")
Back to Journals » Drug Design, Development and Therapy » Volume 14
Adjuvant Vaginal Use of Sildenafil Citrate in a Hormone Replacement Cycle Improved Live Birth Rates Among 10,069 Women During First Frozen Embryo Transfers
Received 13 September 2020
Accepted for publication 12 November 2020
Published 1 December 2020 Volume 2020:14 Pages 5289—5297
DOI https://doi.org/10.2147/DDDT.S281451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Tuo Deng
Yu Tao, Ningling Wang
Department of Assisted Reproduction, Shanghai Ninth People’s Hospital Affiliated to JiaoTong University School of Medicine, Shanghai, People’s Republic of China
Correspondence: Ningling Wang Department of Assisted Reproduction
Shanghai Ninth People’s Hospital Affiliated to JiaoTong University School of Medicine, Shanghai, People’s Republic of China
, Email [email protected]
Purpose: To investigate the effects of sildenafil citrate (SC) on live birth rates (LBR) during women undergoing their first frozen embryo transfers (FET) with hormone replacement therapy (HRT).
Patients and Methods: This retrospective cohort study included a total of 10,069 infertile women with adequate endometrial thickness (≥ 7 mm when progesterone was initiated) in their first FET cycle with hormone replacement therapy. Women received either vaginal SC or no adjuvant during their first transfer cycle depending on patient or physician preference. In the sildenafil group, 1098 women underwent HRT FET with adjuvant vaginal use of SC, and 8971 women were included as controls. The primary outcome measure was LBR, defined as the likelihood of live birth per transfer cycle. Endometrial thickness (EMT), implantation, chemical pregnancy, clinical pregnancy, miscarriage, ongoing pregnancy, birth weight and preterm delivery (PTB) were also recorded.
Results: Baseline characteristics were comparable between the two groups. In the crude analysis, the unadjusted LBR was significantly higher in the vaginal SC group (scHRT-FET) than in the control group (HRT-FET) (40.3% vs 36.1%). After adjustment for 12 pregnancy-related confounding factors, logistic regression analysis showed that LBR remained significantly higher in the scHRT-FET group than in the HRT-FET group (adjusted odds ratio [aOR] 1.31, 95% confidence interval [CI] 1.14– 1.49). Furthermore, after adjustment, the ongoing pregnancy rate was significantly higher (aOR 1.29, 95% CI 1.13– 1.47), and the miscarriage rate was significantly lower (aOR 0.58, 95% CI 0.43– 0.77), in the scHRT-FET group compared to the HRT-FET group. Adjuvant vaginal use of SC did not increase the endometrial thickness and had no significant effect on birth weight or PTB.
Conclusion: Adjuvant vaginal use of SC in HRT FET was associated with higher LBR and improved pregnancy outcomes in an infertile population with adequate endometrial thickness. The beneficial effect of SC may be due not to an increase in EMT but instead to improve endometrial blood flow and receptivity, which might merit clinicians’ attention for improving general IVF practices.
Keywords: sildenafil citrate, frozen embryo transfer, endometrial preparation, hormone replacement therapy, live birth rates, pregnancy outcomes
Introduction
Currently, although much remains controversial regarding perinatal morbidity,1,2 evidence has demonstrated less ovarian hyper-stimulation syndrome (OHSS) and comparable live birth rates (LBR) in frozen embryo transfer (FET) compared with fresh transfer,3–5 which has resulted in the increased use of frozen cycles.6 However, although in several European countries, FET accounted for approximately 40% of all transfer cycles in 2015, the pregnancy rate per thawing varied from 19.3% to 46.0%, and there is still much room for improvement according to one official report containing data from 38 participating countries.7
Many adjuvant therapies are used empirically to enhance pregnancy outcomes during assisted reproductive technology cycles. However, disputes still exist regarding the validation of these practices. For instance, vaginal oestradiol has been used to augment the oestrogen effect on the uterus necessary for uterine endometrial thickness and receptivity.8,9 Low-dose (81 mg) aspirin was reported to improve ovarian responsiveness, uterine and ovarian blood flow and pregnancy rates in patients undergoing IVF.10,11 Recently, the use of sildenafil citrate (SC) has been gradually extended, and attention has also been paid to the adjuvant use of SC in IVF. SC prevents the breakdown of cGMP and potentiates the effect of nitric oxide (NO) on vascular smooth muscles and was first used for male erectile dysfunction.12 Despite some controversy, considering its vasodilatation effects on uterine vessels, SC is regarded as a potential candidate for the treatment of intrauterine growth restriction (IUGR) and preeclampsia.13–15 Furthermore, studies also showed that SC could promote endometrial proliferation and even enhance human trophoblast invasion.16,17 A vaginal route of administration was chosen since the use of intravaginal sildenafil suppositories decreased the incidence of side-effects such as hypotension and headaches by delivering the medication in close proximity to the target organ.12
To our knowledge, despite case reports,12,18,19 there has been only one study of SC in FET cycles and one study in fresh ET cycles, both in thin-EM patients, and the results failed to reach statistical significance in differences in reproductive outcomes due to the limited sample sizes.20,21 Therefore, large-scale clinical studies are urgently needed to validate the increasing empirical use of sildenafil in embryo transfer. Furthermore, as a long-term pregnancy outcome indicator of great significance, it is also crucial to analyse the live birth rate (LBR), since no LBR data have ever been reported in sildenafil research before. Moreover, to date, studies on sildenafil have been confined to only a very small group of thin-endometrium patients; thus, it is also worthwhile to extend this treatment to patients in the broader infertile population.
Therefore, in the present study, we analysed LBR in a population of 10,069 infertile women with adequate endometrium (≥7 mm when progesterone was initiated) who were undergoing their first FET with HRT. To overcome methodologic bias, 12 important confounders were taken into account and adjusted for in our analyses. Furthermore, EM thickness (EMT) and other pregnancy outcomes, such as implantation, chemical pregnancy rate, clinical pregnancy rate, miscarriage, ongoing pregnancy, birth weight and preterm delivery (PTB), were also explored.
