")
Back to Journals » Journal of Inflammation Research » Volume 14
Acute Respiratory Distress Syndrome and COVID-19: A Literature Review
Authors Hussain M, Khurram Syed S, Fatima M, Shaukat S, Saadullah M, Alqahtani AM , Alqahtani T, Bin Emran T , Alamri AH , Barkat MQ, Wu X
Received 12 August 2021
Accepted for publication 17 November 2021
Published 21 December 2021 Volume 2021:14 Pages 7225—7242
DOI https://doi.org/10.2147/JIR.S334043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Musaddique Hussain,1 Shahzada Khurram Syed,2 Mobeen Fatima,1 Saira Shaukat,1 Malik Saadullah,3 Ali M Alqahtani,4 Taha Alqahtani,4 Talha Bin Emran,5 Ali H Alamri,6 Muhammad Qasim Barkat,7 Ximei Wu7
1Department of Pharmacology, Faculty of Pharmacy, The Islamia University of Bahawalpur, Bahawalpur, 63100, Pakistan; 2Department of Basic Medical Sciences, School of Health Sciences, University of Management and Technology Lahore, Lahore, 54000, Pakistan; 3Department of Pharmaceutical Chemistry, Government College University, Faisalabad, 38000, Pakistan; 4Department of Pharmacology, College of Pharmacy, King Khalid University, Abha, 62529, Saudi Arabia; 5Department of Pharmacy, BGC Trust University Bangladesh, Chittagong, 4381, Bangladesh; 6Department of Pharmaceutics, College of Pharmacy, King Khalid University, Abha, 62529, Saudi Arabia; 7Department of Pharmacology, School of Medicine, Zhejiang University, Hangzhou City, 310000, People’s Republic of China
Correspondence: Musaddique Hussain
Department of Pharmacology, Faculty of Pharmacy, The Islamia University of Bahawalpur, Bahawalpur, 63100, Pakistan
Email [email protected]
Ximei Wu
Department of Pharmacology, School of Medicine, Zhejiang University, Hangzhou City, People’s Republic of China
Email [email protected]
Abstract: Acute respiratory distress syndrome (ARDS) is an overwhelming inflammatory disorder of the lung due to direct and indirect insults to the lungs. ARDS is characterized by increased vascular permeability, protein-rich edema, diffuse alveolar infiltrate, and loss of aerated lung tissue, leading to decreased lung compliance, tachypnea, and severe hypoxemia. COVID-19 is generally associated with ARDS, and it has gained prime importance since it started. The mortality rate is alarmingly high in COVID-19-related ARDS patients regardless of advances in mechanical ventilation. Several pharmacological agents, including corticosteroids, nitric oxide, neuromuscular blocker, anti-TNF, statins, and exogenous surfactant, have been studied and some are under investigation, like ketoconazole, lisofylline, N-acetylcysteine, prostaglandins, prostacyclin, and fish oil. The purpose of this review is to appraise the understanding of the pathophysiology of ARDS, biomarkers, and clinical trials of pharmacological therapies of ARDS and COVID-19-related ARDS.
Keywords: acute respiratory distress syndrome, acute lung injury, COVID-19, COVID-19-related ARDS
Introduction
Background
Acute Respiratory Distress Syndrome (ARDS), a life-threatening inflammatory lung injury, was first described in 1967 by Ashbaugh, characterized by bilateral pulmonary infiltrates and acuity of onset. ARDS is manifested by increased alveolar-capillary membrane permeability, pulmonary edema, impaired surfactant formation, neutrophil infiltration, impaired gas exchange, and respiratory failure due to severe hypoxemia. The fatality rate is between 26% and 61.5% and varied according to genetics, gender, age, aetiology, as well as presence of concomitant comorbidities.1 17% of patients required oxygen treatment and intensive care unit (ICU) interventions owing to severe hypoxemia and respiratory failure.2–4 Around 33% of COVID-19 victims developed ALI/ARDS, and 53% of COVID-19-related ARDS fatalities are caused primarily by respiratory failure.5 Blood clots, infections, distorted lungs, and scarring are the short-term complications associated with ARDS, while long-term complications embrace difficulty in breathing, depression, cognitive problems, and muscle weakness.
In 1994, The American European Consensus Conference proposed the definition of ALI/ARDS but had various limitations.6 In 2011, a panel of experts established the Berlin definition, which explains the ARDS as the respiratory failure occurs within seven days of the inciting event, severe hypoxemia, and bilateral infiltration, in the absence of cardiogenic pulmonary edema. In ARDS, hypoxemia (ratio of arterial oxygen tension over fractional inspired oxygen PaO2/FiO2) becomes less than 200 mmHg. According to Berlin criteria, there are 3 categories of ARDS based on the severity of hypoxemia (PaO2/FiO2): A) in mild ARDS, the PaO2/FiO2 is in between 200 and 300 mmHg B) in moderate ARDS, the PaO2/FiO2 is in between 100 and 200 mm Hg and C) in severe ARDS the PaO2/FiO2 is ≤100 mm Hg.7 However, the Berlin criterion is not suitable in the scarcity of resources where access to mechanical ventilation, chest radiography, and arterial blood gas data is difficult. The ARDS defined by Kigali keeps the same criteria of 1 week of insult and origin of edema as that of the Berlin definition. The minimum Positive End-Expiratory Pressure (PEEP) requirement is excluded, and hypoxemia, the ratio of arterial oxygen saturation (SpO2)/inspiratory oxygen fraction (FiO2), as measured by pulse oximetry is equal to or less than 315 with SpO2 ≤97%.8
COVID-19-Related ARDS (CARDS)
At the end of December 2019, a sudden outbreak of the novel respiratory disease was reported in Wuhan, China. Researchers of the Chinese Center for Disease Control and Prevention evaluated the lower respiratory tract of infected patients and discovered a novel coronavirus namedCOVID-19.9 COVID-19 is a systemic infection that mainly damages the endothelial layer of the lungs and transmits from one individual to the other – either from symptomatic or asymptomatic individuals.10,11 A COVID-19 patient with ARDS (CARDS) who is not adequately managed by focusing on the underlying infection area may lead to multiple organ failures, even though the patient experiences no signs of previous illnesses.12 CARDS may have long-term complications including thromboembolism and ICU-acquired disabilities. The mortality rate of individuals with CARD is estimated to be 39%.
COVID-19 outbreak has gained a promised importance since it started, and ARDS has a close relation with COVID-19. In COVID-19 patients, the most decisive predictor for death is the development of ALI/ARDS. A recent study stated that about 85% of COVID-19 individuals admitted to the hospital meet the Berlin ARDS criteria.9 Nevertheless, the explicit mechanism through which COVID-19 exacerbates ARDS remains unexplained. Conversely, various studies have shown that the onset of CARDS viz, time of progression of COVID-19 to ALI/ARDS is about 8–12 days, emphasizing that ALI/ARDS should be treated promptly (within a week).
Generally, ARDS features do not include cardiogenic shock or edema, although the characteristics such as shunt-related hypoxia and the decreased lung size are the prime causes leading to low respiratory compliance.13 The difference between typical ARDS and CARDS is the advent of disease, hypoxemia and lung compliance, which seems to be comparatively higher in CARDS; consequently, thorough assessment and intervention are needed.14 The national health commission (NHC), China, provided management strategies for COVID-19. CARDS was classified into 3 different categories depending on hypoxemia; in mild hypoxemia, it is between 200 and 300 mmHg. In mild-moderate, it varies from 150 to 200 mmHg. In moderate-severe, it is less than 150 mmHg.15 Several ventilatory strategies designed to alleviate ARDS are suggested in CARDS to optimize the oxygenation index and mortality.16,17
Clinical trials for nebulized heparin (NCT04511923), telmisartan (NCT04510662), Pirfenidone (NCT04653831), mesenchymal stem cells (NCT04611256, NCT04371393, NCT04399889, NCT04565665 andNCT04625738), RAPA-501-ALLO cells (NCT04482699) and alteplase-50 as fibrinolytic therapy (NCT04357730), focusing on CARDS are ongoing.18 Ongoing clinical trials for ARDS in relation to COVID-19 are depicted in Table 1.
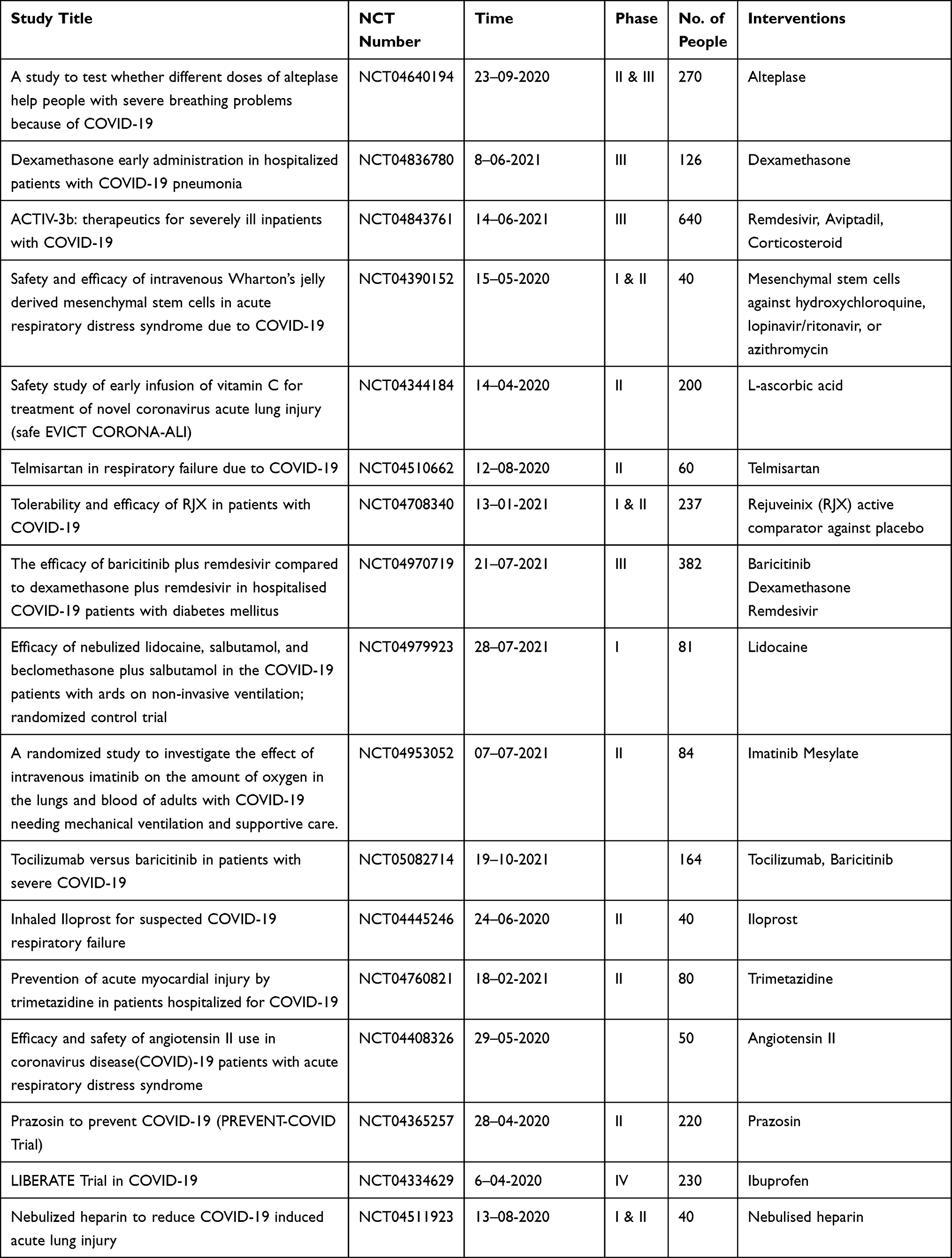 |
Table 1 Ongoing Clinical Trials of Therapies Used for CARDS |
Methods and Materials
Search Strategy
Several electronic databases, particularly PubMed, PubMed Central, and Google Scholar, were used to conduct the search for research works. A search for relevant literature was carried out using the keywords including ARDS/ALI, COVID-19, SARS-CoV-2, ARDS biomarkers, pathophysiology of ARDS or CARDS, epidemiology of ARDS or CARDS and treatment options for ARDS or CARDS, etc. The study was considered to be included whether it was a review paper or full-text publication, an observational study, or a clinical trial.
