")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Adherence to Inhaled Therapy in Patients with COPD Associated to Pneumoconiosis
Authors Peng Y , Duan J , Li X , Zeng Y, Zhou Z, Deng M , Ouyang R, Chen Y, Cai S, Chen P
Received 3 July 2021
Accepted for publication 13 September 2021
Published 27 September 2021 Volume 2021:16 Pages 2697—2706
DOI https://doi.org/10.2147/COPD.S327686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Yating Peng,1– 3 Jiaxi Duan,1– 3 Xin Li,4 Yuqin Zeng,1– 3 Zijing Zhou,1– 3 Minghua Deng,1– 3,5 Ruoyun Ouyang,1– 3 Yan Chen,1– 3 Shan Cai,1– 3 Ping Chen1– 3
1Department of Pulmonary and Critical Care Medicine, The Second Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2Research Unit of Respiratory Disease, Central South University, Changsha, Hunan, People’s Republic of China; 3Hunan Centre for Evidence-Based Medicine, Changsha, Hunan, People’s Republic of China; 4Division of Occupational Lung Disease, Hunan Prevention and Treatment Institute for Occupational Diseases, Changsha, Hunan, People’s Republic of China; 5Department of Respiratory, PLA Rocket Force Characteristic Medical Center, Beijing, People’s Republic of China
Correspondence: Ping Chen Email [email protected]
Background: Pneumoconiosis has high prevalence of chronic obstructive pulmonary disease (COPD), respiratory morbidity, and mortality.
Objective: The aim of the present study was to examine patient characteristics and adherence to inhaled therapy among pneumoconiosis with COPD in a real-world clinical setting.
Methods: A cohort of pneumoconiosis patients with COPD prescript with at least one type of long-acting inhaled drug was followed for adherence for 2 years. Demographic and COPD-related characteristics were collected in baseline.
Results: In baseline, after adjusting for age, dust exposure duration positively correlated with number of acute exacerbation (AE) frequency in the last year. There were close associations among COPD Assessment Tool (CAT) score, modified Medical Research Council Dyspnea Scale (mMRC) grade, number of AE, and pre-FEV1 value. Of 296 participants originally recruited, 213 participants finished the 2-year follow-up for adherence. 122 (57.28%) were non-adherent to inhaled therapy. The most common reason for non-adherence was “relief of symptoms after short-term controller medication use” (53.28%). Patients who were non-adherent reported higher body mass index (BMI), less AE events in the last year, higher pre-FEV1 value, higher post-FEV1 value and low CAT, mMRC scores compared to adherent in baseline. High pre-FEV1 value (OR = 1.04, CI = 1.018– 1.064) and low mMRC scores (OR = 0.406, CI = 0.214– 0.771) were risk factors found associated with non-adherence.
Conclusion: A majority of pneumoconiosis patients complicated with COPD have suboptimal inhaled therapy adherence. Evidence-based, adherence-enhancing interventions should be targeted on less severe subjects.
Keywords: adherence, inhaled therapy, pneumoconiosis, COPD
Introduction
COPD is a common, preventable, and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.1 Cigarette smoking is recognized as the most common and important cause of COPD.2 Besides tobacco smoke, occupational exposures are important factors in COPD and other lung diseases.2,3 Patients exposed to silicosis or coal have increased risk of COPD, our previous study4 and other’s study5 have shown that the prevalence of COPD was up to 40% in pneumoconiosis in China. Notably, our group first reported that patients with COPD who suffered from occupational exposure developed more severe dyspnea than those exposed to tobacco alone.6 Moreover, COPD patients exposed to occupational dust have distinct exposure pattern and different imaging and pathology features compared to those exposed to cigarette smoke.2,7,8 The effect of dust on emphysema is small7 but on opacity profusion and fibrosis8 is prominent when compared to the effect of tobacco smoking. However, owing to the limited research on COPD patients exposed to occupational dust with or without cigarette smoke, relevant clinical characteristics and the prognosis is unclear. Recently, a large retrospective cohort study showed there is excess risk of death from COPD among workers with silicosis in Hong Kong, with smoking-adjusted standardized mortality ratio (SMR) of 2.03.9 These drive us to pay attention to COPD patients with occupation dust exposure.
The first-line drug treatment for COPD are inhaled bronchodilators or in combination with corticosteroids. There have been several studies which have explored adherence to inhaled therapy in COPD with varying results.10 The levels of adherence among COPD patients are ranging from as low as 20% to over 60% in different studies.11,12 Amongst others, some factors found to be associated with non-adherence to inhaled therapy in COPD include age, gender, education, race, disease severity, smoking status, and disease knowledge.13–18And non-adherence to prescribed inhaled therapy contributes to exacerbations, patient mortality, and health care costs in COPD.19–21
The availability of an accurate method to measure inhaled therapy adherence in COPD patients is essential for detecting patients with poor adherence. Depending on the environment and type of treatment, the methods of assessing adherence to medication include electronic monitoring methods (smart-inhaler), pharmacy refill methods, inhaled drug device remaining counts, patient and caregiver report measures or questionnaires, but they are all burdened with important limitations. Electronically monitored inhalers are suitable for intervention studies and pharmacy refill highly relies on the National Medical Record System. While self-reporting of treatment compliance could introduce recall bias by either over-reporting or under-reporting depending on patient’s behavior in the recent past.22 To date, there is no “gold standard” self-report questionnaire to assess treatment adherence in COPD patients.