Patients and Methods
Subjects
This retrospective study was carried out at the Reproductive Medicine Center of the Shanghai Ninth People’s Hospital affiliated with the Shanghai Jiao Tong University School of Medicine and was approved by the Ethics Committee (Institutional Review Board) of the Shanghai Ninth People’s Hospital. Informed written consent was obtained from all patients, and the study was conducted according to the Declaration of Helsinki. To minimize possible bias due to the patient population, all women who were undergoing their first FET cycles with an HRT protocol during the period from January 2013 to December 2018 were enrolled, and each patient was included only once.22 Exclusion criteria were as follows: previous IVF attempts with fresh or frozen embryo transfer; patient older than 40 years of age; patient used adjuvants other than vaginal SC during their FET cycle; a history of recurrent miscarriage (defined as ≥2 previous chemical/clinical losses); patient diagnosed with III or IV stage endometriosis (ASRM staging system); and the presence of congenital uterine anomalies as determined by ultrasound or hysterosalpingography. Patients with hypertension, diabetes, or thyroid dysfunction were also excluded.
Treatment
The details of embryo vitrification and thawing methods can be found in our previous article.23 All laboratory procedures, including thawing process and culture medium conditions, remained constant during this research.24 In brief, cleavage stage embryos were graded with reference to the Cummins criteria.25 Quality assessment of blastocysts was on the basis of the Gardner and School craft scoring system.26 We only thawed embryos on the same day of ET. Post-thaw surviving embryos were defined as those with more than 50% intact blastomeres. A maximum of two embryos were allowed to be transferred in all FET cycles.
Endometrial preparation of HRT was performed as described previously.27,28 In short, oral E2 (ethinyloestradiol 75 µg daily, Shanghai Xinyi Pharma, China; or fematon 4 mg, twice daily, Abbott Healthcare Products B.V.) was commenced on the third day of the menstrual cycle; progesterone exposure was initiated when the endometrial thickness reached ≥7 mm. Embryo transfer was performed 3 days after progesterone administration for day 3 embryos or 5 days later for blastocysts. In the scHRT-FET group, sildenafil citrate (Viagra, Pfizer Inc.) was prescribed and initiated from day 8 of the menstrual cycle at a daily dose of 100 mg until the day before ET. For the best results, the blue outer layer of the drug membrane was carefully removed in creating vaginal suppositories for all patients in this cohort. The sildenafil was administered by the patients themselves. Every patient was taught how to prepare the SC, and confirmation of the technique was repeated on their return visits. In all study groups, luteal support was continued until 10 weeks of gestation if pregnancy was achieved. As patients undergoing their first transfer cycle, women received either vaginal SC or no adjuvant during the FET cycle depending on patient and physician preference.
Outcome Assessment
In this study, the primary outcome was LBR per transfer. The secondary outcomes included EMT, implantation rate, chemical pregnancy rate, clinical and ongoing pregnancy rates, miscarriage rate, birth weight and PTB. Live birth was defined as a baby or babies born alive after ≥24 gestational weeks. The implantation rate was defined as the number of gestational sacs on transvaginal ultrasound (TVUS) divided by the total number of transferred embryos. Chemical pregnancy was defined as a serum hCG level >5 IU/L at 14 days after ET. Clinical pregnancy was defined as the identification of at least one gestational sac in the uterine cavity on TVUS 5 weeks after ET. Ongoing pregnancy was defined as a viable pregnancy that lasts for more than 12 gestational weeks. Miscarriage was defined as clinical pregnancy loss before 24 weeks of gestation, and PTB was defined as delivery before 37 weeks of gestation.
Statistical Analyses
Statistical analyses were carried out using Statistical Package for Social Sciences (SPSS) version 21.0. The numerical data were presented as the mean±SD, and the categorical variables were shown as% (n/N). Continuous variables were compared with Student’s t-test. Categorical variables were compared with Pearson’s χ2 test or with Fisher’s exact test when necessary. A P value <0.05 was considered statistically significant.
We performed logistic regression to explore the effects of different protocols on pregnancy outcomes after adjusting for the following potential confounders: maternal age at transfer, maternal body mass index (BMI), duration of infertility, cause of infertility, maternal smoking habit, maternal gravidity and parity, number of embryos transferred, embryo developmental stage, embryo quality, method of fertilization and EMT on day of ET. Unadjusted and adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by the regression models.
Results
Baseline Characteristics
In total, 10,069 patients who met the inclusion and exclusion criteria were analysed and followed up. In the sildenafil group, 1098 women underwent FET with adjuvant vaginal use of SC (scHRT-FET), whereas 8971 women were included as controls (HRT-FET). The baseline characteristics of the included patients are detailed in Table 1. No significant difference was shown between scHRT-FET and HRT-FET in maternal age at transfer, maternal BMI, smoking habit, duration and causation of infertility or obstetrical history (gravidity and parity). In addition, no significant difference was found in the basic hormonal profiles and antral follicle count (AFC) between the two groups.