Extracted Data
We extracted the data for relevant article using the databases of the Chinese clinical trial registration centre and ClinicalTrials.gov. The collected data includes information on the introduction, risk factors, mechanism and therapy for both ARDS and CARDS. The contents retrieved for clinical trials comprised registration number, the title of the study, research type, the study design, the start date, the sample size, the interventions.
Results
Etiology
The response of ARDS towards multiple factors is invariant. The exact etiology and pathogenesis of ARDS are indeed not ascertainable. However, severe bacterial infections, such as pneumonia and sepsis, are the most common cause of ARDS.19 Factors such as age, gender, genetics, external factors (cigarette smoke), chronic pulmonary diseases, and concomitant diseases increase ARDS risk. ARDS affects individuals of all ages, although the incidence of ARDS increases with age because the elderly are more susceptible to the primary risk of sepsis.20 The risk of developing ARDS also relies on the patient’s profile, such as the diabetic and chronic alcoholic patients are prone to ARDS.21,22
Over 40 candidate genes are linked with ARDS,23 including angiotensin-converting enzyme (ACE), TNF, vascular endothelial growth factor (VEGF), surfactant protein B (SFTPB), and macrophage migration inhibitory factor (MIF).24 The ACE gene-2 protein, which mediates lung vascular permeability, is renowned as the SARS-CoV cell entrance receptor.25 The renin-angiotensin pathway may be inhibited to reduce pulmonary injury induced by SARS-CoV.26
The mode of injury can be direct or indirect and is enlisted in Table 2. In direct lung injury, the stimulus directly hits the structures of the lungs and is characterized by severe epithelial, infiltration of neutrophils, hyaline membrane formation, fibrin deposition, and edema. In indirect lung injury, the more severe endothelial or vascular injury happened with fewer neutrophil recruitment. Thus, personalized therapy according to the interpretation of etiology may enhance the effectiveness of treatment.
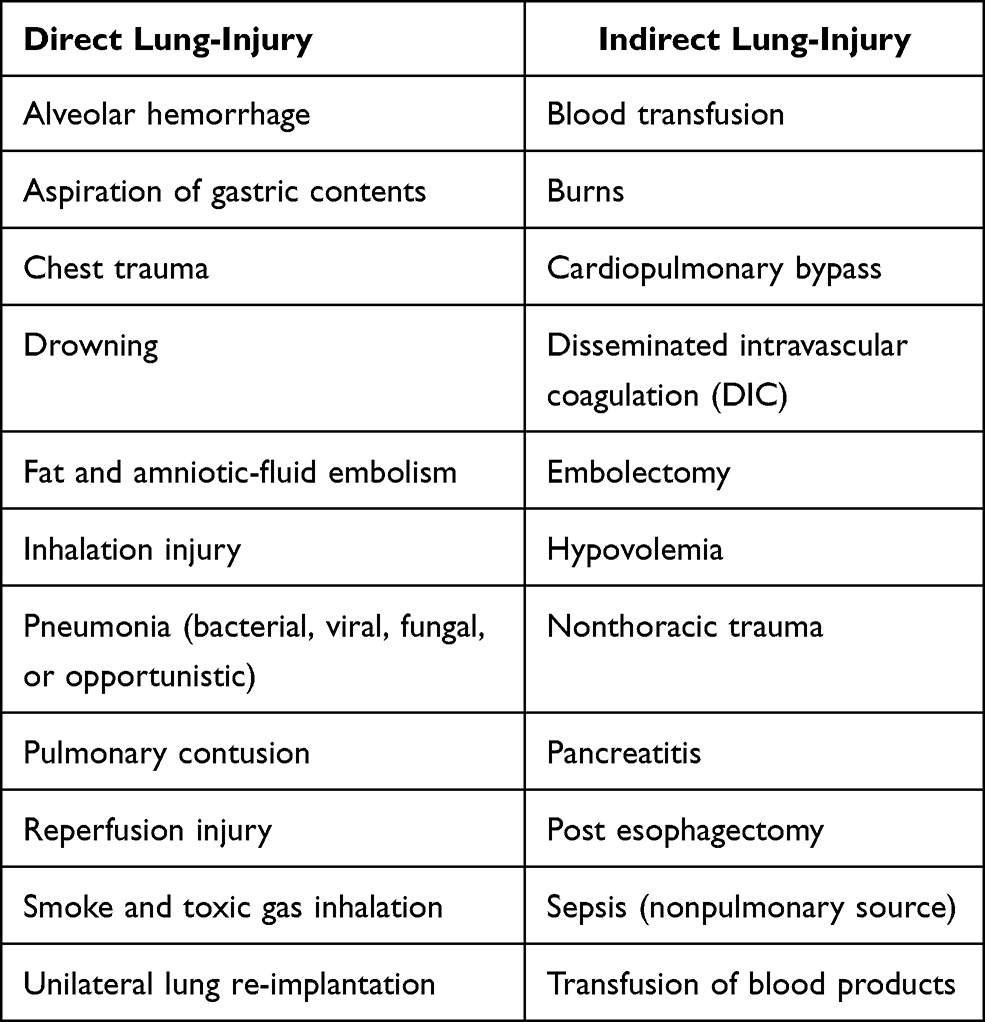 |
Table 2 Risk Factors |
Clinical Manifestation
The SARS-CoV-2 virus invades via adhering to angiotensin converting enzyme 2 (ACE2) receptors.27 COVID-19 patients have significant viral replication during the first phase, which lasts around 5 days following infection. The symptoms often manifested within few hours of the triggering events of ALI/ARDS and progressively worsened over hours to days, necessitating extended mechanical breathing to avoid hypoxia and hospitalisation or ICU treatment. The most common symptoms at this phase are fever, coughing, fatigue, anosmia and dyspnea. Viral replication normally ceases 5–7 days after the onset of symptoms. Some patients may undergo a second phase (seven to ten days) following the onset of symptoms, which is pathophysiologically associated with unrestrained inflammatory reaction in the lungs. At this phase, patients typically developed ARDS.28
Histopathology and Pathophysiology
The pathophysiological mechanism is related to the unrestrained inflammatory reaction in the lungs and is divided into three phases: a) exudative phase, b) proliferative phase, and c) fibrotic phase.29
The early phase that occurs within 72 hours is the exudative phase (0–7 days), characterized by an increase in the permeability of membranes, leakage of protein-rich fluid, inflammatory cellular infiltrates (predominantly neutrophils), and gradual refractory hypoxemia.30
In response to diffuse alveolar damage (DAD), the inflammatory cells and fibroblasts produce cytokines, including TNF-α, IL-1β, IL-6, and chemokines such as IL-8. The onset of ARDS in COVID-19 subjects was believed to be exacerbated by cytokine storm. Cytokines increase the infiltration of neutrophils, which activates and releases toxic mediators such as reactive oxygen species and nitric oxide. These toxic mediators damage the epithelium of alveoli and capillary endothelium, resulting in increased permeability, allowing protein-rich fluid and blood cells to move into the interstitium and alveoli.31
The air spaces become filled with fluid and cellular debris. Eosinophilic depositions termed hyaline membrane is the histopathological hallmark of ARDS. Also, the coagulation pathway becomes disrupted, leading to micro thrombus formation. The impaired surfactant-producing cells, ie, alveolar type II cells, lead to alveolar atelectasis and lung stiffness. These changes and hyaline membrane deposition impair gas exchange.32
The fibro-proliferative/proliferative phase (7–21 days) is characterized by proliferation and architectural changes. The repair process is initiated during this phase, and surfactant production is restored because of type II alveolar cells’ proliferation. Aside from that, the epithelium rejuvenates as a consequence of type I pneumocyte proliferation, culminating in the reabsorption of alveolar edema. The proliferative phase may progress to the fibrotic stage, marked by extensive diffuse fibrosis, obliteration of the typical lung architecture, and patchy emphysematous alterations.31
Biomarkers
Biomarkers enable identifying individuals at risk of developing ARDS, how to diagnose them, and how to monitor their response to therapeutic interventions. Since biomarkers are assumed to provide insight into the disease’s pathophysiology, therefore many biomarkers have been examined in plasma, bronchoalveolar lavage fluid (BALF), and exhaled gas of ARDS patients.
Several studies have suggested that a combination of biomarkers is better at predicting clinical outcomes than single biomarker alone.33,34 Most of the biomarkers in the blood reflect inflammation. Biomarkers investigated in blood for the exudative phase include endothelial protein angiopoietin-1, thrombomodulin, von Willebrand factor (vWF), protein C, intercellular adhesion molecule-1 (ICAM-1), and plasminogen activator inhibitor-1.34,35
Biomarkers, investigated both in blood and BALF, are receptor for advanced glycation endproducts (RAGE), Krebs von den Lungen-6 (KL-6), Clara cells (CC16), interleukins (IL-1β, IL-6, IL-8, IL-10), tumor necrosis factor-α (TNF-α), surfactant protein, matrix metalloproteinases (MMPs), vascular endothelial growth factor (VEGF).36,37
Biomarkers for the fibroproliferative phase include keratinocyte growth factor (KGF), hepatocyte growth factor (HGF), N-terminal procollagen peptide-III (N-PCP-III), and Fas/FasL.38 The benefit of BALF is that it is the closest sample to the site of injury. In the exhaled breath, three volatile organic compounds (VOCs) such as octane, acetaldehyde, and 3-methylheptane are potential markers of ARDS.39
Pharmacological Treatments
Despite the considerable advance in the understanding of ARDS’s pathophysiology and extensive research in both pre-clinical and clinical settings, the effectiveness of available therapeutic options remains inadequate, and mortality remains unacceptably high. While many favorable pharmacological agents, including corticosteroids, statins, beta-agonists, non-steroidal anti-inflammatory drugs, antioxidants, exogenous surfactant, neutrophil elastase inhibitors, anticoagulants, anti-TNF, biologics, nitric oxide, and lysofylline have been investigated in patients with ARDS but none of these pharmacological agents reduced mortality.40 The subsequent section reviews therapies that have been used in patients with ARDS in many clinical trials Table 3.
