")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Adherence to Option B+ Care for the Prevention of Mother-to-Child Transmission Among Pregnant Women in Ethiopia
Authors Wondimu F , Yetwale F , Admassu E, Binu W , Bulto GA , Lake G , Girmaye E , Temesgen K , Marama T
Received 17 September 2020
Accepted for publication 10 November 2020
Published 19 November 2020 Volume 2020:12 Pages 769—778
DOI https://doi.org/10.2147/HIV.S282463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Fikadu Wondimu,1 Fisseha Yetwale,2 Endashew Admassu,2 Wakgari Binu,3 Gizachew Abdissa Bulto,1 Getie Lake,2 Eden Girmaye,1 Kababa Temesgen,1 Taklu Marama4
1Department of Midwifery, College of Medicine and Health Sciences, Ambo University, Ambo, Ethiopia; 2School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4Department of Midwifery, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Wakgari Binu
School of Public Health, College of Health Sciences and Medicine, Wolaita Sodo University, P.o. Box: 138, Wolaita Sodo, Ethiopia
Tel +251 910107704
Email [email protected]
Purpose: Even if progressive efforts were made in Ethiopia, half of new HIV infections result from mother-to-child transmission. Limited studies assessed the level and factors of adherence that differ among different populations across the country. So, this study aimed to investigate the level and predictors of adherence to the prevention of mother-to-child transmission (PMTCT) Option B+ care among pregnant women in central Ethiopia.
Methods: A facility-based cross-sectional study design was conducted to interview 347 HIV positive pregnant women. Using a multistage sampling technique, participants were recruited from twelve health facilities based on probability proportional to the number of clients. The collected data on socio-demographics, healthcare delivery, clinical and individual factors were entered into EpiInfo v7.2.2.6, and further analysis was done using SPSS v23 software. Adherence was measured based on client self-report either as adherent and non-adherent. Bivariate and multivariate logistic regressions were undertaken to see the association between variables. Statistically significant variables were declared using an adjusted odds ratio with a 95% confidence interval.
Results: The overall adherence to option B+ was 80.2% (95% CI: 76.3– 84.5%). Time of ART initiation (AOR=3.23; 95% CI: 1.09– 6.59), fear of stigma for taking ARV (AOR=5.06; 95% CI: 1.79– 10.26), ANC appointment (AOR=4.62; 95% CI: 1.48– 6.42), male partner support (AOR=2.23; 95% CI: 1.11– 4.50), and counseling (AOR=5.36: 95% CI: 1.00– 8.58) were the associated factors with level of adherence.
Conclusion: The overall adherence level to Option B+ care in this study was inadequate to suppress the viral load during pregnancy. The result revealed that keeping adherence to ARVs during pregnancy is still challenging. So, all concerned bodies need to give attention to minimize the barriers from the client, environment, and health system perspectives.
Keywords: PMTCT care, adherence level, pregnant women, Ethiopia
Plain Language Summary
Evidence in Ethiopia focused on adherence at all three phases (pregnancy, delivery, and postnatal) of mother-to-child HIV transmission at the same time. In this study the researchers thought that assessment of adherence to the prevention of mother-to-child transmission (PMTCT) Option B+ cares during the pregnancy period is important to act accordingly. The study was conducted in West Shawa, the central part of Ethiopia, where the infrastructures are expected to be more accessible than other parts of the country. Twelve health facilities providing PMTCT Option B+ cares were selected randomly. Participants were recruited consecutively until the planned sample size was reached based on proportional size allocation among the health facilities.
EpiInfov7.2.2.6 and SPSS statistical software v23 were used for data management. Bivariate and multivariate logistic regression analysis was computed to control confounders and to show predictors of adherence level. The overall adherence level to PMTCT Option B+ care in this study was low when compared to the WHO recommendation. This study had assessed the level of and found factors influencing adherence to PMTCT Option B+ during pregnancy. The finding of this study implied that reaching adequate level of adherence to ARVs during pregnancy is still challenging, even in areas with more accessible infrastructures, in Ethiopia.
