")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 17
Adverse Drug Reactions of Acetylcholinesterase Inhibitors in Older People Living with Dementia: A Comprehensive Literature Review
Authors Ruangritchankul S , Chantharit P , Srisuma S , Gray LC
Received 5 June 2021
Accepted for publication 16 August 2021
Published 4 September 2021 Volume 2021:17 Pages 927—949
DOI https://doi.org/10.2147/TCRM.S323387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Sirasa Ruangritchankul,1 Prawat Chantharit,2 Sahaphume Srisuma,3 Leonard C Gray4
1Division of Geriatric Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Division of Infectious Diseases, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Ramathibodi Poison Center and Division of Clinical Pharmacology and Toxicology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 4Centre for Health Services Research, Faculty of Medicine, The University of Queensland, Brisbane, QLD, Australia
Correspondence: Sirasa Ruangritchankul
Division of Geriatric Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand
Tel +66 816404373
Fax +66 22012588
Email [email protected]
Abstract: The rising of global geriatric population has contributed to increased prevalence of dementia. Dementia is a neurodegenerative disease, which is characterized by progressive deterioration of cognitive functions, such as judgment, language, memory, attention and visuospatial ability. Dementia not only has profoundly devastating physical and psychological health outcomes, but it also poses a considerable healthcare expenditure and burdens. Acetylcholinesterase inhibitors (AChEIs), or so-called anti-dementia medications, have been developed to delay the progression of neurocognitive disorders and to decrease healthcare needs. AChEIs have been widely prescribed in clinical practice for the treatment of Alzheimer’s disease, which account for 70% of dementia. The rising use of AChEIs results in increased adverse drug reactions (ADRs) such as cardiovascular and gastrointestinal adverse effects, resulting from overstimulation of peripheral cholinergic activity and muscarinic receptor activation. Changes in pharmacokinetics (PK), pharmacodynamics (PD) and pharmacogenetics (PGx), and occurrence of drug interactions are said to be major risk factors of ADRs of AChEIs in this population. To date, comprehensive reviews in ADRs of AChEIs have so far been scarcely studied. Therefore, we aimed to recapitulate and update the diverse aspects of AChEIs, including the mechanisms of action, characteristics and risk factors of ADRs, and preventive strategies of their ADRs. The collation of this knowledge is essential to facilitate efforts to reduce ADRs of AChEIs.
Keywords: older adults, dementia, acetylcholinesterase inhibitors, adverse drug reactions, drug–drug interactions
Introduction
Globally, the number of older population aged 60 years or over was 962 million in 2017 and will almost double to reach 2.1 billion by 2050.1,2 The rising geriatric population results in an exponential increase in incidence of neurodegenerative disorders such as dementia.3,4 Worldwide, the population of people living with dementia was estimated at 50 million in 2017 and is predicted to increase to 131.5 million by 2050.5,6 Dementia is described as symptoms related to a cluster of major neurocognitive disorders or conditions which are usually manifested as slowly progressive decline of multiple cortical functions including orientation, comprehension, memory, language, learning skills and problem-solving ability.7 The most common type of dementia is AD (50–75%), followed by vascular dementia (20%), dementia with Lewy bodies (5%) and finally frontotemporal lobar dementia (5%).8–10 In AD, the progressive loss of cholinergic neurons in the basal forebrain leads to a decrease in acetylcholine (ACh) which is essential in cognition and neuroprotection.11 Dementia has a devastating impact on healthcare infrastructures in economic and medical aspects. This neurodegenerative disease is one of the leading causes of death and contributors to premature disability and dependency burdens.5,12,13 With increased disability, dementia could be overwhelming for caregivers and families, leading to increased healthcare needs.3,12,14–17 Appropriate management, including non-pharmacological and pharmacological therapies, are necessary to delay worsening of symptoms and to reduce healthcare burdens.18 Anti-dementia medications are being used worldwide, especially in Alzheimer’s disease (AD), which is the most common type of dementia.19 One-fourth of older people with dementia are prescribed anti-dementia medications which are classified into two classes: Acetylcholinesterase inhibitors (AChEIs) and N-Methyl-D-aspartate (NMDA) receptor antagonists.20,21 AChEIs were the first pharmacological treatment approved by the US Food and Drug Administration (FDA) for AD and have been reported to be used in 10–20% of dementia patients.22–25
The aging population usually have multiple other chronic diseases as well as behavioral and psychological symptoms of dementia (BPSD),12,22,26–35 resulting in the concurrent use of five or more medications or polypharmacy.26 The exposure of 82–98% of people with dementia to polypharmacy was reported in previous studies.36–38 This can lead to a greater risk of undesirable or harmful reactions to medications or adverse drug reactions (ADRs).39–41 The alterations in pharmacokinetics (PK), pharmacodynamics (PD) and pharmacogenetics (PGx) of AChEIs also result in higher risk of AChEIs’ ADR.42–47 Over the last decades, there has been an increase in the reports of AChEI-induced ADRs with 70% being severe and up to 2.3% being fatal ADRs.48–50
Therefore, the significance of the paper is to facilitate effort to address the issue of AChEI-induced ADRs among older patients with dementia. We aim to review and update the diverse aspects of AChEIs such as the mechanisms of action, characteristics and risk factors of ADRs, and preventive strategies of their ADRs.
Search Strategy
PubMed, Scopus and Web of Science databases were searched for relevant articles published in English from January 1, 1976 until March 31, 2021. The search terms were “donepezil”, “galantamine”, “rivastigmine”, “acetylcholinesterase inhibitors”, “dementia”, “Alzheimer’s disease”, “older adults”, “mechanism”, “pharmacokinetics”, “pharmacodynamics”, “pharmacogenetics”, “adverse drug reactions”, “drug-drug interactions”, “prevention”. Google Scholar was searched using main keywords for any additional studies.
Acetylcholinesterase Inhibitors
Mechanism of Acetylcholinesterase Inhibitors
ACh is mostly hydrolyzed by acetylcholinesterase (AChE) and butyrylcholinesterase (BuChE).51 Both enzymes are responsible for rapid hydrolysis of ACh in synaptic clefts, producing the products: Choline and acetate. AChE predominates in the human brain whereas BuChE is widely distributed in peripheral nervous system (PNS) and other organs such as intestine, heart and liver.52–54 In the brain, AChE levels are usually high in synapses while BuChE is distributed in glial cells.53 In AD patients, BuChE has progressively increased activity in particular part of the brain such as hippocampal area and has raised accumulation of Aβ-aggregation and neurofibrillary tangles, resulting in the reduction of ACh.52,55–61 Therefore, a class of AChEIs is developed to block both AChE and BuChE in the synaptic clefts to reduce the degradation of Ach.19 Furthermore, one AChEI has a pharmacological property for modulation of muscarinic or nicotinic receptors, contributing to enhancement of cholinergic activity.62 AChEIs increase cholinergic activities to improve and sustain cognitive functions and ADLs as well as to make better psycho-behavioral symptoms in dementia patients.22 However, AChEIs also inhibit rapid hydrolysis of ACh in PNS including sympathetic autonomic nervous system, and parasympathetic and preganglionic sympathetic neurons. This leads to peripheral adverse outcomes, such as diarrhea, nausea and vomiting, dizziness, and muscle cramping.63
The first-generation of AChEIs such as tacrine, velnacrine, and physostigmine were removed from the market because of high incidence rates of potential drug interactions and serious side effects.64 Three second-generation AChEIs were rapidly developed to replace the first-generation AChEIs. Donepezil, galantamine and rivastigmine have been approved by the FDA for the treatment of AD. Donepezil (58.4%) is the most frequently prescribed AChEIs, followed by rivastigmine (13.6%) and galantamine (12.4%).22,65–67 Donepezil in oral form and rivastigmine transdermal patches have received regulatory approval for the treatment of all stages of AD ranging from mild to severe.19,22,68–80 There is no significant difference between the efficacy of these AChEIs in terms of improving psychometric and cognitive scales.81 However, three AChEIs differ in both PK and PD properties,82–84 as shown in Supplementary Table 1.
Donepezil
Donepezil was the first AChEI approved by the FDA for AD treatment in 1996. It is a piperidine-based reversible inhibitor of AChE.82,85 Donepezil is 500-fold selective for AChE inhibition in comparison with BuChE.86,87 The oral bioavailability is 100% and time to peak plasma concentration (Tmax) approximates 3–5 hours following a single-dose administration.88,89 Plasma albumin binding is 75% and volume of distribution (Vd) is 12 L/kg.88–90 Donepezil readily transports across the blood brain barrier (BBB), resulting in 7-fold higher concentration in the brain compared with plasma. Cytochrome P450 2D6 (CYP2D6) is accounted for the major Phase I metabolism (90%) and the rest by Cytochrome P450 3A4 (CYP3A4).89,91 6-O-desmethyl donepezil (6DD) is the end product of Phase II metabolism which is excreted via kidney route.88,92 The average apparent plasma clearance is approximately 0.13–0.19 L/h/kg. According to its elimination half-life (70 hours), it takes around 15 days to reach the steady state. Then, it is conveniently administered as once daily.88,89 Both 5 mg and 10 mg once daily administration for 24 weeks could improve cognitive and quality of life scales in mild to moderate AD patients.93–95 The initial dose should be administered initially with 5 mg/day, followed by slow-dose titration every 4–6 weeks along with the clinical status monitoring until reaching the maximum dose of 10 mg for mild to moderate AD.64,95 For severe AD, the maximum daily dose of donepezil is 23 mg once daily.76
Rivastigmine
Rivastigmine was approved by the FDA to be marketed in 1997. Rivastigmine is classified as a carbamate substance.81,82,85 Its mechanism of action is a slow reversible or pseudo-irreversible inhibition of both AChE and BuChE.85,96,97 The oral bioavailability is poor, approximate 40% with Tmax ranging from 0.5 to 2 hours following oral single-dose administration.88,98 Plasma protein binding is 40% and Vd is 1.8–2.7 L/kg.88,99,100 Rivastigmine easily passes through the BBB to exert activity in the brain.101,102 Intestinal esterase is the major enzyme responsible for first pass metabolism and the rest is minimally metabolized by liver cytochrome P450.88 The main metabolite is NAP 226–90 which is rapidly excreted by renal system.88 The plasma clearance of rivastigmine is estimated to be 1.5 L/h/kg. Its half-life is short, nearly 1.5 hours. Therefore, twice-daily dosing is recommended in clinical practice.88,100 Several double-blind controlled studies showed significant improvement in cognitive and global functions with 6 month-treatment.103,104 Clinical studies pointed out the effective doses of rivastigmine to be 6 to 12 mg per day.64,105 Rivastigmine is recommended to start at the dose of 1.5 mg twice-daily as capsules or liquid formulations and slowly titrate up to 6 mg twice-daily at intervals of every 2 to 4 weeks.81,103 In terms of other efficacy of rivastigmine, the improvement of peripheral insulin resistance has not been reported.106 Transdermal patch is another preparation which delivers rivastigmine constantly into the blood circulation without level fluctuation.71,97,107 The therapeutic dose of transdermal patch delivering rivastigmine is 4.6 mg per 24 hours to 13.3 mg per 24 hours in clinical practice.107,108 Rivastigmine patch is suggested to be started at 4.6 mg per 24 hours for at least for 4 weeks and then to be increased to 9.5 mg per 24 hours. After a minimum of 6 months a dose of 9.5 mg per 24 hours, 13.3 mg per 24 hours is recommended for well-tolerated patients with progressive cognitive decline.109
Galantamine
Galantamine was approved by the FDA in 2000 for the treatment of AD.110 This agent is a tertiary alkaloid-based compound that acts as both rapidly reversible-competitive inhibitor of AChE and a positive allosteric modulator of nicotinic acetylcholine receptors.62,85,110 The oral bioavailability of galantamine ranges from 85 to 100% with rapid absorption.88,111 The Tmax is approximately 52 minutes following a single oral administration. Unlike donepezil, protein binding of galantamine is less than 50% and the mean Vd is 2.64 L/kg.88,111 This medication is demethylated and oxidized by CYP2D6 and CYP3A4. The active metabolite of galantamine is sanguinine or O-desmethyl galantamine.88,112 Galantamine goes through glucuronidation forming a water-soluble metabolite which is excreted via the renal route.88,111,112 The total plasma clearance of galantamine is 0.34 L/h/kg.113 Due to its short half-life of 6–8 hours, twice-daily dosing is recommended.88,111,113 The formulation of galantamine consists of both immediate-release tablets and extended-release capsules. The efficacy of both extended and immediate release tablets of galantamine was studied in a randomized, double-blind, placebo-controlled trails, using doses titrating up to 16 or 24 mg per day for 6 months duration of treatment in patients with mild to moderate AD.104,114,115 These studies demonstrated a significant improvement in cognitive and neuropsychiatric scales.114 The recommended therapeutic dose of galantamine is 8 mg per day and gradually escalates every 4 weeks up to a maximum daily dose of 24 mg.116
Therefore, the safety and effectiveness of AChEIs should be evaluated in older population in whom adverse reactions may be serious.117 In terms of efficacy and effectiveness assessment of AChEIs, the common tools for cognitive evaluation includes Mini-Mental-State Examination (MMSE),118 Alzheimer’s Disease Assessment Scale-Cognitive subscale (ADAS-Cog),119 and Severe Impairment Battery (SIB).120 Other tests are used to measures functional status and psycho-behavioral symptoms are the Basic and Instrumental Activity of Daily Living121–123 and Neuropsychiatric inventory (NPI),124 respectively. According to previous clinical practice guideline based on systematic reviews,104,125,126 AChEIs treatment for dementia contributed to marginally significant improvement of cognitive function, functional and global status, and psycho-behavioural symptoms.117,125,127 In mild to moderate AD patients, meta-analyses on AChEIs have revealed the results with cognitive improvements on 1.5 points in MMSE and 2.5 points in ADAS-cog, comparing to the placebo.19 The Pooled data presented an improvement of 0.1 standard deviations of ADLs104,125 and 2 of 144 points in NPI.128 Besides cognitive and behavioural improvement, AChEIs have positive effects on balance and gait function without orthostatic hypotension.129 However, there is limited evidence of AChEI efficacy and effectiveness in severe dementia, advanced age and long-term treatment.19,130,131
Adverse Drug Reactions of Acetylcholinesterase Inhibitors
The prevalence of AChEI-induced ADRs tends upward significantly in older population with dementia.48 In a 16-year period study, the number of AChEI-induced ADRs increased from 1924 ADRs in 1998 to 2961 ADRs in 2013.48 Most reported cases are serious ADRs (50–70%) of which 2.3% are fatal ADRs.48–50 AChEIs have a dose-related toxicity and a narrow therapeutic index. Therefore, the prevalence of ADRs has an upward trend with an increasing dose.48 Most ADRs of AChEIs are described as type A reactions which are associated with dose and altered PK and PD. However, most type A reactions are potentially preventable In a recent study, preventable ADRs from prescription and administration errors were presented in 2.0% of all serious cases.48 According to the mechanism of AChEI action, overstimulation of central and peripheral muscarinic and nicotinic receptors may contribute to diarrhea, nausea, vomiting, vagotonic effects (bradycardia, heart block, syncope), tremor, insomnia, urinary incontinence, and seizure.63,132–135 Common ADRs induced by AChEIs are principally neuropsychiatric (17%), gastrointestinal (16.2%), and cardiovascular (11.2%) in nature49 as a result of overstimulation of peripheral cholinergic activity and muscarinic receptor activation, as revealed in Supplementary Table 2.48,72,83,132,133
Gastrointestinal Adverse Effects
Oral administration of AChEIs increases gastric acid secretion of hydrochloric acid and internal propulsion which lead to the increase of gastrointestinal adverse effects, namely gastrointestinal ulceration and bleeding, especially for the concomitant use of AChEI and NSAIDs.136,137 Commonly reported gastrointestinal adverse effects are abdominal pain, nausea, vomiting, diarrhea, and poor appetite.72,133,138–141 The increase of gastrointestinal side effects is associated with the rapid escalation of AChEI dose.142
Cardiovascular Adverse Effects
Both conduction and sinus node function gradually deteriorate with advanced age. Moreover, AChEI increases the availability of choline in the heart and vagotonic effects via muscarinic receptors.143,144 Cardiovascular side effects are some of the most common peripheral adverse cholinergic effects. Therefore, older adults treated with AChEIs are at greater risk of life-threatening conduction dysfunction such as sinoatrial and atrioventricular block,140,145,146 severe sinus bradycardia147 and QT interval prolongation with torsades de pointes (TdP).148–150 Wandering atrial pacemaker (WAP) is another uncommon cardiac side effect in patients treated with donepezil. This condition is an atrial arrhythmia which presents with at least three distinctly different P wave morphologies.151 Negative chronotropic effects contribute to detrimental health outcomes including syncope, pacemaker insertion, falls, fractures, hospitalization.147,152–154 However, there is controversy that AChEIs result in negative chronotropic effects.155–158 Therefore, older people receiving AChEIs should be routinely asked regarding syncope histories and be evaluated for arrhythmia or bradycardia by physical examination and electrocardiogram.159 Concomitant use of AChEIs and drug-induced QT prolongation such as beta-blockers, antiarrhythmic drugs and antipsychotics should be closely monitored by physicians and pharmacists.159 In contrast, AChEIs treatment may be correlated with lower risk of cardiovascular events.158
Neurological and Psychological Adverse Effects
Neurological side effects mainly result from excessive activation of nicotinic receptors. Common neurological adverse effects are dizziness, dyskinesia, convulsion, muscle cramps, insomnia, and vivid dream. The epileptic seizure is a very rare neurological adverse effects induced by AChEIs.160,161 From previous report, patient with mild AD treated with 10 mg donepezil once daily for 3 weeks presented convulsions during the treatment.160 Moreover, AChEI-induced seizures may result from nutritional and metabolic disorders such as hyponatremia.161 The vivid dream results from the disorder of brainstem cholinergic systems in processing rapid eye movement sleep. One characteristic of the vivid dream is extremely realistic. Vivid dreams usually appear in patients treated with donepezil in the evening owing to peak plasma concentration at night.63,162 Psychiatric adverse outcomes in older adults treated with AChEIs may include worsening of hallucination, anxiety, aggression, and confusion.163,164 Psychiatric problems are usually presented in dementia patients treated with high doses of AChEIs.
