")
Back to Journals » Cancer Management and Research » Volume 13
Advances in the Prediction and Risk Assessment of Lung Cancer-Associated Venous Thromboembolism
Authors Di W , Xu H, Xue T, Ling C
Received 11 July 2021
Accepted for publication 26 October 2021
Published 4 November 2021 Volume 2021:13 Pages 8317—8327
DOI https://doi.org/10.2147/CMAR.S328918
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Beicheng Sun
Wenjuan Di, Haotian Xu, Ting Xue, Chunhua Ling
Department of Respiratory and Critical Care Medicine, The First Hospital Affiliated of Soochow University, Suzhou City, Jiangsu Province, People’s Republic of China
Correspondence: Chunhua Ling
Department of Respiratory and Critical Care Medicine, The First Hospital Affiliated of Soochow University, No. 188, Shizi Street, Gusu District, Suzhou City, Jiangsu Province, People’s Republic of China
Tel +86-18351071532
Email [email protected]
Abstract: According to the most recent data from the National Cancer Center, venous thromboembolism (VTE) has unsurprisingly become one of the most common complications in lung cancer. VTE not only interferes with the equilibrium of the clotting system but it also affects tumor progression and prognosis. For the identification of high-risk patients, many clinical risk assessment models have been developed and validated based on the risk factors found in previous studies. In this review, we will summarize advances in prediction and risk assessment of VTE, with a focus on early diagnosis and therapy, reduction of mortality, and the burden of medical costs in lung cancer patients.
Keywords: lung cancer, venous thromboembolism, risk factor, risk assessment model, anticoagulation
Introduction
Since Armand Trousseau first clarified phlegmasia alba dolens as a sign of internal malignancy in 1865, the association between VTE and cancer has been investigated.1 Cancer was recognized as an independent risk factor of VTE. Cancer patients have a 4- to 7-fold increased risk of VTE compared with the general population.2 Currently, the incidence of lung cancer still ranks first among cancers worldwide, which leads to the largest number of absolute events of lung cancer associated VTE, including pulmonary embolism (PE) and deep venous thrombosis (DVT). VTE incidence can even be as high as 4–20% in these patients, based on epidemiological investigations.3 VTE is usually associated with a poor prognosis for individuals with this disease, which increases morbidity, mortality, and medical costs.
Although the relationship between lung cancer and VTE is well known, the specific underlying mechanisms are multifactorial and still under investigation. Virchow’s triad described 3 factors: venous stasis, activation of blood coagulation, and vascular wall damage, which critically explain the underlying mechanism thrombosis among lung cancer patients.4 In addition, there are many risk factors that contribute to the formation of VTE, which can be divided into three mains categories: tumor-, patient-, and treatment-related factors.5 To date, many randomized controlled trials (RCTs) have developed several risk assessment models suitable for patients with gastrointestinal tumors such as pancreatic cancer and colon cancer. However, a standardized risk assessment model which can be applied to lung cancer is still being explored.
According to the 2019 American Society of Clinical Oncology (ASCO) guidelines, most hospitalized patients with cancer require thromboprophylaxis during hospitalization; however, not all outpatients with cancer are routinely recommended for thromboprophylaxis. Clinicians may now offer low-molecular-weight heparins (LMWHs) to selected high-risk ambulatory patients with lung cancer for thromboprophylaxis.6 Therefore, how to precisely identify lung cancer patients at high risk of VTE is an unmet need in clinical practice. This requires a certain number of valuable biomarkers and risk assessment models to further evaluate and distinguish hazard classifications. Although LMWHs treatment is recommended as prophylactic anticoagulation for high-risk patients, considering the greater risks of bleeding and recurrence, clinicians have many concerns while referring to the guidelines. Direct oral anticoagulants (DOACs) offer a potentially promising treatment option for lung cancer patients with VTE,7 but we should take each individual situations into consideration. Furthermore, for higher bleeding risk than LMWHs, a large quantity of randomized clinical trials is needed to weigh the pros and cons.
In this review, we discuss in detail the epidemiology, pathogenesis, promising biomarkers, risk assessment models, and current treatment options for lung cancer-associated VTE.
Epidemiology and Disease Burden of Lung Cancer-Associated VTE
The California Cancer Registry8 has developed a large population-based study of patients with non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). The cumulative incidence rate of VTE was 3% and 3.4% among the 91,933 newly diagnosed lung cancer patients in the first and second years, respectively. However, in the first six months, the person-time rate was 7.2 events/100 patient-years.8 This provides clinicians with an important reminder that they should pay greater attention to the occurrence of VTE within the first six months after diagnosis of lung cancer.
Recently, Maia et al9 reported that the diagnosis of thromboembolism which occurred in the lung and veins was associated with poor prognosis in patients with lung cancer. In this retrospective study, among the 113 recruited lung cancer patients, 78 (69.0%) exhibited lung and venous thromboembolism after lung cancer diagnosis during the one-year follow-up.
Furthermore, cancer-associated VTE increases the risk of recurrence, major bleeding, and even mortality. Based on total population data from the international registry RIETE (Registry Informatizado de la Enfermedad TromboEmbolica), overall 3-month mortality was 7.9%. Significantly more patients died among those with cancer (26.4%, vs 4.1% in the no-cancer group, p < 0.001).10 As well as increased mortality, healthcare costs are higher in lung cancer patients with VTE than those without. To comprehensively consider these factors, clinicians often face a dilemma in the process of diagnosis and treatment.
Potential Mechanisms of Lung Cancer-Associated VTE
Virchow’s triad originally described three factors that could cause venous thrombosis: disruption of vascular wall integrity, blood hypercoagulability, and stagnation of blood flow.5 Specific mechanisms responsible for thrombosis in lung cancer patients remain controversial; however, there is no doubt that the pathogenesis of lung cancer associated thrombosis is multifactorial. Evidence indicates that patients with lung cancer are in a hypercoagulable state, which further illustrated the possibility of VTE, driven in part by the release of procoagulants, such as tissue factors, from the tumor itself as well as from activated endothelial cells and inflammation cells.11
Among different studies, the most convincing findings indicate that lung cancer cells could produce tissue factor (TF), microparticles (MPs), cancer procoagulant (CP), inflammatory factors, and cytokines, which directly activated the blood-clotting cascade, leading to thrombosis formation.12 The exact mechanisms for the induction of VTE in cancer remain to be fully elucidated, but it is widely acknowledged that TF-bearing microparticles (TF(+) MPs) may play a crucial role.
Campello et al13 identified the role of TF(+) MPs in an observational study. The authors showed that patients with lung cancer had statistically significant higher plasma levels of circulating TF(+) MPs (927 ± 415 MPs/μL) than controls (204 ± 112 MPs/μL; p < 0.001). Meanwhile, Et Tesselaar et al14 reported that overexpression of TF in lung carcinoma cells was the initiator of the clotting cascade. Furthermore, MP-associated TF activity might associate lung cancer with thrombosis and play a critical part in the pathogenesis of thrombosis among lung cancer patients.