Introduction
Joint United Nations Program on HIV/AIDS reported that children newly infected with HIV were 160,000 globally, in which more than 90% of cases were from sub-Sahara Africa. Mother-to-child transmission is still one of the major sources of HIV infection among young children and it accounts for 9% worldwide.1,2
The World Health Organization acclaimed Option B+ which recommends a fixed triple regimen having TDF, 3TC, and EFV once daily for life long irrespective of their CD4 count and WHO staging for all HIV positive pregnant women. Globally every year, 1.3 million women living with HIV become pregnant. Despite the increasing ART coverage from 47% to 76% since 2010, only about 1.1 million pregnant women use ART.3,4
The period of pregnancy and breastfeeding is a window in which adherence to ART is reduced posing the mother and infant at risk. Scaling up adherence to ART during pregnancy is one of the important strategies to ensure viral suppression before delivery and during breastfeeding.5,6 Evidence showed that the optimal benefits of option B+ drugs were maintained at the adherence level of ≥95% and 61–80% virologic failure was documented among those with less than 95% adherent to ARVs.7 Similarly, children of women with over 95% of adherence to ART were well protected from HIV infection while children of women with a low adherence were less protected. Non-adherence to ART (<95%) increases the risk of rapid viral replication, the development of drug-resistant HIV strains, maternal HIV disease progression and maximizes the chance of mother-to-child transmission.8–11
In 2018, Ethiopian ministry of health reported that a level of adherence to option B+ cares was not enough to ensure new HIV-free generation and suppression of maternal viral load by ART.12 Accordingly, few evidence had shown that the level of adherence was 87.1% in Tigray, 87.9% in Wollo, and 81.4% in Southern Ethiopia. Findings from these studies also found a varying predictor for adherence to option B+ care from place to place that includes poor counseling on side effects, HIV status disclosure, traveling distance from health facility, time of ART initiation, number of ANC visits, place of residence, and male partner involvement in PMTCT services.13–16
Even though the implementation of PMTCT services was started a long time in Ethiopia following the WHO recommendation, there is scarcity of data on adherence level of PMTCT option B+ in West Shawa. The available evidence did not show clear conclusion on the factors especially the association of ART initiation time with adherence level. So, this study aimed to assess the level of adherence to PMTCT option B+ care and associated factors among pregnant women attending ANC clinics at public health institutions in West Shawa. The finding of this study provides a recent evidence for healthcare providers, local and national health managers to strengthen the health system and minimize the burden of the HIV problem. Additionally, the study findings may be used as input for further researches.
Methods
Study Area and Design
This facility-based cross-sectional study was conducted from November to December 2018 in the West Shawa zone, the center of Ethiopia. The zone has 24 districts, 542 kebeles (lowest administrative level) from which 512 are peasant kebeles, and 30 are sub-city kebeles. The total population in the zone is estimated to be 2,381,079 of which 1,214,350 of them are females and 2013 pregnant women on option B+ in 2017. Currently, the zone consists of 6 hospitals, 90 health centers (HC), and 447 health posts from which 5 hospitals and 22 health centers are giving ART services. They are also providing PMTCT Option B+ services for HIV positive women during pregnancy and breastfeeding period free of charge [Data from West Shawa zone health office annual report, 2017].
Populations and Sampling
All HIV positive pregnant women attending PMTCT clinics in the health facilities were the source of population. HIV positive pregnant women attending PMTCT clinics during study period were the study population and all the selected HIV positive pregnant women attending PMTCT clinics in the health facilities during study period were the study participants. All the selected pregnant women on PMTCT Option B+ follow-up for at least four weeks were included. Pregnant women on PMTCT Option B+ follow-up but were not able to communicate were not included in the study.
A sample of 347 HIV-positive pregnant women took part in the study. The sample size was decided using a single population proportion with the assumption of a 95% CI, 5% margin of error, and estimated level of adherence to PMTCT Option B+ in Hadiya, Ethiopia (83.7%).14 To compensate for non-response, a 10% contingency, and assuming variability that might be introduced due to the multistage nature of the sampling, design effect of 1.5 was considered in advance.
A multistage sampling was used to recruit study participants. First, 12 health facilities were selected randomly from the 27 public health facilities (3 hospitals and 9 HCs) providing PMTCT Option B+ care. So, Ambo Hospital, Hinchini Hospital, Gindabarat HC, Gudar HC, Gedo HC, Ginchi HC, Holota HC, Bako HC, Ejere HC, Ilu Galan HC, Shanan HC, and Awaro HC were selected randomly. The specific sample size for each selected health facility was decided using probability proportion-to-size allocation based on client load obtained from the quarterly report of the zonal health department. Then, within each health facility, pregnant women consulting for PMTCT clinics were consecutively enrolled until the sample size was reached assuming that participants come to the health facility in a random fashion. Consecutive sampling was preferred due to the expected small number of participants per day attending the PMTCT clinic in each health facility, [Figure 1].
