")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Adequacy of Improved Sources of Drinking Water, Sanitation, and Hygiene Practice for the Reduction of Diarrheal Disease Among People Living with HIV/AIDS, Harar Region, Ethiopia
Authors Tessema RA , Alemu BM
Received 15 October 2020
Accepted for publication 17 December 2020
Published 6 January 2021 Volume 2021:13 Pages 1—11
DOI https://doi.org/10.2147/HIV.S286976
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Roba Argaw Tessema, Bezatu Mengistie Alemu
Department of Environmental Health Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Roba Argaw Tessema Email [email protected]
Background: Home-based care services like improved water supply, sanitation, and hygiene (WaSH) practice are vital for people living with HIV/AIDS (PLWHA) to improve their quality of life. The negative impact of inadequate WaSH services is more pronounced among HIV-infected individuals leading them to low economic productivity, poor-nourished, immuno-compromised, and death. The aim of this study was to investigate the adequacy of improved sources of drinking water, sanitation, and hygiene practice for the reduction of diarrheal disease among people living with HIV/AIDS, Harar region, Ethiopia.
Methods: A cross-sectional study was conducted on 422 PLWHA in the Harar region related to WaSH as home-based care services and the prevalence of diarrheal disease using a standardized survey questionnaire. Descriptive statistics and multivariate Poisson regressions models were performed by SPSS Version 25. Using generalized linear models, adjusted prevalence ratio (APR) with 95%Cl and p-value were computed to assess the strength of association between the outcome and explanatory variables. A significant association was assured when the p-value is less than 0.05.
Results: In the present study, the two-week prevalence of diarrheal disease was 25%, of which 16% experienced two or more diarrheal episodes. Moreover, 87% of PLWHA used an improved source of drinking water, 66% used improved sanitation facilities, and 68% have good hygiene practices. Only 37% of the respondents acquired a basic water service level (≥ 20lcd) and 58% of PLWHA acquired the recommended quantity of safe water for drinking (≥ 1.5lcd). In multivariate analysis, the adjusted prevalence ratio of the 2-week prevalence of diarrhea was lower by 8% (APR =1.08; 95%Cl: 1.02, 1.14), 7% (APR =1.07; 95%Cl: 1.01, 1.14), and 5% (APR =1.05; 95%Cl: 1.00, 1.11) among PLWHA who have good hygiene practice, wash their hand with soap 24 hours before the survey, and used sanitation facility consistently, respectively.
Conclusion: The current study results showed that PLWHA has inadequate access to improved drinking water sources, improved sanitation facilities, and hygienic practice; these triggers stakeholders for proper interventions, effective integration of adequate WaSH services to the HIV/AIDS program to enhance the quality of life of PLWHA.
Keywords: water, sanitation, hygiene, PLWHA, diarrheal disease, home-based care service
Background
Diarrheal diseases are the most common opportunistic infections experienced by people living with HIV/AIDS (PLWHA) due to the ability to interfere with the consumption of foods and the absorption of nutrients. Improved WaSH interventions are proven to be effective in reducing diarrheal disease.1 Based on USAID data, 38 million PLWHA of which 68% of adults and 53% of children were receiving lifelong antiretroviral therapy (ART). Ensuring proper WaSH practice leading the HIV-infected people to more economic productivity, well-nourished, and healthier.2
WHO estimated that 1.8 million people die every year from diarrheal diseases, 88% of diarrheal disease attributed to unsafe water supply, inadequate sanitation, and hygiene. Improved water supply, improved sanitation, and hygiene interventions include hygiene education, and the promotion of handwashing reduces diarrheal morbidity by 6% to 25%, 32%, and up to 45%, respectively.3 Improvements in drinking-water quality through household water treatment reduce diarrheal episodes by 35% to 39%.3 Improved hygiene practices include handwashing with soap, treatment, and safe storage of water, and safe feces disposal can reduce the prevalence of the diarrheal disease by 30 to 40%.4 Adequate WaSH intervention reduces opportunistic infections and delays the progression of HIV to AIDS.5
The frequency of diarrheal infections depends on the level of water and sanitation services and hygiene practices available to households affected by HIV/AIDS. Both the facility-based and home-based care services (WaSH) need to be well effectively integrated to improve the overall health of PLWHA.6 Evidence indicates that an HIV-affected person requires more than 20 liters of water per day includes 1.5 liters of safe water for drinking with medicines.7 Inadequate WaSH added not only the health but the economic and psychological burden to the entire family. Hence, a greater need for WaSH services for PLWHA, families, and caregivers are crucial. Ethiopia integrated WaSH to HIV/AIDS programs to prevent a range of opportunistic infections include diarrheal diseases among PLWHA.1
Based on a 2017 estimate, 613,000 people living with HIV (1% being Harari region percentage) in Ethiopia.8 Based on the health and health-related indicator data, the Harari regional state has a total population of 232,000, of which 50.4% were males. The annual growth rate was 2.6. Fifty-six percent of the population lives in an urban area. The households with latrine and water supply percentage of the region were 67.8% and 93.3%, respectively. In the Harari region, the open defecation free (ODF) was 28% (15kebels out of 53 kebeles of the Harari region).9 The HIV prevalence of Harari region was 2.4% (for age 15–49) (0.9% being the national figure).10 The health service coverage of the Harari region is 100% (92% being national coverage).11 Even though considerable proportions of PLWHA suffer from diarrheal disease, there is scanty studies on the adequacy of improved sources of drinking water, sanitation, and hygiene practice for the reduction of diarrheal disease among people living with HIV/AIDS in Ethiopia and a lack of information about the level of WaSH services among PLWHA, especially in the study area. By reducing risk factors for diarrheal diseases, people living with HIV retain more nutrients, allows ART treatment more effective, healthier, and economically productive. Therefore, this research is designed to investigate the adequacy of improved sources of drinking water, sanitation, and hygiene practice for the reduction of diarrheal disease among people living with HIV/AIDS, Harar region, Ethiopia.
