with studies done in Northern Ethiopia, Australia, and worldwide multi-country assessment.18,32 The higher bad obstetrical outcomes like PIH, PPH, and GDM more observed among advanced age mothers might be the fact to have perinatal deaths. However, studies from the UK and South Korea contradicted this study found. The findings showed that there was no statistically significant association of perinatal deaths with advanced maternal age pregnancy.20,31 Economically, Ethiopia and those countries are not comparable. This difference intern attributed to having a difference in the quality of healthcare services. Therefore, the difference in the findings could be due to the high quality of obstetrical care service in later studies.
Correspondingly, this study showed that advanced age mothers were approximately three times more likely to have premature babies when compared with babies from adult mothers. This result is similar to studies done in Ayder Teaching Hospital Ethiopia,17 South Africa, Brazil, and South Korea.31,33,34 Similarly, the result is in line with a multi-country assessment held by the World Health Organization (WHO).18 This might be attributed to the fact that pregnancy complications are more abundant in advanced age mothers. However, this finding is contradicted by the studies done in Malaysia and the UK which showed no association of maternal age with preterm delivery.19,20 This might be due to socio-economic differences, lifestyle quality, and health infrastructural differences in the studies.
In addition, this study disclosed that maternal age was a significant predictor for a low birth weight that is supported by studies done in Ayder Teaching Hospital Ethiopia, Brazil, and a multi-country assessment involved 29 middle- and low-income countries.13,17,30 This similarity might be due to the majority of pregnancy-related complications are observed in advanced age mothers. An iatrogenic immaturity could supplement those adverse pregnancy outcomes. However, the finding of this study is yet inconsistent with studies done in Malaysia and Jordan that showed no significant association between maternal age and low birth weight.19,25 This discrepancy might be due to the difference in sample size and socio-economic differences.
Furthermore, this study revealed that babies born from advanced age mothers were four times more probable to have low fifth minute Apgar score comparing to babies from adult mothers. This result is consistent with the studies done in Ayder Teaching Hospital, Ethiopia, Turkey, India, and Brazil.17,21,24,34 On top of this, the finding is in line with a multi-country assessment conducted in 29 countries.18 But, this finding is inconsistent with the studies in Jordan and Malaysian that show no association between low fifth minute Apgar score and advanced maternal age pregnancy.19,25 That could be due to the difference in sample size and lifestyle of the study participants.
Lastly, this study revealed that there was no statistically significant association between maternal age and macrosomia and post-term pregnancy outcome variables. Although the finding is compatible with a study done in the UK,20 it is discordant with the result from a study in Brazilian that stated that advanced age mothers were associated with macrosomia and post-term pregnancy.34 This disagreement could be due to the difference in sample size used and study design employed. Similarly, the finding of this study showed no association between congenital anomalies and maternal age. In contradiction to this, a study in South Korea showed that there is a statistically significant association.31 This difference mainly due to the difference in sample size.
This study had the strength of inclusion of a large sample size. However, it has the following limitations. The first was the retrospective nature of the design that unable to ascertain the temporality of variables and unable to include other independent predictors like behavior, knowledge, attitude, and other factors that might be the risk factors for various adverse pregnancy outcomes. Second, since the study was institution-based, it is unable to extrapolate the findings to the general population. Lastly, since early pregnancy adverse outcomes like GTDs, ectopic pregnancy, and abortion are not addressed, the investigators recommended future researchers.
Conclusion
This study affirmed that advanced maternal age is an independent predictor of pregnancy-induced hypertension, antepartum hemorrhage, cesarean delivery, and postpartum hemorrhage adverse maternal outcomes. Furthermore, advanced maternal age was statistically significantly associated with perinatal dependent variables such as perinatal death, preterm delivery, low birth weight, and low fifth minute Apgar score.
Therefore, the investigators renowned the healthcare providers especially obstetricians, planners, and the policy-makers, use the result of this study in guiding evidence-based decision-making regarding decreasing adverse obstetrical and perinatal outcomes. Also, these results might use to notify spouses to choose the age of the pregnancy.
