")
Back to Journals » Clinical Interventions in Aging » Volume 14
Addition Of Sauce Enhances Finger-Snack Intake Among Japanese Elderly People With Dementia
Authors Kimura A , Yamaguchi K , Tohara H , Sato Y, Sawada N, Nakagawa Y, Matsuda Y, Inoue M, Tamaki K
Received 2 August 2019
Accepted for publication 30 October 2019
Published 14 November 2019 Volume 2019:14 Pages 2031—2040
DOI https://doi.org/10.2147/CIA.S225815
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Atsushi Kimura,1 Kohei Yamaguchi,2,3 Haruka Tohara,3 Yusuke Sato,4 Naoko Sawada,4 Yasuhide Nakagawa,4 Yukako Matsuda,2,5 Motoharu Inoue,2,5 Kazuhiro Tamaki2,4
1College of Risk Management, Nihon University, Setagaya-ku, Tokyo, Japan; 2Dentistry Nanohana Clinic, Medical Corporation Kanjinkai, Nishitama-gun, Tokyo, Japan; 3Department of Gerodontology and Oral Rehabilitation, Tokyo Medical and Dental University, Bunkyo-ku, Tokyo, Japan; 4Geriatric Health Services Facility Nanohana, Medical Corporation Kanjinkai, Nishitama-gun, Tokyo, Japan; 5Department of Dysphasia Rehabilitation, Nihon University of Dentistry, Chiyoda-Ku, Tokyo, Japan
Correspondence: Atsushi Kimura
College of Risk Management, Nihon University, 3-34-1 Shimouma, Setagaya-ku, Tokyo 154-8513, Japan
Tel +81 3 6453 1600
Fax +81 3 6453 1630
Email [email protected]
Kazuhiro Tamaki
Geriatric Health Services Facility Nanohana, Medical Corporation Kanjinkai, 454 Tonogaya, Mizuho-machi, Nishitama-gun, Tokyo 190-1212, Japan
Tel +81 42 568 5111
Fax +81 42 568 5127
Email [email protected]
Purpose: The previous study demonstrated that the addition of a sauce is an effective means of influencing the consumption of finger foods among French elderly people with dementia. However, it is unclear the relative importance of low-level sensory factors such as flavor and a semi-solid nature and high-level cognitive factors such as memory stimulation and familiarity to the effect of the addition of sauce on food intake. The present study investigated whether the addition of sauce affects finger-snack intake among Japanese elderly people with dementia who were not familiar with sauce dipping.
Patients And Methods: A total of 21 patients with dementia who were recruited in a nursing home in Tokyo received a plate of cut baumkuchen (a very thinly layered German roll cake), which had pieces of baumkuchen both with and without sauce, at their afternoon snack time. The amount of food intake and the first choice between options were measured for each participant. We used chocolate (in Experiment 1, n = 21) and agave (Experiment 2, n =14) syrups as sauce samples.
Results: Results of both experiments demonstrate that snack consumption was greater for the with-sauce options than for the without-sauce options. A 90.5% of the participants in Experiment 1 and 64.3% of participants in Experiment 2 ate more snacks with sauce than without sauce.
Conclusion: These findings imply that low-level sensory factors such as flavor and a semi-solid nature contribute relatively more strongly to the enhancement of food consumption with the addition of sauce than do high-level cognitive factors such as memory stimulation and familiarity, because Japanese elderly people are not always familiar with the custom of wiping up the sauce with food.
Keywords: food consumption, dementia, under nutrition, food improvement, sauce
Introduction
Dementia is a disorder where a significant decline from one’s previous level of cognition causes interference in occupational, domestic, or social functioning. It is characterized by global cognitive impairment with a decline in memory and at least in one other cognitive domain, such as language, visuospatial function or executive function.1,2 Dementia is one of the most significant diseases of aging, and it is estimated that more than 46 million people are currently living with dementia worldwide; without a way to stop or slow its progression, there will be a tripling of this number to more than 131 million by 2050.3,4 Most dementia in the elderly is caused by some degree of neurodegeneration. Some common degenerative dementia in the elderly are Alzheimer’s disease, dementia with Lewy bodies, frontotemporal lobe degeneration and Parkinson’s disease.1
Weight loss and under-nutrition are common problems with dementia. Because dementia leads to both cognitive and physical decline, nutrition is frequently impaired in elderly people with dementia.5–7 As dementia progresses, a decline in cognition may cause individuals to become unable to recognize and communicate hunger and thirst. They may forget to eat or forget how to eat, lose the ability to recognize food items, and lose the ability to concentrate during mealtimes.5,8,9 In addition, physical decline, such as loss of sensory acuity with aging and disease, may lead to a decline in the pleasantness of the taste and smell of foods. Sensory loss which influences the appeal of foods may reduce interest in food.10,11 These cognitive and physical factors can result in a reduction of the amount of food consumed, and inadequate oral intake can lead to impaired swallowing (dysphasia), which can lead to aspiration pneumonia.12
Various interventions have been developed in order to improve food intake in elderly people with dementia. The approaches of these interventions are broadly categorized into the following types: food improvement, nutritional supplements, feeding assistance, meal service delivery style, staff training and dining environment.5,7,13,14
With respect to the food improvement approach, Pouyet et al15 investigated the effects of three factors, including the addition of a sauce, change in shape, and color contrast enhancement, on the consumption of finger foods in elderly Alzheimer’s disease patients living in nursing homes in France. Their results demonstrated that the addition of a sauce is an effective means of influencing first choice and total consumption of finger foods, while also enhancing color contrast by creating two layers. Across four sessions, the finger foods with a sauce were more frequently chosen first and more often consumed than those without sauce. Pouyet et al discussed two possible explanations for why the addition of sauce increased the attractiveness of finger foods: one was derived from low-level sensory factors and another was derived from high-level cognitive factors. One possible explanation for their results lies in the sensory appeal of adding sauce to food. The addition of a sauce could contribute to sensory attractiveness because it influences the taste and flavor of food and produces or enhances the visual contrast between the food and the dish. Such sensory appeal may compensate for sensory losses suffered by elderly people with dementia. A sauce was also identified as a way to moisten the foods, and thus might facilitate chewing and swallowing and aid in the passage of foods through the digestive system.16,17 Another possible explanation for their results lies in high-level cognitive factors such as long-term memory. The presence of a sauce may seem to be an important element because older generations of French people are used to eating dishes that include sauces. Indeed, their participants were suffering from Alzheimer’s disease, but nevertheless retained the habit of wiping up the sauce with the finger foods. These results suggest that the addition of a sauce could trigger memory stimulation in elderly people with dementia. It is widely known that familiarity is a critical factor in food choice and preference,18–21 and the addition of a sauce can enhance the familiarity of food.22
While both low-level sensory factors and high-level cognitive factors contribute to food attractiveness and consumption in elderly people with dementia,15 it would be worthwhile to explore the relative importance of those sensory and cognitive factors to the effect of the addition of sauce on food intake because this knowledge may be useful when considering the effectiveness of adding sauces to daily meal preparations for elderly people with dementia; which is to say, is the addition of sauce on food also effective for elderly people with dementia in countries where the elderly may not be familiar with sauce dipping?
