")
Back to Journals » International Journal of Women's Health » Volume 12
Adequacy of Prenatal Care in Northeast Brazil: Pilot Data Comparing Attainment of Standard Care Criteria for First-Time Adolescent and Adult Pregnant Women
Authors Barbosa de Andrade R, Pirkle CM , Sentell T , Bassani D , Domingues MR , Câmara SMA
Received 18 July 2020
Accepted for publication 2 September 2020
Published 10 November 2020 Volume 2020:12 Pages 1023—1031
DOI https://doi.org/10.2147/IJWH.S272743
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Raísa Barbosa de Andrade,1 Catherine M Pirkle,2 Tetine Sentell,2 Diego Bassani,3 Marlos Rodrigues Domingues,4 Saionara MA Câmara1,5
1Postgraduate Program in Public Health, Faculty of Health Sciences of Trairi, Federal University of Rio Grande do Norte, Natal, Brazil; 2Office of Public Health Studies, University of Hawaii at Mānoa, Honolulu, HI, USA; 3Department of Paediatrics, Faculty of Medicine & Dalla Lana School of Public Health University of Toronto, Toronto, ON, Canada; 4Postgraduate Programme in Physical Education, Federal University of Pelotas, Pelotas, Brazil; 5Postgraduate Program in Rehabilitation Sciences, Faculty of Health Sciences of Trairi, Federal University of Rio Grande do Norte, Natal, Brazil
Correspondence: Saionara MA Câmara
Faculdade de Ciências da Saúde do Trairi, Universidade Federal do Rio Grande do Norte, Rua Teodorico Bezerra, s/n, Centro, Santa Cruz, RN, Brazil
Tel +55 84 99480-6888
Email [email protected]
Background: Adolescent pregnancy is a public health concern worldwide, particularly in low-income settings. Adolescent mothers face higher risks during pregnancy and delivery compared to adult mothers and yet, may also experience worse quality of obstetrical care. This study evaluates adherence to meeting Brazilian recommendations for prenatal care by comparing first-time adolescent versus adult mothers in a rural, low-income setting.
Methods: Using data from the Adolescence and Motherhood Research (AMOR) project, we evaluated adherence to national recommendations as documented in the prenatal cards of 39 adolescents (13– 18 years) and 37 adults (23– 28 years) from a low-income area in northeast Brazil. Recommendations included ≥ 6 prenatal consultations, gestational age ≤ 12 weeks at the first visit, participation in 3 educational activities, 2 serology for syphilis (VDRL) and HIV, 1 Toxoplasmosis serology, 2 urine tests, 2 blood glucose and 2 hemoglobin/hematocrit (Hb/Ht) exams. Chi-square tests were used to compare the proportions of adolescents and adults with a record of these procedures in the prenatal cards.
Results: Compared to adult women, the adolescent group had lower attainment of almost all recommended components of prenatal care compared to the adult group, with statistically significant differences for 2 blood glucose tests (46.2% vs 78.4%; p=0.004), 2 VDRL tests (30.8% vs 54.1%; p=0.040), 2 Hb/Ht exams (35.9% vs 83.8%; p< 0.001), and at least 6 consultations (84.6% vs 100%; p=0.013).
Conclusion: Despite greater health risks of adolescent fertility, the prenatal cards of adolescent mothers presented a poorer record of adherence to recommendations for adequate prenatal care compared to adult mothers from a low-income setting of Brazil. Health policies for both health professionals and the target population are needed to ensure adequacy of prenatal care and appropriate risk reduction for this vulnerable population.
Keywords: prenatal care, delivery of health care, health records, personal, pregnancy in adolescence
Plain Language Summary
Adolescent pregnancy is a public health concern worldwide, particularly in low-income settings. Adolescent mothers face higher risks during pregnancy and delivery compared to adult mothers and yet, may also experience worse quality of obstetrical care. This study evaluates adherence to Brazilian recommendations for adequate prenatal care by comparing first-time adolescent versus adult mothers in a rural low-income setting. Using data from the Adolescence and Motherhood Research (AMOR) project, we evaluated adherence to national recommendations as documented in the prenatal cards of 39 adolescents (13–18 years) and 37 adults (23–28 years) from a low-income area in northeast Brazil. Compared to adult women, the adolescent group had lower compliance of almost all recommended components of prenatal care as recorded in the prenatal cards. The differences were more pronounced in the screening tests for diabetes, syphilis, and anemia. Thus, we found that, despite greater health risks related to adolescent fertility, the prenatal cards of adolescent mothers presented a poorer record of adherence to recommendations for adequate prenatal care compared to adult mothers from a low-income setting of Brazil. Health policies for both health professionals and the target population are needed to ensure adequacy of prenatal care and appropriate risk reduction for this vulnerable population.
