")
Back to Journals » Patient Preference and Adherence » Volume 16
Adherence to HIV Antiretroviral Therapy Among Pregnant and Breastfeeding Women, Non-Pregnant Women, and Men in Burkina Faso: Nationwide Analysis 2019–2020
Authors Zoungrana-Yameogo WN, Fassinou LC, Ngwasiri C, Samadoulougou S , Traoré IT , Hien H, Bakiono F, Drabo M, Kirakoya-Samadoulougou F
Received 21 December 2021
Accepted for publication 29 March 2022
Published 13 April 2022 Volume 2022:16 Pages 1037—1047
DOI https://doi.org/10.2147/PPA.S354242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Wedminere Noëlie Zoungrana-Yameogo,1 Lucresse Corine Fassinou,2 Calypse Ngwasiri,3 Sekou Samadoulougou,4,5 Isidore Tiandiogo Traoré,1,6 Hervé Hien,1,6 Fidèle Bakiono,7 Maxime Drabo,8,9 Fati Kirakoya-Samadoulougou3
1Service d’information et d’épidémiologie, Centre Hospitalier Universitaire de Tengandogo, Ouagadougou, Burkina Faso; 2Institut Supérieur des Sciences de la Santé, Université Nazi Boni, Bobo-Dioulasso, Burkina Faso; 3Centre de Recherche en Epidémiologie, Biostatistique et Recherche Clinique, Ecole de Santé Publique, Université Libre de Bruxelles, Bruxelles, Belgique; 4Evaluation Platform on Obesity Prevention, Quebec Heart and Lung Institute, Quebec, QC, G1V 4G5, Canada; 5Centre for Research on Planning and Development (CRAD), Université Laval, Quebec, QC, G1V 0A6, Canada; 6Centre Muraz, Institut National de Santé Publique, Bobo-Dioulasso, Burkina Faso; 7Secrétariat Permanent du conseil national de lutte contre le SIDA et les infections sexuellement transmissible, ministère de la santé, Ouagadougou, Burkina Faso; 8Département biomédical et santé publique, Institut de recherche en sciences de la santé, Ouagadougou, Burkina Faso; 9Laboratoire de santé publique de l’Ecole doctorale des sciences de la santé (ED2S), Université Joseph Ki Zerbo Ouagadougou, Ouagadougou, Burkina Faso
Correspondence: Lucresse Corine Fassinou, Institut Supérieur des Sciences de la Santé, Université Nazi Boni, Bobo-Dioulasso, Burkina Faso, Email [email protected]
Background: Since the scale-up of antiretroviral therapy (ART) services in Burkina-Faso, achieving an AIDS-free generation depends on optimal ART adherence. However, no data exists on the population group differences on the level of ART adherence in Burkina-Faso. This study analyzes ART adherence among pregnant-and breastfeeding-women, non-pregnant women, and men in Burkina-Faso.
Methods: From December 2019 to March 2020, a cross-sectional study among adult HIV-infected patients in Burkina-Faso, belonging either to the active file or the Prevention of Mother-To-Child Transmission programs was conducted. An analysis was performed and adherence was measured based on the number of times, patients did not meet the number of doses prescribed and did not take the ART treatment in the month prior to the survey. Logistic-regression models were used to identify factors associated with poor ART adherence and the adjusted odds ratios (aORs) with their 95% confidence intervals (95% CI) were reported.
Results: The prevalence of good adherence was higher in the group of pregnant-and breastfeeding-women (86.6%, n = 112) compared to the other groups (73.1%, n=1017 in non-pregnant women and 72.0%, n = 318 in men). No association was found between ART adherence and the socio-demographic, clinical, and therapeutic characteristics of pregnant-and breastfeeding-women and men groups. However, non-pregnant women with a high level of education (aOR = 1.70; 95% CI: 1.16– 2.49), having ever belonged to a support group (aOR= 1.47; 95% CI: 1.07– 2.04), not having income-generating occupations (aOR= 1.53; 95% CI: 1.11– 2.12), and in advanced clinical stage (aOR= 1.42; 95% CI: 1.06– 1.91) were more susceptible to have poor adherence compared to their pairs.
Conclusion: Findings showed a large difference in ART adherence among pregnant-and breastfeeding-women, non-pregnant women and men and highlight the need for differentiated healthcare delivery according to population while specifically considering addressing the interest in early initiation of treatment and the benefit of support groups meeting.
Keywords: adherence, HIV, antiretroviral therapy, PMTCT, Burkina Faso
Introduction
Since the launching of the United Nations (UNAIDS) “90-90-90” global targets in 2014 to end the AIDS epidemic by 2030, the antiretroviral therapy (ART) program in Burkina-Faso has rapidly expanded, with 65% (61,000) of all people living with HIV (PLWH) receiving ART throughout the country in 2017.1,2 However, recent data suggests that the third target of 90% of all people receiving ART to achieve viral suppression is unlikely to be met,3 as only 72% of the adults living with HIV in East and Southern Africa, and 62% of those living in West and Central Africa were virally suppressed by 2020.4
These low rates of viral suppression indicate that a significant proportion of PLWH taking ART have sub-optimal levels of adherence. Optimal adherence is essential for the effectiveness of HIV management programs, and consistently high levels (≥95%) are required to prevent drug resistance and disease progression, and to achieve viral suppression.5,6 Optimal adherence refers to taking medication as prescribed by a healthcare provider, and attending clinic appointments and pharmacy refills as scheduled.7
Prior research on adherence to ART in Burkina-Faso shows sub-optimal levels for guaranteeing the effectiveness of HIV treatment. Between 2008 and 2012, adherence to ART in Bobo-Dioulasso was 63.7%8 in all PLWH, and the global proportion of non-adherence in Ouagadougou was 38.2% in 2014.9 While the gains of treatment are recognized, poor adherence builds a gap between the prospective and accomplished public-health rewards of ART.10
Data from several Sub-Saharan African (SSA) sites suggest that failure to adhere to ART in PLWH is related to structural barriers to care, community and healthcare stigma, medication side effects, depression, health-system-related barriers, supply-chain interruptions, insufficient human health resources, gender norms, and food insecurity.11–13 Furthermore, adherence to ART and its determinants differ across regions and population groups, necessitating context-specific non-adherence profiles.14,15 Most studies show that adherence to ART is higher in children compared to other groups, with near-perfect rates of 95% seen in about 80% of the HIV-infected children.16,17 All women (including pregnant women) are at a higher risk of non-adherence than men,18 and studies on pregnant women show discrepancies depending on location (rural or urban) and healthcare setting (public or private).19–21 Adherence was lower in rural or low-income settings and higher in studies with satisfactory counseling and monitoring.