Recently, Hsieh et al15 discovered that YC-1 could prevent hypoxia-induced TF in lung cancer cells by inhibiting the p38MAPK/NFkB signaling pathway, independently, from the activity attributed to conventional anticoagulants, and could systemically inhibit blood coagulation. Greater efforts should be taken to investigate this new mechanism, which may provide an alternative new treatment option for lung cancer-associated VTE.
Risk Factors and Biomarkers of Lung Cancer-Associated VTE
Here is the summary of risk factors and biomarkers for lung cancer-associated VTE (Table 1).
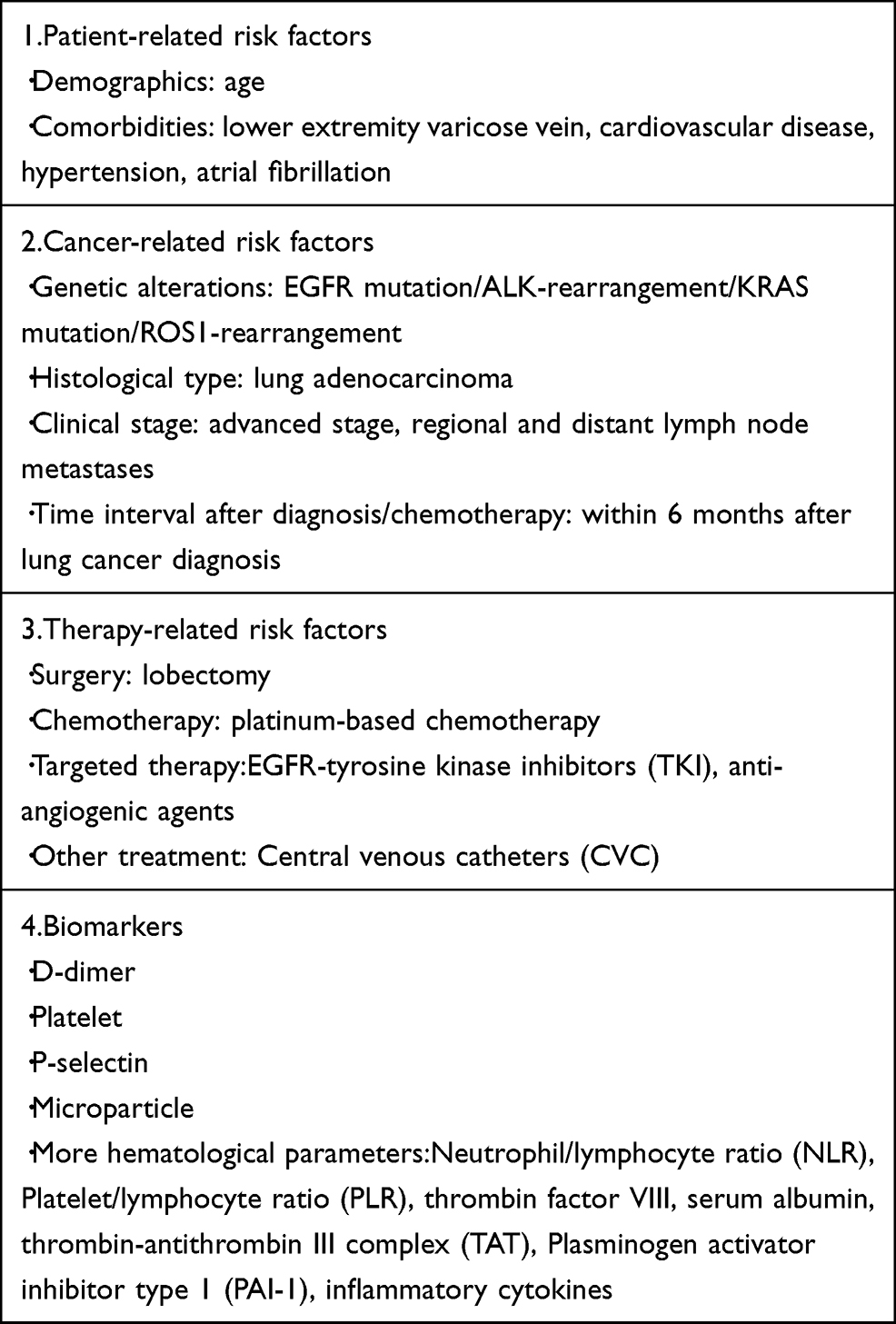 |
Table 1 Summary of Risk Factors and Biomarkers for Lung Cancer-Associated VTE |
Patient-Related Risk Factors
Age
Many studies have reported that older patients with lung cancer or other cancers have an increased risk of developing VTE.16 However, a study investigating the VTE incidence among patients with primary lung cancer showed younger age (≤45 years) was also associated with a higher risk of developing VTE within 1 year of NSCLC diagnosis.17 With the popularization of routine physical examinations, younger lung cancer patients have received greater attention. As indicated by Bigay-Gamé et al18 in a prospective multicenter analysis, the main histopathological type of lung cancer was adenocarcinoma (77%), which was found to be a significant clinical feature among younger lung cancer patients. Given that adenocarcinoma is biologically more aggressive, it acts as an independent risk factor for cancer-associated thrombosis (CAT), while older patients receive thromboprophylaxis more frequently. Age is still a controversial factor for the increased occurrence of VTE in lung cancer and additional investigation is needed to clarify their association.
Comorbidity
A recent study of 283 patients with lung cancer who received systemic therapy showed that patients with lower extremity varicose veins (LVV) had an increased incidence of VTE (50.00% vs 9.89%, P = 0.001) compared to patients without LVV,19 which was consistent with the previous findings reporting the presence of varicose veins in cancer patients could led to an increased risk of developing VTE.20 Whether cardiovascular disease (CVD) risk factors influence VTE occurrence remains unclear. In a retrospective study including 632 patients with newly diagnosed lung cancer, multivariate analysis found that hypertension was significantly associated with VTE in different tumor histology models and different tumor stage models.21 In a retrospective study which was performed on 118 lung cancer patients, atrial fibrillation was significant for VTE development on both the univariate and multivariate analysis.22
Cancer-Related Risk Factors
Genetic Alterations
Cancer is a genetic disease whereby somatic mutations accumulate in cells gradually due to replication errors, chromosome deletions or translocations, or DNA damage, and other mechanisms. Tumor angiogenesis may be affected by the expression of mutated Epidermal Growth Factor Receptor (EGFR) gene, which consistently resulted in overexpression of vascular endothelial growth factor (VEGF) and many other angiogenesis regulators. Conversely, the rate of VTE in patients with ALK-rearranged NSCLC seemed to be higher than previously reported for the general NSCLC population or those without ALK-rearrangements.23 A potential mechanism associated with both thrombosis/hemostasis and ALK-rearranged tumors was that heparin may act as ligand for the ALK receptor.24 A case–control study also described the association of KRAS mutations with an increased risk of VTE (OR: 2.67; 95% CI: 1.12–6.42, P = 0.014) in a NSCLC cohort.25 The authors proposed that the expression of an activated mutant KRAS allele in NSCLC might induce up-regulation of TFs, which also could play a vital role in KRAS-dependent oncogenesis, as they observed in colorectal cancer cell lines. Furthermore, according to data from the METROS trial showed that the incidence of VTE in patients with advanced ROS1-rearranged NSCLC was 3- to 5-fold higher compared to the general population with NSCLC.26 Although the role of these mutations in tumor angiogenesis is currently unknown, and the hazard ratio associated with these mutations in tumor-related thrombosis events has not been determined, further investigations need to be conducted focusing on the genetic mechanisms responsible for neoplastic onset and transformation.