Abbreviation
ANC, Antenatal Care; AOR, Adjusted Odds Ratio; APH, Antepartum Hemorrhage; GDM, Gestational Diabetes Mellitus; PIH, Pregnancy-Induced Hypertension; PPH, Postpartum Hemorrhage.
Data Sharing Statement
All the necessary data are included in the manuscript. The raw data are accessible at the corresponding author with a reasonable request.
Ethical Approval
Ethical clearance was insured from Wollo University, College of Medicine and Health Sciences ethical review committee with a ref. No/515/0-01/12. Similarly, a written permission letter was obtained from the Dessie Specialized Hospital. Since the study design used a retrospective method, we did not consent the participants. However, we have not used personal medical registration numbers (MRN) during data collection for personal anonymity. Allover; the risks, burdens, and benefits that the participants will take were in accordance with the Declaration of Helsinki. The collected data have been kept confidential.
Consent for Publication
Not applicable.
Acknowledgments
We are grateful to thank Wollo University, college of medicine ethical review committee. We also want to gratify all obstetricians at Dessie referral Hospital. The data collectors and data clerks in the hospital accordingly acknowledged. Lastly, we obligated to acknowledge Tesfaye Birhane and Muluken Genetu for their support in data analysis and final manuscript editing.
Funding
This investigation received no specific grant from funding agency in public commercial, or for profit sectors.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Giri A, Srivastav V, Suwal A, Tuladhar AJNMCJ. Advanced maternal age and obstetric outcome. 2012;15(2):87–90.
2. Dekker R. Evidence on: advanced Maternal Age.
3. Wang S-C, Wang L, Lee M-C. Adolescent mothers and older mothers: who is at higher risk for adverse birth outcomes? 2012;126(12):1038–1043.
4. Palmsten K, Buka SL, Michels KBJO. Maternal pregnancy-related hypertension and risk for hypertension in offspring later in life. gynecology. 2010;116(4):858. doi:10.1097/AOG.0b013e3181f3a1f9
5. Ryu HM. Should advanced maternal age be a reasonable indication for invasive diagnostic testing? Obstet Gynecol Sci. 2013;56(3):135–136. doi:10.5468/ogs.2013.56.3.135
6. childbearing SCOoD. J Obstet Gynaecol. 2012;34((1)):80–93.
7. Mais A. The Association of Advanced Maternal Age and Adverse Pregnancy Outcomes, Thesis. Georgia State University; 2015.
8. Van Katwijk C, Peeters L. Clinical aspects of pregnancy after the age of 35 years: a review of the literature. 1998;4(2):185–194.
9. Kirz DS, Dorchester W, Freeman R. Advanced maternal age: the mature gravida. gynecology. 1985;152(1):7–12.
10. Bianco A, Stone J, Lynch L, et al. Pregnancy outcome at age 40 and older. 1996;87(6):917–922.
11. Jacobsson B, Ladfors L, Milsom IJO. Advanced maternal age and adverse perinatal outcome. Gynecology. 2004;104(4):727–733. doi:10.1097/01.AOG.0000140682.63746.be
12. Usta IM, Nassar A. Part I: obstetric complications. Advanced Maternal Age. 2008;25(08):521–534.
13. Yang Y-O, Peden-McAlpine C, Chen C-HJM. A qualitative study of the experiences of Taiwanese women having their first baby after the age of 35 years. Midwifery. 2007;23(4):343–349.
14. Windridge KC, Berryman JCJB. Women’s experiences of giving birth after 35. Birth. 1999;26(1):16–23.
15. Olusanya BOSO. Perinatal correlates of delayed childbearing in a developing country. Arch Gynecol Obstet. 2012;285((4)):951–957. doi:10.1007/s00404-011-2105-5
16. Jolly M, Sebire N, Harris J, Robinson S, Regan L. The risks associated with pregnancy in women aged 35 years or older. Human Reproduction. 2000;15(11):2433–2437.