Here, we explored whether the addition of a sauce affects finger-snack intake among Japanese elderly people with dementia. Compared to France and other Western countries, wiping up the sauce with food may not be common among elderly people in Japan. Thus, if the addition of sauce also enhances food intake among elderly people with dementia in Japan, it could be thought that low-level sensory factors have a stronger contribution to the addition-of-sauce effect than do high-level cognitive factors such as memory stimulation. In the present study, we used a finger snack rather than the finger foods used in Pouyet et al15 because finger snacks are commonly consumed by nursing-home residents in Japan while finger foods (i.e., non-snack foods eaten with one’s fingers) are not. Furthermore, sweet snacks are considered a potential tool for nutritional intervention with elderly people with dementia because they tend to prefer sweet foods.23–25
The present study consisted of two experiments. In Experiment 1, we used paired comparison tests to compare participants’ choices and consumption rates of a finger snack (pieces of cut baumkuchen, which is a thinly layered German roll cake) with chocolate sauce and without sauce in real-life snack-time situations. We used a chocolate sauce because it is a typical sauce for sweets and has a color (dark brown) that has a high visual contrast with the light color of the baumkuchen and the white plate.
In Experiment 2, we used paired comparison tests, as in Experiment 1, to compare participants’ choices and consumption rates of a finger snack (pieces of cut baumkuchen) with agave sauce and without sauce. We used an agave sauce because it has a color (pale yellow) with a low visual contrast with the baumkuchen and the white plate while its sweetness is similar to that of chocolate sauce. By comparing the results between Experiments 1 and 2, we explored whether the addition of a sauce with a highly contrasting color is more effective for enhancing food attractiveness than the addition of a sauce with a less contrasting color.
Materials And Methods
Experiment 1
Design
Experiment 1 was based on a within-subject factor design (with and without chocolate sauce) with participant snack consumption and the type of snack first chosen as dependent variables.
Participants
Twenty-one participants (14 females and 7 males) who had been diagnosed with dementia were recruited for this study, with ages from 73 to 93 years (average age: 84.0±6.1 years). Their cognitive abilities were measured using the Revised Hasegawa’s Dementia Scale (HDS-R), which is widely employed to screen for dementia as well as the Mini-Mental State Examination (MMSE). Participants’ HDS-R scores ranged from 0 (cognition severely impaired) to 17 (cognition moderately impaired). They were not allergic or intolerant to any of the foods provided in this study. They were all recruited in a nursing home in Tokyo, Japan. Their swallowing functions were evaluated by dentists and there were no significant concerns regarding chewing and swallowing abilities. Participants’ BMI ranged from 15.1 kg/m2 to 24.1 kg/m2 with a mean BMI of 19.8 kg/m2 (SD = 2.5). The research followed the tenets of the Declaration of Helsinki. Written family consent was obtained for each participant prior to the experiments. The study was approved by the institutional ethics committee of the Geriatric Health Services Facility Nanohana, Tokyo, Japan.
Food Samples
The finger snack used in this study was cut portions of baumkuchen (Mujirushi Ryohin Atsugiri baum). A large piece of baumkuchen was cut into smaller pieces weighing about 7.8 g each. The sauce used in this experiment was chocolate syrup (Hershey’s chocolate syrup). Details of all food samples are given in Table 1. Each participant was given one white plate with six separate areas, which contained three pieces of cut baumkuchen with sauce and three pieces without sauce (2 × 3 finger snacks, Figure 1A). Additional snacks were also prepared for any participant who might request more. There were no participants who indicated a strong dislike for baumkuchen.