Histological Type
Patients with lung adenocarcinoma seem to have an elevated risk of VTE compared to other histological subtypes. A large cohort study comprising 10,598 individuals with lung cancer after a long follow-up of 14 years revealed that the adenocarcinoma subtype was an independent risk factor of VTE (HR: 2.0; 95% CI: 1.5–2.7, vs squamous cell).27 Accordingly, in a meta-analysis, adenocarcinoma was confirmed to be a risk factor for thrombosis in lung cancer patients (OR: 2.20; 95% CI: 1.68–2.88, p < 0.00001).28
Clinical Stage and Time Interval After Diagnosis
According to the analysis by the Vienna Cancer and Thrombosis Study (CATs), patients with high-grade tumors experienced more thrombotic events than those with low-grade tumors.29 Dickmann et al30 stratified patients into three tumor stages: local, regional, and distant based on the Tumor Node Metastasis (TNM) Classification. The authors showed that patients with regional and distant lymph node metastases had a significantly increased risk of developing VTE. In addition, oppression on blood vessels also posed a burden as described in a case reported by Chin et al,31 a superior vena cava (SVC) syndrome was common in patients with malignant tumors (especially lung cancer). In patients presenting chest distress with persistent dyspnea after remission of facial and upper extremity edema, clinicians should be highly vigilant for PE. A chest computed tomography scan can be used for early screening and diagnosis of PE after treatment of SVC syndrome. Chew et al17 indicated the highest incidence of VTE occurred within 6 months of lung cancer diagnosis, with the overall rates of VTE in the first and second 6 months after cancer diagnosis being 7.2 and 2.4 cases per 100 patient-years, respectively. These findings agreed with the data of other studies indicating that most thromboembolic events in patients with lung cancer undergoing chemotherapy occur within 6 months after diagnosis.3
Therapy-Related Risk Factors
Surgery
A prospective study investigating blood coagulation in lung cancer patients and benign lung disease patients indicated that both patients with lung lobes in a hypercoagulable state pre- and post-operation were prone to thrombosis.32 In a retrospective study, 232 patients undergoing lung cancer surgery were investigated in detail, and of these 5.2% developed VTE after 60 days. Postoperative VTE incidence of patients in the high-risk group was 10.3% based on the Caprini scores.33
Chemotherapy
Patients with unresectable lung cancer receive individualized treatment regimens. In many studies,25,27,34,35 chemotherapy has been identified as a risk factor for VTE events in patients with lung cancer and as described in previous studies, most VTE occurs within 6 months from initiation of chemotherapy. Curiously, VTE is a particularly common event during platinum-based chemotherapy in patients with NSCLC. A large retrospective analysis confirmed an unacceptable incidence (18.1%) of thromboembolic events during cisplatin-based treatment or within 4 weeks after chemotherapy.34
Targeted Therapy
Targeted therapy may be a significant risk factor for VTE in lung cancer patients. The role of EGFR-tyrosine kinase inhibitors (TKI) in VTE development for patients with lung cancer remains unclear. Further, gefitinib and erlotinib do not appear to increase the risk of VTE events.35 A study found patients with lung adenocarcinoma treated with TKI had a reduced risk of VTE compared to other treatment strategies not including TKI (HR: 0.42; 95% CI: 0.29–0.79).25 Nevertheless, several investigations have suggested that anti-angiogenesis drugs, such as bevacizumab, thalidomide, sunitinib, and sorafenib, might also increase risk of VTE in patients with lung cancer.35
Other Treatment
Placement of central venous catheters (CVCs), which are widely used in patients with cancer, may be associated with a greater risk of developing VTE. According to a meta-analysis, patients with a malignancy and had an inserted PICC presented a higher risk of DVT than those with other CVCs (OR: 2.55; 95% CI: 1.54–4.23, P < 0.0001).36 Clinicians should assess the risk of thrombosis in lung cancer patients with PICC after initial diagnosis.
Biomarkers
D-Dimer
D-dimer is a well-known biomarker of thrombosis because it reflects fibrinolytic activity. A negative result for D-dimer has a negative likelihood ratio similar to that of a normal lung scan or negative duplex ultrasonography finding.37 Furthermore, an elevated D-dimer level has been identified as a predictor of VTE and survival in patients with lung cancer in many studies. An investigation evaluating the predictive value of a novel high sensitivity assay for D-dimer measurement in intermediate-risk lung cancer outpatients based on the Khorana score found that a pre-chemotherapy D-dimer level ≥1500 ng/mL could independently predict VTE with an accuracy of 70% (HR: 11; 95% CI: 2.62–46.2, P = 0.001).38 However, older patients who do not have VTE tend to show a false positive result on the D-dimer assay, as D-dimer levels increase with age. Thus, the accuracy of diagnosis could be improved by applying an age adjusted D-dimer cut-off point to exclude VTE in older lung cancer patients.
Platelets
Some investigations have suggested that thrombocytosis might be related to the occurrence of VTE in patients with lung cancer.39,40 An increased platelet count might be an independent predictor of prognosis in patients with primary lung cancer based on the results of many studies,41 though further investigation is needed.
P-Selectin
P-selectin, a cell adhesion molecule which helps platelets and leukocytes attach to the activated vessel wall, appears to be a novel biomarker for VTE.42 A prospective cohort study which evaluated 687 cancer patients (including 86 lung cancer patients) to investigate the predictive value of soluble P-selectin in cancer associated VTE, found that elevated soluble P-selectin levels (≥53.1 ng/mL) correlated with the occurrence of VTE (HR: 2.3; 95% CI: 1.2–4.5, P = 0.009).43 The predictive value of P-selectin for VTE in lung cancer warrants further evaluation.
