")
Back to Journals » International Medical Case Reports Journal » Volume 15
Acute Renal Injury Due to Rhabdomyolysis Induced by Severe Hypothyroidism: First Case Report from Somalia
Authors Adan AM, Özturk S, Adani AA , Jeele MOO
Received 14 July 2022
Accepted for publication 7 October 2022
Published 12 October 2022 Volume 2022:15 Pages 575—578
DOI https://doi.org/10.2147/IMCRJ.S382350
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Abdisamad Mohamed Adan, Sevgi Özturk, Abdulkamil Abdullahi Adani, Mohamed Osman Omar Jeele
Department of Internal Medicine, Mogadishu-Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Osman Omar Jeele, Department of Internal Medicine, Mogadishu-Somali Turkish Training and Research Hospital, Mogadishu, Somalia, Tel +252 615775226, Email [email protected]
Abstract: Rhabdomyolysis is a life-threatening condition which is characterized by muscle injury and leakage of muscle contents into the systemic circulation. It has been known that hypothyroidism is associated with some degree of myalgia and muscle stiffness, but it can also be a cause of life-threatening rhabdomyolysis with end-organ damage. A combination of acute renal impairment due to rhabdomyolysis in patients with hypothyroidism, especially those who have no precipitating factors, is extremely rare. Here, we report a case of a 27-year-old male patient with severe hypothyroidism who presented to the emergency department with acute renal impairment due to rhabdomyolysis induced by severe hypothyroidism. The patient was admitted for 5 days and after levothyroxine 100 μg, intravenous fluid rehydration, input and output follow-up and close monitoring, the patient improved and was discharged in good condition.
Keywords: rhabdomyolysis, hypothyroidism, acute renal injury, Somalia
Introduction
Rhabdomyolysis is a life-threatening condition characterized by muscle injury and leakage of muscle contents into the systemic circulation.1 There are multiple causes of rhabdomyolysis, mainly trauma, strenuous exercises, and medications.2 Clinical features of rhabdomyolysis range from mild increases in creatinine kinase (CK) to medical emergencies like disseminated intravascular coagulation (DIC), acute renal failure, and cardiac arrhythmias.3 Although hypothyroidism-related rhabdomyolysis can be encountered in clinical practice, it is a very unusual combination.4 It has been known that hypothyroidism is associated with some degree of myalgia and muscle stiffness, but it can also be a cause of life-threatening rhabdomyolysis with end-organ damage.5 Notably, there are some case reports that reported the occurrence of acute renal injury in the presence of hypothyroidism. For instance, Choy and coworkers reported a 21-year-old female patient with a poor renal function test along with hypothyroidism.6 They stated that the patient’s renal function resolved promptly after thyroid hormone replacement. In Somalia, such cases have not been reported before. Here, we report a case of a 27-year-old male patient with severe hypothyroidism who presented to the emergency department due to acute renal impairment due to rhabdomyolysis induced by severe hypothyroidism.
Case Report
A 27-year-old male patient presented to our emergency department with a complaint of nausea, vomiting, decreased urine output for 4 days, fatigue, as well as bilateral lower limb pain for 1 month. He noticed a change in his urine color over the past 2 weeks. He had no significant past medical history other than gastroesophageal reflux disease (GERD), and he was not on any medication. His family history was negative for any autoimmune diseases. On examination, the patient looked ill, febrile, and cooperative, and some degree of swelling around the eyes was noted. His pulse rate was 69 beats per minute, blood pressure 120/80 mm Hg, and respiratory rate 18 breaths per minute with oxygen saturation of 99%. A cardiac examination revealed normal heart sounds and no evidence of jugular venous distention. There were no basilar rales on auscultation of the lungs and no wheezing. The abdomen was non-distended, soft and non-tender; there was no organomegaly, and bowel sounds were normal. Bilateral non-pitting edema was noted in the lower extremities with muscle tenderness all over the body and no sign of muscle hypertrophy. The patient had no history of trauma or strenuous physical activity. There was no evidence of lymphadenopathy. The neurological examination was normal. The chest x-ray and ECG findings were unremarkable. Laboratory investigations showed hemoglobin at 11.7 g/dl, white blood count at 9.31×1000/mm3, platelets 249×1000/mm3, urea 77 mg/dl, creatinine 3.62 mg/dL, CK 19920 U/L, myoglobin 5896 U/L, AST 803 U/L, and ALT 421 U/L. Electrolyte levels were all normal. Urinalysis showed no proteinuria or hematuria. TSH was measured at 201mIU/mL (Table 1).
