")
Back to Journals » Advances in Medical Education and Practice » Volume 8
Advances in medical education and practice: role of massive open online courses
Authors Goldberg LR , Crocombe LA
Received 4 April 2017
Accepted for publication 29 June 2017
Published 21 August 2017 Volume 2017:8 Pages 603—609
DOI https://doi.org/10.2147/AMEP.S115321
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Lynette R Goldberg,1 Leonard A Crocombe2
1Wicking Dementia Research and Education Centre, Faculty of Health, 2Centre for Rural Health, Faculty of Health Sciences, University of Tasmania, Hobart, TAS, Australia
Abstract: Massive open online courses (MOOCs) are increasingly available in the area of health and medicine. These MOOCs are offered through various commercial and noncommercial online platforms. When offered through reputable institutions, they can provide valuable access to reliable information without the constraints of time, geographical location, or level of education. Most current courses appear introductory in nature. In its drive for quality health care, the National Academy of Medicine has prioritized a focus on known chronic care conditions. Many of these conditions are shared internationally. Among its initiatives, the academy encourages consumer and professional groups, patients, clinicians, health care organizations, and universities to work together to identify evidence-based care processes consistent with best practices, organize major prevention programs to target key associated health risk behaviors, and develop systems to measure and evaluate improvements in the provision of patient- and family-centered health care. Carefully designed and collaboratively developed MOOCs would appear a valuable resource to contribute to these initiatives. Such MOOCs can, 1) increase the health literacy of the public with regard to the prevention and treatment of known chronic care conditions, 2) provide ready access to continuing professional, and interprofessional, education, and 3) explore innovative teaching models for student learning focused on patient- and family-centered care. MOOCs would also appear helpful to facilitate effective communication among international communities of patients and clinicians, including student clinicians, with shared interests. Further, the accumulation of MOOC data through large-scale measurement and analysis, obtained nationally and internationally, has the potential to assist in greater understanding of the risk for diseases and their prevention, with this translating into medical education, and authentic, patient- and family-centered methods for student learning. This paper explores these issues.
Keywords: interprofessional education, medical education, medical practice, massive open online course, MOOC, patient (or person-) and family-centered care, quality health care
Introduction
The purpose of this narrative review is to stimulate discussion about the role of massive open online courses (MOOCs) as innovative tools in medical education and practice to ensure effective, quality, equitable, and patient- and family-centered health care. Published papers on medically-related MOOCs were identified from searches on PubMed, Google Scholar, CINAHL, and Cochrane databases. MOOCs in general have proliferated since 2012, based on the innovative work of Siemens1 and Downes2 who showed that a large number of participants (frequently thousands = massive) could access, network, and share information rapidly through an authentic, meaningful, and free (open) online learning environment (course). Before delving into how MOOCs may play a role in medical education and practice for health care professionals, academics, policy developers, and people in need of medical care, it is important to understand what is needed for quality health care.
