")
Back to Journals » International Journal of Women's Health » Volume 12
Advanced Sexual Counseling and How to Ask Patients About “Intimate Disclosure”
Authors Marchand GJ , Meassick KS
Received 17 April 2020
Accepted for publication 29 October 2020
Published 20 November 2020 Volume 2020:12 Pages 1105—1108
DOI https://doi.org/10.2147/IJWH.S256250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Greg J Marchand, Katerina S Meassick
Marchand Institute for Minimally Invasive Surgery, Mesa, AZ, USA
Correspondence: Greg J Marchand
Marchand Institute for Minimally Invasive Surgery, 10238 E. Hampton Ave., Suit 212, Mesa, AZ 85209, USA
Tel +1-480-999-0905
Email [email protected]
Abstract: At the forefront of female sexual and reproductive health, OBGYNs play a pivotal role in assessing and managing sexual satisfaction and dysfunction. Satisfying sexuality often relates to a woman’s ability or likelihood to relay to her partner the steps and actions required for her to reach orgasm. Female orgasms, in contrast to male orgasms, can be related to different areas of stimulation and processes (clitoral/vaginal (G-spot)/anal). Despite this knowledge, OBGYNs rarely discuss orgasm with patients or the importance and vulnerability of disclosing this information to their partners to enhance sexual satisfaction. Many women may not realize that sexual complaints are an acceptable subject to discuss at gynecologic visits, while others may feel uncomfortable in general talking about sex. But as the topic of female sexual dissatisfaction becomes less taboo thanks to social media, patients are increasingly likely to turn to their health-care providers to evaluate and treat sexual complaints. While conducting a thorough history, sexual history, physical exam and laboratory tests can help to rule out any biological, physiological or psychological causes of sexual dissatisfaction, it is only one half of the equation. Discussion of the steps and actions required for them to reach orgasm with their partners is paramount in working to achieve satisfying sexuality and orgasm. Despite the importance of satisfying sexuality in a relationship, this topic often leads to feelings of trepidation and vulnerability on behalf of the patient. Recognizing and providing acknowledgment of these feelings help patients feel listened to and validated.
Keywords: counseling, female orgasm, sexual counseling, sexual health, communication, satisfying sexuality
Introduction
Satisfying sexuality often relates to a woman’s ability or likelihood to relay to her partner the steps and actions required for her to reach orgasm. While the point has been raised that orgasms may not be important for female sexual pleasure, the results of surveys on sex overwhelmingly demonstrate the single most important predictor of sexual satisfaction for women of all ages is having an orgasm.1,2 Research has shown that women in heterosexual and bisexual relationships have more trouble in reaching orgasm than their male counterparts, with on average >90% of men usually experiencing orgasm in intercourse while the percentage among women ranged from 50% to 66%.3,4 This is in contrast to women who identify as lesbian, 86% of whom report achieving orgasm.2 This difference can be attributed to a number of factors, some of which are outside a woman’s control, and some of which are within her control (Table 1). Of the factors associated with ability and frequency to obtain orgasm, satisfaction with and communication in the couple relationship are two of the most highly associated.
