")
Back to Journals » Clinical Interventions in Aging » Volume 18
Addressing Unmet Needs in Vaccination for Older Adults in the Asia Pacific: Insights from the COVID-19 Pandemic
Authors Woodward M, Ramasubramanian V, Kamarulzaman A, Tantawichien T, Wang M , Song JY, Choi WS, Djauzi S, Solante R, Lee WS, Tateda K , Pan H, Wang NC, Pang T
Received 31 January 2023
Accepted for publication 8 May 2023
Published 31 May 2023 Volume 2023:18 Pages 869—880
DOI https://doi.org/10.2147/CIA.S406601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Michael Woodward,1,* Venkatasubramanian Ramasubramanian,2 Adeeba Kamarulzaman,3 Terapong Tantawichien,4 Minggui Wang,5 Joon Young Song,6 Won Suk Choi,7 Samsuridjal Djauzi,8 Rontgene Solante,9 Wen-Sen Lee,10 Kazuhiko Tateda,11 HongXing Pan,12 Ning-Chi Wang,13 Tikki Pang14,*
1Aged Care Research, Austin Health, Melbourne, VIC, Australia; 2Department of Infectious Diseases, HIV & Tropical Medicine, Apollo Hospitals, Chennai, TN, India; 3Department of Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia; 4Department of Medicine, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand; 5Institute of Antibiotics, Huashan Hospital, Fudan University, Shanghai, SH, People’s Republic of China; 6Division of Infectious Diseases, Department of Internal Medicine, Korea University Guro Hospital, Korea University College of Medicine, Seoul, Korea; 7Division of Infectious Diseases, Department of Internal Medicine, Korea University Ansan Hospital, Korean University College of Medicine, Ansan, Korea; 8Allergy and Clinical Immunology Division, Department of Internal Medicine, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 9Adult Infectious Diseases and Tropical Medicine, San Lazaro Hospital, Manila, NCR, Philippines; 10Division of Infectious Diseases, Department of Internal Medicine, New Taipei City Hospital, New Taipei, Taiwan; 11Department of Microbiology and Infectious Diseases, Faculty of Medicine, Toho University, Tokyo, Japan; 12Institution of Vaccine Clinical Trials, Jiangsu Provincial Center for Disease Control and Prevention, Nanjing, JS, People’s Republic of China; 13Department of Medicine, Tri-Service Hospital, Taipei, Taiwan; 14Centre for Behavioural and Implementation Science Interventions, Yong Loo Lin School of Medicine, National University of Singapore, Singapore
*These authors contributed equally to this work
Correspondence: Tikki Pang, Centre for Behavioural and Implementation Science Interventions, Yong Loo Lin School of Medicine, National University of Singapore, 10 Medical Dr, 117597, Singapore, Tel +65 6516 1048, Email [email protected]
Abstract: The impact of vaccinating the older population against vaccine-preventable diseases in terms of health, social and economic benefits has been increasingly recognised. However, there is a gap in the utilisation of vaccines worldwide. The population is ageing at an unprecedented pace in the Asia-Pacific (APAC) region, with the number of persons older than 65 years set to double by 2050 to around 1.3 billion. More than 18% of the population in Japan, Hong Kong, and China is over the age of 65 years. This highlights the importance of prioritising resources to address societal obligations toward the needs of the ageing generation. This review provides an overview of the challenges to adult vaccination in APAC, drivers to increase vaccination coverage, vaccination insights gained through the COVID-19 pandemic, and potential measures to increase the uptake of adult vaccines in the region.
Keywords: adult vaccination, vaccine-preventable diseases, VPD, adult vaccines, COVID-19 vaccination
Introduction
COVID-19, influenza, pneumococcal disease, and varicella zoster are the vaccine-preventable diseases (VPDs) that account for the most significant morbidity and mortality among the older adult population who often suffer from several comorbidities and are at a higher risk of complications and death. These VPDs also contribute to decreased functional ability and frailty, potentially pushing older persons towards dependency for their care.1 Vaccines can effectively reduce the impact of disease in the elderly and reduce the socioeconomic burden for societies.2
Immunising older adults promotes positive ageing, prevents suffering, and improves the quality of life, which is possibly more valuable to the older generation than gaining years of life. In addition, healthy older adults often provide support systems for their families, contributing towards childcare and providing financial and emotional support.1 They are increasingly likely to themselves be in the workforce.
Adult vaccines can also help in the global fight against antimicrobial resistance, one of the top ten global health threats. Influenza immunisation is associated with a decrease in antibiotic use, and pneumococcal vaccines reduce the carriage and transmission of antimicrobial-resistant strains of pneumococcus.1 Vaccinations also reduce disease-related hospitalisations reducing healthcare expenditure substantially.3 Australia saw a decrease in antiviral prescriptions following an anti-zoster vaccination drive, implying a reduced financial burden associated with this disease.4
Current Vaccination Practices and Policy Preparedness
Vaccination of older adults has, in general, remained low in APAC, although there is considerable variation in the uptake in different nations. For example, the influenza vaccine has an uptake of only 14.9% among the Asian general population and 37.3% among high-risk groups, much less than the WHO target rate of 75%.5 Given the socioeconomic and political diversity of the region, the levels of funding and campaign efforts around life-course immunisation differ across Asian region (Table 1). Other reasons, including differences in public education, misinformation and misconceptions, and lack of vaccine confidence, also contribute to low uptake rates.3 Many nations lack data, policies, political will and resources.1