Achieving quality health care
In 2001, the Institute of Medicine (IOM; now the National Academy of Medicine) in the United States published a pivotal paper, Crossing the quality chasm, focusing attention on six essential aims of health care: services provided must be safe, effective, patient-centered, timely, efficient, and equitable.3 To achieve these aims and address evident gaps in health care, the IOM advocated redesigned systems to improve the quality of medical care, and thus medical education. Principles guiding system redesign focused on care that was: 1) evidence-based to translate scientific knowledge into practice, 2) able to address individual needs of patients and families, 3) transparent to enable patients and their families to make informed choices, 4) proactive rather than reactive, and 5) characterized by collaborative, interdisciplinary, integrated work, and effective communication.3
The importance of ongoing communication between all health care providers and the people in need of care resulted in renewed recognition of the value of interprofessional education (IPE) for medical, paramedical, nursing, pharmacy, dental, allied and public health, and social work students in preparation for effective interprofessional practice (IPP).4 Although the nuance may be subtle, the term “interprofessional” is preferred to “interdisciplinary” due to its focus on collaborative relationships that address both education and practice as preprofessional students learn with, from, and about each other.5 This learning occurs through scaffolded opportunities that expose students to IPE, engage them in integrated work, and develop their competence for IPP.5–7 Data show that IPE experiences increase students’ confidence and readiness for effective teamwork and shared decision-making in professional practice.8 Results from eight randomized controlled trials have documented positive outcomes in varying aspects of health care, including increased practitioner competencies and patient satisfaction.4
While much has been achieved to improve the quality and safety of health care since the publication of the IOM’s 2001 report, there is still work to be performed. A systematic analysis of evidence from 18 international studies, based on the IOM’s six aims, documented that care redesign has not been so systematic; more robust research designs need to be implemented, and care design focused on patient- and family-centered care needs to be strengthened.9,10 In a recent report developed for the National Academy of Medicine, Frampton et al11 expressed concern at the ongoing difficulty in changing the culture of medical education and practice to focus on patient- and family-centered care, communication, and empathy – core competencies in modern health care.12 These investigators argued that the comprehensive framework needed to ensure safe, effective, patient-centered, timely, efficient, and equitable health care must include the lived experiences of the people who are ill, or at-risk, and those who care for them. This focus on patient (or person-) centeredness will facilitate patients’ active engagement in their care, identify meaningful and functional outcomes that are not solely practitioner driven, and facilitate the development of a patient- and family-centered evidence base that is integral to effective, quality care.8,11–14 Contrasting this approach to evidence-based care focused on more controlled experimental designs, some have termed it “practice-based evidence.”15 Both approaches are important in maintaining and evaluating quality health care. To develop and establish a culture of patient-centered care, Frampton et al11 stressed the need for innovative and inclusive training for patients, their families, and health care personnel. While there are valuable case-based reports of the effectiveness of patient-centered care, Singer et al16 advocated continued work based on the theory of collective learning – how learning from leadership and effective communication among groups and organizations can establish a person-centered framework to promote the quality and safety of health care beyond individual or local levels.
Prioritizing chronic care conditions in facilitating quality health care
In its drive for quality health care, the National Academy of Medicine has prioritized a focus on known chronic care conditions to make the best use of available resources. The academy encourages health care organizations, consumer and professional groups, patients, clinicians, private and public payment providers, and other stakeholders to work together to: 1) identify evidence-based care processes consistent with best practices, 2) organize major prevention programs to target key associated health risk behaviors, 3) develop and provide a supportive outcomes-based information infrastructure, 4) align reimbursement policies with the goal of quality improvement, and 5) develop systems to measure and evaluate improvements in the provision of health care.3
Currently in Australia, the top five causes of death are: heart disease, dementia, cerebrovascular disease (stroke), lung cancer, and chronic respiratory disease.17 In America, the top five causes of death are heart disease, malignant cancers (particularly lung cancer), chronic respiratory disease, accidents (unintentional injuries), and cerebrovascular disease; dementia is sixth.18 Dementia, a progressive and terminal condition, is now accepted as one of the major causes of disability and dependency among older people and a global public health issue.19 There is particular concern about the increasing number of people with dementia and associated medical conditions in developing countries.20 Heart disease, stroke, chronic obstructive respiratory disease, lung cancer (and related cancers of the airway), diabetes, and obesity also remain global concerns.21
The characteristics and contributions of MOOCs
The IOM recognized the inherent potential of the Internet to transform health care, particularly in addressing known chronic care conditions, and information is now widely available to consumers, students, and health care providers through an increasing number of health- and medicine-related MOOCs. These MOOCs are offered through various commercial and noncommercial online platforms and, when offered through reputable institutions, can provide valuable access to reliable information. Figure 1 shows the potential contributions of health- and medicine-related MOOCs to both professional and consumer-based audiences, and these potential contributions are explored in the following section.