A review of adherence among pregnant women receiving ART in SSA showed that the fear of HIV status disclosure to partners and family members, stigma, and discrimination were major barriers to ART adherence.22
As the “90-90-90” target is reviewed in terms of adherence to ART, understanding the patterns of adherence according to population groups in Burkina-Faso informs interventions to maximize health and reproductive choices for women, infants, and families. However, to date, no study has assessed population-group differences in ART adherence in Burkina-Faso. Therefore, we conducted a nationwide analysis of adherence to ART among HIV-infected pregnant-and breastfeeding-women, non-pregnant women, and men in Burkina-Faso in 2020 to better understand the adherence patterns.
Methods
Study Design and Setting
We performed a cross-sectional analysis on data obtained from the national survey database on factors determining adherence to ART in Burkina-Faso. This survey was approved by the institutional review board of the ethics committee of the biomedical centre “Centre MURAZ” from the ministry of health and was conducted from December 2019 to March 2020.
The survey covered all public and private facilities that cared for PLWH in Burkina-Faso (the active file and the prevention of mother-to-child transmission of HIV (PMTCT) programs). Data were separately collected for participants from the active files outside PMTCT, pregnant- and breastfeeding-women with positive serology, patient caregivers, health authorities, prescribers, facilitators, radiotherapists and the religious.
Participants
This study included Persons Living with HIV from both the active file and PMTCT and who were under treatment at the start of the study. For the active file, 02 categories of persons were concerned such as: Non-pregnant women and men followed in the program, under treatment and who were at least aged 18 years at the start of the study. These participants were selected using a systematic random-draw procedure from the active file’s PLWH list. Concerning the PMTCT program, all pregnant-and breastfeeding-women under treatment benefitting from the program and aged 18 years at the start of the study were included. All participants that stayed outside the country in the 3 months preceding the start of the study were excluded from the study. Overall, 1447 participants were included for analyses (Figure 1). Participants were aware of the study’s aims and provided a written consent before participating. All study procedures were performed in accordance with the Declaration of Helsinki and were approved by the institutional review board of the ethics committee of the biomedical centre “Centre MURAZ” from the ministry of health (Deliberation N° 2019–72/MS/SG/INSP/DG/CEI of November, 20, 2019).
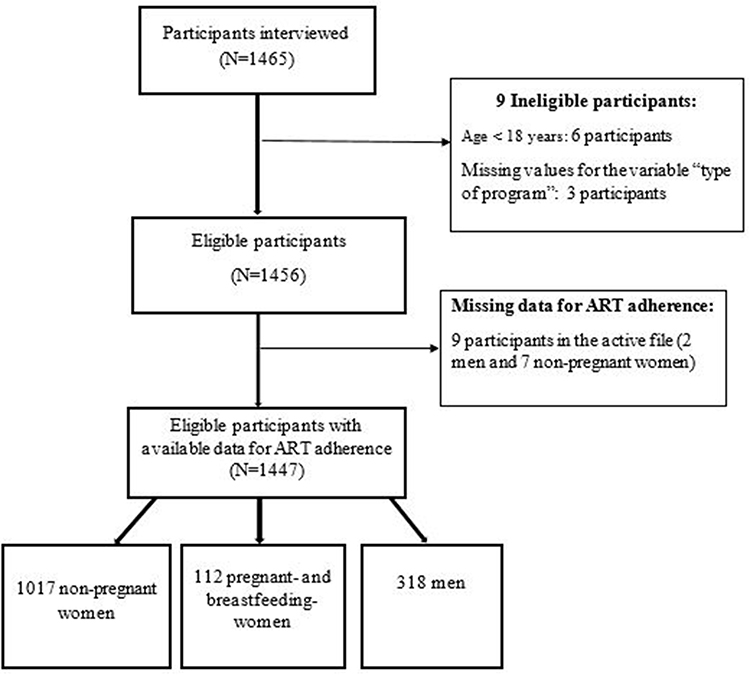 |
Figure 1 Flow chart of participants included in the study. |
Measures
The dependent variable was adherence to ART treatment, which was determined on the basis of the number of times that the patient had not respected clinic appointments in the month preceding the survey and the number of times the patient did not take ARV treatment in the past month. Adherence indicator has been measured according to the following two variables: 1) the number of times the patient did not meet the number of doses in the last month prior to the survey and 2) the number of times the patient did not take antiretroviral treatment in the past month. Were classified as having good adherence, all participants who had taken all the medications while respecting the prescribed number of doses. Those who had at least once missed the treatment or who had not followed the prescribed number of doses were classified as having poor adherence. The independent variables were categorized as described in the Table 1 below.
