")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 11
Acute kidney injury in elderly patients: narrative review on incidence, risk factors, and mortality
Authors Yokota LG, Sampaio BM, Rocha EP, Balbi AL, Sousa Prado IR, Ponce D
Received 5 April 2018
Accepted for publication 12 June 2018
Published 14 August 2018 Volume 2018:11 Pages 217—224
DOI https://doi.org/10.2147/IJNRD.S170203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Laís Gabriela Yokota,1 Beatriz Mota Sampaio,1 Erica Pires Rocha,1 André Luís Balbi,1 Iara Ranona Sousa Prado,1 Daniela Ponce1,2
1Botucatu School of Medicine, São Paulo State University (UNESP), Sao Paulo, Brazil; 2Course of Medicine, University of Sao Paulo (USP), Sao Paulo, Brazil
Abstract: Acute kidney injury (AKI) is characterized by a sudden renal dysfunction with consequent increase of nitrogenous products, hydroelectrolytic and acid–base disorders. Its prevalence is high in hospitalized populations (4.9%–7.2%), especially in intensive care units (ICUs). Despite all the technical and therapeutic advances that have occurred in the last few decades, the overall mortality of AKI patients remains high, reaching 80% in ICU patients. Several conditions predispose a patient to progress with AKI, including age, sepsis, surgeries, and comorbidities, such as systemic arterial hypertension, diabetes mellitus, heart disease, neoplasia, and chronic renal disease. Among these risk factors, age is emphasized, since, due to advances in the health area, there has been an increase in life expectancy, hence an increase in the demand of the elderly population for health services. At the same time, the elderly present a greater predisposition to the development of AKI, either due to kidney senility, or because of the high prevalence of comorbidities present, and medical interventions such as the use of contrasts and medications, which can also trigger AKI. Considering the relevance of the social role of the elderly and the scarcity of studies on AKI in the elderly admitted to the ICU, further studies are needed. This review article was elaborated considering the purpose: to assess incidence, risk factors, and mortality of AKI in elderly patients admitted to ICUs. Published studies were collected using the following inclusion criteria: be accessible in online databases (Lilacs, Scielo, and PubMed), have been published since 2000 and written in English, Portuguese, or Spanish. The descriptors used for the survey were “Acute Kidney Injury”, “Aging”, and “Elderly”. All items that did not fit in the above inclusion criteria were discarded. We have also presented a synthesis of the knowledge acquired during this review.
Keywords: comorbidities, risk factors, elderly, acute kidney injury, mortality, intensive care unit
Introduction
Acute kidney injury (AKI) is characterized by a sudden renal function impairment followed by electrolyte and acid–base balance disorders as well as an increase in nitrogen products.1,2 The prevalence of AKI is shown higher in hospitalized populations (4.9%–7.2%), especially in patients admitted to the intensive care unit (ICU; 40%),3 when compared with the community (0.4%–0.9%).
Despite all therapeutic advances in the past decades, the overall mortality of patients with AKI remains around 50% and can reach up to 80% in critically ill patients,4–6 depending on clinical conditions, comorbidities, and the need for renal replacement therapy.4–7
Although AKI is a frequent disorder associated with high mortality, only recently was there a consensus on its definition: in 2012 a new definition and staging criteria of AKI, covering both Acute Kidney Injury Network and Risk, Injury, Failure, Loss and End Stage criteria, was proposed by Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. Therefore, AKI is now defined as an increase in serum creatinine (SCr) ≥0.3 mg/dL in 48 hours or an increase up to 1.5 times the SCr baseline within 7 days or a urine output <0.5 mL/kg/hour for more than 6 hours.8
The KDIGO criteria, besides defining AKI, also classify it into stages, as shown in Table 1.
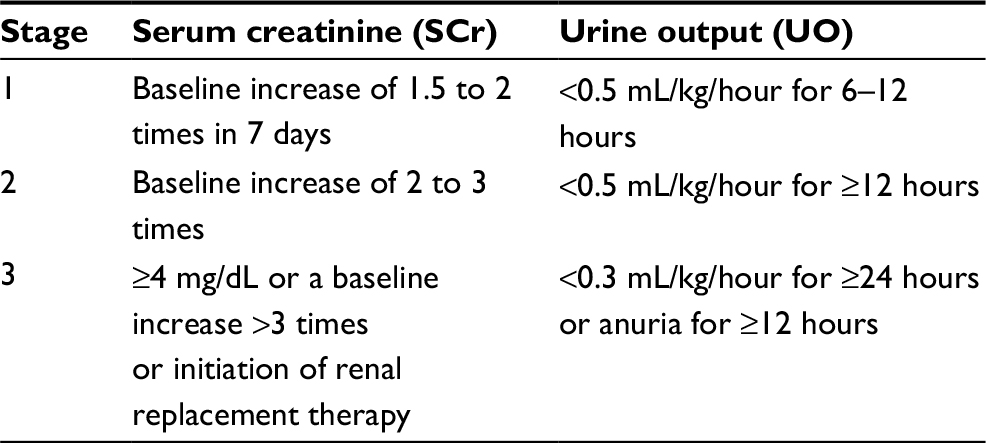 | Table 1 KDIGO classification criteria for acute kidney injury Abbreviation: KDIGO, Kidney Disease: Improving Global Outcomes. |
AKI can also be classified according to its pathophysiology. It may be caused by three main mechanisms: low renal perfusion, renal parenchymal injury, and excretory system obstruction, leading respectively to prerenal, renal, and postrenal AKI, as shown in Figure 1.