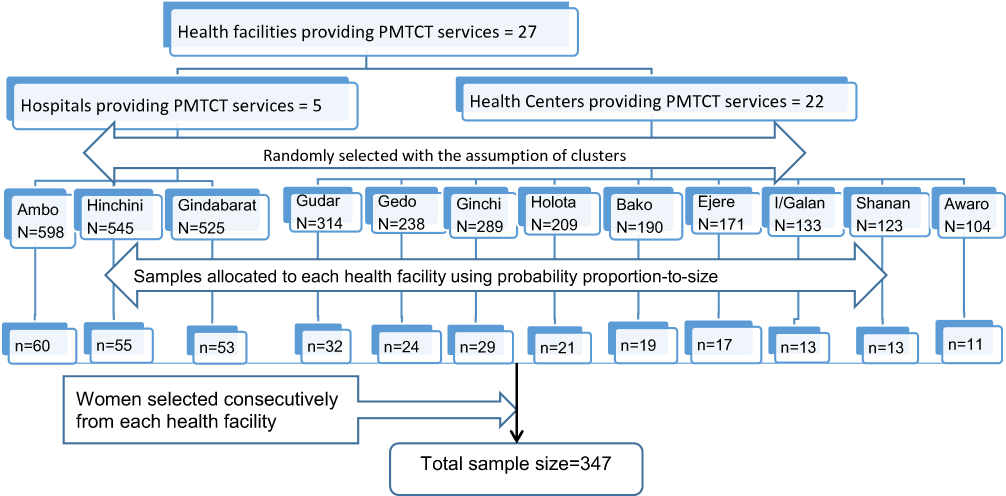 |
Figure 1 Schematic presentation of the sampling procedure. |
Data Collection Tools and Procedures
Data were collected using an interviewer-administered structured questionnaire. After prepared in English, the questionnaire was translated to Afaan Oromoo and back-translated to English by different experts to keep consistency in the meaning of words and concepts. The questionnaire included the following independent variables influencing adherence: socio-demographic characteristics, knowledge on PMTCT, attitude towards PMTCT, male partner involvement, HIV disclosure status, healthcare services, ANC follow-up.
Four questions, adapted from a standardized multi-method ART adherence measurement tool recommended for low resource settings, were used to assess self-reported adherence.17 On the day of data collection, mothers were asked to take part freely in the study, and exit-interview was made after they attended ANC follow-up visit in a private room that was arranged in each health facility for the data collection purpose. After completion of the interview, medical record review was also made to collect information on clinical characteristics of the participants like CD4 count, WHO stages, date of HIV diagnosis, date of ARV initiation. Then, both the interview and record review were sorted in the software for further analysis.
Measurements and Operational Definition
Adherence to ART
Adherence was measured using a self-reported A HIV positive pregnant woman was considered as “Adherent” if she responded “NO” to all four adherence measuring items otherwise she is “Non-adherent” adapted from the experience in South Africa. The adherence level was defined using the self-reporting method due to low recall bias in the self-report measurement tool. This method was used in earlier studies because it has been recommended for developing countries.17
Knowledge of Women About Option B+
In this study, there were six questions assessing knowledge of a woman on risk reductions of HIV transmission being on option B+ PMTCT services. A woman has “High,” “Moderate” and “Low” knowledge, if she responded a correct answer for all, 4–5, and less than 4 of the six items, respectively.13
An Attitude of the Women Toward Option B+
There were 6 items assessing attitude coded as “1=Disagree; 2=Not sure; 3=Agree” so that the score ranging from 6 to 18. In this study, a woman has “Favorable” if she scored the mean score and above (≥14 scores) otherwise she has an “Unfavorable” attitude.13
Male Involvement
The male involvement was considered as “good”, “moderate” and “low” for those who scored ≥7, 4–6, and ≤ 3, respectively, out of 10 self-reported questions.18
Data Quality Assurance and Data Management
The data collection tool was developed in English and translated to the local language “Afaan Oromoo” and then translated back to English by a different language expert. The data were collected with the tool in the Afan Oromo version. A pre-test was done on 18 (5%) of the questionnaires at the nearby health facility, Walliso Hospital. Then two days of training was given for eight data collectors and four supervisors on the data collection tool and collection procedure before the actual data collection. The completeness of each questionnaire was checked by the supervisors on daily basis. The overall process was monitored by the principal investigator.
The collected data were coded and entered to EpiInfo v7.2.2.6. Then the data were exported to SPSS statistical software v23 for further analysis. Descriptive analysis was done to describe the socio-demographic characteristics of participants and results were presented with texts, proportions, tables, and figures. The results for the negative statements were re-coded in reverse before analysis to ensure that the scoring system was consistent (e.g., attitude questions), so that all higher scores reflect a better outcome. Missing data on one of the four variables assessing the adherence level was not included the final analysis.
Bivariate logistic regression was computed and independent variables with P-value <0.2 were entered into a multivariable logistic regression to control the possible confounders. A multi-collinearity was tested using variance of inflation factor (VIF=1.88) and tolerance=0.53. The Hosmer-Lemeshow goodness of fit test was used to check the ability of the model whether it can discriminate between those participants who were adherent and those who did not (P-value >0.58). The statistical significance of independent predictor adherence to PMTCT B+ was declared using AOR with 95% CI. The result was presented with texts, tables, charts, and graphs.