Respiratory Adverse Effects
Bronchospasm was presented as a pulmonary side effect after AChEI administration.165 Therefore, patients with a history of bronchoconstriction should be closely monitored during treatment.165 Furthermore, nasal problems could be presented among patients treated with AChEI.165 There is no report of respiratory failure from AChEIs for dementia treatment.
Genitourinary Adverse Effects
Urinary incontinence may occur after treatment with AChEIs, in particular for galantamine.166 The mechanism is related to nicotinic Ach receptor stimulation at the neuromuscular junction, resulting in an increased peripheral ACh.
Dermatological Adverse Effects
Rivastigmine could be used in the form of a skin patch. The most common skin adverse reaction is irritant contact dermatitis as a local skin reaction which is not associated with an immunological process. Its manifestation is localized erythema and itching.167,168 These symptoms usually resolve within 48 hours after patch removal. As a rare dermatological adverse reaction, allergic contact dermatitis is delayed type-IV immunologic reaction and manifests as erythema, vesicles and edema appearing more than 48 hours after rivastigmine patch removal. The life-threatening skin adverse reaction called Stevens-Johnson Syndrome (SJS) can occur in patients treated with oral or dermal administration and was reported in patients treated with galantamine.138,167–169
Uncommon Adverse Effects
According to post-marketing surveillance, a rare dystonic reaction called Pisa syndrome has been reported in patients receiving AChEIs. This syndrome is described as tonic flexion of the head and trunk one side accompanied by slight axial rotation.170 The pathophysiology of the syndrome results from dopaminergic-cholinergic imbalance. Pisa syndrome was reported in a patients receiving 9 mg per day rivastigmine for 2 years.171,172 However, this abnormal syndrome disappeared when the drug dose was decreased.171 Rhabdomyolysis and neuroleptic malignant syndromes are uncommon side effects which have been reported in older adults receiving donepezil.173–175 Furthermore, hemolytic anemia, syndrome of inappropriate antidiuretic hormone (SIADH),161 and severe hepatitis176 also present as uncommon adverse effects in clinical practice.
AChEI-induced adverse effects may provide chance for prescribing cascades. AChEIs activate muscarinic receptors in urinary tract, leading to strong contraction of detrusor muscle and urinary incontinence. Therefore, bladder anticholinergic agents such as oxybutynin, tolterodine, trospium and solifenacin are usually used to relieve urge incontinence which called AChEI-induced urinary incontinence prescribing cascade.177 Another common prescribing cascade is AChEI-induced rhinorrhea which is concomitant use of rhinorrhea medications to relieve side effects of AChEIs. The rhinorrhea medications consist of antihistamine, nasal anticholinergics and nasal glucocorticoids.178 These co-medications may contribute to negative side effects. Therefore, physicians should consider dose reduction of AChEIs instead of adding other medications to treat adverse effects of AChEIs.179
Factors Associated with Adverse Drug Reactions of Acetylcholinesterase Inhibitors in Older Adults with Dementia
In geriatric patients with dementia, changes in PK and PD are major risk factors of ADRs. In terms of PK, hepatic and renal functions usually decline in these patients, resulting in decreased drug elimination. Older patients are vulnerable to get an uneventful ADRs from these medications according to their sensitivity to the pharmacodynamic effects.180 Additionally, patients with AD are prone to be sensitive to ADRs as a result of increased BBB permeability and decreased P-gp activity in the brain.43,101,102,181,182 Polypharmacy is common in aging populations and is an important risk factor for drug-related problems (DRPs) such as potentially inappropriate medications (PIMs), drug–drug interactions (DDIs), ADRs and poor compliance.183,184 ADRs derived from DDIs, PIMs or poor compliance are often reported in older patients with dementia.183,184 ADRs are major causes of hospitalization, morbidity and mortality in older people with dementia.185,186
Changes in Pharmacokinetics
PK is what an individual’s body does to a medication after its administration, and refers to absorption, distribution, metabolism and excretion.42–47 In geriatric population, the alteration of absorption does not lead to major adverse effects whereas changes in distribution, metabolism and excretion play important roles in clinical outcomes. The alterations of PK and PD of AChEIs among older people living with dementia were presented in Tables 1 and 2.
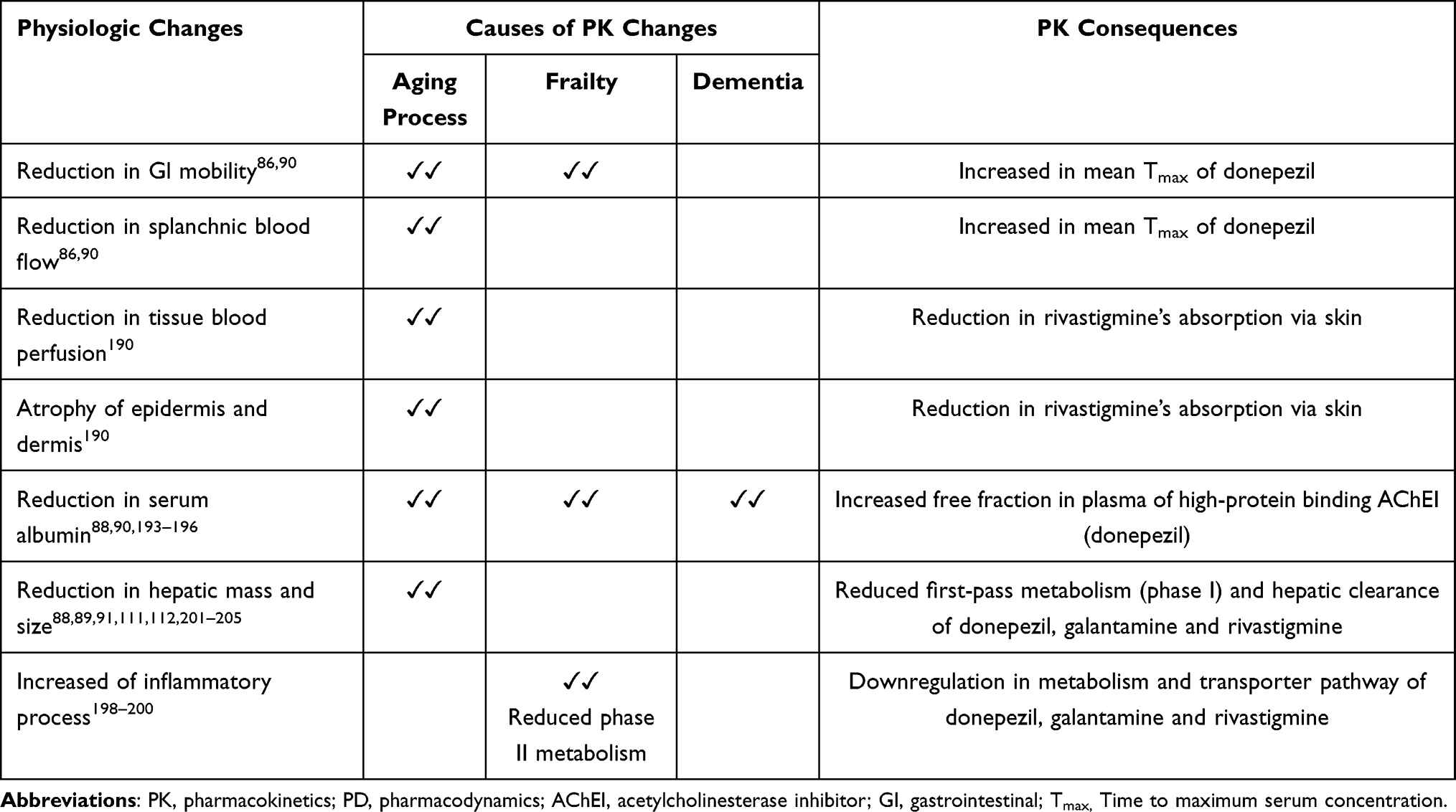 |
Table 1 The Changes in Pharmacokinetics of Acetylcholinesterase Inhibitors Among Older Adults Living with Dementia |
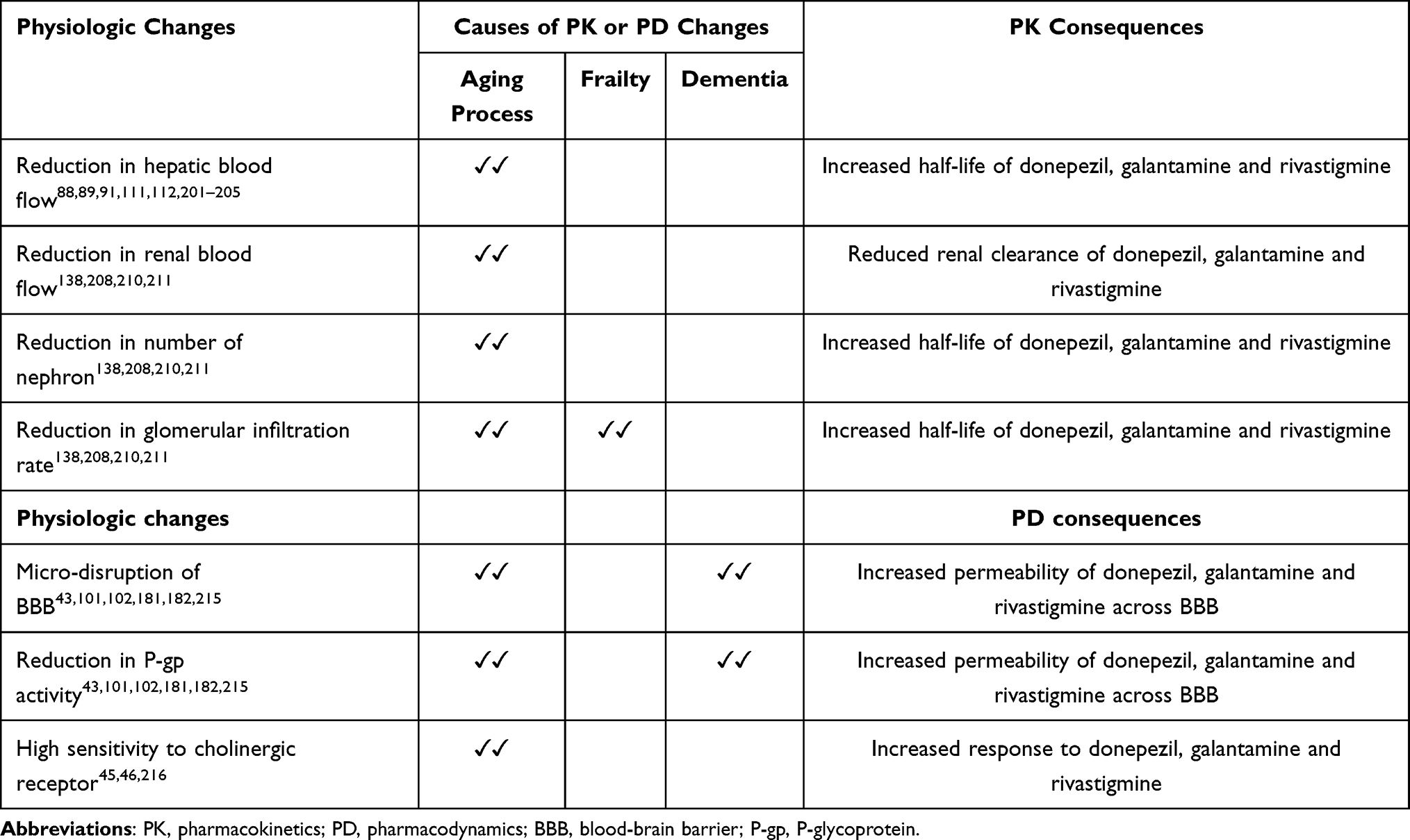 |
Table 2 The Changes in Pharmacokinetics and Pharmacodynamics of Acetylcholinesterase Inhibitors Among Older Adults Living with Dementia |
Absorption
Age-related gastrointestinal tract changes often affect the oral absorption. Hypochlorhydria in older adults alleviate the degree of absorption of weakly basic drugs. Furthermore, reduced splanchnic blood flow and gastrointestinal motility as well as delayed gastric emptying time result in longer staying of drug in the gastrointestinal tract and delaying absorption of the drug. Older adults treated with donepezil presented a significant increase in mean Tmax but not in plasma level concentration contributing to slower donepezil’s absorption.86,90 In contrast, the bioavailability and absorption of rivastigmine have no significant change with advancing age.187 Concomitant administration of galantamine with food delays Tmax by 1.5 hours and slows its absorption rate but does not affect the extent of absorption.74 A moderate food effect was found in previous studies of rivastigmine.54 Food slows the absorption of rivastigmine and reduces Tmax by 30%.54,188 Therefore, the coadministration of food and galantamine or rivastigmine is indicated to reduce cholinergic adverse effects such as nausea and vomiting. Conversely, food intake has no significant effect on the absorption of donepezil.54,189
Rivastigmine could also be administered via a skin patch. Age-related changes in skin includes atrophy of epidermis and dermis and decreased blood perfusion, leading to reduced drug absorption via the skin.190 Nevertheless, age-related changes to drug absorption have minimal effects on the pharmacotherapy of dermal medications.
Distribution
Many factors affect volume of distribution. Patients with dementia are more likely to experience malnutrition and frailty as a result of inability to feed by themselves, changes in feeding behaviours, and difficulty with swallowing.191 Changes in the body composition of older adults with dementia also occur including, 10–15% reduction in total body water, 25–30% reduction in muscle mass, and a 25–30% relative increase in body fat.192,193 The aging and frailty processes in this group of patients also contributes to a 10–20% reduction in serum albumin concentration which plays a major role in plasma protein binding.193–196 Medication that predominately binds albumin such as donepezil (75% bind to albumin), a reduction in albumin binding may contribute to the rising of unbound fraction being pharmacologically active, resulting in greater potency and toxicity.88,90 Furthermore, donepezil may displace other high-protein binding medications such as warfarin, benzodiazepine and valproate, leading to an increased unbound form of these medications and serious adverse effects. Due to age-related changes, the Vd throughout the whole body of donepezil is substantially increased by approximately 40%, resulting in a prolonged half-life.90,197
Metabolism
Liver CYP enzymes system plays a major role in drug metabolism and may be affected by increasing age. CYP2C19 functions are reduced with age while other isoenzymes show minimal reduction or no change.45 In contrast, there is no significant change in phase II metabolism, especially conjugation in older adults. However, phase II metabolism and downregulation of the transporter pathway of AChEIs are decreased in frail older adults, leading to a greater risk of drug toxicity.198–200 The decrease of drug metabolism in the geriatric population, especially in phase I metabolism, results from a 30% and 40% reduction in liver mass and in hepatic blood flow, respectively.201–205 The reduction in drug metabolism may account for decreased hepatic clearance, prolonged half-life and increased dose-dependent ADRs. In terms of AChEIs, there are diverse pharmacological properties and differences of clinical outcomes. Data from clinical trials of geriatric patients with AD reveal that the steady-state concentrations of galantamine are 40% higher than those in a healthy younger population as a result of reduced galantamine’s metabolism.88,111,112,138 Based on a population pharmacokinetic analysis, the hepatic clearance of donepezil and of rivastigmine has a tendency to decrease with increasing age.88,89,91,187 Apart from age-related changes in metabolism, most older adults with dementia have multiple chronic diseases including hepatic diseases or cirrhosis, which may lead to decreased hepatic function and drug metabolism. The clearance of both galantamine and rivastigmine was reduced by 25% and 65%, respectively in patients with moderate hepatic impairment (Child-Pugh score of 7–9).88,111,121 Hence, dose adjustment is recommended for these populations. The use of galantamine for such patients should be initiated with a low dose (4 mg per day) and slowly titrated to a maximum daily dose (16 mg per day).88,111,138 However, no data is available on the use of galantamine or rivastigmine in patients with severe hepatic impairment (Child-Pugh score of 10–15).88,111,112,138 Consequently, the use of galantamine or rivastigmine in patients with severe hepatic impairment is contraindicated in clinical practice.138 A recent study showed a 20% reduction in the clearance of donepezil in dementia patients with cirrhosis.206 However, there is no clinically significant alteration in the PK of donepezil in AD patients with moderate or severe hepatic impairment.206,207 This may explain why dose modification of donepezil is not required.