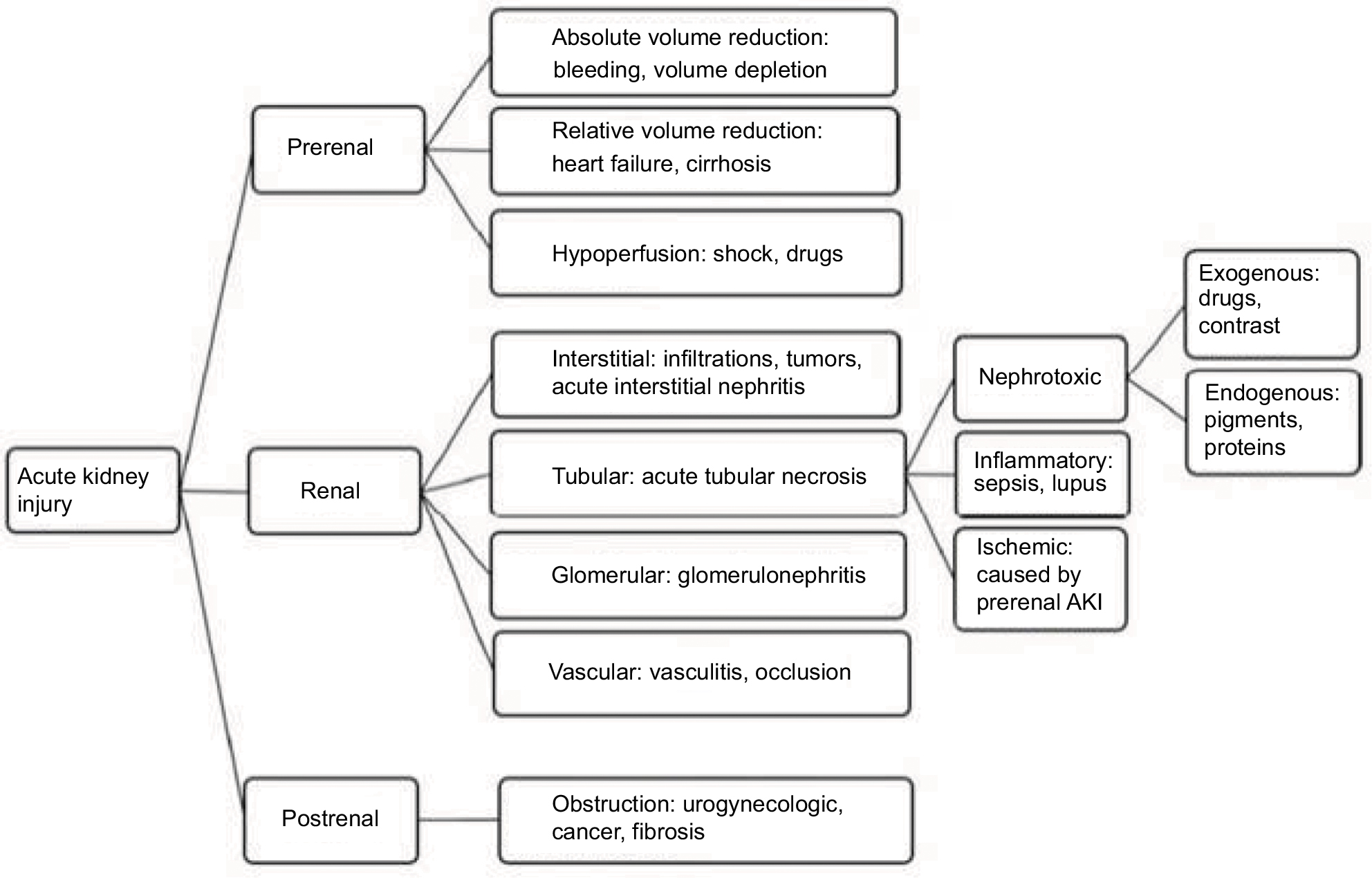 | Figure 1 AKI classification according to its pathophysiology. Abbreviation: AKI, acute kidney injury. |
The prerenal or “functional” AKI is defined as an accumulation of nitrogenous products secondary to renal plasma flow and glomerular filtration rate (GFR) reduction. It is the most common form of AKI (40%–60%)7 and is reversible when its basic causes are treated. The main causes of prerenal AKI are as follows: absolute volume reduction (hemorrhage and volume depletion), relative volume reduction (cirrhosis and heart failure [HF] – also known as cardiorenal syndrome [CRS]), and hypoperfusion (by shock or medication).