In the clinic, we found COPD patients with only tobacco smoke have a higher diagnosis rate, have more opportunities to take smoking cessation and other education programs, and receive more active treatments compared to COPD patients with other risk factors. We hypothesize that COPD patients with occupational dust exposure are different from the rest of COPD. Despite compelling evidence on non-adherence to long-term inhaled medications in COPD and its consequences elsewhere, there is paucity of information on adherence of this hard-to-reach population of pneumoconiosis with COPD. Therefore, this analysis, set within a prospective observational study of pneumoconiosis complicated with COPD prescript with inhaled therapy, aims to: describe patient characteristics; describe rates and reasons of non-adherence to inhaled therapy; and access main risk factors of non-adherence to inhaled therapy.
Methods
Setting and Participants
The study was performed in the Second Xiangya Hospital and Hunan Prevention and Treatment Institute for Occupational Diseases. This study was registered on the Chinese Clinical Trial Registry (ChiCTRPOC-17010431, http://www.chictr.org.cn/). This study was performed following the ethics principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University in Changsha, Hunan (NO. 2016032).
Patients with International Classification of Diseases (ICD)-10 diagnosis code for pneumoconiosis and COPD and receiving inhaled therapy between March 2017 and May 2019 were recruited and observed for 2 years. Individuals were excluded if they were seriously ill or refused to participate. In baseline, participants completed a questionnaire detailing demographic data, self-reported smoking index, and dust exposure duration. Smoking index was calculated as pack×year. Dust exposure duration was calculated as hour×year. A smoker was defined as continuous smoking exposure of more than 10 pack-years. Patients who had sustained abstinence for more than 6 months were former smokers. The impact of COPD on health status was assessed using the 8-item CAT score.23 The level of breathlessness experienced by the patient was assessed via the mMRC dyspnea scale.24 The number of AE referred in the last year was also evaluated. Meanwhile, spirometric measurements were performed by experienced and skilled technicians and met the standards of the American Thoracic Society and the European Respiratory Society.25 Patients were also classified into one of four Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2017 categories (ABCD) based on the intensity of respiratory symptoms and previous exacerbations.1
Assessment of Adherence
During the 2 years of follow-up, telephone contact follow-ups were arranged every 6 months following the first visit at the outpatient clinic through a follow-up questionnaire, including months of inhaled drug use in the past 6 months, reasons for withdrawal, and change in therapies. Adherence to inhaler therapy, based on the 2-year follow-up periods, was defined by the proportion of reported total months of inhaled drug usage to 24 months. The 80% cut-off has been shown to offer the optimal balance between specificity and sensitivity for self-reported and prescription refill adherence measures.26 Adherence was classified as follows: adherent (≥80%), non-adherent (<80%).
For each visit, patients gave us reasons for poor-adherence behaviors and reasons for good-adherence behaviors in their own words, answering open questions. This new information obtained from patients themselves was then classified and re-written. We defined eight potential causes for non-adherence, based on the WHO proposal,10 previous studies,27 and the patient’s answer in our study: 1) high cost of medication; 2) diminished treatment effectiveness with long-term use; 3) poor self-efficacy; 4) relief of symptoms after short-term controller medication use; 5) occurrence/fear of side effects; 6) difficulty obtaining medication; 7) not specifically stated by their doctor or other health care professional that inhaled therapy should be long-term use; and 8) other.
Statistical Analyses
Variables are presented as mean values with standard deviation or frequency and percentage. Potential associations were tested using partial correlation, the χ2 test, Fisher’s exact test, or the Kruskal–Wallis test, as appropriate. Factors that were associated (p < 0.05) with non-adherence in the univariate analysis were included in the multivariate regression analysis with a stepwise procedure to identify risk factors that were independently associated with non-adherence. Results were considered statistically significant when p-values were below 0.05.
Results
Study Recruitment
A total of 296 participants had pneumoconiosis with COPD and were eligible for inclusion. All of them were male. During follow-up, 15 (5.07%) were dead, 56 (18.92%) were lost follow-up, and 12 (4.05%) refused to participate. Finally, 213 participants completed the 2-year follow-up of adherence since the baseline visit (Figure 1).
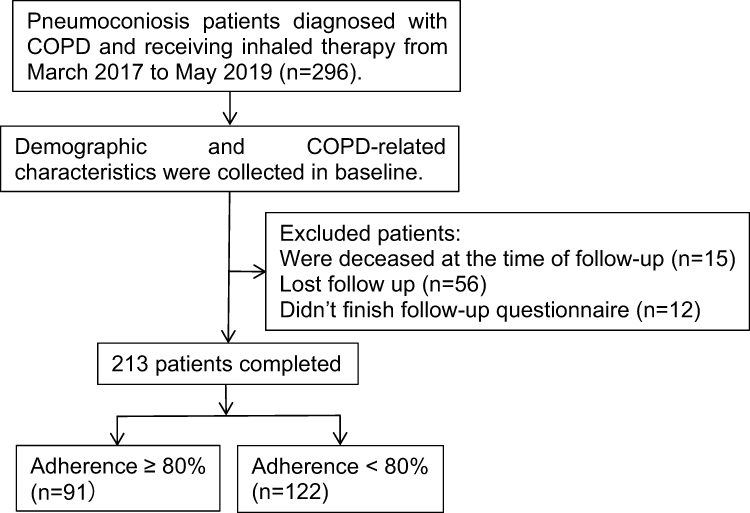 |
Figure 1 Study flow diagram. |
Demographic and clinical characteristics of the 296 participants in baseline are shown in Table 1. Mean age was 58.82 ± 8.64 years, mean BMI was 23.33 ± 11.98 kg/m2. The majority of patients had low educational level, 44.26% were middle school, 49.66% were primary school and below. Tobacco smoking was common in the subjects. Overall, 34.46% were current smokers, 47.97% were former smokers, and only 17.57% were never smokers. In 47.97% of all cases, mono-therapy (LAMA) was prescribed, 29.73% was prescript with triple-therapy (LAMA + LABA + ICS), and 22.3% were prescript with dual-therapy (ICS+LABA). According to CAT (≥10) and mMRC (≥2) tools, uncontrolled poor health status was found in 209 (70.61%) and 201 (67.91%) subjects, respectively. Number ≥2 and ≥1 AE in the past year were seen in 124 (41.89%) and 181 (61.15%) subjects, with GOLD group B (44.59%) being the largest followed by groups D (39.86%), A (13.51%), and C (2.03%).