Background
Adolescent fertility is a global concern, but of particular interest in low-income settings due to higher pregnancy rates among youth in these settings compared to better-off ones.1,2 In Brazil, even though adolescent fertility has declined overall since 2000, there are marked regional differences across the country with certain poorer regions experiencing recent increases in adolescent fertility rates.3,4
The incidence of conditions such as eclampsia, puerperal endometritis, and systemic infections are higher among pregnant adolescents compared to pregnant adults.5 Preterm birth, stillbirths and newborn deaths are also more frequent among adolescents.6,7 Prenatal care is an important strategy to reduce infant morbidity and mortality and to promote positive health behaviors of pregnant women, including birth preparedness.8 Quality prenatal care may assist in the early identification and treatment of dangerous health conditions as well as mitigate certain obstetrical risks related to early childbearing.
The quality of prenatal care may not be the same for adolescents compared to adults. Results of studies comparing the prenatal care of adolescent versus adult mothers report poorer care for adolescents.9,10 This may reflect a need for health policies targeting young populations, as well as the impact of cultural factors, such as stigma and discrimination against adolescent mothers, on the prenatal assistance. To our knowledge, there is very limited research on this topic in Brazil, especially in the poorer and more rural areas where adolescent fertility is frequent.
In 2011, the Brazilian Ministry of Health implemented a strategy, called Rede Cegonha, which aims to improve the quality of prenatal care for all pregnant women in the country.11 This strategy aligns with international standards for maternal and child health and was part of national actions seeking to meet two of the Millennium Development Goals established by the United Nations in 2000: #4 reduce child mortality and #5 improve maternal health.12 Health professionals are expected to follow all procedures in Rede Cegonha and record these in a pregnant woman’s national prenatal card (Caderneta da Gestante). Not doing so would represent a deviation from standard accepted practice in Brazil.
The national prenatal card is a standardized instrument established in 2014 and updated in subsequent years. It serves as a source of rapid consultation for health-care professionals and ensures continuity of care for the patient. The record of the health-care procedures documented in the prenatal cards, as well the quality of the records, reflects the patient’s quality of care and serves as a parameter to guide future clinical decisions.13 Evaluation of prenatal records and how consistently recorded practice adheres to national recommendations may also serve to identify weaknesses and strengths in the health-care delivery system and inform health policies aiming to improve maternal and child health.
Thus, using pilot data collected as part of the Adolescence and Motherhood Research (AMOR) project, this study compares the adequacy of prenatal care for first-time adolescent and adult mothers from a rural, low-income population in northeast Brazil. It uses data recorded in national prenatal cards and compares these records with each of the national recommendations for adequate prenatal care (Rede Cegonha strategy).
Methods
This is a cross-sectional analysis of data from the prospective longitudinal AMOR pilot project, which aimed to establish a research platform to examine the pathways linking adolescent childbearing to adverse health consequences later in life. The AMOR pilot was designed to assess the feasibility of a study that could be used to test the hypothesis that adolescent pregnancy increases the risk of Non-Communicable Diseases over the long term.14 This study was performed in the Trairi region of the Rio Grande do Norte state from July 2017 to January 2019. The AMOR project consisted of three waves of data collection: baseline within the first 16 weeks of pregnancy, first follow-up during the third trimester, and final follow-up between 4 and 6 weeks postpartum. Because the AMOR pilot collected data on both adolescent and adult women pregnant for the first time in a high-fertility, rural region of Brazil, it provided a unique opportunity to explore the research objective presented in this study. For this study, we used data from the third wave of data collection, when information about prenatal care across the pregnancy was expected to be fully recorded.
Study Sample
The baseline sample size for AMOR was established at 100 participants because this number provided sufficient power to assess most epidemiological instruments and biomarker concentrations of interest to the pilot study. The current study uses the unique data collected from AMOR, but sample size estimates were not calculated for this specific study, a limitation we cover in the discussion.