Renal AKI, also known as “intrinsic” or “structural”, is caused by a dysfunction of the kidney itself and it can occur in many different renal structures, such as vascular (vasculitis and occlusion), glomerular (glomerulonephritis), tubular (acute tubular necrosis [ATN]), and interstitial (infiltrations, tumors and acute interstitial nephritis). The most common cause of renal AKI is ATN (>70%), and it can have ischemic or toxic etiology. Other less frequent causes of renal AKI are as follows: tubulointerstitial nephritis (10%–20%) caused by drugs or infections, glomerulonephritis, and cortical necrosis (1%–10%).7–14
Postrenal AKI, also called “nonobstructive” AKI, is secondary to obstruction of the urinary tract by stones, clots, tumors, or retroperitoneal fibrosis. It is the least frequent type of AKI (2%–4%) and increases up to 10% with patients’ age.10–20
Some authors described that the most prevalent type of AKI in ICUs is prerenal, while others affirmed that renal AKI caused by ATN was responsible for >50% of AKI cases in hospitalized patients and >76% of AKI cases in ICU patients.5,18,21
It can be noted that data on the most prevalent type of AKI are conflicting; therefore, further studies to clarify this epidemiology are necessary.
Even though there is no consensus on what kind of AKI is the most prevalent in ICUs, it is known that both prerenal and renal AKI have a similar underlying pathology: they stem from a decrease of renal perfusion secondary to hypovolemia or hypotension,3,11–13 therefore being called, together, ischemic AKI. Furthermore, in the case of permanence of prerenal AKI >2 days, death and necrosis of the renal parenchyma may occur secondary to decreased perfusion, leading to ischemic ATN.10 Thus, prerenal AKI can often be followed by renal AKI, and these two main subtypes are responsible for the high prevalence of this syndrome, corresponding to about 92.5% of cases of AKI in ICUs.14
The ischemic AKI’s pathophysiology is complex because it involves hemodynamic, oxidative stress, and inflammatory mechanisms, as shown in Figure 2.
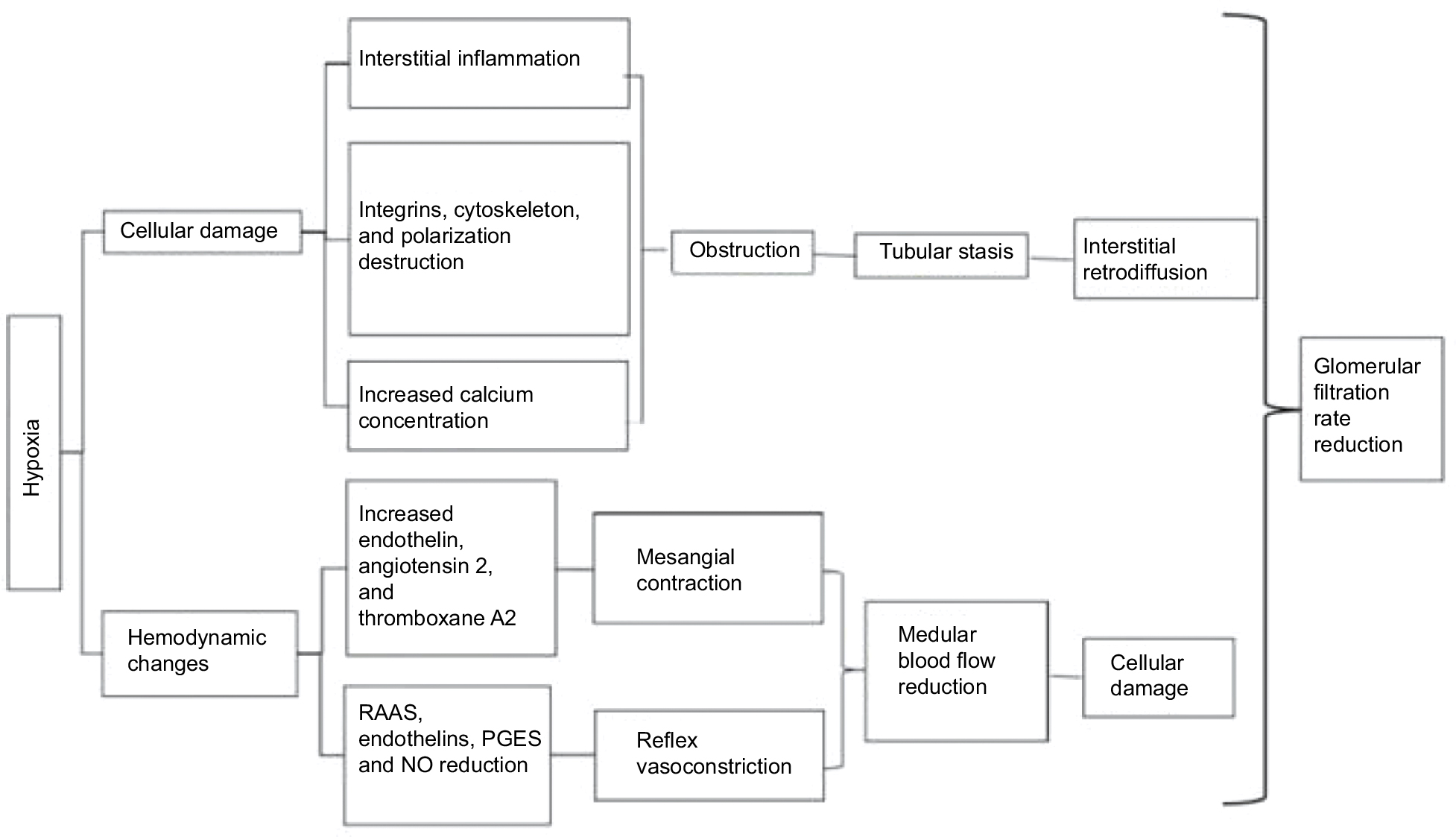 | Figure 2 Ischemic AKI’s pathophysiology. Abbreviations: AKI, acute kidney injury; NO, nitric oxide; PGES, prostaglandins; RAAS, renin–angiotensin–aldosterone system. |
Several factors can predispose a patient to AKI. Among them, the most highlighted ones are age, sepsis, surgery, prolonged hospital stay, and presence of comorbidities such as hypertension (HT), diabetes mellitus (DM), heart disease, chronic kidney disease (CKD), and liver diseases. Bucuvic et al3 identified in their research that 62% of patients diagnosed with AKI were male, 65.2% were >60 years, 61.9% had DM, 44.4% were hypertensive, and 21.9% had CKD. Oweis and Alshelleh5 reported that 62% of ICU patients with AKI were male, 51.5% were >60 years, 57.7% of patients had HT, 27.4% had heart disease, and 26.6% had DM. Junior et al12 showed in their work that 62% of patients with AKI in ICU were men, 48.4% of AKI was caused by hypotension, 40.6% by sepsis, and 21.9% by nephrotoxic drugs. The most common comorbidities associated with the AKI are respiratory failure (28.9%), cardiovascular disease (25.8%), HT (19.5%), DM (9.4%), surgical complications (9.4%), and liver disease (7.8%).