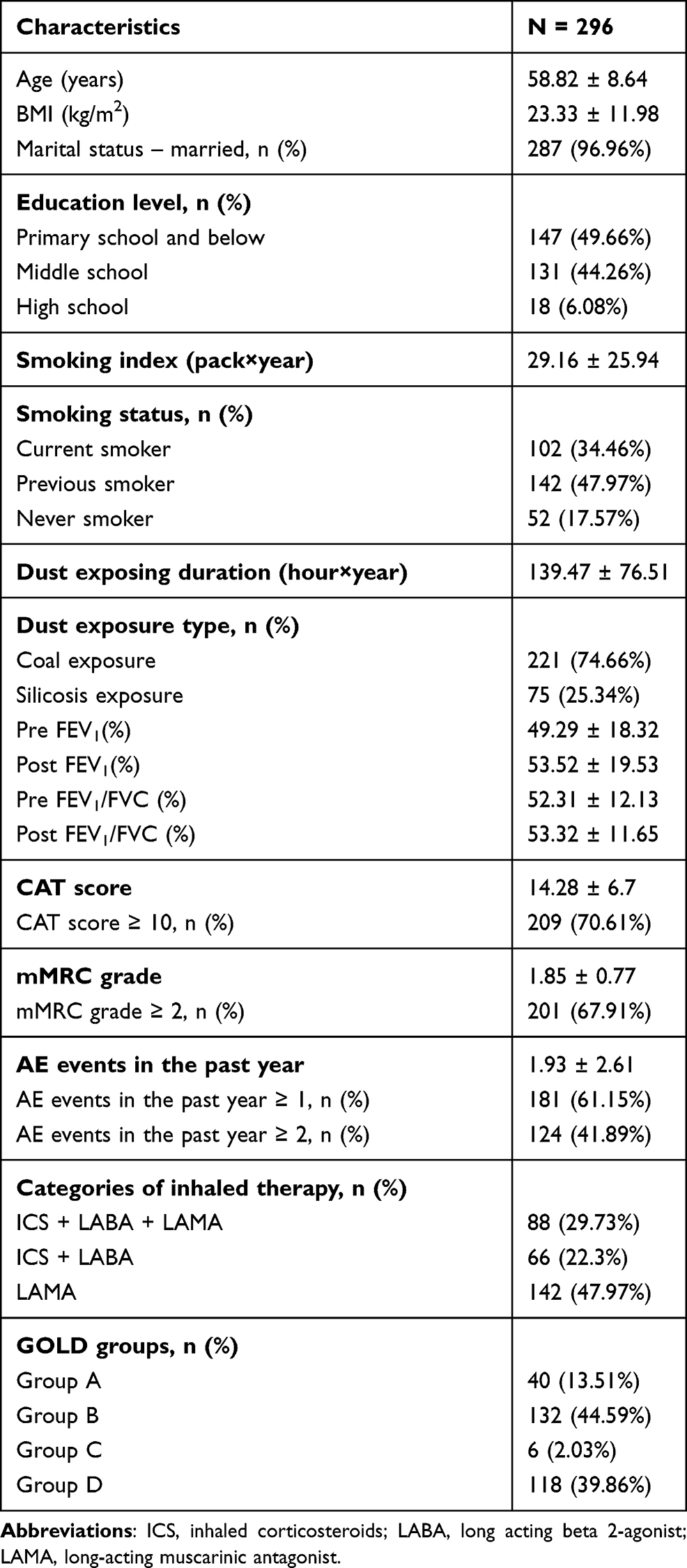 |
Table 1 Demographic, Clinical, and Functional Characteristics of Pneumoconiosis with COPD |
Correlation of Dust Exposure and Smoke Exposure to COPD-Related Characteristics
After adjusting for age, we found dust exposure duration was positively correlated with number of AE in the last year (r = 0.181, p = 0.002) for pneumoconiosis with COPD. CAT score (r = −0.355, p < 0.001), mMRC grade (r = −0.333, p = 0.002), and number of AE in the last year (r = −0.270, p < 0.001) were negatively correlated with pre-FEV1. Meanwhile, there is strong association among CAT score and mMRC grade (r = 0.504, p < 0.001), CAT score and number of AE (r = 0.378, p < 0.001), and mMRC grade and number of AE (r = 0.378, p < 0.001). There is no association between smoking index to any of these COPD-related characteristics (p > 0.05) (Table 2).