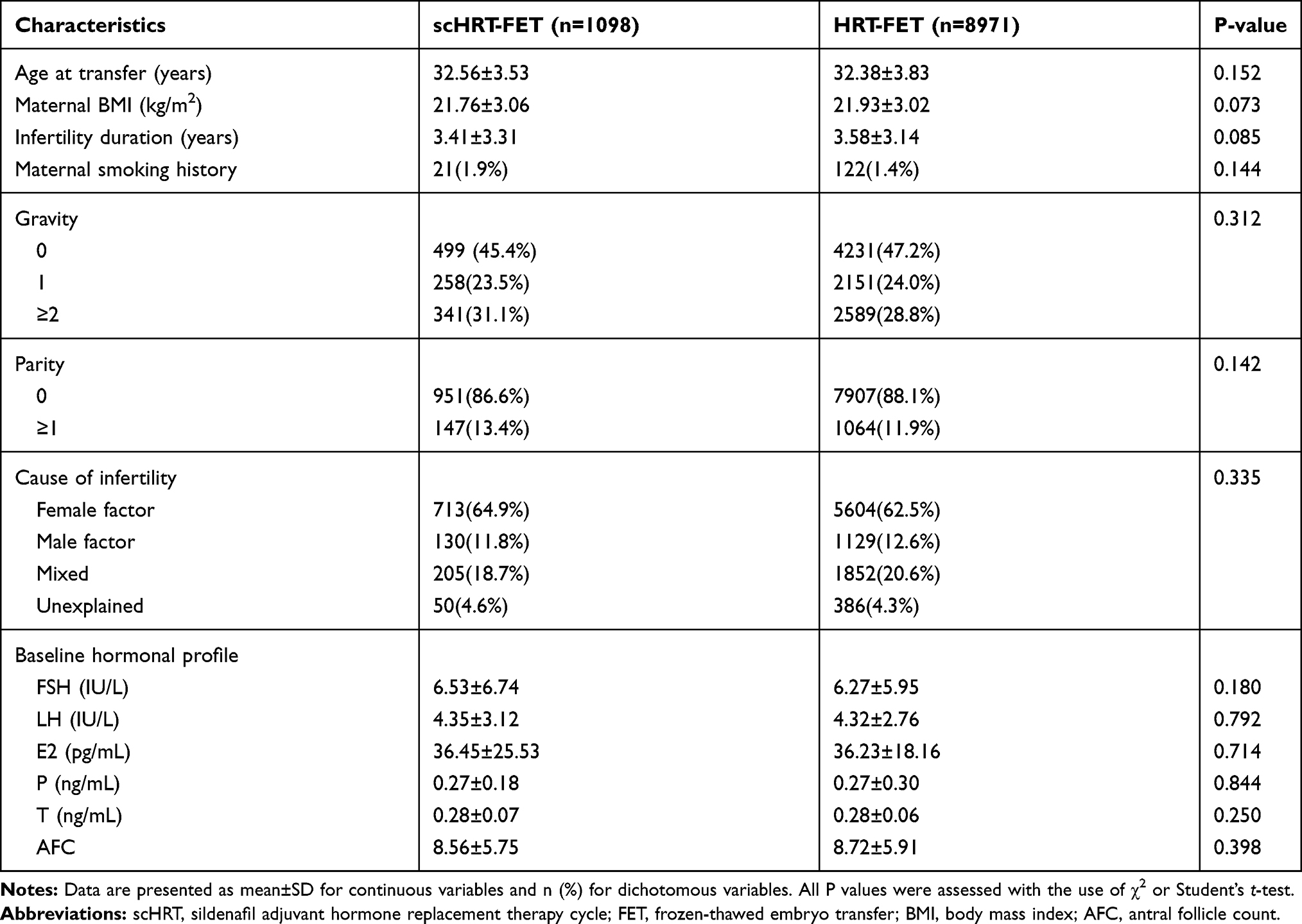 |
Table 1 Baseline characteristics and hormonal profile of patients |
Cycle Characteristics of Embryo Transfers
The characteristics of transfer cycles are presented in Table 2. The number of embryos transferred (P=0.067), embryo fertilization method (P=0.070), embryo developmental stage at cryopreservation (P=0.373), post-thaw embryo survival rate (P= 0.497) and embryo quality at transfer (P=0.166) were similar between the scHRT-FET and HRT-FET groups. It should be noted that in both groups, most embryos transferred were day 3 cleavage stage embryos. Furthermore, EMT on the day of P supplementation (P= 0.892) and EMT on the day of ET (P= 0.370) were similar between the two groups.
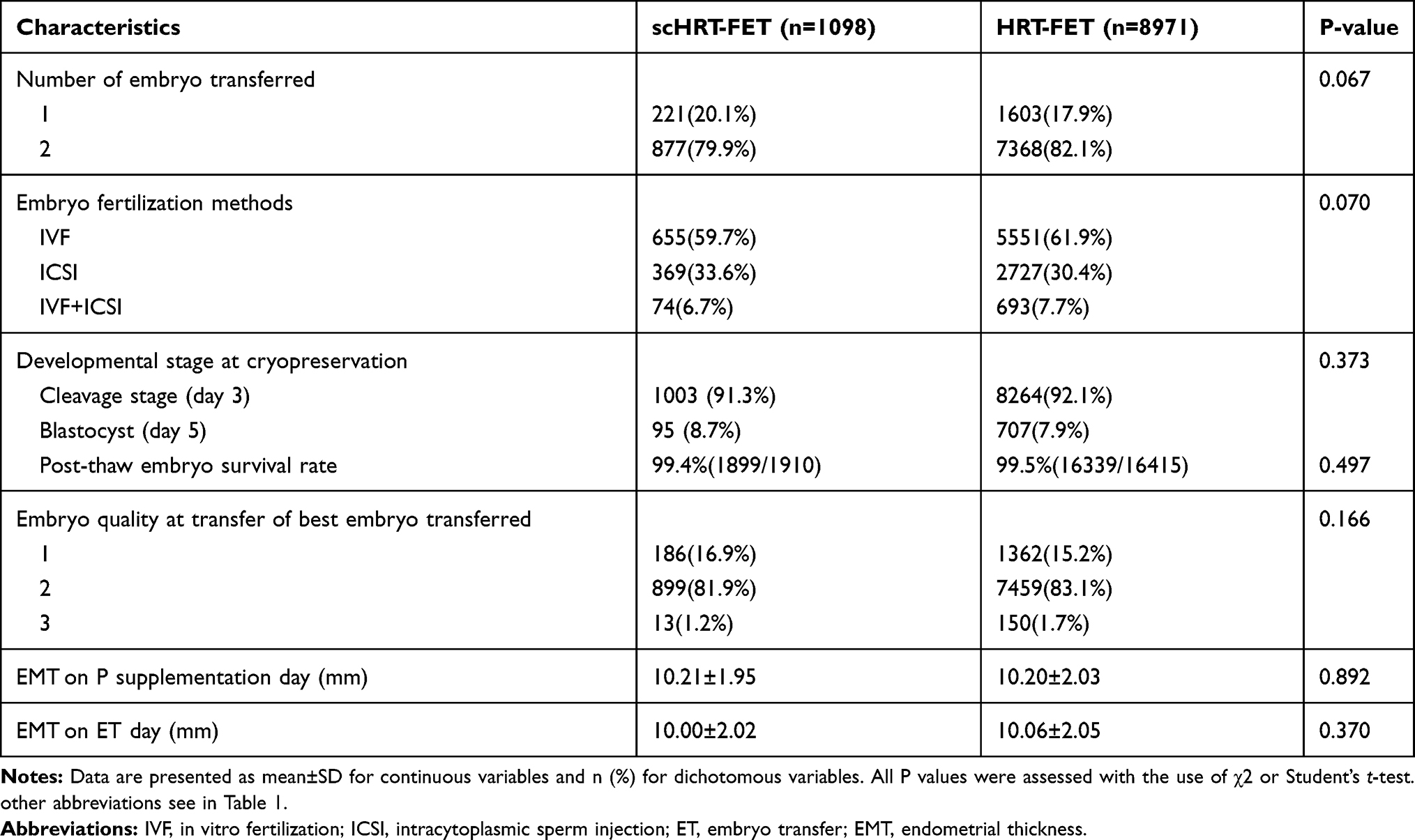 |
Table 2 Cycle characteristics of the scHRT and HRT-FET groups |
Pregnancy Outcomes of FET
In our crude analysis (Table 3), the LBR per transfer in scHRT-FET was significantly higher than that in HRT-FET (40.3% vs 36.1%, P<0.01). The multiple pregnancy rate was significantly lower in the scHRT-FET group (9.2% vs 12.4%; P<0.01). Specifically, the incidence of singleton newborns per transfer was significantly higher in scHRT-FET (33.5% vs 27.1%; P<0.01), and the incidence of twin newborns per transfer was lower in scHRT-FET compared to HRT-FET (6.8% vs 9.0%; P=0.017). The miscarriage rate and especially the first trimester miscarriage rate were significantly lower in scHRT-FET (10.6% vs 18.2%, 9.0% vs 15.9%, respectively; both P<0.001), and the ongoing pregnancy rate was significantly higher in scHRT-FET compared to HRT-FET (41.3% vs 37.3%; P<0.05). However, the implantation, chemical pregnancy, ectopic pregnancy and clinical pregnancy rates were similar between the two groups. In addition, birth weight, gestational weeks and PTB were also similar between the two groups.
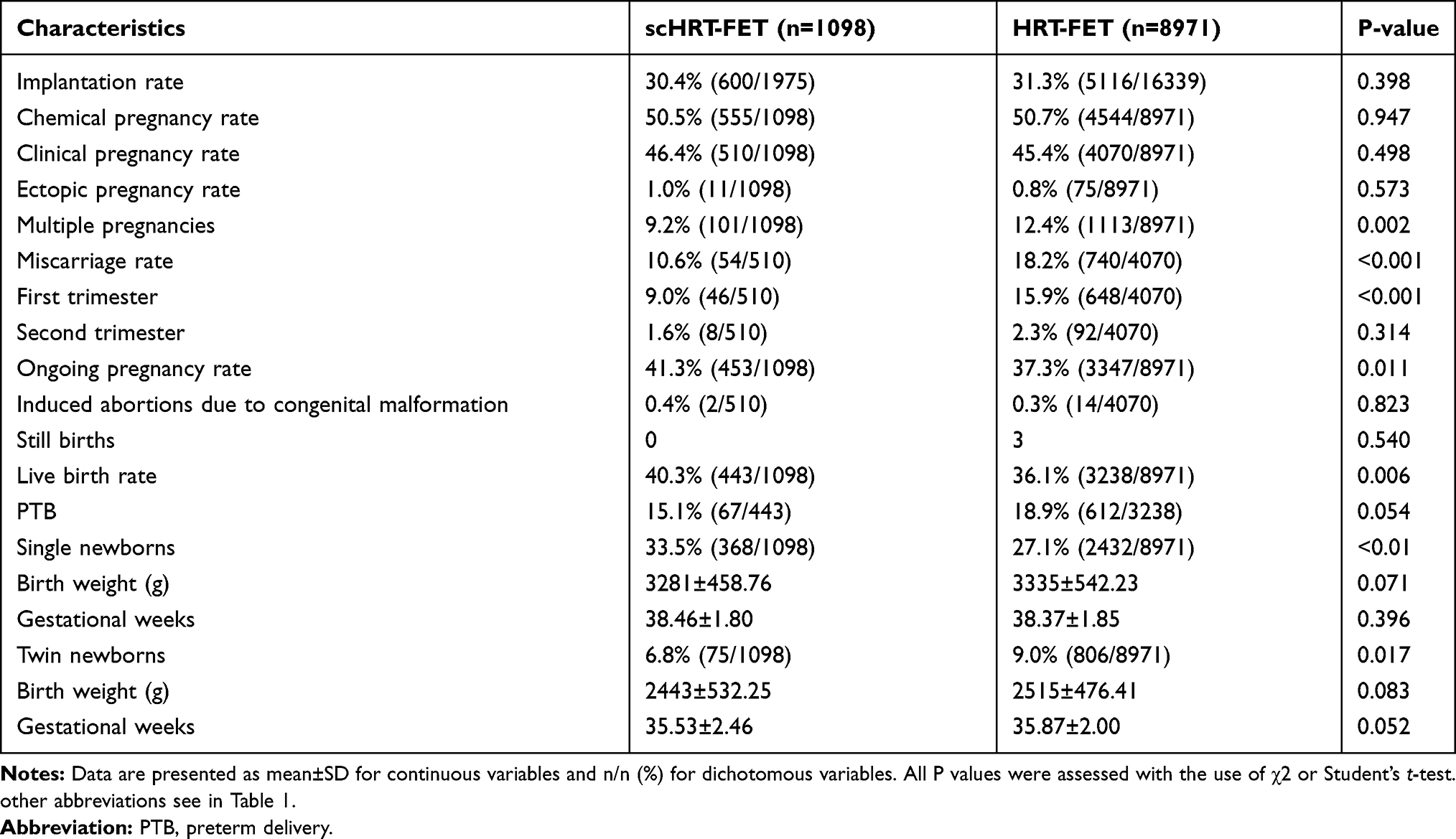 |
Table 3 The pregnancy outcomes of the scHRT and HRT-FET groups |