Santos and Matos15 performed a study that compared patients who acquired AKI in ICU with those who did not, and showed that patients affected by AKI were older (56.4±18.8 vs 46.8±16.5 years, P=0.0028); had more septic shock (19.2% vs 6.5%, P<0.05), and sepsis (17.3% vs 3.9%, P=0.012). Pedersen et al13 found that 36% of patients with AKI in ICU were >70 years, 65% were male, 51% were in the postoperative period, 28% developed ischemic AKI, 31% had AKI associated with sepsis, 35% were nephrotoxic, and 7.7% had an obstructive cause. It is important to point out that among elderly population the most frequent causes of AKI were nephrotoxicity and obstruction of the urogenital system.
Thus, it can be observed that there is a convergence in terms of risk factors for AKI with emphasis on elderly patients admitted to ICUs, comorbidities such as HT and DM, presence of sepsis, and previous surgery.
Among these risk factors, the age of patients stands out as one of the most important factors because due to advances in health care, people are living longer and, therefore, getting older which leads to an increase in the demand of the elderly population in health care services. In Brazil, the proportion of people aged ≥60 increased from 6.7% in 1990 to 8.1% in 2000, and the projections of the Brazilian Institute of Geography and Statistics suggest that this population will reach up to 64 million by 2050, which corresponds to 24.6% of total Brazilian inhabitants.21
The average age of patients admitted to the ICU has also increased in recent years. In Western countries, people >65 years represent 18% of the population, corresponding to 45.5% of total hospital admissions. In ICUs, about 60% of patients are >65 years, demonstrating how relevant the study of the elderly is, as this population is now and will be even more in the future, the primary user of health care services.20
Finally, the elderly can have AKI because of kidney senility and high frequency of comorbidities, which lead them to undergo several medical procedures, which are also risk factors for AKI.13,16–22
Considering the high incidence of AKI in the elderly and the social role of the elderly, we can conclude that more AKI studies in the elderly are necessary.
Risk factors for AKI in the elderly
Although there is no uniformity in the epidemiology of AKI in the elderly due to changes in diagnostic criteria used by different authors as well as population variations between different areas, all studies converge on the high incidence and mortality of AKI in elderly patients.
The risk factors that make the elderly prone to develop AKI can be divided into three types: 1) related to kidney senility, 2) secondary to the elderly’s comorbidities, and 3) associated with medical intervention,13,16,17 as shown in Figure 3.
