")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
ADHD and lifestyle habits in Czech adults, a national sample
Authors Weissenberger S , Ptacek R , Vnukova M , Raboch J , Klicperova-Baker M, Domkarova L, Goetz M
Received 11 August 2017
Accepted for publication 13 October 2017
Published 15 January 2018 Volume 2018:14 Pages 293—299
DOI https://doi.org/10.2147/NDT.S148921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Simon Weissenberger,1,2 Radek Ptacek,1,2 Martina Vnukova,1,2 Jiri Raboch,1 Martina Klicperova-Baker,3 Lucie Domkarova,1 Michal Goetz4
1Department of Psychiatry, First Faculty of Medicine, Charles University in Prague and General University Hospital in Prague, Prague, 2Department of Psychology, University of New York in Prague, Prague, 3Institute of Psychology, Czech Academy of Sciences, Prague, 4Department of Paediatric Psychiatry, Second Faculty of Medicine, Charles University in Prague and Motol University Hospital, Prague, Czech Republic
Background: Adult attention-deficit/hyperactivity disorder (ADHD) has been added as a diagnosis to the Diagnostic and Statistical Manual of Mental Disorders version 5 (DSM5) in 2013, thus making ADHD, which has been classically known as a childhood disorder, a lifelong disorder. Those suffering from the condition show very specific behavioral traits, which manifest as lifestyle habits; they also show comorbidities that can be the symptoms and/or consequences of certain lifestyles.
Materials and methods: The targeted population was adults aged 18–65 years. The total sample was 1,012 (507 males and 505 females). The Adult ADHD Self-Report Scale (ASRS V. 1.1) was administered to evaluate the current symptoms of ADHD and a questionnaire regarding lifestyles that are pertinent to ADHD, exercise, drug use, and diet.
Results: An ASRS score of 4–6 points was found in 11.4% of the male population and 9.7% of the female population (5–6 points indicate very high-intensity symptoms). A score of 6, the highest intensity of symptomatology, was found in 1.18% of males and 0.99% of females. Gender differences in scores were not statistically significant. In terms of self-reported lifestyles, we calculated an ordered logistic regression and the odds ratios of those with ASRS scores >4. Those with higher ASRS scores had higher rates of self-reported unhealthy lifestyles and poor diets with high consumption of sweets. We also ascertained a paradoxical finding that is not in line with the current literature on the disorder – lower rates of cigarette smoking among people with higher ADHD symptomatology.
Conclusion: Several specific lifestyles were found to be associated with higher ADHD symptoms such as poor diet and cannabis use. Other factors classically associated with the disorder such as cocaine addiction and nicotinism were either insignificant or surprisingly less prominent among the Czech sample. However, ADHD-prone respondents reported to be more physically active, which fits the clinical picture of hyperactivity but contrasts with literature that reports sedentary ADHD lifestyle.
Keywords: ADHD, lifestyle, diet, adulthood, ASRS, obesity
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a lifelong neurodevelopmental disorder that is marked by various symptoms and behavioral manifestations. The core symptoms include impulsivity, inattention, and hyperactivity. Categorically speaking, it is these symptoms that are listed in diagnostic criterions such as the Diagnostic and Statistical Manual of Mental Disorders version 5 (DSM5). The disorder is most frequently seen among children with ~50% of those affected carrying ADHD symptomatology into adulthood.1 It should also be noted that ADHD may be viewed as a continuum of symptoms and not only as a categorical construct. Twin studies have shown the importance of using the idea of the disorder as a dimensional construct that includes genetic influences and environment as risk factors, thus making the picture of the disorder very complex and not black and white.35 Furthermore, ADHD has been linked to a wide range of structural and functional brain abnormalities that are presently documented by neuroimaging studies in both children and adults.2–4
There is a probable gender discrepancy in the disorder with more males diagnosed than females, this can be explained by a possible gender bias and/or error in diagnostic criteria.5 There is also a strong genetic link associated with the disorder.6 In the case of adult ADHD, it has been associated with perilous lifestyles such as drug abuse, smoking, poor dietary habits, in particular compulsive eating, as well as a general preference for sedentary living.7,8
Most of these lifestyles are likely associated with hedonism and impulsive behavior.9 The majority of these lifestyles can result in serious health issues (obesity, hypertension, heart disease, and risky behaviors, such as reckless driving and suicidal ideation).9,10 ADHD is often connected with sleep problems, and it is not clear whether it is a real comorbidity or a result of specific sleeping habits. This is especially noted in children.11,12