Fifty first-time pregnant adolescents (13–18 years) and 50 adults (23–28 years) from five cities of the Trairi region (Santa Cruz, Lajes Pintadas, Tangará, Campo Redondo and São Bento do Trairi) comprised the baseline study sample. The age range for the adolescent group was defined as a minimum of 13 years old because the median age of menarche in Brazil is of 12.1 years,15 and thus very few girls are capable of pregnancy before 13 years. The maximum age cap at 18 years was defined because childbirth-related risks decline dramatically at and after that age,16 which suggests that a woman’s body after that age has become sufficiently mature for childbirth. It also represents the age of majority in Brazil. The age group of 23–28 for the adults was selected based on evidence suggesting this age group is at lowest childbirth-associated risk of chronic disease, which was an endpoint of interest in AMOR.17–19
Participants were recruited from the primary health-care units of the participant cities between July 2017 and May 2018. Primary care is universally funded by the Brazilian government and there is almost complete coverage of prenatal care in the region.20,21 Participants with up to 16 weeks of pregnancy were included and followed across their pregnancies. Chronic conditions diagnosed before pregnancy, and prolonged use of medications such as antidepressants and anxiolytics were considered as exclusion criteria since the AMOR study examined cardiometabolic biomarker concentrations across time (n=1). For the present analysis, we excluded participants whose prenatal cards were not provided during the postpartum evaluation. From the 100 participants evaluated at the baseline, 9 (5 adults and 4 adolescents) were excluded from the present analysis for having had a miscarriage, 4 (1 adult and 3 adolescents) for having withdrawn consent, and 1 (adolescent) for having not been located for follow-up evaluations. Another 10 participants were excluded for not having provided the prenatal card during data collection (3 adults and 2 adolescents) or they provided a version of the card that is used only in private health-care centers (4 adults and 1 adolescent), which do not have all necessary information to evaluate the adherence to national recommendations for prenatal care. This led to a final sample of 76 participants (39 adolescents and 37 adults).
Study Procedures
Interviewers were trained on conducting epidemiological research with vulnerable populations, as part of an international capacity strengthening project.22 Data were collected in the public health-care units of the towns included in the study or in the university research center located in the municipality of Santa Cruz.
We collected the following participant demographic information: age, marital status (single/dating or married/stable union), education (years of study), family income sufficiency (very good, suitable, not very good/not at all), and ethnicity (white, brown or black). We also asked if the pregnancy was planned with the following response options: totally planned, somewhat planned or not at all.
The participants’ prenatal cards were recorded by photographing all pages using a tablet device (Samsung, Galaxy model A 10.1), which was protected by a password known only by the interviewers and research coordinator. The images were later analyzed to evaluate the adequacy of the prenatal care provided (as described below).
We evaluated whether the following set of tests and exams, as recommended by Rede Cegonha, were adhered to or not: ABO/Rh blood test, Toxoplasmosis serology (IgM), HBsAg examination, hemoglobin electrophoresis, obstetric ultrasonography, cervico-vaginal cytopathology, two urine tests, two fasting glycaemia, two serologic tests for syphilis (VDRL), two hemoglobin/hematocrit (Hb/Ht) exams, and two HIV tests. We also evaluated the record of participation in at least three educational activities during pregnancy, which refers to group meetings led by health professionals aiming to discuss important health-related subjects on pregnancy and childbirth.
Additionally, we analyzed the signal indicators for adequate prenatal care according to national recommendations: a minimum of six prenatal visits, early admission to health services (before the 12th week of pregnancy), and adhering to the timeline for when certain exams and tests must be performed. The recommendations establish that the Hb/Ht exam, fasting glycaemia, VDRL, and HIV tests must be performed once up to the 20th week of pregnancy and repeated between the 28th and 36th weeks; an ordinary urine test must be performed up to the 20th week; and a urine culture exam between the 28th and 36th weeks.
Statistical Analysis
Data were analyzed using SPSS software, version 20.0. First, we described the socioeconomic characteristics of the two groups of women (adolescent versus adult) and compared them using Chi-square and Mann–Whitney tests. Next, we calculated levels of adherence to the national recommendations based on percentage attainment and compared the groups with a Chi-square test. With this, we compared both groups in relation to the adherence to each recommendation. We calculated 95% CI and p<0.05 for each analysis.
Results
Table 1 presents the sample characteristics. There were limited differences in sociodemographic characteristics between the groups. Education was statistically different between groups, as would be expected given the age differences between the groups. Importantly, the two groups did not differ significantly in terms of pregnancy planning.
 |
Table 1 Sample Characteristics of First-Time Pregnant Adolescent and Adult Women (N=76) |
Table 2 presents the proportion of first-time pregnant adolescents and adults whose prenatal cards documented receiving the tests and exams as recommended by Rede Cegonha. When comparing both groups, of the 25 items analyzed, the adolescent group presented a lower proportion of compliance on 18, with significantly different results for: 2 fasting glycaemia tests (p=0.01), fasting glycaemia between 28th and 36th weeks of pregnancy (p=0.04), 2 VDRL exams (p= 0.04), 2 Hb/Ht tests (p<0.01), Hb/Ht between 28th and 36th weeks of pregnancy (p<0.01) and “at least 6 consultations” (p=0.01).