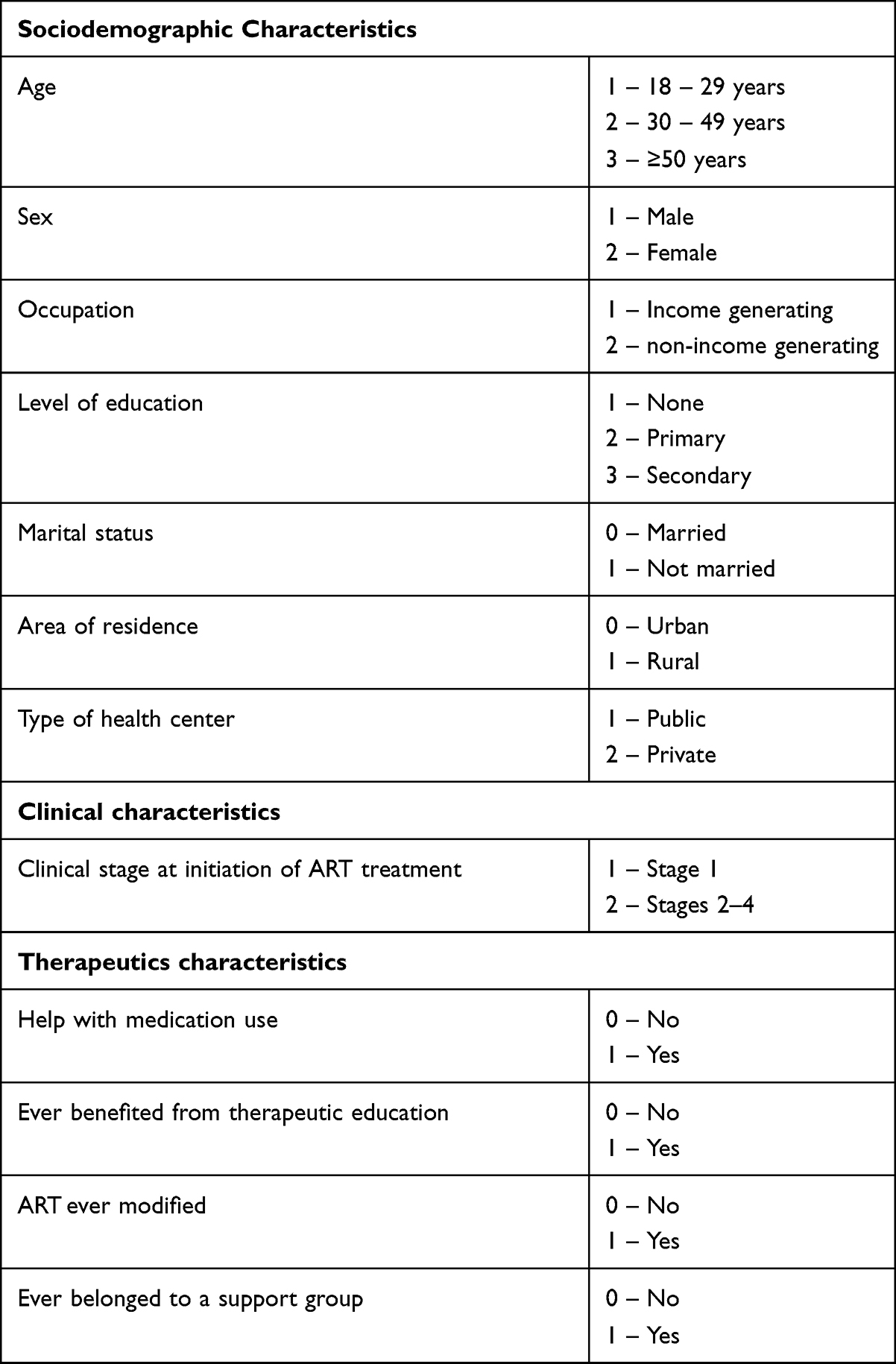 |
Table 1 Operational Definition of Sociodemographic, Clinical, and Therapeutic Characteristics of Study Participants Retained for Analysis |
Statistical Analysis
Statistical analysis was performed on participants with available data for ART adherence, and all other variables of interest. The distribution of participant characteristics was summarized by descriptive statistics in the whole sample, and the results are presented as proportions.
Bivariate analysis was conducted using a chi-squared test to assess the association between ART adherence (dependent variable) and the independent variables (age, sex, occupation, level of education, marital status, residence, type of health center, clinical Stage at initiation, help with medication use, ever benefiting from therapeutic education, ART ever modified, belonging to a support group, and type of program). A P-value < 0.05 was considered as statistically significant.
To identify factors associated with poor adherence according to the various population groups, multivariable logistic regressions were performed, and the adjusted odds ratios (aORs) with their 95% confidence intervals (95% CI) were reported.
Data analysis was performed with STATA version 16.1, and reporting was conducted according to the Strengthening Research for Observational Studies (STROBE) guidelines.
Results
In total, 1465 participants were interviewed, among whom 1456 were eligible. Nine of these eligible participants were excluded due to missing data. Therefore, 1447 participants were included in the final analyses (Figure 1).
Sample Characteristics
Characteristics of adults with available data for ART adherence and all covariates are summarized below (Table 2).