Poor diet is a significant lifestyle issue associated with ADHD; it is common both in children and in adults with some light differences seen between the genders, with binge eating being more common among men and eating disorders, such as bulimia nervosa, more seen among women. These comorbidities can mask ADHD and can lead to misdiagnosis especially in girls; furthermore, women with the disorder tend to express less externalizing behaviors, and the disorder is often unnoticed and not diagnosed leading to an apparent gender disparity.13,14
Children with the disorder are often stigmatized within the school setting. This is especially common among males and in schools which provide less recreational time and physical exercise for the students.15
Good parenting styles seem to be a protective factor for certain ADHD-related lifestyles and behaviors, this is consistent with previous research on the benefits of authoritative parenting in managing children and adolescents with the disorder. The protective effects extend to lower rates of externalizing disorders and notable improvement in the quality of life for the individuals.16 Recently the benefits and protective effects of parenting have also been noted in adults with ADHD. An American study exploring this factor followed a sample of 92 undergraduate students; it was found that the students with ADHD were at a higher risk of sexually transmitted diseases/infections compared with healthy controls, and that previous closeness with their mothers in childhood had a protective effect, compared with those with ADHD, but with neglectful mothers.17
Nicotinism and substance abuse are very also associated with ADHD – one explanation may be a genetic predisposition.18 ADHD and substance abuse tend to share genetic liabilities; one of the risk factors is an abnormality in the DRD-4 gene that is partially responsible for dopamine regulation. The genetic factor should be looked at from an epigenetic perspective; it is a risk factor that is raised substantially with a poor environment, such as with low socioeconomic status and neglectful parenting and family conflicts.19 From an epidemiological perspective, adults with ADHD tend to have higher rates of nicotinism and cannabis use as well as a tendency to abuse other illegal drugs, to a higher extent than non-diagnosed individuals and individuals without ADHD symptoms. Those with ADHD also report that they begin to experiment with drugs at a much earlier age than other drug users. Paradoxically, compared with other types of drug addictions such as cocaine addiction and nicotinism, ADHD was found to be negatively correlated with problem drinking and/or alcoholism. Furthermore, other common comorbidities associated with adult ADHD are antisocial personality disorder, substance abuse and binge eating, especially among males.20
The recent research on ADHD and cerebellar dysfunction and abnormalities helps to shed light on ADHD and the associated neural mechanisms of substance abuse. For example, cigarette smoking is generally associated with cognitive and structural dysfunction in the general population but was found to have positive effects on ADHD symptoms. The positive effects of smoking on ADHD symptoms can be directly attributed to nicotine, which was found to increase attentiveness and alertness in those with the disorder; this could be one of the reasons for higher rates of nicotinism among those affected with the disorder and could be a possible form of self-medication.21–23
As was previously mentioned, those with the disorder tend to experiment with drugs at a very early age. In a study conducted in patients inside a major addiction clinic in Brazil, over 60% of those with cocaine addiction had ADHD; they were also likely to have initiated their drug use at a much earlier age than the other individuals not diagnosed with ADHD.24 Interestingly, some medications for ADHD tend to have a protective factor against later addiction and drug abuse. For example, those prescribed D-amphetamine were much less likely to use either cannabis and/or cocaine.25 The same was noted in long-term animal studies, especially in rodents where mixed amphetamine salts had a protective effect and resulted in later abstinence from cocaine use in the laboratory setting. However, methylphenidate when administered in adolescence was suspected to be a risk factor for later cocaine abuse and addiction.26
In a similar way to substance abuse and chemical dependencies, those affected with ADHD are often more prone to electronic addictions such as pathological internet use, which includes impulsive gaming and addictive behaviors associated with social media.27 An especially dangerous correlation found in those with high ADHD symptomatology was an urge to use the social network sites while driving. It was noted that those with ADHD symptoms had higher stress levels and felt a much more impulsive need to use the sites/applications even while behind the wheel of a car, thus raising the risk of automobile accidents, endangering themselves and others. Males showed higher impulsivity and addictive behaviors with social media sites, often logging in and checking “updates” as a way to relieve the discomfort of not being connected.10
To our knowledge, there is currently no study focusing on lifestyles and general ADHD symptoms in the Czech population. We believe that the lifestyles associated with adult ADHD are one of the core elements of the disorder and can give insight into treatment and management of the disorder.