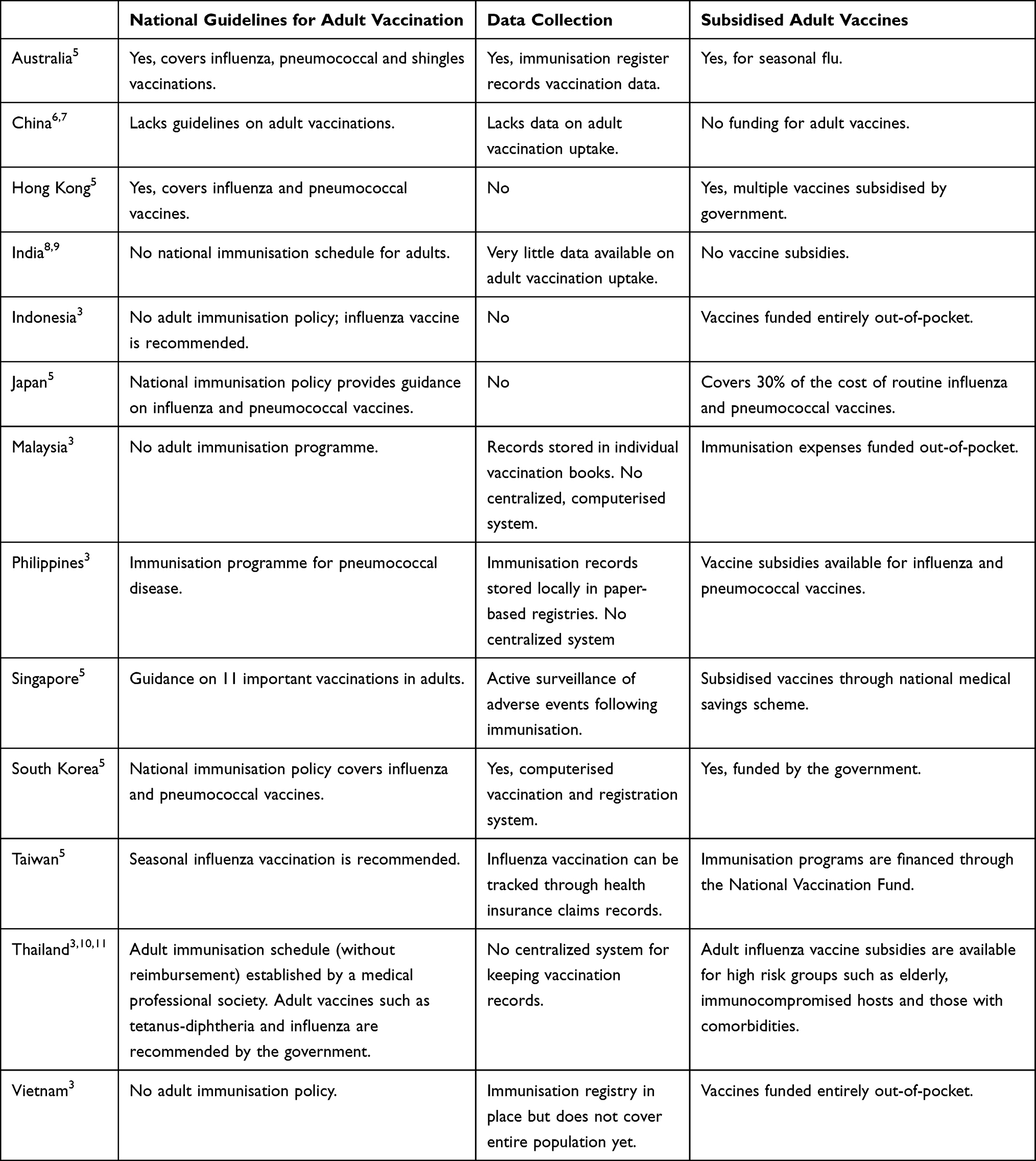 |
Table 1 Summary of Adult Vaccination Policies, Data Surveillance and Vaccine Subsidies in Asia-Pacific |
Australia
The proportion of Australian adults above 60 is expected to rise exponentially to 25% in 2056, with more people in aged care facilities. Australia has a National Immunisation Program (NIP) and a National Immunisation Register, which records and tracks the immunisation status of individuals. The government fully reimburses the annual influenza vaccine, which has a high uptake.3 Other vaccines on the NIP include pneumococcal and Zoster vaccines for specified groups/ages. Coverage is suboptimal for pneumococcal vaccination, and there is only recently a consolidated national database for adult pneumococcal immunisation. Further, multiple changes and the complexity of the national recommended protocol are likely to dissuade pneumococcal vaccination.12 Zoster vaccination rates are also suboptimal, but the addition of the adjuvanted antigen vaccine would likely improve this.
China
China lacks guidelines on adult vaccines. In most areas, influenza and pneumococcal vaccination rates are relatively low, and public awareness of vaccination is insufficient.13 Influenza vaccine is optional and not funded by the government, except in certain cities with higher development.6 A study found a high prevalence of hesitancy towards influenza vaccination among the Chinese elderly, especially well-educated and urban-dwelling respondents.14
Hong Kong
The NIP provides guidance and funds for adult influenza and pneumococcal vaccines for older adults; however, there are no data for adult vaccinations. Free influenza vaccination is provided to the underprivileged elderly through the “care for the Elderly Programme”.3
India
There is no national immunisation schedule for the elderly population in India,8 even though the population over 50 years has quadrupled over the last 50 years and is expected to represent 27% of the projected population in 2036.9
Very little data are available for older adult immunisations and vaccine uptake.15 India accounts for a significant portion of the global VPD burden being the second most populous nation with a prevalence of VPDs that is 2.2–3.4 times higher than the global prevalence. Due to the absence of real-time infectious disease reporting, there is not enough data on the actual burden. The true VPD disease burden is expected to be higher than reported because of poor surveillance networks, under-diagnosis, and under-reporting.9
Adult vaccination guidelines favouring pneumococcal and influenza vaccination have been issued by the Geriatric Society of India, the Association of Physicians of India, the Research Society for Study of Diabetes in India, the Indian Society of Nephrology, and the Indian Medical Association.9 However, these vary, leading to confusion among physicians. Other barriers to adult immunisation include vaccine hesitancy, missed opportunities, cost,16 lack of disease surveillance systems, lower vaccine confidence, and limited access to vaccines.9
A recent study conducted in India estimated that the uptake of influenza, pneumococcal, typhoid and hepatitis B vaccination was less than 2% among adults. Vaccine uptake was higher among males, urban residents, wealthier households, educated, and persons with existing medical conditions.9
Indonesia
Indonesia does not have any national adult immunisation policy. Influenza vaccine is recommended to older adults, adults with underlying chronic diseases, Hajj pilgrims, and healthcare workers but has to be financed out of pocket. The geographically diverse population and fragmented healthcare system make it difficult for older adults to access healthcare and vaccinations. Furthermore, there is a lack of awareness and understanding of vaccines and vaccine-preventable diseases in adults.3 The availability of refrigerators and temperature monitoring equipment to maintain the vaccines was a challenge during the pandemic.17 Cultural and social biases also hamper the COVID-19 vaccination drive. Factors associated with COVID-19 vaccine hesitancy included the old age, having comorbidity, religious prohibitions, not being exposed to information about COVID-19, not trusting that vaccines could prevent COVID-19 infection, and mild-moderate anxiety levels.18
Japan
The NIP guides influenza and pneumococcal vaccines for older adults in Japan, but no vaccination data are collected.3 Vaccination of older adults is plagued by vaccine hesitancy and inefficient public awareness campaigns, especially for influenza and pneumococcal vaccines.19 Despite free vaccines and reduced copayment support, the vaccine coverage for influenza was 50.2%, and the pneumococcal vaccine coverage was 37.8% in 2021.19
Lack of effective communication and dialogue with the target population has contributed to distrust towards vaccination.19 Japanese society is highly apprehensive of vaccination-related health hazards, and immunisation policies have had to be reconsidered due to media reports and lawsuits. There is significant vaccine hesitancy, where people hesitate or refuse to vaccinate themselves or their children. As a result, routine immunisations have suffered, leading to reported VPDs.19
Malaysia