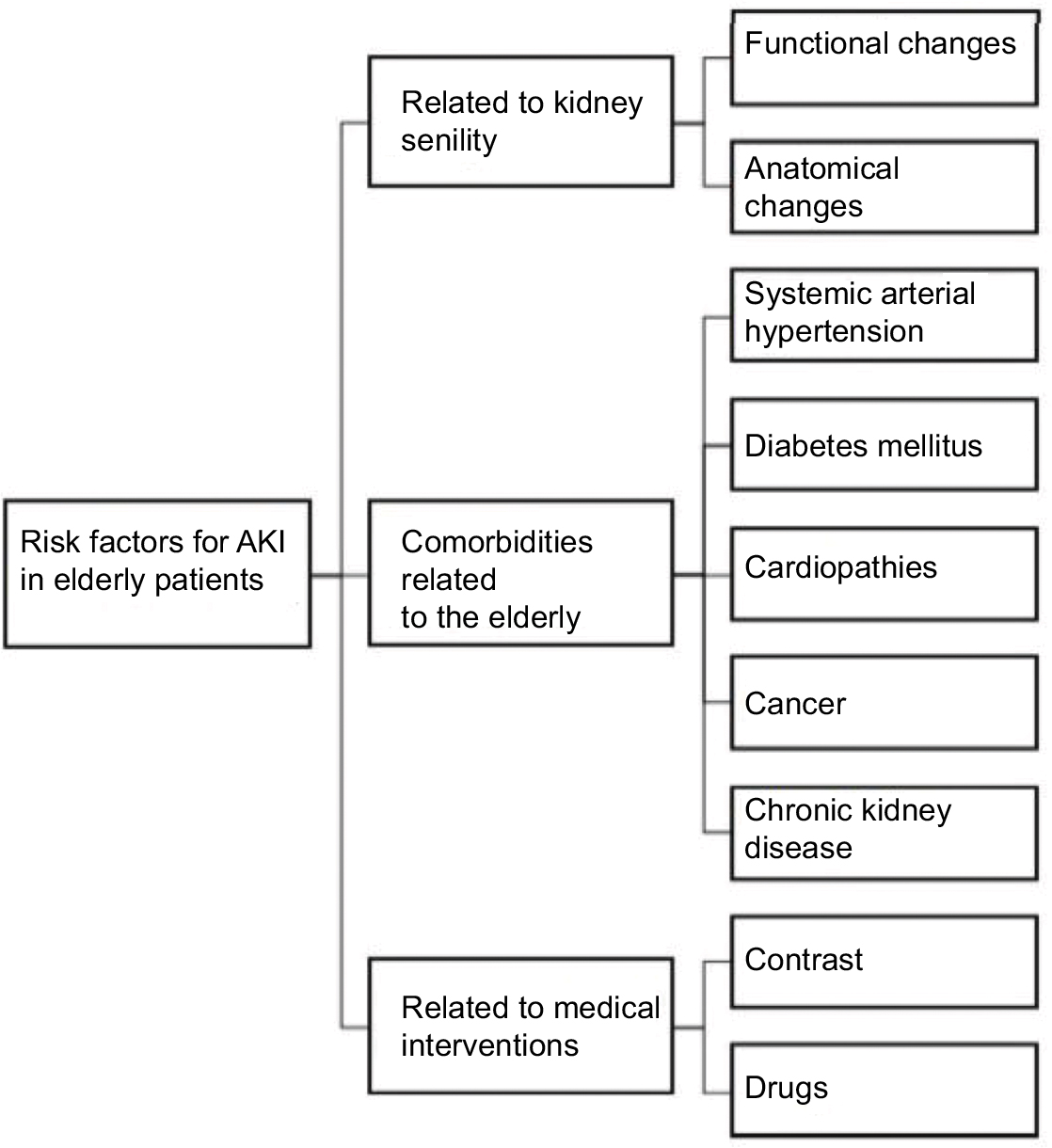 | Figure 3 Risk factors for acute kidney injury in elderly patients. Abbreviation: AKI, acute kidney injury. |
Risk factors related to kidney senility
The kidneys, as well as the rest of the body, get old, and in the aging process, atrophy and cease to perform their basic functions. It involves glomerulosclerosis, tubular atrophy, interstitial fibrosis, and atherosclerosis, thus defining senile nephrosclerosis. This kidney senility can be characterized by morphological, anatomical, and functional changes that ultimately lead to lower performance of the filtration process, therefore, facilitating the installation of AKI and consequent azotemia or even uremic syndrome.
Among the morphological and anatomical changes caused by kidney aging, one can cite the decreased renal mass caused by a reduction of the weight, volume, and the number of functional glomeruli (glomerular sclerosis)16,17,21 concomitant to a compensatory glomeruli hypertrophy, secondary to a hyperfiltration injury. Also, it can be noted that the kidney starts to develop mesangium expansion; interstitial fibrosis; decrease in the amount, size, and extent of the tubules; atherosclerosis; and fibrointimal hyperplasia caused by an internal elastic lamina growth, lumen hyalinization, and stenosis.16,17,21,22
Decrease of the mitochondrial energy production leading to impairment in active transport by the tubule can be cited as another functional change triggered by kidney senility. This leads to a change in reabsorption of glucose and an increase of protein content in urine, which indicates a tubular damage that is not associated with the injury itself.16
With age, there is also an increase in the kidney’s cellular apoptosis rate, leading to a lower number of functional nephrons, thus contributing to a reduction in GFR and creatinine clearance ratio, which induces a decrease in renal functional reserve, making the kidney more susceptible to AKI.16,17,21,22 The reduction in the number of nephrons also leads to an impairment of the sodium retention mechanism16 leading to changes in urine concentration as well as a larger volume depletion and urine dilution, which can cause dehydration. This loss of nephrons also means that there is an increase filtration load, which induces a nephron hyperfiltration injury.
The elderly, besides having a higher apoptotic rate, present with a smaller amount of growth factors as well as a downregulated cellular transduction. This causes a lower cell division rate and, as a consequence, slower regeneration response after injury.17,21
At the same time, flaws in the acidification mechanism during physiological stress lead to metabolic acidosis and decreased production of renal 1-alphahydroxylase, which induces alterations in calcium metabolism and may trigger renal osteoporosis.