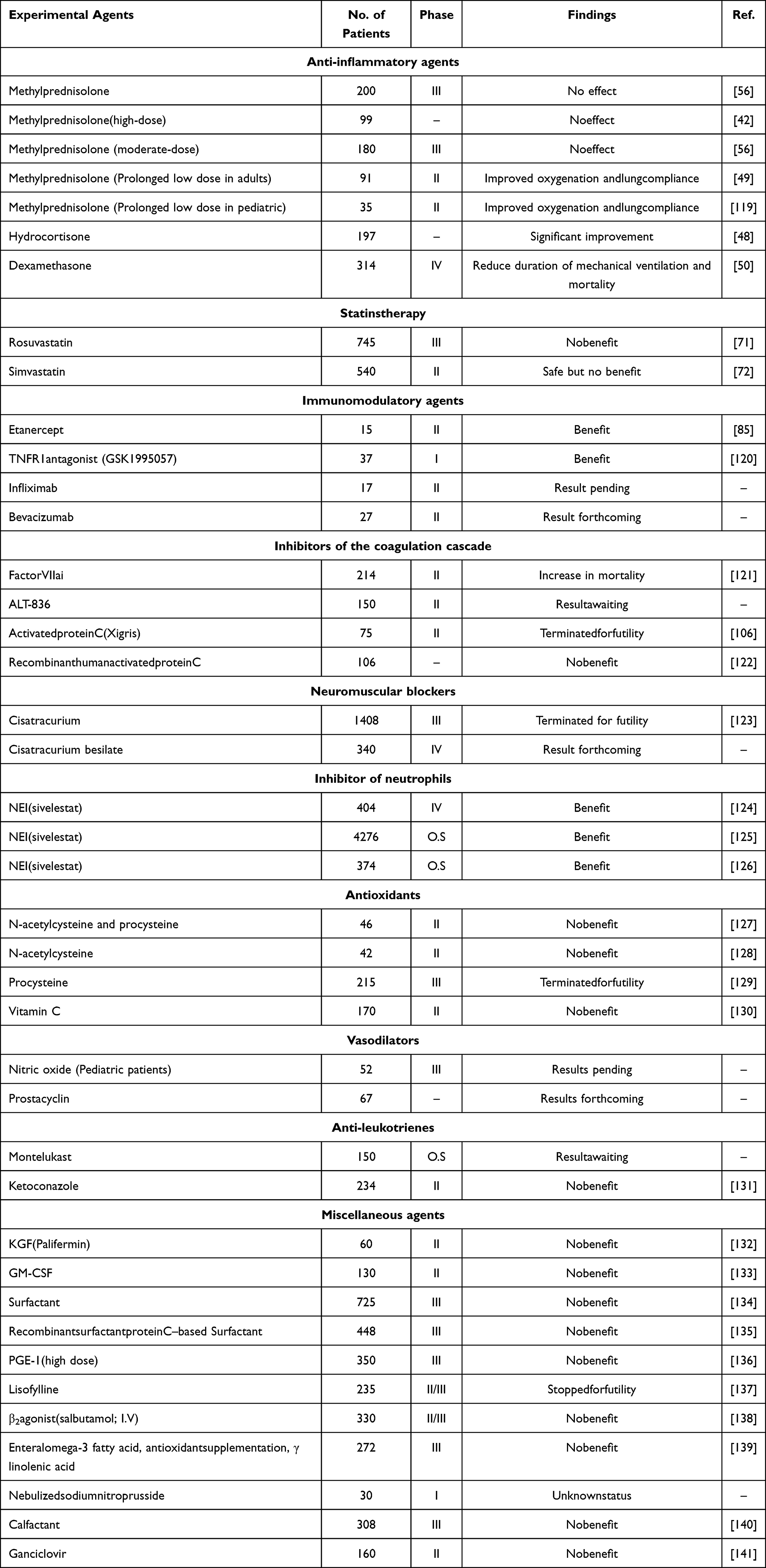 |
Table 3 Completed Clinical Trials of Therapies Used in ALI/ARDS |
Corticosteroids
Corticosteroids are double-edged swords that effectively treat numerous conditions such as allergic conditions, asthma, septic shock, cancers, and autoimmune diseases. Corticosteroids are potent anti-inflammatory and anti-fibrotic agents that inhibit the inflammatory cascade at different stages of the process via an independent mechanism.41 The transcription of numerous cytokines, including interleukin (IL-1, 3, 4, 5, 6 and 8) and TNF-α, is inhibited by these agents. A striking inflammatory process characterizes ARDS; thus, systematic corticosteroid treatment is evident to attenuate pulmonary inflammation.
Corticosteroid therapy has been studied in 4 different situations: 1) Dose (high or low), 2) treatment timing, ie, early or late phase, 3) Duration of treatment, 4) ARDS associated with COVID-19.
Many randomized clinical trials (RCT) demonstrate that a high dose of corticosteroids does not modify the ARDS course with short-term therapy.42,43 In Japan, a nationwide retrospective observational study was done to evaluate the mortality of ARDS patients after a high and non-high dose of corticosteroid therapy. They estimated that the mortality rate is higher in patients treated with high doses (500 mg/kg of methylprednisolone every 12 h) than those receiving a low corticosteroid dose (1 mg/kg of methylprednisolone per day).44 However, prolonged treatment with low doses of corticosteroids has better results in early severe ARDS& appeared more promising.45,46
Timing of initiation of treatment (within 14 days from insult) is also crucial to reduce the duration of mechanical ventilation, ICU stays, and mortality.47 Many clinical trials (NCT01284452) recommended that early administration of low-dose corticosteroid improves outcomes in patients of ARDS.48,49 In Spain, a recent randomized clinical trial (NCT01731795) revealed that early administration of dexamethasone improves oxygenation and reduces the mortality rate in ARDS subjects.50 According to Phase II randomized clinical trial (NCT01783821), the early administration of inhaled corticosteroid (formoterol/budesonide) in combination with inhaled β2-agonists improved the oxygenation and inhibited the progression of ARDS in patients at the risk of ARDS.51
ARDS is the major complication that contributes to the high mortality rate in hospitalized patients of COVID-19. Corticosteroid therapy, including dexamethasone, methylprednisolone and hydrocortisone, is beneficial in treating and reducing the mortality rate in many clinical cases of COVID-19 patients. A study (NCT04244591) suggested that methylprednisolone (40 mg) improves the prognosis. A systematic review performed on 10,815 patients of COVID-19 estimated that low-dose corticosteroid treatment seems to have satisfactory outcomes.52
A clinical trial (NCT04381936) suggested that dexamethasone was recognized to have an inhibitory effect against COVID-19 protease. Mortality rate decreases with low dose dexamethasone in patients receiving invasive ventilators by one-third and one-fifth for those on oxygen but showed no benefit in patients who did not require respiratory support.53 Moderate doses of methylprednisolone (80–100 mg), which is comparable to 15–19 mg of dexamethasone, can modify the immune response by occupying the GRα receptors. A prospective, Phase IV, randomized controlled trial (NCT04663555) recruits the patients to evaluate that 20 mg of dexamethasone is superior over 6 mg. An observational study is directed for COVID-19 patients with an age limit of more than 60 years to study the effect of corticosteroids. Using Cox regression, they analyze that low-dose corticosteroid therapy reduces the risk of death in patients who developed ARDS within 60 days. In this cohort, viral RNA clearance is not due to corticosteroid therapy.54
Contrary to the trials mentioned earlier, corticosteroids may not be beneficial in reducing mortality after a certain period.55 A multi-center randomized clinical trial (NCT00295269) was conducted and sponsored by National Heart, Lung, and Blood Institute (NHLBI) in patients with persistent ARDS. According to this RCT, methylprednisolone (2 mg/kg/d) for 21 days increases the number of ventilator-free and shock-free days. Thus, methylprednisolone could not be used for long-term treatment due to the adverse effects associated with corticosteroids.49,56 The findings of meta-analysis (of about 15 RCTs) have revealed that corticosteroids are associated with a decrease in mortality and progression of ARDS.57,58
Data from the above-mentioned clinical trials are conflicting because of the differences in pharmacological agents, dosing and timing of initiation and duration of treatment. Moreover, most of the clinical trials were conducted with mechanical ventilation; thus, it is unclear whether corticosteroids have significant benefits.
Statins
Statins are the inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMG-CoA) and are frequently used to treat hypercholesterolemia. The statins’ pleiotropic effect includes anti-inflammatory, immunomodulatory, and antithrombotic.59 Because of immunosuppressive properties, statins can reduce inflammation by modulating the TNF-α and NF-kB transcription factors. Some preliminary studies suggested that statins interfere with viral membrane receptors (ACE2) by up-regulating the ACE2 through epigenetic alterations. The clinical outcomes of patients with CARDS could be improved with statin as adjunctive therapy.
Statin prevents ARDS progression in many pre-clinical trials of murine models.60,61 Numerous studies and clinical trials also predict that statins can improve the survival of patients with ARDS. Prehospital use of statin and aspirin decreases sepsis and mortality rates as investigated in a cohort study.62 In healthy volunteers, pulmonary and systemic inflammation induce by inhalation of lipopolysaccharide can be reduced by pretreatment with simvastatin.63 As the ARDS is mainly caused by sepsis, statin could have a beneficial effect in improving the clinical course of sepsis-associated ARDS. The observational cohort studies also confirmed the assumption but only in patients who were already receiving simvastatin and atorvastatin.64,65 A randomized controlled trial recommends simvastatin as it improves respiratory mechanics by reducing pulmonary and systemic inflammation. Simvastatin (80 mg) lessened the level of IL-8 in the bronchoalveolar lavage of patients by 2.5-fold.66
Ulinastatin is an inhibitor of the serine protease (trypsin and α-chymotrypsin) and has been used to treat ARDS. Ulinastatin has anti-inflammatory activity as it decreases the elevation of interleukins andTNF-α produced by neutrophils.67 Several studies have shown its use in ARDS to reduce the duration of stay in the hospital, mortality rate and need for mechanical ventilation.68 Two randomized controlled trialsNCT03089957 and NCT02895191 (phase II) are enrolling the ARDS patients to examine the safety and efficacy of ulinastatin.