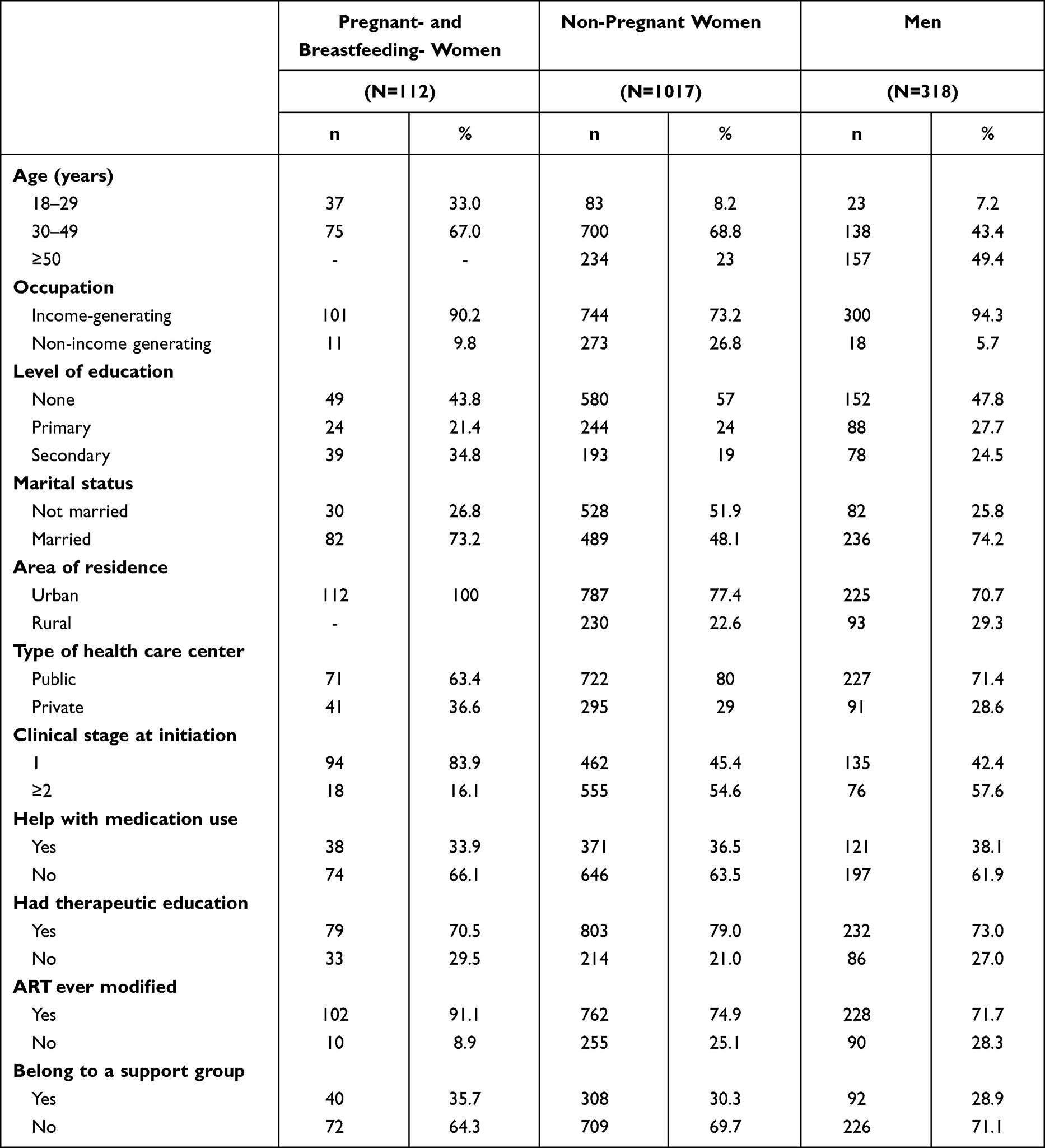 |
Table 2 Socio-Demographic, Clinical and Therapeutic Characteristics of Study Subjects |
Overall, more than half of the study participants were aged between 30 and 39 years (63.1%), lived in urban areas (77.7%), had income-generating occupations (79.1%), used public healthcare centers (70.5%), and had benefited from at least one instance of therapeutic education (77.0%). Furthermore, most patients were at clinical Stage 1 upon ART initiation and needed no help with medication intake. More than half of the participants in the three groups had had their ART modified and had never belonged to a support group (Table 2).
Prevalence of Good Adherence to ART
The overall prevalence of good adherence to ART in the study population was 73.9% (95% CI: 71.5–76.1) with an overall prevalence of 86.6%, 73.1% and 72.0% in the pregnant- and breastfeeding-women, non-pregnant women, and men groups, respectively. Among populations living in urban areas, this prevalence was higher in the group of pregnant- and breastfeeding-women using PMTCT services (86.6%; 95% CI: 78.9–92.3) compared to the other groups: non-pregnant women (71.9%; 95% CI: 68.9–75.0) and men (72.9%; 95% CI: 66.6–78.6). In the rural areas, good adherence was higher amongst non-pregnant women (77.0%; 95% CI: 71.0–82.2) compared to the men group (69.9%; 95% CI: 59.5–79.0).
Table 3 demonstrates the prevalence of adherence to ART according to the socio-demographic, clinical, and therapeutic characteristics of the study participants. In the active file group, among the non-pregnant women, adherence to ART was significantly higher among those with income-generating occupations, no level of education, at clinical Stage 1 of HIV at initiation, and those with no support group. In men, adherence to ART was significantly higher among those treated at public facilities. Pregnant- and breastfeeding-women treated and followed at public health facilities also had a significantly higher prevalence of ART adherence compared to those treated at private health facilities.
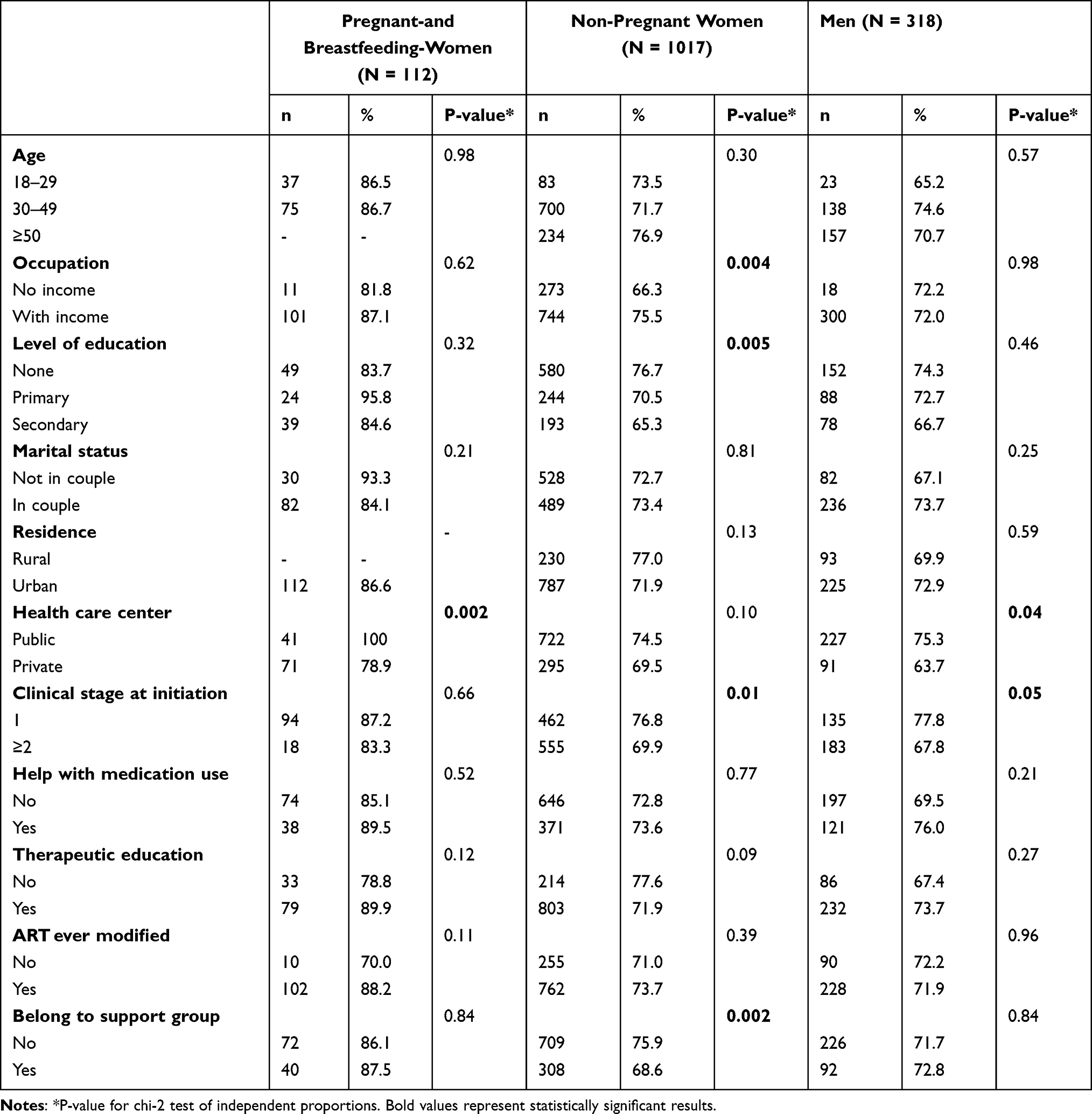 |