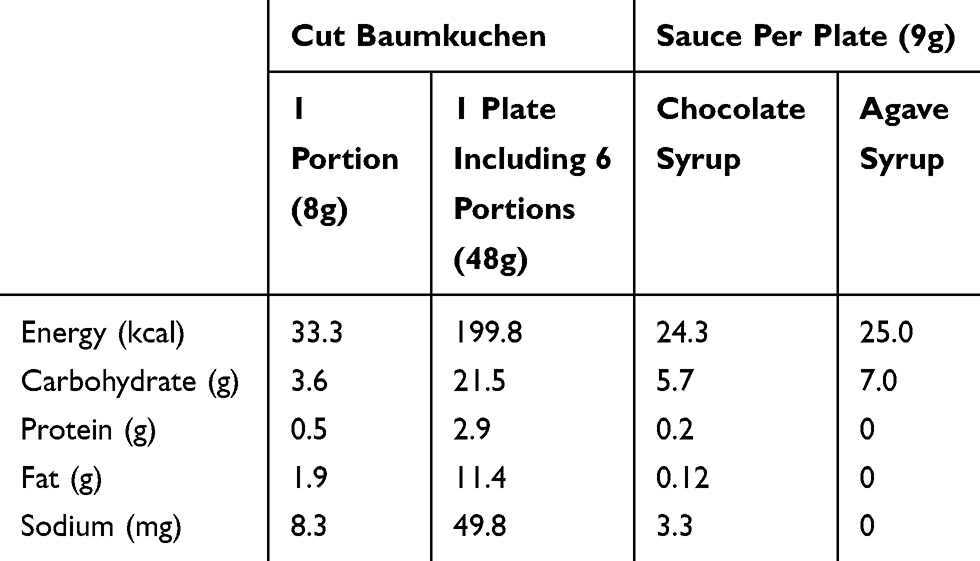 |
Table 1 Nutritional Details Of Food Samples Used In This Study |
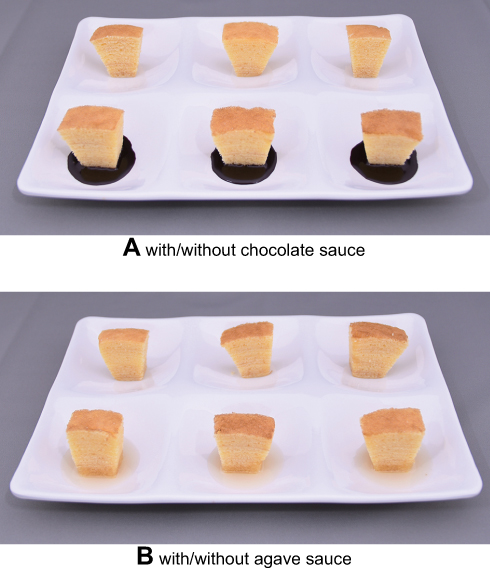 |
Figure 1 Food samples used in this study. |
Procedure
The study session was conducted in a nursing home during the afternoon snack time, from 14:30 to 15:00 hrs. Staff members accompanied each participant to her/his own chair or wheelchair space in the dining room. After that, a plate of snacks containing three pieces of baumkuchen with sauce and three pieces without sauce and a cup of tea were put in front of each participant. Which snacks, with or without sauce, were oriented closest to the participant was counterbalanced among participants. The care staff informed the participants that they could use their fingers to eat. If a participant refused to taste a finger snack, the staff removed the plate and offered an ordinary snack of the day. If a participant requested only pieces without sauce, the staff served 6 pieces all without sauce. If a participant finished her/his plate and asked for more snacks, the care staff could supply one more plate of snacks. Thus, each participant could consume a maximum of 12 pieces of baumkuchen (with the standard consumption choices being 6 with and 6 without sauce). Once the participant no longer wanted any more snacks, the care staff removed the plate. The remainder of snack time did not change from the usual program.
Following Pouyet et al,15 the care staff were asked to complete a questionnaire on how the participants behaved during snack time, including their first choice and their snack consumption. In the first-choice section of the questionnaire, the care staff were asked to answer which type of snack the participant put in her/his mouth first (with or without sauce). In the snack consumption section of the questionnaire, the care staff were asked to record the number of each type of finger snack left on the plate by the participant. If a participant spontaneously dipped any of her/his snacks without sauce in the remaining sauce and ate them, it was counted as with sauce. The care staff were also asked to note if participants requested additional finger snacks and anything else they noticed.
Data Analyses
For each participant, the consumption of snacks with and without sauce was measured based on the number of finger snacks given to them. A finger snack left unfinished on a plate was counted as half a finger snack having been consumed. To determine whether the addition of sauce affected finger-snack intake, a paired t-test with the addition of sauce on finger-snack consumption was performed.
We also calculated how many people chose snacks with sauce first during the experimental session. The probability that a snack with or without sauce would be chosen first most frequently was calculated using the binomial test with a two-sided hypothesis.
Experiment 2
Design
Experiment 2 was based on a within-subject factor design (with and without agave sauce) with participant snack consumption and the type of snack first chosen as dependent variables.
Participants
Fourteen participants (9 females and 5 males) who had been diagnosed with dementia were recruited for this study, with ages from 73 to 93 years (average age: 82.9±6.6 years). Participants’ HDS-R scores ranged from 0 (cognition severely impaired) to 24 (roughly normal cognition). Participants’ BMI ranged from 15.1 kg/m2 to 22.0 kg/m2 with a mean BMI of 19.3 kg/m2 (SD = 2.3). All of them had participated in Experiment 1 at least 1 month earlier.
Food Samples
The finger snack used in this study was almost the same as that used in Experiment 1, but had a different type of sauce (Figure 1B). The sauce used in this experiment was an agave syrup (Maya Gold Organic agave syrup). Details of all food samples are given in Table 1.
Procedure
The overall procedure for Experiment 2 was identical to that for Experiment 1.