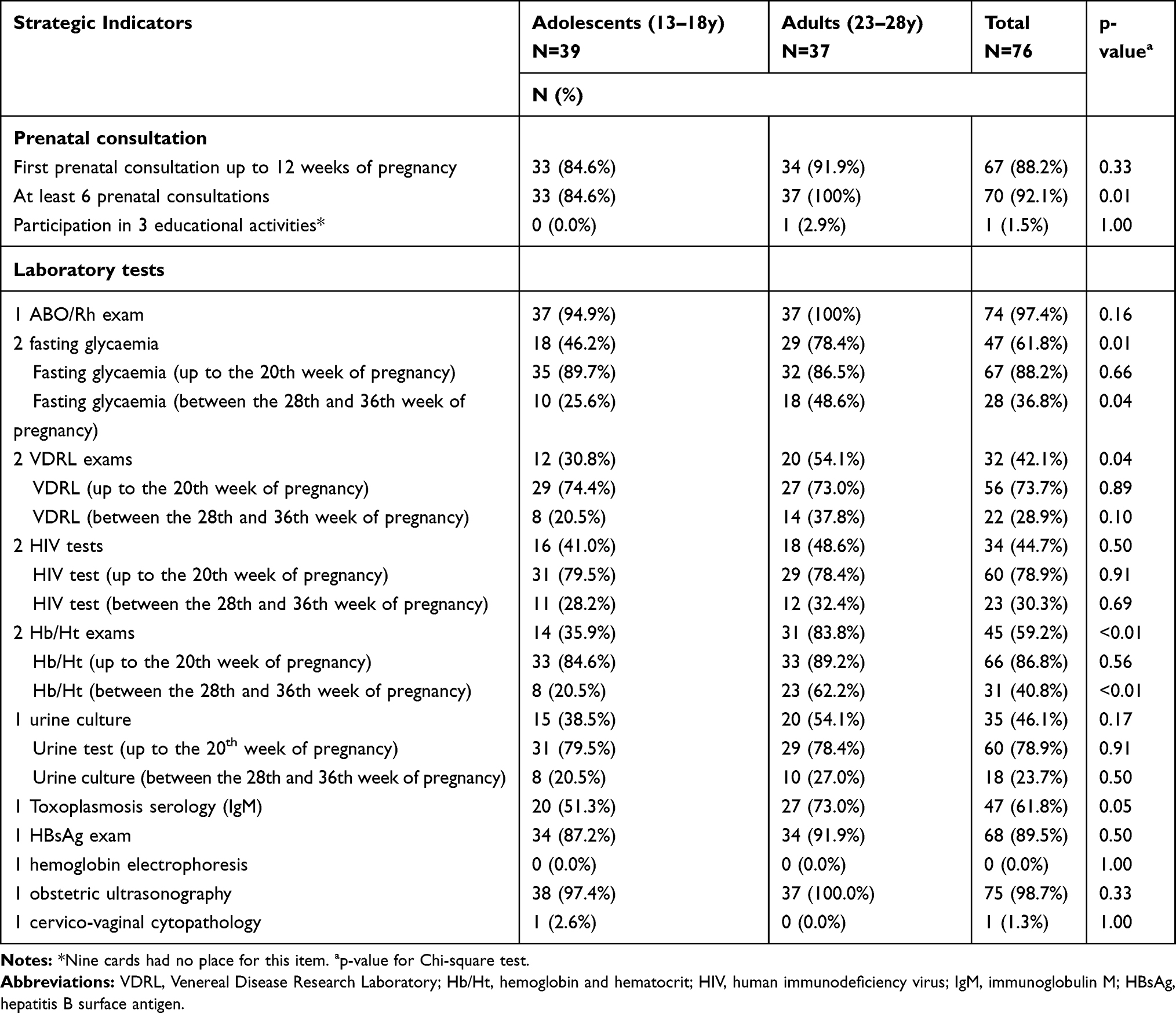 |
Table 2 Proportion of Participants Whose Prenatal Cards Recorded the Indicators of Rede Cegonha for Adequate Care (N=76) |
Only 5 recommendations presented high compliance rates for the total sample (around 90%): first prenatal consultation up to 12 weeks of pregnancy, at least 6 prenatal consultations, 1 ABO/Rh exam, fasting glycaemia and Hb/Ht up to the 20th week of pregnancy. The recommendations for attending at least three educational activities, one hemoglobin electrophoresis and one cervico-vaginal cytopathology presented very low compliance rates, being recorded in only one or none of the prenatal cards.
Discussion
This paper highlights that compliance with the Rede Cegonha strategy prenatal recommendations are, in general, poorer for first-time adolescent mothers than for first-time adult mothers in a low-income area of northeast Brazil, according to records containing in these women’s national prenatal cards. According to all 25 recommendations analyzed, the cards of the adolescent group presented lower proportions of compliance for 18 recommendations, with statistically significant differences (p<0.05) for six of them.