Methods
Study Design and Populations
A cross-sectional study was conducted from June 1 to August 31, 2013, on 422 people living with HIV/AIDS and follow-up ART services from Hiwot-Fana specialize University Hospital, Jugla Hospital, and Army Hospital in Harari region, Ethiopia. All People living with HIV/AIDS served ART in all health institutions found in the Harari region were considered as source populations. All people living with HIV/AIDS followed ART in three selected health institutions were considered as the study population.
Sample Size Determination and Sampling Procedures
The sample size was determined by using a single population proportion formula considering the proportion (p) of poor hygiene practice is 52% (P=0.52);12 5% for margin of error with a 95% confidence level. The calculated sample size was 422 (including a 10% non-response rate).
n = [(zα/2) 2 *p(1-p)]/d2 = [(1.96) 2 *0.52(1–0.48)]/(0.05)2 =383 +10% = 422 PLWHA were included in the study. A separate place was prepared near a place where clients get service at the selected hospitals. Randomly every other individual was asked for their informed consent and willingness to participate in the study when they come for ART follow-up, seek support, and counseling. Upon their permission, data collectors followed them to their home and conduct interviews and observational checkups about home-based care services related to WaSH and diarrhea episodes using a standardized survey questionnaire.
Data Collection Method, Instruments and Quality Control
A standardized questionnaire was adopted from WHO and UNICEF core questions related to drinking water and sanitation for household surveys with slight modifications to meet the current study objectives.13 Four persons with previous experience in data collection and one supervisor were involved in the study after one-day training on how to administer the questionnaire. The face-to-face interview was conducted related to sources of water supply, sanitation, hygiene facilities, and the occurrence of diarrheal disease and episodes in two-weeks before the survey. The questionnaire was prepared in English and translated into the local language, Afan Oromo. The Afan Oromo version back-translated to English to avoid any inconsistencies. The questionnaire was pre-tested on 5% of the sample outside the study area. The principal investigator checked the collection process daily.
Operational Definitions
Improved sources of drinking water include water supply source from piped water in-dwelling or yard connection, public tap or standpipe, protected tube well or borehole, protected well and spring, and rainwater. Unimproved sources of drinking water include water supply sources from unprotected dug well and springs, the cart with a small tank, tanker-truck, surface water, and bottled water. Basic water service level includes accessing a minimum of 20lcd of acceptable quality of water from an improved source not spending more than 30 minutes to fetch. Improved sanitation facilities include the facilities with sewer connections, septic tank connections, pour-flush latrines, ventilated improved pit (VIP) latrines, and pit latrines with a slab or covered pit. Unimproved sanitation facilities include a pit latrine without squatting slab and bucket used for the retention of faces and periodically removed for treatment and disposal. Good hygiene practices include human excreta contained in the toilet, available of handwashing and bathing facilities with soap and other detergents used by the household members, otherwise poor hygiene practice.13–15
Study Variables, Data Processing and Analysis
The two-week self-reported prevalence of diarrheal disease (yes/no), source of drinking water (improved/unimproved), sanitation (improved/unimproved), and hygiene practice (good/poor) were considered as outcome variables. The socio-demographic factors, factors related to the source of drinking water, sanitation facility, and hygiene practice were considered as explanatory variables. The analysis was made using SPSS Version 25 statistical package. When the outcome of interest is more common (greater than 10%), the odds ratio (OR) overestimates the prevalence ratio (PR). Hence, the Poisson regression analysis model with robust variance estimation produces a better estimate than the logistic regression model to investigate the association between outcome and explanatory variable.16,17 The adjusted prevalence ratio (APR) with 95%Cl and p-value computed to assess the strength of association between the outcome and explanatory variables. A significant association was assured when the p-value is less than 0.05.
Ethical Approval and Consent to Participate
Ethical approval was obtained from Haramaya University, College of Health and Medical Science of institutional research ethics review committee. A formal letter of permission and support was written to each hospital and health bureau from College of Health and Medical Science, Haramaya University. Informed consent was obtained from each participant before the interview. Confidentiality was secured for their HIV-positive status and participants were informed that they have the right to withdraw from the interview at any stage.
Result
Descriptive Statistics
Socio-Demographic Characteristics of PLWHA, Harar Town, Ethiopia
In this study, 416 respondents have completed the interview with a response rate of 98.6%. Forty-eight percent of the respondents’ ages range from 31 to 40 years. The mean age of respondents was 37.0 years (SD+9.0). Nearly 78% of the respondent have families more than three, 47% attend tertiary education, 54% was government employees, and 31% of the respondents were below the poverty line (Table 1).