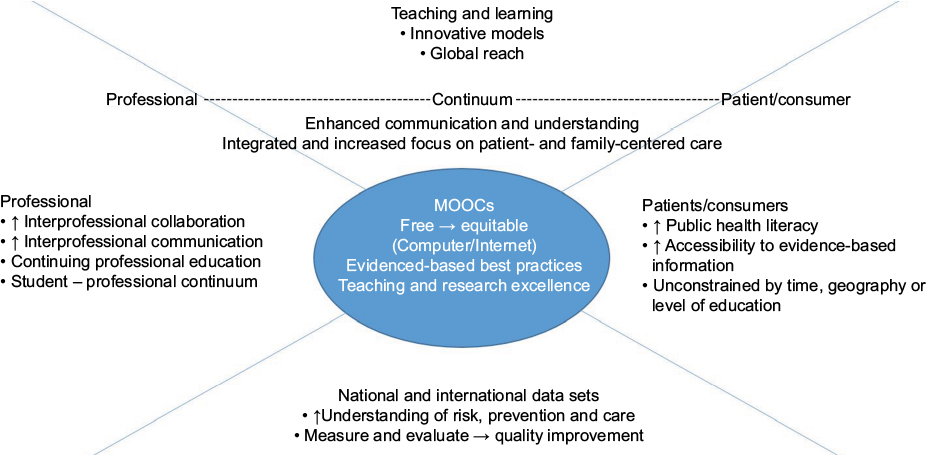 | Figure 1 Potential contributions of health- and medicine-related MOOCs. Abbreviation: MOOCs, massive open online courses. |
In a recent systematic review of health- and medicine-related MOOCs, Liyanagunawardena and Williams22 identified 225 courses, of which 113 were listed on the MOOC aggregator site “Class Central.” They examined 98 of these MOOCs that fit the following criteria: no cost, specified start and end dates, and not related to psychology, biology, life sciences, or animal health and disease unrelated to human health. The majority of the selected MOOCs were offered in English, predominantly by universities in North America. The courses ranged in length from 3 to 20 weeks. Completion of some MOOCs provided participants with continuing professional education (medical, nursing, or dental) credit but most courses appeared introductory, as judged from their “Introduction to…” titles. A search of the Class Central site in March 2017 showed that the number of listed health- and medicine-related MOOCs had increased from 113 in 2014 to 511.
As long as one has access to a computer and the Internet, MOOCs can provide access to information compiled and presented by experts without the constraints of time, geography, or level of education.23 The ability to read and write in English may be a constraint. Although some detractors fear that MOOCs may undermine current higher education models, the more common view for health and medicine is that MOOCs offered by universities appear a valuable way to address three important issues: 1) increase the health literacy of the public – and older adults can indeed benefit,24,25 2) provide continuing professional, and interprofessional, education for practitioners – serving as a ready resource for evidence-based care, as scientific evidence and expert consensus about best practices often take a long time to reach clinicians and patients, and 3) explore innovative teaching models for student learning, including the promotion of effective interprofessional teams, and problem-based quality improvement learning that enhances in-person traditional learning, facilitates leadership, and removes barriers frequently experienced by international students.22,25–33 These three complementary and important components of effective medical education and practice can assist in redesigning systems of care and translating knowledge into effective care and prevention. These three components also can facilitate organizational support, efficiency modeling processes, and transparent reimbursement systems to promote effective, outcome-based care, taking advantage of collective learning and focusing on patient and family needs.
MOOCs would also appear helpful to facilitate effective communication among international communities of patients and clinicians, including student clinicians, with shared interests, strengthening the cooperative relationships essential to effective online learning.34,35 Further, the accumulation of MOOC data through large-scale measurement and analysis, “big data”36 obtained nationally and internationally, has the potential to assist in greater understanding of the risk for diseases and their prevention, as well as increased efficiency in systematic care,37 with this translating into medical and IPE, authentic, patient-centered assessment methods for student learning, and wider access for student recruitment. As universities strive to develop innovative strategies to maintain teaching and research excellence in medical education and practice in an increasingly competitive environment, participating in collaboratively developed MOOCs may prove valuable to facilitate students’ understanding of the importance of patient perspectives to drive patient-centered quality care38,39 (Table 1).