Table 3 Prevalence of Good Adherence to ART According to Sociodemographic, Clinical and Therapeutic Characteristics of Pregnant- and Breastfeeding-Women, Non-Pregnant-Women, and Men in Burkina-Faso |
Factors Associated with Poor Adherence to ART
On multivariate logistic regression, no association was found between adherence to ART and the socio-demographic, clinical and therapeutic characteristics of pregnant- and breastfeeding-women and men groups (Table 4). However, for the non-pregnant women, there were strong independent associations between adherence to ART and occupation, level of education, clinical stage at initiation, and having ever belonged to a support group (Table 4). Compared to women with income-generating occupations, those with non-income-generating occupations were more likely to have poor adherence to ART (aOR = 1.53; 1.11–2.12). Furthermore, those who were at clinical Stage 2 or more upon initiation were also more likely to have poor adherence to ART (aOR = 1.42; 1.06–1.91). On the other hand, women with a secondary level of education (aOR = 1.70; 1.16–2.49) and those with a support group treatment (aOR = 1.47; 1.07–2.04) were more likely to have poor adherence to ART, respectively.
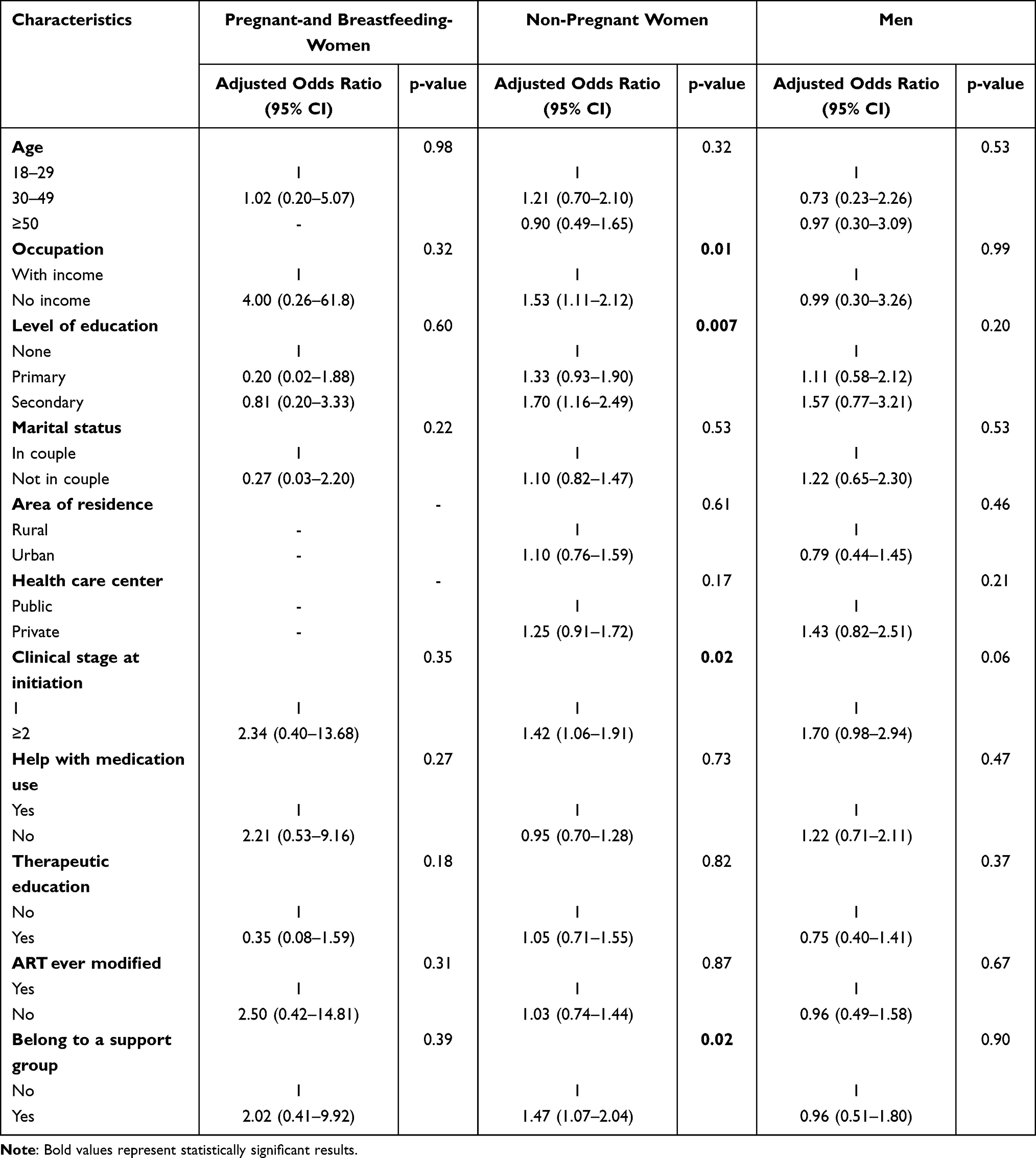 |
Table 4 Association Between Sociodemographic, Clinical, and Therapeutic Characteristics of Study Participants, and Poor Adherence to ART Among Pregnant- and Breastfeeding-Women, Non-Pregnant Women and Men Groups in Burkina-Faso in 2020 |
Discussion
In this nationwide study comparing adherence to ART between different populations in Burkina-Faso, 73.9% of HIV-infected individuals had adequate self-reported ART adherence in 2020, with large differences between pregnant- and breastfeeding-women, non-pregnant women, and men. Among non-pregnant women, non-income-generating occupations, secondary level of education, clinical Stage 2 or more at initiation and having ever belonged to a support group were independently associated with poor adherence levels. In the group of men, the type of healthcare facility independently affected adherence to ART, with higher adherence rates amongst those treated in public facilities. After adjustments, these associations remained strong and consistent in the non-pregnant women group.