Data Analyses
Data analysis for snack consumption and the first choice was identical to that of Experiment 1. In order to determine whether the type of sauce affected finger-snack intake, a paired t-test with the type of sauce on snack consumption was performed using the data of fourteen participants who participated in both Experiments 1 and 2.
Results
Experiment 1
Snack Consumption
Figure 2 shows snack intake in the presence or absence of sauce. The mean amount of snacks with chocolate sauce consumed was 7.8 pieces (SD = 2.9). This is 82.8% of the mean total amount (9.4 pieces; SD = 3.0) of snacks consumed. In this experiment, 90.5% of the participants ate more snacks with sauce than without sauce and 81.0% of them spontaneously dipped their snacks without sauce in the remaining sauce and ate them. The mean finger-snack intake was greater with sauce than without sauce, t (20) = 8.3, p < 0.001, d = 2.6. Nineteen of twenty-one participants exhibited greater intake of snacks with sauce than without sauce, while two participants had equal consumption.
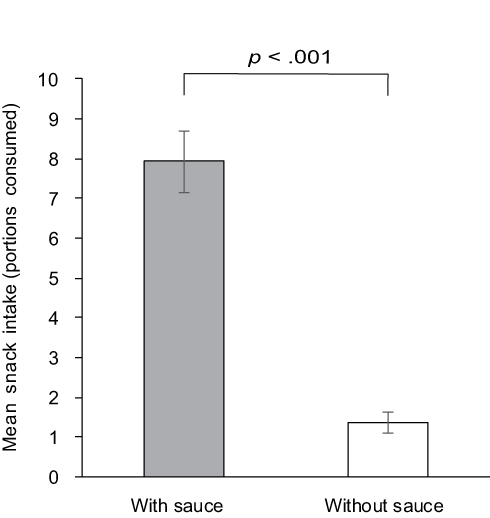 |
Figure 2 Mean snack intake in Experiment 1. |
In order to clarify the relationship between the cognitive status of a participant and the selection rate of snacks with sauce chosen, we calculated the correlation coefficient between the HDS-R score and the selection rate of snacks with sauce (this is calculated by the amount of snacks with sauce consumed/total amount of snacks consumed). The results showed that there was no significant correlation between HDS-R scores and the selection rate of snacks with sauce (r = 0.21, t (19) = 0.9, n.s.).
First Choice
The results of a binominal test showed that neither snack (with or without sauce) was chosen first significantly more often than the other (33.3% for snacks with sauce, 66.7% for snacks without sauce, p = 0.189).
Although the position of sauce/no-sauce snacks on the plate was counterbalanced across participants, the care staff reported that many participants took their first snack from the front side (oriented closer to the participant) of their plates regardless of whether or not it had sauce. In order to confirm these observations, we performed an additional binominal test to examine whether the position of the snacks (front side (closer to the participant) or back side) affected the first choice of snacks consumed. Results showed that participants significantly chose snacks from the front side first more frequently than from the back side (76.2% for snacks on the front side, 23.8% for snacks on the back side, p = 0.027; Table 2).
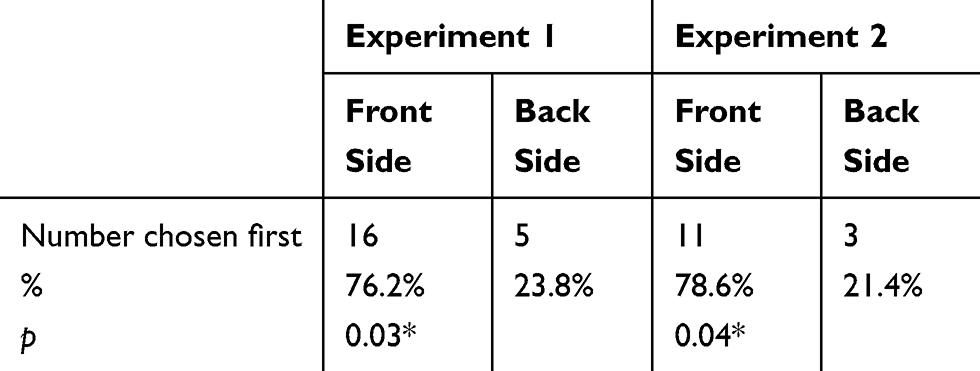 |
Table 2 Relationship Between The Position Of Snacks On A Plate And Participant’s First Choice In Snack Intake |
Experiment 2
Snack Consumption
Figure 3 shows snack intake in the presence or absence of sauce. The mean amount of snacks with agave sauce (low visual contrast) consumed was 6.9 pieces (SD = 2.2). This is 66.9% of the mean total amount (10.4 pieces; SD = 2.6) of snacks consumed. In this experiment, 64.3% of the participants ate more snacks with sauce than without sauce and 50.0% of the participants spontaneously dipped their snacks without sauce in the remaining sauce and ate them. The mean finger-snack intake was greater with sauce than without sauce, t (13) = 3.5, p < 0.001, d = 1.4. Nine of fourteen participants exhibited greater intake of snacks with sauce than without sauce, while five participants had equal intake.
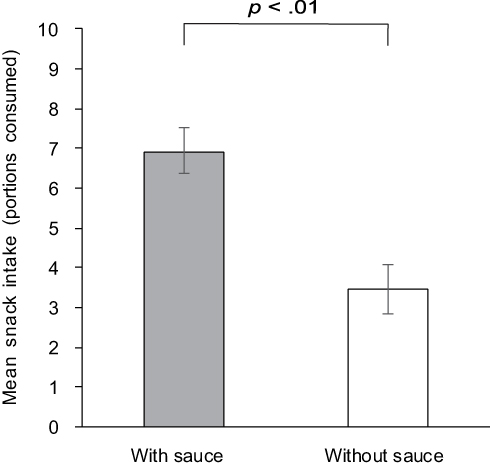 |
Figure 3 Mean snack intake in Experiment 2. |
As with Experiment 1, the correlation coefficient between the HDS-R scores and the selection rate of snacks with sauce was calculated. The results showed that there was no significant correlation between HDS-R scores and the selection rate of snacks with sauce (r = 0.14, t (12) = 0.5, n.s.).