Results
Socio-Demographic and Economic Characteristics of Participants
A total of 343 participants were undertaken all components of the survey making the response rate of 98.8% with the mean age of 28.94 (SD: 5.03) years. Most respondents were from urban 250 (72.9%), one fourth 88 (25.1%) were educated from grades 9–12 and, 138 (40%) were housewives, [Table 1].
 |
Table 1 Demographic and Socio-Economic Characteristics of Pregnant Women Attending PMTCT Clinic West Shawa, Ethiopia, 2018 (N= 343) |
Healthcare Delivery and Clinical Characteristics of Participants
About half of the respondents 167 (48.7%) started option B+ PMTCT drugs on the same day of HIV diagnosis. More than three-quarters of the participants were in WHO clinical stage one category at the time of ART initiation 263 (76.7%) and after treatment was started 278 (81%). The average time to reach the PMTCT site was less than one hour for about 281 (81.9%) respondents. Regarding counseling on adherence, 97.1% of the respondents were counseled on the side effects of ARV drugs, [Table 2].
 |
Table 2 Healthcare Delivery and Clinical Characteristics by Level of Adherence Among Pregnant Women in West Shawa, Ethiopia, 2018 |
Male Involvement, Knowledge on Risk Reductions, and Attitude
Our data also illustrate that 200 (58%) of the respondents’ partners had good involvement during PMTCT services for pregnant mothers [Figures 2 and S1]. About 204 (59.5%) of the respondents had high knowledge concerning the risk reduction of HIV transmission from mother to child, [Figure 3 and Table S1]. Also, the composite measure of the respondents’ attitude towards option B+ PMTCT care showed that 274 (79.9%) of the respondents had a favorable attitude on option B+ PMTCT care, [Table S2].
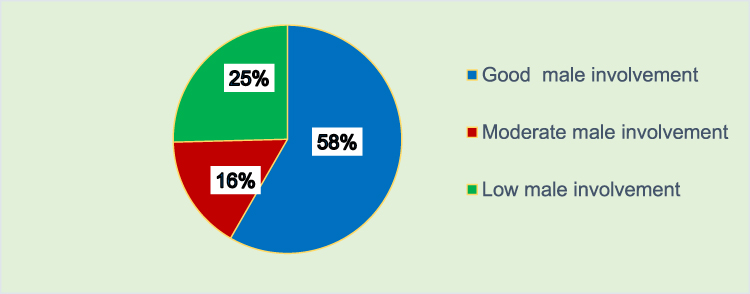 |
Figure 2 The composite proportion of male partner involved in PMTCT option B+ care for HIV positive pregnant women in West Shawa, Ethiopia, 2018. |
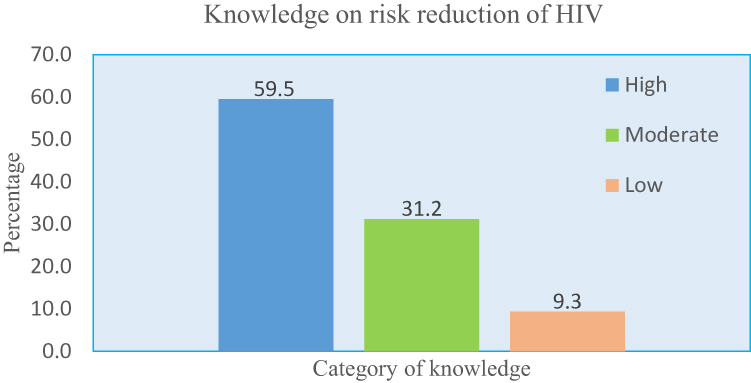 |
Figure 3 Knowledge of risk reductions among HIV positive pregnant women in West Shawa, Ethiopia, 2018. |
Adherence to Option B+ PMTCT Drugs
This study showed that the respondent’s adherence to option B+ PMTCT drugs was 80.2% (95% CI: 76.3–84.5%). All the non-adherent respondents, 68 (19.8%), had missed their ARV drugs within the last three days preceding the study. The most dominant mentioned reasons for missing drugs were forgetting when to take the medication 26 (38.2%) followed by stigma from different individuals 23 (33.8%), [Figure S2].