Materials and methods
Study population
A sample of adults aged 18–60 years from the Czech Republic was recruited by a professional polling and statistics agency (STEM/MARK, a.s.). The subjects were randomly chosen from a Czech National Panel and the questioning was done through computer-assisted web interviewing method. Participants aged 18–49 years (N=756) were recruited online and participants aged ≥50 years (N=256) via direct phone interview. This distinction was made due to easier accessibility of participants in each age category. Because of the use of this method, the dropout rate remains unknown. The sample consisted of 1,012 participants, of whom 507 were males and 505 were females. There were no statistical differences between the two types of data collections.
All data were analyzed through frequency tables and a logistic regression model which was build for ADHD Self-Report Scale (ASRS V. 1.1) score and lifestyle questionnaire using the Stata V. 14 program. The study was approved by the Ethical Committee of the First Medical Faculty of Charles University in Prague. All participants signed written informed consent forms prior to taking part in the study.
Standardized tests and a lifestyle questionnaire
The participants of this study were administered using ASRS V. 1.1 to assess ADHD symptomatology with scores from 0 to 6, with 0 being no ADHD symptoms and 6 being extremely severe symptoms. The range of 5–6 points is considered indicative of high symptomatology of adult ADHD, that is, the individual is diagnosable as having ADHD. The result of 4 points suggests that the clinician must further investigate whether the patient is suffering from the disorder. Scores of 0–3 indicate none or weak symptoms (0) to a low number of symptoms and low probabilities of ADHD. The ASRS V. 1.1 questionnaire is standardized and considered a very reliable method of assessing ADHD symptomatology within the adult population.28 Following the demographic information and ASRS, the participants filled out self-report questions regarding their lifestyles in this order: healthy lifestyles such as their diet and exercise routines, cigarette and tobacco usage, use of illegal substances, physical activity and sports, hours watching TV per day, how many meals they consume per day, sweets and sugar consumption, daytime tiredness and sleepiness, and sleeping habits. The questions were both open and closed, for example, “Do you smoke cigarettes?” Yes or No, and “How many do you smoke?” Some were put into ranges such as, “How many hours of television do you watch per day?” with ranges including 0–1 hours up to 12 hours or more. Furthermore, certain questions regarding drug use were rated 0–4 with 0 being a protective factor (eg, Do you use cocaine? No =0). For the regression model, we included only certain lifestyle behaviours and observed their association with higher ADHD symptomatology. The questionnaire was built on previous research from the authors.
Results
ADHD and gender
The ASRS results for men and women are presented in Table 1. We found no statistically significant gender differences in ASRS scores. In total, 449 males and 456 females (77.52% of males and 78.42% of females) scored below the threshold of high ADHD symptomatology with 0–3 ASRS score. In the mild symptom category of ASRS 4, there were 37 males and 36 females (7.3% and 7.13% of the sample, respectively). The high symptomatology of 5 or 6 ASRS score was observed in 21 males (4.14% of the male sample) and 13 females (2.57% of the female sample).
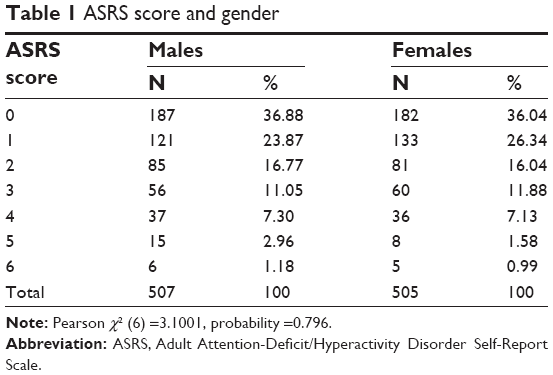 | Table 1 ASRS score and gender |
ADHD and lifestyles
Table 2 provides information on the results of ordered logistic regression of ASRS scores and significant variables inquiring about various lifestyles of the respondents. While some results confirmed our expectations, others conveyed unexpected results.