First Choice
The results of a binominal showed that neither snack (with or without sauce) was chosen first significantly more often than the other (35.7% for snacks with sauce, 64.3% for snacks without sauce, p = 0.607). However, the results of an additional binominal test which explored whether the position of snacks (front side (closer to participants) or back side) affected the first choice showed that participants tended to choose snacks from the front side first more frequently than those from the back side (a marginal significance: 78.6% for snacks on the front side, 21.4% for snacks on the back side, p = 0.057; Table 2).
Comparison Of The Snack Intake Between Chocolate And Agave Sauce
Table 3 shows the amount of snack intake in the presence of chocolate or agave sauce. The mean finger-snack intake was greater with chocolate sauce than with agave sauce, t (13) = 3.1, p < 0.01, d = 1.2. The total amount of snacks consumed, including snacks with and without sauce, did not differ significantly between experimental sessions (t (13) = 0.1, n.s.; Table 3).
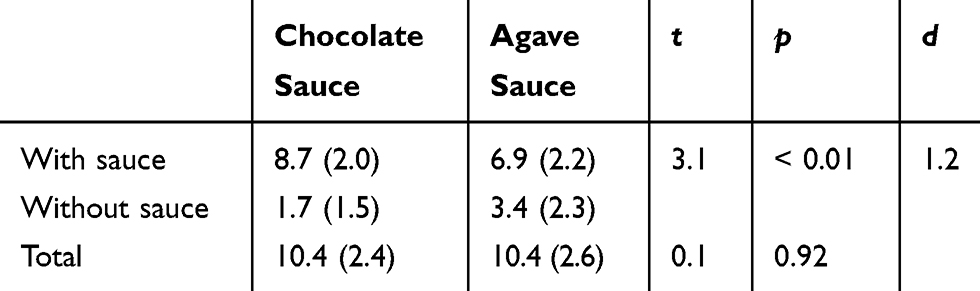 |
Table 3 Comparison Of The Mean Number Of Snacks Consumed (SD) Between Chocolate And Agave Sauces |
Discussion
The main objective of the current study was to examine whether the addition of sauce affects finger-snack intake among Japanese elderly people with dementia. Results of both experiments conducted in this study demonstrate that snack consumption was greater for the with-sauce options than for the without-sauce options among Japanese elderly people with dementia. These results are consistent with Pouyet et al,15 who showed that French elderly people with Alzheimer’s disease consumed more finger foods with a sauce than without sauce. The present findings imply that low-level sensory factors have a relatively stronger contribution to the enhancement of food consumption with the addition of sauce than do high-level cognitive factors because Japanese elderly people are not always accustomed to wiping up the sauce with food. While, to the best of our knowledge, there is no custom of eating baumkuchen with sauce in Japan, we obtained no direct measure of participants’ familiarity with or habit of wiping up the sauce with food, so we cannot be certain whether eating snacks with sauce was unfamiliar to each participant. Some participants spontaneously reported that they had never eaten such a delicious snack after the experiment, but such comments are only qualitative introspections of participants and are not quantitative. This prevented us from precisely determining which factors led to the current results. The present results demonstrate that food consumption was greater for the with-sauce options than for the without-sauce options among Japanese elderly people with dementia, results which are in accord with those from a study conducted in France. To make clear the influences of the sensory and cognitive factors of the addition of sauce on food consumption among elderly people with dementia, further studies that control for the familiarity with or eating habit of wiping up the sauce with food among participants are necessary.
According to the total amount of finger snacks consumed, our participants ate more snacks with sauce than without sauce, regardless of the kind of sauce. In Experiment 1, the mean amount of snacks with chocolate sauce (high visual contrast) consumed was 7.8 pieces (SD = 2.9). This is 82.8% of the mean total amount (10.4 pieces; SD = 2.4) of snacks consumed. In Experiment 2, the mean amount of snacks with agave sauce (low visual contrast) consumed was 6.9 pieces (SD = 2.2). This is 66.9% of the mean total amount (10.4 pieces; SD = 2.6) of snacks consumed. In Japan, people usually eat baumkuchen without sauce, as in other countries, and, thus, it is considered that the addition of sauce is an unfamiliar way to eat baumkuchen for Japanese elderly people. Appleton16 examined the effect of the addition of sauce on food intake among elderly people in the UK. She found that the energy consumed in meals was higher for meals in a with-sauce condition than for those in a without-sauce condition, whereas the results of a self-report questionnaire showed that there were no significant differences in food preference and familiarity between conditions. Furthermore, the flavor enhancement of food would contribute to enhancing the pleasure of eating and interest in food among elderly people with dementia because they usually have some olfactory dysfunctions related to age and disease which influence their decreased food consumption.26,27 It has been suggested that sensory factors such as the semi-solid nature and flavor of sauces might contribute to increased meal consumption.