Risk factors associated with comorbidities
Several common comorbidities may make the elderly prone to AKI. Among them, the presence of HT, DM, heart disease, and CKD stand out, according to most studies.
Currently, more than 50% of the world’s elderly population is hypertensive, and Brazil’s projections indicate that by 2025 about 16 million Brazilians will be hypertensive elders.16 The presence of hypertension acts as a stressor of the vessel walls, damaging them chronically, which induces thickening and reduces the elasticity of the tunica intima by proliferating the internal elastic lamina as well as inducing hyalinization and stenosis of the lumen, thereby contributing to a decrease in renal blood flow and, consequently, increases the susceptibility to prerenal AKI.16,21,26
By the same mechanism of endothelial injury, hypertension also leads to the formation of atheromatous plaques that reduce the renal blood supply by decreasing the vessel lumen and damaging the self-regulatory mechanisms of the renin–angiotensin–aldosterone system (RAAS). This way, aged people’s RAAS may be reduced by 30%–50% when compared with the younger population.16 In order to have a negative feedback by RAAS in response to the decline of renal perfusion, the arteries must be elastic and in proper condition for vasoconstriction (efferent) and vasodilation (afferent), which may not occur in the elderly due to atheromatous plaques that decrease both the arterial lumen and elasticity of vessels, thereby complicating the vasodilatation and vasoconstriction response to ischemic insults and facilitating the occurrence of a prerenal AKI.
Another very common comorbidity in the aged population is DM. About 20%–30% of the elderly has DM, therefore, are at risk of developing diabetic nephropathy. Diabetic nephropathy consists of glomerular and microvascular changes. The microvascular injury component of DM is secondary to excess blood glucose toxicity, which leads to microinfarcts, decreased amount of nephrons, and hence renal functional reserve reduction. Also, the diabetic hyperglycemia induces secondary metabolic pathway formations such as nonenzymatic glycation and pathway of polyols. The metabolites of nonenzymatic glycation cause disturbances in the production of extracellular matrix components leading to glomerular occlusion. The pathway of polyols presents sorbitol as a metabolite, which in large quantities leads to hyperosmotic stress and consequent cellular damage.24,26
HF is characteristically a disease of the elderly, accounting for up to 20% of the causes of hospital admission in patients >65 years of age.27 It is a complex clinical syndrome defined as a cardiac dysfunction that causes inadequate blood supply to the tissue in the presence of normal venous return. Thus, the hemodynamic changes commonly found in HF involve inadequate response of cardiac output and elevation of pulmonary and systemic venous pressures. When decompensated, renal function changes frequently and its presence is associated with increased mortality. CRS type one is the term used to characterize the association between abrupt worsening of cardiac function (such as acute HF or decompensated chronic HF) causing AKI. The worsening renal function may be due to low renal perfusion, low cardiac output, hypovolemia, venous congestion, renal intrinsic disease, or caused by drugs used in the treatment of HF, such as ACE inhibitors and angiotensin receptor blockers. Other factors associated with renal dysfunction are peripheral vasoconstriction and use of contrast agents to obtain diagnostic images.28
Cancer, which is more and more frequent with advancing age, presents as an important risk factor, either because of the presence of tumors capable of obstructing the urinary tract, or because of the need for chemotherapy for its treatment, which can become nephrotoxic. In addition, it can increase the production of inflammatory cytokines,16 which may also predispose to AKI as cytokines play an important role in AKI’s physiopathology.
CKD may also make the elderly prone to AKI because it is a syndrome characterized by a reduction of viable nephrons, with consequent reduction of renal functional reserve. Thus, the kidney with CKD, although it can take advantage of adaptation mechanisms, when affected by acute stressors, cannot maintain its functionality for too long, thereby leading to AKI.17
Risk factors associated with medical procedures
Because of their wide range of comorbidities, the elderly population is one of the main users of the health system and is often subjected to medical procedures, which can also induce AKI due to the lower drug excretion capacity of these patients. Among the main causes of iatrogenic AKI, the use of contrasts and nephrotoxic drugs should be mentioned.16–23
The elderly are usually submitted to a large number of tests for which the use of nephrotoxic contrast is necessary. The radiographic contrast, in addition to direct tubular damage, alters renal perfusion and intrarenal hemodynamics.
Also, the elderly make chronic use of medications such as antiinflammatory and angiotensin-converting enzyme inhibitors. These drugs may impair renal autoregulation and trigger ATN.18
It is also important to emphasize the correct dosage calculation of the medications and administered contrast agents in these patients because due to the reduction of body mass, overdose of drugs can occur.17
The diagnosis of AKI in the elderly
SCr continues to be the most commonly used renal function marker once it is totally excreted by the kidney. If renal filtration is inefficient, SCr levels rise. But this biomarker is not considered the ideal marker for AKI because of its late rise, when kidney damage and decrease of GFR have already happened. Also, there are many variables that influence SCr concentration, age being one of them. As you age, you lose muscle mass and therefore the SCr baseline of the elderly may be lower than the normal standards. That lower SCr baseline may mask a pathological increase due to kidney damage and thus lead to subdiagnosis or late diagnosis. Likewise, the elderly’s low protein intake also influences creatinine, leading to a lower basal SCr as well.16,17,22 Therefore, AKI’s diagnosis based on SCr levels is most of the time, inefficient.30
As SCr may not be the ideal AKI biomarker, other earlier markers such as cystatin C, interleukin-18, neutrophil gelatinase-associated lipocalin, and kidney injury molecule-1 may be considered as alternatives.21–25 Many studies have validated their efficacy as early predictors of AKI in HF, post cardiac surgery in both adults and pediatric population, and in septic ICU patients, but none were performed specifically in the elderly.17–19,23–25
Short- and long-term evolution of elderly patients with AKI
Although short-term mortality rates identified by different researchers may vary, they all agree that the mortality of elderly patients with AKI is high and may be higher than in other age groups. Most studies of elderly ICU patients with AKI indicate mortality rates around 63.5% reaching up to 76.2%, as described by Mataloun et al.11 Pedersen et al13 identified a mortality rate of 53.1% in their study, similar to Mårtensson et al23 who reported a mortality of 50%.