Excretion
After metabolism, most substances are transformed to products that are readily excreted via the kidneys. As a results of age-related physiological changes, the reduction in renal blood flow (50%), renal mass and size (20–30%), and number of nephrons (60%), lead to a decline in drug excretion and drug half-life prolongation.208 Apart from metabolism changes, dosage adjustment should be done based on renal function which is calculated from laboratory measurement (serum creatinine) by using a mathematical equation including the Cockcroft-Gault (CG) formula to ensure proper drug dose for older adults.45,46,209 However, serum creatinine level in older frail individuals may not accurately present renal function because of decreased muscle mass.209 Older AD patients presented a 30% reduction in renal clearance of galantamine, compared with healthy individuals.210 As a consequence of increasing age and frailty, the clearance rate of galantamine, rivastigmine and donepezil in older patients with AD is reduced, compared to healthy individuals.138,210 The clearance of galantamine and rivastigmine is decreased by 25% and 64%, respectively in AD patients with moderate renal impairment.138 This PK alteration may necessitate dose modification and close monitoring to avoid adverse outcomes.138 A total daily dose of galantamine should not exceed 16 mg in patients with moderate renal decline or creatinine clearance 9–59 mL/min138 whereas specific-dose adjustment of rivastigmine is not indicated.211 Nevertheless, the use of galantamine is not recommended given the insufficient data for patients with severe renal impairment or creatinine clearance less than 9 mL/min.138 On the contrary, donepezil disposition is not affected by renal dysfunction. The renal clearance of donepezil in patients with moderate to severe renal impairment has no difference to sex- and age-matched healthy population despite donepezil and its metabolites are mostly excreted by kidneys. In a population pharmacokinetic study of AD patients with moderate to severe renal impairment, there is no clinically significant change of PK or PD parameters of donepezil, compared with healthy population. Therefore, dose adjustments are not necessary in AD patients with renal impairment.64,207
As a result of decreased elimination of rivastigmine, dose adjustments with close monitoring should be done. Nevertheless, no study has been reported for rivastigmine transdermal patches in AD patients with renal or hepatic impairment. Therefore, rivastigmine transdermal patches should be avoided in AD patients with severe renal or hepatic impairment.107,108
Changes in the Blood-Brain Barrier
The BBB is a highly selective semipermeable layer of endothelial cells which limits the access of water-soluble and large molecules transporting from blood circulation into the brain parenchyma. Older adults with dementia have changes in the permeability and integrity of the BBB, as presented in Table 2. BBB mechanism includes reabsorption of CSF and efflux pumps for molecules such as p-glycoprotein (P-gp) which assists the maintenance of hemostasis in the brain and in the clearance of beta-amyloid.43,101,102 P-gp is a phosphorylated protein encoded by multidrug resistance gene 1 (MDR1) and belongs to the family of ATP-binding cassette (ABC) membrane transporters.102,212 It is located on the apical surface of endothelial cells and is involved in limiting the transfer of small molecules into the brain.213,214 With aging process and dementia, levels and activity of P-gp have a tendency to decline.101,102,181,215 Furthermore, micro-disruption of the BBB is found in patients with dementia, contributing to increased allowance of some medications across BBB around the disruption areas.181 These changes may lead to increased permission of AChEIs to the brain as a predisposing factor of AChEI-induced ADRs in this population.43
Changes in Pharmacodynamics
By definition, PD is described as what medication does to the body such as receptor binding and chemical interaction.42–47 The changes of PD are difficult to predict and evaluate in individuals. In the aging process, the sensitive affinity of receptors for particular medications may change. Moreover, the number of receptor sites may alter and may impact on the efficacy of many medications. The geriatric population is more susceptible to certain central nervous system (CNS) adverse outcomes of AChEIs due to increased permeability of the BBB and decreased P-gp activity.101,102,181,182,215 Furthermore, high sensitivity to cholinergic receptors in the brain and the reduction in homeostasis are found in the older adult population.45,46,216 These alterations result in an elevated responses to AChEIs and contribute to PNS and CNS cholinergic ADRs, as presented in Table 2. However, changes in the PD of AChEIs in older patients with dementia have not been extensively explored.
Changes in Pharmacogenetics
Pharmacogenetics is defined as genetic variations in individuals which contribute to different responses to medications. PGx plays a major role in ADRs and therapeutic failures (TFs). Polymorphism of CYP enzymes for AChEIs results in PK and PD difference.84,217 In terms of AChEIs, PGx of encoded gene on P-gp, CYP2D6, and CYP3A4 plays an important role in PK of donepezil and galantamine.218 Interesting studies presented genetic variations of single nucleotide polymorphisms (SNP) in cholinergic markers on AChE and BuChE which have effects on clinical responses to AChEIs as well.82,219 Moreover, polymorphism in the gene encoding choline acetyltransferase (ChAT), acetylcholine biosynthetic enzyme, and a genetic variation of paraoxonase-1 (PON-1) 192Q/R (rs662) which influences the activity of this arylesterase, are involved as the prognostic indicators of response to AChEIs.220,221 Pharmacogenetic considerations for AChEIs should be heeded because they could help predict drug toxicity and efficacy in individuals. In recent decades, genetic polymorphism on CYP2D6 genotype was increasingly studied in various populations.222–225 CYP2D6 phenotypes are categorized into four types of metabolizers: Poor metabolizers (PMs), intermediate metabolizers (IMs), extensive metabolizers (EMs), and ultra-rapid metabolizers (UMs). PMs have functional deficiency of CYP2D6 due to mutated allele of CYP2D6. EMs have normal functions of CYP2D6 while UMs have a very low concentration of AChEI owing to multiple copies of CYP2D6 gene. IMs metabolize medications with a rate between PMs and EMs.222,223,225 According to PGx of CYP2D6 (PGX-CYP2D6), approximately 30% of older AD patients have poor metabolite of galantamine and donepezil.226 This situation can be explained by the phenotypic profile of CYP2D6 genotypes being associated with the presence of the APOE-4 allele.227–229 Furthermore, the prevalence of each CYP2D6 polymorphism differs according to race and ethnicity.84,230 In Caucasian populations, PMs, IMs, EMs and UMs account for approximately 5–10%, 10–17%, 70–80% and 3–5% of individuals, respectively.231,232 Asians, Africans and African Americans have a greater percentage of reduced-function of CYP2D6 (50%), compared with Caucasians (26%).233 CYP3A4 polymorphism is not responsible for the variation in metabolism of donepezil and galantamine. The effect of genetic variation in ATP-binding cassette sub-family B member 1 (ABCB1) on membrane transporter P-gp plays an important role in donepezil transporters across the BBB and in the clearance of amyloid β (Aβ) peptide related to APOE, ABCB1 gene polymorphisms which have an impact on distribution, excretion, and absorption of donepezil.102,212,234,235
Drug–Drug Interactions
DDI is defined as the pharmacological activities of one drug changed by the concomitant administration of another medication.236 Generally, drug interactions are responsible for 20% to 30% of ADRs. Over 30% of reported ADRs caused by AChEIs result from DDIs.237 The major risk factors for DDIs are polypharmacy and age-related PK and PD changes.238,239 DDIs are classified into two types: PK and PD drug interactions. By definition, PK drug interaction involves one medication altering the absorption, distribution, transport, metabolism or excretion of another medication.240 PD drug interaction is defined as one medication changing the response to another medication.240 CYP enzymes-mediated and transporter-mediated PK drug interactions as well as synergistic or antagonistic PD drug interactions are common DDIs among dementia patients treated with AChEIs.241–243 Inducers and inhibitors of CYP2D6 and CYP3A4 enzyme play important roles in the mechanism of PK drug interactions of donepezil and galantamine.226,244 P-gp inducers and inhibitors are involved in transporter-mediated PK drug interactions of donepezil, which is considered a weak P-gp substrate.245
Potent CYP2D6 and CYP3A4 inhibitors such as antidepressants (paroxetine, fluoxetine), and antifungal drugs (ketoconazole) contribute to increased plasma concentration of donepezil and galantamine, as shown in Table 3.138,242,246–249 The adverse outcomes may be hypercholinergic effects of AChEIs, such as bradycardia, diarrhea and hypersalivation. However, there is no significant CYP2D6 and CYP3A4 inducers of donepezil and galantamine. In terms of transporter-mediated PK drug interactions, PK of donepezil is affected by P-gp inhibitors and inducers. Most medications, which are transported by P-gp, are also metabolized by CYP3A4.214,245,250 Many P-gp inhibitors and inducers are also inhibitors and inducers of CYP3A4. Therefore, many DDIs are associated with inhibition or induction of both CYP3A4 and P-gp.250 The most common P-gp inhibitors in patients with dementia are antibiotics (azithromycin, clarithromycin, erythromycin), cardiovascular medications (carvedilol, verapamil) and antiplatelets (cilostazol, ticagrelor), resulting in the rising of donepezil plasma concentration.250–252 There was the clinical report of cardiotoxicity owing to coadministration of donepezil and cilostazol.252 Due to P-gp interaction with cilostazol, the concentration of donepezil in the heart tissue was increased, leading QT prolongation.252 In the case of P-gp inducers, the plasma concentration of donepezil is decreased by carbamazepine, phenobarbital, phenytoin and rifampicin,250–252 as presented in Table 4.
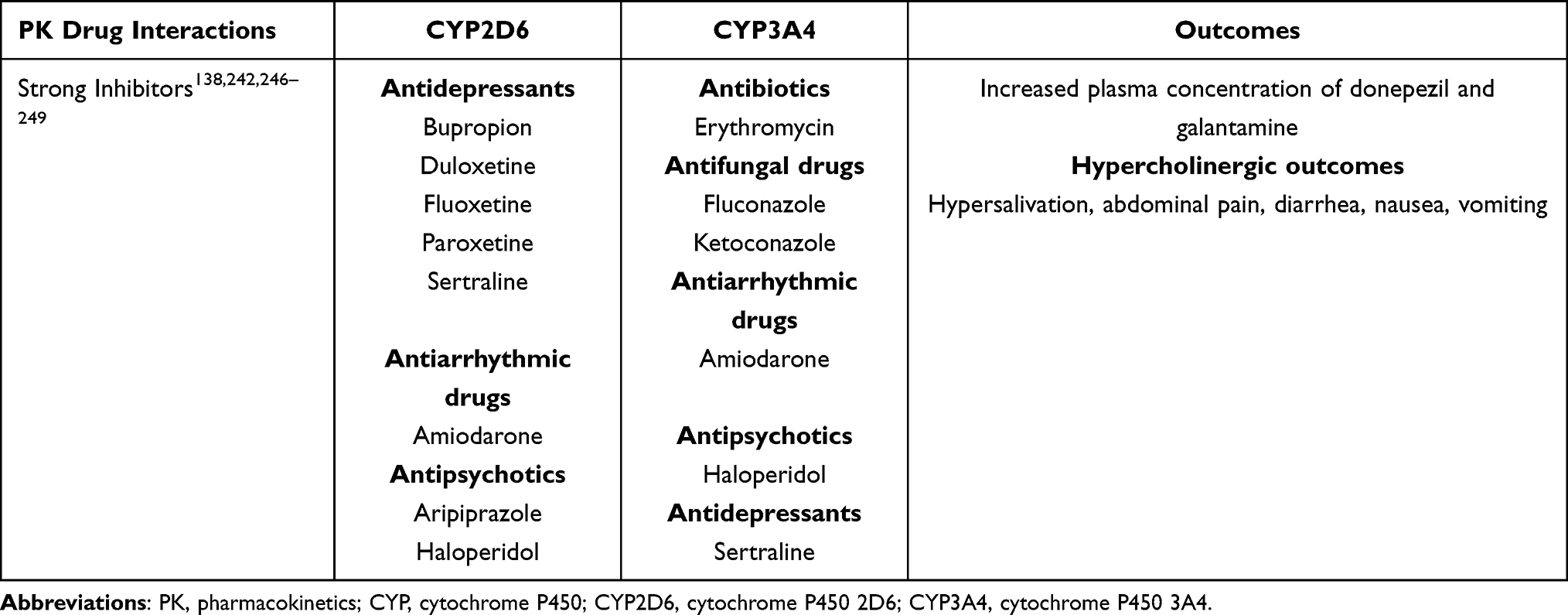 |
Table 3 Common CYP Enzymes-Mediated Pharmacokinetic Drug Interactions of Acetylcholinesterase Inhibitors in Older Adults Living with Dementia |
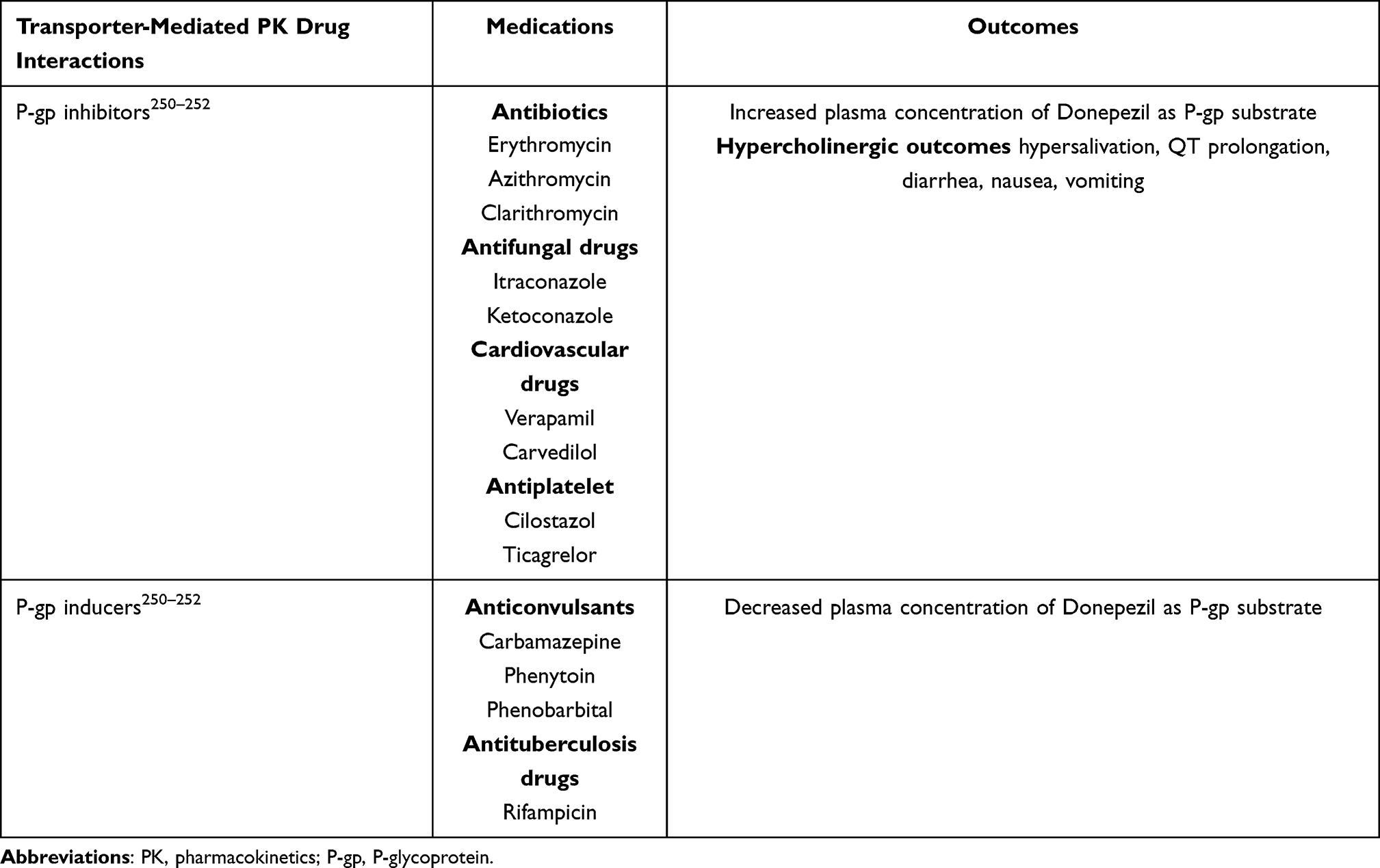 |
Table 4 Common Transporter-Mediated Pharmacokinetic Drug Interactions of Acetylcholinesterase Inhibitors in Older Adults Living with Dementia |
Pharmacoepidemiological studies in people with dementia have revealed that anticholinergics, antidepressants, antipsychotics, non-steroidal anti-inflammatory drugs (NSAIDs), and cardiovascular drugs are common co-medications with AChEIs, resulting in PD drug interactions.237,243,253,254 Synergistic PD drug interactions of AChEIs with cholinomimetics or cholinergic agonists have additional cholinergic effects such as hypersalivation, diarrhea, nausea, and vomiting, as presented in Table 5.255–257 Many antagonistic PD drug interactions of AChEIs are related to changes in PD from advancing age and to dementia processes. In the aging process, a reduction in the number of cholinergic and dopaminergic neurons and dopamine D2 receptors are reported. Therefore, the uses of anticholinergics and antipsychotics which affect cholinergic and dopaminergic neurotransmitters, potentially interfere with the activity of cholinesterase inhibitors and can cause adverse clinical outcomes.253,254,258,259 The clinical report described rigidity, parkinsonism and immobilization in AD patients treated with donepezil and risperidone which these adverse symptoms resolved after risperidone was discontinued.260 Furthermore, concomitant use of beta-blockers, calcium channel blockers or antiarrhythmics in older patients with dementia treated with AChEIs may result in adverse cardiovascular effects such as bradyarrhythmia, heart block, syncope and QT prolongation,63,243,261 as presented in Table 5.