Factors Associated with Level of Adherence to Option B+ PMTCT Care
The result of multivariate logistic regression analysis showed that women who started ART after one month of diagnosis of HIV were 3.23 times more likely to have good adherence than those who started on the same day of their HIV diagnosis (AOR=3.23; 95% CI: 1.09–6.59). Women who have no fear of stigma for taking their ART drugs were 5.06 times more likely to have good adherence than those who have fear of stigma (AOR=5.06; 95% CI: 1.79–10.26). Those who did not miss their ANC appointment were 4.62 times more likely to have good adherence than those who missed their ANC appointment (AOR=4.62; 95% CI: 1.48–6.42). Those women whose male partner brought ARV drugs from health facility had 2.23 times more likely to have good adherence than those whose male partner support them (AOR=2.23; 95% CI: 1.11–4.50). Women who had favorable attitude towards PMTCT services were 3.78 times more likely to be adherent than who had unfavorable attitude (AOR = 3.78; 95% CI: 1.93 −7.39). Women counseled on common side effects of ARV drugs were 5.36 times more likely to be adherent to option B+ drugs than who were not counseled (AOR= 5.36: 95% CI: 1.00–8.58), [Table 3]
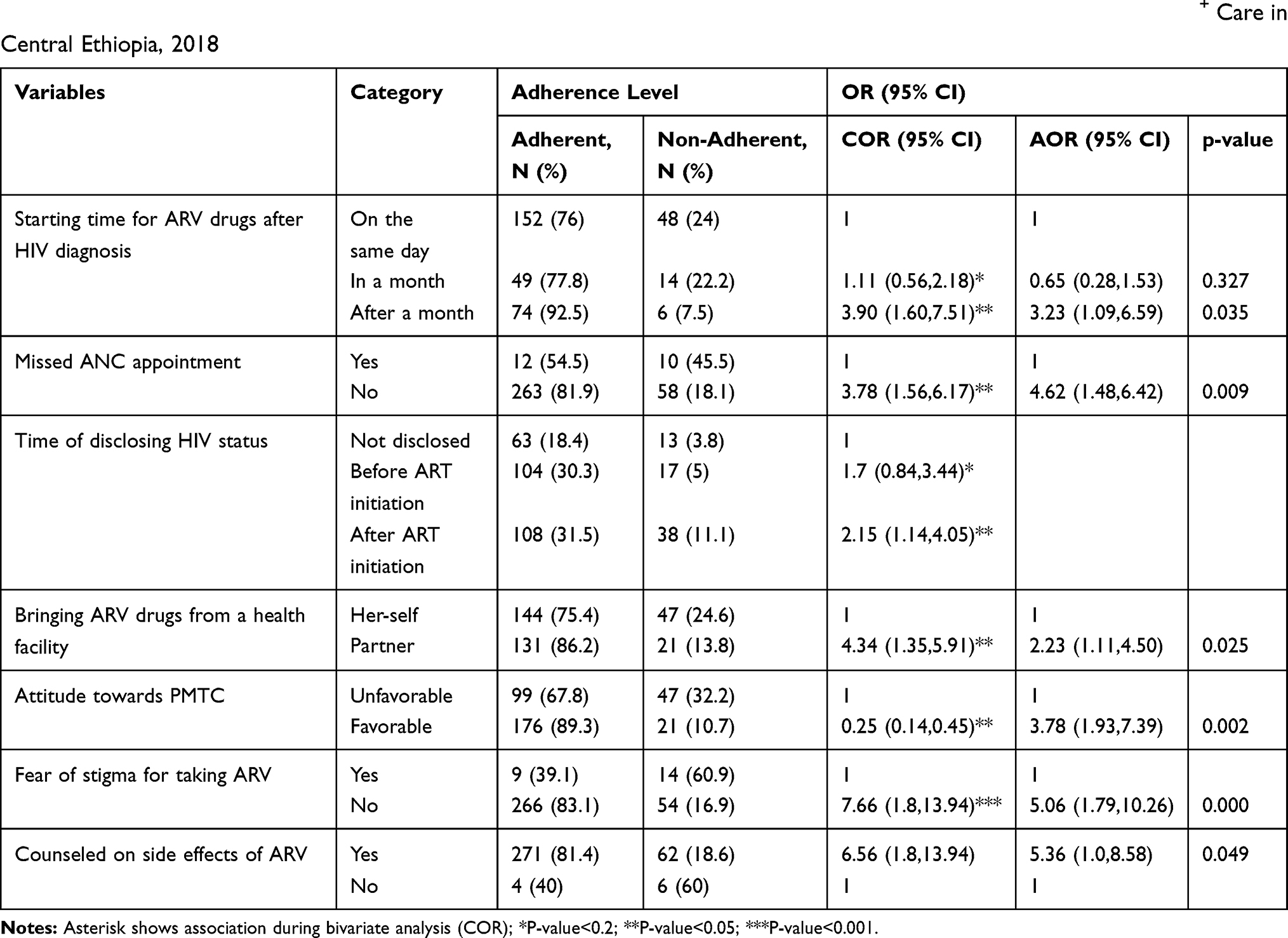 |
Table 3 Bivariate and Multivariable Logistic Regression Analysis of Associated Factors with Adherence to PMTCT Option B+ Care in Central Ethiopia, 2018 |
Discussion
In this study, we had assessed the level of adherence to PMTCT option B+ and showed associated factors among pregnant women attending antenatal clinic at a public health facilities in Wester Shawa. The time of ART initiation, fear of stigma for taking ARV drugs, ANC appointment, male partner participation during PMTCT services, attitude towards drugs, and counseling on common side effects of drugs were found as influencing factors.