AKI’s short-term prognosis in aged patients remains bleak due to the high degree of severity and complexity of these patients. So, it may vary according to the presence or absence of oliguria, sepsis, and multiple organ failure.5,21 According to some studies, the age of the patient is not a determining factor for the development and therapeutic decision-making, while it can be influenced by the severity the lesion, presence of comorbidities, and renal functional status.20,23
There are few studies that keep tracking the elderly and assess their progress in the post hospital stage.5 Coca21 reports that AKI is independently related to long-term mortality in the elderly, as about 28% of elderly patients aged >65 years did not recover renal function after an episode of AKI, developing CKD afterward because of the lack of compensatory mechanisms and adequate regeneration. Acunak et al25 reported that 18.9% of elderly patients with AKI progress to dialysis treatment and 66.7% of this population die within 1 year. Brown et al29 report that the stigma suffered by elderly dialysis patients is very large, and secondarily, their quality of life is reduced.
Prevention of AKI in the elderly
The high rate of mortality and no specific treatment reinforce the need for efficient prevention of AKI in the elderly. Among the main strategies used, the following can be mentioned: careful clinical monitoring, hydroelectrolyte control, and balance and correction of factors such as hypovolemia and hypotension. When performing invasive procedures, AKI can be prevented by maintaining the mean arterial blood pressure >80 mmHg, hematocrit >30%, adequate oxygenation, and blood volume restoration.5
To prevent drug nephrotoxicity-induced AKI, drugs such as diuretics, antiinflammatory, angiotensin-converting enzyme inhibitors, and other vasodilators should be used with caution. It is advisable to individualize the treatment by adjusting the drug’s doses according to the patient’s GFR calculated by the formulas, Modification of Diet in Renal Disease or CKD-EPI. Both formulas take into account age, ethnicity, gender, and baseline creatinine. They have the advantage of not requiring knowledge of the weight or height of the individual, since they are often not accessible. Both calculations, however, may overestimate the results in the elderly.21
When it comes to image tests such as tomography and magnetic resonance imaging, it is recommended not to use contrast and, if necessary, use isoosmotic or nonionic low osmolar contrast in small quantities. If there are no contraindications, volume expansion with saline or sodium bicarbonate before and after the examination may help prevent contrast-induced AKI. The use of acetylcysteine, 1 day before and 1 day after the examination is also indicated.18
Although there are several ways to prevent AKI, early detection of renal failure and greater attention of health professionals to recognize the elderly’s vulnerability to AKI are still the best options to reduce the complications of this syndrome and, consequently, its mortality rate.
Finally, there is no consensus in the epidemiology of AKI in the elderly; all studies agree about its high incidence and mortality. Risk factors that make the elderly likely to develop AKI are related to kidney senility, secondary to comorbidities and, associated with medical procedures. Recognizing the vulnerability of the elderly to AKI and the early diagnosis of this syndrome are the best options to reduce its high prevalence, complications, and consequently, mortality.
Acknowledgments
We acknowledge and thank the following institutions for their contribution to this study: FAPESP (Sao Paulo’s State Research Support Foundation) and FMB – UNESP (Botucatu Medical School – University of Sao Paulo).
Disclosure
The authors report no conflicts of interest in this work.