With no adult immunisation programme, the vaccination rates in adults remain low in Malaysia, with less than 2% of the population vaccinated for influenza. The Ministry of Health recommends adult vaccines, but immunisation expenses are financed entirely out-of-pocket. Influenza vaccines are primarily accessed through private healthcare facilities, with only 10% of adult vaccinations administered through public healthcare facilities. The uptake of vaccines is further hampered by vaccine hesitancy and anti-vaccine sentiments fostered by misinformation spread through social media. Perceived harmful effects of vaccines, religious prohibitions and beliefs in the adequacy of traditional complementary and alternative medicines in tackling infectious diseases among the population and even healthcare workers have discouraged vaccination uptake. These perceptions also extend to childhood vaccinations, with a 12.5% prevalence of vaccine hesitancy among urban parents.3 A study attributed vaccine refusal in Malaysia to an interplay of social, cultural and religious perspectives influencing perceived religious prohibition, pseudoscience beliefs, and the usage of Traditional, Complementary and Alternative Medicine.20
Philippines
The Filipino population is relatively young, but the proportion of the elderly is expected to increase significantly in the coming decades. Immunisation rates among older adults depend on the extent of financial coverage. The Expanded Pneumococcal Immunisation Programme was launched in 2016, which provides free pneumococcal vaccines for the elderly. While this has facilitated an adult pneumococcal vaccine coverage rate of 52.9%, the vaccine coverage rate for influenza remains low at 36.3% due to the lack of a comprehensive immunisation policy. Influenza vaccines procured are inadequate to cover the entire older adult population and are provided free only to the indigent older population.3
A study reported low awareness of pneumococcal and influenza vaccines in the Philippines, with better awareness among females, educated urban residents and higher socioeconomic groups.21 Spread of misinformation, vaccine brand hesitancy through social media, and sensationalism in traditional media are also prevalent in the Philippines.22
Singapore
Life expectancy has increased with healthcare infrastructure improvements, and almost 20% of Singaporeans are projected to be 65 years, and above by 2030.23 The National Adult Immunisation Schedule (NAIS) recommends 11 essential vaccinations for adults covered under the medical savings scheme Medisave. There is a push from the government and targeted communications to the public and physicians through awareness campaigns to increase vaccination uptake. Singapore has a good health infrastructure, and mobile vaccination teams were deployed to create easy COVID-19 vaccination access for adults over 60 years.3 Immunisation data are stored centrally and easily accessible for providers and patients through the National Immunisation Register.
South Korea
The NIP covers influenza and pneumococcal vaccination for older adults, and the government provides free vaccines to private and public health clinics. Immunisation is tracked through an automated and standardised vaccination registration and management system.3 The addition of elderly pneumococcal vaccination to the national immunisation program in 2013 increased vaccination from 5% to 57.9% in 20 months without shortage or safety issues.24 There is also a dedicated hotline to answer queries related to vaccination free of charge at any time. South Korea is the only nation from APAC that attained the 75% target of WHO for influenza vaccination in 2019 (at 86%).5
Taiwan
The government funds the seasonal flu vaccines for all adults over 50 years and vulnerable groups under the NIP. The influenza vaccination can be tracked using Taiwan’s National Health insurance claims records. The overall pneumococcal vaccination rate in the elderly increased from <1% in 2007 to almost 30% in 2015 since the pneumococcal vaccine was provided free of cost.25 According to a recent study, older adults who were women, current smokers, or those with low peak expiratory flow are less likely to receive the pneumococcal vaccine.25
Thailand
Thailand’s Immunisation rates remain low, although the Advisory Committee on Immunisation Practice of Thailand has prioritized the seasonal influenza vaccinations for older adults. Though there is no formal adult immunisation schedule, adult influenza vaccines are subsidised through the Expanded Programme on Immunisation (EPI). Influenza vaccination rate in the healthy older adults was around 20% in 2012 but has increased steadily to nearly 30%, with much higher rates in persons with comorbidities.10,11 Pneumococcal vaccines are not included in the NIP and have a coverage of only around 5% in the elderly. However, a limited supply of reimbursed influenza vaccines is available only for a few months, though influenza occurs throughout the year in Thailand.3
Vietnam
Vietnam is one of the fastest ageing populations in Asia. There is a lack of ongoing research into VPD in older adults and information on VPD burden. Since 2019, vaccines have been locally produced in collaboration with the WHO. However, access to vaccines is limited by the low physician-to-population ratio of 0.8 per 1000 persons and low awareness and acceptance of vaccines in the population. With the help of WHO and the Program for Appropriate Technology in Health (PATH), a National Immunisation Information System (NIIS) has been developed to digitise the immunisation database and track immunisation records, vaccine stocks and distribution. However, the NIIS covered less than 25% of the population in 2020, and older adults were yet to be included onto the database. Moreover, the EPI does not cover adult immunisations; hence, these must be financed entirely out-of-pocket.
Challenges for the Utilisation of Vaccines in Older Adults
The reasons and challenges for low vaccination coverage of older adults are many and involve all stakeholders, including the government, research and development, public policy, health infrastructure, physicians in the public and private sectors and individuals.