Microparticles
MPs are small vesicles released from activated cells, injured, or apoptotic cells, and contain surface proteins such as TF and phosphatidylserine. TF(+) MPs, which mainly derived from tumor cells, are procoagulants and may promote the formation of tumor-associated VTE.13 However, the predictive value of MPs and TF(+) MPs in lung cancer associated VTE remains to be clarified. In a case–control study, the results showed that patients with VTE had a statistically higher proportion of MPs and TF(+) MPs than those without VTE in multivariate analysis (OR: 1.153; 95% CI: 1.068–1.245, P < 0.001).20 As a result, TF(+) MP appeared to be a novel marker able to improve the early diagnostic efficiency of tumor-related thrombosis.
Other Hematological Parameters
Hematological parameters have been reported to play different roles in predicting the thrombotic events of lung cancer in the literature. A single-center analysis of the neutrophil/lymphocyte ratio (NLR) and platelet/lymphocyte ratio (PLR) for predicting the risk of VTE in ambulatory cancer patients enrolled 810 cancer out-patients before initiation of a chemotherapy course. The study indicated that high inflammation-based markers (NLR > 3, PLR > 16) was associated with a nearly 2-fold increased VTE risk and patients with high NLR or PLR had the worst 1-year VTE-free survival.44 Furthermore, plasminogen activator inhibitor type 1 (PAI-1), thrombin, factor VIII, fibrin monomer, inflammatory cytokines, serum albumin, thrombin-antithrombin III complex (TAT), and many other hematological biomarkers have been proposed to correlate with the occurrence of lung cancer associated VTE,42 but more evidence is needed to confirm their predictive value.
Risk Assessment Models of Lung Cancer-Associated Venous Thromboembolism
In order to improve the efficiency of prophylaxis, multiple models have been proposed to predict the onset of VTE in lung cancer patients (Table 2). Several factors have been incorporated based on the literature, and biomarkers related to thrombosis should also be taken into consideration. How to accurately select suitable indexes and improve the efficiency of joint diagnosis is the focus of current research.
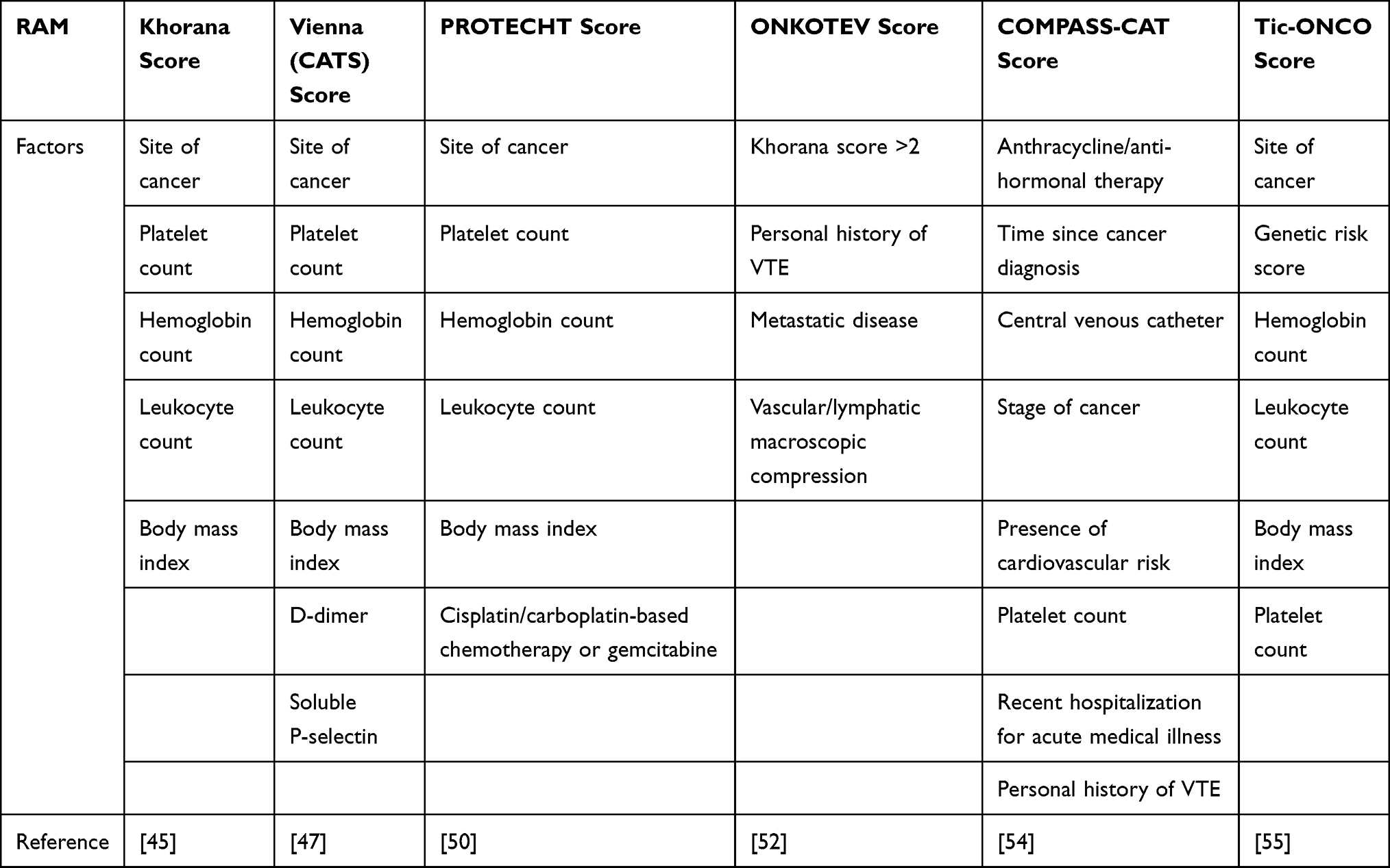 |
Table 2 Summary of Risk Assessment Models for Lung Cancer-Associated VTE |
Currently, a well-known risk assessment model (RAM), the Khorana risk score (KRS), which stratifies cancer patients into different risk levels and identifies a high-risk group for thromboprophylaxis, is the most commonly used.45 Five baseline clinical and laboratory variables are evaluated in this model: site of cancer, platelet count, hemoglobin count and/or use of erythropoiesis-stimulating agents, leukocyte count, and the body mass index. In addition to the cancer site, which is assigned two points, each impact factor is assigned one point. A KRS ≥3 is considered to indicate a high-risk. However, when Mansfield et al46 tried to validate the KRS among lung cancer patients, they frustratingly determined that although a high KRS was apparently associated with all-cause mortality, it was not predictive of VTE.