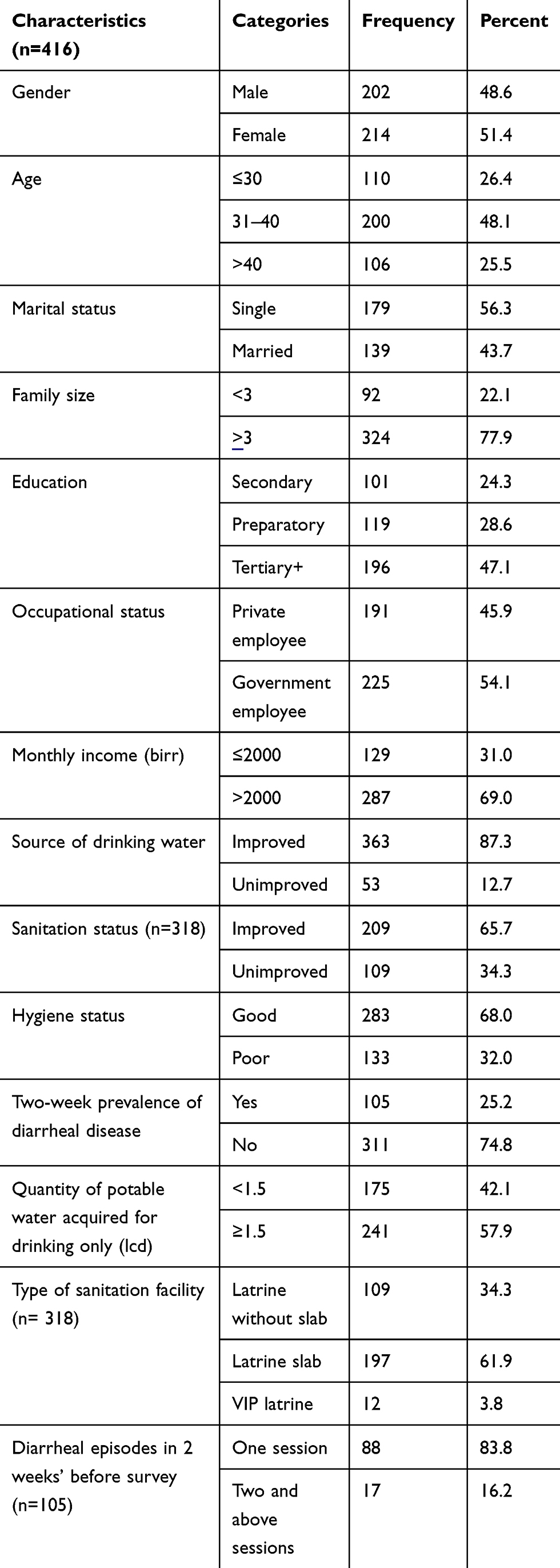 |
Table 1 Socio-Demographic and WASH Characteristics of PLWHA, Harari Region, Ethiopia |
Multivariate Analyses
Prevalence of Diarrhea Disease and Associated Factors
The current study showed that 25% of the respondents were experienced diarrheal disease 2 weeks before the survey, of which 16% of them experienced two or more diarrheal episodes. In multivariate analysis, the adjusted prevalence ratio of the 2-week prevalence of diarrhea was lower by 8% (APR =1.08; 95%Cl: 1.02, 1.14), 7% (APR =1.07; 95%Cl: 1.01, 1.14), and 5% (APR =1.05; 95%Cl: 1.00, 1.11) among PLWHA who have good hygiene practice, wash their hand with soap in 24 hours before the survey and consistently used sanitation facility, respectively (Table 2).
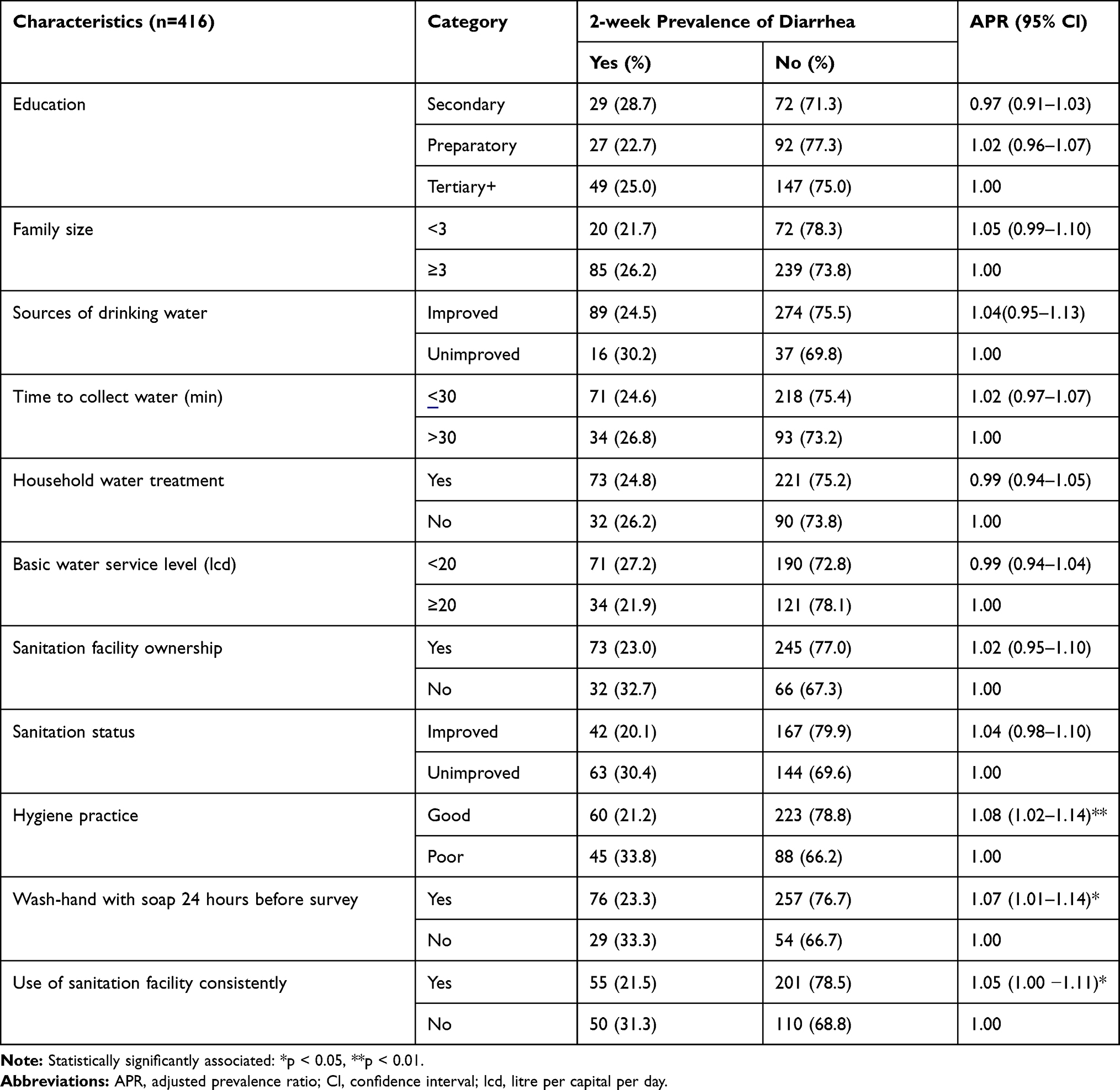 |
Table 2 2-Week Prevalence of Diarrhea and Associated Factors of PLWHA, Harari Region, Ethiopia |
Factors Associated with Drinking Water Source
In the present study, 87% of the respondents used improved drinking water sources, 94% have knowledge of at least one method of household water treatment, 71% have practiced household water treatment in 24 hours before the survey, 70% have reported that they spent 30 minutes or less to fetch water, 77% have perceived that disease could be transmitted via water, and 75% have treated water to make it safe. In multivariate analysis, the adjusted prevalence ratio of the unimproved source of drinking water use was lower by 14% (APR =0.86; 95%Cl: 0.81, 0.91), 11% (APR =0.89; 95%Cl: 0.80, 0.99), and 21% (APR =0.79; 95%Cl: 0.73, 0.85) among PLWHA who treat their water at home, have Knowledge at least one method of household water treatment and perceived that disease could transmit through water, respectively (Table 3).