Governmental Issues
Governments from low- and middle-income nations in the Asia Pacific face challenges in financing sustainable immunisation with domestic resources. Childhood immunisation is given priority and fully subsidised in most Asian Pacific nations. However, adult vaccinations are either partially subsidised or not covered at all.3
Vaccination uptake is hindered by complicated funding and reimbursement policies. For instance, the reimbursement policy for influenza vaccines varies between regions in China, leading to low uptake. The governmental investments towards routine immunisation are low for most governments in APAC and vary across nations, regions and population sizes.3
Many nations lack surveillance systems and data for adult vaccination or disease burden, hampering efforts to collect and interpret information required to develop coherent and meaningful adult immunisation policies.3 Uniform regional guidelines that are updated in a timely manner are also lacking. Nations such as Indonesia and the Philippines are challenged by the transport and delivery of vaccines and healthcare issues due to the geographical variations in healthcare and population distribution.3
Research Issues
Effectively vaccinating older adults has inherent difficulties associated with the physiological changes associated with ageing. These include decreased immunity (immunosenescence), higher prevalence of comorbidities, and a predisposition to developing severe disease. The likelihood of experiencing potentially life-threatening complications of both the vaccine-preventable disease and from the vaccine itself adds some complexities with respect to decisions to vaccinate and overall support of vaccination programs.26 Ageing also reduces the clinical efficacy of vaccines, for example, the effectiveness of standard influenza vaccines was estimated to be only 50% in population, aged 60 years or older.27 Many candidate vaccines have shown immunogenicity and safety but failed to protect older adults in clinical trials.2
As older adults do not form a large proportion of clinical trial subjects, data on vaccine efficacy in older adults and in the presence of chronic diseases are lacking.2 As a result, many healthcare providers hesitate to vaccinate older adults due to a lack of data on the effectiveness of the vaccines.28
There is a need for vaccines with improved efficacy and suitability for older adults, achievable by processes including the use of adjuvants, new vaccines against additional pathogens, universal vaccines targeting variable pathogens, induction of cellular immune responses, mucosal delivery, and the prevention of immunosenescence.2,29
Individual Issues
Older adults and their caretakers are also responsible for accessing the healthcare provided. The cost of vaccines and accessibility are critical issues in many developing nations. Even in places with suitable provisions (including funding) for adult vaccinations, uptake can be poor. This low uptake is attributed to individual biases, lack of information and awareness and misconceptions. The COVID-19 pandemic highlighted the existence of vaccine hesitancy and vaccine apathy in many locations in the APAC region, despite the provision of vaccines free of charge and at the doorstep for older adults in most of the region.
The high costs of vaccines, lack of health insurance coverage and patient unwillingness to pay out-of-pocket for vaccines are significant deterrents to the uptake of vaccines.3 The pay-it-forward intervention effectively increased influenza vaccine uptake and improved community engagement in China.
A lack of awareness of the benefits of adult immunisation, in both patients and healthcare providers is a crucial barrier to the uptake of vaccines, even in regions where the vaccines are free and easily accessible. In Australia, low vaccination rates are attributed to the perceptions in the local population that vaccines are not needed for adults, are not effective and have side effects. Among older adults in Singapore, a perceived lack of vulnerability, trivialisation of influenza and fear of side effects were commonly cited reasons for not taking the vaccines.3
Vaccine Hesitancy and Apathy
“Vaccine hesitancy” refers to delayed acceptance or refusal of vaccines despite their availability. Vaccine hesitancy results from a complex interplay of psychosocial, socio-demographic, contextual, and physical factors. The phenomenon has been seen globally and is not restricted to any specific country, community or religion.30 The reasons for vaccine hesitancy vary across countries based on society’s attitudes, confidence in government and healthcare professionals, the inclusion of ethnic minorities and many other societal issues. A study in Japan attributed vaccine hesitancy to rumours about the vaccine, side effects and risk profile, and the time and cost involved in getting vaccinated.31 Vaccine hesitancy is not a problem that can be solved by vaccine education and awareness alone. Social issues, including distrust in the medical, social and political entities that are promoting the vaccines, also need to be addressed.31 A study evaluating vaccine hesitancy in communities from Asia, Africa and South America during the COVID-19 pandemic identified being Muslim and female as associated with a high risk of vaccine hesitancy.32 A UK survey found that COVID-19 vaccine hesitancy was highest among black, Bangladeshi and Pakistani ethnic populations compared to those with white ethnicity.33 The trust among minority populations is eroded by systemic racism and discrimination, under-representation of minorities in research and clinical trials, and poor experiences in culturally-insensitive systems.33
Understanding the reasons for vaccine hesitancy in the general population can help improve vaccine acceptance.30 Psychosocial interventions are the most effective method to address this issue.26 Psychosocial factors include a lower sense of community responsibility to address disease, higher vaccine risk perceptions, a preference for natural immunity, and concerns about commercial profiteering.26 Religiosity and community beliefs also play an important role in vaccine hesitancy, as was seen with the COVID-19 vaccination programme. Community and religious leaders can help advocate vaccination, particularly among the older population segment.34 It is seen that a significant proportion of individual perceptions are shaped by exposure to misinformation spread through media, the community, and the health system. Social networks also play an increasing role in influencing people in the digital era, including older adults. Political biases, inefficiency and inflexibility of systems also play a role in vaccine brand hesitancy, delays and refusals. Unfortunately, this affects the most vulnerable and marginalised groups.22 Collaborative efforts of governments, health policymakers, social media and communications companies are needed to build trust regarding vaccinations among the general public.35 Vaccine manufacturers and government and health institutions at national and international levels need to propagate and promote beliefs and trust regarding vaccination in the general population.33 Figure 1 outlines a multisectoral approach for building trust to overcome vaccine hesitancy.