Since KRS model is not applicable to lung cancer, D-dimer and soluble P-selectin were added in the Vienna Cancer and Thrombosis Study (CATS), the prediction of VTE was greatly improved.47 Ay et al48 subsequently assessed the prognostic value of D-dimer levels in a prospective and observational cohort study. Thus, CATS tends to be a new research focus, which may more efficiently recognize cancer patients who are likely to have high risk of developing VTE, as indicated by various biomarkers (such as D-dimer, soluble P-selectin, and platelet count.)49
Although a high risk of VTE is supported by the KRS and the Vienna CATS, routine thromboprophylaxis is still not recommended by ASCO guidelines.6 As a result, additional risk assessment models are needed to precisely predict the VTE in cancer patients. In the past few years, new models, such as the PROTECHT score, the ONKOTEV score, have been designed and published. Furthermore, the COMPASS-CAT score and the Tic-ONCO score have also been proposed. Ay et al50 performed a prospective and observational cohort study to improve the predictive performance of the KRS. The original KRS was modified by adding chemotherapy agents in the PROTECHT score, such as platinum-based regimens and gemcitabine, and biomarkers, which significantly improved the ability to identify high risk of VTE in cancer patients. Subsequently, in a prospective cohort study, a multivariable analysis showed that patients with high-risk scores were more likely to develop VTE when assessed using the Vienna CATS score and the PROTECHT.51 Cella et al52 proposed a new risk assessment model, the ONKOTEV score, which added the variables metastatic disease, the compression of the tumor mass and the history of previous VTE with a KRS >2. Considering the vascular endothelial injury mechanisms caused by tumor compression, Godinho et al53 suggested the ONKOTEV score was a more suitable indicator for selecting cancer patients for primary thromboprophylaxis. Despite the development of these new models, most of them are applicable to scoring the initial phase of lung cancer treatment, more external validation tests are needed. In recent years, the most popular model is the COMPASS-CAT,54 a risk assessment tool that incorporates the patient, tumorigenesis, tumor therapy, and even tumor comorbidities. Compared with the relatively authoritative KRS, the COMPASS-CAT score incorporated more influential factors, compensating for the shortcomings of the KRS. Furthermore, the score is not only applicable to pre-treatment screening of tumors, but allows dynamic monitoring of tumor development and risk trends during treatment.
Rupa-Matysek et al22 compared the following VTE risk assessment models: the Khorana risk score (KRS), the PROTECHT score, the CONKO score and the COMPASS-cancer-associated thrombosis score (COMPASS-CAT) in lung cancer patients. Only the COMPASS-CAT score was able to fully recognize patients who developed VTE during a median of 2.5 months from diagnosis, and was the most valuable in discriminating high- and low-risk of VTE development in lung cancer patients. In addition to the classical VTE risk factors, the COMPASS-CAT score incorporates new predictive variables, such as time since cancer diagnosis, cancer stage, cardiovascular risk, treatment with antihormonal therapy or anthracyclines, and personal medical history of VTE. The inclusion of these factors compensates for failures in the Khorana score. This likewise extends its applicability, not only in the initial phase of treatment (as used in the Khorana score) but also at any time after initiation of cancer-directed therapy, where it has potential value.
Research in recent years has focused on cancer therapy, which likely represents a potential risk for enhancing the incidence of thromboembolic diseases. Currently, the role of genetic risk factors, such as EGFR and ALK mutations, have been recognized to play major role in lung cancer pathogenesis. Consequently, greater efforts should address the validity of the TiC-Onco risk score, which focuses on clinical and genetic risk factors for cancer associated VTE55 in the modern epoch of lung cancer therapy. As a new risk assessment score which considers both genetic and therapeutic factors, it may play a major role in predicting the occurrence of VTE in lung cancer patients.
Treatment and Prophylaxis of Lung Cancer-Associated VTE
Treatment of VTE
In general, lung cancer patients have a higher incidence of thrombotic events during both disease progression and treatment. Many evidence-based guidelines on the treatment of VTE in lung cancer patients have been already published.6,56–58 Furthermore, a large number of RCTs evaluating the treatment of lung cancer associated VTE have reached an agreement that LMWHs represent the recommended pharmacologic prophylaxis agent for initial and long-term treatment.57 In addition, recent RCTs have demonstrated that DOACs could represent an alternative option.58 However, whether lung cancer patients should receive routine anticoagulation therapy is still under investigation and requires more prospective studies. Management of VTE in patients with lung cancer is currently a therapeutic challenge and remains controversial worldwide.
Initial Treatment
According to the 2019 ASCO guidelines, options for initial anticoagulation therapy include LMWHs, unfractionated heparin(UFH), fondaparinux, or rivaroxaban.6 With regard to parenteral anticoagulation therapy, for patients without absolute contraindications, it is preferred to select LMWHs as initial anticoagulant therapy. In a recent meta-analysis, Robertson et al59 determined that mortality was significantly lower in patients treated with LMWHs than those treated with UFH during the initial treatment period (OR: 0.53; 95% CI: 0.33–0.85, p = 0.009). Moreover, in another meta-analysis, Hakoum et al57 found that LMWHs reduced mortality at three months compared to UFH treatment (RR: 0.66; 95% CI, 0.40–1.10); however, it did not show any significant increase or decrease when considering VTE recurrence (RR: 0.69; 95% CI: 0.27–1.76).
Given the number of new investigations, a challenging and promising viewpoint has been proposed by researchers: Should DOACs be used as initial thromboprophylaxis therapy in lung cancer patients? Recently, Howlett et al60 compared both efficacy and tolerance of DOACs for lung cancer patients. Despite the large decrease in medical costs accompanies the use of DOACs, and considering the associated adverse medication interactions and bleeding risks, the authors preferred not to recommend DOACs for lung cancer patients with VTE. In a recent review comparing old and new therapies on lung cancer-associated VTE, the study61 concluded that cancer type, stage, prognosis, and bleeding risk should be all taken into consideration when beginning anticoagulation therapy. In addition, a sub-analyses in this review showed that there was a decrease on bleeding and thromboembolic events when comparing warfarin with DOACs, indicating a particularly promising future for anticoagulation therapy. Based on lessons from our predecessors when choosing appropriate therapy for lung cancer patients who develop or experience recurrent VTE, all factors should be taken into consideration to establish individually adequate therapeutic anticoagulation. Furthermore, we need more RCTs concentrating on efficacy and bleeding complications to clarify the role of DOACs in lung cancer patients with VTE.
Duration of Anticoagulation
For lung cancer patients, VTE recurrence after initial treatment is significantly correlated with morbidity and mortality. The balance between the risk of recurrence and long-term anticoagulation is essential for overall survival of lung cancer patients. As discussed in the latest studies, this approach can maximize benefits when treated with anticoagulants continuously for at least six months after diagnosis of cancer-associated thrombosis.62
With the development of risk assessment models, it seems to be more convenient to predict and timely diagnose VTE in lung cancer patients. Nonetheless, the question remains on how to better treat and manage lung cancer associated VTE? No available data can answer this question at the moment.