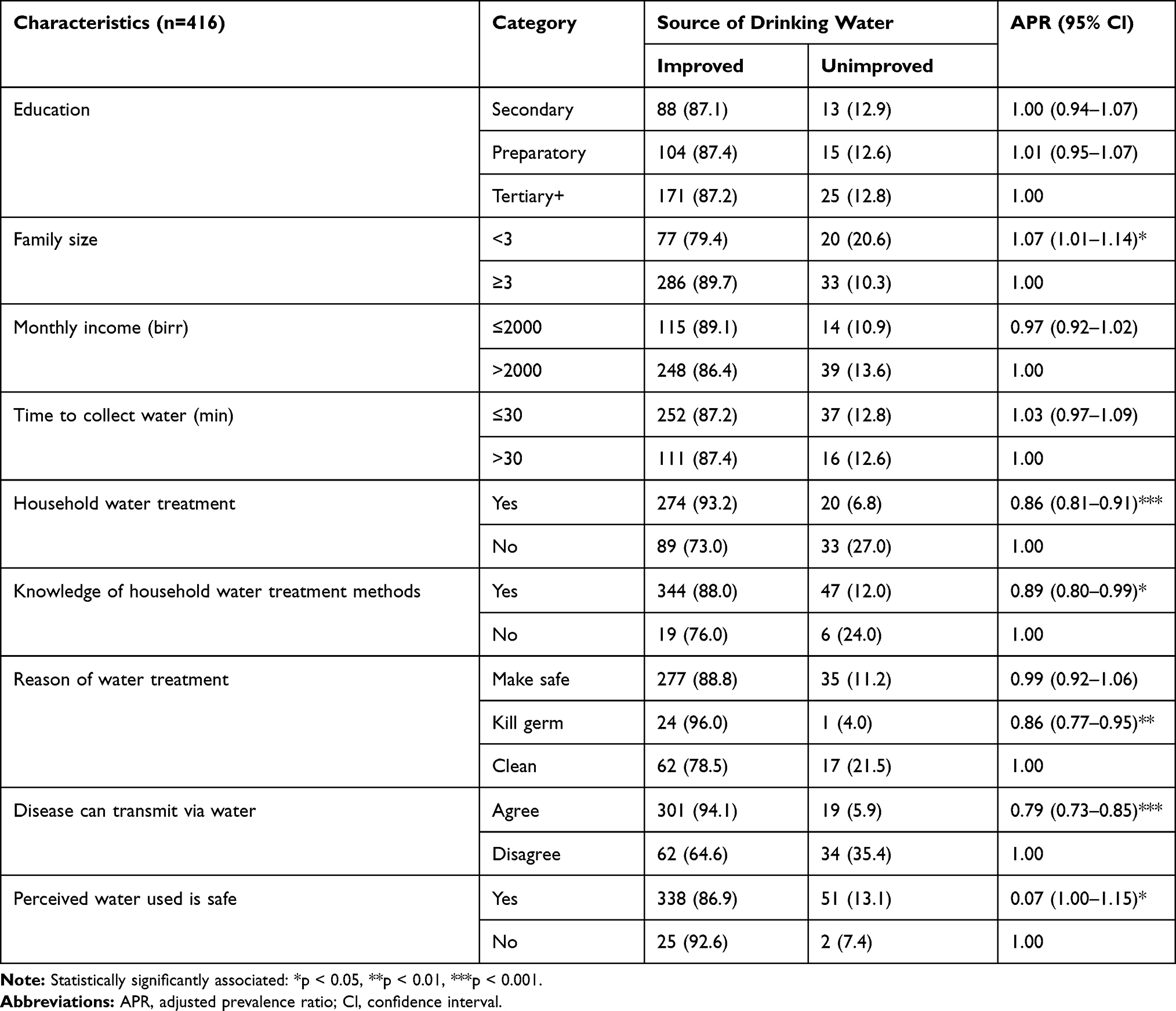 |
Table 3 Sources of Drinking Water Used and Associated Factors of PLWHA, Harari Region, Ethiopia |
Factors Associated with Sanitation Facilities
The current study indicated that 76% of the respondents have a sanitation facility, of which 26% share, and 23% were kept clean. Moreover, 66% of the respondent used improved sanitation facilities; 65% of respondents used the sanitation facilities consistently. The multivariate analysis indicated that the adjusted prevalence ratio of unimproved sanitation was higher by 26% (APR =1.26; 95%Cl: 1.18, 1.36) and 11% (APR =1.11; 95%Cl: 1.03, 1.19) among PLWHA who did not receive basic water service level, and disposing of waste inappropriately while lower by 11% (APR =0.89; 95%Cl: 0.81, 0.97) and 7% (APR =0.93; 95%Cl: 0.86, 0.99) among PLWHA who have clean sanitation facilities and attended hygiene education, respectively (Table 4).