Many observational studies and controlled trials provide undesirable consequences of statin therapy in mechanically ventilated patients of ARDS.69,70 A meta-analysis of 13 studies described no noteworthy difference in the outcomes (ventilator-free days, oxygenation index and length of stay in hospital) after initiation of statin therapy.70 In a multi-center trial, rosuvastatin therapy causes hepatic and renal failure in the patients recruited (NCT00979121).71 In contrast to rosuvastatin, simvastatin therapy is safe and possesses fewer adverse effects. Therefore, simvastatin therapy was used for 28 days in Phase II, a multi-center, double-blind clinical trial (ISRCTN88244364) to improve the ventilator-free days in ARDS patients, but the results were negative as it did not mend the clinical outcomes.72
Although the intention of using statin in managing COVID-19 is debatable, it could be biologically credible. Older people with cardiovascular diseases are at greater risk of developing COVID-19. In a Phase III trial of RCTs, statins could be considered for the treatment of COVID-19 because of their cardio-protective effect.73 Atorvastatin (NCT04407273) mitigates the effect of SARS-CoV-2 infection and mortality.74 To inscribe the relation between statins and mortality rates in patients with COVID-19 a recent well-organized survey was conducted on 52,122 patients. The study shows that in-hospital use of statin was associated with a reduced risk of mortality.75 Nevertheless, there is a delay in administering statin in CARDS due to dearth of conclusive data on the use of statins in ARDS patients. The previous meta-analysis of 35 studies showed that statin did not give positive results in COVID-19 patients.76 Additional research is needed to illustrate the potential effect of statin therapy in ARDS.
Immunomodulatory Agents
Anti-IL-6 and anti-TNF treatments can suppress the important inflammatory cytokines in ALI, thus improving the clinical outcomes.Therefore the anti-IL-6 and anti-TNF therapy are worth considering. Many immunomodulatory agents improve the outcomes in clinical trials of CARDS, such as inhibitors of IL-6 (sarilumab, siltuximab and tocilizumab) and anti-TNF (infliximab, adalimumab, etanercept, afelimomab and golimumab).
Observational studies propose that IL-6 inhibitors have a convincing influence onCOVID-19 and lower mortality rate, as suggested by a meta-analysis of 9 studies.77 Sarilumab, an IL-6 antagonist, is a human monoclonal antibody (IgG1). It could act as a promising therapeutic agent by neutralizing the elevated IL-6 levels in ARDS patients. Many clinical trials (including NCT04324073) investigating the use of sarilumab (intravenously or subcutaneously) at a dose of 200mg or 400mg in patients with CARDS to assess the benefit-risk profile. Investigators also conducted a trial (NCT04330638) on the benefits of siltuximab (11 mg/kg) either alone or in combination with anakinra and tocilizumab with the results forthcoming.78 Tocilizumab is useful in CARDS at 8mg/kg dose.79 In China, tocilizumab (400mg) was approved for COVID-19 patients because of improved respiratory function in patients treated with tocilizumab. Its effectiveness worldwide is limited because of the lack of a comparator group.80,81 Tocilizumab reduces the biomarkers of COVID-19 and decreases the severity of COVID-19, as shown in a recent meta-analysis of 9 studies.82
During inflammation, many inflammatory mediators produce TNF-α (a multi-functional polypeptide) primarily by macrophages and monocytes. Anti-TNF therapy has potential benefits in severe sepsis,83 idiopathic pneumonia,84,85 COVID-19,86 and ventilator-induced lung injury (VILI) with positive outcomes and improved survival.87 In a pre-clinical study, the mortality rate is about 75% with anti-TNF therapy in an animal model of SARS-CoV-19.88 They inactivate the TNF-α andare effectively used in many inflammatory diseases like psoriatic arthritis and rheumatoid arthritis. Afelimomab therapy showed favorable outcomes in severe sepsis and improved mortality.83 In a study, the level of cytokines was tracked for 10 days in seven COVID-19 patients after a single dose of infliximab (5 mg/kg).86
Recently, adalimumab therapy has been approved in China to reduce ventilator-induced lung injury (VILI)87 and to prevent the development of community infection into respiratory failure; a trial of adalimumab is in the pre-enrollment phase (ISRCTN33260034).
Baricitinib’s antiviral effect is due to its ability to prevent SARS-CoV-2 from invading and infecting lung cells. Several RCTs (NCT04401579, NCT04421027) have shown thatCOVID-19 patients who were treated with baricitinib had better clinical outcomes.89,90 Many RCTs, including, NCT05074420 and NCT04970719are currently recruiting patients suffering from COVID-19 to evaluate the efficacy and safety of baricitinib.
Other immunomodulatory agents include GSK1995057, an anti-TNFreceptors monoclonal which lessened the pulmonary inflammation,91 and bevacizumab (vascular endothelial growth factor inhibitor) that reduced BAL protein levels and lung fluid.92 Atrial (NCT04275414) was completed on the use of bevacizumab for patients with SARS-CoV-2 pneumonia with the results forthcoming. Although several observational studies may support the use of anti-TNF, the results from several RCTs are still needed to confirm the benefits; thus, further research is encouraged.
Neuromuscular Blockers
Neuromuscular blockers (NMB) may exert their favorable effect with moderate or severe ARDS by preventing spontaneous breathing. Continuous cisatracurium therapy for 2 days is associated with improved oxygenation in patients with ARDS.93 In ARDS patients, the use of NMB lowers the proinflammatory cytokines and improves the PaO2/FiO2 ratio.94 A clinical trial (NCT00299650) evaluated that early administration of cisatracurium besylate in patients with severe ARDS enhances the time off the ventilator and improves survival without increasing muscle weakness.95 A meta-analysis of 3 RCTs piloted on critically ill adult patients suggested that cisatracurium besylate when given in continuous infusion, increases the survival rate consistently at 28 days, but does not affect the length of mechanical ventilation.96 The prolonged use of NMB is observed in a recent observational study that enrolled patients with COVID-19 induce ARDS. About 41% of patients received NMB for more than 2 days and the outcomes indicate no significant difference between the two groups indicating that prolonged use of NMB is not related to lower the extubation rate at 28 day.97
Elastase Inhibitors
Neutrophils are the type of white blood cells that make about 40–50% of total WBCs. Neutrophils and neutrophil derivatives exhibit the principal role in the underlying pathologic process responsible for ARDS.
Sivelestat – a selective inhibitor of leukocyte elastase – had been a point of consideration for ARDS treatment.98 However, an interventional, multi-center, and double-blind study (NCT00036062) for testing its efficacy in a broad spectrum of ALI and ARDS did not give any satisfactory results. Another interventional study for sivelestat sodium hydrate (NCT00219375) was conducted in Japan. Phase III and Phase IV studies considering the long-term use of sivelestat came out to be beneficial, resulting in improved pulmonary function, duration of stay in ICU, and the betterment of mechanical ventilation.99 In other studies conducted to check the efficacy, sivelestat has been proven effective in treating sepsis in ALI by reducing the alveoli function.100
In non-clinical studies, sivelestat was found beneficial without impacting the host’s immune system. However, not clear and convincing data regarding the efficacy of sivelestat in ALI/ARDS has been found. So, it can be stated that although certain evidence obtained from the research supports the efficacy of sivelestat when given for a long period, yet the results from some other trials did not prove it to be a good option for ARDS rendering the drug use to be controversial with no clear and expected results. As far as safety is concerned, no specific adverse effects or any clues for sivelestat to worsen the disease have been documented. In short, present data suggest that sivelestat can be beneficial in the treatment of pulmonary diseases, including ARDS/ALI, yet there is an extreme need of conducting randomized clinical trials at a larger scale and for a longer duration to check the efficacy and safety.99
While in the present condition of COVID-19, where the world is more concerned about pulmonary drugs, sivelestat has not yet been tested for SARS or COVID-19 infections. There is a need to check its efficacy and safety regarding use in COVID-19 so that it can be considered as an option for treatment.101 When the utility of another elastase inhibitor, AZD9668 was studied for bronchiectasis through a 4-week, randomized, double-blind phase II study (NCT00769119), it proved to be effective in reducing the sputum inflammatory biomarkers. However, for better evaluation, larger studies are required to confirm the associated benefits of sivelestat for the treatment of bronchiectasis.
Targeting Coagulating Cascade
Tissue factors (TF) are released in the alveolar space to initiate the extrinsic coagulation cascade, leading to thrombi and microthrombi formation, injury of vessels, and activate the platelets and WBCs via complement mediation. These tissue factors are dependent on coagulant action and the affiliated inflammation plays a vital role in worsening and developing ALI/ARDS. According to the studies, it was observed that TF levels were higher in the patients with ARDS and ALI. In contrast to these conditions, the TF levels in patients with pulmonary edema were low. Elevated TF-levels in ARDS/ALI were a significant cause behind the high mortality rates with fewer ventilator-free days. This situation was backed by intravascular coagulation and septic conditions in ARDS and ALI patients. Hence, all these apparent situations suggested that the coagulation cascade supported by TF factors is an important factor in worsening these conditions leading to higher mortality rates. Thus, it can be inferred that to maintain the levels of TF factors, the blockade by anti-TF antibody can be beneficial therapy to prevent the coagulation and resulting worsening of the condition.
In a prospective, randomized, multi-center, double-blind, phase II study, the safety and effectiveness of anti-TF antibody (ALT-836) was checked in the septic patients with ALI/ARDS. Desired outcomes were the shortening of the duration of mechanical ventilation for these patients with ARDS/ALI. ALT-836, a recombinant chimeric anti-tissue factor antibody that binds to TF or TF-Factor VIII complex was tested in patients with ARDS/ALI against placebo (NCT00879606) and the results provided there are no safety concerns. At the same time, the final results regarding efficacy are still awaited. Another clinical study checked the safety and efficacy of active site-inactivated recombinant factor VIIa (FFR-rFVIIa) in patients with ARDS. In this phase II, multicentered, randomized, double-blind, placebo-controlled study, the outcome parameters were coagulation related, ventilator-free days, lung injury score, and vital signs. However, the Safety Committee discontinued the study prematurely because of increased bleeding complications with an increase in the FFR-rFVIIa dose in the patients. While the effect FFR-rFVIIa on concerning vital signs was not satisfactory.102
Another treatment option for targeting the coagulation cascade is heparin. In the present COVID-19 conditions, there is an increased risk associated with the lungs. Randomized, interventional clinical studies of nebulized heparin (NCT04397510) for treatment of CARDS are ongoing recently.103 Nebulized heparin was supposed to be associated with reduced pulmonary inflammation and fibrin deposition. However, it did not come out according to a study where it was associated with fewer days of mechanical ventilation. However, it did not worsen the condition or no adverse events resulted from heparin. However, further studies need to be conducted to check the efficacy of heparin in the treatment of ARDS/ALI. As platelet activation has a vital role in the pathogenesis of ARDS and aspirin with a statin has been associated with a decrease in ARDS severity.