Discussion
In the etiology statistics released by the National Cancer Center, lung cancer still ranks first among cancers.63 Thus, the incidence of VTE events remains high in patients with lung cancer. In addition, as mortality and medical cost increase, epidemiologists and clinicians have placed greater attention on finding a suitable solution. The main difficulties remain how to accurately diagnose VTE in patients with lung cancer. Regrettably, many patients die due to VTE not diagnosed in a timely manner, and in some cased VTE was determined at autopsy. With the development of medical science in the past years, technologies such as computed tomography angiography and Doppler venous ultrasound, have greatly improved diagnostic efficiency in identifying patients with high clinical suspicion of VTE. In order to achieve a better overall survival rate, it is imperative to diagnose VTE of lung cancer patients as early as possible.
The risk factors of lung cancer-associated VTE are mainly divided into four categories: cancer-related factors, patient-related factors, treatment-related factors, and biomarkers. The histological type plays an important role in cancer-related factors, for patients with lung adenocarcinoma are these patients are more likely to develop VTE when compared to those with other histological types. Meanwhile, recent evidence indicates that lung adenocarcinoma patients harboring ALK rearrangement or ROS1 mutations are more likely to develop thrombosis within 6 months of diagnosis, which means genetic alterations might be closely related with lung cancer-associated VTE.64 In addition, both clinical stage and time interval after diagnosis are implicated in the occurrence of VTE among lung cancer patients. Regarding patient-related risk factors, comorbidities occupy the top priority. Lung cancer patients with comorbidities, such as CVD present an elevated risk of VTE. Thus, poor performance status might contribute to increase thrombosis events. Recent RCTs and studies have demonstrated that different treatment options might also affect the occurrence of VTE, especially chemotherapy with platinum or targeted therapy with anti-angiogenic drugs.
Although there are many factors that can contribute to the formation of VTE in lung cancer patients, current studies have shown that VTE can be predicted by biomarkers. First of all, D-dimer is a well-known biomarker of thrombosis because it is an indicator of fibrinolytic activity. Furthermore, the significant changes in plasma D-dimer levels reflect not only thrombus formation but also tumor progression.65 Thus, regular evaluation of D-dimer levels may be the easiest approach to monitor thrombus formation, followed by timely imageology examinations in high-risk patients. Furthermore, TF(+) MPs play a predominant role in predicting VTE formation, which remains the main mechanism of thrombosis generation and can directly activate coagulation. With the aim of improving prediction of VTE in lung cancer patients, thousands of large-scale multi-center studies have been conducted, focusing on the design and validation of risk assessment models. So far, the KRS has been most widely used. Disappointingly, evidence-based studies have demonstrated its unsuitability for lung cancer patients. Thus, another risk assessment model, the COMPASS-CAT score, has been confirmed to be most appropriate for lung cancer patients. In addition, we should place greater attention on the TiC-Onco risk score, which considers the impact of genetic risk factors on clinical outcomes. Thus, an effective risk assessment model could greatly improve the diagnostic efficiency of VTE in lung cancer patients. We still need to invest more efforts and time to achieve this goal.
Evidence-based ASCO guidelines recommend LMWHs as pharmacologic prophylaxis for initial and long-term treatment.6 However, recurrence after initial treatment is significantly correlated with morbidity and mortality for lung cancer patients, and is also associated with a substantial medical burden. The duration of anticoagulation treatment should also be considered during therapy. As for whether to offer prophylaxis for VTE, clinicians should make a careful assessment prior to initiating therapy.
Conclusion
This review summarized the available information on the pathogenesis, risk factors, risk assessment models, treatment, and prevention options of VTE in patients with lung cancer. Although substantial literatures is available, there are still many problems to be resolved. The exact pathogenesis of VTE in lung cancer, as well as its accurate prediction still requires further investigation. In the future, with the development a more accurate risk prediction model, clinicians will be more confident in managing CAT in lung cancer patients.
Abbreviations
VTE, venous thromboembolism; PE, pulmonary embolism; DVT, deep venous thrombosis; RCTs, randomized controlled trials; LMWHs, low-molecular-weight heparins; DOACs, direct oral anticoagulants; CATS, Cancer and Thrombosis Study; NSCLC, non-small cell lung cancer; SCLC, small cell lung cancer; TF (+) MPs, tissue factor-positive microparticles; AC, adenocarcinoma; LVV, lower extremity varicose vein; CVD, cardiovascular disease; EGFR, Epidermal Growth Factor Receptor; ALK, Anaplastic Lymphoma Kinase; VEGF, vascular endothelial growth factor; TKI, tyrosine kinase inhibitors; CVCs, central venous catheters; NLR, neutrophil/lymphocyte ratio.
Disclosure
The authors declare that they have no competing interests.
References
1. Büyükçelik A, Akbulut H. Thromboembolism in patients with cancer. Turk J Haematol. 2004;21(1):1.
2. Noble S, Pasi J. Epidemiology and pathophysiology of cancer-associated thrombosis. Br J Cancer. 2010;102(Suppl 1):S2–S9. doi:10.1038/sj.bjc.6605599
3. Suzuki T, Fujino S, Inaba S, et al. Venous thromboembolism in patients with lung cancer. Clin Appl Thromb Hemost. 2020;26:1076029620977910. doi:10.1177/1076029620977910
4. Kushner A, West WP, Pillarisetty LS. Virchow triad. In: StatPearls. Treasure Island (FL): StatPearls Publishing; September 13, 2020.
5. Nasser NJ, Fox J, Agbarya A. Potential mechanisms of cancer-related hypercoagulability. Cancers. 2020;12(3):566. doi:10.3390/cancers12030566
6. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(5):496–520. doi:10.1200/JCO.19.01461
7. Lyman GH, Kuderer NM. Clinical practice guidelines for the treatment and prevention of cancer-associated thrombosis. Thromb Res. 2020;191(Suppl 1):S79–S84. doi:10.1016/S0049-3848(20)30402-3
8. Pages P, Cottenet J, Mariet A, Bernard A, Quantin C. In-hospital mortality following lung cancer resection: nationwide administrative database. Eur Respir J. 2016;47(6):1809–1817. doi:10.1183/13993003.00052-2016
9. Maia R, Neves I, Morais A, Queiroga H. Venous and lung thromboembolism in the context of lung cancer: clinical manifestations, risk factors and prognosis. Acta Med Port. 2019;32(10):
10. Gussoni G, Frasson S, La Regina M, Di Micco P, Monreal M; RIETE Investigators. Three-month mortality rate and clinical predictors in patients with venous thromboembolism and cancer. Findings from the RIETE registry. Thromb Res. 2013;131(1):24–30. doi:10.1016/j.thromres.2012.10.007
11. Canale ML, Bisceglia I, Lestuzzi C, Parrini I; ANMCO Cardio-Oncology Task Force. Arterial thrombosis in cancer: spotlight on the neglected vessels. Anticancer Res. 2019;39(9):4619–4625. doi:10.21873/anticanres.13642
12. Date K, Ettelaie C, Maraveyas A. Tissue factor-bearing microparticles and inflammation: a potential mechanism for the development of venous thromboembolism in cancer. J Thromb Haemost. 2017;15(12):2289–2299. doi:10.1111/jth.13871
13. Campello E, Spiezia L, Radu CM, et al. Endothelial, platelet, and tissue factor-bearing microparticles in cancer patients with and without venous thromboembolism. Thromb Res. 2011;127(5):473–477. doi:10.1016/j.thromres.2011.01.002