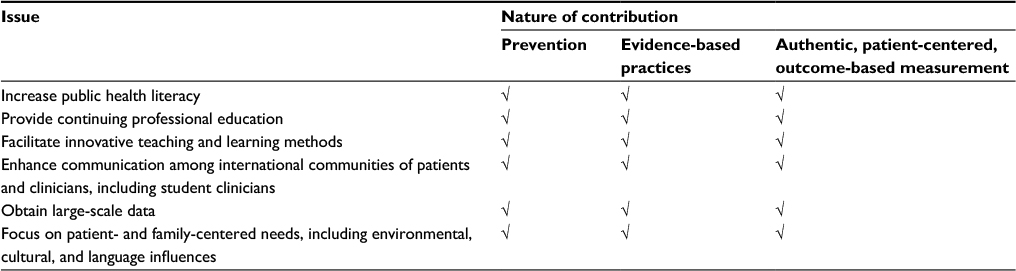 | Table 1 Contributions of MOOCs to national and international issues in medical education and practice Abbreviation: MOOCs, massive open online courses. |
MOOCs can be costly to produce, in terms of the required infrastructure and technology, including meaningful assessment methods, invited expertise, the time needed for staff to respond to participants’ discussion board posts to maintain a personal connection online, and tangible staff incentives.27,40 Future MOOC offerings may include a user fee, parallel to a workshop fee for face-to-face learning, or a fee for providing a certificate of completion. Some universities may feel a need to cap the number of participants, particularly if the MOOC is specific to student skill or competency development. However, collaborative work in leadership across consumer-based organizations, medical professions, universities, policy developers, and funding agencies may mitigate these challenges.
How best to measure learning through MOOCs?
In reporting data to document the success of MOOCs, investigators have focused on the types of engagement activities used to encourage social interaction and problem-solving, number of participants who engaged, the length of time spent on particular activities, and the number of participants who completed the course, with subsequent surveys and interviews of participants used as available.23,41–43 Reich44 argued that many of these measures show what participants do, but not necessarily what they learn. He stressed that ongoing MOOC design and policy development need to focus on three characteristics to document learning: 1) pretesting, then repeated testing throughout the duration of the course, 2) procedural as well as conceptual measures of learning and thinking, and 3) reliance on validated assessments to facilitate comparative cross-course analysis. In the meantime, embedded experiments, quizzes with correct answers provided, and thematic analyses of posted comments and responses on interactive discussion boards may provide valuable insights into participant learning, particularly in an interprofessional and person-centered context.
The shorter length of MOOCs may also facilitate engagement and completion, and thus learning.23 To address the global public health issue of dementia, investigators at the Wicking Dementia Research and Education Centre (University of Tasmania) have developed an innovative 9-week “Understanding Dementia” MOOC (first offered in 2013)23 and a 5-week “Preventing Dementia” MOOC (first offered in 2016). Both the “Understanding Dementia” and the “Preventing Dementia” MOOCs contain a pretest, the “Dementia Knowledge Assessment Scale.”45 The “Preventing Dementia” MOOC also contains a validated instrument to enable participants to ascertain their risk for developing dementia46 and has been translated into Chinese. Both MOOCs include presentations from recognized national and international experts in the cause, care, and prevention of dementia, interviews with people living with dementia, and a variety of interactive activities. These activities include “thought trees” to probe participants’ understanding and experiences, and “ask an expert” discussion boards.