Logistic Regression Analyses for the Pregnancy Outcomes
After adjustment for a number of important pregnancy-related confounding factors, such as maternal age at embryo transfer, BMI, infertility duration, maternal smoking history, gravidity, parity, cause of infertility, number of embryos transferred, embryo developmental stage and embryo quality at transfer, method of fertilization and EM thickness on day of ET (Table 4), the LBR remained significantly higher in scHRT-FET (adjusted odds ratio [aOR] 1.31, 95% confidence interval [CI] 1.14–1.49, P<0.001). Furthermore, the miscarriage rate remained lower (aOR 0.58, 95% CI 0.43–0.77; P<0.001), and the ongoing pregnancy rate remained higher (aOR 1.29, 95% CI 1.13–1.47; P<0.001), in scHRT-FET after adjustment for confounders. However, the implantation rate (aOR 0.95, 95% CI 0.85–1.05; P=0.315), chemical pregnancy rate (aOR1.05, 95% CI 0.92–1.20; P=0.459), and clinical pregnancy rate (aOR1.12, 95% CI 0.98–1.27; P=0.107) were similar between the two groups after correcting for confounders.
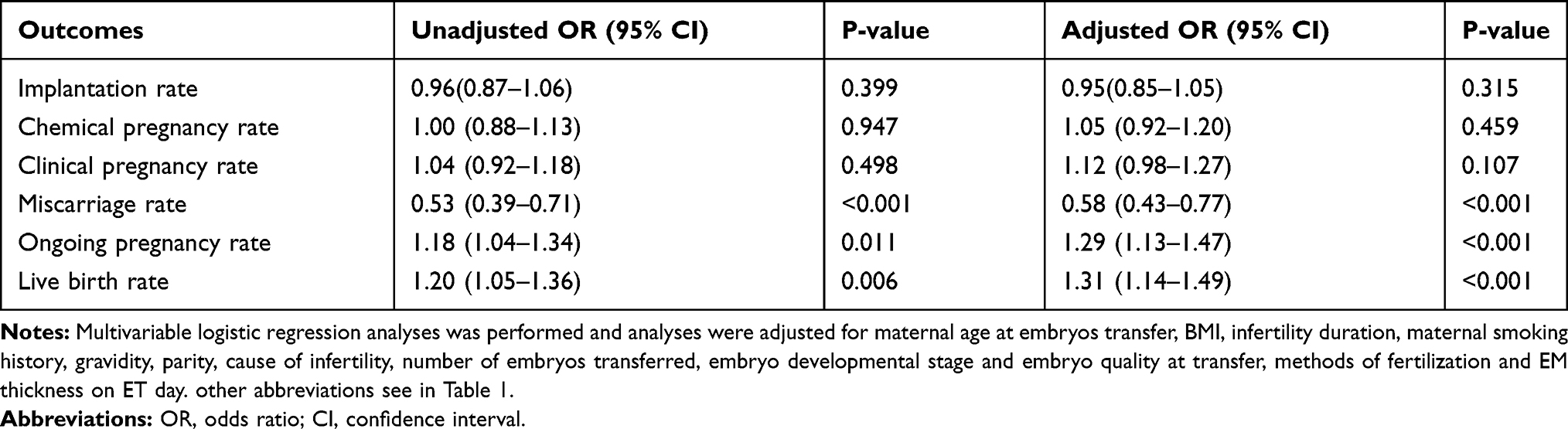 |
Table 4 Logistic regression on reproductive outcomes of scHRT-FET versus HRT-FET |
Discussion
The results of this study indicated that adjuvant vaginal use of sildenafil significantly improved the LBR compared with no adjuvant in the first FET cycle with an HRT programme in the whole population of infertile women with adequate endometrium. Furthermore, adjuvant use of SC significantly increased the ongoing pregnancy rate and reduced the miscarriage rate, especially the rate of early pregnancy loss, which might be attributed to the ameliorative effects of endometrial blood supply and receptivity. However, no significant difference was observed in the thickness of endometrium, and no significant differences were shown in birth weight or PTB between the two groups.