14. Tesselaar ME, Osanto S. Risk of venous thromboembolism in lung cancer. Curr Opin Pulm Med. 2007;13(5):362–367.
15. Hsieh KY, Wei CK, Wu CC. YC-1 prevents tumor-associated tissue factor expression and procoagulant activity in hypoxic conditions by inhibiting p38/NF-κB signaling pathway. Int J Mol Sci. 2019;20(2):244. doi:10.3390/ijms20020244
16. Roselli M, Riondino S, Mariotti S, La Farina F, Ferroni P, Guadagni F. Clinical models and biochemical predictors of VTE in lung cancer. Cancer Metastasis Rev. 2014;33(2–3):771–789. doi:10.1007/s10555-014-9500-x
17. Chew HK, Davies AM, Wun T, Harvey D, Zhou H, White RH. The incidence of venous thromboembolism among patients with primary lung cancer. J Thromb Haemost. 2008;6(4):601–608. doi:10.1111/j.1538-7836.2008.02908.x
18. Bigay-Gamé L, Bota S, Greillier L, et al.; GFPC Investigators. Characteristics of lung cancer in patients younger than 40 years: a prospective multicenter analysis in France. Oncology. 2018;95(6):337–343. doi:10.1159/000489784
19. Konigsbrugge O, Lotsch F, Reitter EM, et al. Presence of varicose veins in cancer patients increases the risk for occurrence of venous thromboembolism. J Thromb Haemost. 2013;11(11):1993–2000. doi:10.1111/jth.12408
20. Liu Y, Gu Y, Yi F, Cao B. [Retrospective analysis of risk factors for venous thromboembolism in 283 patients with lung cancer during systemic therapy]. Zhongguo Fei Ai Za Zhi. 2019;22(7):419–426. Chinese
21. Zhang Y, Yang Y, Chen W, et al. Hypertension associated with venous thromboembolism in patients with newly diagnosed lung cancer. Sci Rep. 2016;6(1):19603. doi:10.1038/srep19603
22. Rupa-Matysek J, Lembicz M, Rogowska EK, Gil L, Komarnicki M, Batura-Gabryel H. Evaluation of risk factors and assessment models for predicting venous thromboembolism in lung cancer patients. Med Oncol. 2018;35(5):1. doi:10.1007/s12032-018-1120-9
23. Zer A, Moskovitz M, Hwang DM, et al. ALK-rearranged non-small-cell lung cancer is associated with a high rate of venous thromboembolism. Clin Lung Cancer. 2017;18(2):156–161. doi:10.1016/j.cllc.2016.10.007
24. Murray PB, Lax I, Reshetnyak A, et al. Heparin is an activating ligand of the orphan receptor tyrosine kinase ALK. Sci Signal. 2015;8(360):360. doi:10.1126/scisignal.2005916
25. Corrales-Rodriguez L, Soulieres D, Weng X, Tehfe M, Florescu M, Blais N. Mutations in NSCLC and their link with lung cancer-associated thrombosis: a case-control study. Thromb Res. 2014;133(1):48–51. doi:10.1016/j.thromres.2013.10.042
26. Chiari R, Ricciuti B, Landi L, et al. ROS1-rearranged non-small-cell lung cancer is associated with a high rate of venous thromboembolism: analysis from a Phase II, prospective, multicenter, two-arms trial (METROS). Clin Lung Cancer. 2020;21(1):15–20. doi:10.1016/j.cllc.2019.06.012
27. Walker AJ, Baldwin DR, Card TR, Powell HA, Hubbard RB, Grainge MJ. Risk of venous thromboembolism in people with lung cancer: a cohort study using linked UK healthcare data. Br J Cancer. 2016;115(1):115–121. doi:10.1038/bjc.2016.143
28. Zhang M, Wu S, Hu C. Do lung cancer patients require routine anticoagulation treatment? A meta-analysis. J Int Med Res. 2020;48(1):300060519896919.
29. Ahlbrecht J, Dickmann B, Ay C, et al. Tumor grade is associated with venous thromboembolism in patients with cancer: results from the Vienna Cancer and Thrombosis Study. J Clin Oncol. 2012;30(31):3870–3875. doi:10.1200/JCO.2011.40.1810
30. Dickmann B, Ahlbrecht J, Ay C, et al. Regional lymph node metastases are a strong risk factor for venous thromboembolism: results from the Vienna Cancer and Thrombosis Study. Haematologica. 2013;98(8):1309–1314. doi:10.3324/haematol.2012.073338
31. Chin CG, Yeh JS, Lin YK, Tam WC. Superior vena cava syndrome complicated with acute pulmonary thromboembolism in a patient with lung cancer. J Cardiol Cases. 2018;17(1):9–11. doi:10.1016/j.jccase.2017.08.004
32. Xu C, Fu X. [The changes of blood coagulation in surgical patients with lung cancer]. Zhongguo Fei Ai Za Zhi. 2010;13(2):136–139. Chinese.
33. Hachey KJ, Hewes PD, Porter LP, et al. Caprini venous thromboembolism risk assessment permits selection for postdischarge prophylactic anticoagulation in patients with resectable lung cancer. J Thorac Cardiovasc Surg. 2016;151(1):37–44.e1. doi:10.1016/j.jtcvs.2015.08.039
34. Moore RA, Adel N, Riedel E, et al. High incidence of thromboembolic events in patients treated with cisplatin-based chemotherapy: a large retrospective analysis. J Clin Oncol. 2011;29(25):3466–3473. doi:10.1200/JCO.2011.35.5669
35. Salla E, Dimakakos EP, Tsagkouli S, et al. Venous thromboembolism in patients diagnosed with lung cancer. Angiology. 2016;67(8):709–724. doi:10.1177/0003319715614945
36. Chopra V, Anand S, Hickner A, et al. Risk of venous thromboembolism associated with peripherally inserted central catheters: a systematic review and meta-analysis. Lancet. 2013;382(9889):311–325. doi:10.1016/S0140-6736(13)60592-9
37. Ferroni P, Martini F, Portarena I, et al. Novel high-sensitive D-dimer determination predicts chemotherapy-associated venous thromboembolism in intermediate risk lung cancer patients. Clin Lung Cancer. 2012;13(6):482–487. doi:10.1016/j.cllc.2012.03.005
38. Gong CY, Li ZW, Zhou DX, et al. [Risk factors of lung cancer complicated with symptomatic venous thromboembolism]. Zhonghua Jie He He hu Xi Za Zhi. 2016;39(6):454–458. Chinese.