Among the Brazilian recommendations of laboratory tests for low-risk prenatal women, there are the minimum of two fasting glycaemia, two VDRL and two Hb/Ht. In this study, total compliance to these recommendations was around 60% for the total sample. This is a concerning result since these tests allow for the screening and/or management of gestational diabetes, syphilis and anemia, respectively. These clinical conditions, when present during pregnancy, are associated with several complications for the mother and the child.23,24 The situation is even more concerning when comparing the group of adolescents with adults, since records of completing these exams were worse among the adolescents. Previous studies have reported that adolescent pregnancy is associated with higher incidence of complications during pregnancy than during adulthood, including conditions such as anemia, urinary and vaginal infections, as well as higher rates of preterm birth, low birth weight and perinatal mortality.7,25 The lack of records for these exams may contribute to the increased risk for this group, since it reduces the possibility of identification and, consequently, mitigation of these risk factors. Thus, it is worrying that despite overall greater risk, adolescents may be receiving poorer prenatal care than adults.
The fasting glucose tests were recorded on 62% of the prenatal cards for the total sample, with significant differences between adolescents and adults. Although 88% of the total sample had a record on the prenatal cards of this exam being performed during the first 20 weeks of pregnancy, this proportion was only 36.8% for the exam being performed during the third trimester, and even lower for the adolescent group compared to the adults. Another study found similar results, with 77% of the women in northeast Brazil having a record of the first glycaemia exam in the prenatal cards, and only 28% of the second exam.20 The low compliance with this recommendation is particularly concerning, because the prevalence of gestational diabetes has increased over the past years in the Brazilian population.26 Identification of gestational diabetes is necessary for proper management during pregnancy, which can reduce many of the related risks such as induced labor, gestational hypertension, preeclampsia, excessive weight gain and post-partum hemorrhage.24
The VDRL exam is necessary to diagnose syphilis, which is a major public health concern in Brazil and the Americas. A national report showed that from 2007 to 2017, there was an increase in the rates of congenital syphilis in Brazil among children under one year,27 despite the condition being entirely preventable through low-cost treatment. Similarly, according to a report from the Pan American Health Organization (PAHO), 85% of all congenital syphilis cases diagnosed in the Americas are from Brazil.28 Data from 2017 indicate that northeast Brazil ranked second highest among the Brazilian regions for congenital syphilis, representing 28% of total registered cases of this condition in the country.27 In areas characterized by the high rates of vertical transmission of congenital syphilis, it is strongly recommended that every pregnant woman be tested for syphilis twice during pregnancy,11 because of the immunological window of syphilis and the possibility of contamination occurring between the first and the second tests. In our study, less than half of the total sample recorded two VDRL tests during pregnancy in their cards, with significantly lower percentages among adolescents than adults. Most of the participants performed this test in the first 20 weeks of pregnancy, but only one-fifth of the adolescents and 38% of the adults had documentation of a VDRL test during their third trimester. A study conducted in Brazil between 2011 and 2012 also reported lower records of the second serology for syphilis among pregnant women from the north and northeast regions compared to the other Brazilian regions, with poorer results for adolescents than for adults.29 This inadequate screening of syphilis during pregnancy may explain why the rates of congenital syphilis continue to increase irrespective of the high access to prenatal care for women in Brazil and the Americas (around 80%).28
Anemia is a major public health concern worldwide, with pregnant women and low-income populations considered high-risk groups for this condition.23 Anemia during pregnancy is associated with low birth weight, preterm delivery and perinatal mortality.30 Given these risks and because treatment of anemia is relatively inexpensive and straightforward, all pregnant women should be screened.30 Hb/Ht exams are recommended to diagnose anemia during pregnancy, and in this study, records of these exams at two time points during pregnancy were found for only 60% of the total sample, being much higher for the adults when compared to adolescents. Although more than 80% of the adolescent group completed the Hb/Ht test during the first 20 weeks of pregnancy, record of the second test (third trimester) was found for only 20% of this group. This is a concerning result given that adolescent mothers have the highest prevalence of anemia during pregnancy of any age group, and because iron and folic acid deficiencies, important causes of anemia, increase during the third trimester of pregnancy.30
Another important indicator of adequate prenatal care is the early admission to health services and the number of prenatal consultations. While access to prenatal care has increased in the Americas in the past decade, reaching around 80% of the population, these high rates mask disparities among different socioeconomic, ethnic, and age groups.28 In our study, there was no difference between adolescents and adults in relation to early admission to prenatal care; however, the percentage of adolescents with six prenatal consultations was significantly lower than the percentage of adults. It has been reported that adolescent pregnancy is associated with low adherence to prenatal care, manifested by the low number of consultations, which may contribute to a higher prevalence of low birth weight and premature births in this group.25
The lower adherence to prenatal care in adolescents may also explain differences in completion of the exams between the two groups, especially those occurring during the third trimester of pregnancy. In our study, pregnant adolescents had lower percentages than adults of documentation of all tests performed in the third trimester of pregnancy, with significant differences for fasting blood glucose and Hb/Ht. Failure to perform such tests or to perform them outside the established timeframe does not allow for the proper identification and management of important health conditions such as diabetes and gestational anemia during pregnancy. Moreover, among the six recommendations to be performed more than once during prenatal care (educational activities, urine tests, blood glucose, VDRL, Hb/Ht and HIV test), three were less frequent among adolescents.