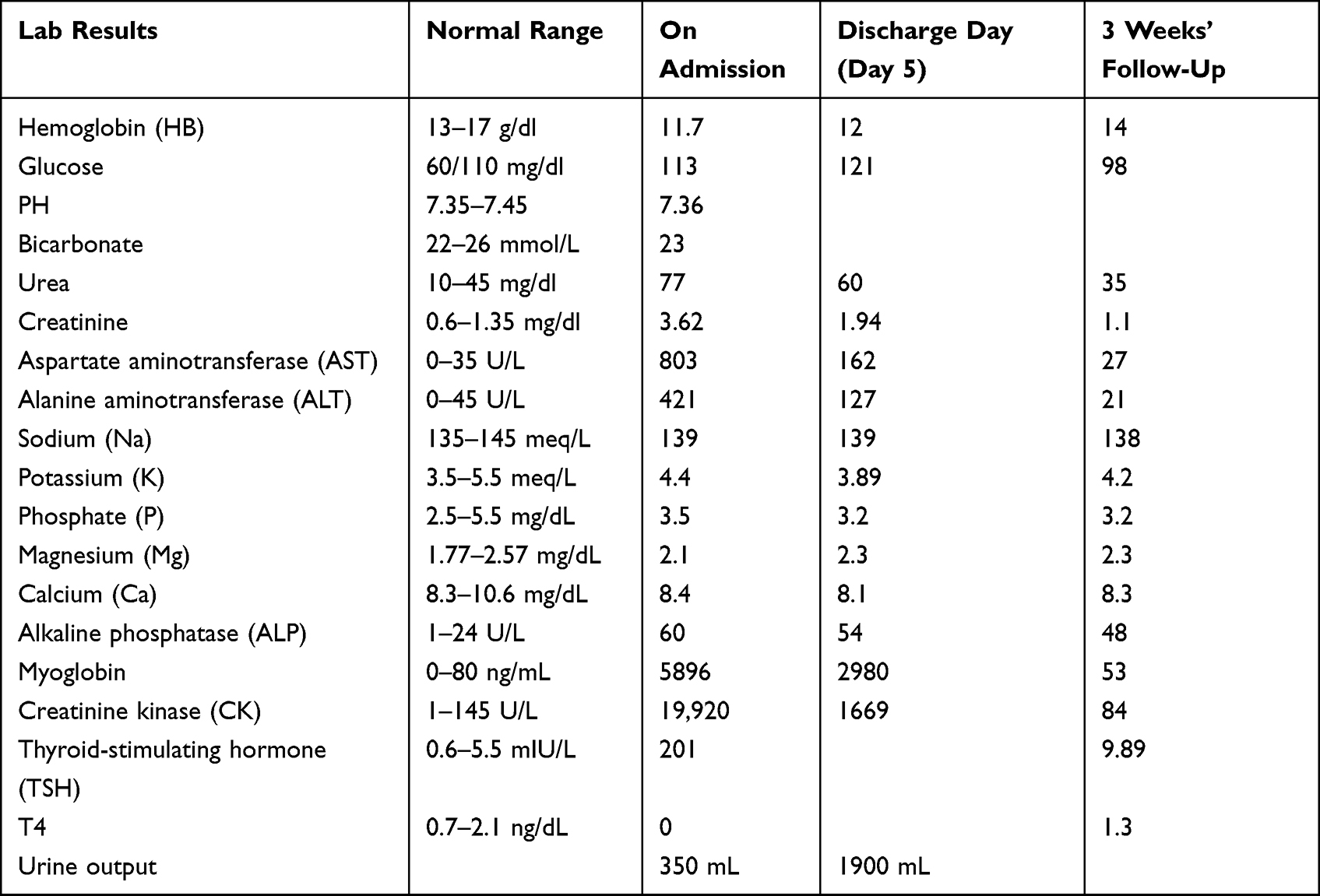 |
Table 1 Laboratory Results from Presentation to 3 Weeks’ Follow-Up |
Abdominal ultrasound showed normal sized kidneys with normal echogenicity and normal parenchyma with no stone or evidence of hydronephrosis. A thyroid ultrasound scan was requested and revealed a small thyroid that was hypoechoic and heterogeneous with diminished vascularity. The findings are suggestive of prior episodes of long-standing thyroiditis such as Hashimoto thyroiditis.