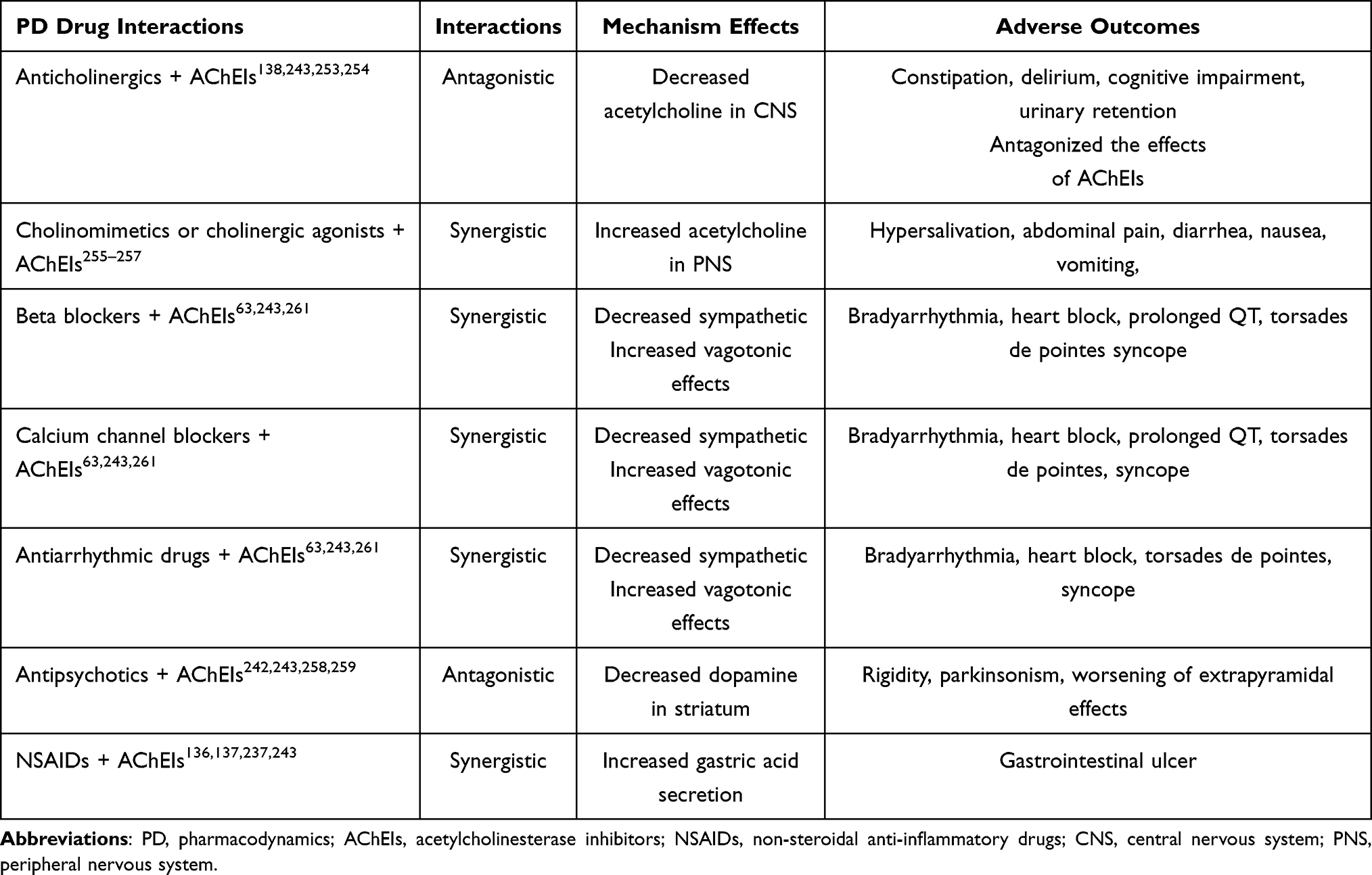 |
Table 5 Pharmacodynamic Interactions in Older Adults with Dementia |
Principles for Prescribing Acetylcholinesterase Inhibitors
Recommendations for Prescribing Acetylcholinesterase Inhibitors
AChEI should be initiated at a low efficient dose and titrated slowly upward. The starting dose of donepezil is 5 mg once daily. Donepezil dosage should not be adjusted too quickly because the time to reach the steady state is within 15 days. Therefore, donepezil should be slowly titrated after the first dose is started over 4–6 weeks. Older adults with moderate to severe AD could slowly titrate the donepezil dose to 23 mg per day,262 as presented in Supplementary Table 1. However, gastrointestinal complaints and poor appetite may be reported in patients receiving high donepezil doses.75,139,262,263 Among patients with mild to moderate hepatic insufficiency, a low dose (5 mg daily) consumption of donepezil is safe and the use of its doubling dose should be monitored.264 Galantamine is a daily oral medication ranging from 8 to 24 mg per day,116 as shown in Supplementary Table 1. Galantamine doses must be adjusted for people with moderate hepatic impairment. Furthermore, galantamine should not be recommended to patients with severe liver and kidney dysfunction. Rivastigmine may be a good choice for older demented patients exposed to polypharmacy to reduce the incidence of PK drug interactions related to CYP enzymes. Rivastigmine prescriptions start at 1.5 mg and could be gradually increased to 6 mg twice a day,64,81,103,105 as shown in Supplementary Table 1. Rivastigmine transdermal patches are usually recommended for dementia patients with severe gastrointestinal side effects from oral administration. Transdermal patches have a long half-life and are easily applied only once a day. The dose of rivastigmine in a patch can be titrated from 4.6 mg per 24 hours to 13.3 mg per 24 hours.107–109 However, some patients treated with a transdermal patch may develop dermatological side effects such as pruritus or an allergic reaction. Therefore, patients should be examined for adverse skin reactions during treatment.108
Contraindication and Caution in the Prescribing of Acetylcholinesterase Inhibitors
Allergic reaction to the medication itself and chemicals in the same structural group is an absolute contraindication. Donepezil is a piperidine-based compound.81,82,85 Rivastigmine is derived from carbamate compound whereas galantamine is belonged to alkaloid substance.62,81,82,85 Rivastigmine patches are contraindicated for patients with suggestive allergic contact dermatitis.107–109 Galantamine is also contraindicated for patients with severe hepatic and renal dysfunction.212 Additionally, patients with sick sinus syndrome (SSS) and second or third heart block should avoid using AChEIs.138,140,141 AChEIs should be used with cautions in people with severe hepatic impairment, severe obstructive pulmonary disease, active gastrointestinal ulcers or bleeding, seizure and significant conduction abnormalities such as supraventricular conduction problems, and arrhythmias.138,140,141 However, older patients treated with AChEIs rarely develop cholinergic crisis in the clinical practice.
Recommendations for Discontinuation of Acetylcholinesterase Inhibitors
The continuous use of AChEIs should be often weighted the risks and the benefits. According to the Food and Drug Administration Adverse Event Reporting System database, serious ADRs related to AChEIs were reported, especially in long-term treatment.135,136,179,213,265,266 Advanced dementia patients may be offered unnecessary treatment that may not provide positive effects, resulting in increased adverse outcomes.267 Therefore, many studies offered recommendations to discontinue AChEI treatment in particular conditions to optimize medication prescribing.268 The common reason for deprescribing AChEIs were lack of response, significantly impaired functional status, severe cognitive impairment (MMSE score < 10), and side effects.268 Besides minimized medication prescribing, the benefits of AChEI discontinuation are improved medication non-adherence, and reduced DDI, medication management burden and cost of medications.269 The discontinuation of AChEIs should be slowly tapered the dose by halving the previous dose and stepping down to the lowest available dose.269 The abrupt cessation should be done in patients with experiencing ADRs. After discontinuation, physicians should closely monitor the withdrawal symptoms and the changes of cognitive function, psycho-behavioral symptoms and functional status.269
Strategies to Prevent Adverse Drug Reactions of Acetylcholinesterase Inhibitors
Many strategies have been developed and implemented to prevent ADRs in patients using AChEIs, as shown in Table 6. Minimizing effective dose is required to reduce the occurrence of adverse outcomes. The “start low go slow” strategy is widely recommended as the lowest initial dose, slow-dose titration and close monitoring.270,271 The dose adjustment of AChEIs is recommended according to the alteration of PK or PD.47,270,272–275 Furthermore, older patients usually have comorbidities for which multiple medications are taken, resulting in DRPs including potential DDIs, drug–disease interactions, inappropriate medications and medication non-adherence.270,272–274,276 Thus, comprehensive medication reviews and optimizing medications prescribing are necessary to address DRPs.275 Another potential strategy could be using tools such as the Micromedex Drug Interaction Database277 and the 2019 American Geriatrics Society Beers criteria278 to evaluate DDIs and PIMs, respectively.238,279 The discontinuation of AChEIs in older adults with particular circumstances including lack of treatment response, severe cognitive function, significantly impaired functional status, could have reduced DDIs and PIMs.268 Moreover, computerized alert systems for screening prescriptions and flagging DDIs and PIMs could also prevent ADRs.275,280,281 Medication non-adherence is another major DRP in older adults, resulting from language barriers, complex regimens and physiological changes including cognitive impairment, visual and auditory problems and bone-joint deformities.282–286 Many techniques could provide benefits to people with medication non-adherence; for example, readily openable containers, clearly written instructions in large print, the simple possible dosage regimens and supporting technology (alarm clock and drug calendar).287,288
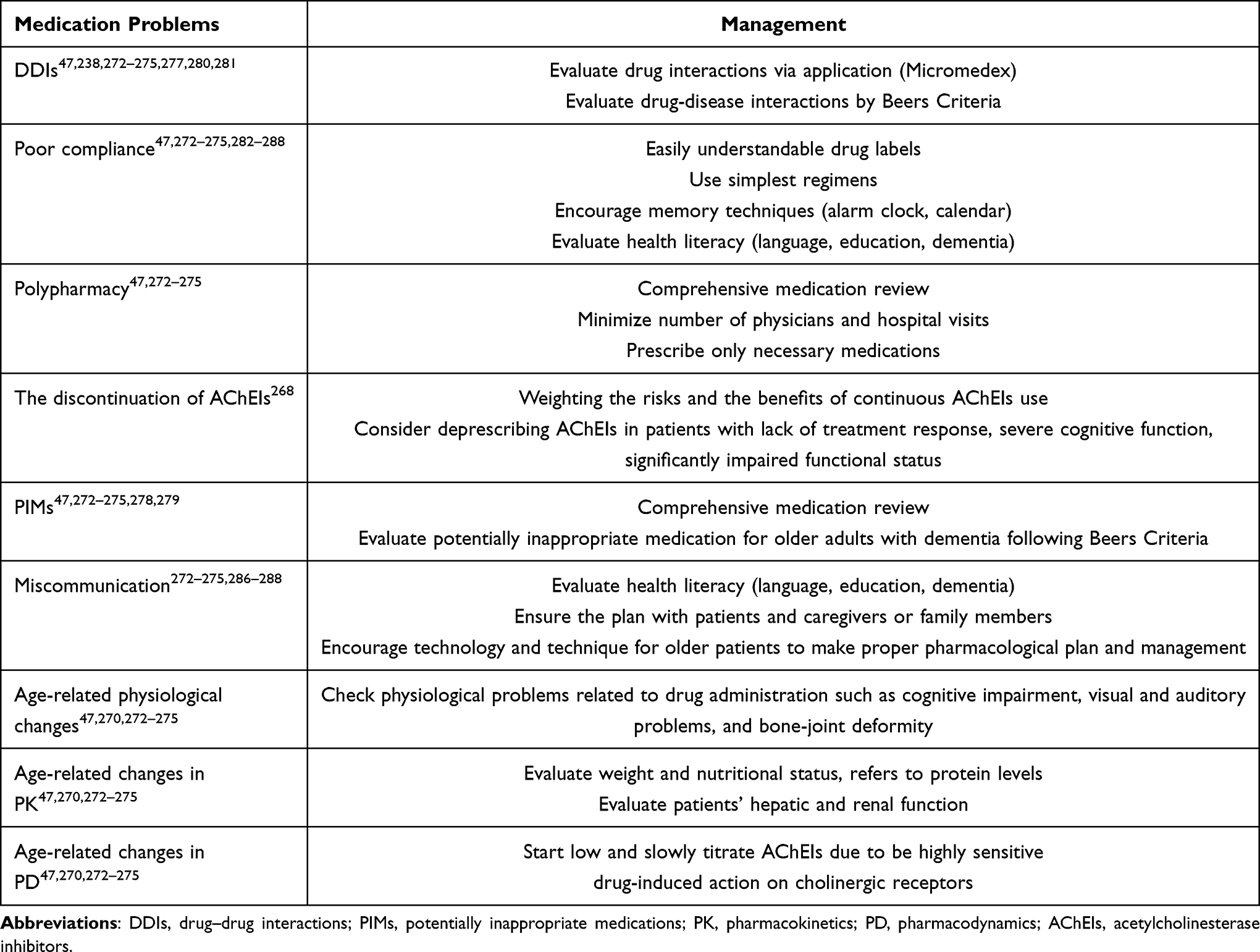 |
Table 6 Prevention Strategies for Adverse Drug Reactions of Acetylcholinesterase Inhibitors |
Conclusions
AChEIs have been widely prescribed to delay worsening of cognitive functions and psycho-behavioral problems in older people living with dementia. In the aging population, age-related PK and PD changes, and multiple comorbidities lead to altered pharmacological responses and increased ADRs. Furthermore, geriatric people are more likely to be sensitive to pharmacological toxicity. The most common negative effects of AChEIs are adverse neuropsychiatric, gastrointestinal, and cardiovascular outcomes. Thus, prescribing of AChEIs for dementia treatment should carefully consider both risks and benefits. The discontinuation of AChEIs in older people with particular circumstances such as lack of treatment response, severe cognitive impairment and side effects, could reduce DRPs. Many strategies have been developed to prevent adverse effects. The “start low go slow” strategy as well as comprehensive medication review are highly recommended to address ADRs.
Abbreviation
ABCB1, ATP-binding cassette sub-family B member 1; Aβ, amyloid β; Ach, acetylcholine; AChE, acetylcholinesterase; AChEIs, acetylcholinesterase inhibitors; AD, Alzheimer’s disease; ADRs, adverse drug reactions; AGS Beers Criteria, American Geriatrics Society Beers Criteria; BBB, blood brain barrier; BPSD, behavioral and psychological symptoms; BuChE, butyrylcholinesterase; CG, Cockcroft-Gault; ChAT, choline acetyltransferase; CNS, central nervous system; CSF, cerebrospinal fluid; CYP, cytochrome P450; CYP2D6, cytochrome P450 2D6; CYP3A4, cytochrome P450 3A4; DDIs, drug–drug interactions; DRPs, Drug-related problems; Ems, extensive metabolisers; FDA, Food and Drug Administration; GI, gastrointestinal; IMs, intermediate metabolisers; MDR1, multidrug resistance gene 1; nAChRs, nicotinic acetylcholine receptors; NMDA, N-Methyl-D-aspartate; NSAIDs, non-steroidal anti-inflammatory drugs; PD, pharmacodynamics; P-gp, p-glycoprotein; PIMs, potentially inappropriate medications; PGx, pharmacogenetics; PGx-CYP2D6, pharmacogenetics of CYP2D6; PK, pharmacokinetics; PMs, poor metabolisers; PNS, peripheral nervous system; PON-1, paraoxonase-1; SIADH, syndrome of inappropriate antidiuretic hormone; SJS, Stevens-Johnson Syndrome; SNP, single nucleotide polymorphism; SSS, sick sinus syndrome; TdP, torsades de pointes; TFs, therapeutic failures; Tmax, time to peak plasma concentration; Ums, ultra-rapid metabolisers; Vd, volume of distribution; WAP, wandering atrial pacemaker; 6DD, 6-O-desmethyl donepezil.