A retrospective study realized in Bobo-Dioulasso from 2008 to 2012 showed a prevalence of good adherence of 63.7%.8 Although, our study was at a national level, which could justify the higher observed prevalence, there was an increase over the last decade; however, unfortunately, this increase is still sub-optimal, indicating that maintaining high levels of adherence remains a major issue in the country. Among persons living in urban areas, adherence levels were the highest among pregnant- and breastfeeding-women, and the lowest in the non-pregnant women group. This could be explained by the fact that pregnancy appears to be a period that has a positive influence on the women’s ability to adhere.23 A qualitative study conducted in Malawi revealed that, for some pregnant women, the desire to prevent HIV from infecting their unborn children, to maintain their health, and to be able to work, motivated them to adhere to ART.24 The better adherence in this group could also be due to the follow-up from which they benefited in the PMTCT program, especially with the recently implemented WHO option B+. Another qualitative study conducted in Uganda, revealed that good ART adherence was attributed to the effectiveness of option B+ ART in comparison to the strategies before the option B+ era, which motivated patients to take ART.25
Considering the population living in rural areas, non-pregnant women were more adherent than men were. This may be because HIV-infected women in Burkina-Faso demonstrate better health-seeking behaviors than men do, which may be motivated by their role as principal caregivers in their families and by representations of masculinity that are fully implicated in the cultural construction of men’s reluctance to attend care facilities for PLWH.26
In all the three groups, adherence to ART was higher among patients that used public health facilities. However, this difference was not statistically significant in the group of non-pregnant women unlike the other groups. Our findings are consistent with those of Shet et al, in India who found that adherence and treatment success were significantly higher among patients from public settings compared with patients from private facilities.27 Private health facilities are increasingly labeled as the neglected partner in the provision of HIV services.28
After the multivariate analysis, occupation, level of education, clinical Stage at initiation, and having ever belonged to a support group were significantly associated with poor adherence to ART treatment in non-pregnant women. Those with non-income-generating occupations were more likely to have poor adherence to ART compared to those with income-generating occupations. The lack of income meant that most of these people were unable to buy food or to afford transportations costs to meet their ART clinic appointment dates.29 Our result is consistent with that of several studies.30–32 Concerning the clinical stage at initiation, non-pregnant women who had begun ART treatment at clinical Stage 2 or more, were more likely to have poor adherence compared to those who had started at clinical Stage 1. In fact, the aspirations for an AIDS-free generation depends on optimal ART adherence in individuals initiating ART during an early stage of the infection.33 As such, we assume that individuals that initiate at an early disease stage might be less likely to face the problem of multiple medications from concomitant opportunistic infections, more likely to have better tolerance and lower chances of medication side effects, and hence a higher likelihood of optimal treatment adherence. Our result is consistent with those found in Uganda and South Africa in 2019.33
Although formal education enhances the ability of PLWH to follow instructions related to treatment given by the health providers, which logically leads to better adherence to treatment, our study revealed that non-pregnant women with a secondary level of education, were more likely to have poor adherence to ART compared to those with no level of education. Our surprising results are consistent with those of other studies, which found most literate PLWH to have low adherence to ART.34,35 One explanation about these findings is the fact that patients with higher level of education may be confronted by busy occupations that hindered the intake of antiretroviral drugs.34,35 Another explanation could be the encountered difficulties for most educated patients to be observant in their professional environment. Regarding belonging to a support group, women who have ever belonged to a support group were more likely to have poor adherence compared to their pairs. This result that seems the opposite from our expectations, could be justified by the fact that these activities might be much more relevant to patients experiencing compliance difficulties. Many studies postulate that social support from PLWH peers through PLWH support-group mechanisms plays an important part in ART adherence,36,37 but the duration of involvement and participation in support-group activities could also influence adherence to medication among PLWH belonging to such groups. The effect does not persist when the support is discontinued.37,38 This suggests that communication strategies to demonstrate the positive effect of continued participation in support groups must be established and actors that lead these groups should be aware of the importance of communication and improve their messages on compliance and adherence within these groups.
Lastly, among the pregnant- and breastfeeding-women and men groups, no association was found between adherence to ART and the socio-demographic, clinical, and therapeutic characteristics of study participants. The small sample size in each group meant that there was less statistical power to detect any significant associations, and this could be a possible explanation for this finding.
Strengths and Limitations of the Study
This study is the first one that provides nationwide data on ART adherence among adult PLWH in Burkina-Faso across multiple treatment centers. It is also not only limited to severely immunocompromised PLWH and can thus be generalized to the population adopting the “test and treat approach”.