17. Maeruf H, Robles CC, Woldemariam S, et al. Advanced maternal age pregnancy and its adverse obstetrical and perinatal outcomes in Ayder comprehensive specialized hospital, Northern Ethiopia, 2017: a comparative cross-sectional study. BMC pregnancy and childbirth. 2020;20(1):60.
18. Laopaiboon M, Lumbiganon P, Intarut N, et al. Advanced maternal age and pregnancy outcomes: a multicountry assessment. An International Journal of Obstetrics & Gynaecology. 2014;121:49–56.
19. Rashed HEM, Awaluddin S, Ahmed N, Supar NHM, Lani ZM, Aziz FJSM. Advanced maternal age and adverse pregnancy outcomes in Muar, Johor, Malaysia. Sains Malaysiana. 2016;45(10):1537–1542.
20. Khalil A, Syngelaki A, Maiz N, Zinevich Y, Nicolaides K. Maternal age and adverse pregnancy outcome: a cohort study. Gynecology. 2013;42(6):634–643.
21. Ertuğrul Yılmaz ÖAT, Tarhan N, et al. Perinatal outcomes in advanced age pregnancies. J Clin Experimental Investigations. 2016;7(2):157–162.
22. Abdel-Hady El-Gilany SH. Obstetric outcomes of teenagers and older mothers: experience from Saudi Arabia. Int J Collaborative Res Internal Med Public Health. 2012;4(6).
23. Franklin SSLM, Khan SA, et al. Does the relation of blood pressure to coronary heart disease risk change with aging? Framingham Heart Study. 2001;103:1245. doi:10.1161/01.CIR.103.9.1245
24. Kamlesh NDC, Gauret K, et al. Pregnancy outcome comparison in elderly and non elderly primigravida attending at mahila chikitsalay. Jaipur (Rajasthan) India International Multispecialty J Health (IMJH). 2015;1(1).
25. Amarin V. Effect of maternal age on pregnancy outcome: a hospital based study. J Med Med Res. 2013;1(4):28–31.
26. Hung T-H, Shau W-Y, Hsieh -C-C, Chiu T-H, Hsu -J-J-JO. Risk factors for placenta accreta. Gynecology. 1999;93(4):545–550.
27. Wang Y, Tanbo T, Åbyholm T, Henriksen T. The impact of advanced maternal age and parity on obstetric and perinatal outcomes in singleton gestations. Obstetrics. 2011;284(1):31–37.
28. Dulitzki M, Soriano D, Schiff E, et al. Effect of very advanced maternal age on pregnancy outcome and rate of cesarean delivery. Obstetrics & Gynecology. 1998;92(6):935–939.
29. Driul L, Londero AP, Bertozzi S, et al. Pregnancy outcome and neonatal health by mothers aged 40 years and over. Journal of Medicine and Medical Sciences. 2010;1(5):148–155.
30. El-Gilany A-H, Hammad S, Health P. Obstetric outcomes of teenagers and older mothers: experience from Saudi Arabia. International Journal of Collaborative Research on Internal Medicine & Public Health. 2012;4(6):901.
31. Koo Y-J, Ryu H-M, Yang J-H, et al. Pregnancy outcomes according to increasing maternal age. Taiwanese Journal of Obstetrics and Gynecology. 2012;51(1):60–65.
32. Arnold ABM, Flenady V, et al. Term stillbirth in older women. Aust N Z J Obstet Gynaecol. 2012;52((3)):286–289. doi:10.1111/j.1479-828X.2011.01404.x
33. Hoque M. Advanced maternal age and outcomes of pregnancy: A retrospective study from South Africa biomedical research. 2012;23((2)):281–285.
34. Núbia Karla O, Almeida R. Adverse perinatal outcomes for advanced maternal age: a cross-sectional study of Brazilian births. J Pediatr. 2015;91((5)):493–498. doi:10.1016/j.jped.2014.12.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.