The “Understanding Dementia” MOOC is a pathway to the Wicking Dementia Research and Education Centre’s fully online Bachelor of Dementia Care program. MOOC participants can enroll in an elective unit (CAD110: Negotiated Study in Understanding Dementia) to receive academic credit for completing the MOOC. A similar pathway is planned to enable completers of the “Preventing Dementia” MOOC to gain academic credit through enrolling in a Bachelor of Dementia Care unit on prevention. To date, more than 83,000 participants from multiple countries and diverse educational backgrounds have participated in and completed the two MOOCs. The 34–49% completion rates are substantially more than the reported 5–15% completion rates for other medically related MOOCs.23,47 Further, there is no statistically significant difference in completion rates between “Understanding Dementia” MOOC participants who had previous university level experience and those who did not.23 These high completion rates across a range of levels of education and occupation highlight the scale of unmet need for in-depth education about dementia prevention and care. The completion rates document the appropriateness of carefully designed MOOCs to contribute to medical education and practice, particularly for nationally and internationally known chronic care conditions. That said, a focus on chronic care conditions does not minimize the importance of MOOCs developed to address acute medical conditions, such as the Ebola crisis.48
To optimize the contribution of MOOCs to the dissemination of information and learning, Reich44 encouraged universities to
prioritize courses[…] designed from the outset to address fundamental questions about teaching and learning. Journal editors and conference organizers should prioritize publication of work conducted jointly across institutions, examining learning rather than engagement outcomes, and carefully designed research[…] Funding agencies should share these priorities…and support these initiatives.
These principles apply when situated within the framework of known chronic care conditions to improve national and international efforts in prevention, evidence-based care, and collaborative and interprofessional medical education focused on the needs of patients and authentic outcomes-based assessment.
Implications for research and practice
A recognized gap in health care is the lack of, or inconsistent focus on, patient- and family-centered care. Making this focus consistent can facilitate patients’ active engagement in their care, identify meaningful and functional outcomes that are not solely practitioner or policy driven, and facilitate the development of a patient- and family-centered evidence base that is integral to effective, quality care. Integrating the lived experiences of those who are ill and those who care for them into health- and medically-related MOOCs appears an important step in promoting patient- and family-centered care in medical education and practice. Integrating these lived experiences, including access and reimbursement issues, addresses important components of medical education, namely increasing health literacy, providing continuing medical education, and facilitating the development of innovative, problem-based teaching. Optimizing the advantages offered by carefully designed, well-structured, and outcomes-based MOOCs, the frequent MOOC titles of “Introduction to…” can be replaced with titles such as “Integrated perspectives on…” reflecting meaningful, authentic, evidence-based, collaborative, and integrated health and medical information to which thousands of people can have ready access.
Summary
MOOCs can provide valuable access to reliable information without the constraints of time, geographical location, or level of education. To document the effectiveness of any MOOC, its design needs to include the following features: 1) pretesting, then periodic testing of intended outcomes throughout the course, 2) procedural as well as conceptual measures of learning and thinking, including embedded interactive activities to facilitate engagement; and 3) validated assessment measures to enable comparison of learning and effectiveness across MOOCs. In this way, carefully designed and collaboratively developed MOOCs have the potential to bring together people in consumer, professional, and policy development groups, health care organizations, and universities to facilitate inclusive learning about evidence- and practice-based patient- and family-centered care. This learning can focus on prevention, intervention, and authentic, culturally appropriate, patient-centered outcomes, particularly for known chronic care conditions, many of which are global health concerns. Thus, MOOCs can play a role in increasing public health literacy, providing continuing professional education and stimulating the development of innovative teaching models for student learning focused on patient- and family-centered care.
Acknowledgments
The development of this paper was supported by funding from the JO and JR Wicking Trust (Equity Trustees). We thank Dr Susanne Becker for her assistance in the development of Figure 1.
Disclosure
The authors report no conflicts of interest in this work.