In a propensity-adjusted analysis for testing the prehospital effectiveness of aspirin in ARDS patients, it came out to be associated with decreased risks of ARDS. However, there is a need for prospective clinical trials to check the benefits of preventing ARDS.104 A phase II randomized control trial (STAR) to test aspirin as a treatment of ARDS (NCT02326350) was terminated because of very slow recruitment, while another clinical trial (ARENA NCT01659307) for using aspirin in ARDS is recruiting the individuals for checking the oxygenation index of patients. In an interventional phase II study, the evaluation of early aspirin for lung injury prevention was performed (NCT01504867). The results did not support the conduction of the phase III study because of no visible betterment in the condition of the condition patients with ARDS.105 Moreover, to find the treatment for ARDS, recombinant human activated protein C (Xigris) was checked by randomized clinical trials (NCT00112164) in human beings but was terminated because of negative outcomes in the patients with ARDS and sepsis.106
Focusing the Growth Factors
ALI/ARDS can be reversed if there is hastened repair and regeneration of epithelium in such patients. Certain growth factors such as KGF have been observed to reduce and repair lung injury in the animal models of ARDS. When tested in human models against placebo, this KGF produced no alteration in the infiltration of biomarkers. It increases the proliferation of type 2 alveolar cells to repair the injury that occurred to alveoli during ARDS. Although previously, the KFG (Palifermin) has been effective in human models of ARDS107 according to the results of more recent, randomized, double-blind, placebo-controlled phase II clinical trial, the KGF did not improve the physiological and clinical outcomes and due to chances of being harmful, cannot be recommended to use in ARDS.108
While another randomized, double-blind study for testing the safety and efficacy of mesenchymal stromal cells in the patients with ARDS is continued (NCT03818854) that is a continuation of a previous study (NCT01775774). A randomized trial of recombinant human granulocyte-macrophage colony-stimulating factor (GM-CSF) in patients with ARDS was conducted, resulting in no satisfactory outcomes. GM-CSF did not increase the ventilator-free days at that study level and there is a requirement to conduct the trials at larger levels for proper outcomes.109
Meanwhile, there is another ongoing trial (NCT02595060) to check the inhaled granulocyte-macrophage colony-stimulating growth factors (rhGM-CSF, Molgramostim). A randomized, double-blind, ascending-dose, Phase I study (NCT02468908) for inhaled molgramostim in patients with ARDS has been completed while the results are being awaited. Two other clinical trials (NCT00319631 and NCT01314066) checked the efficacy and safety of vascular endothelial growth factors in ARDS but had to be stopped because of poor enrollment and funding issues.
Miscellaneous Agents
Ascorbic acid (Vitamin C) is an essential water-soluble antioxidant that has a significant role in decreasing the disastrous effects of reactive oxidation species that are the reason for increased oxidative stress resulting in damage to macromolecules. According to the data obtained from the most recent clinical studies, high doses of ascorbic acid have essential effects in protecting against oxidative stress due to critical illness, as happens in ARDS/ALI. Vitamin C significantly improves the functioning of the immune system and improves tissue perfusion and reduces tissue hypoxia and subsequent organ dysfunction.
Many randomized, interventional clinical studies (NCT03780933, NCT04710329, and NCT04357782) were conducted to check the efficacy of a high dose of vitamin C in critically ill patients with ARDS and COVID-19. Although the studies have been completed, yet the results are awaited. While the study of infused ascorbic acid for the treatment of sepsis and organ failure in patients with lung injury (NCT02106975) showed that a 96-hour infusion of vitamin C did not significantly improve organ failure and vascular injury. Recently, an interventional trial (NCT04344184) is enrolling participants who have a confirmed SARS-CoV-2 infection in order to determine the impact of vitamin C. Thus, more studies are required for understanding the role of ascorbic acid in sepsis and ARDS.110
Vitamin D plays a vital role in the pathogenesis of long-term morbidities due to the newborn’s respiratory distress syndrome (RDS). An observational, cohort, prospective study (NCT01812681) was completed to check the role of low and normal vitamin D levels in newborns’ RDS. The results indicated that decreased cord blood 25(OH)D values might be related with an enhanced danger of RDS in low birth weight infants.111 In a recent meta-analysis of 11 studies, vitamin D administration was associated with enhanced benefits, including relatively low ICU admission, less use of mechanical ventilation, and decreased COVID-19 mortality rate.112 Many RCTs, including phase III trials (NCT04536298&NCT04385940) and a phase IV trial (NCT04552951), are recruiting patients to determine if vitamin D lowers the severity of illness in the participants with COVID-19.
N-acetylcysteine (NAC) and procysteine assist in enhancing the level of glutathione and better oxygenation of the airways,113 rendering these a promising therapy for ARDS.114 Recently, a clinical trial (NCT04570254) was completed to evaluate the effect of NAC, vitamin C, melatonin, and vitamin E in COVID-19 subjects, with the findings expected soon.
Insulin has shown an anti-inflammatory response by inhibiting the nuclear factor-kappa B (NF-κB). To further confirm the effects of insulin in ARDS, a phase II trial (NCT00605696) of insulin therapy in the prevention of ARDS has been completed, while the results of the trial are being awaited. In ARDS/ALI the major complication is inflammation that has life-threatening outcomes. An interventional, randomized, phase II clinical trial (NCT00605696) consisting of the study of the effects of insulin at low and high doses to prevent the complications associated with ARDS/ALI, and the results are awaited. A recent meta-analysis of 18 studies has suggested that insulin-treated patients with COVID-19 may experience an increased risk of mortality as well as severe symptoms.115 Therefore, clinicians should be more vigilant or use additional care while dealing with diabetic patients who are on insulin treatment.115,116
Several studies have shown that ivermectin has antiviral efficacy against a variety of viruses, in addition to its anti-parasitic properties. It has also been proposed that ivermectin may be beneficial in enhancing the COVID-19 endpoints, owing to its influence on the inhibition of SARS-CoV-2 proteins from accessing the host cell nucleus. According to a meta-analysis of 19 studies, ivermectin seems to have a beneficial effect on COVID-19 results (including alleviations of symptoms, hospital stay, severity and mortality rate).117
Colchicine exhibits anti-inflammatory effects that may help alleviate the cytokine storm by inhibiting the activation of IL-1, IL-6, and IL-18. Nevertheless, the justification for a relation between colchicine administration and COVID-19 is still inconclusive. The findings of meta-analysis (about 8 studies) support the regular use of colchicine in the management of COVID-19 patients.118 Furthermore, numerous trials (NCT04375202, NCT04360980, NCT04492358, NCT04818489) are enrolling COVID-19 patients to see if colchicine has a potential effect on COVID-19 sufferers.
Other treatment strategies that have been considered include, inhaled NO, exogenous surfactants, prostaglandin, omega 3, sodium nitroprusside, furosemide, beta 2 agonists, and calfactant and there is a need for further testing by focusing on some drug combinations or modified doses. While several ongoing clinical trials are focusing on the efficacy and safety of certain agents, including inhaled carbon monoxide, HCR040, intravenous Wharton’s jelly derived mesenchymal stem cells, iloprost, brexanolone in COVID-19, angiotensin II in COVID-19, PLN-78809, vadadustat, sevoflurane, propofol, LEAF-4L6715, HLCM051, poractant alfa, alteplase and several others mentioned in Table 2. Researchers hope to get some positive outcomes from the results of these clinical trials as until now there are no satisfactory results regarding the treatment of ARDS/ALI, especially in the time where COVID-19 is also participating in the worsening of such pulmonary conditions.
Conclusion
ARDS and COVID-19 share a close relationship as both are predators of the respiratory system, and both have gained the status of a “Bermuda Triangle” in the field of drug development because no appropriate treatment is available. The most-focused treatment strategies include sivelestat, mesenchymal stem cells, corticosteroids, aspirin, heparin, and iloprost. Innovative therapeutic techniques such as gene therapy and targeting immunology must also be considered and applied while the most likely candidates with improved outcomes for CARDS include dexamethasone, baricitinib, tocilizumab, and heparin. Moreover, animal modeling appropriation, different designs for clinical trials, several prognostic and predictive techniques along with the application of more advanced and realistic therapies as well as analytical approaches for reduction of heterogenicity can be favorable to come out with some safe and effective therapy for ARDS and COVID-19.
Abbreviations
ARDS, acute respiratory distress syndrome; ALI, acute lung injury; CARDS, COVID-19-related ARDS; PEEP, positive end-expiratory pressure; DAD, diffuse alveolar damage; BALF, bronchoalveolar lavage fluid; ICAM-1, intercellular adhesion molecule-1; IL-1β, interleukins; TNF-α, tumor necrosis factor-α; MMPs, matrix metalloproteinases; VEGF, vascular endothelial growth factor; KGF, keratinocyte growth factor; HGF, hepatocyte growth factor; RCT, randomized clinical trials; NMB, neuromuscular blockers; TF, tissue factors; GM-CSF, granulocyte-macrophage colony-stimulating factor; NF-κB, nuclear factor kappa B.
Ethics Approval
Not applicable.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article was submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The authors are thankful to King Khalid University (KKU), Saudi Arabia for providing financial support through the Small Research Program (Grant Approval Number: 275/1442).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
2. Schmidt M, Hajage D, Demoule A, et al. Clinical characteristics and day-90 outcomes of 4244 critically ill adults with COVID-19: a prospective cohort study. Intensive Care Med. 2021;47(1):60–73. doi:10.1007/s00134-020-06294-x
3. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA. 2020;323(20):2052–2059. doi:10.1001/jama.2020.6775
4. Docherty AB, Harrison EM, Green CA, et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: prospective observational cohort study. BMJ. 2020;369:m1985. doi:10.1136/bmj.m1985
5. Tzotzos SJ, Fischer B, Fischer H, Zeitlinger M. Incidence of ARDS and outcomes in hospitalized patients with COVID-19: a global literature survey. Crit Care. 2020;24(1):516. doi:10.1186/s13054-020-03240-7
6. Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med. 1994;149(3 Pt 1):818–824. doi:10.1164/ajrccm.149.3.7509706
7. Ferguson ND, Fan E, Camporota L, et al. The Berlin definition of ARDS: an expanded rationale, justification, and supplementary material. Intensive Care Med. 2012;38(10):1573–1582. doi:10.1007/s00134-012-2682-1
8. Riviello ED, Kiviri W, Twagirumugabe T, et al. Hospital incidence and outcomes of the acute respiratory distress syndrome using the Kigali modification of the Berlin definition. Am J Respir Crit Care Med. 2016;193(1):52–59. doi:10.1164/rccm.201503-0584OC
9. Tan W, Zhao X, Ma X, et al. A novel coronavirus genome identified in a cluster of pneumonia cases - Wuhan, China 2019–2020. China CDC Weekly. 2020;2(4):61–62. doi:10.46234/ccdcw2020.017
10. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
11. Sungnak W, Huang N, Becavin C, et al. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med. 2020;26(5):681–687. doi:10.1038/s41591-020-0868-6
12. Xu W, Sun -N-N, Gao H-N, et al. Risk factors analysis of COVID-19 patients with ARDS and prediction based on machine learning. Sci Rep. 2021;11(1):2933. doi:10.1038/s41598-021-82492-x
13. Gattinoni L, Marini J, Pesenti A, Quintel M, Mancebo J, Brochard L. The ”baby lung” became an adult. Intensive Care Med. 2016;42(5):663–673. doi:10.1007/s00134-015-4200-8
14. Lascarrou J-B. COVID-19-related ARDS: one disease, two trajectories, and several unanswered questions. Lancet Respir Med. 2021. doi:10.1016/S2213-2600(21)00381-7
15. Tanner T, Offor OL, You JY, Hope AA, Gong MN, Chen J-T. Descriptive comparison between pre-COVID ARDS and COVID-19 related ARDS.