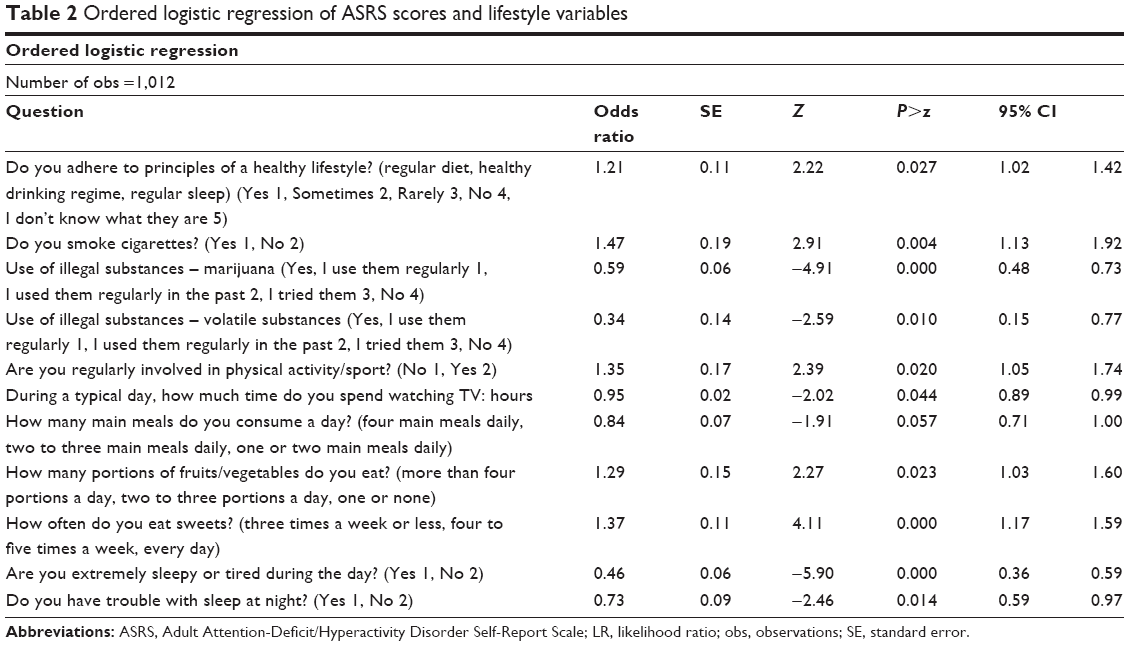 | Table 2 Ordered logistic regression of ASRS scores and lifestyle variables |
The results generally confirm that high ADHD symptoms such as impulsivity and inattentiveness as measured by the ASRS V. 1.1 are associated with specific lifestyles. We also found some surprising behavioral tendencies. As expected, those respondents with higher ADHD tendencies/symptoms were significantly more prone to an overall unhealthy lifestyle – assessed by a general question regarding regular diet, healthy drinking regime, and regular sleep (OR =1.21). Also, as we expected, respondents with increased ADHD symptoms admitted a 41% higher tendency to higher use of marijuana (OR =0.59) and an increased tendency to abuse other substances (OR =0.34); but very surprisingly, high ADHD symptoms score was negatively related to smoking (OR =1.41).
With respect to meals, participants with higher ADHD symptoms reported more frequent eating of main meals (OR =0.84) but, in concordance with expectations, less frequent consumption of portions of fruits and vegetables (OR =1.29) and more frequent snacking on sweets (OR =1.37). Our sample confirms that ADHD symptoms correlate with sleep issues, both with sleep disorders (OR =0.73) and sleepiness during the day (OR =0.46). During their free time, respondents with high ADHD symptomatology appear to spend only slightly less time watching TV than their counterparts with lower ASRS scores (OR =0.95) but they report higher engagement in physical activity and sports (OR =1.35).
Surprisingly, other drugs of abuse such as cocaine and heroin were not found to have significance among either the non-diagnosable low ASRS scorers or the ADHD high symptoms group.
Discussion
This study is the first in the Czech Republic reviewing adult symptoms of ADHD in terms of their intensity and the associated lifestyles, regardless of diagnosis. With an average of 3.36% of the individuals sample displaying increased ADHD symptomatology, the lifestyles are of the utmost importance for the study and for learning more about what could constitute key aspects of the disorder. Many of the lifestyles that we explored are consistent with previous research regarding the negative health outcomes of ADHD, such as poor diets, obesity, and poorer overall health.9
In terms of standardized tests we opted for the ASRS V. 1.1 which is one of the most reliable tests for assessing ADHD symptoms and is used in the clinical realm to assist clinicians in diagnosing individuals.28 Nonetheless, it is very important to note that a high symptoms score, such as 5–6, is not enough to draw a definite ADHD diagnosis and is only indicative of strong symptomatology, according to this instrument. Therefore, further exploration into association between ADHD diagnosis and lifestly would be advised.