Acknowledgments
The authors would like to thank Leila Shafiee Hanjani, Centre for Health Services Research, Faculty of Medicine, The University of Queensland, for providing valuable advice and comments.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research.
Disclosure
The authors declare no potential conflicts of interest regarding this work.
References
1. World Health Organization. World report on ageing and health. Geneva: World Health Organization; 2015. Available from http://www.who.int/ageing/events/world-report-2015-launch.
2. Wilson T. An introduction to population projections for Australia.Australian Population Studies.2019;3(1):40–56.
3. Prince MJ, Wimo A, Guerchet MM, Ali GC, Wu Y-T, Prina M. World Alzheimer Report 2015; The Global Impact of Dementia: An analysis of prevalence, incidence, cost and trends. London: Alzheimer's Disease International, 2015. Available from: http://www.alz.co.uk/research/world-report-2015. Accessed November 22, 2020.
4. Ahmadi-Abhari S, Guzman-Castillo M, Bandosz P, et al. Temporal trend in dementia incidence since 2002 and projections for prevalence in England and Wales to 2040: modelling study. BMJ. 2017;358:j2856. doi:10.1136/bmj.j2856
5. World Health Organization. Dementia. Geneva: World Health Organization; 2019. Available from: http://www.who.int/news-room/fact-sheets/detail/dementia.
6. Alzheimer’s Disease International. Dementia Statistics. London: Alzheimer’s Disease International; 2017. Available from: https://www.alz.co.uk/research/statistics.
7. ICD-10. Organic, including symptomatic, mental disorders (F00-F09); 2016. Available from: https://icd.who.int/browse10/2016/en#/F00-F09.
8. Dementia Australia 2018a. Types of Dementia. Australia: Dementia Australia; 2018. Available from: https://www.dementia.org.au/information/about-dementia/types-of-dementia.
9. Dementia Australia 2018c. Alzheimer’s disease. Australia: Dementia Australia; 2018. Available from: https://www.dementia.org.au/about-dementia/types-of-dementia/alzheimer-disease.
10. Alzheimer’s Association. 2016 Alzheimer’s Disease Facts and Figures. Alzheimers Dement. 2016;12(4):459–509.
11. Epperly T, Dunay MA, Boice JL. Alzheimer Disease: pharmacologic and Nonpharmacologic Therapies for Cognitive and Functional Symptoms. Am Fam Physician. 2017;95(12):771–778.
12. Australian Institute of Health and Welfare 2012. Dementia in Australia. Cat. no. AGE 70. Canberra: AIHW; 2012. Available from: https://www.aihw.gov.au/getmedia/13995.pdf.aspx.
13. Australian Bureau of Statistics 2019. Causes of Death, Australia, 2019, Catalogue No. 3303.0, ABS. Canberra: Australian Bureau of Statistics (ABS); 2019. Available from: http://www.abs.gov.au/ausstats/[email protected]/mf/3303.0.
14. Winblad B, Amouyel P, Andrieu S, et al. Defeating Alzheimer’s disease and other dementias: a priority for European science and society. Lancet Neurol. 2016;15(5):455–532.
15. Malone DC, McLaughlin TP, Wahl PM, et al. Burden of Alzheimer’s disease and association with negative health outcomes. Am J Manag Care. 2009;15(8):481–488.
16. Sharma S, Mueller C, Stewart R, et al. Predictors of falls and fractures leading to hospitalization in people with dementia: a representative cohort study. J Am Med Dir Assoc. 2018;19(7):607–612. doi:10.1016/j.jamda.2018.03.009
17. The National Centre for Social and Economic Modelling NATSEM (2016) Economic Cost of Dementia in Australia 2016–2056; 2017 Feb. Available from: http://www.dementia.org.au/files/NATIONAL/documents/The-economic-cost-of-dementia-in-Australia-2016-to-2056.pdf.
18. Dyer SM, Harrison SL, Laver K, et al. An overview of systematic reviews of pharmacological and non‐pharmacological interventions for the treatment of behavioral and psychological symptoms of dementia. Int Psychogeriatr. 2017;30(03):
19. Birks J. Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database Syst Rev. 2006;1:CD005593.
20. O’Brien JT, Holmes C, Jones M, et al. Clinical practice with anti-dementia drugs: a revised (third) consensus statement from the British Association for Psychopharmacology. J Psychopharmacol. 2017;31(2):147–168. doi:10.1177/0269881116680924
21. Rabins PV, Rummans T, Schneider LS, et al. Practice Guideline for the Treatment of Patients with Alzheimer’s Disease and Other Dementias.
22. Australian Institute of Health and Welfare 2019. Dispensing patterns for anti-dementia medications 2016–17. Cat. no. AGE 95. Canberra: AIHW; 2019. Available from: https://www.aihw.gov.au/reports/dementia/dispensing-patterns-for-anti-dementia-medications/contents.
23. Calvó-Perxas L, Turró-Garriga O, Vilalta-Franch J, et al. Trends in the Prescription and Long-Term Utilization of Antidementia Drugs Among Patients with Alzheimer’s Disease in Spain: a Cohort Study Using the Registry of Dementias of Girona. Drugs Aging. 2017;34(4):303–310. doi:10.1007/s40266-017-0446-x
24. Moraes FS, Souza MLC, Lucchetti G, Lucchetti ALG. Trends and disparities in the use of cholinesterase inhibitors to treat Alzheimer’s disease dispensed by the Brazilian public health system - 2008 to 2014: a nation-wide analysis. Arq Neuropsiquiatr. 2018;76(7):444–451. doi:10.1590/0004-282x20180064
25. Pariente A, Helmer C, Merliere Y, Moore N, Fourrier-Réglat A, Dartigues JF. Prevalence of cholinesterase inhibitors in subjects with dementia in Europe. Pharmacoepidemiol Drug Saf. 2008;17(7):655–660. doi:10.1002/pds.1613
26. Clague F, Mercer SW, McLean G, Reynish E, Guthrie B. Comorbidity and polypharmacy in people with dementia: insights from a large, population-based cross-sectional analysis of primary care data. Age Ageing. 2017;46(1):33–39.
27. Parsons C. Polypharmacy and inappropriate medication use in patients with dementia: an underresearched problem. Ther Adv Drug Saf. 2017;8(1):31–46. doi:10.1177/2042098616670798
28. Hoffmann F, van den Bussche H, Wiese B, et al. Impact of geriatric comorbidity and polypharmacy on cholinesterase inhibitors prescribing in dementia. BMC Psychiatry. 2011;11:190. doi:10.1186/1471-244X-11-190
29. Kales HC, Gitlin LN, Lyketsos CG. Assessment and management of behavioral and psychological symptoms of dementia. BMJ. 2015;350(mar02 7):h369. doi:10.1136/bmj.h369
30. Masopust J, Protopopová D, Vališ M, et al. Treatment of behavioral and psychological symptoms of dementias with psychopharmaceuticals: a review. Neuropsychiatr Dis Treat. 2018;14:1211–1220. doi:10.2147/NDT.S163842
31. Gabryelewicz T. Pharmacological treatment of behavioral symptoms in dementia patients. Przegl Lek. 2014;71(4):215–220.
32. Andersen F, Viitanen M, Halvorsen DS, Straume B, Engstad TA. Co-morbidity and drug treatment in Alzheimer’s disease. A cross sectional study of participants in the dementia study in northern Norway. BMC Geriatr. 2011;11:58. doi:10.1186/1471-2318-11-58
33. Fereshtehnejad SM, Johnell K, Eriksdotter M. Anti-dementia drugs and co-medication among patients with Alzheimer’s disease: investigating real-world drug use in clinical practice using the Swedish Dementia Quality Registry (SveDem). Drugs Aging. 2014;31(3):215–224. doi:10.1007/s40266-014-0154-8
34. Crugel M, Paton G, Singh P, et al. Antipsychotics in people with dementia: frequency of use and rationale for prescribing in a UK mental health service. Psychiatrist. 2012;36(5):165–169. doi:10.1192/pb.bp.111.034579
35. Seitz DP, Adunuri N, Gill SS, Gruneir A, Herrmann N, Rochon P. Antidepressants for agitation and psychosis in dementia. Cochrane Database Syst Rev. 2011;2:CD008191.
36. Kable A, Fullerton A, Fraser S, et al. Comparison of potentially inappropriate medications for people with dementia at admission and discharge during an unplanned admission to hospital: results from the SMS dementia study. Healthcare (Basel). 2019;7(1):8. doi:10.3390/healthcare7010008
37. Molist-Brunet N, Sevilla-Sa´nchez D, Ambla´s-Novellas J, et al. Optimizing drug therapy in patients with advanced dementia: a patient-centered approach. Eur Geriatr Med. 2014;5(1):66–71. doi:10.1016/j.eurger.2013.10.011
38. von Renteln-kruse W, Neumann L, Klugmann B, et al. Geriatric patients with cognitive impairment: patient characteristics and treatment results on a specialized ward. Dtsch Arztebl Int. 2015;112(7):103–112.
39. Maher RL
40. Rodrigues MC, Oliveira C. Drug-drug interactions and adverse drug reactions in polypharmacy among older adults: an integrative review. Rev Lat Am Enfermagem. 2016;24:e2800. doi:10.1590/1518-8345.1316.2800
41. Wastesson JW, Morin L, Tan ECK, Johnell K. An update on the clinical consequences of polypharmacy in older adults: a narrative review. Expert Opin Drug Saf. 2018;17(12):1185–1196. doi:10.1080/14740338.2018.1546841
42. Reeve E, Trenaman SC, Rockwood K, Hilmer SN. Pharmacokinetic and pharmacodynamic alterations in older people with dementia. Expert Opin Drug Metab Toxicol. 2017;13(6):651–668. doi:10.1080/17425255.2017.1325873
43. Mehta DC, Short JL, Hilmer SN, Nicolazzo JA. Drug access to the central nervous system in Alzheimer’s disease: preclinical and clinical insights. Pharm Res. 2015;32(3):819–839.
44. Massoud L, Agha HA, Taleb M. Pharmacokinetic and pharmacodynamic changes in elderly people. World j Pharm Med. 2017;3(11):14–23.
45. Hutchison LC, O’Brien CE. Changes in pharmacokinetics and pharmacodynamics in the elderly patient. J Pharm Prac. 2007;20:4–12. doi:10.1177/0897190007304657
46. Mangoni AA, Jackson SH. Age-related changes in pharmacokinetics and pharmacodynamics: basic principles and practical applications. Br J Clin Pharmacol. 2004;57(1):6–14. doi:10.1046/j.1365-2125.2003.02007.x
47. Wooten JM. Pharmacotherapy considerations in elderly adults. South Med J. 2012;105(8):437–445. doi:10.1097/SMJ.0b013e31825fed90
48. Kröger E, Mouls M, Wilchesky M, et al. Adverse Drug Reactions Reported with Cholinesterase Inhibitors: an Analysis of 16 Years of Individual Case Safety Reports from VigiBase. Ann Pharmacother. 2015;49(11):1197–1206. doi:10.1177/1060028015602274
49. Pariente A, Sanctussy DJ, Miremont-Salamé G, et al. Factors associated with serious adverse reactions to cholinesterase inhibitors: a study of spontaneous reporting. CNS Drugs. 2010;24(1):55–63. doi:10.2165/11530300-000000000-00000
50. Ali TB, Schleret TR, Reilly BM, Chen WY, Abagyan R. Adverse Effects of Cholinesterase Inhibitors in Dementia, According to the Pharmacovigilance Databases of the United-States and Canada. PLoS One. 2015;10(12):e0144337.
51. Silva T, Reis J, Teixeira J, Borges F. Alzheimer’s disease, enzyme targets and drug discovery struggles: from natural products to drug prototypes. Ageing Res Rev. 2014;15:116–145.
52. Guillozet AL, Smiley JF, Mash DC, Mesulam MM. Butyrylcholinesterase in the life cycle of amyloid plaques. Ann Neurol. 1997;42(6):909–918. doi:10.1002/ana.410420613
53. Giacobini E. Selective inhibitors of butyrylcholinesterase: a valid alternative for therapy of Alzheimer’s disease? Drugs Aging. 2001;18(12):891–898. doi:10.2165/00002512-200118120-00001
54. Weinstock M. Selectivity of cholinesterase inhibition: clinical implications for the treatment of Alzheimer’s disease. CNS Drugs. 1999;12(4):307–323. doi:10.2165/00023210-199912040-00005
55. Mesulam MM, Geula C. Butyrylcholinesterase reactivity differentiates the amyloid plaques of aging from those of dementia. Ann Neurol. 1994;36(5):722–727. doi:10.1002/ana.410360506
56. Op Den Velde W, Stam FC. Some cerebral proteins and enzyme systems in Alzheimer’s presenile and senile dementia. J Am Geriatr Soc. 1976;24(1):12–16. doi:10.1111/j.1532-5415.1976.tb03247.x
57. Perry EK, Perry RH, Blessed G, Tomlinson BE. Changes in brain cholinesterases in senile dementia of Alzheimer type. Neuropathol Appl Neurobiol. 1978;4(4):273–277. doi:10.1111/j.1365-2990.1978.tb00545.x
58. Geula C, Darvesh S. Butyrylcholinesterase, cholinergic neurotransmission and the pathology of Alzheimer’s disease. Drugs Today (Barc). 2004;40(8):711–721. doi:10.1358/dot.2004.40.8.850473
59. Arendt T, Bruckner MK, Lange M, Bigl V. Changes in acetylcholinesterase and butyrylcholinesterase in Alzheimer’s disease resemble embryonic development – a study of molecular forms. Neurochem Int. 1992;21(3):381–396. doi:10.1016/0197-0186(92)90189-X
60. Davies P. Neurotransmitter-related enzymes in senile dementia of the Alzheimer type. Brain Res. 1979;171(2):319–327. doi:10.1016/0006-8993(79)90336-6
61. Wright CI, Geula C, Mesulam MM. Neurological cholinesterases in the normal brain and in Alzheimer’s disease: relationship to plaques, tangles, and patterns of selective vulnerability. Ann Neurol. 1993;34(3):373–384. doi:10.1002/ana.410340312
62. Maelicke A. Allosteric modulation of nicotinic receptors as a treatment strategy for Alzheimer’s disease. Dement Geriatr Cogn Disord. 2000;11(Suppl 1):11–18. doi:10.1159/000051227
63. Gauthier S. Cholinergic adverse effects of cholinesterase inhibitors in Alzheimer’s disease: epidemiology and management. Drugs Aging. 2001;18(11):853–862. doi:10.2165/00002512-200118110-00006
64. Thompson S, Lanctôt KL, Herrmann N. The benefits and risks associated with cholinesterase inhibitor therapy in Alzheimer’s disease. Expert Opin Drug Saf. 2004;3(5):425–440.
65. Patel M, Joshi A, Suthar J, Desai S. Drug utilization pattern in patients with different types of dementia in Western India. Int J Alzheimers Dis. 2014;2014:435202.
66. Li Q, He S, Chen Y, et al. Donepezil-based multi-functional cholinesterase inhibitors for treatment of Alzheimer’s disease. Eur J Med Chem. 2018;158:463–477. doi:10.1016/j.ejmech.2018.09.031
67. Cheewakriengkrai L, Gauthier S. A 10-year perspective on donepezil. Expert Opin Pharmacother. 2013;14(3):331–338. doi:10.1517/14656566.2013.760543
68. FDA approved drug products. Available from: http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm.
69. Howard R, McShane R, Lindesay J, et al. Donepezil and memantine for moderate-to-severe Alzheimer’s disease. N Engl J Med. 2012;366(10):893–903. doi:10.1056/NEJMoa1106668
70. Rodda J, Carter J. Cholinesterase inhibitors and memantine for symptomatic treatment of dementia. BMJ. 2012;344:e2986. doi:10.1136/bmj.e2986
71. Birks JS, Grimley EJ. Rivastigmine for Alzheimer’s disease. Cochrane Database Syst Rev. 2015;4:CD001191.
72. Tan CC, Yu JT, Wang HF, et al. Efficacy and safety of donepezil, galantamine, rivastigmine, and memantine for the treatment of Alzheimer’s disease: a systematic review and meta-analysis. J Alzheimers Dis. 2014;41(2):615–631. doi:10.3233/JAD-132690
73. Di Santo SG, Prinelli F, Adorni F, et al. A meta-analysis of the efficacy of donepezil, rivastigmine, galantamine, and memantine in relation to severity of Alzheimer’s disease. J Alzheimers Dis. 2013;35(2):349–361. doi:10.3233/JAD-122140
74. Tsoi KK, Chan JY, Chan FC, et al. Monotherapy is good enough for patients with mild-to moderate Alzheimer’s disease: a network meta-analysis of 76 randomized controlled trials. Clin Pharmacol Ther. 2019;105(1):121–130. doi:10.1002/cpt.1104
75. Deardorff WJ, Feen E, Grossberg GT. The Use of Cholinesterase Inhibitors Across All Stages of Alzheimer’s Disease. Drugs Aging. 2015;32(7):537–547. doi:10.1007/s40266-015-0273-x
76. Farlow MR, Salloway S, Tariot PN, et al. Effectiveness and tolerability of high-dose (23 mg/d) versus standard-dose (10 mg/d) donepezil in moderate to severe Alzheimer’s disease: a 24 week, randomized, double-blind study. Clin Ther. 2010;32(7):1234–1251. doi:10.1016/j.clinthera.2010.06.019
77. Sabbagh M, Cummings J, Christensen D, et al. Evaluating the cognitive effects of donepezil 23 mg/ d in moderate and severe Alzheimer’s disease: analysis of effects of baseline features on treatment response. BMC Geriatr. 2013;13:56. doi:10.1186/1471-2318-13-56
78. Molinuevo JL, Frölich L, Grossberg GT, et al. Responder analysis of a randomized comparison of the 13.3 mg/24 h and 9.5 mg/24 h rivastigmine patch. Alzheimers Res Ther. 2015;7(1):9. doi:10.1186/s13195-014-0088-8
79. Farlow MR, Grossberg GT, Sadowsky CH, Meng X, Somogyi MA. 24-week, randomized, controlled trial of rivastigmine patch 13.3 mg/24 h versus 4.6 mg/24 h in severe Alzheimer’s dementia. CNS Neurosci Ther. 2013;19(10):745–752. doi:10.1111/cns.12158
80. Farlow MR, Grossberg G, Gauthier S, Meng X, Olin JT. The ACTION study: methodology of a trial to evaluate safety and efficacy of a higher dose rivastigmine transdermal patch in severe Alzheimer’s disease. Curr Med Res Opin. 2010;26(10):2441–2447. doi:10.1185/03007995.2010.513849
81. Colović MB, Krstić DZ, Lazarević-Pašti TD, Bondžić AM, Vasić VM. Acetylcholinesterase inhibitors: pharmacology and toxicology. Curr Neuropharmacol. 2013;11(3):315–335.