References
Siemens G. Connectivism: Learning as Network-Creation. ELearnspace; 2005. Available from: http://www.elearnspace.org/blog/2005/08/11/connectivism-learning-as-network-creation/. Accessed March 18, 2017. | ||
Downes S. An introduction to connective knowledge. In: Hug T, editor. Media, Knowledge & Education – Exploring New Spaces, Relations and Dynamics in Digital Media Ecologies: Proceedings of the International Conference. Innsbruck University Press; Innsburck: 2007. | ||
Institute of Medicine, Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: Natl Acad Sci; 2001. | ||
Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M. Interprofessional education: effects on professional practice and healthcare outcomes (update). Cochrane Database Syst Rev. 2013;3:CD002213. | ||
World Health Organization. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva, Switzerland: World Health Organization; 2010. | ||
Goldberg LR, Scott Koontz J, Rogers N, Brickell J. Considering accreditation in gerontology: the importance of interprofessional collaborative competencies to ensure quality health care for older adults. Gerontol Geriatr Educ. 2012;33(1):95–110. | ||
Wingo MT, Havyer RDA, Comfere NI, Nelson DR, Reed DA. Interprofessional collaboration milestones: advocating for common assessment criteria in graduate medical education. BMC Med Educ. 2015;15:149. | ||
Goldberg LR, Brown G, Mosack VA, Fletcher PA. Student reflections following exposure to a case-based interprofessional learning experience: preliminary findings. J Interprof Care. 2014;29(4):380–382. | ||
Lindenthal JJ, DedLisa JA, Heinrich GF, Calderón Gerstein WS. Exposing medical students to expanding populations. Adv Med Educ Pract. 2015;6:177–182. | ||
van Leijen-Zeelenberg JE, Elissen AMJ, Grube K, et al. The impact of redesigning care processes on quality of care: a systematic review. BMC Health Serv Res. 2016;16:19. | ||
Frampton SB, Guastello S, Hoy L, Naylor M, Sheridan S, Johnston-Fleece M. Harnessing evidence and experience to change culture: a guiding framework for patient and family engaged care. Natl Acad Med. 2017. | ||
Berghout M, van Exel J, Leensvaart L, Cramm JM. Healthcare professionals’ views on patient-centered care in hospitals. BMC Health Serv Res. 2015;15:385. | ||
Noel MA, Kaluzynski TS, Templeton VH. Quality dementia care: integrating caregivers into a chronic disease management model. J Appl Gerontol. 2017;36(2):195–212. | ||
Zachariae R, O’Connor M, Lassesen B, et al. The self-efficacy in patient centeredness questionnaire – a new measure of medical student and physician confidence in exhibiting patient-centered behaviors. BMC Med Educ. 2015;15:150. | ||
Swisher AK. Practice-based evidence. Cardiopulm Phys Ther J. 2010;21(2):4. | ||
Singer SJ, Benzer JK, Hamdan SU. Improving health care quality and safety: the role of collective learning. J Healthc Leadersh. 2015;7:91–107. | ||
Australian Institute of Health and Welfare [webpage on the Internet]. Leading Causes of Death. 2017. Available from: http://www.aihw.gov.au/deaths/leading-causes-of-death/. Accessed March 20, 2017. | ||
Centers for Disease Control and Prevention [webpage on the Internet]. Chronic Diseases. Atlanta, Georgia: 2017. Available from: https://www.cdc.gov/chronicdisease/stats/index.htm. Accessed March 20, 2017. | ||
World Health Organization [webpage on the Internet]. Dementia. Geneva, Switzerland: 2016. Available from: http://www.who.int/mediacentre/factsheets/fs362/en/. Accessed March 20, 2017. | ||
Ferri CP, Prince M, Brayne C, et al; Alzheimer’s Disease International. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366(9503):2112–2117. | ||
World Health Organization [webpage on the Internet]. Top 10 Causes of Death Worldwide. Geneva, Switzerland: 2015. Available from: http://www.who.int/mediacentre/factsheets/fs310/en/. Accessed March 20, 2017. | ||
Liyanagunawardena TR, Williams SA. Massive open online courses on health and medicine: review. J Med Internet Res. 2014;16(8):e191. | ||
Goldberg LR, Bell E, King C, et al. Relationship between participants’ level of education and engagement in their completion of the understanding dementia massive open online course. BMC Med Educ. 2015; 15:60. | ||