The present results show that there are no significant correlations between HDS scores and the selection rate of snacks with sauce. These results suggest that the addition of sauce had a generally positive impact on snack intake regardless of the cognitive ability of participants. On the other hand, some previous studies have shed light on the individual differences in the effects of food improvements on food intake and preference among older adults. For instance, Appleton28 demonstrated that there are some individual differences in the impact of the addition of sauce on a meal among healthy free-living older adults. In her study, 50.0% of the participants showed greater protein intakes at a lunch meal served with sauce. However, 36.5% of the participants showed lower protein intake in response to adding the sauce. She discussed that these differences were not explained by participants’ gender, age or subjective evaluations toward foods. Pouyet27 also demonstrated that food liking in response to the flavor enhancement manipulation was dependent on the cognitive status in older adults, whereas food intake was increased by the same manipulation regardless of the cognitive status of participants. In the present study, 9.5% of the participants in Experiment 1 and 35.7% of the participants in Experiment 2, who are of various genders, ages and HDS-R scores, exhibited equal intake between snacks with and without sauce, while the majority of both sets of participants exhibited greater intake of snacks with sauce than without sauce. In order to make clear the factors determining these individual differences in the effect of the addition of sauce on food intake and evaluation, further studies are required.
In the current study, some differences in food consumption depending on the kind of sauce were observed. In Experiment 2, participants ate larger amounts of finger snacks with agave sauce than those without sauce. These results suggest that participants perceived the presence of the sauce despite its low-contrast color compared with the snack. However, the mean finger-snack intake was significantly greater for snacks with the chocolate sauce than for those with the agave sauce even though the total amount of snacks consumed, including snacks with and without sauce, did not differ significantly between experimental sessions. One may argue that there is a possibility that the order effect was responsible for the participants’ eating behavior because all of our participants were presented the chocolate sauce option first (Experiment 1) and the agave sauce option second (Experiment 2). These confounding settings in the experiments were concessions mainly due to clinical and ethical issues: It was thought that differences of menu between participants or division of the dining room to allow separate areas for each condition might give rise to anxiety and restlessness among elderly people with dementia. If the order effect was a critical influence on the present results, it is hypothesized that the amount of snacks with sauce eaten would be greater in Experiment 2 than in Experiment 1 because familiarity with the eating style of wiping up the sauce with food would be greater in the later session than in the earlier session. As mentioned above, it is widely known that familiarity is a critical factor in food choice and preference. Our participants, however, showed the opposite pattern of consumption; thus, the present results cannot be explained by the order effect alone. One possible reason for the present results is the difference in visual contrast, especially in the lightness contrast between the chocolate and agave sauces. Several studies on food improvement, dishware and eating environment have demonstrated that a high visual contrast aids in the perception of the presence of and the remaining amount of a meal for elderly people with dementia.15,29 For instance, Dunne et al29 demonstrated that food and fluid intake increased among patients with severe Alzheimer’s disease when high-contrast (red) dishes, compared to low-contrast (white) dishes, were provided. The researchers pointed out that elderly people with Alzheimer’s disease tend to exhibit deficits in visual contrast sensitivity, and therefore to have difficulty distinguishing a plate from a table setting, food from a plate, or liquid from its container without sufficient contrast. These difficulties might lead to a reduction in consumption. Thus, enhancing contrast in the eating environment would be an effective way to help elderly people with Alzheimer’s disease in the aspect of food recognition. The present results suggest that the chocolate sauce with its dark brown color may have aided our participants in distinguishing the snack from the white plate.
Another possible explanation for the present results lies in the difference in flavor between the sauces. The flavors of the chocolate and agave sauces differed, while the sweetness of the sauces was similar. None of the participants exhibited distaste toward the flavor of either sauce during the experimental sessions. However, we did not quantitatively measure their preferences toward the sauces by self-report because of reliability concerns. In the present study, we did not tightly control the flavor of the sauces used because we focused mainly on the relative importance of low-level sensory factors, including visual contrast and flavor, and high-level cognitive factors, such as eating culture, in the effect of the addition of a sauce on food intake among elderly people with dementia. To elucidate the relative importance of several sensory factors, further experiments tightly controlling sauce stimuli for color, flavor, taste and order of presentation are required. A promising strategy would be the use of agave sauce with artificial coloring (low-, middle-, and high-contrast colors) because agave sauce basically has a low-contrast color that is not canonical for Japanese people.
The current results also show that there were no significant differences between with- and without-sauce options for first choice regardless of the kind of sauce. These results are inconsistent with Pouyet et al,15 who reported that finger foods with sauce were chosen before those without sauce. Our additional analyses revealed that the participants tended to choose snacks from the front side (closest to the participant) of the dish in both Experiments 1 and 2. While it is thought that the first choice of food reflects the attractiveness of that food,15 the present results imply that the accessibility of the food may also affect food-choice behavior among elderly people with dementia. While several studies have argued that accessibility plays an important role in food choice and food intake,30–36 the present findings suggest that minimal accessibility, such as how foods are arranged on a single dish, affects food choice among elderly people with dementia. In the present study, because the total snack consumption was greater for the with-sauce option than for the without-sauce option regardless of the first choice, it is thought that this accessibility effect is limited to the first choice. To generalize and elucidate the relationship between food arrangement on a dish and first-choice behavior, further experiments that include healthy elder and young people are required. If the present results are replicated, this very simple implication that people tend to take food from the closer side of a dish could contribute to the feeding assistance of elderly people.
The present findings may provide some important insight into menu improvements both in households and in residential or nursing homes as well as for product development in the food industry. The addition of a sauce may be an effective approach for improving food consumption among elderly people with dementia because adding sauce to solid food can not only aid in the passage of food through the digestive system, but also enhance the flavor and visual contrast of the food. Furthermore, sauce is an option and each individual can decide how much sauce she/he uses. Thus, using sauces may be an easy way to address individual differences such as taste preferences and degree of swallowing ability. Milte et al37 argued that the sensory appeal of food is highly important despite cognitive impairment. The addition of sauce is one simple way to improve the sensory appeal of a meal and may have high applicability for menu arrangement.