As is well known, compared to fresh ET with supra-physiologic hormones, embryos can be transferred into a more physiologic intrauterine environment in FET programmes; furthermore, to enhance the cycle outcome during endometrium preparation, several adjuvant therapies, including vaginal sildenafil, have come into empiric use. The first studies of vaginal sildenafil administration were three clinical case reports with samples of 4, 10 and 105 fresh ETs, all of which showed improved endometrial blood supply and endometrial development; however, all patients had extremely thin endometrium (<7 mm), there were no control groups, and no further analyses were presented.12,18,19 To date, only two case–control studies that explore the effect of sildenafil for endometrial preparation before embryo transfer have been published. One study involving FET cycles and the adjuvant use of oral sildenafil with thin-endometrium (<7 mm) patients (40 cases in the sildenafil group and 40 cases in the control group) showed better endometrial thickness and morphology (triple line patterns) in the sildenafil group; however, due to the limited sample size, they failed to reach statistical significance in terms of pregnancy outcomes, such as implantation and chemical pregnancy rate.20 The other study, involving fresh ET cycles and the adjuvant use of vaginal sildenafil in thin endometrium (<7 mm) patients with repeated implantation failures (22 cases in the sildenafil group and 22 cases in the control group), showed seemingly better chemical (33.3% vs 17.6%; P=0.490) and clinical pregnancy rates (19.0% vs 17.6%; P=0.464); however, they also failed to reach statistical significance due to the exceedingly small sample size.21 Furthermore, both studies failed to report LBR, a very convincing indicator of long-term follow-up of eventual pregnancy outcomes, and their results were not adjusted by known confounding factors, especially maternal age, maternal body mass index (BMI), number of embryos transferred and embryo quality.