Liyanagunawardena TR, Williams SA. Elderly learner and massive open online courses: a review. Interact J Med Res. 2016;5(1):e1. | ||
Gitlin LN, Hodgson N. Online Training: Can It Prepare an Eldercare Workforce?. American Society on Aging; 2016. Available from: http://www.asaging.org/blog/online-training-can-it-prepare-eldercare-workforce. Accessed March 18, 2017. | ||
Heller R. Learning by MOOC or by crook. Med J Aust. 2014;200(4):192–193. | ||
Heller N [webpage on the Internet]. LaptopU: Has the Future of College Moved Online?. New Yorker; 2013. Available from: http://www.newyorker.com/magazine/2013/05/20/laptop-u. Accessed March 18, 2017. | ||
Kearney RC, Premaraj S, Smith BM, Olson GW, Williamson AE, Romanos G. Massive open online courses in dental education: two viewpoints. J Dent Educ. 2016;80(2):121–127. | ||
Mourad A, Jurjus A, Hussein IH. The what or how: a review of teaching tools and methods in medical education. Med Sci Educ. 2016;26(4):723–728. | ||
Mubuuke AG, Louw AJN, van Schalkwyk S. Utilizing students’ experiences and opinions of feedback during problem based learning tutorials to develop a facilitator feedback guide: an exploratory qualitative study. BMC Med Educ. 2016;16:6. | ||
Attrill S, Lincoln M, McAllister S. Supervising international students in clinical placements: perceptions of experiences and factors influencing competency development. BMC Med Educ. 2016;16:180. | ||
Karpa KD, Hom LL, Huffman P, et al. Medication safety curriculum: enhancing skills and changing behaviors. BMC Med Educ. 2015;15:234. | ||
Bergh AM, Bac M, Hugo J, Sandars J. Making a difference – medical students’ opportunities for transforming change in health care and learning through quality improvement projects. BMC Med Educ. 2016;16:171. | ||
Scherer Bassani PB. Interpersonal exchanges in discussion forums: a study of learning communities in distance learning settings. Comput Educ. 2011;56(4):931–938. | ||
Woo Nam C, Zellner RD. The relative effects of positive interdependence and group processing on student achievement and attitude in online cooperative learning. Comput Educ. 2011;56(3):680–688. | ||
Hofmann-Apitius M. Is dementia research ready for big data approaches? BMC Med. 2015;13:145. | ||
Frogner BK, Frech HE 3rd, Parente ST. Comparing efficiency of health systems across industrialized countries: a panel analysis. BMC Health Serv Res. 2015;15:415. | ||
Wells J. Unis struggling to define innovation: report. Campus Rev. 2017, March 10. | ||
Shweiki E, Martin ND, Beekley AC, et al. Applying expectancy theory to residency training: proposing opportunities to understand resident motivation and enhance residency training. Adv Med Educ Pract. 2015;6:339–346. | ||
Back DA, Behringer F, Harms T, Plener J, Sostmann K, Peters H. Survey of e-learning implementation and faculty support strategies in a cluster of mid-European medical schools. BMC Med Educ. 2015;15:145. | ||
Deng R, Benckendorff P. A contemporary review of research methods adopted to understand students’ and instructors’ use of massive open online courses (MOOCs). Int J Inf Educ Technol. 2017;7(8):601–607. | ||
Swinnerton B, Hotchkisst S, Morris NP. Comments in MOOCs: who is doing the talking and does it help? J Comput Assist Learn. 2017;33(1):51–64. | ||
Gooding I, Klaas B, Yager JD, Kanchanaraksa S. Massive open online course in public health. Front Public Health. 2013;1:59. | ||
Reich J. Rebooting MOOC research: improve assessment, data sharing, and experimental design. Science. 2015;347(6217):34–35. | ||
Annear MJ, Toye CM, Eccleston CE, et al. Dementia knowledge assessment scale: development and preliminary psychometric properties. J Am Geriatr Soc. 2015;63(11):2375–2381. | ||
Farrow M. User perceptions of a dementia risk reduction website and its promotion of behavior change. JMIR Res Protoc. 2013;2(1):e15. | ||
Goldberg LR, King AE, Cook AL, et al. Education as an essential intervention in dementia literacy and care. BMC Med Educ. under review. | ||
Ruiz De Castenada R, Valticos A, Pittet D, Flahault A. MOOCs (massive open online courses) as innovative tools in infections prevention and control: reflections from the first MOOC on Ebola. Antimicrob Resist Infect Control. 2015;4(S1):16. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.