82. Noetzli M, Eap CB. Pharmacodynamic, pharmacokinetic and pharmacogenetic aspects of drugs used in the treatment of Alzheimer’s disease. Clin Pharmacokinet. 2013;52(4):225–241. doi:10.1007/s40262-013-0038-9
83. Campos C, Rocha NB, Vieira RT, et al. Treatment of Cognitive Deficits in Alzheimer’s disease: a psychopharmacological review. Psychiatr Danub. 2016;28(1):2–12.
84. Cacabelos R. Pharmacogenomics and therapeutic prospects in Alzheimer’s disease. Expert Opin Pharmacother. 2005;6(12):1967–1987. doi:10.1517/14656566.6.12.1967
85. Lane RM, Potkin SG, Enz A. Targeting acetylcholinesterase and butyrylcholinesterase in dementia. Int J Neuropsychopharmacol. 2006;9(1):101–124. doi:10.1017/S1461145705005833
86. Heydorn WE. Donepezil (E2020): a new acetylcholinesterase inhibitor. Review of its pharmacology, pharmacokinetics, and utility in the treatment of Alzheimer’s disease. Expert Opin Investig Drugs. 1997;6(10):1527–1535. doi:10.1517/13543784.6.10.1527
87. Kosasa T, Kuriya Y, Matsui K, Yamanishi Y. Inhibitory effects of donepezil hydrochloride (E2020) on cholinesterase activity in brain and peripheral tissues of young and aged rats. Eur J Pharmacol. 1999;386(1):7–13. doi:10.1016/S0014-2999(99)00741-4
88. Gauthier S. Acetylcholinesterase inhibitors in the treatment of Alzheimer’s disease. Exp Opin Invest Drugs. 1999;8:1511–1520. doi:10.1517/13543784.8.10.1511
89. Tiseo PJ, Rogers SL, Friedhoff LT. Pharmacokinetic and pharmacodynamic profile of donepezil HCl following evening administration. Br J Clin Pharmacol. 1998;46(Suppl 1):13–18. doi:10.1046/j.1365-2125.1998.0460s1013.x
90. Ohnishi A, Mihara M, Kamakura H, et al. Comparison of the pharmacokinetics of E2020, a new compound for Alzheimer’s disease, in healthy young and elderly subjects. J Clin Pharmacol. 1993;33(11):1086–1091. doi:10.1002/j.1552-4604.1993.tb01945.x
91. Coin A, Pamio MV, Alexopoulos C, et al. Donepezil plasma concentrations, CYP2D6 and CYP3A4 phenotypes, and cognitive outcome in Alzheimer’s disease. Eur J Clin Pharmacol. 2016;72(6):711–717. doi:10.1007/s00228-016-2033-1
92. Riyath AA, Ammar BB, Faris TA. In vitro kinetic study of donepezil N-oxide metabolites. Irq J Pharm. 2011;11:1–9.
93. Winblad B, Engedal K, Soininen H, et al. Donepezil Nordic Study Group. A 1-year, randomized, placebo-controlled study of donepezil in patients with mild to moderate AD. Neurology. 2001;57(3):489–495. doi:10.1212/WNL.57.3.489
94. Mohs RC, Doody RS, Morris JC, et al.; “312” Study Group. A 1-year, placebo-controlled preservation of function survival study of donepezil in AD patients. Neurology. 2001;57(3):481–488. doi:10.1212/WNL.57.3.481
95. Rogers SL, Farlow MR, Doody RS, et al.; Donepezil Study Group. A 24-week, double-blind, placebo-controlled trial of donepezil in patients with Alzheimer’s disease. Neurology. 50;1998:136–145. doi:10.1212/WNL.50.1.136
96. Potocnik F. Dementia. S Afr J Psychiatr. 2013;19(3):141–152.
97. Jann MW. Rivastigmine, a new generation cholinesterase inhibitor for the treatment of Alzheimer’s disease. Pharmacotherapy. 2000;20(1):1–12. doi:10.1592/phco.20.1.1.34664
98. Hossain M, Jhee SS, Shiovitz T, et al. Estimation of the absolute bioavailability of rivastigmine in patients with mild to moderate dementia of the Alzheimer’s type. Clin Pharmacokinet. 2002;41(3):225–234. doi:10.2165/00003088-200241030-00006
99. Obburu JV, Tammara V, Lesko L, et al. Pharmacokinetic, pharmacodynamic modeling of rivastigmine, a cholinesterase inhibitor, in patients with Alzheimer’s disease. J Clin Pharmacol. 2001;41(10):1082–1090. doi:10.1177/00912700122012689
100. Spencer CM, Noble S. Rivastigmine: a review of its use in Alzheimer’s disease. Drugs Aging. 1998;13(5):391–411. doi:10.2165/00002512-199813050-00005
101. Banks WA. Drug delivery to the brain in Alzheimer’s disease: consideration of the blood-brain barrier. Adv Drug Deliv Rev. 2012;64(7):629–639. doi:10.1016/j.addr.2011.12.005
102. van Assema DM, Lubberink M, Bauer M, et al. Blood-brain barrier P-glycoprotein function in Alzheimer’s disease. Brain. 2012;135(Pt 1):181–189. doi:10.1093/brain/awr298
103. Rösler M, Anand R, Cicin-Sain A, et al. Efficacy and safety of rivastigmine in patients with Alzheimer’s disease: international randomised controlled trial. BMJ. 1999;318(7184):633–638. doi:10.1136/bmj.318.7184.633
104. Raina P, Santaguida P, Ismaila A, et al. Effectiveness of cholinesterase inhibitors and memantine for treating dementia: evidence review for a clinical practice guideline. Ann Intern Med. 2008;148(5):379–397. doi:10.7326/0003-4819-148-5-200803040-00009
105. Farlow MR. Update on rivastigmine. Neurologist. 2003;9(5):230–234. doi:10.1097/01.nrl.0000087724.73783.5f
106. Isik AT, Bozoglu E, Eker D. aChE and BuChE inhibition by rivastigmin have no effect on peripheral insulin resistance in elderly patients with Alzheimer disease. J Nutr Health Aging. 2012;16(2):139–141. doi:10.1007/s12603-011-0095-4
107. Greenspoon J, Herrmann N, Adam DN. Transdermal rivastigmine: management of cutaneous adverse events and review of the literature. CNS Drugs. 2011;25(7):575–583. doi:10.2165/11592230-000000000-00000
108. Amanatkar HR, Grossberg GT. Transdermal rivastigmine in the treatment of Alzheimer’s disease: current and future directions. Expert Rev Neurother. 2014;14(10):1119–1125. doi:10.1586/14737175.2014.955852
109. Lefevre G, Sedek G, Jhee SS, et al. Pharmacokinetics and pharmacodynamics of the novel Daily rivastigmine transdermal patch compared with twice-daily capsules in Alzheimer’s disease patients. Clin Pharmacol Ther. 2008;83(1):106–114. doi:10.1038/sj.clpt.6100242
110. Sramek JJ, Frackiewicz EJ, Cutler NR. Review of the acetylcholinesterase inhibitor galantamine. Expert Opin Investig Drugs. 2000;9(10):2393–2402. doi:10.1517/13543784.9.10.2393
111. Bickel U, Thomsen T, Weber W, et al. Pharmacokinetics of galanthamine in humans and corresponding cholinesterase inhibition. Clin Pharmacol Ther. 1991;50(4):420–428. doi:10.1038/clpt.1991.159
112. Bachus R, Bickel U, Thomsen T, Roots I, Kewitz H. The O-demethylation of the antidementia drug galanthamine is catalysed by cytochrome P450 2D6. Pharmacogenetics. 1999;9:661–668. doi:10.1097/00008571-199912000-00001
113. Kewitz H. Pharmacokinetics and metabolism of galanthamine. Drugs Today. 1997;33:265–272. doi:10.1358/dot.1997.33.4.425052
114. Raskind MA, Peskind ER, Wessel T, Yuan W; The Galantamine USA-1 Study Group. Galantamine in [Alzheimer’s disease]. A 6-month randomized, placebo-controlled trial with a 6-month extension. Neurology. 2000;54:2261–2268. doi:10.1212/WNL.54.12.2261
115. Zhao Q, Brett M, Van ON, et al. Galantamine pharmacokinetics, safety, and tolerability profiles are similar in healthy Caucasian and Japanese subjects. J Clin Pharmacol. 2002;42(9):1002–1010. doi:10.1177/0091270002042009007
116. Tayeb HO, Yang HD, Price BH, Tarazi FI. Pharmacotherapies for Alzheimer’s disease: beyond cholinesterase inhibitors. Pharmacol Ther. 2012;134(1):8–25.
117. Buckley JS, Salpeter SR. A Risk-Benefit Assessment of Dementia Medications: systematic Review of the Evidence. Drugs Aging. 2015;32(6):453–467. doi:10.1007/s40266-015-0266-9
118. O’Bryant SE, Humphreys JD, Smith GE, et al. Detecting dementia with the mini-mental state examination in highly educated individuals. Arch Neurol. 2008;65(7):963–967. doi:10.1001/archneur.65.7.963
119. Doraiswamy PM, Kaiser L, Bieber F, et al. The Alzheimer’s Disease Assessment Scale: evaluation of psychometric properties and patterns of cognitive decline in multicenter clinical trials of mild to moderate Alzheimer’s disease. Alzheimer Dis Assoc Disord. 2001;15(4):174–183. doi:10.1097/00002093-200110000-00003
120. Panisset M, Roudier M, Saxton J, et al. Severe impairment battery. A neuropsychological test for severely demented patients. Arch Neurol. 1994;51(1):41–45. doi:10.1001/archneur.1994.00540130067012
121. Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: a reliability study. Int Disabil Stud. 1988;10(2):61–63. doi:10.3109/09638288809164103
122. Wade DT, Collin C. The Barthel ADL Index: a standard measure of physical disability? Int Disabil Stud. 1988;10(2):64–67. doi:10.3109/09638288809164105
123. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179–186. doi:10.1093/geront/9.3_Part_1.179
124. Cummings JL, Mega M, Gray K, et al. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology. 1994;44(12):2308–2314. doi:10.1212/WNL.44.12.2308
125. Qaseem A, Snow V, Cross JT, et al. Current pharmacologic treatment of dementia: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med. 2008;148(5):370–378. doi:10.7326/0003-4819-148-5-200803040-00008
126. Santaguida PS, Raina P, Booker L, et al. Pharmacological treatment of dementia. Evid Rep Technol Assess (Summ). 2004;97:1–16.
127. Tricco AC, Ashoor HM, Soobiah C, et al. Comparative Effectiveness and Safety of Cognitive Enhancers for Treating Alzheimer’s Disease: systematic Review and Network Metaanalysis. J Am Geriatr Soc. 2018;66(1):170–178. doi:10.1111/jgs.15069
128. Trinh NH, Hoblyn J, Mohanty S, et al. Efficacy of cholinesterase inhibitors in the treatment of neuropsychiatric symptoms and functional impairment in Alzheimer disease: a meta- analysis. JAMA. 2003;289(2):210–216. doi:10.1001/jama.289.2.210
129. Isik AT, Soysal P, Usarel C. Effects of Acetylcholinesterase Inhibitors on Balance and Gait Functions and Orthostatic Hypotension in Elderly Patients With Alzheimer Disease. Am J Alzheimers Dis Other Demen. 2016;31(7):580–584. doi:10.1177/1533317516666195
130. Winblad B, Kilander L, Eriksson S, et al. Donepezil in patients with severe Alzheimer’s disease: double-blind, parallel-group, placebo-controlled study. Lancet. 2006;367(9516):1057–1065. doi:10.1016/S0140-6736(06)68350-5
131. Froelich L, Andreasen N, Tsolaki M, et al. Long-term treatment of patients with Alzheimer’s disease in primary and secondary care: results from an international survey. Curr Med Res Opin. 2009;25(12):3059–3068. doi:10.1185/03007990903396626
132. Lockhart IA, Mitchell SA, Kelly S. Safety and tolerability of donepezil, rivastigmine and galantamine for patients with Alzheimer’s disease: systematic review of the “real-world” evidence. Dement Geriatr Cogn Disord. 2009;28:389–403. doi:10.1159/000255578
133. Hansen RA, Gartlehner G, Webb AP, Morgan LC, Moore CG, Jonas DE. Efficacy and safety of donepezil, galantamine, and rivastigmine for the treatment of Alzheimer’s disease: a systematic review and meta-analysis. Clin Interv Aging. 2008;3:211–225.
134. Kröger E, Van Marum R, Souverein P, Carmichael PH, Egberts T. Treatment with rivastigmine or galantamine and risk of urinary incontinence: results from a Dutch database study. Pharmacoepidemiol Drug Saf. 2015;24:276–285. doi:10.1002/pds.3741
135. Colovic MB, Krstic DZ, Lazarevic-Pasti TD, Bondzic AM, Vasic VM. Acetylcholinesterase inhibitors: pharmacology and toxicology. Curr Neuropharmacol. 2013;11:315–335. doi:10.2174/1570159X11311030006
136. Galligan JJ, Burks TF. Cholinergic neurons mediate intestinal propulsion in the rat. J Pharm Exper Ther. 1986;238(2):594–598.
137. Lewin MJ. Cellular mechanisms and inhibitors of gastric acid secretion. Drugs Today (Barc). 1999;35(10):743–752. doi:10.1358/dot.1999.35.10.561693
138. Full prescription information. Razadyne (galantamine). Available from: https://www.janssenmd.com/pdf/razadyne/PI-Razadyne-RazadyneER.pdf.
139. Soysal P, Isik AT, Stubbs B, et al. Acetylcholinesterase inhibitors are associated with weight loss in older people with dementia: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry. 2016;87(12):1368–1374. doi:10.1136/jnnp-2016-313660
140. Full prescription information. Aricept (donepezil). Available from: https://www.labeling.pfizer.com/ShowLabeling.aspx?id=510.
141. Full prescription information. Exelon (rivastigmine). Available from: https://www.pharma.us.novartis.com/product/pi/pdf/exelon.pdf.
142. Cutler NR, Anand R, Hartman RD, et al. Antiemetic therapy for Alzheimer’s patients receiving the cholinesterase inhibitor SDZ ENA 713 [abstract]. Clin Pharmacol Ther. 1998;63(2):188.