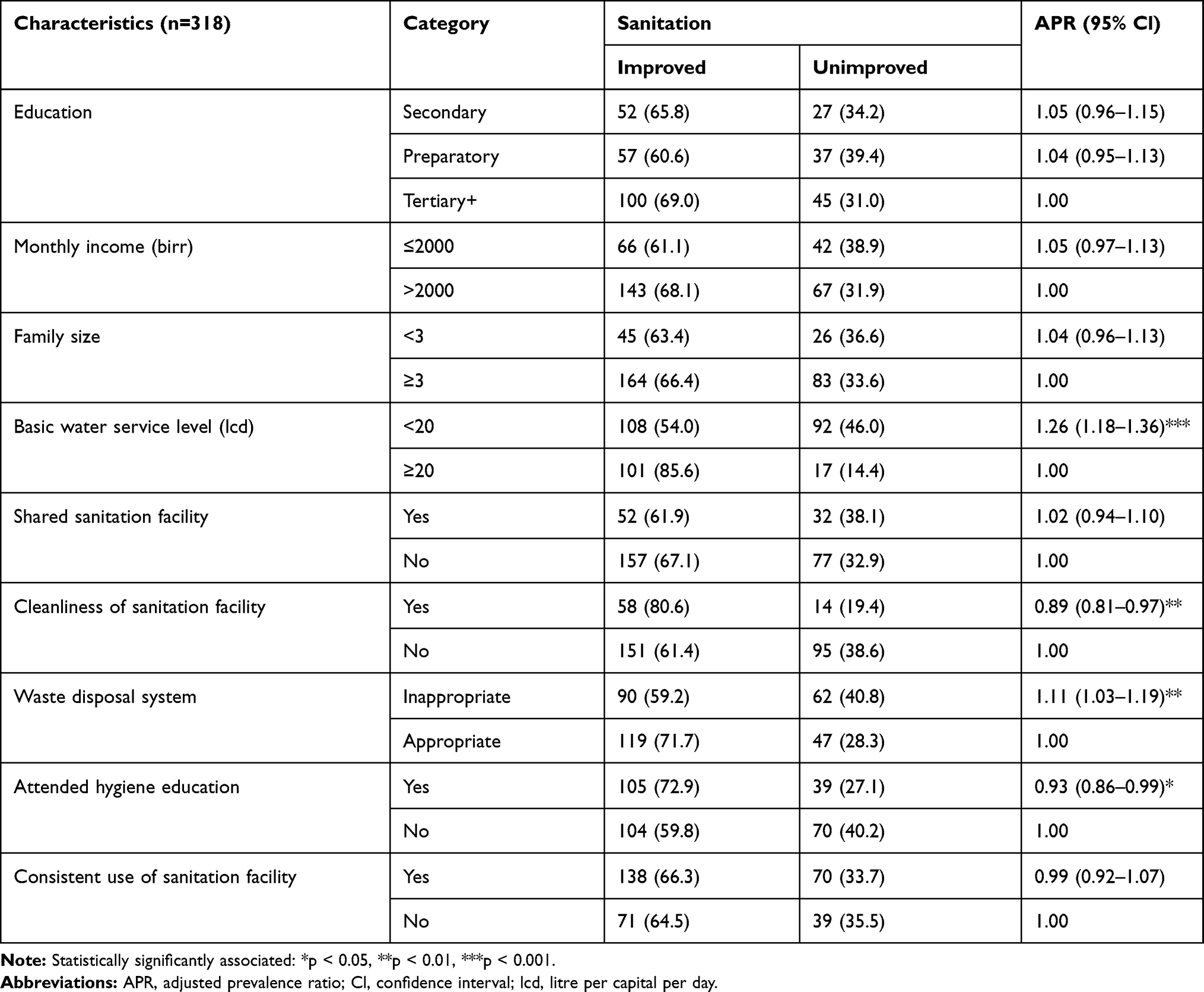 |
Table 4 Sanitation Status and Associated Factors of PLWHA, Harari Region, Ethiopia |
Factors Associated with Hygienic Practice and Risky Behaviors
This study showed that 68% of the respondent have good hygiene practice. The multivariate analyses indicated that the adjusted prevalence ratio of poor hygiene practice was higher by 10% both among PLWHA who could not receive basic water service level (less than 20L/c/d) and attend hygiene education. The handwashing practice at the critical time showed that the adjusted prevalence ratio of poor hygiene practice was lower by 8%, 12%, and 9% among PLWHA wash their hand before eating, after visiting the toilet, and after cleaning children defecation, respectively (Table 5).