16. Li L, Li R, Wu Z, et al. Therapeutic strategies for critically ill patients with COVID-19. Ann Intensive Care. 2020;10(1):45. doi:10.1186/s13613-020-00661-z
17. Li X, Ma X. Acute respiratory failure in COVID-19: is it ”typical” ARDS? Crit Care. 2020;24(1):198. doi:10.1186/s13054-020-02911-9
18. Van Haren F, Page C, Laffey J, et al. Nebulised heparin as a treatment for COVID-19: scientific rationale and a call for randomised evidence. Critical Care. 2020;24:24. doi:10.1186/s13054-020-03148-2
19. Gattinoni L, Pelosi P, Suter PM, Pedoto A, Vercesi P, Lissoni A. Acute respiratory distress syndrome caused by pulmonary and extrapulmonary disease. Different syndromes? Am J Respir Crit Care Med. 1998;158(1):3–11. doi:10.1164/ajrccm.158.1.9708031
20. Diamond M, Peniston Feliciano HL, Sanghavi D, Mahapatra S. Acute Respiratory Distress Syndrome. StatPearls Publishing Copyright © 2021, StatPearls Publishing LLC; 2021.
21. Moss M, Guidot DM, Steinberg KP, et al. Diabetic patients have a decreased incidence of acute respiratory distress syndrome. Crit Care Med. 2000;28(7):2187–2192. doi:10.1097/00003246-200007000-00001
22. Moss M, Bucher B, Moore FA, Moore EE, Parsons PE. The role of chronic alcohol abuse in the development of acute respiratory distress syndrome in adults. JAMA. 1996;275(1):50–54. doi:10.1001/jama.1996.03530250054027
23. Liu C, Li J. Role of genetic factors in the development of acute respiratory distress syndrome. J Transl Int Med. 2015;2(3):107–110. doi:10.4103/2224-4018.141831
24. Meyer NJ, Christie JD. Genetic heterogeneity and risk of acute respiratory distress syndrome. Semin Respir Crit Care Med. 2013;34(4):459–474. doi:10.1055/s-0033-1351121
25. Kuba K, Imai Y, Rao S, et al. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus–induced lung injury. Nat Med. 2005;11(8):875–879. doi:10.1038/nm1267
26. Hussain M, Jabeen Q, Ahmad F, et al. COVID-19 and inhibitors of the renin–angiotensin–aldosterone system. Expert Rev Anti Infect Ther. 2021;19(7):815–816. doi:10.1080/14787210.2021.1851197
27. Zhu R-F, Gao Y-L, Robert S-H, Gao J-P, Yang S-G, Zhu C-T. Systematic review of the registered clinical trials for coronavirus disease 2019 (COVID-19). J Transl Med. 2020;18(1):274. doi:10.1186/s12967-020-02442-5
28. Pfortmueller CA, Spinetti T, Urman RD, Luedi MM, Schefold JC. COVID-19-associated acute respiratory distress syndrome (CARDS): current knowledge on pathophysiology and ICU treatment – a narrative review. Best Pract Res Clin Anaesthesiol. 2021;35(3):351–368. doi:10.1016/j.bpa.2020.12.011
29. Thompson BT, Chambers RC, Liu KD. Acute Respiratory Distress Syndrome. N Engl J Med. 2017;377(6):562–572. doi:10.1056/NEJMra1608077
30. Matthay MA, Zemans RL. The acute respiratory distress syndrome: pathogenesis and treatment. Annu Rev Pathol. 2011;6:147–163. doi:10.1146/annurev-pathol-011110-130158
31. Ware LB. Pathophysiology of acute lung injury and the acute respiratory distress syndrome. Semin Respir Crit Care Med. 2006;27(4):337–349. doi:10.1055/s-2006-948288
32. Greene KE, Wright JR, Steinberg KP, et al. Serial changes in surfactant-associated proteins in lung and serum before and after onset of ARDS. Am J Respir Crit Care Med. 1999;160(6):1843–1850. doi:10.1164/ajrccm.160.6.9901117
33. Fremont RD, Koyama T, Calfee CS, et al. Acute lung injury in patients with traumatic injuries: utility of a panel of biomarkers for diagnosis and pathogenesis. J Trauma. 2010;68(5):1121–1127. doi:10.1097/TA.0b013e3181c40728
34. Ware LB, Koyama T, Billheimer DD, et al. Prognostic and pathogenetic value of combining clinical and biochemical indices in patients with acute lung injury. Chest. 2010;137(2):288–296. doi:10.1378/chest.09-1484
35. Terpstra ML, Aman J, van Nieuw Amerongen GP, Groeneveld AB. Plasma biomarkers for acute respiratory distress syndrome: a systematic review and meta-analysis*. Crit Care Med. 2014;42(3):691–700. doi:10.1097/01.ccm.0000435669.60811.24
36. Binnie A, Tsang JL, Dos Santos CC. Biomarkers in acute respiratory distress syndrome. Curr Opin Crit Care. 2014;20(1):47–55. doi:10.1097/mcc.0000000000000048
37. Sweeney TE, Khatri P. Generalizable biomarkers in critical care: toward precision medicine. Crit Care Med. 2017;45(6):934–939. doi:10.1097/ccm.0000000000002402
38. Albertine KH, Soulier MF, Wang Z, et al. Fas and fas ligand are up-regulated in pulmonary edema fluid and lung tissue of patients with acute lung injury and the acute respiratory distress syndrome. Am J Pathol. 2002;161(5):1783–1796. doi:10.1016/s0002-9440(10)64455-0
39. Bos LD, Weda H, Wang Y, et al. Exhaled breath metabolomics as a noninvasive diagnostic tool for acute respiratory distress syndrome. Eur Respir J. 2014;44(1):188–197. doi:10.1183/09031936.00005614
40. Raghavendran K, Pryhuber GS, Chess PR, Davidson BA, Knight PR, Notter RH. Pharmacotherapy of acute lung injury and acute respiratory distress syndrome. Curr Med Chem. 2008;15(19):1911–1924. doi:10.2174/092986708785132942
41. Weigelt JA, Norcross JF, Borman KR, Snyder WH
42. Bernard GR, Luce JM, Sprung CL, et al. High-dose corticosteroids in patients with the adult respiratory distress syndrome. N Engl J Med. 1987;317(25):1565–1570. doi:10.1056/NEJM198712173172504
43. Luce JM, Montgomery AB, Marks JD, Turner J, Metz CA, Murray JF. Ineffectiveness of high-dose methylprednisolone in preventing parenchymal lung injury and improving mortality in patients with septic shock. Am Rev Respir Dis. 1988;138(1):62–68. doi:10.1164/ajrccm/138.1.62
44. Kido T, Muramatsu K, Asakawa T, et al. The relationship between high-dose corticosteroid treatment and mortality in acute respiratory distress syndrome: a retrospective and observational study using a nationwide administrative database in Japan. BMC Pulm Med. 2018;18(1):28. doi:10.1186/s12890-018-0597-5
45. Annane D, Sébille V, Bellissant E. Effect of low doses of corticosteroids in septic shock patients with or without early acute respiratory distress syndrome. Crit Care Med. 2006;34(1):22–30. doi:10.1097/01.ccm.0000194723.78632.62
46. Liu L, Li J, Huang YZ, et al. [The effect of stress dose glucocorticoid on patients with acute respiratory distress syndrome combined with critical illness-related corticosteroid insufficiency]. Zhonghua Nei Ke Za Zhi. 2012;51(8):599–603. Chinese.
47. Hirano Y, Madokoro S, Kondo Y, Okamoto K, Tanaka H. Corticosteroid treatment for early acute respiratory distress syndrome: a systematic review and meta-analysis of randomized trials. J Intensive Care. 2020;8(1):91. doi:10.1186/s40560-020-00510-y
48. Tongyoo S, Permpikul C, Mongkolpun W, et al. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: results of a randomized controlled trial. Crit Care. 2016;20(1):329. doi:10.1186/s13054-016-1511-2
49. Meduri GU, Golden E, Freire AX, et al. Methylprednisolone infusion in early severe ARDS: results of a randomized controlled trial. Chest. 2007;131(4):954–963. doi:10.1378/chest.06-2100
50. Villar J, Ferrando C, Martínez D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicentre, randomised controlled trial. Lancet Respir Med. 2020;8(3):267–276. doi:10.1016/s2213-2600(19)30417-5
51. Festic E, Carr GE, Cartin-Ceba R, et al. Randomized Clinical Trial of a Combination of an Inhaled Corticosteroid and Beta Agonist in Patients at Risk of Developing the Acute Respiratory Distress Syndrome*. Crit Care Med. 2017;45(5):798–805. doi:10.1097/ccm.0000000000002284
52. Hasan SS, Capstick T, Ahmed R, et al. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: a systematic review and meta-analysis. Expert Rev Respir Med. 2020;14(11):1149–1163. doi:10.1080/17476348.2020.1804365
53. Noreen S, Maqbool I, Madni A. Dexamethasone: therapeutic potential, risks, and future projection during COVID-19 pandemic. Eur J Pharmacol. 2021;894:173854. doi:10.1016/j.ejphar.2021.173854
54. Wu C, Hou D, Du C, et al. Corticosteroid therapy for coronavirus disease 2019-related acute respiratory distress syndrome: a cohort study with propensity score analysis. Crit Care. 2020;24(1):643. doi:10.1186/s13054-020-03340-4
55. Meduri G, Chinn A, Leeper K, et al. Corticosteroid rescue treatment of progressive fibroproliferation in late ARDS. Chest. 1994;105:1516–1527. doi:10.1378/chest.105.5.1516
56. Steinberg KP, Hudson LD, Goodman RB, et al. Efficacy and safety of corticosteroids for persistent acute respiratory distress syndrome. N Engl J Med. 2006;354(16):1671–1684. doi:10.1056/NEJMoa051693
57. Pulakurthi YS, Pederson JM, Saravu K, et al. Corticosteroid therapy for COVID-19: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2021;100(20):e25719. doi:10.1097/md.0000000000025719
58. Ma S, Xu C, Liu S, et al. Efficacy and safety of systematic corticosteroids among severe COVID-19 patients: a systematic review and meta-analysis of randomized controlled trials. Signal Transduction Targeted Therapy. 2021;6(1):83. doi:10.1038/s41392-021-00521-7
59. Lee KCH, Sewa DW, Phua GC. Potential role of statins in COVID-19. Int J Infect Dis. 2020;96:615–617. doi:10.1016/j.ijid.2020.05.115
60. Jacobson JR, Barnard JW, Grigoryev DN, Ma SF, Tuder RM, Garcia JG. Simvastatin attenuates vascular leak and inflammation in murine inflammatory lung injury. Am J Physiol Lung Cell Mol Physiol. 2005;288(6):L1026–32. doi:10.1152/ajplung.00354.2004