In the self report questions about lifestyle, we found that most subjects with high ADHD symptomatology (ASRS scores of 5–6) rated their lifestyles as unhealthy (OR =1.24). This showed a high level of awareness and a finding that could be quite beneficial for those seeking psychotherapy, and for clinicians to focus on.
The literature on dietary habits and certain deficits seen in children diagnosed with ADHD is quite abundant, often reporting that those with the disorder tend to have iron deficiency, omega 3 and 6 imbalances, consume high amounts of fast food and sweets, resulting in an overall imbalanced diet,29 as well as obesity and hypertension.7,9 This can be the result of a possible form of self-medicating with unhealthy food, binge eating, and addiction to problematic food (ie, sugary food). This would especially be the case when the poor diet is combined with a sedentary lifestyle. Surprisingly, ADHD-prone respondents from our sample reported more physical activity and less TV watching and computer gaming than we expected. We did not ask about other games such as console systems or games on their cell phones, which may be a limitation for looking into the electronic gaming factor.
Insomnia and daytime fatigue were both statistically relevant results found in the high symptom group. This was consistent with both research in the field and our hypothesis. For instance, a previous study observing adults diagnosed with ADHD found that within the group, 62% suffered from fatigue or daytime sleepiness, often in connection with insomnia.30 We did not take into account the information on the individuals taking ADHD drugs or other psychiatric drugs in relation to sleep. This may be seen as a confound when looking at insomnia, especially since most drugs used for ADHD are stimulants. In a previous study on ADHD and insomnia, it was found that ~67% of the ADHD group suffered from insomnia compared with 20% of the healthy control group. Paradoxically, those taking stimulant prescription drugs for ADHD had lower rates of insomnia than the unmedicated individuals with the disorder.31
Sports and/or physical exercise have been consistently found to improve the outcome of the disorder in both children and adults.32 Paradoxically in our study, those who reported regular physical activity also had higher odds of ADHD symptomatology, which is something that needs to be further investigated. The study was cross-sectional a design and thus we might conclude that people with higher ADHD symptoms may excercise more. An extensive literature review found that cardiovascular exercise such as running or team sports have the most benefit for ADHD patients but non-cardio exercise such as weight lifting also had a protective effect.33
One of the most surprising results of our study was the lower rates of nicotine use and cigarette smoking among those with higher ASRS scores. This was unexpected due to the fact that most of the literature on ADHD and nicotinism focuses on those already diagnosed with the disorder and their smoking rates. Some indications show nicotine as reducing ADHD symptoms such as inattentiveness and helping those with the disorder in concentrating.22 This is a finding that could possibly explain the fact that lower rates of smoking are seen in our study in terms of higher symptoms. Nicotine could be helpful in reducing the symptoms and can be used as a form of self-medication, thus those with more intense symptoms may be self-medicating less with nicotine.34,35 A study examining nicotine and its implications in lowering symptoms of ADHD found that it lowered ADHD symptoms by up to 9% in both nicotine-naive individuals and regular smokers.23 This association needs further investigation as it could play an important role in the neurological factors associated with ADHD.
In terms of drug use, cannabis and experimentation with solvents were found among the ADHD population at an increased level. The higher rates of cannabis use/abuse was consistent with our hypothesis and predictions as well as with a vast amount of literature on the subject. One very surprising finding was the lower use of cocaine among those in our sample. This is surprising as generally cocaine addiction along with nicotinism are the most common dependencies seen in those with ADHD.8,18,20 The low use of cocaine in our sample may be due to lower availability of the drug or high price in the Czech Republic and/or other factors.
Overall, we believe that the negative lifestyle habits associated with high-intensity symptoms should be well noted by clinicians in order to help those suffering from the disorder. These lifestyles could possibly constitute one of the core manifestations of the disorder in its adult form, and we hope our research will inspire more investigation into this topic.