Three recommendations presented very low proportions of compliance in the total sample: participation in 3 educational activities, hemoglobin electrophoresis test, and cervico-vaginal cytopathology. These health promotion educational activities aim to increase pregnant women’s knowledge about gestation, childbirth and post-partum procedures, and to encourage healthy behaviors. The hemoglobin electrophoresis test screens for sickle cell anemia and has been a recommended test for all pregnant women in Brazil since 2011, as the test supports early management of the disease and subsequent reduction of its associated risks.11 However, it is an expensive exam, performed by only few laboratories, which may explain low adherence to this national recommendation. The cervico-vaginal cytopathology screens for cervical cancer and its precursor lesions.31 Because women are accessing care more frequently during pregnancy, this procedure is recommended without restrictions during pregnancy since it is considered an opportune period for detection of preneoplastic lesions.31 The low compliance with this national recommendation is concerning given the fact that cervical cancer is the most common malignancy in the world and one of the greatest causes of death due to cancer among women. A previous study carried out in northeast Brazil also found that only a low percentage (11%) of women completed a cervico-vaginal cytopathology during pregnancy. These authors report that lack of information and encouragement by health professionals were the main determinants of not having this exam.32
Although we did not assess the reasons for the lower compliance with the prenatal recommendations among the adolescent group, some hypothesis can be raised. Pregnant adolescents may miss exams and procedures during prenatal care more frequently than adults because of their lower knowledge about the importance of prenatal care for their health and that of their child. Supporting this hypothesis, unpublished results from the AMOR project showed that 95% of the adolescent group had inadequate health literacy, which may contribute to insufficient prenatal care. Another hypothesis is related to cultural aspects. National guidelines for prenatal care highlight the importance of health services providing support to young pregnant women, making no value judgments or discrimination against them, and ensuring services offer privacy and are confidential. However, teenage pregnancy is often considered socially shameful, mainly among non-officially married girls, and it is still viewed with prejudice and discrimination by some health professionals.33 It is possible that pregnant adolescents may avoid visiting the health-care units for fear of being judged negatively or mistreated.
This study has several limitations. By evaluating the records on women’s prenatal cards, it is not possible to decisively confirm whether the exams and tests were not performed or if they were simply not recorded by health professionals. Although it is unlikely that the proportion of failure by the health professionals to document compliance to the recommendations differed between groups, it is possible that the lower compliance among adolescents is because they may have more frequently forgotten to take their cards to prenatal appointments when compared to adults. However, national guidelines for prenatal care advise that health professionals must record all procedures in women’s medical records, which remain in the health-care unit, and update the prenatal cards with the missing information in subsequent visits. Moreover, other causes may explain the failure in performing some exams and may explain the different proportions in relation to the different blood exams that could be performed with the same blood sample, such as failure in requesting some of them by the health-care provider or the lack of necessary reagents to perform all tests. Irrespective of the reason, it is an indication that there is an inadequacy of prenatal assistance according to national recommendations mainly for pregnant adolescents, and each of them have a different implication for the care of the pregnant woman. Additionally, since this is a secondary analysis of a cohort study, some results may reflect our recruitment process and eligibility criteria. For instance, we included participants at ≤16 weeks in their pregnancy at baseline. Thus, it was expected that almost all participants from both groups were receiving prenatal care relatively early in their pregnancies, which may not be representative of all women in the region (e.g. those who present late for care). However, given their early recruitment into prenatal care, we would expect all women in the sample to have more opportunities for proper compliance with the Rede Cegonha strategy. Thus, these results may overestimate the level of compliance with this strategy compared to the underling sample frame. Finally, the small sample size limited the power of our analyses, as AMOR pilot was designed for the purposes of this study.
This study also has several strengths. It provides valuable information on an understudied population. Our results may reflect the situation of other low-income settings with similar characteristics and can inform the implementation of health policies aiming to improve adequacy of prenatal care in these regions. Furthermore, regardless of reasons for poorer documentation of adherence to national recommendations for adequate prenatal care among pregnant adolescents, this study highlights the need for improvements in these records to ensure higher quality of care for this high-risk group. Additionally, analyzing the information recorded in prenatal cards reduces any participant recall bias about the examinations performed during pregnancy.
Conclusions
Despite greater risks for short- and long-term adverse health outcomes for both mother and child, adolescent women appear to be receiving poorer prenatal care than their older counterparts in this low-income region of northeast Brazil. This underscores the need for awareness and education policies for both health professionals and the target population on the importance of adhering to and recording prenatal recommendations to ensure adequacy of prenatal care. Further work is also needed to assess if these results are similar in other regions of Brazil.