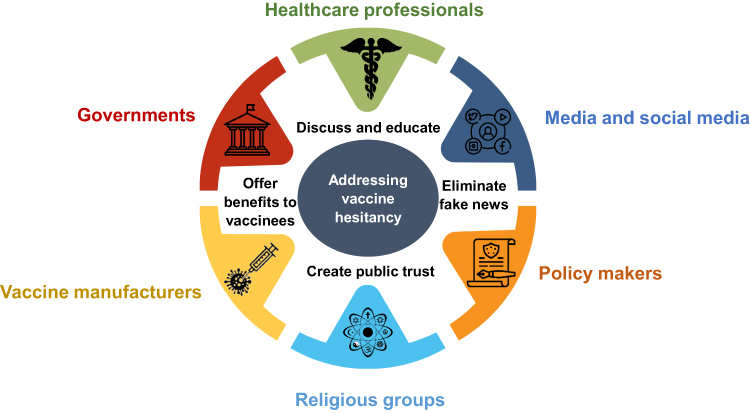 |
Figure 1 Multisectoral approach for building trust to overcome vaccine hesitancy. Notes: Addressing vaccine hesitancy involves building trust between the population, government, and health associations. To overcome distrust and marginalisation, particularly among minorities, a multisectoral approach must be adopted to address vaccine hesitancy. |
Vaccine apathy describes disinterest or slightly negative attitudes towards vaccines or vaccination. A vaccine apathetic population lacks the motivation to receive the vaccine and does not care whether or not they are vaccinated. This differs from vaccine hesitancy, in which people are more reluctant to receive safe and recommended vaccines than apathetic individuals. Recognising these two populations’ differences is essential while developing effective vaccination promotion campaigns.36
To address vaccine hesitancy and apathy, tailored and targeted communications are needed. However, population-wide communication campaigns do not always resonate with older adults. This is particularly true of mass information campaigns that use social media and frequently fail to fully reach the older generation, despite their increasing familiarity with such media. Traditional interventions such as home-based vaccinations, reminder calls and community outreach programmes may be more successful in targeting older adults.3
Drivers for Increasing Vaccination Rates
Vaccination rates in older adults can be improved with targeted interventions by the government, payers, healthcare providers and other stakeholders. While the older generation typically requires more healthcare assistance, they often receive minor health insurance coverage and lack the income to cover healthcare expenses in this region. Consequently, the responsibility for meeting their healthcare needs falls onto individuals, families, and the public health system.3
Government Policies
The highest vaccination rates are seen in regions with a government-driven public health policy directed at older adults. Governments can be convinced to invest in adult vaccination by emphasising the social and economic benefits of a healthy ageing population and reduced disease burden on healthcare and social infrastructures. Government policies such as mandatory vaccination and eligibility for schemes can increase adult vaccination coverage.37
Governments can improve access to vaccination services for adults by making systems less complicated, improving convenience and expanding immunisation services. Leveraging the existing primary healthcare infrastructure and programmes can improve access to adult vaccinations and healthcare.1 Access to vaccination services at community health centres, after-hour clinics or pharmacies and simplifying immunisation schedules and reminder systems can also improve vaccination rates and compliance.3
Improved Awareness in Patient and Healthcare Provider Groups
Improving patient awareness and acceptance can go a long way in increasing adult vaccination rates. In addition, vaccination-related advice or recommendations from national agencies or physician associations are deemed important by the general population.26
Campaigns and awareness programs should focus on the knowledge, attitudes and behaviours of older adults and identify factors that are amenable to change.37 A study in Japan reported that vaccination coverage could be increased by educating the population on personal risk, the severity of influenza illness, and the efficacy of vaccination.38
Health care providers (HCPs), including doctors, nurses, community health workers and pharmacists, are effective sources of information for patients and can help address vaccine hesitancy. However, HCPs differ in their knowledge and attitudes toward adult vaccination, and not all may be motivated to push their patients towards immunisation. A recent study reported that some HCPs carried notions of vaccine-induced influenza, lack of disease risk and poor awareness of the preventative value of vaccination of themselves, as HCPs.3 Studies suggest that the failure of physicians to offer vaccination is a significant missed opportunity to increase adult vaccination.39,40
Improvements in Vaccine Quality
For the successful implementation of immunisation programs, adult vaccines must be both perceived as effective and indeed shown to be so for the public, payers, and health professionals. Improvements in vaccines are needed to address issues of immunosenescence. Strategies include high doses of the antigen and the use of adjuvants. Recombinant influenza, conjugated pneumococcal, and recombinant adjuvanted shingles vaccines have demonstrated improved efficacy and effectiveness in older adults.1 mRNA technology has also increased vaccine efficacy, as seen with some COVID-19 vaccines.41 The development of combination vaccines may also improve uptake.42
Identify and Address Gaps in Coverage
Identification and assessment of gaps in vaccine coverage are crucial to instituting policies and programs to address inequities. National immunisation registries monitor and can assist in managing the performance of immunisation programmes in adults.1 The computerisation of clinical and immunisation registers helps to provide easy access to vaccination data through the ages.28
Life-course immunisation prevents diseases later in life and helps to build herd immunity, to reduce disease impact. Adult and child immunisation programs need to be perceived as essential to preventing infectious diseases in the community and promoting better health for adults.1
Effect of the Pandemic on Adult Vaccination and Lessons Learned
The COVID-19 pandemic reignited interest in vaccination, with many pharmaceutical companies in a race against time for developing vaccine(s) against the COVID-19 virus. Among the population, an increased interest in vaccination and health-seeking behaviour was also observed, especially regarding conditions whose symptoms mimicked COVID-19 infection.43 During the pandemic, there was an increase in interest and demand for influenza and pneumococcal vaccines.43 A study in China observed that high susceptibility to COVID-19 increased the coverage of influenza and pneumonia vaccines.44 Also, the high efficacy of COVID vaccines, including in older adults, reduced concerns about immunosenescence being a phenomenon affecting all older adult vaccines.