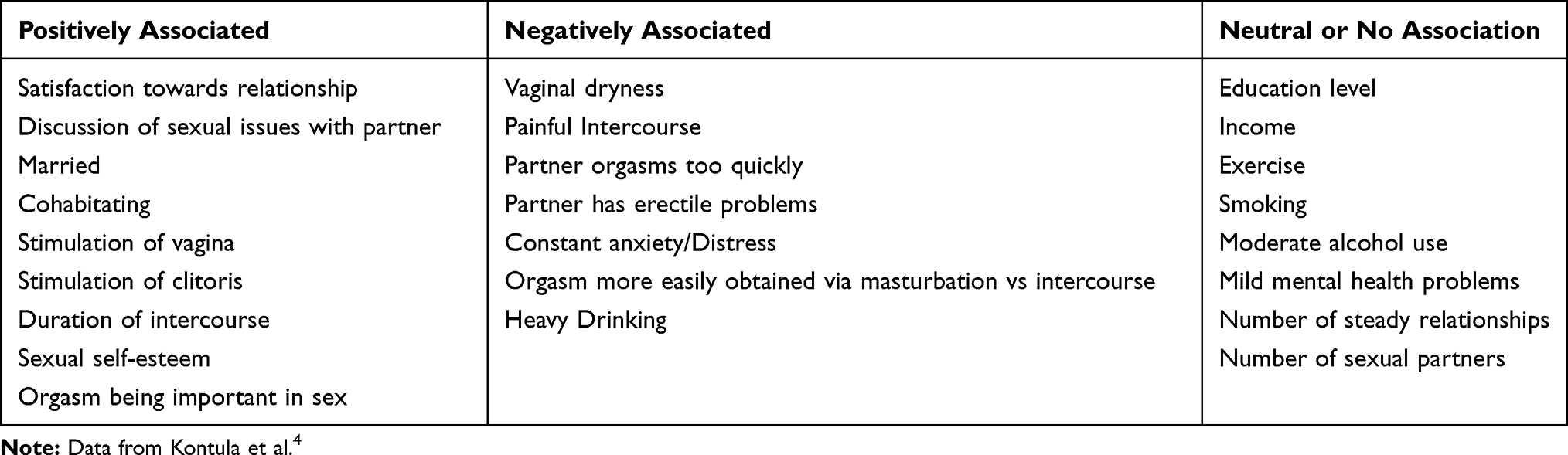 |
Table 1 Factors Associated with Frequency and Ability to Obtain Orgasm |
Discussion
Physiology and Processes of Orgasm
While male orgasms are usually the result of one area of stimulation, female orgasms can be a result of a variety of areas and processes of stimulation (clitoral/vaginal (G-spot)/anal). From what we currently understand, a multitude of pre-stimulation factors such as desire and a woman’s receptiveness towards sexual stimuli play a critical role in initiating sexual arousal.5 Subsequently, female orgasm is achieved by stimulating one or more of three genital nerves; the pudendal (clitoris, anus), pelvic (vagina, anus), and hypogastric (cervix, uterus).6,7 When asked how they normally achieve an orgasm with intercourse, more than half of women report needing both clitoral and vaginal stimulation, while only a third report needing only clitoral stimulation, and less than a fifth report orgasm through vaginal stimulation alone.8 The steps and activities needed to achieve adequate stimulation for orgasm also varied. In women who received oral or manual stimulation from partners, orgasm was achieved more often than those who did not. This was found to be true in women in heterosexual, bisexual and lesbian relationships.2 Additionally, in couples who found discussing sexual issues difficult, receiving oral sex was highly associated with achieving orgasm.4 Partner related factors such as duration of intercourse, technique of stimulation, and position are all strongly associated with ability to orgasm and often vary between individuals.1 This demonstrates the importance of relaying not only the actions but the steps required by a woman to orgasm to her partner.
Communication
Without regular and open communication, partners may not have adequate knowledge in order to enact the steps and provide the stimulation needed to achieve orgasm. While little empirical research on the role of partner communication in promoting orgasm, many researchers suggest that communication promotes behaviors that increase the likelihood of orgasm. The first barrier to such communication is the woman herself knowing what is required for her to achieve orgasm. Surveys suggest that between 4% and 10% of women report never having achieved orgasm from intercourse.9 If after assessing her level of self-knowledge such a deficit is found, counseling may include suggesting trying different methods and techniques, either alone or with the partner. Another barrier to open communication is that women feel that asking for stimulation, either of specific areas or using specific techniques, in the presence of their male partner would not be welcome and that their orgasm was more of a “bonus” than a goal of sexual intercourse.4 This belief persists despite the majority of men feeling that they have the responsibility to stimulate their partner to orgasm and that the inability to do so leads to self judgement, and lower self-esteem.10 Another barrier to honest communication may stem from the pressure felt by both men and women to provide a satisfying sexual experience for their partner is pretending, or “faking”, orgasm. Over half of women report having pretended to orgasm at least once and nearly a quarter report pretending in nearly every encounter, making it a very prevalent barrier to achieving orgasm.11 The most common reason reported in Herbenick et al was not wanting to hurt a partner’s feelings, this practice provides misinformation and obscures necessary feedback. In counseling patients, the occurrence and frequency of this practice should be discussed and moreover discouraged. Care must be taken not to shame or induce feelings of embarrassment but rather encourage disclosure of the steps and processes required to achieve orgasm by providing accurate verbal and physical feedback and communication.