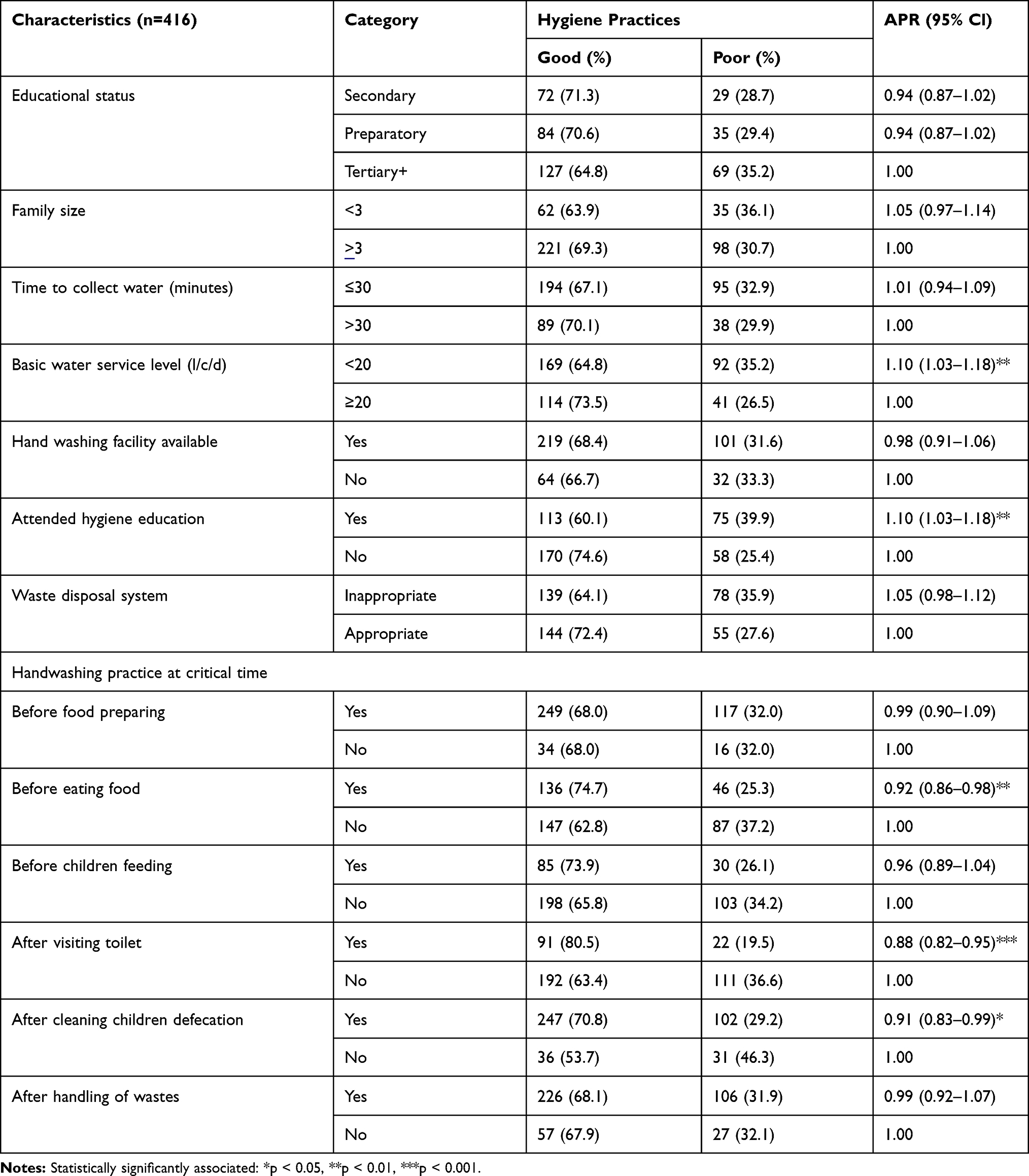 |
Table 5 Hygiene Practices and Associated Factors of PLWHA, Harari Region, Ethiopia |
Discussion
The present study has shown that people living with HIV/AIDS have inadequate access to improved drinking water sources, improved sanitation facilities, and hygienic practice that invariably call for urgent attention for all stakeholders to address the gaps. Based on sustainable developmental goal (SDG) 6, the United Nations declared that access to adequate drinking water and sanitation are considered as a basic human need, public goods, and indeed a human right.18 The WHO recommended WASH services as one of the most cost-effective interventions in reducing diarrhea for PLWHA in resource-limited settings.19
The current study findings indicated that the 2-week prevalence of diarrheal disease was 25% of which 16% experienced two or more diarrheal episodes. This finding is higher than the studies conducted in Ethiopia by Yallew and Haftu where 8%12 and 9%20 of the client experienced diarrhea for the past 24 hours, respectively. A study conducted by Uzma and colleagues in New York City indicated that 28%21 of the HIV-infected patients experienced three or more bowel movements per day within the preceding 7 days of the survey. In another study conducted by David on the effects of handwashing with soap on diarrhea rates in PLWHA indicated that a 58% reduction in diarrheal incidence from three episodes of diarrhea to one episode.22 The study conducted in less developed countries on hygiene and hand washing showed that a 30 to 40% reduction in diarrheal disease associated with handwashing with soap.23 This discrepancy may be attributed to the difference in duration of measurement of the prevalence of the diarrheal disease, consistent utilization of WaSH services, and socio-economic conditions among the study population. This study indicated that hygiene practice, handwash with soap 24 hours before the survey, and consistent utilization of sanitation facility were significantly associated with a 2-week prevalence of diarrhea. This finding is dissimilar with a study conducted by Missaye in northeast Ethiopia where the overall prevalence of intestinal parasite on-ART patients was significantly associated absence of sanitation facility, use of an unprotected source of water, and poor living condition.24 This trigger the local government to improve more WaSH services among the current study population to decrease the risk of transmission of waterborne and other enteric pathogens. In addition to the physical presence of WaSH facilities, proper and consistent utilization of the facilities have to be secured to reduce morbidity and mortality from diarrhea disease among PLWHA. This could be achieved by enhancing their knowledge of WaSH services, improve their economic condition, and improve the availability of WaSH services in the region through the coordinated effort of local government and non-governmental organizations.