143. Kistler PM, Sanders P, Fynn SP, et al. Electrophysiologic and electroanatomic changes in the human atrium associated with age. J Am Coll Cardiol. 2004;44(1):109–116. doi:10.1016/j.jacc.2004.03.044
144. Jones SA, Lancaster MK, Boyett MR. Ageing-related changes of connexins and conduction within the sinoatrial node. J Physiol (Lond). 2004;560(Pt 2):429–437. doi:10.1113/jphysiol.2004.072108
145. Jane Newby V, Anne Kenny R, McKeith IG. Donepezil and cardiac syncope: case report. Int J Geriatr Psychiatry. 2004;19(11):1110–1112. doi:10.1002/gps.1183
146. Shahani L. Donepezil-associated sick sinus syndrome. J Neuropsychiatry Clin Neurosci. 2014;26(1):E5. doi:10.1176/appi.neuropsych.12110270
147. Park-Wyllie LY, Mamdani MM, Li P, Gill SS, Laupacis A, Juurlink DN. Cholinesterase inhibitors and hospitalization for bradycardia: a population-based study. PLoS Med. 2009;6(9):e1000157. doi:10.1371/journal.pmed.1000157
148. Tanaka A, Koga S, Hiramatsu Y. Donepezil-induced adverse side effects of cardiac rhythm: 2 cases report of atrioventricular block and Torsade de Pointes. Intern Med. 2009;48(14):1219–1223. doi:10.2169/internalmedicine.48.2181
149. Takaya T, Okamoto M, Yodoi K, et al. Torsades de Pointes with QT prolongation related to donepezil use. J Cardiol. 2009;54(3):507–511. doi:10.1016/j.jjcc.2009.03.011
150. Hadano Y, Ogawa H, Wakeyama T, et al. Donepezil-induced torsades de pointes without QT prolongation. J Cardiol Cases. 2013;8(2):e69–e71. doi:10.1016/j.jccase.2013.05.004
151. Celik IE, Acar B, Çay S. An unusual cardiovascular adverse effect of donepezil. Intern Med J. 2015;45(8):877–878. doi:10.1111/imj.12827
152. Gill SS, Anderson GM, Fischer HD, et al. Syncope and its consequences in patients with dementia receiving cholinesterase inhibitors: a population-based cohort study. Arch Intern Med. 2009;169(9):867–873. doi:10.1001/archinternmed.2009.43
153. Kim DH, Brown RT, Ding EL, Kiel DP, Berry SD. Dementia medications and risk of falls, syncope, and related adverse events meta-analysis of randomized controlled trials. J Am Geriatr Soc. 2011;59(6):1019–1031. doi:10.1111/j.1532-5415.2011.03450.x
154. Hernandez RK, Farwell W, Cantor MD, Lawler EV. Cholinesterase inhibitors and hospitalizations for bradycardia. J Am Geriatr Soc. 2009;57:1997–2003. doi:10.1111/j.1532-5415.2009.02488.x
155. Isik AT, Yildiz GB, Bozoglu E, et al. Cardiac safety of donepezil in elderly patients with Alzheimer disease. Intern Med. 2012;51(6):575–578. doi:10.2169/internalmedicine.51.6671
156. Isik AT, Soysal P, Yay A. Which rivastigmine formula is better for heart in elderly patients with Alzheimer’s disease: oral or patch? Am J Alzheimers Dis Other Demen. 2014;29(8):735–738. doi:10.1177/1533317514536598
157. Isik AT, Bozoglu E, Yay A, et al. Which cholinesterase inhibitor is the safest for the heart elderly patients with Alzheimer’s disease? Am J Alzheimers Dis Other Demen. 2012;27(3):171–174. doi:10.1177/1533317512442999
158. Isik AT, Soysal P, Stubbs B, et al. Cardiovascular Outcomes of Cholinesterase Inhibitors in Individuals with Dementia: a Meta-Analysis and Systematic Review. J Am Geriatr Soc. 2018;66(9):1805–1811. doi:10.1111/jgs.15415
159. Rowland JP, Rigby J, Harper AC, et al. Cardiovascular monitoring with acetylcholinesterase inhibitors: a clinical protocol. Adv Psychiatr Treat. 2007;13:178–184. doi:10.1192/apt.bp.106.002725
160. Babic T, Zurak N. Convulsions induced by donepezil. J Neurol Neurosurg Psychiatry. 1999;66(3):410. doi:10.1136/jnnp.66.3.410
161. Shareef J, Joseph J, Adithi K. A single case report on hyponatremia seizure induced by acetylcholinesterase inhibitors. Int J Pharm Pharm Sci. 2017;9(7):165–166. doi:10.22159/ijpps.2017v9i7.19057
162. Ross JS, Shua-Haim JR. Aricept-induced nightmares in Alzheimer’s disease: 2 case reports. J Am Geriatr Soc. 1998;46(1):119–120. doi:10.1111/j.1532-5415.1998.tb01033.x
163. Bouman WP, Pinner G. Violent behavior associated with donepezil. Am J Psychiatry. 1998;155(11):1626–1627. doi:10.1176/ajp.155.11.1626a
164. Yorston GA, Gray R. Hypnopompic hallucinations with donepezil. J Psychopharmacol. 2000;14(3):303–304. doi:10.1177/026988110001400315
165. Wong CW. Pharmacotherapy for Dementia: a Practical Approach to the Use of Cholinesterase Inhibitors and Memantine. Drugs Aging. 2016;33(7):451–460. doi:10.1007/s40266-016-0372-3
166. Hashimoto M, Imamura T, Tanimukai S, Kazui H, Mori E. Urinary incontinence: an unrecognised adverse effect with donepezil. Lancet. 2000;356(9229):568. doi:10.1016/S0140-6736(00)02588-5
167. Ale I, Lachapelle JM, Maibach HI. Skin tolerability associated with transdermal drug delivery systems: an overview. Adv Ther. 2009;26(10):920–935. doi:10.1007/s12325-009-0075-9
168. Wohlrab J, Kreft B, Tamke B. Skin tolerability of transdermal patches. Expert Opin Drug Deliv. 2011;8(7):939–948. doi:10.1517/17425247.2011.574689
169. Osada T, Watanabe N, Asano N, Adachi Y, Yamamura K. Adverse drug events affecting medication persistence with rivastigmine patch application. Patient Prefer Adherence. 2018;12:1247–1252. doi:10.2147/PPA.S166680
170. Zannas AS, Okuno Y, Doraiswamy PM. Cholinesterase inhibitors and Pisa syndrome: a pharmacovigilance study. Pharmacotherapy. 2014;34(3):272–278. doi:10.1002/phar.1359
171. Hsu CW, Lee Y, Lee CY, Lin PY. Reversible Pisa Syndrome Induced by Rivastigmine in a Patient With Early-Onset Alzheimer Disease. Clin Neuropharmacol. 2017;40(3):147–148. doi:10.1097/WNF.0000000000000215
172. Miyaoka T, Seno H, Yamamori C, et al. Pisa syndrome due to a cholinesterase inhibitor (donepezil): a case report. J Clin Psychiatry. 2001;62(7):573–574. doi:10.4088/JCP.v62n07d13
173. Fleet JL, McArthur E, Patel A, et al. Risk of rhabdomyolysis with donepezil compared with rivastigmine or galantamine: a population-based cohort study. CMAJ. 2019;191(37):e1018- e1024. doi:10.1503/cmaj.190337
174. Health Canada. Summary Safety Review - ARICEPT (donepezil) - Risk of Rhabdomyolysis and Neuroleptic Malignant Syndrome [Internet]. Drug Heal Prod. 2015. Available from. http://www.hc-sc.gc.ca/dhp-mps/medeff/reviews-examens/aricept-eng.php#fnb1
175. Ekinci F, Soyaltin UE, Ugur MC, Develi A, Akar H. A rare case of Rhabdomyolysis probably due to donepezil. J Clin Case Rep. 2014;4:465.
176. Verrico MM, Nace DA, Towers AL. Fulminant chemical hepatitis possibly associated with donepezil and sertraline therapy. J Am Geriatr Soc. 2000;48:1659–1663. doi:10.1111/j.1532-5415.2000.tb03879.x
177. Trenaman SC, Bowles SK, Kirkland S, et al. An examination of three prescribing cascades in a cohort of older adults with dementia. BMC Geriatr. 2021;21(1):297. doi:10.1186/s12877-021-02246-2
178. Vouri SM, Possinger MC, Usmani S, et al. Evaluation of the Potential Acetylcholinesterase Inhibitor-Induced Rhinorrhea Prescribing Cascade. J Am Geriatr Soc. 2020;68(2):440–441. doi:10.1111/jgs.16224
179. Gill SS, Mamdani M, Naglie G, et al. A prescribing cascade involving cholinesterase inhibitors and anticholinergic drugs. Arch Intern Med. 2005;165(7):808–813. doi:10.1001/archinte.165.7.808
180. Bowie MW, Slattum PW. Pharmacodynamics in older adults: a review. Am J Geriatr Pharmacother. 2007;5:263–303. doi:10.1016/j.amjopharm.2007.10.001
181. Maher D, Ailabouni N, Mangoni AA, Wiese MD, Reeve E. Alterations in drug disposition in older adults: a focus on geriatric syndromes. Expert Opin Drug Metab Toxicol. 2021;17(1):41–52. doi:10.1080/17425255.2021.1839413
182. Farrall AJ, Wardlaw JM. Blood-brain barrier: ageing and microvascular disease - systematic review and meta-analysis. Neurobiol Aging. 2009;30(3):337–352. doi:10.1016/j.neurobiolaging.2007.07.015
183. Nobili A, Garattini S, Mannucci PM. Multiple diseases and polypharmacy in the elderly: challenges for the internist of the third millennium. J Comorbidity. 2011;1:28–44. doi:10.15256/joc.2011.1.4
184. Onder G, Marengoni A, Russo P, et al. Advanced age and medication prescription: more years, less medications? A Nationwide report from the Italian Medicines Agency. J Am Med Dir Assoc. 2016;17(2):168–172. doi:10.1016/j.jamda.2015.08.009
185. Gustafsson M, Sjölander M, Pfister B, Jonsson J, Schneede J, Lövheim H. Drug-related hospital admissions among old people with dementia. Eur J Clin Pharmacol. 2016;72(9):1143–1153. doi:10.1007/s00228-016-2084-3
186. Pirmohamed M, James S, Meakin S, et al. Adverse drug reactions as cause of admission to hospital: prospective analysis of 18 820 patients. BMJ. 2004;329(7456):15–19. doi:10.1136/bmj.329.7456.15
187. Desai AK, Grossberg GT. Rivastigmine for Alzheimer’s disease. Expert Rev Neurother. 2005;5(5):563–580. doi:10.1586/14737175.5.5.563
188. Desai AK, Grossberg GT. Review of rivastigmine and its clinical applications in Alzheimer’s disease and related disorders. Expert Opin Pharmacother. 2001;2(4):653–666. doi:10.1517/14656566.2.4.653
189. Román GC, Rogers SJ. Donepezil: a clinical review of current and emerging indications. Expert Opin Pharmacother. 2004;5(1):161–180. doi:10.1517/14656566.5.1.161
190. Kurz A, Farlow M, Lefèvre G. Pharmacokinetics of a novel transdermal rivastigmine patch for the treatment of Alzheimer’s disease: a review. Int J Clin Pract. 2009;63(5):799–805. doi:10.1111/j.1742-1241.2009.02052.x
191. Wysokiński A, Sobów T, Kłoszewska I, Kostka T. Mechanisms of the anorexia of aging-a review. Age (Dordr). 2015;37(4):9821. doi:10.1007/s11357-015-9821-x
192. Thompson CM, Johns DO, Sonawane B, et al. Database for physiologically based pharmacokinetic (PBPK) modeling: physiological data for healthy and health-impaired elderly. J Toxicol Environ Health B Crit Rev. 2009;12(1):1–24. doi:10.1080/10937400802545060
193. Hughes VA, Frontera WR, Wood M, et al. Longitudinal muscle strength changes in older adults: influence of muscle mass, physical activity, and health. J Gerontol a Biol Sci Med Sci. 2001;56(5):B209–217. doi:10.1093/gerona/56.5.B209
194. Hubbard RE, O’Mahony MS, Calver BL, Woodhouse KW. Nutrition, inflammation, and leptin levels in aging and frailty. J Am Geriatr Soc. 2008;56(2):279–284. doi:10.1111/j.1532-5415.2007.01548.x
195. Reeve E, Wiese MD, Mangoni AA. Alterations in drug disposition in older adults. Expert Opin Drug Metab Toxicol. 2015;11(4):491–508. doi:10.1517/17425255.2015.1004310
196. Le Couteur DG, Blyth FM, Creasey HM, et al. The association of alanine transaminase with aging, frailty, and mortality. J Gerontol a Biol Sci Med Sci. 2010;65(7):712–717. doi:10.1093/gerona/glq082
197. Dooley M, Lamb HM. Donepezil: a review of its use in Alzheimer’s disease. Drugs Aging. 2000;16(3):199–226. doi:10.2165/00002512-200016030-00005
198. Hubbard RE, O’Mahony MS, Calver BL, Woodhouse KW. Plasma esterases and inflammation in ageing and frailty. Eur J Clin Pharmacol. 2008;64(9):895–900. doi:10.1007/s00228-008-0499-1
199. Renton KW. Regulation of drug metabolism and disposition during inflammation and infection. Expert Opin Drug Metab Toxicol. 2005;1(4):629–640. doi:10.1517/17425255.1.4.629
200. Aitken AE, Richardson TA, Morgan ET. Regulation of drug-metabolizing enzymes and transporters in inflammation. Annu Rev Pharmacol Toxicol. 2006;46:123–149. doi:10.1146/annurev.pharmtox.46.120604.141059
201. Wynne H. Drug metabolism and ageing. J Br Menopause Soc. 2005;11(2):51–56. doi:10.1258/136218005775544589
202. Zoli M, Magalotti D, Bianchi G, et al. Total and functional hepatic blood flow decrease in parallel with ageing. Age Ageing. 1999;28(1):29–33. doi:10.1093/ageing/28.1.29
203. Wynne HA, Cope LH, Mutch E, Rawlins MD, Woodhouse KW, James OFW. The effect of age upon liver volume and apparent liver blood flow in healthy man. Hepatology. 1989;9(2):297–301. doi:10.1002/hep.1840090222
204. Klotz U. Pharmacokinetics and drug metabolism in the elderly. Drug Metab Rev. 2009;41(2):67–76. doi:10.1080/03602530902722679
205. Butler JM, Begg EJ. Free drug metabolic clearance in elderly people. Clin Pharmacokinet. 2008;47(5):297–321. doi:10.2165/00003088-200847050-00002
206. Tiseo PJ, Vargas R, Perdomo CA, Friedhoff LT. An evaluation of the pharmacokinetics of donepezil HCl in patients with impaired hepatic function. Br J Clin Pharmacol. 1998;46 Suppl 1(Suppl 1):51–55. doi:10.1046/j.1365-2125.1998.0460s1051.x
207. Tiseo PJ, Foley K, Friedhoff LT. An evaluation of the pharmacokinetics of donepezil HCl in patients with moderately to severely impaired renal function. Br J Clin Pharmacol. 1998;46 Suppl 1(Suppl1):56–60. doi:10.1046/j.1365-2125.1998.0460s1056.x
208. Fliser D, Zeier M, Nowack R, Ritz E. Renal functional reserve in healthy elderly subjects. J Am Soc Nephrol. 1993;3(7):1371–1377. doi:10.1681/ASN.V371371
209. Viallon A, Guyomarch P, Marjollet O, et al. Creatinine clearance and drug prescriptions for the elderly. A study of 419 patients older than 70 years admitted through the emergency department. Presse Med. 2006;35:413–417. doi:10.1016/S0755-4982(06)74605-X
210. Farlow MR. Clinical pharmacokinetics of galantamine. Clin Pharmacokinet. 2003;42(15):1383–1392. doi:10.2165/00003088-200342150-00005
211. Gottwald MD, Rozanski RI. Rivastigmine, a brain-region selective acetylcholinesterase inhibitor for treating Alzheimer’s disease: review and current status. Expert Opin Investig Drugs. 1999;8(10):1673–1682. doi:10.1517/13543784.8.10.1673
212. Hrycyna CA. Molecular genetic analysis and biochemical characterization of mammalian P- glycoproteins involved in multidrug resistance. Semin Cell Dev Biol. 2001;12(3):247–256. doi:10.1006/scdb.2000.0250
213. Alavijeh MS, Chishty M, Qaiser MZ, Palmer AM. Drug metabolism and pharmacokinetics, the blood-brain barrier, and central nervous system drug discovery. NeuroRx. 2005;2(4):554–571. doi:10.1602/neurorx.2.4.554
214. van Waterschoot RA, Schinkel AH. A critical analysis of the interplay between cytochrome P450 3A and P-glycoprotein: recent insights from knockout and transgenic mice. Pharmacol Rev. 2011;63(2):390–410. doi:10.1124/pr.110.002584
215. van Assema DM, Lubberink M, Rizzu P, et al. Blood-brain barrier P-glycoprotein function in healthy subjects and Alzheimer’s disease patients: effect of polymorphisms in the ABCB1 gene. EJNMMI Res. 2012;2(1):57. doi:10.1186/2191-219X-2-57
216. Trifirò G, Spina E. Age-related changes in pharmacodynamics: focus on drugs acting on central nervous and cardiovascular systems. Curr Drug Metab. 2011;12(7):611–620. doi:10.2174/138920011796504473
217. Bishop JR. Pharmacogenetics. Handb Clin Neurol. 2018;147:59–73.
218. Noetzli M, Guidi M, Ebbing K, et al. Population pharmacokinetic approach to evaluate the effect of CYP2D6, CYP3A, ABCB1, POR and NR1I2 genotypes on donepezil clearance. Br J Clin Pharmacol. 2014;78(1):135–144. doi:10.1111/bcp.12325
219. Darvesh S, Hopkins DA, Geula C. Neurobiology of butyrylcholinesterase. Nat Rev Neurosci. 2003;4(2):131–138. doi:10.1038/nrn1035
220. Harold D, Macgregor S, Patterson CE, et al. A single nucleotide polymorphism in CHAT influences response to acetylcholinesterase inhibitors in Alzheimer’s disease. Pharmacogenet Genomics. 2006;16(2):75–77. doi:10.1097/01.fpc.0000189799.88596.04
221. Pola R, Flex A, Ciaburri M, et al. Responsiveness to cholinesterase inhibitors in Alzheimer’s disease: a possible role for the 192 Q/R polymorphism of the PON-1 gene. Neurosci Lett. 2005;382(3):338–341. doi:10.1016/j.neulet.2005.03.027
222. Varsaldi F, Miglio G, Scordo MG, et al. Impact of the CYP2D6 polymorphism on steady-state plasma concentrations and clinical outcome of donepezil in Alzheimer’s disease patients. Eur J Clin Pharmacol. 2006;62(9):721–726. doi:10.1007/s00228-006-0168-1
223. Pilotto A, Franceschi M, D’Onofrio G, et al. Effect of a CYP2D6 polymorphism on the efficacy of donepezil in patients with Alzheimer disease. Neurology. 2009;73(10):761–767. doi:10.1212/WNL.0b013e3181b6bbe3
224. Albani D, Martinelli Boneschi F. Replication study to confirm the role of CYP2D6 polymorphism rs1080985 on donepezil efficacy in Alzheimer’s disease patients. J Alzheimers Dis. 2012;30(4):745–749. doi:10.3233/JAD-2012-112123
225. Seripa D, Bizzarro A, Pilotto A, et al. Role of cytochrome P4502D6 functional polymorphisms in the efficacy of donepezil in patients with Alzheimer’s disease. Pharmacogenet Genomics. 2011;21(4):225–230. doi:10.1097/FPC.0b013e32833f984c
226. Campbell NL, Skaar TC, Perkins AJ, et al. Characterization of hepatic enzyme activity in older adults with dementia: potential impact on personalizing pharmacotherapy. Clin Interv Aging. 2015;10:269–275. doi:10.2147/CIA.S65980
227. Cacabelos R, Martínez R, Fernández-Novoa L, et al. Genomics of Dementia: APOE- and CYP2D6-Related Pharmacogenetics. Int J Alzheimers Dis. 2012;2012:518901.