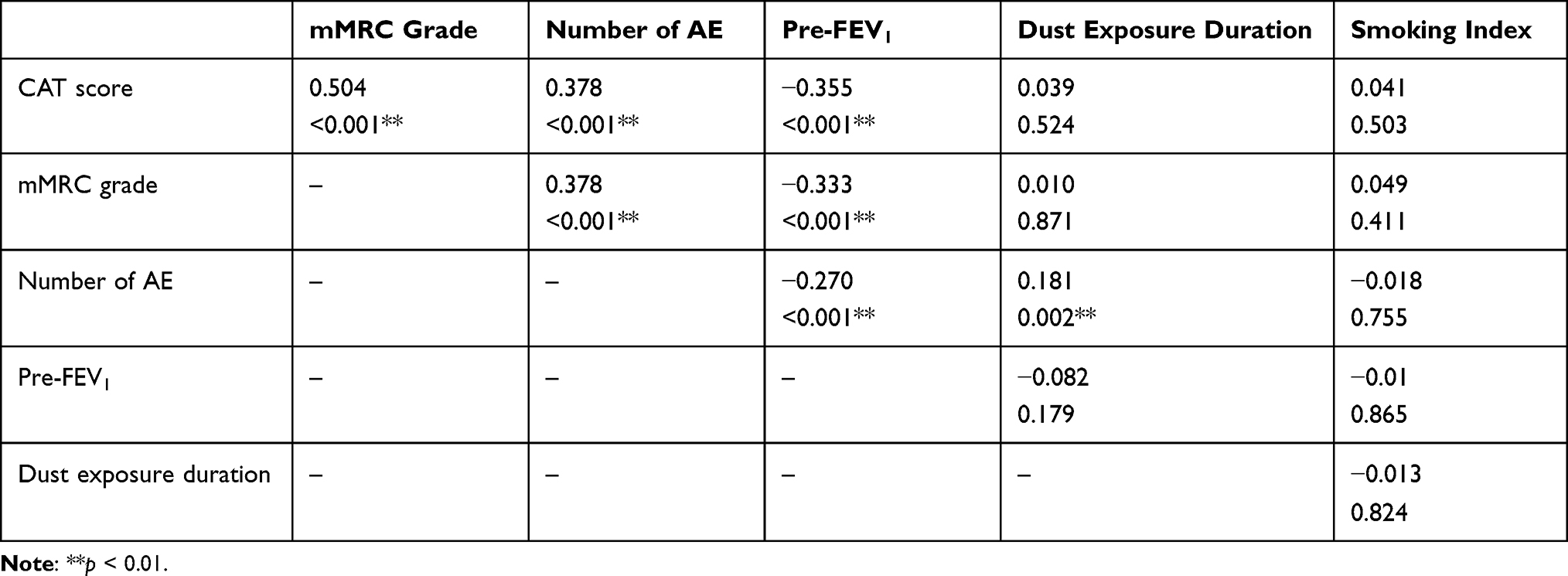 |
Table 2 Correlations Between Symptoms (CAT and mMRC Grade), Lung Function, Exacerbation Frequency in the Last Year, and Dust Exposure Duration in Baseline (n = 296) |
Adherence to COPD Treatment
Among the participants, 122 (57.28%) were non-adherent to the inhaled therapy in 2-year follow-up. Characteristics of adherent and non-adherent are presented in Table 3. There was no significant difference observed in age, smoking index, dust exposing duration, dust exposure type, education level, marital status, categories of inhaled therapy, and smoking status between adherence classes. Compared to adherent, non-adherent had higher FEV1 value, lower mMRC grade, lower CAT scores, and less severe disease (GOLD group). They also experienced less number of AE in the past year in baseline (p < 0.001). A higher proportion of non-adherent had a BMI ≥ 25 kg/m2 (p < 0.05).
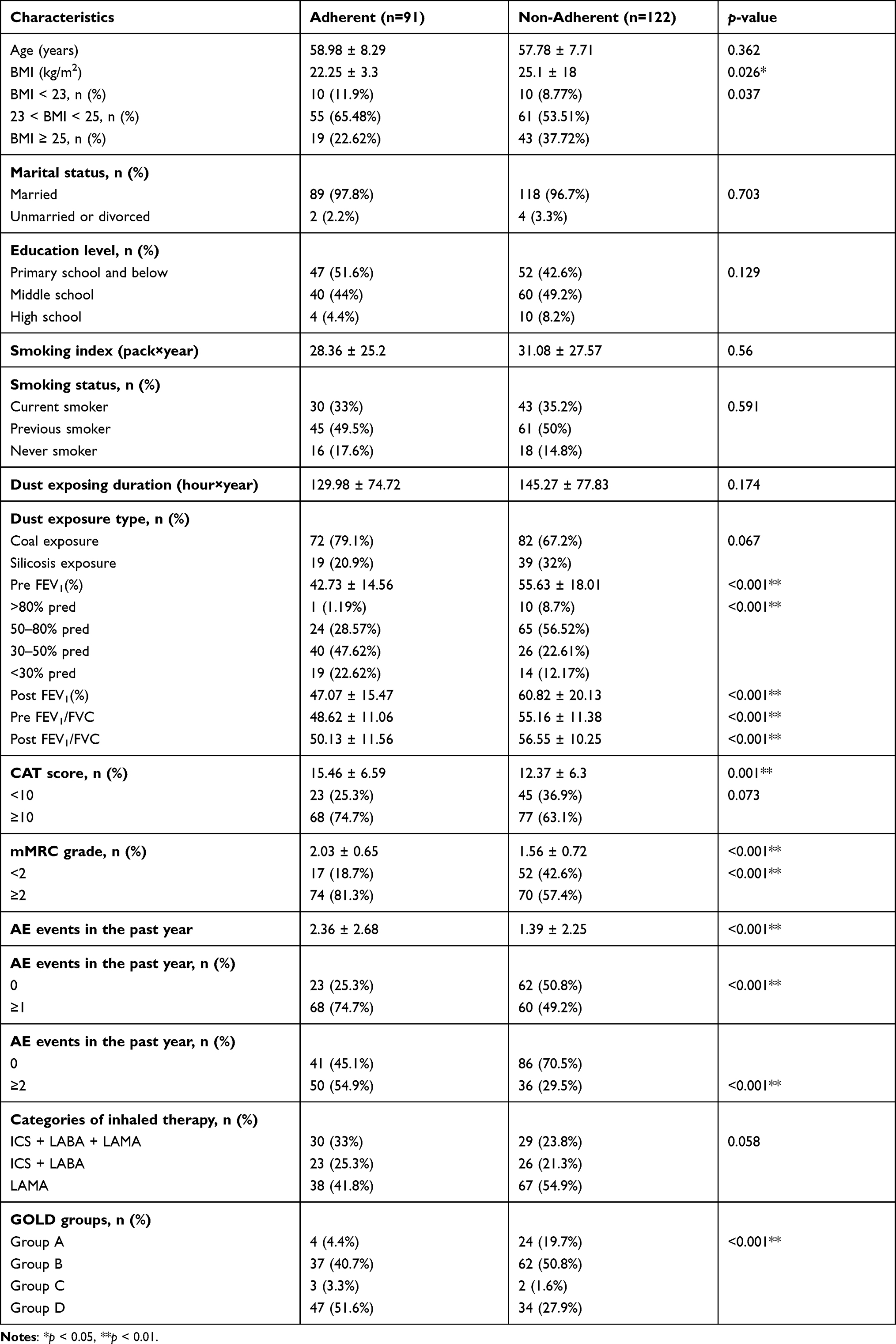 |
Table 3 Socio-Demographic and Clinical Characteristics of Adherent and Non-Adherent |
Reasons for Non-Adherence
A number of factors were identified as the reason for non-adherence of the patients towards their inhaled therapy. “Relief of symptoms after short-term controller medication use” was the major reason for patient non-adherence, 53.28%, followed by “High