The study result has revealed that 80.2% (95% CI: 76.4–84.3) of participants were adherent to PMTCT Option B+ which was in line with the earlier studies conducted in the Hadiya zone (83.7%), Afar region (81.1%), and Kisumu Kenya (84%).16,18,19 This similarity may be due to similarities in study designs and measurement methods which was a self-reported adherence measurement.
However, the finding of this study was lower than the level of adherence reported from the study conducted in the Tigray region (87.1%), South Wollo zone (87.9%), Nigeria (89.2%), and Malawi (91%).13,15,20,21 The difference might be that the earlier studies involved both pregnant and lactating mothers. The discrepancy might also be the study settings that the study conducted in Tigray had been conducted at hospitals only that might be more equipped than health centers while this study had involved both hospitals and health centers. This study reported higher finding than the findings from systematic review and meta-analysis conducted in low, middle, and high-income countries (73.5%).9 This difference might be due to the difference in study design; the pooled meta-analysis in those countries had been focused on mixed methods while ours focused on only self-reported measurement of adherence level.
In this study, respondents who started to take ARV drugs after one month of HIV diagnosis were more likely to be adherent than those who started on the same day of HIV diagnosis. This association might be supported by findings from other studies in Wollo zone of Eastern Ethiopia and Malawi. These studies reported that HIV-positive mothers who faced challenges in initiating option B plus treatment at the same day of HIV diagnosis had shown poor adherence15,22,23 But our finding was contrary to the finding from the study conducted in Southern Ethiopia in which starting ART at the time of diagnosis was significantly associated with good adherence to option B plus ART.16 Even though it needs further investigation, this might imply that initiating ARV drugs needs some period for clients to be prepared. It also implies that those mothers might feel enforced by healthcare providers to start ART cares with little support for decision-making power on their future health.
Pregnant women who did not miss their ANC appointment were more likely to be adherent than their counterparts. Similar findings were reported in Malawi and Uganda.24,25 The possible justification might be that as pregnant women stick to their ANC schedule, they may get education and relevant information about the prevention of HIV from mothers to their unborn fetus. The frequent contact with healthcare providers may also be the best opportunity to get proper counseling on adherence. Respondents whose male partner has been brought PMTCT drugs from health institutions for them were more likely to be adherent than those who brought by them-selves. This might imply that the more male partners are involved in PMTCT services, the more pregnant women are adherent to ARV drugs.
Studies reported that proper counseling on common side effects of ARV drugs was significantly associated with adherence to Option B+ PMTCT care.9,14,26 In line with this, our finding showed that pregnant women who were counseled on common side effects of ARV drugs were more likely to be adherent than those who were not well counseled. This might show that proper counseling would empower those women on decision-making so that they are more likely to be confident in the treatment, which may have an encouraging effect on adherence. Our study also showed that pregnant women who did not fear stigma to take PMTCT drugs were more likely to be adherent than those who feared stigma aroused due to being HIV positive and taking ART. A similar finding was reported by other studies.26–29 This might imply that ending stigma from family members, providers, and the local community helps clients to be more adherent to ARV drugs.
In this study, the pregnant women who had a favorable attitude toward option B+ PMTCT care were more likely to be adherent than their counterparts. This finding is supported by studies conducted in other countries.30–33 This might be is because clients with a favorable attitude towards health services have better healthcare-seeking behavior that helps them stick to their prescribed medication and recommendation given from healthcare workers.
This study had showed factors influencing adherence at a specific phase of mother-to-child transmission of HIV which is important to intervene accordingly. In our study, the level of adherence was measured based on individual self-report which might be prone to social desirability bias and might lead to overestimation of the PMTCT adherence of the pregnant mothers. Besides, future research may need to use the qualitative sampling method at the organizational and individual levels to show more factors.
Conclusion
The overall adherence level to option B+ PMTCT care in this study was low when compared to the required greater than 95% adherence level to keep adequate viral suppression before delivery. Initiating ARV drugs one month after HIV diagnosis, not missing ANC visits, male partner support for PMTCT services, absence of stigma for taking ARV drugs, favorable attitude toward PMTCT services, and good counseling on common side effects of ARV drugs were the identified factors enhancing the adherences to PMTCT Option B+ care. The result of this study implied that still there are challenges to reach the required adherence level. So, all concerned bodies need to give attention to minimize the barriers from the client, environmental, and health system perspectives.