61. Jain MK, Ridker PM. Anti-inflammatory effects of statins: clinical evidence and basic mechanisms. Nat Rev Drug Discov. 2005;4(12):977–987. doi:10.1038/nrd1901
62. O’Neal HRJ, Koyama T, Koehler EAS, et al. Prehospital statin and aspirin use and the prevalence of severe sepsis and acute lung injury/acute respiratory distress syndrome*. Crit Care Med. 2011;39(6):1343–1350. doi:10.1097/CCM.0b013e3182120992
63. Shyamsundar M, McKeown STW, O’Kane CM, et al. Simvastatin Decreases Lipopolysaccharide-induced Pulmonary Inflammation in Healthy Volunteers. Am J Respir Crit Care Med. 2009;179(12):1107–1114. doi:10.1164/rccm.200810-1584OC
64. Mansur A, Steinau M, Popov AF, et al. Impact of statin therapy on mortality in patients with sepsis-associated acute respiratory distress syndrome (ARDS) depends on ARDS severity: a prospective observational cohort study. BMC Med. 2015;13(1):128. doi:10.1186/s12916-015-0368-6
65. Kruger P, Bailey M, Bellomo R, et al. A multicenter randomized trial of atorvastatin therapy in intensive care patients with severe sepsis. Am J Respir Crit Care Med. 2013;187(7):743–750. doi:10.1164/rccm.201209-1718OC
66. Craig TR, Duffy MJ, Shyamsundar M, et al. A Randomized Clinical Trial of Hydroxymethylglutaryl– coenzyme A Reductase Inhibition for Acute Lung Injury (The HARP Study). Am J Respir Crit Care Med. 2011;183(5):620–626. doi:10.1164/rccm.201003-0423OC
67. Zhang X, Zhu Z, Jiao W, Liu W, Liu F, Zhu X. Ulinastatin treatment for acute respiratory distress syndrome in China: a meta-analysis of randomized controlled trials. BMC Pulm Med. 2019;19(1):196. doi:10.1186/s12890-019-0968-6
68. Leng YX, Yang SG, Song YH, Zhu X, Yao GQ. Ulinastatin for acute lung injury and acute respiratory distress syndrome: a systematic review and meta-analysis. World J Crit Care Med. 2014;3(1):34–41. doi:10.5492/wjccm.v3.i1.34
69. Gao X-Q, Li Y-F, Jiang Z-L. Impact of statins on ALI/ARDS: a meta-analysis. Pulm Pharmacol Ther. 2016;39:85–91. doi:10.1016/j.pupt.2016.06.010
70. Xiong B, Wang C, Tan J, et al. Statins for the prevention and treatment of acute lung injury and acute respiratory distress syndrome: a systematic review and meta-analysis. Respirology. 2016;21(6):1026–1033. doi:10.1111/resp.12820
71. Truwit JD, Bernard GR, Steingrub J, et al. Rosuvastatin for sepsis-associated acute respiratory distress syndrome. N Engl J Med. 2014;370(23):2191–2200. doi:10.1056/NEJMoa1401520
72. McAuley DF, Laffey JG, O’Kane CM, et al. Simvastatin in the Acute Respiratory Distress Syndrome. N Eng J Med. 2014;371(18):1695–1703. doi:10.1056/NEJMoa1403285
73. Castiglione V, Chiriacò M, Emdin M, Taddei S, Vergaro G. Statin therapy in COVID-19 infection. Eur Heart J. 2020;6(4):258–259. doi:10.1093/ehjcvp/pvaa042
74. Masana L, Correig E, Rodríguez-Borjabad C, et al. EFFECT oF STATIN THERAPY oN SARS-CoV-2 INFECTION-RELATED. Eur Heart J Cardiovasc Pharmacother. 2020. doi:10.1093/ehjcvp/pvaa128
75. Permana H, Huang I, Purwiga A, et al. In-hospital use of statins is associated with a reduced risk of mortality in coronavirus-2019 (COVID-19): systematic review and meta-analysis. Pharmacol Rep. 2021;73(3):769–780. doi:10.1007/s43440-021-00233-3
76. Hariyanto TI, Kurniawan A. Statin and outcomes of coronavirus disease 2019 (COVID-19): a systematic review, meta-analysis, and meta-regression. Nutrition, Metab Cardiovas Dis. 2021;31(6):1662–1670. doi:10.1016/j.numecd.2021.02.020
77. Aziz M, Fatima R, Assaly R. Elevated interleukin-6 and severe COVID-19: a meta-analysis. J Med Virol. 2020;92(11):2283–2285. doi:10.1002/jmv.25948
78. Maes B, Bosteels C, De Leeuw E, et al. Treatment of severely ill COVID-19 patients with anti-interleukin drugs (COV-AID): a structured summary of a study protocol for a randomised controlled trial. Trials. 2020;21(1):468. doi:10.1186/s13063-020-04453-5
79. Mehta P, McAuley DF, Brown M, Sanchez E, Tattersall RS, Manson JJ. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1033–1034. doi:10.1016/s0140-6736(20)30628-0
80. Stone JH, Frigault MJ, Serling-Boyd NJ, et al. Efficacy of Tocilizumab in Patients Hospitalized with Covid-19. N Eng J Med. 2020;383(24):2333–2344. doi:10.1056/NEJMoa2028836
81. Hermine O, Mariette X, Tharaux P-L, et al. Effect of Tocilizumab vs Usual Care in Adults Hospitalized With COVID-19 and Moderate or Severe Pneumonia: a Randomized Clinical Trial. JAMA Intern Med. 2021;181(1):32–40. doi:10.1001/jamainternmed.2020.6820
82. Ivan Hariyanto T, Kurniawan A. Tocilizumab administration is associated with the reduction in biomarkers of coronavirus disease 2019 infection. J Med Virol. 2021;93(3):1832–1836. doi:10.1002/jmv.26698
83. Panacek EA, Marshall JC, Albertson TE, et al. Efficacy and safety of the monoclonal anti-tumor necrosis factor antibody F(ab’)2 fragment afelimomab in patients with severe sepsis and elevated interleukin-6 levels. Crit Care Med. 2004;32(11):2173–2182. doi:10.1097/01.ccm.0000145229.59014.6c
84. Yanik GA, Grupp SA, Pulsipher MA, et al. TNF-receptor inhibitor therapy for the treatment of children with idiopathic pneumonia syndrome. A joint Pediatric Blood and Marrow Transplant Consortium and Children’s Oncology Group Study (ASCT0521). Biol Blood Marrow Transplant. 2015;21(1):67–73. doi:10.1016/j.bbmt.2014.09.019
85. Yanik GA, Ho VT, Levine JE, et al. The impact of soluble tumor necrosis factor receptor etanercept on the treatment of idiopathic pneumonia syndrome after allogeneic hematopoietic stem cell transplantation. Blood. 2008;112(8):3073–3081. doi:10.1182/blood-2008-03-143412
86. Stallmach A, Kortgen A, Gonnert F, Coldewey SM, Reuken P, Bauer M. Infliximab against severe COVID-19-induced cytokine storm syndrome with organ failure—a cautionary case series. Critical Care. 2020;24(1):444. doi:10.1186/s13054-020-03158-0
87. Correger E, Marcos J, Laguens G, Stringa P, Cardinal-Fernández P, Blanch L. Tratamento prévio com adalimumabe reduz lesão pulmonar induzida por ventilação mecânica em um modelo experimental. Revista Brasileira de Terapia Intensiva. 2020;32:58–65. doi:10.5935/0103-507x.20200010
88. Channappanavar R, Fehr AR, Vijay R, et al. Dysregulated Type I Interferon and Inflammatory Monocyte-Macrophage Responses Cause Lethal Pneumonia in SARS-CoV-Infected Mice. Cell Host Microbe. 2016;19(2):1520–1529. doi:10.1164/rccm.201310-1892OC
89. Kalil AC, Patterson TF, Mehta AK, et al. Baricitinib plus Remdesivir for Hospitalized Adults with Covid-19. N Eng J Med. 2020;384(9):795–807. doi:10.1056/NEJMoa2031994
90. Marconi VC, Ramanan AV, de Bono S, et al. Efficacy and safety of baricitinib for the treatment of hospitalised adults with COVID-19 (COV-BARRIER): a randomised, double-blind, parallel-group, placebo-controlled Phase 3 trial. Lancet Respir Med. 2021. doi:10.1016/S2213-2600(21)00331-3
91. Proudfoot AG, O’Kane CM, Bayliffe A, et al. A Novel TNFR1-Targeting Domain Antibody Attenuates Pulmonary Inflammation In A Human Model Of Lung Injury, Via Actions On The Lung Micro-Vascular Endothelium.
92. Watanabe M, Boyer JL, Crystal RG. Genetic delivery of bevacizumab to suppress vascular endothelial growth factor-induced high-permeability pulmonary edema. Hum Gene Ther. 2009;20(6):598–610. doi:10.1089/hum.2008.169
93. Gainnier M, Roch A, Forel JM, et al. Effect of neuromuscular blocking agents on gas exchange in patients presenting with acute respiratory distress syndrome. Crit Care Med. 2004;32(1):113–119. doi:10.1097/01.Ccm.0000104114.72614.Bc
94. Forel JM, Roch A, Marin V, et al. Neuromuscular blocking agents decrease inflammatory response in patients presenting with acute respiratory distress syndrome. Crit Care Med. 2006;34(11):2749–2757. doi:10.1097/01.Ccm.0000239435.87433.0d
95. Papazian L, Forel J-M, Gacouin A, et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N Eng J Med. 2010;363(12):1107–1116. doi:10.1056/NEJMoa1005372
96. Alhazzani W, Alshahrani M, Jaeschke R, et al. Neuromuscular blocking agents in acute respiratory distress syndrome: a systematic review and meta-analysis of randomized controlled trials. Critical Care. 2013;17(2):R43. doi:10.1186/cc12557
97. Courcelle R, Gaudry S, Serck N, Blonz G, Lascarrou JB, Grimaldi D. Neuromuscular blocking agents (NMBA) for COVID-19 acute respiratory distress syndrome: a multicenter observational study. Critical Care. 2020;24:24. doi:10.1186/s13054-020-03164-2
98. Fukimbara S, Niibe K, Yamamoto M, Yamaguchi T. Adjustment for propensity score in nonrandomized clinical studies: comparison of sivelestat versus conventional therapy for acute respiratory distress syndrome. Therapeutic Innovatio Regulatory Sci. 2017;5(1):89–99. doi:10.1177/2168479016659103
99. Endo S, Sato N, Yaegashi Y, et al. Sivelestat sodium hydrate improves septic acute lung injury by reducing alveolar dysfunction. Res Commun Mol Pathol Pharmacol. 2006;119(1–6):53–65.
100. Sahchbnasagh A, Saghafi F, Safdari M, et al. Neutrophil Elastase Inhibitor (Sivelestat), may be a Promising Therapeutic Option for Management of Acute Lung Injury/Acute Respiratory Distress Syndrome or Disseminated Intravascular Coagulation in COVID-19. Authorea. 2020;4:548.