cost of medication”, 9.84%, and “Diminished treatment effectiveness with long-term use”, 9.02%, and “Not specifically stated by their doctor or other health care professional that inhaled therapy should be long-term use” accounts for 9.02%. 1.64% discontinued their inhaled therapy because of the occurrence of side effect, difficulty obtaining medication and poor self-efficacy, 13.93% gave no reasons for non-adherence. We found that different levels of adherence and poor-adherence behaviors were mainly intentional.
Predictors of Non-Adherence
In the multivariable model, low mMRC scores (OR = 0.406, CI = 0.214–0.771) and high pre-FEV1 value (OR = 1.04, CI = 1.018–1.064) were risk factors found for non-adherent of inhaled therapy (Table 4). The patients’ age, smoking index, dust exposing duration, dust exposure type, education level, marital status, categories of inhaled therapy, and smoking status did not influence adherence.
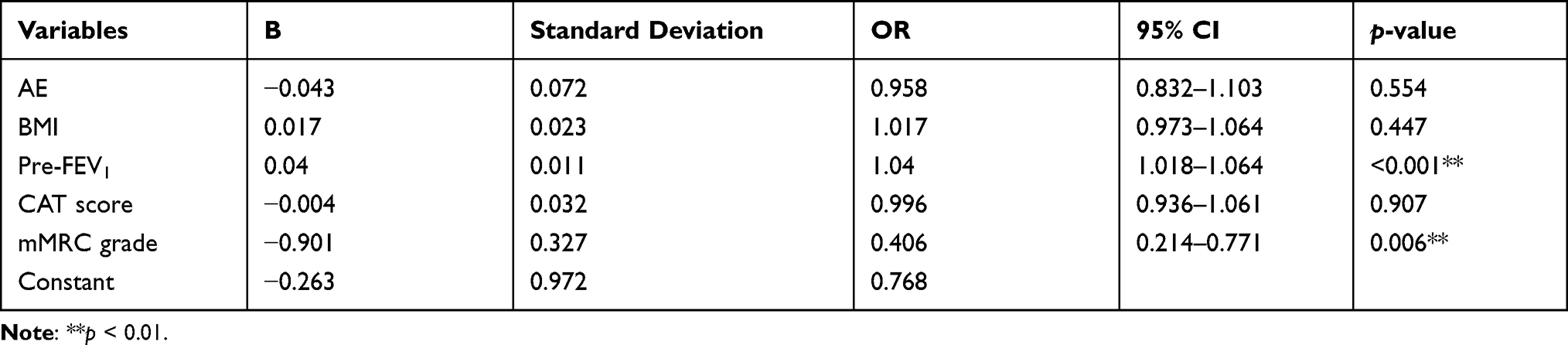 |
Table 4 Multivariable Regression Analysis for Non-Adherent of Inhaled Therapy in Pneumoconiosis with COPD |
Discussion
To the best of our knowledge, this is the first study to describe the current status of adherence to inhaled therapy in pneumoconiosis complicated with COPD. These findings help to define potential targets for intervention.