Although the mechanisms underlying the beneficial effect of adjuvant use of vaginal sildenafil on pregnancy outcomes remain unknown, the improvement is most likely due to the vasodilation effect of sildenafil in the uterus. In murine studies, sildenafil has been shown to improve uterine arterial blood flow, increase birth weight and placental weight and decrease foetal mortality in pregnant rats29; another study concluded that sildenafil had a significant effect on the resistance index in the uterine artery in pre-eclamptic rats and could improve weight gain and increase survival rates without fetotoxic effects30; and a study by Dilworth confirmed and extended the evidence that sildenafil may improve foetal growth even in normal placental blood flow mouse models, indicating that sildenafil might be helpful in even broader populations.31 In clinical research, despite controversy, sildenafil was found to promote human foetal weight gain by increasing blood flow within the uteroplacental bed and extending pregnancy time in IUGR and preeclampsia.32,33 Second, rather than increasing EM thickness, sildenafil may enhance trophoblast function and improve endometrial receptivity. Although some studies suggested that sildenafil improved the EM thickness among thin-endometrium patients,12,16 another study failed to show that sildenafil could increase the EM thickness,34 and micro-morphological assessments of uterine luminal epithelium height did not show notable alterations in EM thickness after administration of sildenafil,35 which was in accordance with our findings that no significant difference was observed in EM thickness after sildenafil suppositories. Other studies showed that sildenafil could prevent apoptosis of human first-trimester trophoblast cells exposed to oxidative stress;36 alter the trophoblast phenotype and stimulate human trophoblast invasion;17 and directly enhance endometrial receptivity by affecting β3 integrin and VEGF expression levels in the murine implantation window period.37 Third, other mechanisms are still being discovered in relation to sildenafil; one study showed that sildenafil could block inflammatory injury in an LPS-induced mouse abortion model, therefore decreasing pregnancy loss,38 and another study showed that sildenafil could decrease natural killer cell activity and could enhance the chance of successful pregnancy in women with recurrent miscarriage.39 Moreover, an animal model demonstrated that pretreatment with sildenafil could protect the ovaries from cisplatin-induced damage in rats40; and Trakakis reported that sildenafil could improve ovarian response and result in a successful live birth in a woman with previous nonresponse to the sole use of gonadotropin as an adjunct to COH protocols.41 All these findings together might contribute to the decreased miscarriage rate and elevated ongoing pregnancy rate and LBR with the vaginal supplementation of sildenafil.
The use of assisted reproductive technologies (ARTs), including IVF, has contributed to the increase of twin birth rates compared to natural conception.42 In our study, the implantation rates between the two groups were comparable; however, the proportion of multiple pregnancies during the implantation stage was higher in the non-SC group (supplementary Table 1). This phenomenon is complicated, and we still do not fully understand it. Previous studies have suggested that endometrial receptive perturbation might be a risk factor for multiple pregnancies, especially monozygotic twinning after in vitro fertilization; since the majority of the multiple pregnancies in this study are dizygotic, we speculate that this might also be applied to dizygotic twinning.43 Although prior research showed that twin pregnancies after IVF have a greater likelihood of survival than singleton pregnancies,44 in our study, the proportions of multiple pregnancies among miscarriages between the two groups are statistically no different (supplementary Table 1). Moreover, a recent study suggested that peri-implantation cytokine profiles differ between singleton and twin IVF pregnancies; specifically, maternal serum levels of CXCL10 were found to be significantly lower in the earliest implantation phase in dizygotic twin conceptions compared to singleton conceptions.45 We believe that, as a vasodilator, SC might influence the cytokine microenvironment during the implantation stage. Whether SC could shift the peri-implantation cytokine profile is an interesting question, and future studies are needed to further confirm the influence of SC on multiple pregnancy during the peri-implantation period.
This study is a retrospective cohort study, with the associated inherent bias. With this in mind, we took steps to minimize possible flaws in our data. The greatest advantages of this study were that 10,069 women undergoing their first hormone replacement FET were included, possible confounding factors related to reproductive outcomes were adjusted for, and LBR was reported; all of these efforts were missing from existing studies. Another limitation of previous studies was that only patients with thin EM (<7 mm) were studied; the results of this study might suggest a new clinical practice to improve reproductive outcomes in a much larger infertile population.
In summary, after adjustment for pregnancy-related confounding factors, our large retrospective study demonstrated that adjuvant vaginal use of sildenafil citrate significantly increased the ongoing pregnancy rate and decreased the miscarriage rate, especially the early miscarriage rate, in hormone replacement FET, thus significantly improving the LBR compared with the control group. This improvement might be due to enhanced endometrial blood supply and receptivity in the sildenafil group. No significant differences were found in EM thickness, birth weight or PTB after adjuvant vaginal use of sildenafil in hormone replacement FET. In addition, future studies to further investigate human endometrial receptivity after adjuvant use of sildenafil and larger prospective studies are also welcomed.
Acknowledgments
We gratefully acknowledge all the staff of the department of assisted reproduction of Shanghai Ninth People’s Hospital for their support and cooperation.
Funding
Grants supporting this study were provided by the National Natural Science Foundation of China (NSFC) (81501334 to Y.T., 81801527 to N.L.W.).