Abbreviations
AMOR, Adolescence and Motherhood Research; CI, confidence interval; Hb/Ht, hemoglobin and hematocrit; HBsAg, hepatitis B surface antigen; HIV, human immunodeficiency virus; IgM, immunoglobulin M; PAHO, Pan American Health Organization; VDRL, Venereal Disease Research Laboratory.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. The project was approved by the local Ethical Committee of the Faculty of Health Sciences of Trairi (CEP-FACISA) and the National Commission for Research Ethics (CONEP), approval number 1.902.815. All adult participants and legal guardians of the adolescent participants provided written consent for participation on this study. Moreover, all adolescent participants provided written assent to participate, according to ethical principles.
Acknowledgments
The authors would like to thank Juliana Barbosa, MSc, Sarah Hipp, MPH, and Sabrina Fernandes, MSc, for their assistance in the activities of this project. We would like also to thank the Graduate School of the Federal University of Rio Grande do Norte for their valuable support.
Funding
Activities reported in this publication were supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brasil (CAPES) (Finance Code 001), and the Fogarty International Center of the National Institutes of Health (Award Number R21TW010466). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or CAPES.
Disclosure
Dr Catherine M Pirkle reports grants from Fogarty International Center, during the conduct of the study. Dr Saionara MA Câmara reports grants from Fogarty International Center, National Institutes of Health, during the conduct of the study. The authors declare that they have no other potential conflicts of interest for this work.
References
1. Caffe S, Plesons M, Camacho AV, et al. Looking back and moving forward: can we accelerate progress on adolescent pregnancy in the Americas? Reprod Health. 2017;14(1):83. doi:10.1186/s12978-017-0345-y
2. United Nations Population Fund [UNFPA]. Fertility and adolescent motherhood in the Southern Cone: notes for building a common agenda. 2016. Available from: http://www.unfpa.org.br/Arquivos/fecundidade_maternidade_adolescente_conesul.pdf.
3. Borges ALO, Chofakian CBN, Sato APS, Fujimori E, Duarte LS, Gomes MN. Fertility rates among very young adolescent women: temporal and spatial trends in Brazil. BMC Pregnancy Childbirth. 2016;16:57. doi:10.1186/s12884-016-0843-x
4. Vaz RF, Monteiro DLM, Rodrigues NCP. Trends of teenage pregnancy in Brazil, 2000–2011. Rev Assoc Med Bras. 2016;62(4):330–335. doi:10.1590/1806-9282.62.04.330
5. Ganchimed T, Ota E, Morisaki N, et al. Pregnancy and childbirth outcomes among adolescent mothers: a World Health Organization multicountry study. BJOG. 2014;121(Suppl 1):40–48. doi:10.1111/1471-0528.12630
6. Althabe F, Moore JL, Gibbons L, et al. Adverse maternal and perinatal outcomes in adolescent pregnancies: the Global Network’s Maternal Newborn Health Registry study. Reprod Health. 2015;12(Suppl 2):S8. doi:10.1186/1742-4755-12-S2-S8
7. Wong SPW, Twynstra J, Gilliland JA, Cook JL, Seabrook JA. Risk factors and birth outcomes associated with teenage pregnancy: a Canadian sample. J Pediatr Adolesc Gynecol. 2020;33(2):153–159. doi:10.1016/j.jpag.2019.10.006
8. Campbel OMR, Graham WJ. Strategies for reducing maternal mortality: getting on with what works. Lancet. 2006;368(9543):1284–1299. doi:10.1016/S0140-6736(06)69381-1
9. Cesar JA, Mendoza-Sassi RA, Mano OS, Goulart-Filha SM. Socio-demographic characteristics and prenatal and childbirth care in southern Brazil. Cad Saude Publica. 2011;27(5):985–994. doi:10.1590/S0102-311X2011000500016
10. Lee SH, Lee SM, Lim NG, et al. Differences in pregnancy outcomes, prenatal care utilization, and maternal complications between teenagers and adult women in Korea: a nationwide epidemiological study. Medicine (Baltimore). 2016;95(34):e4630. doi:10.1097/MD.0000000000004630
11. Ministry of Health (Brazil). Ordinance nº 1.459 of June 24th, 2011. Establishes, within the scope of the Unified Health System - SUS - the Rede Cegonha. Off Diary Union Braz. 2011;section 1:109.
12. United Nations. United nations millennium declaration. 2000. Available from: https://www.unric.org/html/portuguese/uninfo/DecdoMil.pdf.