101. Stockley R, DeSoyza A, Gunawardena K, et al. Phase 2 study of a neutrophil elastase inhibitor (AZD9668} in patients with bronchiectasis. Respir Med. 2013;107(4):524–533. doi:10.1016/j.rmed.2012.12.009
102. Edwards A, Taggart C, Elborn J, Calfee CS, Matthay MA, O’Kane C. Keratinocyte growth factor promotes epithelial survival and resolution in a human model of lung injury. Am J Respir Crit Care Med. 2014;189(12):1520–1529. doi:10.1164/rccm.201310-1892OC
103. Dixon B, Schultz MJ, Smith R, Fink JB, Santamria JD, Campbell DJ. Nebulized heparin is associated with fewer days of mechanical ventilation in critically ill patients: a randomized controlled trial. Critical Care. 2010;14(5):180. doi:10.1186/cc9286
104. Chen W, Janz DR, Bastarache JA, et al. Prehospital aspirin use is associated with reduced risk of acute respiratory distress syndrome in critically ill patients: a propensity-adjusted analysis. Crit Care Med. 2015;43(4):801–807. doi:10.1097/CCM.0000000000000789
105. Kor DJ, Carter RE, Park PK, et al. Lung injury prevention with aspirin on Development of ARDS in At-Risk Patients Presenting to the Emergency Department: the LIPS-A Randomized Clinical Trial. JAMA. 2016;315(22):2406. doi:10.1001/jama.2016.6330
106. Liu KD, Levitt J, Zhuo H, et al. Randomized clinical trial of activated protein C for the treatment of acute lung injury. Am J Respir Crit Care Med. 2008;178(6):618–623. doi:10.1164/rccm.200803-419OC
107. Shyamsundar M, McAuley DF, Ingram RJ, et al. Keratinocyte growth factor promotes epithelial survival and resolution in a human model of lung injury. Am j Respir Critical Care Med. 2014;189(12):1520–1529.
108. McAuley DF, Cross LM, Hamid U, et al. Keratinocyte growth factor for the treatment of the acute respiratory distress syndrome (KARE): a randomized, double-blind, placebo-controlled phase 2 trial. Lancet Respir Med. 2017;5(6):484–491. doi:10.1016/S2213-2600(17)30171-6
109. Paine R, Standiford TJ, Dechert RE. A randomized trial of recombinant human granulocyte-macrophage colony stimulating factor for patients with acute lung injury. Crit Care Med. 2012;40(1):90–97. doi:10.1097/CCM.0b013e31822d7bf0
110. Fowler AA, Truwit JD, Hite RD. Effect of vitamin C Infusion on Organ Failure and Biomarkers of Inflammation and Vascular Injury in Patients With Sepsis and Severe Acute Respiratory Failure: the CITRIS-ALI Randomized Clinical Trial. JAMA. 2019;322(13):1261–1270. doi:10.1001/jama.2019.11825
111. Grant WB. Vitamin D supplementation of mother and infant could reduce risk of sepsis in premature infants. Early Hum Dev. 2010;86(2):133. doi:10.1016/j.earlhumdev.2010.02.003
112. Hariyanto TI, Intan D, Hananto JE, Harapan H, Kurniawan A. Vitamin D supplementation and Covid-19 outcomes: a systematic review, meta-analysis and meta-regression. Rev Med Virol. 2015:1;e2269. doi:10.1002/rmv.2269
113. Suter PM, Domenighetti G, Schaller MD, Laverriere MC, Ritz R, Perret C. N-acetylcysteine enhances recovery from acute lung injury in man. A randomized, double-blind, placebo-controlled clinical study. Chest. 1994;105(1):190–194. doi:10.1378/chest.105.1.190
114. Paterson RL, Galley HF, Webster NR. The effect of N-acetylcysteine on nuclear factor-kappa B activation, interleukin-6, interleukin-8, and intercellular adhesion molecule-1 expression in patients with sepsis. Crit Care Med. 2003;31(11):2574–2578. doi:10.1097/01.Ccm.0000089945.69588.18
115. Hariyanto TI, Lugito NPH, Yanto TA, Siregar JI, Kurniawan A. Insulin therapy and outcome from coronavirus disease 2019 (COVID-19): a Systematic Review, Meta-Analysis, and Meta-Regression. Endocr Metab Immune Disord Drug Targets. 2021;5:55. doi:10.2174/1871530321666210709164925
116. Yang Y, Cai Z, Zhang J. Insulin Treatment May Increase Adverse Outcomes in Patients With COVID-19 and Diabetes: a Systematic Review and Meta-Analysis. Original Research. Front Endocrinol (Lausanne). 2021;12:894. doi:10.3389/fendo.2021.696087
117. Hariyanto TI, Halim DA, Rosalind J, Gunawan C, Kurniawan A. Ivermectin and outcomes from Covid-19 pneumonia: a systematic review and meta-analysis of randomized clinical trial studies. Rev Med Virol. 2015:1;e2265. doi:10.1002/rmv.2265
118. Hariyanto TI, Halim DA, Jodhinata C, Yanto TA, Kurniawan A. Colchicine treatment can improve outcomes of coronavirus disease 2019 (COVID-19): a systematic review and meta-analysis. Clin Exp Pharmacol Physiol. 2021;48(6):823–830. doi:10.1111/1440-1681.13488
119. Drago BB, Kimura D, Rovnaghi CR, et al. Double-blind, placebo-controlled pilot randomized trial of methylprednisolone infusion in pediatric acute respiratory distress syndrome. Pediatr Crit Care Med. 2015;16(3):e74–81. doi:10.1097/PCC.0000000000000349
120. Proudfoot A, Bayliffe A, O’Kane CM, et al. Novel anti-tumour necrosis factor receptor-1 (TNFR1) domain antibody prevents pulmonary inflammation in experimental acute lung injury. Thorax. 2018;73(8):723–730. doi:10.1136/thoraxjnl-2017-210305
121. Vincent JL, Artigas A, Petersen LC, Meyer C. A multicenter, randomized, double-blind, placebo-controlled, dose-escalation trial assessing safety and efficacy of active site inactivated recombinant factor VIIa in subjects with acute lung injury or acute respiratory distress syndrome. Crit Care Med. 2009;37(6):1874–1880. doi:10.1097/CCM.0b013e31819fff2c
122. Cornet AD, Groeneveld ABJ, Hofstra JJ, et al. Recombinant human activated protein C in the treatment of acute respiratory distress syndrome: a randomized clinical trial. PLoS One. 2014;9(3):e90983–e90983. doi:10.1371/journal.pone.0090983
123. Moss M, Huang DT, Brower RG, et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl J Med. 2019;380(21):1997–2008. doi:10.1056/NEJMoa1901686
124. Aikawa N, Ishizaka A, Hirasawa H, et al. Reevaluation of the efficacy and safety of the neutrophil elastase inhibitor, Sivelestat, for the treatment of acute lung injury associated with systemic inflammatory response syndrome; a phase IV study. Pulm Pharmacol Ther. 2011;24(5):549–554. doi:10.1016/j.pupt.2011.03.001
125. Kido T, Muramatsu K, Yatera K, et al. Efficacy of early sivelestat administration on acute lung injury and acute respiratory distress syndrome. Respirology. 2017;22(4):708–713. doi:10.1111/resp.12969
126. Fukimbara S, Niibe K, Yamamoto M, Yamaguchi T. Adjustment for propensity score in nonrandomized clinical studies: comparison of sivelestat versus conventional therapy for acute lung injury in acute respiratory distress syndrome. Ther Innov Regul Sci. 2017;51(1):89–99. doi:10.1177/2168479016659103
127. Bernard GR, Wheeler AP, Arons MM, et al. A trial of antioxidants N-acetylcysteine and procysteine in ARDS. The Antioxidant in ARDS Study Group. Chest. 1997;112(1):164–172. doi:10.1378/chest.112.1.164
128. Domenighetti G, Suter PM, Schaller MD, Ritz R, Perret C. Treatment with N-acetylcysteine during acute respiratory distress syndrome: a randomized, double-blind, placebo-controlled clinical study. J Crit Care. 1997;12(4):177–182. doi:10.1016/s0883-9441(97)90029-0
129. Morris PE, Papadakos P, Russell JA, et al. A double-blind placebo-controlled study to evaluate the safety and efficacy of L-2-oxothiazolidine-4-carboxylic acid in the treatment of patients with acute respiratory distress syndrome. Crit Care Med. 2008;36(3):782–788. doi:10.1097/ccm.0b013e318164e7e4
130. Fowler AA
131. ARDS Network Authors For The ARDS Network T. Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. The ARDS Network. JAMA. 2000;283(15):1995–2002. doi:10.1001/jama.283.15.1995
132. McAuley DF, Cross LM, Hamid U, et al. Keratinocyte growth factor for the treatment of the acute respiratory distress syndrome (KARE): a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Respir Med. 2017;5(6):484–491. doi:10.1016/s2213-2600(17)30171-6
133. Paine R
134. Anzueto A, Baughman RP, Guntupalli KK, et al. Aerosolized surfactant in adults with sepsis-induced acute respiratory distress syndrome. N Eng J Med. 1996;334(22):1417–1422. doi:10.1056/NEJM199605303342201
135. Spragg RG, Lewis JF, Walmrath HD, et al. Effect of recombinant surfactant protein C-based surfactant on the acute respiratory distress syndrome. N Engl J Med. 2004;351(9):884–892. doi:10.1056/NEJMoa033181
136. Abraham E, Baughman R, Fletcher E, et al. Liposomal prostaglandin E1 (TLC C-53) in acute respiratory distress syndrome: a controlled, randomized, double-blind, multicenter clinical trial. TLC C-53 ARDS Study Group. Crit Care Med. 1999;27(8):1478–1485. doi:10.1097/00003246-199908000-00013
137. Network ACT. Randomized, placebo-controlled trial of lisofylline for early treatment of acute lung injury and acute respiratory distress syndrome. Crit Care Med. 2002;30(1):1–6. doi:10.1097/00003246-200201000-00001.
138. Gao Smith F, Perkins GD, Gates S, et al. Effect of intravenous β-2 agonist treatment on clinical outcomes in acute respiratory distress syndrome (BALTI-2): a multicentre, randomised controlled trial. Lancet. 2012;379(9812):229–235. doi:10.1016/S0140-6736(11)61623-1
139. Rice TW, Wheeler AP, Thompson BT, et al. Enteral omega-3 fatty acid, gamma-linolenic acid, and antioxidant supplementation in acute lung injury. JAMA. 2011;306(14):1574–1581. doi:10.1001/jama.2011.1435
140. Willson DF, Truwit JD, Conaway MR, Traul CS, Egan EE. The adult calfactant in acute respiratory distress syndrome trial. Chest. 2015;148(2):356–364. doi:10.1378/chest.14-1139
141. Limaye AP, Stapleton RD, Peng L, et al. Effect of ganciclovir on IL-6 levels among Cytomegalovirus-seropositive adults with critical illness: a randomized clinical trial. JAMA. 2017;318(8):731–740. doi:10.1001/jama.2017.10569
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.