Disclosure
None of the authors have any conflicts of interest to declare.
References
1. Saito K, Kuwahara A, Ishikawa T, et al. Endometrial preparation methods for frozen-thawed embryo transfer are associated with altered risks of hypertensive disorders of pregnancy, placenta accreta, and gestational diabetes mellitus. Hum Reprod. 2019;34(8):1567–1575. doi:10.1093/humrep/dez079
2. Maheshwari A, Raja EA, Bhattacharya S. Obstetric and perinatal outcomes after either fresh or thawed frozen embryo transfer: an analysis of 112,432 singleton pregnancies recorded in the Human Fertilisation and Embryology Authority anonymized dataset. Fertil Steril. 2016;106(7):1703–1708. doi:10.1016/j.fertnstert.2016.08.047
3. Stormlund S, Sopa N, Zedeler A, et al. Freeze-all versus fresh blastocyst transfer strategy during in vitro fertilisation in women with regular menstrual cycles: multicentre randomised controlled trial. BMJ. 2020;370:m2519.
4. Santos-Ribeiro S, Mackens S, Popovic-Todorovic B, et al. The freeze-all strategy versus agonist triggering with low-dose hCG for luteal phase support in IVF/ICSI for high responders: a randomized controlled trial. Hum Reprod. 2020.
5. Maheshwari A, Pandey S, Amalraj Raja E, Shetty A, Hamilton M, Bhattacharya S. Is frozen embryo transfer better for mothers and babies? Can cumulative meta-analysis provide a definitive answer? Hum Reprod Update. 2018;24(1):35–58.
6. Hipp H, Crawford S, Kawwass JF, et al. National trends and outcomes of autologous in vitro fertilization cycles among women ages 40 years and older. J Assist Reprod Genet. 2017;34(7):885–894.
7. De Geyter C, Calhaz-Jorge C, Kupka MS, et al. ART in Europe, 2015: results generated from European registries by ESHRE. Hum Reprod Open. 2020;2020(1):hoz038.
8. Fanchin R, Righini C, Schonauer LM, Olivennes F, Cunha Filho JS, Frydman R. Vaginal versus oral E(2) administration: effects on endometrial thickness, uterine perfusion, and contractility. Fertil Steril. 2001;76(5):994–998.
9. Jung H, Roh HK. The effects of E2 supplementation from the early proliferative phase to the late secretory phase of the endometrium in hMG-stimulated IVF-ET. J Assist Reprod Genet. 2000;17(1):28–33.
10. Rubinstein M, Marazzi A. Polak de Fried E. Low-dose aspirin treatment improves ovarian responsiveness, uterine and ovarian blood flow velocity, implantation, and pregnancy rates in patients undergoing in vitro fertilization: a prospective, randomized, double-blind placebo-controlled assay. Fertil Steril. 1999;71(5):825–829.
11. Hurst BS, Bhojwani JT, Marshburn PB, Papadakis MA, Loeb TA, Matthews ML. Low-dose aspirin does not improve ovarian stimulation, endometrial response, or pregnancy rates for in vitro fertilization. Journal of Experimental & Clinical Assisted Reproduction. 2005;2(1):8. doi:10.1186/1743-1050-2-8
12. Sher G. Vaginal sildenafil (Viagra): a preliminary report of a novel method to improve uterine artery blood flow and endometrial development in patients undergoing IVF. Hum Reprod. 2000;15(4):806–809. doi:10.1093/humrep/15.4.806
13. Shehata NAA, Ali HAA, Fahim AS, Katta MA, Hussein GK. Addition of sildenafil citrate for treatment of severe intrauterine growth restriction: a double blind randomized placebo controlled trial. J Matern Fetal Neonatal Med. 2018;1–7.
14. Sharp A, Cornforth C, Jackson R, et al. Maternal sildenafil for severe fetal growth restriction (STRIDER): a multicentre, randomised, placebo-controlled, double-blind trial. Lancet Child Adolesc Health. 2018;2(2):93–102. doi:10.1016/S2352-4642(17)30173-6
15. Gillis EE, Mooney JN, Garrett MR, Granger JP, Sasser JM. Sildenafil Treatment Ameliorates the Maternal Syndrome of Preeclampsia and Rescues Fetal Growth in the Dahl Salt–Sensitive Rat. Hypertension. 2016;67(3):647–653. doi:10.1161/HYPERTENSIONAHA.115.06071
16. Takasaki A, Tamura H, Miwa I, Taketani T, Shimamura K, Sugino N. Endometrial growth and uterine blood flow: a pilot study for improving endometrial thickness in the patients with a thin endometrium. Fertil Steril. 2010;93(6):1851–1858. doi:10.1016/j.fertnstert.2008.12.062
17. Bolnick JM, Kilburn BA, Bolnick AD, et al. Sildenafil stimulates human trophoblast invasion through nitric oxide and guanosine 3′,5′-cyclic monophosphate signaling. Fertil Steril. 2015;103(6):1587. doi:10.1016/j.fertnstert.2015.02.025
18. Paulus WE, Strehler E, Zhang M, Jelinkova L, El-Danasouri I, Sterzik K. Benefit of vaginal sildenafil citrate in assisted reproduction therapy. Fertil Steril. 2002;77(4):846–847. doi:10.1016/S0015-0282(01)03272-1
19. Sher G, Fisch JD. Effect of vaginal sildenafil on the outcome of in vitro fertilization (IVF) after multiple IVF failures attributed to poor endometrial development. Fertil Steril. 2002;78(5):1073–1076. doi:10.1016/S0015-0282(02)03375-7
20. Dehghani Firouzabadi R, Davar R, Hojjat F, Mahdavi M. Effect of sildenafil citrate on endometrial preparation and outcome of frozen-thawed embryo transfer cycles: a randomized clinical trial. Iran J Reprod Med. 2013;11(2):151–158.