Clinical Guidance
Unfortunately, despite this knowledge, OBGYNs rarely discuss orgasm or satisfying sexuality with their patients regardless of sexual orientation. This may be in part due to the lack of guidance or discomfort on the part of the physician, especially with elderly patients.12,13 As satisfying sex and sexuality are quickly becoming less taboo topics, more women are seeking guidance and education from reputable sources on how to address difficulties they may be facing in these areas. Ultimately as the experts in women’s health and reproduction, these topics fall squarely within scope of OBGYNs. While pathologic and physiologic causes should be ruled out, physicians must also discuss the amount of communication and comfort level patients have when discussing these matters with their partners. Counseling patients on the importance of communicating the steps and processes necessary to orgasm with their partners is both low risk and procedurally non-invasive making it an ideal initial step in evaluating unsatisfying sexuality (Table 2). Due to the personal and private nature of this topic, it can often lead to feelings of discomfort and vulnerability. By recognizing these feelings and validating them, this may help reduce or dispel some of the stigma patients feel making it easier to discuss this information in a clinical setting and have intimate disclosure with their partners. Additionally, providing a safe and comfortable environment to speak about sensitive topics, such as this, allows for a strengthening of the physician–patient relationship.
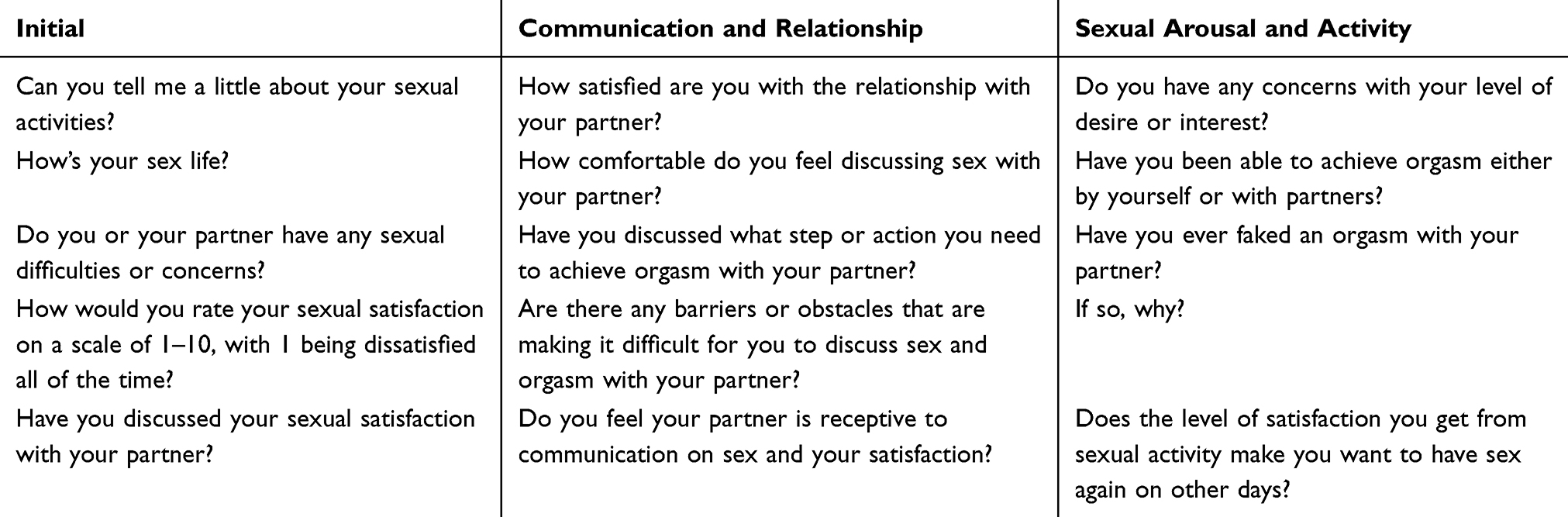 |
Table 2 Suggested Sentences for Clinicians |
Conclusions
As the pursuit of satisfying sexual activity becomes a topic increasingly brought to OBGYNs, clinicians must understand the importance of assessing communication and intimate disclosure. Advanced sexual counseling as an initial step in the evaluation of unsatisfying sexuality provides a low risk, economical, and non-invasive assessment that often may preclude the need for more invasive labs. Equipped with the knowledge that communicating the steps and processes of stimulation may be necessary and paramount to achieve orgasm, clinicians should emphasize the necessity of disclosing this information to partners. By acknowledging the feelings of vulnerability this topic elicits, clinicians can provide assurance of normalcy and dispel some of the trepidation that may be felt by patients in disclosing this information to both clinicians and their partners.