The present results are subject to some limitations. Firstly, the effects of the addition of sauce on finger-food consumption among Japanese elderly people with dementia were examined for only baumkuchen. While baumkuchen is a familiar and popular snack in Japanese nursing homes, further studies that involve various snacks and meals are required to generalize the present findings. Secondly, following Pouyet at al,15 the present study employed paired comparison techniques to compare the participants’ choice of snacks between with- and without-sauce options. This prevents us from examining the impact of the addition of sauce on the energy intake among elderly people with dementia accurately because we cannot assume how much of a snack would be consumed if only one option was presented. Thus, further studies based on a two-group experimental design (the addition of sauce: with sauce vs without sauce), in which participants’ food consumption is tracked, are also required. Furthermore, Appleton28 also considered compensation for earlier intake at subsequent meals in the effect of the addition of sauce. To make clear the degree of the compensation effect with the addition of sauce among elderly people with dementia, measuring the amount of consumption at subsequent meals is also required. Thirdly, psychological evaluations, including preference and taste intensity of food, were not measured in this study because such rating tasks may be difficult for cognitively impaired older adults to answer. However, such evaluations of foods may contribute to why participants had more pieces with sauce than without sauce. Thus, more convenient methods to assess participants’ evaluations are needed. For instance, Pouyet et al27 proposed a step-by-step evaluation of food liking for cognitively impaired older adults and indicated that there was a moderately positive correlation between food liking and food intake among their participants. Such techniques would be useful in assessing psychological evaluations of food in elderly people with dementia.
Conclusion
The main interest of the present study is whether the wiping up of sauce with food is effective for increasing the amount of food consumed by elderly people with dementia not only in French but also in Japanese samples. The results show that snack consumption was greater for the with-sauce options than for the without-sauce options among Japanese elderly people with dementia. These results confirm previous findings, which demonstrated that the addition of sauce had a positive impact on food consumption among French elderly people with dementia.15 Although there are some methodological limitations, as mentioned above, these findings serve as one step towards understanding eating behavior among elderly people with dementia. To accelerate progress in this area, further research is necessary in order to clarify what and how sensory and cognitive factors contribute to food acceptance and attractiveness among elderly people with dementia.
Acknowledgments
We are extremely grateful to all participants and staff at the nursing home involved. We would like to acknowledge Ms. Kimika Ishikawa, Ms. Masumi Hayashi, Ms. Minami Osumi and Mr. Teppei Takemiya for their assistance and to English Language Consultation Services for examination of the manuscript. This work is supported in part by Grant-in-Aid for Scientific Research (C) from the Japan Society for Promotion of Science 18K02193.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gale SA, Acar D, Daffner KR. Dementia. Am J Med. 2018;131:1161–1169. doi:10.1016/j.amjmed.2018.01.022
2. Volkert D, Chourdakis M, Faxen-Irving G, et al. ESPEN guidelines on nutrition in dementia. Clin Nutr. 2015;34:1052–1073. doi:10.1016/j.clnu.2015.09.004
3. Prince MJ, Wimo A, Guerchet MM, Ali GC, Wu Y-T, Prina M. World Alzheimer Report 2015: The Global Impact of Dementia. An Analysis of Prevalence, Incidence, Cost and Trends. London: Alzheimer’s Disease International; 2015.
4. Poulos CJ, Bayer A, Beaupre L, et al. A comprehensive approach to reablement in dementia. Alzheimers Dement. 2017;3:450–458.
5. Douglas JW, Lawrence JC. Environmental considerations for improving nutritional status in older adults with dementia: a narrative review. J Acad Nutr Diet. 2015;115:1815–1831. doi:10.1016/j.jand.2015.06.376
6. Lin LC, Watson R, Wu SC. What is associated with low food intake in older people with dementia? J Clin Dement. 2010;19:53–59.