39. Kadlec B, Skrickova J, Merta Z, Dusek L, Jarkovsky J. The incidence and predictors of thromboembolic events in patients with lung cancer. Sci World J. 2014;2014:125706. doi:10.1155/2014/125706
40. Bai Y, Chen H. [Biomarkers and risk assessment scores for prediction of chemotherapy-associated venous thromboembolism in lung cancer patients]. Zhonghua Jie He He Hu Xi Za Zhi. 2015;38(10):767–769. Chinese.
41. Vitale C, D’Amato M, Calabro P, Stanziola AA, Mormile M, Molino A. Venous thromboembolism and lung cancer: a review. Multidiscip Respir Med. 2015;10(1):28. doi:10.1186/s40248-015-0021-4
42. Anghel L, Sascau R, Radu R, Statescu C. From classical laboratory parameters to novel biomarkers for the diagnosis of Venous Thrombosis. Int J Mol Sci. 2020;21(6):1920. doi:10.3390/ijms21061920
43. Ay C, Simanek R, Vormittag R, et al. High plasma levels of soluble P-selectin are predictive of venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). Blood. 2008;112(7):2703–2708. doi:10.1182/blood-2008-02-142422
44. Ferroni P, Riondino S, Formica V, et al. Venous thromboembolism risk prediction in ambulatory cancer patients: clinical significance of neutrophil/lymphocyte ratio and platelet/lymphocyte ratio. Int J Cancer. 2015;136(5):1234–1240. doi:10.1002/ijc.29076
45. Khorana AA, Kuderer NM, Culakova E, Lyman GH, Francis CW. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008;111(10):4902–4907. doi:10.1182/blood-2007-10-116327
46. Mansfield AS, Tafur AJ, Wang CE, Kourelis TV, Wysokinska EM, Yang P. Predictors of active cancer thromboembolic outcomes: validation of the Khorana score among patients with lung cancer. J Thromb Haemost. 2016;14(9):1773–1778. doi:10.1111/jth.13378
47. Thaler J, Ay C, Pabinger I. Venous thromboembolism in cancer patients - risk scores and recent randomised controlled trials. Thromb Haemost. 2012;108(6):1042–1048.
48. Ay C, Dunkler D, Pirker R, et al. High D-dimer levels are associated with poor prognosis in cancer patients. Haematologica. 2012;97(8):1158–1164. doi:10.3324/haematol.2011.054718
49. Königsbrügge O, Pabinger I, Ay C. Risk factors for venous thromboembolism in cancer: novel findings from the Vienna Cancer and Thrombosis Study (CATS). Thromb Res. 2014;133(Suppl 2):S39–S43. doi:10.1016/S0049-3848(14)50007-2
50. Ay C, Dunkler D, Marosi C, et al. Prediction of venous thromboembolism in cancer patients. Blood. 2010;116(24):5377–5382. doi:10.1182/blood-2010-02-270116
51. van Es N, Di Nisio M, Cesarman G, et al. Comparison of risk prediction scores for venous thromboembolism in cancer patients: a prospective cohort study. Haematologica 2017;102(9):1494–1501. doi:10.3324/haematol.2017.169060
52. Cella CA, Di Minno G, Carlomagno C, et al. Preventing Venous Thromboembolism in ambulatory cancer patients: the ONKOTEV Study. Oncologist. 2017;22(5):601–608. doi:10.1634/theoncologist.2016-0246
53. Godinho J, Casa-Nova M, Moreira-Pinto J, et al. ONKOTEV score as a predictive tool for thromboembolic events in pancreatic cancer–A retrospective analysis. Oncologist. 2019;25(2):e284.
54. Spyropoulos AC, Eldredge JB, Anand LN, et al. External validation of a venous thromboembolic risk score for cancer outpatients with solid tumors: the COMPASS-CAT venous thromboembolism risk assessment model. Oncologist 2020;25(7):e1083–e1090. doi:10.1634/theoncologist.2019-0482
55. Muñoz Martín AJ, Ortega I, Font C, et al. Multivariable clinical-genetic risk model for predicting venous thromboembolic events in patients with cancer. Br J Cancer. 2018;118(8):1056–1061. doi:10.1038/s41416-018-0027-8
56. Kuderer NM, Poniewierski MS, Culakova E, et al. Predictors of venous thromboembolism and early mortality in lung cancer: results from a global prospective study (CANTARISK). Oncologist. 2018;23(2):
57. Hakoum MB, Kahale LA, Tsolakian IG, et al. Anticoagulation for the initial treatment of venous thromboembolism in people with cancer. Cochrane Database Syst Rev. 2018;1(1):CD006649.
58. Wojtukiewicz MZ, Skalij P, Tokajuk P, et al. Direct oral anticoagulants in cancer patients. Time for a change in paradigm. Cancers. 2020;12(5):E1144. doi:10.3390/cancers12051144
59. Robertson L, Jones LE. Fixed dose subcutaneous low molecular weight heparins versus adjusted dose unfractionated heparin for the initial treatment of venous thromboembolism. Cochrane Database Syst Rev. 2017;2(2):CD001100.
60. Howlett J, Benzenine E, Fagnoni P, Quantin C. Are direct oral anticoagulants an economically attractive alternative to low molecular weight heparins in lung cancer associated venous thromboembolism management? J Thromb Thrombolysis. 2020;50(3):642–651. doi:10.1007/s11239-020-02047-1
61. Rhea IB, Lyon AR, Fradley MG. Anticoagulation of cardiovascular conditions in the cancer patient: review of old and new therapies. Curr Oncol Rep. 2019;21(5):45. doi:10.1007/s11912-019-0797-z
62. Khalil L, Wong HS, Keeling DM, Desborough MJ. Venous thromboembolism: risk of recurrence and long-term anticoagulation. Br J Hosp Med. 2015;76(2):72–77. doi:10.12968/hmed.2015.76.2.72
63. Zhang S, Sun K, Zheng R, et al. Cancer incidence and mortality in China, 2015. J Natl Cancer Center. 2021;1(1):2–11. doi:10.1016/j.jncc.2020.12.001
64. Orly L, Connors Jean M, Hanny A-S. Impact of tumor genomic mutations on Thrombotic risk in cancer patients. Cancers. 2020;12:1958.
65. Wang P, Zhao H, Zhao Q, et al. Risk factors and clinical significance of D-dimer in the development of postoperative venous thrombosis in patients with lung tumor. Cancer Manag Res. 2020;12:5169–5179. doi:10.2147/CMAR.S256484
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.