The present study showed that 87% of the PLWHA used improved drinking water sources. This finding is promising compared to the study conducted in Gonder town (57%)12 and Arbaminch town (77%)20 in Ethiopia, Zimbabwe (75%),25 and Nepal (85%).26 This may be due to the better involvement of the local government to improve the water system service in the region, improve the water source by improving water handling and utilization system among PLWHA, improve their knowledge related to WaSH, and their economic condition. The present study also indicated that 37% and 31% of the PLWHA gained basic water service level (20lcd) and spent more than 30 minutes to fetch water, respectively. This result lower than the study conducted in South Asia where most home-based care gained more than the 20lcd that is considered basic water service level, and the majority of the households spent 15 minutes or less than one kilometer to fetch water.27 Similarly, a study conducted in Indian showed that women spend an average of 2.2 hours per day to collect water;28 likewise, a study conducted in Ethiopia in Gonder town support this finding where 71% of PLWHA gained 16lcd to 20lcd of water and 10% of them forced to go far distance to fetch water.12 This indicates that there is still a high unmet need for an adequate quantity of water and accessibility to potable water. It is known that as the severity of HIV/AIDS increases more liters of water could be required daily. Access to sufficient supplies of potable water is an integral element to mitigate the impacts of HIV/AIDS. Hence, more effort of individual, collective, governmental, and non-governmental organizations is crucial to alleviate the problem in the region.
This study indicated that 76% of the PLWHA have a sanitation facility of which 66% were improved. This finding is higher than the studies conducted by Haftu and Yallew in Ethiopia where both studies showed 58% of the PLWHA have sanitation faculties with 47%20 and 33%12 were improved, respectively. But lower than the findings of the study conducted in Nepal and Zimbabwe, where 74%25 and 98%26 of PLWHA have used improved sanitation facilities, respectively, while consistent with a study conducted in Zambia, where 75% of home-based care clients have a latrine where 20% of the latrines were contaminated with the fecal matter indicating prime transmission sites for water-borne pathogens.29 This discrepancy may be due to the difference in the study population in terms of the socio-economic characteristics, level of government involvement to improve the availability and accessibility of sanitation facilities, cleanliness and consistent utilization, and the level of life-saving information about diarrhea disease risk factors and their prevention.
The present study indicated that 68% of PLWHA were practiced good hygiene. This finding is promising compared to the studies conducted in Ethiopia in Gonder and Arbaminch cities, where 48% and 59% of the PLWHA were practiced good hygiene, respectively. This may be due to better effort made related to knowledge of hygiene practices, presence of handwashing facility, promotion, and awareness creation activities regarding handwashing and general hygiene among the current study population. In the present study, 45% of PLWHA attended hygiene education in the past 12 months. This finding is lower than the study conducted in Nepal (72%). This urges the need to target specific WaSH/HIV education among the current study population. In this study, the handwashing practice at a critical time seems very low; only 44% and 27% of PLWHA washed their hand before eating and after visiting the toilet, respectively. This finding is lower than the study conducted in Nepal where 86% and 100% of PLWHA washed their hand before eating food and after visiting the toilet, respectively.26 This indicates that there is a high-risk diarrheal disease incidence among this study population, their family members, and caregivers. This may demand behavioral change communications (BCC) targeted to these groups and urgent interventions by all concerned bodies to bring safe WaSH service to this study population.
Conclusion
In this study, a considerable proportion of PLWHA suffering from life-threatening opportunistic infections due to unsafe drinking water supply, inadequate sanitation, and poor hygiene for this study. The two-week prevalence of diarrheal disease and the frequency of episodes among the study population are considerably high. The improved source of drinking water supply, improved sanitation facilities availability, cleanliness and utilization, and good hygiene practice were inadequate. Substantial proportions of PLWHA could not acquire the recommended quantity of safe water for drinking (≥1.5lcd) and the basic water service level (≥20lcd). Conversely, considerable proportions of respondents washed their hands with soap 24 hours before the survey, and have knowledge of at least one method of water treatment that is considered a promising result of this study. Overall, adequate quantity and potable quality of water, safe handling and disposal of human excreta and management of waste, and effective hygiene practices including handwashing and regular hygiene education are the urgent need of this study population to improve their all-rounded quality of life.
Abbreviation
PLWHA, people living with HIV/AIDS; WaSH, water, sanitation and hygiene; APR, adjusted prevalence ratio; CI, confidence interval; WHO, World Health Organization; ART, antiretroviral therapy; HIV/AIDS, human immunodeficiency virus/Acquired immunodeficiency syndrome; lcd, liter per capital per day; USAID, United States Agency for International Development; ODF, Open defecation free; UNICEF, United Nations Children’s Fund.
Data Sharing Statement
All data pertinent to the study are included in the article and available in the supplementary material. All data are fully available to interested researchers upon request from the authors.
Ethics Approval and Consent
We obtained ethical approval from the Institutional Health Research Ethics Review Committee (IHRERC) of the Haramaya University College of Health and Medical Science. All participants provided verbal informed consent after informing the purpose, benefit, risk, the confidentiality of the information, and voluntary nature of participation in the study, and the use of verbal consent was approved by the Haramaya University College of Health and Medical Sciences IHRERC Board. This study was conducted in accordance with the Declaration of Helsinki. To keep confidentiality no identifier was used during data collections.
Acknowledgments
We would like to acknowledge the Haramaya University college of health and medical science for funding this project. We would like to extend our gratitude to Hiwot-Fana specialize University Hospital, Jugla Hospital, and Army Hospital for all aspects of unreserved support when needed. Our special thank goes to study participants, data collectors, and supervisors.
Author Contributions
Both authors made a significant contribution to the work from its conception, study design, execution, acquisition of data, analysis and interpretation, drafting, critically reviewing the article; gave final approval to be published, and accountable for all aspects of the work.
Funding
This project has funded by Haramaya University College of Health and Medical Science.
Disclosure
The authors declared that they have no competing interests.