References
Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39(5):930–936. | ||
Mehta RL, Chertow GM. Acute renal failure definitions and classification: time for change? J Am Soc Nephrol. 2003;14(8):2178–2187. | ||
Bucuvic EM, Ponce D, Balbi AL. Risk factors for mortality in acute kidney injury. Rev Assoc Med Bras. 2011;57(2):158–163. | ||
Medeiros P, Nga HS, Menezes P, Bridi R, Balbi A, Ponce D. Acute kidney injury in septic patients admitted to emergency clinical room: risk factors and outcome. Clin Exp Nephrol. 2015;19(5):859–866. | ||
Oweis AO, Alshelleh SA. Incidence and outcomes of acute kidney injury in octogenarians in Jordan. BMC Res Notes. 2018;11(1):279. | ||
Yao HK, Omer Binan AY, Konan SD, N’Da KJ, Diopoh SP. Mortality in the elderly with acute kidney injury in an internal medicine department in Abidjan, Cote D’Ivoire. Saudi J Kidney Dis Transpl. 2018;29(2):414–421. | ||
Rosner MH, La Manna G, Ronco C. Acute Kidney Injury in the Geriatric Population. Contrib Nephrol. 2018;193:149–160. | ||
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138. | ||
Turgutalp K, Bardak S, Horoz M, Helvacı I, Demir S, Kiykim AA. Clinical outcomes of acute kidney injury developing outside the hospital in elderly. Int Urol Nephrol. 2017;49(1):113–121. | ||
Chaumont M, Pourcelet A, van Nuffelen M, Racapé J, Leeman M, Hougardy JM. Acute kidney injury in elderly patients with chronic kidney disease: do angiotensin-converting enzyme inhibitors carry a risk? J Clin Hypertens. 2016;18(6):514–521. | ||
Mataloun SE, Machado FR, Senna APR, Guimarães HP. Amaral J.L.G. Incidence, risk factors and prognostic factors of acute renal failure in patients admitted to and intensive care unit. Rev Braz Med Biol Res. 2006;39(10):1339–1347. | ||
Junior GBS, Daher EF, Mota RMS, Menezes FA. Risk factors for death among critically ill patients with acute renal failure. Rev São Paulo Med J. 2006;12(5):257–263. | ||
Pedersen AB, Gammelager H, Kahlert J, Sørensen HT, Christiansen CF. Impact of body mass index on risk of acute kidney injury and mortality in elderly patients undergoing hip fracture surgery. Osteoporos Int. 2017;28(3):1087–1097. | ||
Nga HS, Medeiros P, Menezes P, Bridi R, Balbi A, Ponce D. Sepsis and AKI in Clinical Emergency Room Patients: The Role of Urinary NGAL. Biomed Res Int. 2015;2015:413751. | ||
Santos ER, Matos JD. Perfil epidemiologico dos pacientes com injúria renal aguda em uma unidade de terapia intensiva. Arq Cat de Med. 2008;37(4):7–11. | ||
Chronopoulos A, Cruz DN, Ronco C. Hospital-acquired acute kidney injury in the elderly. Nat Rev Nephrol. 2010;6(3):141–149. | ||
Chronopoulos A, Rosner MH, Cruz DN, Ronco C. Acute kidney injury in elderly intensive care patients: a review. Intensive Care Med. 2010;36(9):1454–1464. | ||
Funk I, Seibert E, Markau S, Girndt M. Clinical course of acute kidney injury in elderly individuals above 80 years. Kidney Blood Press Res. 2016;41(6):947–955. | ||
Petronijevic Z, Selim G, Petkovska L, Georgievska-Ismail L, Spasovski G, Tozija L. The effect of treatment on short-term outcomes in elderly patients with acute kidney injury. Open Access Maced J Med Sci. 2017;5(5):635–640. | ||
Hsu RK, Siew ED. The growth of AKI: half empty or half full, it’s the size of the glass that matters. Kidney Int. 2017;92(3):550–553. | ||
Coca SG. Acute kidney injury in elderly persons. Am J Kidney Dis. 2010;56(1):122–131. | ||
Schinstock CA, Semret MH, Wagner SJ, et al. Urinalysis is more specific and urinary neutrophil gelatinase-associated lipocalin is more sensitive for early detection of acute kidney injury. Nephrol Dial Transplant. 2013;28(5):1175–1185. | ||
Mårtensson J, Bell M, Oldner A, Xu S, Venge P, Martling CR. Neutrophil gelatinase-associated lipocalin in adult septic patients with and without acute kidney injury. Intensive Care Med. 2010;36(8):1333–1340. | ||
Anderson S, Eldadah B, Halter JB, et al. Acute kidney injury in older adults. J Am Soc Nephrol. 2011;22(1):28–38. | ||
Acunak, CE, Grover A, Camelo A, Junior RS. Características clínico-epidemiológicas de adultos e idosos atendidos em unidade de terapia intensiva pública da Amazônia (Rio Branco, Acre). Rev. bras. ter. intensiva 2007;19(3):304–309. | ||
Silveira Santos CGD, Romani RF, Benvenutti R, Ribas Zahdi JO, Riella MC, Mazza do Nascimento M. Acute Kidney Injury in Elderly Population: A Prospective Observational Study. Nephron. 2018;138(2):104–112. | ||
Shih CH, Lee YJ, Chao PW, et al. Association between influenza vaccination and the reduced risk of acute kidney injury among older people: A nested case-control study. Eur J Intern Med. 2018;pii: S0953-6205(18):30174-2. | ||
Davison BA, Metra M, Cotter G, et al. Worsening Heart Failure Following Admission for Acute Heart Failure: A Pooled Analysis of the PROTECT and RELAX-AHF Studies. JACC Heart Fail. 2015;3(5):395–403. | ||
Brown MA, Collett GK, Josland EA, Foote C, Li Q, Brennan FP. CKD in elderly patients managed without dialysis: survival, symptoms, and quality of life. Clin J Am Soc Nephrol. 2015;10(2):260–268. | ||
Chao CT, Lin YF, Tsai HB, Wu VC, Ko WJ. Acute kidney injury network staging in geriatric postoperative acute kidney injury patients: shortcomings and improvements. J Am Coll Surg. 2013;217(2):240–250. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.