Abbreviation
PMTCT, prevention of mother-to-child transmission; HC, health center; AOR, adjusted odds ratio; CI, confidence interval; ARV, antiretroviral; HIV, human immunodeficiency virus; ANC, antenatal care; WHO, World Health Organization; ART, antiretroviral therapy; SPSS, Statistical Package for the Social Sciences; CD4, cluster for differentiation 4; TDF, tenofovir disoproxil fumarate; 3TC, lamivudine; EFV, efavirenz.
Data Sharing Statement
All data relevant to the study are included in the article or available in the Supplementary materials. And all data are fully available to interested researchers upon reasonable request from the authors ([email protected]) if more information is needed.
Ethics Approval and Consent
We obtained ethical approval from Midwifery Ethical Review Committee of the University of Gondar with Ref. No. MIDW/10/489/2018. We had obtained verbal informed consent from participants after informing them the purpose, benefit, risk, confidentiality of the information and voluntary nature of participation in the study. The ethical review committee had approved the process of the consent and we had conducted the study as per the Declaration of Helsinki. To keep confidentiality no identifier was used and participants were interviewed in a separate room which was next to the PMTCT clinic to ensure privacy.
Acknowledgments
We would like to acknowledge the University of Gondar for giving us the opportunity for this study. We would like to extend our gratitude to the West Shawa zone Health department and the respective hospitals for all aspects of unreserved support when we needed. Our acknowledgment also goes to data collectors, supervisors, and study participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The University of Gondar, College of Health Sciences and Medicine has funded this research as part of a thesis project only but had no role in deciding to publish or preparation of the manuscript.
Disclosure
The authors declared that they have no competing interests.
References
1. World Health Organization. Global Guidance on Criteria and Processes for Validation: Elimination of Mother-To-Child Transmission of HIV and Syphilis; 2017.
2. Luzuriaga K, Mofenson LM, Campion EW. Challenges in the elimination of pediatric HIV-1 infection. N Engl J Med. 2016;374(8):761–770. doi:10.1056/NEJMra1505256
3. HIV/AIDS JUNPo. UNAIDS Data 2017. Geneva: Joint United Nations Programme on HIV. AIDS; 2017.
4. World Health Organization. Mother-To-Child Transmission of HIV; 2018.
5. Tubiana R, Le Chenadec J, Rouzioux C, et al. Factors associated with mother-to-child transmission of HIV-1 despite a maternal viral load <500 copies/mL at delivery: a case-control study nested in the French perinatal cohort (EPF-ANRS CO1). Clin Infect Dis. 2010;50(4):585–596.
6. Vrazo AC, Sullivan D, Ryan Phelps B. Eliminating mother-to-child transmission of HIV by 2030: 5 strategies to ensure continued progress. Glob J Health Sci. 2018;6(2):249–256. doi:10.9745/GHSP-D-17-00097
7. Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
8. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection: Recommendations for a Public Health Approach. World Health Organization; 2016.
9. Nachega JB, Uthman OA, Anderson J, et al. Adherence to antiretroviral therapy during and after pregnancy in low-income, middle-income, and high-income countries: a systematic review and meta-analysis. AIDS. 2012;26(16):2039–2052. doi:10.1097/QAD.0b013e328359590f
10. Awittor RJE. Adherence to Antiretroviral Therapy (ART) Among HIV Positive Women at Antiretroviral Centers in Tema. University of Ghana; 2012.
11. Sabate E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2016.
12. Ethiopian Federal Minstry of Health. National Consolidated Guidelines for Comprehensive Hiv Prevention, Care and Treatment; August, 2018:2018.
13. Ebuy H, Yebyo H, Alemayehu M. Level of adherence and predictors of adherence to the option B+ PMTCT program in Tigray, northern Ethiopia. Int J Infect Dis. 2015;33:123–129. doi:10.1016/j.ijid.2014.12.026
14. Lodebo TM, Suloro JA. Level of adherence and associated factors to option B+ PMTCT among HIV positive pregnant women in Hadiya Zone, Southern Ethiopia. Glob J Health Sci. 2017;2(1):39–58.
15. Tsegaye D, Deribe L, Wodajo S. Levels of adherence and factors associated with adherence to option B+ prevention of mother-to-child transmission among pregnant and lactating mothers in selected government health facilities of South Wollo Zone, Amhara Region, northeast Ethiopia, 2016. Epidemiol Health. 2016;38:e2016043. doi:10.4178/epih.e2016043
16. Tesfaye DJ, Hibistu DT, Abebo TA, et al. Option B plus antiretroviral therapy adherence and associated factors among HIV positive pregnant women in Southern Ethiopia. BMC Pregnancy Childbirth. 2019;19(1):82. doi:10.1186/s12884-019-2228-4
17. Steel G, Nwokike J, Joshi M. Development of a Multi-Method Tool to Measure ART Adherence in Resource-Constrained Settings: The South Africa Experience. Submitted to the U.S. Agency for International Development by the Rational Pharmaceutical Management Plus Program. Arlington, VA: Management Sciences for Health; 2007.