References
1. Wilbert EQ, Jay PG. Integration of WASH interventions into HIV/AIDS programs in sub-Saharan Africa. Waterlines. 2014;33(2):168–186.
2. Wateraid. Water, sanitation and hygiene and HIV and AIDS: opportunities for integration.
3. WHO. Water, sanitation and hygiene links to health. Facts and figures updated. November, 2004. Available from: https://www.who.int/water_sanitation_health/publications/facts2004/en/.
4. Seremet C. Water, sanitation and hygiene considerations in home-based care for people living with HIV. 2010.
5. Walson JL, Sangaré LR, Singa BO, et al. Evaluation of impact of long-lasting insecticide-treated bed nets and point-of-use water filters on HIV-1 disease progression in Kenya. AIDS. 2013;27(9):1493–1501. doi:10.1097/QAD.0b013e32835ecba9
6. Lule JR, Mermin J, Ekwaru JP, et al. Effect of home-based water chlorination and safe storage on diarrhea among persons with human immunodeficiency virus in Uganda. Am J Trop Med Hyg. 2005;73(5):926–933. doi:10.4269/ajtmh.2005.73.926
7. WSP. Field note: water, sanitation, and hygiene for people living with HIV and AIDS. 2007.
8. Federal HIV/AIDS Prevention and Control Office (FHAPCO). HIV prevention in Ethiopia National Road Map 2018–2020. Ethiopia; 2018.
9. Federal Ministry of Health (FMOH). Federal democratic republic of Ethiopia ministry of health. Health and health related indicator. 2015.
10. Central Statistical Agency (CSA) and ICF. Ethiopia demographic and health survey: HIV report. Addis Ababa, Ethiopia and Rockville, Maryland, USA: CSA and ICF; 2016.
11. Federal Ministry of Health (FMOH). Health and health related indicators. Version 2. Ethiopia: Policy Planning Directorate, Ministry of Health; 2014.
12. Yallew WW, Terefe MW, Herchline TE, et al. Assessment of water, sanitation, and hygiene practice and associated factors among people living with HIV/AIDS home based care services in Gondar city, Ethiopia. BMC Public Health. 2012;12:1057. doi:10.1186/1471-2458-12-1057
13. WHO/UNICEF. Core questions on drinking-water and sanitation for household surveys. Switzerland: World Health Organization; 2006.
14. Patrick M, Charles B, Catarina F, et al. Ladders for Assessing and Costing Water Service Delivery.
15. WHO/UNICEF/JMP: WASH in the 2030 Agenda. New global indicators for drinking water, sanitation and hygiene. JMP ‘ladders’ for monitoring drinking water, sanitation and hygiene in the 2030 agenda. 2017.
16. JDB A, Vânia NH. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol. 2003;3:21. doi:10.1186/1471-2288-3-21
17. Ashutosh RT, Andrew OW, Greer AB, et al. Prevalence odds ratio versus prevalence ratio: choice comes with consequences. Stat Med. 2016;35(30):5730–5735. doi:10.1002/sim.7059
18. Guppy L, Praem M, Manzoor Q. Sustainable development goal 6: two gaps in the race for indicators. Sustain Sci. 2019;14:501–513. doi:10.1007/s11625-018-0649-z
19. WHO. Essential prevention and care interventions for adults and adolescents living with hiv in resource-limited settings. strengthening health services to fight HIV/AIDS. HIV/AIDS Programme. WHO; 2008.
20. Haftu D, Gebrekiros G, Desalegn A, et al. Water, sanitation and hygiene practice and associated factors among HIV infected people in Arba Minch town, Southern Ethiopia. J Water Health. 2017;15(4):615–625. doi:10.2166/wh.2017.373
21. Siddiqui U, Bini EJ, Chandarana K, et al. Prevalence and impact of diarrhea on health-related quality of life in HIV-infected patients in the era of highly active antiretroviral therapy. J Clin Gastroenterol. 2007;41(5):484–490. doi:10.1097/01.mcg.0000225694.46874.fc
22. Huang DB, Zhou J. Effect of intensive handwashing in the prevention of diarrheal illness among patients with AIDS: a randomized controlled study. J Med Microbiol. 2007;56:659–663. doi:10.1099/jmm.0.46867-0
23. Fewtrell L, Kaufmann RB, Kay D, et al. Water, sanitation, and hygiene interventions to reduce diarrhoea in less developed countries: a systematic review and meta-analysis. Lancet Infect Diseases. 2005;5(1):42–52. doi:10.1016/S1473-3099(04)01253-8
24. Missaye A, Mulat D, Abebe A, et al. Prevalence of intestinal parasites and associated risk factors among HIV/AIDS patients with pre-ART and on-ART attending dessie hospital ART clinic, Northeast Ethiopia. AIDS Res Ther. 2013;10:7. doi:10.1186/1742-6405-10-7
25. Natasha P, Tendayi BM, Tobias GB. The impact water, sanitation and hygiene infrastructures have on people living with HIV and AIDS in Zimbabwe. 2011. doi: 10.5772/19431
26. Gautam OP, Bhandari A, Gurung S. Access to water, sanitation and hygiene for people living with HIV and AIDS: a cross-sectional study in Nepal. The future of water, sanitation and hygiene in low-income countries - Innovation, adaptation and engagement in a changing world:35th WEDC International Conference. Loughborough, UK; July 6-8, 2011:4.
27. USAID/HIP. Analysis of research on the effects of improved water, sanitation, and hygiene on the health of people living with HIV and AIDS and programmatic implications. 2007.
28. USAID. Integrating sanitation in to the services for people living with HIV and AIDS. NW Washington: US Agency for International Development; 2012.
29. Maric K, Cindy R, James C, et al. Water and Sanitation assessment of home-based care clients in Zambia. Catholic Relief Services, WHO and USAID; 2006.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.