13. Barreto FDFP, Albuquerque RM. Discrepâncias entre o informe verbal e os registros no cartão da gestante, um instrumento negligenciado. Rev Bras Ginecol Obstet. 2012;34(6):259–267. doi:10.1590/S0100-72032012000600004
14. Güneş PM. The effects of teenage childbearing on long-term health in the US: a twin-fixed-effects approach. Rev Econ Househ. 2016;14(4):891–920. doi:10.1007/s11150-016-9326-0
15. Castilho SD, Nucci LB. Age at menarche in schoolgirls with and without excess weight. J Pediatr (Rio J). 2015;91(1):75–80. doi:10.1016/j.jped.2014.05.008
16. Allal N, Sear R, Prentice AM, Mace R. An evolutionary model of stature, age at first birth and reproductive success in Gambian women proceedings. Biol Sci Royal Soc. 2004;271(1538):465–470. doi:10.1098/rspb.2003.2623
17. Gallagher LG, Davis LB, Ray RM, et al. Reproductive history and mortality from cardiovascular disease among women textile workers in Shanghai, China. Int J Epidemiol. 2011;40(6):1510–1518. doi:10.1093/ije/dyr134
18. Grundy E, Kravdal O. Fertility history and cause-specific mortality: a register-based analysis of complete cohorts of Norwegian women and men. Soc Sci Med. 2010;70(11):1847–1857. doi:10.1016/j.socscimed.2010.02.004
19. Merritt MA, Riboli E, Murphy N, et al. Reproductive factors and risk of mortality in the European Prospective investigation into cancer and nutrition; a cohort study. BMC Med. 2015;13:252. doi:10.1186/s12916-015-0484-3
20. Viellas EF, Domingues RMSM, Dias MAB, et al. Prenatal care in Brazil. Cad Saude Publica. 2014;30(Suppl 1):85–100. doi:10.1590/0102-311X00126013
21. Silva EP, Leite AFB, Lima RT, Osorio MM. Prenatal evaluation in primary care in Northeast Brazil: factors associated with its adequacy. Rev Saude Publica. 2019;53:43. doi:10.11606/s1518-8787.2019053001024
22. Câmara SMA, Sentell T, Bassani DG, Domingues MR, Pirkle C. Strengthening health research capacity to address adolescent fertility in Northeast Brazil. J Glob Health. 2019;9(1):010303. doi:10.7189/jogh.09.010303
23. Balarajan Y, Ramakrishnan U, Ozaltin E, Shankar AH, Subramanian SV. Anaemia in low-income and middle-income countries. Lancet. 2011;378(9809):2123–2135. doi:10.1016/S0140-6736(10)62304-5
24. Beucher G, Viares de Lesegno B, Dreyfus M. Maternal outcome of gestational diabetes mellitus. Diabetes Metab. 2010;36(6):522–537. doi:10.1016/j.diabet.2010.11.006
25. Azevedo WF, Diniz MB, Fonseca ESVB, Azevedo LMR, Evangelista CB. Complicações da gravidez na adolescência: revisão sistemática de literatura. Einstein. 2015;13(4):618–626. doi:10.1590/S1679-45082015RW3127
26. Pan American Health Organization (PAHO), Ministry of Health (Brazil), Brazilian Federation of Gynecology and Obstetrics Associations, Brazilian Diabetes Society. Screening and diagnosis of gestational diabetes mellitus in Brazil. 2017. Available from: https://www.diabetes.org.br/profissionais/images/pdf/diabetes-gestacional-relatorio.pdf.
27. Ministry of Health (Brazil). Health Surveillance Secretariat. Syphilis Epidemiological Bulletin. 2018. Available from: http://www.aids.gov.br/pt-br/pub/2018/boletim-epidemiologico-de-sifilis-2018.
28. Pan American Health Organization (PAHO). New generations free of HIV, syphilis, hepatitis B, and chagas diseases: EMTCT plus in the Americas. 2018. Available from: http://iris.paho.org/xmlui/bitstream/handle/123456789/50993/9789275120675_eng.pdf?sequence=2&isAllowed=y.
29. Domingues RMSM, Szwarcwald CL, Souza PRB
30. American College of Obstetricians and Gynecologists (ACOG). ACGO practice bulletin no. 95: anemia in pregnancy. Obstet Gynecol. 2008;112(1):201–207. doi:10.1097/AOG.0b013e3181809c0d
31. Gonçalves CV, Duarte G, Costa JSD, Quintana SM, Marcolin AC. Missed opportunities for cervical cancer prevention during prenatal care. Cien Saude Colet. 2011;16(5):2501–2510.
32. Monteiro PB, Monteiro-Filho MP, Figueirêdo JT, Saintrain MVL, Bruno ZV, Carvalho FHC. Cytology-based screening during antenatal care as a method for preventing cervical cancer. Asian Pac J Cancer Prev. 2017;18(9):2513–2518. doi:10.22034/APJCP.2017.18.9.2513
33. Buendgens BB, Zampieri MFM. A adolescente grávida na percepção de médicos e enfermeiros da atenção básica. Esc Anna Nery. 2012;16(1):64–72. doi:10.1590/S1414-81452012000100009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.