In our retrospective analysis, cumulative dust exposure duration but not smoking index was positively correlated with number of AE in the last year. Although it was statistically significant, the correlation between dust exposure and number of AE in the last year was weak. This may be explained by the definition of dust exposure duration in our study, since we use both hour and year to quantify this indicator. Objective indicators such as cumulative dust exposure dose are believed as more appropriate measurements if available. Exacerbations of COPD indicate progression of the disease and are associated with reduced health status,28 our findings link the impact of dust exposure in clinical outcomes in occupational COPD. We also found there were close correlations between pre-FEV1 and scores for CAT, mMRC, and number of AE. The association between lung function parameters and health status measures is known from results of previous cross-sectional studies.29
In the follow-up, patient-reported non-adherence to prescript inhaler therapy was as high as 57.28% in pneumoconiosis with COPD. Medication adherence among patients with COPD is always a matter of concern worldwide.30 In the real world, adherence for maintenance medications of COPD is bad. By using a large administrative claims database, Dhamane et al observed that 79.2% of patients were non-adherent to maintenance COPD medications.31 A large prospective cohort study conducted in China also showed COPD patients had adherence rates of 74.65%, 49.63%, and 33.61% at 4-, 12-, and 24-week telephone follow-ups.32 Another retrospective cohort study reported that approximately two-thirds of patients with COPD failed to continue treatment after 12 months.33 Our study was based on a 2-year follow-up on a relative severe stage of COPD and reports patients with pneumoconiosis and COPD had a significantly high discontinuation rate overall.
The factors that contribute to sub-optimal adherence in COPD can grouped into 3 major categories.27 They are medication (complex regimen, multiple inhalers, inhaler technique, efficacy to onset, side effect, cost), unintentional (age-related factors, forgetfulness, misunderstood directions, comorbidities, health literacy), and intentional (perception of treatment, denial about disease, inappropriate expectations, dissatisfaction with health care providers, cultural issues). In this study, “Relief of symptoms after short-term controller medication use” and “Diminished treatment effectiveness with long-term use” are the main intentional reason patients give for non-adherence. This finding is consistent with other studies.16,32 To address these patient related factors, there is need for more regular follow-up visits, comprehensive self-management programs involving patient education activities,34 and counseling sessions. “High cost of medication” accounts for the main medication reason for non-adherence. Inequity in health service utilization is a major health policy challenge in China,35 however, rare insurance covers the maintenance medications of COPD. And in reality, the social and economic factors may be interacting and affecting patient related factors, so economic reason needs more attention and effort.10 Surprisingly, we found some patients indicate that they were not specifically stated by their doctor or other health care professional that inhaled therapy should be long-term use since baseline. This points to us that ineffective doctor–patient communication is a potential hazard for these patients.36 Improved patient–provider communication may help solve this problem and promote inhaled therapy adherence.37
Factors associated with non-adherence in patients with COPD have also been largely explored in several previous studies. Socioeconomic factors, including unemployment, low income status, immigration status, and living alone, social/familial support, health literacy, specific comorbidities,17 inhaled therapy type,18 and smoking status16 have been shown to influence adherence in COPD. However, level of education, marital status, dust exposure type, categories of inhaled therapy, and smoking status was found not to be associated with adherence in our study. This difference could be attributed to variations in the socio-economic status, cultural backgrounds, and health care services across the study settings. Importantly we found risk factors associated with non-adherence in pneumoconiosis with COPD were fewer dyspnea burden and more mild airflow limitation. This is in accordance with previous studies, where adherence was better in patients with more severe COPD.16,21,38,39 Owing to the fact that inhaled medications in some COPD patients have symptomatic effect, relief of clinical symptoms can be misinterpreted and can lead to treatment interruption and cessation.40 More severe patients are more adherent probably because they are more symptomatic or experience more relief of symptoms, while patients with milder disease may not see the need to regularly take their prescribed medication as they may believe that their symptoms are not serious or their condition is controlled.41 As observed in our study, more than half (53.28%) of the non-adherent did not use drug because of symptom relief after short-term use. COPD patients suffered from occupational exposure developed more severe dyspnea than those exposed to tobacco alone.6 However, non-adherence to therapy can be surprising high in our study, that in very symptomatic patients (mMRC grade ≥ 2) and less symptomatic patients (mMRC grade < 2), the future non-adherence rate was as high as 48.61% (70/144) and 75.36% (52/69), respectively. Disease heterogeneity for pneumoconiosis with COPD and subjective cognition on COPD may play a role in individual adherence behavior.15,42
This study was based in a “real life” setting and adherence is measured by self-report. Self-reports may have introduced some recall, social desirability, and/or interviewer bias, leading to an over-estimate of the patient’s actual medication adherence. However, the researchers pose such questions in a non-judgmental fashion and that the question be prefaced by a normalizing statement, allowing the patient to feel more comfortable about telling the truth. Self-reported medication adherence measures are ease and cost-effectiveness of implementation in a clinical setting and they may also have the benefit of demonstrating high specificity in capturing people who are truly non-adherent. Referring to non-adherence, the present study shows that a substantial number of patients (42.72%) purposely chose not to take their inhaled medication, which was deliberate non-adherence. Moreover, the methods used in our study measure adherence in long-term periods instead of adherence in recent weeks.
This study had some limitations. First, no control group such as tobacco smokers with COPD was used. However, a recent large sample study in our center showed 33.2% of COPD had poor inhaled drug adherence after 6 months of follow-up.43 Referred to these data, pneumoconiosis with COPD have worse inhaled drug adherence despite similar baseline status. Second, assessment of medication adherence was based on self-reports which could introduce recall bias and inaccuracy in the data collected, when compared to other objective methods. We see the following strengths of our study. First, it was possible for us to reach a relative large population of pneumoconiosis with COPD. Second, our pneumoconiosis patients complicated with COPD were evaluated and treated in an described outpatient structure based on existing guidelines for patients with COPD.