A study evaluating the increased uptake of adult pneumococcal vaccine reported that knowledge, performance expectancy, effort expectancy, attitude, and trust were associated with the uptake of vaccines. To increase adult pneumococcal vaccination, experts must provide adequate health education, thus improving knowledge, positive attitude and trust.45
Interestingly, surveillance during the pandemic revealed selective hesitancy towards Chinese-manufactured vaccines in certain regions with public distrust of the national governments and/or of China.46 This sentiment brought forth the role of political factors in addition to efficacy and religious permissibility as drivers of vaccine hesitancy. Studies show that religious concerns motivated 20.8% and 8% of vaccine hesitancy in Malaysia and Indonesia, respectively. There were concerns and certain misgivings in Indonesia regarding the non-halal origins of the COVID-19 vaccine Sinovac developed by a Chinese company. In Thailand, drivers of vaccine hesitancy included low education, lack of confidence in the healthcare system’s ability to treat patients with COVID-19, perceived issues around vaccine manufacturers, being offered a vaccine from an unknown manufacturer, and the low number of daily COVID-19 cases reported.47
In contrast, the Chinese-manufactured vaccines Sinovac and Sinopharm have more appeal than other vaccines among Singaporeans, particularly among older adults. This was due to apprehensions over the newer mRNA-based vaccines, whereas the Chinese-manufactured vaccines are based on established inactivated virus technology. Though Singapore was one of the fastest in the pace of vaccinations, the elder generation (aged 71–75) had poorer vaccination rates, driven partly by scepticism regarding the efficacy or safety of COVID-19 vaccines. A study revealed that respondents who did not intend to vaccinate were less socially integrated, were of lower socioeconomic status, and had one or more chronic conditions.48,49 The COVID-19 Vaccination for the Elderly (COVE) program, a person-centric proactive approach by healthcare workers, addressed vaccine hesitancy in Singapore and helped to increase the COVID-19 vaccination uptake from 84.6% to 96.3% in older adults.50
The pandemic also highlighted the importance of surveillance and emergency preparedness for infectious diseases. Unfortunately, significant gaps in influenza surveillance exist in many low income nations.1
An adequate supply of vaccines is essential for the effectiveness of immunisation programmes. Predictive analytics can help governments gain better clarity around expected vaccine demand. For example, vaccine management analytics have been boosted because of supply issues with COVID-19 vaccines. These models can help nations be more confident about making longer-term commitments and better contracting arrangements for vaccines.3
Building infrastructure and logistics for supply and distribution are also vital. The Asia Pacific includes China and Japan, the second and third largest national economies globally. However, it also includes nine Gavi (The Vaccine Alliance)–eligible nations and regions that meet Gavi low-income eligibility criteria. The region thus represents all stages of vaccine innovation, production, and consumption, along with paradoxical overlaps of reliance on aid for global vaccination programs by nations that also are vaccine exporters. China, India, Indonesia, Vietnam and Korea are home to manufacturers that produce 75% of United Nations (UN) agency-procured vaccine doses.51
In the post-pandemic era healthcare systems in many countries, especially in the developing world, will face continued stress due to limited and stretched resources, and competing priorities. In this regard, successful immunisation of older adults can play a vital role in reducing the burden of care in an already fragile healthcare delivery system.
Recommendations and the Way Ahead
Various strategies, including the Global Strategy and Action Plan on Aging and Health, the Decade of Healthy Aging and the Immunisation Agenda 2030, have called for a life-course approach to immunisation policy. However, many nations still lack policies and funding for the existing vaccines.50 Political support for immunisation can be gathered by articulating an evidence-based narrative on the benefits of adult immunisation to the economy, the fight against non-communicable diseases and antimicrobial resistance, and addressing equity despite gender, medical, social or financial vulnerability.1,50
The International Council on Adult Immunisation (ICAI) has outlined a high-level roadmap to stimulate action, provide policy guidance, and envision a global adult immunisation platform that nations could adapt to fit their local contexts. This Council has highlighted the importance of programs to deliver existing influenza, pneumococcal, herpes zoster vaccines, and future COVID-19 vaccines to over a billion older adults at substantially higher risk of death and disability due to vaccine-preventable diseases.1
To drive the uptake of vaccines, it is crucial to identify and address the gaps in the following:
Monitoring systems to assess disease burden and vaccination uptake.
Uniform guidelines on adult vaccinations, preferably integrated with childhood immunisation to offer life-course immunisation.
Identification of population to target for vaccination and engagement with patient advocacy groups.
Additionally, each country needs to have a national adult immunisation policy complemented by a robust and sustainable implementation plan supported by sufficient resources. Where government subsidies are not possible, regional collaborations could be explored to make vaccines more affordable. Figure 2 illustrates the suggested key steps to optimise adult vaccination in the Asia-Pacific region using an Integrated and multifaceted approach.
 |
Figure 2 Integrated and multifaceted approach for optimising vaccine uptake in older adults. Notes: A successful strategy for increasing vaccine uptake in older adults should involve multiple approaches working together in an integrated and coordinated manner. By combining these through a comprehensive and organised plan, healthcare providers and public health officials can optimize vaccine uptake in older adults and help protect this vulnerable population from vaccine-preventable diseases. |
Conclusion
Some nations in the Asia Pacific region tend to lag behind Western nations in adult immunisation in the areas of the utilization of quality vaccines, financing and/or increasing national commitment to adult immunisation. The coverage of adult vaccination can be improved through strong political will and commitment, collaborative efforts from politicians, policymakers, HCPs and medical associations, non-government organisations, community organisations and academia towards supporting adult immunisations and improving systems, processes and collaboration within the regions and nations.
Acknowledgments
An Asia-Pacific regional meeting on the topic ‘Optimising Vaccine Utilisation in Older Adults in Asia-Pacific’, convened by Janssen Pharmaceuticals was a springboard for subsequent manuscript development by all authors. Editorial and medical writing support was provided by Transform Medical Communications, which was funded by Janssen Pharmaceuticals Asia Pacific. The authors sincerely appreciate the medical writing support provided by Dr Sajita Setia, Executive Director, Transform Medical Communications, Auckland, New Zealand, and Dr Veena Angle, Singapore, on behalf of Transform Medical Communications.
Disclosure
Professor Michael Woodward reports advisory board membership and personal fees from Janssen/Johnson and Johnson, GSK, Merck/MSD, Pfizer, and CSL/Seqirus, during the conduct of the study. The views and opinions expressed in this article are those of the authors and do not represent or reflect in any way the official policy or position of their current or previous employers or collaborators. No author received an honorarium for the preparation of the article. The authors report no other conflicts of interest in this work.
References
1. Privor-Dumm LA, Poland GA, Barratt J, et al. A global agenda for older adult immunization in the COVID-19 era: a roadmap for action. Vaccine. 2021;39(37):5240–5250. doi:10.1016/j.vaccine.2020.06.082
2. Wagner A, Weinberger B. Vaccines to prevent infectious diseases in the older population: immunological challenges and future perspectives. Front Immunol. 2020;11:717.
3. Sachet G, Hardesty C, Aizan T, et al. The decade of healthy ageing in ASEAN: role of life-course immunisation; 2021. Available from: https://www.eu-asean.eu/wp-content/uploads/2022/02/The-Decade-of-Healthy-Ageing-in-ASEAN-Role-of-Life-course-Immunisation-2021.pdf.