Abbreviation
OBGYNs, obstetricians and gynecologists.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Acknowledgments
The Marchand Institute for Minimally Invasive Surgery would like to acknowledge the efforts of all of the students, researchers, residents and fellows at the institute who put their time and effort into these projects without compensation, only for the betterment of medicine. We firmly assure them that the future of medicine belongs to them.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no funding or financial support for the research, authorship, or publication of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Kontula O, Miettinen A. Determinants of female sexual orgasms. Socioaffect Neurosci Psychol. 2016;6:31624. doi:10.3402/snp.v6.31624
2. Velten J, Margraf J. Satisfaction guaranteed? How individual, partner, and relationship factors impact sexual satisfaction within partnerships. PLoS One. 2017;12(2):e0172855. doi:10.1371/journal.pone.0172855
3. Frederick DA, St. John HK, Garcia JR, Lloyd EA. Differences in orgasm frequency among gay, lesbian, bisexual, and heterosexual men and 151 women in a U.S. National Sample. Arch Sex Behav. 2018;47(1):273–288. doi:10.1007/s10508-017-0939-z
4. Kontula O, Mäkinen M. Between Sexual Desire and Reality: The Evolution of Sex in Finland. Vol. 153. Publications of the Population Research Institute; 2009:49.
5. Basson R. Women’s sexual dysfunction: revised and expanded definitions. Can Med Assoc J. 2005;172(10):1327–1333. 155. doi:10.1503/cmaj.1020174
6. Munarriz R, Kim NN, Goldstein I, Traish AM. Biology of female sexual function. Urol Clin North Am. 2002;29(3):685–693. doi:10.1016/S0094-0143(02)00069-1
7. Blackledge C. The Story of V: A Natural History of Female Sexuality. Rutgers University Press; 2004.
8. Herbenick D, Fu T-CJ, Arter J, Sanders SA, Dodge B. Women’s experiences with genital touching, sexual pleasure, and orgasm: results from a U.S. Probability sample of women ages 18 to 94. J Sex Marital Ther. 2018;44(2):201–212. doi:10.1080/0092623X.2017.1346530
9. Wallen K, Lloyd EA. Female sexual arousal: genital anatomy and orgasm in intercourse. Horm Behav. 2011;59(5):780–792. doi:10.1016/j.yhbeh.2010.12.004
10. Salisbury CMA, Fisher WA. “Did you come?” A qualitative exploration of gender differences in beliefs, experiences, and concerns regarding female orgasm occurrence during heterosexual sexual interactions. J Sex Res. 2014;51(6):616–631. doi:10.1080/00224499.2013.838934
11. Herbenick D, Eastman-Mueller H, Fu T-C, Dodge B, Ponander K, Sanders SA. Women’s sexual satisfaction, communication, and reasons for (No Longer) faking orgasm: findings from a U.S. probability sample. Arch Sex Behav. 2019;48(8):2461–2472. doi:10.1007/s10508-019-01493-0
12. Castleman M Does your doctor ask about sexual issues? Psychology Today website; February 15, 2010. Available from: http://www.psychologytoday.com/blog/all-about-sex/201002/does-your-doctor-ask-about-sexual-issues.
13. Gott M, Hinchliff S, Galena E. General practitioner attitudes to discussing sexual health issues with older people. Soc Sci Med. 2004;58(11):2093–1682103. doi:10.1016/j.socscimed.2003.08.025
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.