Conclusions
Overall, 57.28% of the pneumoconiosis with COPD were non-adherent to the inhaled therapy in 2-year follow-up. Mild airflow limitation and low dyspnea burden were risk factors for non-adherence in pneumoconiosis with COPD. Interventions to improve adherence to inhaled therapy should include aggressive counseling and health education with a focus on patients with low dyspnea burden and mild airway limitation. A better understanding of the clinical factors influencing patient adherence, and strategies to improve adherence, could lead to beneficial interventions in pneumoconiosis with COPD.
Abbreviations
COPD, chronic obstructive pulmonary disease; AE, acute exacerbation; CAT, COPD Assessment Tool; mMRC, modified Medical Research Council Dyspnea Scale; BMI, body mass index; SMR, standardized mortality ratio; ICD, International Classification of Diseases; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Statement
The study was registered in the Chinese Clinical Trial Registry (Title: The analysis of current status in diagnosis and treatment of COPD. Registration number: ChiCTRPOC-17010431.http://www.chictr.org.cn/). This study was performed following the ethics principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University in Changsha, Hunan (NO. 2016032). All participants provided written informed consent.
Acknowledgments
We acknowledge and thank the patients who participated in this study. The authors would like to thank the staff of Second Xiangya Hospital and Hunan Prevention and Treatment Institute for Occupational Diseases for their cooperation in collecting the study data. We also wish to acknowledge the educational and mentorship contributions of the Methods in Epidemiologic, Clinical, and Operations Research (MECOR) program of the American Thoracic Society, with support from the Song Qingling Foundation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Clinical Specialty Construction Projects ((2012)No. 650), the National Natural Science Foundation of China (NSFC, Grants 81770046), (NSFC, Grants 81970044) and Xiangya Mingyi grant (2013).
Disclosure
The authors report no conflicts of interest.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
2. Eisner MD, Anthonisen N, Coultas D, et al. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;182(5):693–718. doi:10.1164/rccm.200811-1757ST
3. Furlow B. Occupational exposures are important factors in COPD and other lung diseases. Lancet Respir Med. 2019;7(10):840. doi:10.1016/S2213-2600(19)30304-2
4. Peng Y, Li X, Cai S, et al. Prevalence and characteristics of COPD among pneumoconiosis patients at an occupational disease prevention institute: a cross-sectional study. BMC Pulm Med. 2018;18(1):22. doi:10.1186/s12890-018-0581-0
5. Fan Y, Xu W, Wang Y, et al. Association of occupational dust exposure with combined chronic obstructive pulmonary disease and pneumoconiosis: a cross-sectional study in China. BMJ Open. 2020;10(9):e038874. doi:10.1136/bmjopen-2020-038874
6. Duan JX, Cheng W, Zeng YQ, et al. Characteristics of patients with chronic obstructive pulmonary disease exposed to different environmental risk factors: a large cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2020;15:2857–2867. doi:10.2147/COPD.S267114
7. Hnizdo E, Sluis-Cremer GK, Abramowitz JA. Emphysema type in relation to silica dust exposure in South African gold miners[J]. Am Rev Respir Dis. 1991;143(6):1241–1247. doi:10.1164/ajrccm/143.6.1241
8. Ruckley VA, Fernie JM, Chapman JS, et al. Comparison of radiographic appearances with associated pathology and lung dust content in a group of coalworkers[J]. Occup Environ Med. 1984;41(4):459–467. doi:10.1136/oem.41.4.459
9. Tse LA, Yu IT, Leung CC, et al. Mortality from non-malignant respiratory diseases among people with silicosis in Hong Kong: exposure-response analyses for exposure to silica dust. Occup Environ Med. 2007;64(2):87–92. doi:10.1136/oem.2006.028506
10. Worlds Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Geneva: WHO; 2003.
11. López-Campos JL, Quintana Gallego E, Carrasco Hernández L. Status of and strategies for improving adherence to COPD treatment. Int J Chron Obstruct Pulmon Dis. 2019;14:1503–1515. doi:10.2147/COPD.S170848
12. Unni EJ, Gupta S, Sternbach N. Using the medication adherence reasons scale (MAR-Scale) in asthma and chronic obstructive pulmonary disease to determine the extent and identify the reasons for non-adherence. Respir Med. 2021;179:106337. doi:10.1016/j.rmed.2021.106337
13. Nishi SPE, Maslonka M, Zhang W, et al. Pattern and adherence to maintenance medication use in medicare beneficiaries with chronic obstructive pulmonary disease: 2008–2013. Chronic Obstr Pulm Dis. 2018;5(1):16–26.
14. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):163. doi:10.1186/s12890-018-0724-3
15. López-Pintor E, Grau J, González I, et al. Impact of patients’ perception of COPD and treatment on adherence and health-related quality of life in real-world: study in 53 community pharmacies. Respir Med. 2021;176:106280. doi:10.1016/j.rmed.2020.106280
16. Duarte-de-araújo A, Teixeira P, Hespanhol V, et al. COPD: understanding patients’ adherence to inhaled medications. Int J Chron Obstruct Pulmon Dis. 2018;13:2767–2773. doi:10.2147/COPD.S160982
17. Ierodiakonou D, Sifaki-Pistolla D, Kampouraki M, et al.; Greek UNLOCK group. Adherence to inhalers and comorbidities in COPD patients. A cross-sectional primary care study from Greece. BMC Pulm Med. 2020;20(1):253. doi:10.1186/s12890-020-01296-3
18. Yu AP, Guerin A, Ponce de Leon D, et al. Therapy persistence and adherence in patients with chronic obstructive pulmonary disease: multiple versus single long-acting maintenance inhalers. J Med Econ. 2011;14(4):486–496. doi:10.3111/13696998.2011.594123
19. Wisniewski D, Porzezinska M, Gruchala-Niedoszytko M, et al. Factors influencing adherence to treatment in COPD patients and its relationship with disease exacerbations. Pneumonol Alergol Pol. 2014;82(2):96–104. doi:10.5603/PiAP.2014.0015
20. Koehorst-Ter Huurne K, Groothuis-Oudshoorn CG, vanderValk PD, et al. Association between poor therapy adherence to inhaled corticosteroids and tiotropium and morbidity and mortality in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:1683–1690. doi:10.2147/COPD.S161374
21. Vestbo J, Anderson JA, Calverley PM, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
22. Świątoniowska N, Chabowski M, Polański J, Mazur G, Jankowska-Polańska B. Adherence to therapy in chronic obstructive pulmonary disease: a systematic review. Adv Exp Med Biol. 2020;1271:37–47.
23. Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
24. Bestall JC, Paul EA, Garrod R, et al. Usefulness of the Medical Research Council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
25. Laszlo G. Standardisation of lung function testing: helpful guidance from the ATS/ERS Task Force. Thorax. 2006;61(9):744–746. doi:10.1136/thx.2006.061648
26. Hansen RA, Kim MM, Song L, Tu W, Wu J, Murray M. Comparison of methods to assess medication adherence and classify nonadherence. Ann Pharmacother. 2009;43:413–422. doi:10.1345/aph.1L496
27. George M, Bender B. New insights to improve treatment adherence in asthma and COPD. Patient Prefer Adherence. 2019;13:1325–1334. doi:10.2147/PPA.S209532
28. Wedzicha JA, Seemungal TA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370(9589):786–796. doi:10.1016/S0140-6736(07)61382-8
29. Agusti A, Calverley PM, Celli B, et al. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res. 2010;11(1):122. doi:10.1186/1465-9921-11-122
30. Sanduzzi A, Balbo P, Candoli P, et al. COPD: adherence to therapy. Multidiscip Respir Med. 2014;9(1):60. doi:10.1186/2049-6958-9-60
31. Dhamane AD, Schwab P, Hopson S, et al. Association between adherence to medications for COPD and medications for other chronic conditions in COPD patients. Int J Chron Obstruct Pulmon Dis. 2017;12:115–122. doi:10.2147/COPD.S114802
32. Zhang M, Tang T, Wan M, et al. Self-reported reasons for treatment nonadherence in chronic obstructive pulmonary disease (COPD) patients: a 24-week prospective cohort study in China. Ann Palliat Med. 2020;9(5):3495–3505. doi:10.21037/apm-20-1741
33. Mueller S, Wilke T, Bechtel B, et al. Non-persistence and non-adherence to long-acting COPD medication therapy: a retrospective cohort study based on a large German claims dataset. Respir Med. 2017;122:1–11. doi:10.1016/j.rmed.2016.11.008
34. Incorvaia C, Riario-Sforza GG. Effect of patient education on adherence to drug treatment for chronic obstructive pulmonary disease. Ann Thorac Med. 2011;6(4):242–243. doi:10.4103/1817-1737.84783
35. Wang HQ, Jia JL, Jiang ZQ, et al. Analysis of health service utilization and its influencing factors among patients with pneumoconiosis in china. Biomed Environ Sci. 2021;34(1):83–88.
36. Martinez FJ, Thomashow B, Sapir T, et al. Does Evaluation and management of COPD Follow therapeutic strategy recommendations? Chronic Obstr Pulm Dis. 2021;8(2):230–242.
37. Basu S, Garg S, Sharma N, et al. Enhancing Medication adherence through improved patient-provider communication: the 6A’s of intervention. J Assoc Physicians India. 2019;67(7):69–71.
38. Cramer JA, Bradley-Kennedy C, Scalera A. Treatment persistence and compliance with medications for chronic obstructive pulmonary disease. Can Respir J. 2007;14(1):25–29. doi:10.1155/2007/161652
39. Huetsch JC, Uman JE, Udris EM, et al. Predictors of adherence to inhaled medications among veterans with COPD. J Gen Intern Med. 2012;27(11):1506–1512. doi:10.1007/s11606-012-2130-5
40. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax. 2008;63(9):831–838. doi:10.1136/thx.2007.086041
41. Price D, Keininger DL, Viswanad B, et al. Factors associated with appropriate inhaler use in patients with COPD - lessons from the REAL survey. Int J Chron Obstruct Pulmon Dis. 2018;13:695–702. doi:10.2147/COPD.S149404
42. Gruenberger JB, Vietri J, Keininger DL, et al. Greater dyspnea is associated with lower health-related quality of life among European patients with COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:937–944. doi:10.2147/COPD.S123744
43. Zeng Y, Cai S, Chen Y, et al. Current Status of the Treatment of COPD in China: a Multicenter Prospective Observational Study. Int J Chron Obstruct Pulmon Dis. 2020;15:3227–3237. doi:10.2147/COPD.S274024
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.