The patient was admitted to the internal medicine inpatient department and was started on levothyroxine 50 µg for the first 3 days and then 100 µg to avoid heart palpitation and intolerance. In addition, sufficient rehydration with maintenance fluids and input and output follow-up was initiated. After 5 days of close follow-up and monitoring, the patient’s urine output started to increase, his renal function test improved (urea 60 mg/dL, creatinine 1.94 mg/dL), and his creatinine kinase (CK) decreased to 1669 ng/mL. His bilateral lower limb edema and muscle cramps also improved, along with his overall condition, and he was discharged on a three-week follow-up rendezvous. After 3 weeks, the patient presented with a normal renal function test, his CK almost returned to normal, his muscle pain has subsided and his thyroid function test improved drastically (Table 1). He was advised to do a thyroid function test every 4 weeks. The patient was also advised to adhere to his medication as this condition could recur again if he left the medication and thus could cause serious complications.
Discussion
This unusual combination of hypothyroidism and rhabdomyolysis with acute renal injury is the first of its kind reported from Somalia. Our patient had no history of thyroid disorder before, nor had he experienced any trauma recently or taken part in any strenuous exercises. His renal function test, along with oliguria, thyroid function test, and creatinine kinase levels on presentation were suggestive of acute renal injury due to rhabdomyolysis induced by severe hypothyroidism. The principal cause of this scenario was identified as hypothyroidism, and after administering thyroid replacement therapy with intravenous fluid and close monitoring, the patient’s clinical condition improved drastically and he was discharged from the hospital on short notice.
Rhabdomyolysis is generally sub-grouped as trauma-related and non-trauma-related.1 Clinical features of rhabdomyolysis are said to be myoglobinuria, myalgia, and weakness.5 Although hypothyroidism is a well-known cause of rhabdomyolysis, it is an unusual and a rarely encountered complication.7 Most rhabdomyolysis with hypothyroidism usually has precipitating factors such as exercise or after treatment with statins,8 but it can also happen without any precipitating factors, as in our patient. Biochemically, an increased plasma level of creatinine kinase five times more than the normal level is usually referred to as rhabdomyolysis.9 The prevalence of acute renal injury in rhabdomyolysis patients is thought to be 5–30%, and rhabdomyolysis patients with acute renal injury have a 50% mortality rate compared to the general population.10,11
Similar cases to this report have been noticed all around the world. Anyfantakis et al in 2021 reported a middle-aged man who developed rhabdomyolysis following intramuscular injection. The patient’s laboratory tests revealed hypothyroidism and he did not develop renal injury.12 In contrast to this case report, our patient had no precipitating factors and he also presented with acute renal injury. Another case report by Baghi et al in 2021 reported a 42-year-old man who presented with acute renal failure due to rhabdomyolysis induced by hypothyroidism. The patient was also treated with intravenous fluids and levothyroxine treatment.3 Similar to our report, this patient had no precipitating factors.