However, the study had several limitations. First, there was incomplete data ascertainment for some factors, such as place of residence (rural), which can affect adherence in terms of patient attributes and healthcare-related factors. Second, factors associated with adherence were limited only to baseline clinical and therapeutic data. In addition, the cross-sectional and observational design of this study means that the associations do not necessarily demonstrate causality. Lastly, our analysis was limited only to the adult population of PLWH in Burkina-Faso. ART-treated adolescents and children in Burkina-Faso may have different adherence barriers to those identified in this study. As the study relied on self-reported measures, it may be susceptible to various biases such as memory and desirability bias.
Conclusions
Even though adherence to ART is still sub-optimal in Burkina-Faso, pregnant-and breastfeeding-women showed to have the best adherence compared to non-pregnant women and men. Assessing ART adherence and comparing its determinants between three population groups in Burkina-Faso offered the potential to identify at-risk patients and guide targets for developing interventions to enhance adherence, thus addressing the national challenge of providing effective long-term treatment to thousands of PLWH. The study findings emphasized that ART adherence remains suboptimal in Burkina-Faso in 2020 despite the scaling up of ART services. Factors such as psychosocial factors (having never belonged to a support group), low level of education, income-generating occupation, and clinical Stage 1 at initiation positively influenced ART adherence. Consequently, adherence-enhancing interventions need to address patient-reported barriers, prioritizing those with a formal educational level and those who belonged to a support group.
Ethics Approval and Informed Consent
The participants were informed about the study’s aims and details and voluntary joined the survey with the right to withdraw at any time they want. Written informed consent was obtained from each participant and all study procedures were performed in accordance with the Declaration of Helsinki and were approved by the institutional review board of the ethics committee of the biomedical centre “Centre MURAZ” from the ministry of health (Deliberation N° 2019-72/MS/SG/INSP/DG/CEI of November, 20, 2019).
Acknowledgments
We are grateful to the Health Ministry for data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
This research received funding by the World Bank. Also, Wedminere Noëlie Zoungrana-Yameogo and Lucresse Corine Fassinou received a fellowship from the Commission de la Coopération au Développement (CDD) from the Académie de Recherche et d’Enseignement Supérieur (ARES). Sekou Samadoulougou received a postdoctoral fellowship from the Fonds de recherche du Québec Santé (FRQS).
Disclosure
The authors report no conflicts of interest relevant to this manuscript.
References
1. United Nations Joint Programme on HIV/AIDS. 90-90-90 treatment target. UNAIDS; 2020. Available from: https://www.unaids.org/en/90-90-90.
2. United Nations Joint Programme on HIV/AIDS. Focus on: burkina Faso. UNAIDS; 2021. Available from: https://www.unaids.org/en/20190402_country_focus_BurkinaFaso.
3. United Nations Joint Programme on HIV/AIDS. Ending AIDS: progress towards the 90-90-90 targets. UNAIDS; 2017. Available from: http://www.unaids.org/en/resources/documents/2017/20170720_Global_AIDS_update_2017.
4. United Nations Joint Programme on HIV/AIDS. UNAIDS data 2021. UNAIDS; 2022. Available from: https://www.unaids.org/sites/default/files/media_asset/JC3032_AIDS_Data_book_2021_En.pdf.
5. Martin M, Del Cacho E, Codina C, et al. Relationship between adherence level, type of the antiretroviral regimen, and plasma HIV type 1 RNA viral load: a prospective cohort study. AIDS Res Hum Retrovir. 2008;24(10):1263–1268. doi:10.1089/aid.2008.0141
6. Bangsberg DR, Kroetz DL, Deeks SG. Adherence-resistance relationships to combination HIV antiretroviral therapy. Curr HIV/AIDS Rep. 2007;4(2):65–72. doi:10.1007/s11904-007-0010-0
7. Vreeman RC, Nyandiko WM, Liu H, et al. Measuring adherence to antiretroviral therapy in children and adolescents in western Kenya. J Int AIDS Soc. 2014;17(1):19227. doi:10.7448/IAS.17.1.19227
8. Ouedraogo SM, Zoungrana J, Sondo A, et al. Caractéristiques sociodémographiques, cliniques, biologiques, thérapeutiques et déterminants de la réponse immuno virologique chez les adultes infectés par le VIH, sous traitement antirétroviral à l’hôpital De jour de Bobo-Dioulasso (Burkina Faso). Rev Afr Méd Interne. 2014;1(2):24–29.
9. Guira O, Kaboré DSR, Dao G, et al. The modalities of nonadherence to highly active antiretroviral therapy and the associated factors related to patients’ sociodemographic characteristics and their caregiving perceptions in Ouagadougou (Burkina Faso). J Int Assoc Provid AIDS Care. 2016;15(3):256–260. doi:10.1177/2325957415616492
10. Amico KR, Orrell C. Antiretroviral therapy adherence support: recommendations and future directions. J Int Assoc Provid. 2013;12:128–137. doi:10.1177/1545109712459041
11. Langebeek N, Gisolf EH, Reiss P, et al. Predictors and correlates of adherence to combination antiretroviral therapy (ART) for chronic HIV infection: a meta-analysis. BMC Med. 2014;12:142. doi:10.1186/PREACCEPT-1453408941291432
12. Soomro N, Fitzgerald G, Seeley J, Schatz E, Nachega JB, Negin J. Comparison of antiretroviral therapy adherence among HIV-infected older adults with younger adults in Africa: systematic review and meta-analysis. AIDS Behav. 2019;23(2):445–458. doi:10.1007/s10461-018-2196-0
13. Weiser SD, Palar K, Frongillo EA, Tsai AC, Kumbakumba E. Longitudinal assessment of associations between food insecurity, antiretroviral adherence and HIV treatment outcomes in rural Uhganda. AIDS. 2014;28(1):115–120. doi:10.1097/01.aids.0000433238.93986.35
14. Ware NC, Idoko J, Kaaya S, et al. Explaining adherence success in sub-Saharan Africa: an ethnographic study. PLoS Med. 2009;6:e11. doi:10.1371/journal.pmed.1000011
15. Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;296:679–690. doi:10.1001/jama.296.6.679
16. Azmeraw D, Wasie B. Factors associated with adherence to highly active antiretroviral therapy among children in two referral hospitals, northwest Ethiopia. Ethiop Med J. 2012;50(2):115–124.
17. Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14:365. doi:10.1186/1471-2458-14-365
18. Ortego C, Huedo-Medina TB, Santos P, et al. Sex differences in adherence to highly active antiretroviral therapy: a meta-analysis. AIDS Care. 2012;24(12):1519–1534. doi:10.1080/09540121.2012.672722
19. Kirsten I, Sewangi J, Kunz A, et al. Adherence to combination prophylaxis for prevention of mother-to-child-transmission of HIV in Tanzania. PLoS One. 2011;6:e21020. doi:10.1371/journal.pone.0021020
20. Mukosha M, Chiyesu G, Vwalika B. Adherence to antiretroviral therapy among HIV infected pregnant women in public health sectors: a pilot of Chilenje level one Hospital Lusaka, Zambia. Pan Afr Med J. 2020;35:49. doi:10.11604/pamj.2020.35.49.20078
21. Matthews LT, Orrell C, Bwana MB, et al. Adherence to HIV antiretroviral therapy among pregnant and postpartum women during the Option B+ era: 12‐month cohort study in urban South Africa and rural Uganda. J Int AIDS Soc. 2020;23(8):e25586. doi:10.1002/jia2.25586
22. Omonaiye O, Kusljic S, Nicholson P, Manias E. Medication adherence in pregnant women with human immunodeficiency virus receiving antiretroviral therapy in sub-Saharan Africa: a systematic review. BMC Public Health. 2018;18:805. doi:10.1186/s12889-018-5651-y
23. Vitalis D, Hill Z. Antiretroviral adherence perspectives of pregnant and postpartum women in Guyana: barriers and facilitators. J Int Assoc Provid AIDS Care. 2017;16(2):180–188. doi:10.1177/2325957416680297
24. Elwell K. Facilitators and barriers to treatment adherence within PMTCT programs in Malawi. AIDS Care. 2016;28(8):971–975. doi:10.1080/09540121.2016.1153586
25. Mukose AD, Bastiaens H, Makumbi F, et al. What influences uptake and early adherence to Option B+ (lifelong antiretroviral therapy among HIV positive pregnant and breastfeeding women) in Central Uganda? A mixed methods study. PLoS One. 2021;16(5):e0251181. doi:10.1371/journal.pone.0251181
26. Bila B, Egrot M. Gender asymmetry in healthcare-facility attendance of people living with HIV/AIDS in Burkina Faso. Soc Sci Med. 2009;69(6):854–861. doi:10.1016/j.socscimed.2009.05.035
27. Shet A, DeCosta A, Heylen E, Shastri S, Chandy S, Ekstrand M. High rates of adherence and treatment success in a public and public-private HIV clinic in India: potential benefits of standardized national care delivery systems. BMC Health Serv Res. 2011;11(1):277. doi:10.1186/1472-6963-11-277
28. Chirambo L, Valeta M, Kamanga TMB, Nyondo-Mipando AL. Factors influencing adherence to antiretroviral treatment among adults accessing care from private health facilities in Malawi. BMC Public Health. 2019;13:1382. doi:10.1186/s12889-019-7768-z
29. Moomba K, Wyk BV. Social and economic barriers to adherence among patients at Livingstone General Hospital in Zambia. Afr J Prim Health Care Fam Med. 2019;11(1):6. doi:10.4102/phcfm.v11i1.1740
30. Suryana K, Suharsono H, Antara IGPJ. Factors associated with adherence to anti-retroviral therapy among people living with HIV/AIDS at Wangaya hospital In Denpasar, Bali, Indonesia: a Cross-Sectional Study. HIV/AIDS. 2019;11:307–312. doi:10.2147/HIV.S219695
31. Prah J, Hayfron-Benjamin A, Abdulao M, Lasim O, Nartey Y, Obiri-Yeboah D. Factors affecting adherence to antiretroviral therapy among HIV/AIDS patients in Cape Coast Metropolis, Ghana. J HIV AIDS. 2018;4:1–7. doi:10.16966/2380-5536.149
32. Suleiman IA, Momo A. Adherence to antiretroviral therapy and its determinants among persons living with HIV/AIDS in Bayelsa state, Nigeria. Pharm Pract. 2016;14(1):631. doi:10.18549/PharmPract.2016.01.631
33. Haberer JE, Bwana BM, Orrel C, et al. ART adherence and viral suppression are high among most non‐pregnant individuals with early‐stage, asymptomatic HIV infection: an observational study from Uganda and South Africa. J Int AIDS Soc. 2019;22:e25232. doi:10.1002/jia2.25232
34. Hansana V, Sanchaisuriya P, Durham J, et al. Adherence to Antiretroviral Therapy (ART) among People Living With HIV (PLHIV): a cross-sectional survey to measure in Lao PDR. BMC Public Health. 2013;13:617. doi:10.1186/1471-2458-13-617
35. Chesney MA. Factors Affecting Adherence to Antiretroviral Therapy. Clin Infect Dis. 2000;30(suppl 2):S171–6. doi:10.1086/313849
36. Tumwikirize S, Torpey K, Adedokun O, Badru T. The value of support group participation in influencing adherence to antiretroviral treatment among people living with Human Immunodeficiency Virus (HIV). World J AIDS. 2015;5:189–198. doi:10.4236/wja.2015.53022
37. Chime OH, Arinze-Onyia SU, Obionu CN. Do peer support groups have an effect on medication adherence? A study among people living with HIV/AIDS in Enugu State, Nigeria. Proc Singap Healthc. 2018;27(4):256–264. doi:10.1177/2010105818760923
38. Simoni JM, Huh D, Frick PA, et al. Peer support and pager messaging to promote antiretroviral modifying therapy in Seattle: a randomized controlled trial. J Acquir Immune Defic Syndr. 2009;52(4):465–473. doi:10.1097/qai.0b013e3181b9300c
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.