228. Liu M, Zhang Y, Huo YR, et al. Influence of the rs1080985 Single Nucleotide Polymorphism of the CYP2D6 Gene and APOE Polymorphism on the Response to Donepezil Treatment in Patients with Alzheimer’s Disease in China. Dement Geriatr Cogn Dis Extra. 2014;4(3):450–456. doi:10.1159/000367596
229. Choi SH, Kim SY, Na HR, et al. Effect of ApoE genotype on response to donepezil in patients with Alzheimer’s disease. Dement Geriatr Cogn Disord. 2008;25(5):445–450. doi:10.1159/000124752
230. Cacabelos R. Influence of pharmacogenetic factors on Alzheimer’s disease therapeutics. Neurodegener Dis. 2008;5(3–4):176–178. doi:10.1159/000113695
231. Zanger UM, Raimundo S, Eichelbaum M. Cytochrome P450 2D6: overview and update on pharmacology, genetics, biochemistry. Naunyn Schmiedebergs Arch Pharmacol. 2004;369(1):23–37. doi:10.1007/s00210-003-0832-2
232. Zhou SF. Polymorphism of human cytochrome P450 2D6 and its clinical significance: part I. Clin Pharmacokinet. 2009;48(11):689–723.
233. Bradford LD. CYP2D6 allele frequency in European Caucasians, Asians, Africans and their descendants. Pharmacogenomics. 2002;3:229–243. doi:10.1517/14622416.3.2.229
234. Martinelli-Boneschi F, Giacalone G, Magnani G, et al. Pharmacogenomics in Alzheimer’s disease: a genome-wide association study of response to cholinesterase inhibitors. Neurobiol Aging. 2013;34(6):
235. Lu J, Fu J, Zhong Y, et al. Association between ABCA1 gene polymorphisms and the therapeutic response to donepezil therapy in Han Chinese patients with Alzheimer’s disease. Brain Res Bull. 2018;140:1–4. doi:10.1016/j.brainresbull.2018.03.014
236. Triplitt C. Drug interactions of medications commonly used in diabetes. Diabetes. 2006;19(4):202–211.
237. Tavassoli N, Sommet A, Lapeyre-Mestre M, Bagheri H, Montrastruc JL. Drug interactions with Cholinesterase inhibitors: an analysis of the French pharmacovigilance database and a comparison of two national drug formularies (Vidal, British National Formulary). Drug Saf. 2007;30(11):1063–1071. doi:10.2165/00002018-200730110-00005
238. Delafuente JC. Understanding and preventing drug interactions in elderly patients. Crit Rev Oncol Hematol. 2003;48(2):133–143. doi:10.1016/j.critrevonc.2003.04.004
239. Johnell K, Klarin I. The relationship between number of drugs and potential drug-drug interactions in the elderly: a study of over 600,000 elderly patients from the Swedish Prescribed Drug Register. Drug Saf. 2007;30(10):911–918. doi:10.2165/00002018-200730100-00009
240. Gallicano K, Drusano G. Introduction to drug interactions. In: Piscitelli SC, Rodvold K, editors. Drug Interactions in Infectious Diseases.
241. Pasqualetti G, Tognini S, Calsolaro V, et al. Potential drug-drug interactions in Alzheimer patients with behavioral symptoms. Clin Interv Aging. 2015;10:1457–1466.
242. Magnuson TM, Keller BK, Burke WJ. Extrapyramidal side effects in a patient treated with risperidone plus donepezil. Am J Psychiatry. 1998;155(10):1458–1459. doi:10.1176/ajp.155.10.1458a
243. Mehrpouya M, Ataei S, Nili-Ahmadabadi A. Potential drug interactions with cholinesterase inhibitors in Alzheimer patients: a guideline for Neurologists. J Appl Pharm Sci. 2017;7(1):223–226. doi:10.7324/JAPS.2017.70134
244. Lin JH, Lu AYH. Inhibition and induction of cytochrome P450 and the clinical implications. Clin Pharmacokinet. 1998;35(5):361–390. doi:10.2165/00003088-199835050-00003
245. McEneny-King A, Edginton AN, Pp R. Investigating the binding interactions of the anti- Alzheimer’s drug donepezil with CYP3A4 and P-glycoprotein. Bioorg Med Chem Lett. 2015;25(2):297–301. doi:10.1016/j.bmcl.2014.11.046
246. Spina E, Scordo MG, D’Arrigo C. Metabolic drug interactions with new psychotropic agents. Fundam Clin Pharmacol. 2003;17(5):517–538. doi:10.1046/j.1472-8206.2003.00193.x
247. Tiseo PJ, Perdomo CA, Friedhoff LT. Concurrent administration of donepezil HCl and ketoconazole: assessment of pharmacokinetic changes following single and multiple doses. Br J Clin Pharmacol. 1998;46(Suppl 1):30–34. doi:10.1046/j.1365-2125.1998.0460s1030.x
248. Defilippi JL, Crismon ML. Drug interactions with cholinesterase inhibitors. Drugs Aging. 2003;20(6):437–444. doi:10.2165/00002512-200320060-00003
249. Carrier L. Donepezil and paroxetine: possible drug interaction. J Am Geriatr Soc. 1999;47(8):1037. doi:10.1111/j.1532-5415.1999.tb01306.x
250. Finch A, Pillans P. P-glycoprotein and its role in drug-drug interactions. Aust Prescr. 2014;37:137–139. doi:10.18773/austprescr.2014.050
251. US Food and Drug Administration. Clinical drug interaction studies-Cytochrome P450 enzyme- and transporter-mediated drug interactions guidance for industry; January 2020. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/clinical-drug-interaction-studies-cytochrome-p450-enzyme-and-transporter-mediated-drug-interactions.
252. Takeuchi R, Shinozaki K, Nakanishi T, Tamai I. Local Drug-Drug Interaction of Donepezil with Cilostazol at Breast Cancer Resistance Protein (ABCG2) Increases Drug Accumulation in Heart. Drug Metab Dispos. 2016;44(1):68–74. doi:10.1124/dmd.115.066654
253. Johnell K, Fastbom J. Concurrent use of anticholinergic drugs and cholinesterase inhibitors: register-based study of over 700,000 elderly patients. Drugs Aging. 2008;25:871–877. doi:10.2165/00002512-200825100-00006
254. Modi A, Weiner M, Craig BA, Sands LP, Rosenman MB, Thomas J. Concomitant use of anticholinergics with acetylcholinesterase inhibitors in Medicaid recipients with dementia and residing in nursing homes. J Am Geriatr Soc. 2009;57:1238–1244. doi:10.1111/j.1532-5415.2009.02258.x
255. Walker C, Perks D. Do you know about donepezil and succinylcholine? Anaesthesia. 2002;57:1041. doi:10.1046/j.1365-2044.2002.00117.x
256. Sprung J, Castellani WJ, Srinivasan V, Udayashankar S. The effects of donepezil and neostigmine in a patient with unusual pseudocholinesterase activity. Anesth Analg. 1998;87(5):1203–1205.
257. Sánchez Morillo J, Demartini Ferrari A, Roca de Togores López A. Interacción entre donepezilo y bloqueantes musculares en la enfermedad de Alzheimer [Interaction of donepezil and muscular blockers in Alzheimer’s disease]. Rev Esp Anestesiol Reanim. 2003;50(2):97–100.
258. Carcenac D, Martin-Hunyadi C, Kiesmann M, Demuynck-Roegel C, Alt M, Kuntzmann F. Syndrome extrapyramidal sous donepezil [Extra-pyramidal syndrome induced by donepezil]. Presse Med. 2000;29(18):992–993.
259. Shimizu S, Mizuguchi Y, Sobue A, Fujiwara M, Morimoto T, Ohno Y. Interaction between anti- Alzheimer and antipsychotic drugs in modulating extrapyramidal motor disorders in mice. J Pharmacol Sci. 2015;127(4):439–445. doi:10.1016/j.jphs.2015.03.004
260. Bentue-Ferrer D, Tribut O, Polard E, Allain H. Clinically significant drug interactions with cholinesterase inhibitors: a guide for neurologists. CNS Drugs. 2003;17:947–963. doi:10.2165/00023210-200317130-00002
261. [No authors listed]. Bradycardia due to cholinesterase inhibitors: identify adverse effects and take them into account. Prescrire Int. 2011;20(115):95.
262. Hong YJ, Han HJ, Youn YC, et al. Safety and tolerability of donepezil 23 mg with or without intermediate dose titration in patients with Alzheimer’s disease taking donepezil 10 mg: a multicenter, randomized, open-label, parallel-design, three-arm, prospective trial. Alzheimers Res Ther. 2019;11(1):37. doi:10.1186/s13195-019-0492-1
263. Christensen DD. Higher-dose (23 mg/day) donepezil formulation for the treatment of patients with moderate-to-severe Alzheimer’s disease. Postgrad Med. 2012;124(6):110–116. doi:10.3810/pgm.2012.11.2589
264. Reyes JF, Vargas R, Kumar D, et al. Steady-state pharmacokinetics, pharmacodynamics and tolerability of donepezil hydrochloride in hepatically impaired patients. Br J Clin Pharmacol. 2004;58(Suppl 1):9–17. doi:10.1111/j.1365-2125.2004.01802.x
265. Ali TB, Schleret TR, Reilly BM, et al. Adverse effects of cholinesterase inhibitors in dementia, according to the pharmacovigilance databases of the United-States and Canada. PLoS One. 2015;10(12):e0144337. doi:10.1371/journal.pone.0144337
266. Sheffrin M, Miao Y, Boscardin WJ, et al. Weight loss associated with cholinesterase inhibitors in individuals with dementia in a national healthcare system. J Am Geriatr Soc. 2015;63(8):1512–1518. doi:10.1111/jgs.13511
267. Vetrano DL, Tosato M, Colloca G, et al. Polypharmacy in nursing home residents with severe cognitive impairment: results from the SHELTER Study. Alzheimers Dement. 2013;9(5):587–593. doi:10.1016/j.jalz.2012.09.009
268. Renn BN, Asghar-Ali AA, Thielke S, et al. A Systematic Review of Practice Guidelines and Recommendations for Discontinuation of Cholinesterase Inhibitors in Dementia. Am J Geriatr Psychiatry. 2018;26(2):134–147. doi:10.1016/j.jagp.2017.09.027
269. Reeve E, Farrell B, Thompson W, et al. Deprescribing cholinesterase inhibitors and memantine In dementia: guideline summary. Med J Aust. 2019;210(4):174–179. doi:10.5694/mja2.50015
270. Corsonello A, Pedone C, Incalzi RA. Age-related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Curr Med Chem. 2010;17(6):571–584. doi:10.2174/092986710790416326
271. Gurwitz JH, Field TS, Harrold LR, et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA. 2003;289(9):1107–1116. doi:10.1001/jama.289.9.1107
272. Eshetie TC, Nguyen TA, Gillam MH, Kalisch Ellett LM. A narrative review of problems with medicines use in people with dementia. Expert Opin Drug Saf. 2018;17(8):825–836. doi:10.1080/14740338.2018.1497156
273. Pfister B, Jonsson J, Gustafsson M. Drug-related problems and medication reviews among old people with dementia. BMC Pharmacol Toxicol. 2017;18(1):52. doi:10.1186/s40360-017-0157-2
274. Wucherer D, Thyrian JR, Eichler T, et al. Drug-related problems in community-dwelling primary care patients screened positive for dementia. Int Psychogeriatrics. 2017;29(11):1857–1868. doi:10.1017/S1041610217001442
275. Mallet L, Spinewine A, Huang A. The challenge of managing drug interactions in elderly people. Lancet. 2007;370(9582):185–191. doi:10.1016/S0140-6736(07)61092-7
276. Lau DT, Mercaldo ND, Harris AT, Trittschuh E, Shega J, Weintraub S. Polypharmacy and potentially inappropriate medication use among community-dwelling elders with dementia. Alzheimer Dis Assoc Disord. 2010;24(1):56–63. doi:10.1097/WAD.0b013e31819d6ec9
277. Micromedex® HealthCare Series (internet database) Version 2.0. Greenwood Village, Colorado: Thomson Healthcare Inc; 2013. Available from: http://www.micromedexsolutions.com.
278. By the 2019 American Geriatrics Society Beers Criteria Update Expert Panel. American Geriatrics Society 2019 updated AGS Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694.
279. Gustafsson M, Sjölander M, Pfister B, Schneede J, Lövheim H. Effects of Pharmacists’ Interventions on Inappropriate Drug Use and Drug-Related Readmissions in People with Dementia-A Secondary Analysis of a Randomized Controlled Trial. Pharmacy (Basel). 2018;6(1):7. doi:10.3390/pharmacy6010007
280. Heikkilä T, Lekander T, Raunio H. Use of an online surveillance system for screening drug interactions in prescriptions in community pharmacies. Eur J Clin Pharmacol. 2006;62(8):661–665. doi:10.1007/s00228-006-0149-4
281. Horn JR, Hansten PD, Chan LN. Proposal for a new tool to evaluate drug interaction cases. Ann Pharmacother. 2007;41(4):674–680. doi:10.1345/aph.1H423
282. Le Couteur DG, Robinson M, Leverton A, et al. Adherence, persistence and continuation with cholinesterase inhibitors in Alzheimer’s disease. Australas J Ageing. 2012;31(3):164–169. doi:10.1111/j.1741-6612.2011.00564.x
283. Cotrell V, Wild K, Bader T. Medication management and adherence among cognitively impaired older adults. J Gerontol Soc Work. 2006;47(3–4):31–46. doi:10.1300/J083v47n03_03
284. Thiruchselvam T, Naglie G, Moineddin R, et al. Risk factors for medication nonadherence in older adults with cognitive impairment who live alone. Int J Geriatr Psychiatry. 2012;27(12):1275–1282. doi:10.1002/gps.3778
285. Maxwell CJ, Stock K, Seitz D, Herrmann N. Persistence and adherence with dementia pharmacotherapy: relevance of patient, provider, and system factors. Can J Psychiatry. 2014;59(12):624–631. doi:10.1177/070674371405901203
286. Elliott RA, Goeman D, Beanland C, Koch S. Ability of older people with dementia or cognitive impairment to manage medicine regimens: a narrative review. Curr Clin Pharmacol. 2015;10(3):213–221. doi:10.2174/1574884710666150812141525
287. Arlt S, Lindner R, Rösler A, von Renteln-kruse W. Adherence to medication in patients with dementia: predictors and strategies for improvement. Drugs Aging. 2008;25(12):1033–1047. doi:10.2165/0002512-200825120-00005
288. Kröger E, Tatar O, Vedel I, et al. Improving medication adherence among community-dwelling seniors with cognitive impairment: a systematic review of interventions. Int J Clin Pharm. 2017;39(4):641–656. doi:10.1007/s11096-017-0487-6
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.