Conclusion
In our study, several lifestyle habits that were noted in previous ADHD literature were found to be associated with higher intensity of ADHD symptoms, such as cannabis use and poor diet (including higher consumption of sweets). Other factors usually associated with the disorder such as cocaine addiction were less prominent among the Czech sample. Nicotine use and smoking were less associated with high-intensity ADHD symptoms possibly due to self-medication phenomena and lowering of symptoms. In other words, as we looked only at symptoms and not diagnosis, it could mean that nicotine is improving symptomatology in these individuals. However, we did not observe the same effect in physical activity: we observed increased levels of exercise in those with high ASRS scores. We believe that studying the lifestyles associated with adult ADHD is very important to help those suffering from it, as they could represent core aspects of the clinical presentation of the disorder. From the finding that those in our sample showed high awareness of their poor lifestyle habits and choices, we believe that this gives clinicians a further tool for inquiry and investigation of whether ADHD is present. We recommend that clinicians take a holistic approach and not neglect lifestyles along with social and environmental influences when dealing with adults who may be suffering from the adult form of ADHD.
Acknowledgment
This article was supported by Progres Q06/1.LF and GAČR 18-11247S.
Disclosure
The authors report no conflicts of interest in this work.
References
Fayyad J, Kessler RC. The epidemiology and societal burden of ADHD. In: Adler LA, Spencer TJ, Wilens TE, editors. Attention-Deficit Hyperactivity Disorder in Adults and Children. New York: Cambridge University Press; 2015:24–41. | ||
Frodl T, Skokauskas N. Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects. Acta Psychiatr Scand. 2012;125(2):114–126. | ||
Cortese S, Kelly C, Chabernaud C, et al. Toward systems neuroscience of ADHD: A meta-analysis of 55 fMRI studies. Am J Psychiatry. 2012;169(10):1038–1055. | ||
Shaw P, Polanczyk GV. Combining epidemiological and neurobiological perspectives to characterize the lifetime trajectories of ADHD. Eur Child Adolesc Psychiatry. 2017;26(2):139–141. | ||
Williamson D, Johnston C. Gender differences in adults with attention-deficit/hyperactivity disorder: a narrative review. Clin Psychol Rev. 2015;40:15–27. | ||
Ptacek R, Kuzelova H, Stefano GB. Genetics in psychiatry up-to-date review 2011. Neuro Endocrinol Lett. 2011;32(4):389–399. | ||
Semeijn EJ, Kooij JJ, Comijs HC, Michielsen M, Deeg DJ, Beekman AT. Attention-deficit/hyperactivity disorder, physical health, and lifestyle in older adults. J Am Geriatr Soc. 2013;61(6):882–887. | ||
Weissenberger S, Klicperova-Baker M, Zimbardo P, et al. ADHD and present hedonism: time perspective as a potential diagnostic and therapeutic tool. Neuropsychiatr Dis Treat. 2016;12:2963–2971. | ||
Nigg JT. Attention-deficit/hyperactivity disorder and adverse health outcomes. Clin Psychol Rev. 2013;33(2):215–228. | ||
Turel O, Bechara A. Social networking site use while driving: ADHD and the mediating roles of stress, self-esteem and craving. Front Psychol. 2016;7:455. | ||
Prihodova I, Paclt I, Kemlink D, Skibova J, Ptacek R, Nevsimalova S. Sleep disorders and daytime sleepiness in children with attention-deficit/hyperactivity disorder: a two-night polysomnographic study with a multiple sleep latency test. Sleep Med. 2010;11(9):922–928. | ||
Novakova M, Paclt I, Ptacek R, Kuzelova H, Hajek I, Sumova A. Salivary melatonin rhythm as a marker of the circadian system in healthy children and those with attention-deficit/hyperactivity disorder. Chronobiol Int. 2011;28(7):630–637. | ||
Ptacek R, Kuzelova H, Stefano GB, et al. Disruptive patterns of eating behaviors and associated lifestyles in males with ADHD. Med Sci Monit. 2014;20:608–613. | ||
Ptacek R, Stefano GB, Weissenberger S, et al. Attention deficit hyperactivity disorder and disordered eating behaviors: links, risks, and challenges faced. Neuropsychiatr Dis Treat. 2016;12:571–579. | ||