4. Litt J, Booy R, Bourke D, et al. Early impact of the Australian national shingles vaccination program with the herpes zoster live attenuated vaccine. Hum Vaccin Immunother. 2020;16(12):3081–3089. doi:10.1080/21645515.2020.1754702
5. Seth A, Pangestu T. Promoting older adults immunization: a pathway to healthy aging in the Asia Pacific; 2021. Available from: https://medicine.nus.edu.sg/apic/wp-content/uploads/sites/28/2022/06/APIC_Policy_Brief_Life_Course_Immunisation_Final_June-2022-1.pdf.
6. Jiang X, Shang X, Lin J, Zhao Y, Wang W, Qiu Y. Impacts of free vaccination policy and associated factors on influenza vaccination behavior of the elderly in China: a quasi-experimental study. Vaccine. 2021;39(5):846–852. doi:10.1016/j.vaccine.2020.12.040
7. Bai X, Chen L, Liu X, et al. Adult hepatitis B virus vaccination coverage in China from 2011 to 2021: a systematic review. Vaccines. 2022;10(6). doi:10.3390/vaccines10060900
8. Verma R, Khanna P, Chawla S. Vaccines for the elderly need to be introduced into the immunization program in India. Hum Vaccin Immunother. 2014;10(8):2468–2470. doi:10.4161/hv.29254
9. Vora A, Di Pasquale A, Kolhapure S, Agrawal A. Vaccination in older adults: an underutilized opportunity to promote healthy aging in India. Drugs Aging. 2021;38(6):469–479. doi:10.1007/s40266-021-00864-4
10. Cowling BJ, Caini S, Chotpitayasunondh T, et al. Influenza in the Asia-Pacific region: findings and recommendations from the Global Influenza Initiative. Vaccine. 2017;35(6):856–864. doi:10.1016/j.vaccine.2016.12.064
11. Owusu JT, Prapasiri P, Ditsungnoen D, et al. Seasonal influenza vaccine coverage among high-risk populations in Thailand, 2010–2012. Vaccine. 2015;33(5):742–747. doi:10.1016/j.vaccine.2014.10.029
12. Menzies R, Stein AN, Booy R, Van Buynder PG, Litt J, Cripps AW. The impact of the changing pneumococcal national immunisation program among older Australians. Vaccine. 2021;39(4):720–728. doi:10.1016/j.vaccine.2020.12.025
13. Chen Q, Wang L, Xie M, Li X; Recommendations for Influenza SpViEPiCWGGRG, Chinese Society of G. Recommendations for influenza and Streptococcus pneumoniae vaccination in elderly people in China. Aging Med. 2020;3(1):4–14. doi:10.1002/agm2.12102
14. Hou Z, Guo J, Lai X, et al. Influenza vaccination hesitancy and its determinants among elderly in China: a national cross-sectional study. Vaccine. 2022;40(33):4806–4815. doi:10.1016/j.vaccine.2022.06.063
15. Krishnan A, Dar L, Amarchand R, et al. Cohort profile: Indian Network of Population-based surveillance platforms for Influenza and Other Respiratory Viruses among the Elderly (INSPIRE). BMJ Open. 2021;11(10):e052473. doi:10.1136/bmjopen-2021-052473
16. Dash R, Agrawal A, Nagvekar V, et al. Towards adult vaccination in India: a narrative literature review. Hum Vaccin Immunother. 2020;16(4):991–1001. doi:10.1080/21645515.2019.1682842
17. Zahra. The availability of vaccines in Indonesia is adequate, but the availability of cold chain infrastructure facilities is still experiencing obstacles; 2021. Available from: https://feb.ugm.ac.id/en/news/3494-The-availability-of-vaccines-in-indonesia-is-adequate-but-The-availability-of-cold-chain-infrastructure-facilities-is-still-experiencing-obstacles.
18. Utami A, Margawati A, Pramono D, Nugraheni A, Pramudo SG. Determinant factors of COVID-19 vaccine hesitancy among adult and elderly population in Central Java, Indonesia. Patient Prefer Adherence. 2022;16:1559–1570. doi:10.2147/PPA.S365663
19. Vaccinations; 2021. Available from: http://japanhpn.org/en/vaccinations-2/.
20. Wong LP, Wong PF, AbuBakar S. Vaccine hesitancy and the resurgence of vaccine preventable diseases: the way forward for Malaysia, a Southeast Asian country. Hum Vaccin Immunother. 2020;16(7):1511–1520. doi:10.1080/21645515.2019.1706935
21. Cruz GT, Laguna EP, Paguirigan MRB, et al. Vaccinating the most vulnerable group in the time of pandemic: insights from a national survey of older people (UPPI/DRDF Research Brief No. 9); 2021. Available from: https://www.uppi.upd.edu.ph/research/covid-19/rb9.