21. Moini A, Zafarani F, Jahangiri N, et al. The effect of vaginal sildenafil on the outcome of assisted reproductive technology cycles in patients with repeated implantation failures: a randomized placebo-controlled trial. Int J Fertil Steril. 2020;13(4):289–295.
22. Pirtea P, de Ziegler D, Poulain M, Ayoubi JM. Which key performance indicators are optimal to assess clinical management of assisted reproduction cycles? Fertil Steril. 2020;114(1):24–30.
23. Kuang Y, Chen Q, Fu Y, et al. Medroxyprogesterone acetate is an effective oral alternative for preventing premature luteinizing hormone surges in women undergoing controlled ovarian hyperstimulation for in vitro fertilization. Fertil Steril. 2015;104(1):62–70.
24. Zhang J, Liu H, Wang Y, et al. Letrozole use during frozen embryo transfer cycles in women with polycystic ovary syndrome. Fertil Steril. 2019;112(2):371–377.
25. Cummins JM, Breen TM, Harrison KL, Shaw JM, Wilson LM, Hennessey JF. A formula for scoring human embryo growth rates in in vitro fertilization: its value in predicting pregnancy and in comparison with visual estimates of embryo quality. J in vitro Fert Embryo Transf. 1986;3(5):284–295.
26. Gardner DK, Lane M, Stevens J, Schlenker T, Schoolcraft WB. Blastocyst score affects implantation and pregnancy outcome: towards a single blastocyst transfer. Fertil Steril. 2000;73(6):1155–1158.
27. Zhang J, Liu H, Mao X, et al. Effect of body mass index on pregnancy outcomes in a freeze-all policy: an analysis of 22,043 first autologous frozen-thawed embryo transfer cycles in China. BMC Med. 2019;17(1):114.
28. Du T, Wang Y, Fan Y, et al. Fertility and neonatal outcomes of embryos achieving blastulation on Day 7: are they of clinical value? Hum Reprod. 2018;33(6):1038–1051.
29. Ramesar SV, Mackraj I, Gathiram P, Moodley J. Sildenafil citrate improves fetal outcomes in pregnant, L-NAME treated, Sprague-Dawley rats. Eur J Obstet Gynecol Reprod Biol. 2010;149(1):22–26.
30. Herraiz S, Pellicer B, Serra V, et al. Sildenafil citrate improves perinatal outcome in fetuses from pre-eclamptic rats. BJOG. 2012;119(11):1394–1402.
31. Dilworth MR, Andersson I, Renshall LJ, et al. Sildenafil citrate increases fetal weight in a mouse model of fetal growth restriction with a normal vascular phenotype. PLoS One. 2013;8(10):e77748.
32. von Dadelszen P, Dwinnell S, Magee LA, et al. Sildenafil citrate therapy for severe early-onset intrauterine growth restriction. BJOG. 2011;118(5):624–628.
33. Trapani A, Goncalves LF, Trapani TF, Vieira S, Pires M, Pires MM. Perinatal and hemodynamic evaluation of sildenafil citrate for preeclampsia treatment: a randomized controlled trial. Obstet Gynecol. 2016;128(2):253–259.
34. Check JH, Graziano V, Lee G, Nazari A, Choe JK, Dietterich C. Neither sildenafil nor vaginal estradiol improves endometrial thickness in women with thin endometria after taking oral estradiol in graduating dosages. Clin Exp Obstet Gynecol. 2004;31(2):99–102.
35. Golkar MH, Saeedi Borujeni MJ, Rashidi B. The effects of administrated sildenafil citrate on uterine luminal epithelium height associated with ovarian angiogenesis: an experimental animal study. Adv Biomed Res. 2017;6:164.
36. Bolnick JM, Kilburn BA, Bolnick AD, et al. Sildenafil prevents apoptosis of human first-trimester trophoblast cells exposed to oxidative stress: possible role for nitric oxide activation of 3ʹ,5ʹ-cyclic guanosine monophosphate signaling. Reprod Sci. 2015;22(6):718–724.
37. Biyiksiz PC, Filiz S, Vural B. Is sildenafil citrate affect endometrial receptivity? An immunohistochemical study. Gynecol Endocrinol. 2011;27(10):767–774.
38. Luna RL, Nunes AK, Oliveira AG, et al. Sildenafil (Viagra(R)) blocks inflammatory injury in LPS-induced mouse abortion: a potential prophylactic treatment against acute pregnancy loss? Placenta. 2015;36(10):1122–1129.
39. Jerzak M, Kniotek M, Mrozek J, Gorski A, Baranowski W. Sildenafil citrate decreased natural killer cell activity and enhanced chance of successful pregnancy in women with a history of recurrent miscarriage. Fertil Steril. 2008;90(5):1848–1853.
40. Taskin MI, Yay A, Adali E, Balcioglu E, Inceboz U. Protective effects of sildenafil citrate administration on cisplatin-induced ovarian damage in rats. Gynecol Endocrinol. 2015;31(4):272–277.
41. Trakakis E, Vaggopoulos V, Sioulas VD, et al. The contribution of sildenafil (Viagra) to ovarian stimulation with gonadotropins in a woman with poor ovarian response. Gynecol Endocrinol. 2014;30(7):478–480.
42. Pinborg A. IVF/ICSI twin pregnancies: risks and prevention. Hum Reprod Update. 2005;11(6):575–593.
43. Busnelli A, Dallagiovanna C, Reschini M, Paffoni A, Fedele L, Somigliana E. Risk factors for monozygotic twinning after in vitro fertilization: a systematic review and meta-analysis. Fertil Steril. 2019;111(2):302–317.
44. Tummers P, De Sutter P, Dhont M. Risk of spontaneous abortion in singleton and twin pregnancies after IVF/ICSI. Hum Reprod. 2003;18(8):1720–1723.
45. Simpson S, Kaislasuo J, Peng G, et al. Peri-implantation cytokine profile differs between singleton and twin IVF pregnancies. Am J Reprod Immunol. 2020;e13348.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.