Gwernan-Jones R, Moore DA, Cooper P, et al. A systematic review and synthesis of qualitative research: the influence of school context on symptoms of attention deficit hyperactivity disorder. Emot Behav Diffic. 2016;21(1):83–100. | ||
Molina MF, Musich FM. Perception of parenting style by children with ADHD and its relation with inattention, hyperactivity/impulsivity and externalizing symptoms. J Child Fam Stud. 2016;25(5):1656–1671. | ||
Huggins SP, Rooney ME, Chronis-Tuscano A. Risky sexual behavior among college students with ADHD: Is the mother–child relationship protective? J Atten Disord. 2015;19(3):240–250. | ||
Groenman AP, Greven CU, van Donkelaar MM, et al. Dopamine and serotonin genetic risk scores predicting substance and nicotine use in attention deficit/hyperactivity disorder. Addict Biol. 2016;21(4):915–923. | ||
Dadds MR, Schollar-Root O, Lenroot R, Moul C, Hawes DJ. Epigenetic regulation of the DRD4 gene and dimensions of attention-deficit/hyperactivity disorder in children. Eur Child Adolesc Psychiatry. 2016;25(10):1081–1089. | ||
Estévez N, Dey M, Eich-Höchli D, Foster S, Gmel G, Mohler-Kuo M. Adult attention-deficit/hyperactivity disorder and its association with substance use and substance use disorders in young men. Epidemiol Psychiatr Sci. 2016;25(3):255–266. | ||
Vnukova M, Ptacek R, Raboch J, Stefano GB. Decreased central nervous system grey matter volume (GMV) in smokers affects cognitive abilities: a systematic review. Med Sci Monit. 2017;20(23):1907–1915. | ||
Poltavski DV. Nicotine Effects on Attention: Implications for ADHD Therapy [Dissertation]. US: The University of North Dakota; 2003. | ||
Gehricke JG, Hong N, Whalen CK, Steinhoff K, Wigal TL. Effects of transdermal nicotine on symptoms, moods, and cardiovascular activity in the everyday lives of smokers and nonsmokers with attention-deficit/hyperactivity disorder. Psychol Addict Behav. 2009;23(4):644–655. | ||
Guerreiro MM. Attention deficit-hyperactivity disorder in patients in rehabilitation of drug addiction. Arq Neuropsiquiatr. 2016;74(12):951–952. | ||
Notzon DP, Mariani JJ, Pavlicova M, et al. Mixed-amphetamine salts increase abstinence from marijuana in patients with co-occurring attention deficit/hyperactivity disorder and cocaine dependence. Am J Addict. 2016;25(8):666–672. | ||
Jordan CJ, Harvey RC, Baskin BB, Dwoskin LP, Kantak KM. Cocaine-seeking behavior in a genetic model of attention-deficit/hyperactivity disorder following adolescent methylphenidate or atomoxetine treatments. Drug Alcohol Depend. 2014;140:25–32. | ||
Carli V, Durkee T, Wasserman D, et al. The association between pathological internet use and comorbid psychopathology: a systematic review. Psychopathology. 2012;46(1):1–13. | ||
Adler LA, Spencer T, Faraone SV, et al. Validity of pilot adult ADHD self-report scale (ASRS) to rate adult ADHD symptoms. Ann Clin Psychiatry. 2006;18(3):145–148. | ||
Millichap JG, Yee M. The diet factor in attention deficit/hyperactivity disorder. Pediatrics. 2012;129(2):330–337. | ||
Rogers DC, Dittner AJ, Rimes KA, Chalder T. Fatigue in an adult attention deficit hyperactivity disorder population: a trans-diagnostic approach. Br J Clin Psychol. 2017;56(1):33–52. | ||
Brevik EJ, Lundervold AJ, Halmøy A, et al. Prevalence and clinical correlates of insomnia in adults with attention deficit hyperactivity disorder. Acta Psychiatr Scand. 2017;136(2):220–227. | ||
Den Heijer AE, Groen Y, Tucha L, et al. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with ADHD: a systematic literature review. J Neural Transm (Vienna). 2017;124(Suppl 1):S3–S26. | ||
Halperin JM, Healey DM. The influences of environmental enrichment, cognitive enhancement, and physical exercise on brain development: can we alter the developmental trajectory of ADHD? Neurosci Biobehav Rev. 2011;35(3):621–634. | ||
Stefano GB, Ptacek R, Kuzelova H, Kream RM. Endogenous morphine: up-to-date review. Folia Biol (Praha). 2012;58(2):49–56. | ||
Greven CU, Merwood A, van der Meer JM, Haworth CM, Rommelse N, Buitelaar JK. The opposite end of the attention deficit hyperactivity disorder continuum: genetic and environmental aetiologies of extremely low ADHD traits. J Child Psychol Psychiatry. 2016;57(4):523–531. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.