22. Amit AML, Pepito VCF, Sumpaico-Tanchanco L, Dayrit MM. COVID-19 vaccine brand hesitancy and other challenges to vaccination in the Philippines. PLOS Glob Public Health. 2022;2(1):e0000165. doi:10.1371/journal.pgph.0000165
23. Nguyen MH, Li Chen L, Lim KW, Chang WT, Mamun K. Vaccination in older adults in Singapore: a summary of recent literature. Proceed Singapore Healthc. 2015;24(2):94–102. doi:10.1177/201010581502400205
24. Yang TU, Kim E, Park Y-J, et al. Successful introduction of an underutilized elderly pneumococcal vaccine in a national immunization program by integrating the pre-existing public health infrastructure. Vaccine. 2016;34(13):1623–1629. doi:10.1016/j.vaccine.2016.01.043
25. Chen CH, Wu MS, Wu IC. Vaccination coverage and associated factors for receipt of the 23-valent pneumococcal polysaccharide vaccine in Taiwan: a nation-wide community-based study. Medicine. 2018;97(5):e9773. doi:10.1097/MD.0000000000009773
26. Nicholls LAB, Gallant AJ, Cogan N, Rasmussen S, Young D, Williams L. Older adults’ vaccine hesitancy: psychosocial factors associated with influenza, pneumococcal, and shingles vaccine uptake. Vaccine. 2021;39(26):3520–3527. doi:10.1016/j.vaccine.2021.04.062
27. Govaert TME, Thijs CT, Masurel N, Sprenger MJW, Dinant GJ, Knottnerus JA. The efficacy of influenza vaccination in elderly individuals: a randomized double-blind placebo-controlled trial. JAMA. 1994;272(21):1661–1665. doi:10.1001/jama.1994.03520210045030
28. Raina MacIntyre C, Menzies R, Kpozehouen E, et al. Equity in disease prevention: vaccines for the older adults – a national workshop, Australia 2014. Vaccine. 2016;34(46):5463–5469. doi:10.1016/j.vaccine.2016.09.039
29. Woodward M. Immunisation of older people. J Pharm Pract Res. 2012;42(4):316–322. doi:10.1002/j.2055-2335.2012.tb00197.x
30. Dhama K, Sharun K, Tiwari R, et al. COVID-19 vaccine hesitancy – reasons and solutions to achieve a successful global vaccination campaign to tackle the ongoing pandemic. Hum Vaccin Immunother. 2021;17(10):3495–3499. doi:10.1080/21645515.2021.1926183
31. Hosoda M. Vaccine hesitancy in Japan: from a perspective on medical uncertainty and trans-scientific theory [version 2; peer review: 2 approved, 1 approved with reservations]. F1000Research. 2023;11(1103):1103. doi:10.12688/f1000research.125159.2
32. Harapan H, Anwar S, Yufika A, et al. Vaccine hesitancy among communities in ten countries in Asia, Africa, and South America during the COVID-19 pandemic. Pathog Glob Health. 2022;116(4):236–243. doi:10.1080/20477724.2021.2011580
33. Razai MS, Osama T, McKechnie DGJ, Majeed A. Covid-19 vaccine hesitancy among ethnic minority groups. BMJ. 2021;372:n513. doi:10.1136/bmj.n513
34. Garcia LL, Yap JFC. The role of religiosity in COVID-19 vaccine hesitancy. J Public Health. 2021;43(3):e529–e30. doi:10.1093/pubmed/fdab192
35. Sallam M. COVID-19 vaccine hesitancy worldwide: a concise systematic review of vaccine acceptance rates. Vaccines. 2021;9(2):160. doi:10.3390/vaccines9020160
36. Vaccine apathy: status, challenges, and prospects; 2022. Available from: https://www.frontiersin.org/research-topics/41534/vaccine-apathy-status-challenges-and-prospects#overview.
37. Barratt DJ, Beckett MR, Acton MM, Sebastian MS, Nguyen MW. Adult Vaccination in the Asia Pacific: mobilizing policy and practice knowledge; 2019. Available from: https://ifa.ngo/wp-content/uploads/2019/10/Adult-Vaccination-in-The-Asia-Pacific-%E2%80%93-Mobilizing-Policy-and-Practice-Knowledge.pdf.
38. Matsui D, Shigeta M, Ozasa K, Kuriyama N, Watanabe I, Watanabe Y. Factors associated with influenza vaccination status of residents of a rural community in Japan. BMC Public Health. 2011;11(1):149. doi:10.1186/1471-2458-11-149
39. Liu S, Xu E, Liu Y, et al. Factors associated with pneumococcal vaccination among an urban elderly population in China. Hum Vaccin Immunother. 2014;10(10):2994–2999. doi:10.4161/21645515.2014.972155
40. Jiang M, Li P, Yao X, et al. Preference of influenza vaccination among the elderly population in Shaanxi province, China. Hum Vaccin Immunother. 2021;17(9):3119–3125. doi:10.1080/21645515.2021.1913029
41. Melo A, de Macêdo LS, Invenção M, et al. Third-generation vaccines: features of nucleic acid vaccines and strategies to improve their efficiency. Genes. 2022;13(12):2287. doi:10.3390/genes13122287
42. Skibinski DA, Baudner BC, Singh M, O’Hagan DT. Combination vaccines. J Glob Infect Dis. 2011;3(1):63–72. doi:10.4103/0974-777X.77298
43. Paguio JA, Yao JS, Dee EC. Silver lining of COVID-19: heightened global interest in pneumococcal and influenza vaccines, an infodemiology study. Vaccine. 2020;38(34):5430–5435. doi:10.1016/j.vaccine.2020.06.069
44. Gong L, Zhang X, Qu Z, et al. Public interest in distribution and determinants of influenza and pneumonia vaccination during the COVID-19 pandemic: an infodemiology and cross-sectional study from China. Vaccines. 2021;9:1329. doi:10.3390/vaccines9111329
45. Zhou M, Zhan J, Kong N, Campy KS, Chen Y. Factors associated with intention to uptake pneumococcal vaccines among Chinese elderly aged 60 years and older during the early stage of COVID-19 pandemic. Psychol Health Med. 2022;27(1):91–105. doi:10.1080/13548506.2021.1905862
46. Zaini K, Ha HT. Understanding the selective hesitancy towards Chinese vaccines in Southeast Asia; 2021. Available from: https://www.iseas.edu.sg/articles-commentaries/iseas-perspective/2021-115-understanding-The-selective-hesitancy-towards-chinese-vaccines-in-southeast-asia-by-khairulanwar-zaini-and-hoang-thi-ha/.
47. Thanapluetiwong S, Chansirikarnjana S, Sriwannopas O, Assavapokee T, Ittasakul P. Factors associated with COVID-19 vaccine hesitancy in Thai seniors. Patient Prefer Adherence. 2021;15:2389–2403. doi:10.2147/PPA.S334757
48. Singapore’s older adults resist COVID-19 vaccinations; 2021. Available from: https://news.smu.edu.sg/news/2021/07/06/singapores-older-adults-resist-covid-19-vaccinations.
49. Ang LW, Cutter J, James L, Goh KT. Factors associated with influenza vaccine uptake in older adults living in the community in Singapore. Epidemiol Infect. 2017;145(4):775–786. doi:10.1017/S0950268816002491
50. Moosa AS, Wee YMS, Jaw MH, et al. A multidisciplinary effort to increase COVID-19 vaccination among the older adults. Front Public Health. 2022;10:904161. doi:10.3389/fpubh.2022.904161
51. Tsai TF, Rao RD, Xu ZY. 75 - immunization in the Asia-Pacific region. In: Plotkin SA, Orenstein WA, Offit PA, Edwards KM, editors. Plotkin’s Vaccines.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.