7. Stone L. Eating/feeding issues in dementia: improving the dining experience. End Life J. 2014;4:1–7. doi:10.1136/eoljnl-04-01.1
8. Aselage MB, Amella EJ. An evolutionary analysis of mealtime difficulties in older adults with dementia. J Clin Nurs. 2010;19:33–41. doi:10.1111/j.1365-2702.2009.02969.x
9. Stanner S. Older people with dementia: eating and drinking healthily. Nurs Resid Care. 2007;9:18–21. doi:10.12968/nrec.2007.9.1.22574
10. Hetherington MM. Taste and appetite regulation in the elderly. Proc Nutr Soc. 1998;57:625–663. doi:10.1079/PNS19980091
11. Schiffman SS, Gatlin CA. Clinical physiology of taste and smell. Annu Rev Nutr. 1993;13:405–436. doi:10.1146/annurev.nu.13.070193.002201
12. Kalia M. Dysphasia and aspiration pneumonia in people with Alzheimer’s disease. Metab. 2003;52:36–38. doi:10.1016/S0026-0495(03)00300-7
13. Abbott RA, Whear R, Thompson-Coon J, et al. Effectiveness of mealtime interventions on nutritional outcomes for the elderly living in residential care: a systematic review and meta-analysis. Ageing Res Rev. 2013;12:967–981. doi:10.1016/j.arr.2013.06.002
14. Liu W, Cheon J, Thomas SA. Interventions on mealtime difficulties in older adults with dementia: a systematic review. Int J Nurs Stud. 2014;51:14–27. doi:10.1016/j.ijnurstu.2012.12.021
15. Pouyet V, Giboreau A, Benattar L, Cuvelier G. Attractiveness and consumption of finger foods in elderly Alzheimer’s disease patients. Food Qual Prefer. 2014;34:62–69. doi:10.1016/j.foodqual.2013.12.011
16. Appleton KM. Increases in energy, protein and fat intake following the addition of sauce to an older person’s meal. Appetite. 2009;52:161–165. doi:10.1016/j.appet.2008.09.009
17. Best RL, Appleton KM. Comparable increases in energy, protein and fat intakes following the addition of seasonings and sauces to an older person’s meal. Appetite. 2011;56:179–182. doi:10.1016/j.appet.2010.10.011
18. Borgogno M, Corazzin M, Saccà E, Bovolenta S, Piasentier E. Influence of familiarity with goat meat on liking and preference for capretto and chevon. Meat Sci. 2015;106:69–77. doi:10.1016/j.meatsci.2015.04.001
19. Fischer ARH, Frewer LJ. Consumer familiarity with foods and the perception of risks and benefits. Food Qual Prefer. 2009;20:576–585. doi:10.1016/j.foodqual.2009.06.008
20. Giacalone D, Frøst MB, Bredie WL, et al. Situational appropriateness of beer is influenced by product familiarity. Food Qual Prefer. 2015;39:16–27. doi:10.1016/j.foodqual.2014.06.012
21. Pliner P, Pelchat M, Grabski M. Reduction of neophobia in humans by exposure to novel foods. Appetite. 1993;20:111–123. doi:10.1006/appe.1993.1013
22. Pliner P, Stallberg-White C. “Pass the ketchup, please”: familiar flavors increase children’s willingness to taste novel foods. Appetite. 2000;34:95–103. doi:10.1006/appe.1999.0290
23. Cullen P, Abid F, Patel A, Coope B, Ballard CG. Eating disorders in dementia. Int J Geriatr Psychiatry. 1997;12:559–562. doi:10.1002/(SICI)1099-1166(199705)12:5<559::AID-GPS550>3.0.CO;2-W
24. Mungas D, Cooper JK, Weiler PG, Gitzen D, Franzi RN, Bernick CB. Dietary preference for sweet foods in patients with dementia. J Am Geriatr Soc. 1990;38:999–1007. doi:10.1111/j.1532-5415.1990.tb04423.x
25. Young KWH, Greenwood CE, van Reekum R, Binns MA. A randomized, crossover trial of high-carbohydrate foods in nursing home residents with Alzheimer’s disease: associations among intervention response, body mass index, and behavioral and cognitive function. J Gerontol Med Sci. 2005;60:1039–1045. doi:10.1093/gerona/60.8.1039
26. Alves J, Petrosyan A, Magalhães R. Olfactory dysfunction in dementia. World J Clin Cases. 2014;2:661–667. doi:10.12998/wjcc.v2.i11.661
27. Pouyet V, Cuvelier G, Benattar L, Giboreau A. Influence of flavour enhancement on food liking and consumption in older adults with poor, moderate or high cognitive status. Food Qual Prefer. 2015;44:119–129. doi:10.1016/j.foodqual.2015.04.014
28. Appleton KM. Limited compensation at the following meal for protein and energy intake at a lunch meal in healthy free-living older adults. Clin Nutr. 2018;37:970–977. doi:10.1016/j.clnu.2017.03.032
29. Dunne TE, Neargarder SA, Cipolloni PB, Cronin-Golomb A. Visual contrast enhances food and liquid intake in advanced Alzheimer’s disease. Clin Nutr. 2004;23:533–538. doi:10.1016/j.clnu.2003.09.015
30. Elsbernd SL, Reicks MM, Mann TL, Redden JP, Mykerezi E, Vickers ZM. Serving vegetables first: a strategy to increase vegetable consumption in elementary school cafeterias. Appetite. 2016;96:111–115. doi:10.1016/j.appet.2015.09.001
31. Hearn MD, Baranowski T, Baranowski J, et al. Environmental influences on dietary behavior among children: availability and accessibility of fruits and vegetables. J Health Educ. 1989;29:26–32. doi:10.1080/10556699.1998.10603294
32. Kimura A, Tamaki T, Tokunaga H, Mukawa N, Wada Y. Effects of perceived quality of container on water and snack intake and dyadic communication. Food Qual Prefer. 2018;64:181–186. doi:10.1016/j.foodqual.2017.09.009
33. Mayers AW, Stunkard AJ, Coll M. Food accessibility and food choice. Arch Gen Psychiatry. 1980;37:1133–1135. doi:10.1001/archpsyc.1980.01780230051007
34. Strpebele N, De Castro JM. Effect of ambience on food intake and food choice. Nutrition. 2004;20:821–838. doi:10.1016/j.nut.2004.05.012
35. Swanson M, Branscum A, Nakayima PJ. Promoting consumption of fruit in elementary school cafeterias. The effects of slicing apples and oranges. Appetite. 2009;53:264–267. doi:10.1016/j.appet.2009.07.015
36. Wansink B. Environmental factors that increase the food intake and consumption volume of unknowing consumers. Annu Rev Nutr. 2004;24:455–479. doi:10.1146/annurev.nutr.24.012003.132140
37. Milte R, Shulver W, Killington M, Bradley C, Miller M, Gotty M. Struggling to maintain individuality: describing the experience of food in nursing homes for people with dementia. Arch Gerontol Geriatr. 2017;72:52–58. doi:10.1016/j.archger.2017.05.002
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.