18. Belayihun B, Negus R. Antiretroviral Treatment Adherence Rate and Associated Factors among People Living with HIV in Dubti Hospital, Afar Regional State, East Ethiopia. International Scholarly Research Notices. 2015. doi:10.1155/2015/187360
19. Benta Akoth M, Masaba RO, Fowler MG, et al. CD4, viral load response, and adherence among antiretroviral-naive breastfeeding women receiving triple antiretroviral prophylaxis for prevention of mother-to-child transmission of HIV in Kisumu, Kenya. J Acquir Immune Defic Syndr. 2012;61(2):249–257. doi:10.1097/QAI.0b013e318262514f
20. Joseph A, Ogah OE, Robinson O, et al. Determinants of adherence to antiretroviral therapy among HIV-positive women accessing prevention of mother to child transmission services in Ebonyi State, Nigeria. Ann Med Health Sci Res. 2018;8(4).
21. Ng’ambi W, Tweya H, Speight C, et al. Determinants of antiretroviral treatment adherence among women accessing PMTCT “Option B+”: a retrospective study at Bwaila Hospital, Malawi.
22. Gugsa S, Potter K, Tweya H, et al. Exploring factors associated with ART adherence and retention in care under Option B+ strategy in Malawi: a qualitative study. PLoS One. 2017;12(6):e0179838. doi:10.1371/journal.pone.0179838
23. Haas AD, Msukwa MT, Egger M, et al. Adherence to antiretroviral therapy during and after pregnancy: a cohort study on women receiving care in Malawi’s Option B+ program. Clin Infect Dis. 2016;63(9):1227–1235.
24. Tenthani L, Haas AD, Tweya H, et al. Retention in care under universal antiretroviral therapy for HIV-infected pregnant and breastfeeding women (“Option B+”) in Malawi. AIDS. 2014;28(4):589. doi:10.1097/QAD.0000000000000143
25. Buregyeya E, Naigino R, Mukose A, et al. Facilitators and barriers to uptake and adherence to lifelong antiretroviral therapy among HIV infected pregnant women in Uganda: a qualitative study. BMC Pregnancy Childbirth. 2017;17(1). doi:10.1186/s12884-017-1276-x
26. Lumbantoruan C, Kermode M, Giyai A, et al. Understanding women’s uptake and adherence in Option B+ for prevention of mother-to-child HIV transmission in Papua, Indonesia: a qualitative study. PLoS One. 2018;13(6):e0198329. doi:10.1371/journal.pone.0198329
27. Hodgson I, Plummer ML, Konopka SN, et al. A systematic review of individual and contextual factors affecting ART initiation, adherence, and retention for HIV-infected pregnant and postpartum women. PLoS One. 2014;9(11):e111421. doi:10.1371/journal.pone.0111421
28. Cornelius LJ, Erekaha SC, Okundaye JN, et al. A socio-ecological examination of treatment access, uptake and adherence issues encountered by HIV-positive women in Rural North-Central Nigeria. J Evid Inf Soc Work. 2018;15(1):38–51. doi:10.1080/23761407.2017.1397580
29. Atanga PN, Ndetan HT, Achidi EA, et al. Retention in care and reasons for discontinuation of lifelong antiretroviral therapy in a cohort of cameroonian pregnant and breastfeeding HIV-positive women initiating ‘Option B+’ in the South West Region. Trop Med Int Health. 2017;22(2):161–170. doi:10.1111/tmi.12816
30. Omonaiye O, Kusljic S, Nicholson P, Manias E. Medication adherence in pregnant women with human immunodeficiency virus receiving antiretroviral therapy in sub-Saharan Africa: a systematic review. BMC Public Health. 2018;18(1). doi:10.1186/s12889-018-5651-y
31. Boateng D, Kwapong GD, Agyei-Baffour P. Knowledge, perception about antiretroviral therapy (ART) and prevention of mother-to-child-transmission (PMTCT) and adherence to ART among HIV positive women in the Ashanti Region, Ghana: a cross-sectional study. BMC Womens Health. 2013;13(1). doi:10.1186/1472-6874-13-2
32. Kohler PK, Ondenge K, Mills LA, et al. Shame, guilt, and stress: community perceptions of barriers to engaging in Prevention of Mother to Child Transmission (PMTCT) programs in Western Kenya. AIDS Patient Care STDS. 2014;28(12):643–651. doi:10.1089/apc.2014.0171
33. Clouse K, Schwartz S, Van Rie A, et al. “What they wanted was to give birth; nothing else”: barriers to retention in Option B+ HIV care among postpartum women in South Africa. J Acquir Immune Defic Syndr. 2014;67(1):e12–e18. doi:10.1097/QAI.0000000000000263
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.