In 2021, Ghayur et al reported a 68-year-old hypothyroid patient who was non-compliant with his levothyroxine treatment and presented with rhabdomyolysis with acute renal injury requiring hemodialysis for 4 weeks. Our patient did not need any hemodialysis sessions for his acute renal injury, but it is a scenario that similar patients could face if not adherent to their thyroid replacement therapies.13
Conclusion
In this case report, we report an occurrence of acute renal impairment due to rhabdomyolysis induced by severe hypothyroidism. Acute renal impairment due to rhabdomyolysis in patients with hypothyroidism is quite rare, and even when the patient has no precipitating factors, it is extremely rare. Physicians should keep in mind this rare combination when dealing with non-traumatic-related rhabdomyolysis.
Abbreviations
CK, creatinine kinase; DIC, disseminated intravascular coagulation; GERD, gastroesophageal reflux disease; ECG, electrocardiogram.
Ethics Committee Approval and Consent for Publication
Mogadishu-Somali Turkish Training and Research Hospital ethics committee waived approval for this case report. Written informed consent was obtained from the patient to publish the details in this case report anonymously.
Disclosure
The authors declare that they have no conflicts of interest in relation to this work.
References
1. Stanley M, Chippa V, Aeddula NR, et al. Rhabdomyolysis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
2. Zutt R, Van Der Kooi AJ, Linthorst GE, Wanders RJ, De Visser M. Rhabdomyolysis: review of the literature. Neuromuscul Disord. 2014;24(8):651–659. doi:10.1016/j.nmd.2014.05.005
3. Baghi MA, Sirajudeen J, Naushad VA, Alarbi KS, Benshaban N. Severe hypothyroidism‐induced rhabdomyolysis: a case report. Clin Case Rep. 2021;9(12):e05107. doi:10.1002/ccr3.5107
4. Boryushkina V, Ahmed S, Quadri K, Ramdass A. Recurrent rhabdomyolysis induced by severe hypothyroidism. Cureus. 2019;11(6). doi:10.7759/cureus.4818
5. Cervellin G, Comelli I, Lippi G. Rhabdomyolysis: historical background, clinical, diagnostic and therapeutic features. Clin Chem Lab Med. 2010;48(6):749–756. doi:10.1515/CCLM.2010.151
6. Choy J, Yaxley J, Yaxley W, Rare A. Case of renal impairment caused by primary hypothyroidism. Korean J Fam Med. 2018;39(3):204. doi:10.4082/kjfm.2018.39.3.204
7. Yeter E, Keles T, Durmaz T, Bozkurt E. Rhabdomyolysis due to the additive effect of statin therapy and hypothyroidism: a case report. J Med Case Rep. 2007;1(1):1–2. doi:10.1186/1752-1947-1-130
8. Gurala D, Rajdev K, Acharya R, Idiculla PS, Habib S, Krzyzak M. Rhabdomyolysis in a young patient due to hypothyroidism without any precipitating factor. Case Rep Endocrinol. 2019;2019:1–3. doi:10.1155/2019/4210431
9. Michelsen J, Cordtz J, Liboriussen L, et al. Prevention of rhabdomyolysis‐induced acute kidney injury–a DASAIM/DSIT clinical practice guideline. Acta Anaesthesiol Scand. 2019;63(5):576–586.
10. Melli G, Chaudhry V, Cornblath DR. Rhabdomyolysis: an evaluation of 475 hospitalized patients. Medicine. 2005;84(6):377–385. doi:10.1097/01.md.0000188565.48918.41
11. Danielak D, Karaźniewicz-łada M, Główka F. Assessment of the risk of rhabdomyolysis and myopathy during concomitant treatment with ticagrelor and statins. Drugs. 2018;78(11):1105–1112. doi:10.1007/s40265-018-0947-x
12. Anyfantakis D, Kastanakis S. Hypothyroidism induced rhabdomyolysis in a young male after a single intramuscular injection: a case report. Maedica. 2021;16(2):328. doi:10.26574/maedica.2020.16.2.328
13. Ghayur A, Elahi Q, Patel C, Raj R. Rhabdomyolysis-induced acute kidney injury in a patient with non-compliance to levothyroxine therapy. Endocrinol Diabetes Metabol Case Rep. 2021;2021(1). doi:10.1530/EDM-21-0034
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.