")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Acupuncture Treatment is Associated with a Decreased Risk of Dementia in Patients with Depression: A Propensity Score-Matched Cohort Study
Authors Chen KY, Huang MC , Lin CL, Lee YC , Wu MY , Yen HR
Received 25 July 2021
Accepted for publication 12 October 2021
Published 4 November 2021 Volume 2021:17 Pages 3255—3266
DOI https://doi.org/10.2147/NDT.S331026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Kuan-Yu Chen,1 Ming-Cheng Huang,2,3 Cheng-Li Lin,4 Yu-Chen Lee,2,3,5 Mei-Yao Wu,2,6,* Hung-Rong Yen2,3,7– 9,*
1Department of Chinese Medicine, Taipei City Hospital, Yangming Branch, Taipei, Taiwan; 2Department of Chinese Medicine, China Medical University Hospital, Taichung, Taiwan; 3Graduate Institute of Chinese Medicine, School of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 4Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan; 5Graduate Institute of Acupuncture Science, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 6School of Post-Baccalaureate Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan; 7Research Center for Traditional Chinese Medicine, Department of Medical Research, China Medical University Hospital, Taichung, Taiwan; 8Chinese Medicine Research Center, China Medical University, Taichung, Taiwan; 9Department of Medical Laboratory Science and Biotechnology, Asia University, Taichung, Taiwan
*These authors contributed equally to this work
Correspondence: Hung-Rong Yen
Graduate Institute of Chinese Medicine, School of Chinese Medicine, College of Chinese Medicine, China Medical University, 91 Hsueh-Shih Road, North District, Taichung, 404328, Taiwan
Tel +886-4-22053366 ext. 3001
Fax +886-4-22365141
Email [email protected]
Mei-Yao Wu
School of Post-Baccalaureate Chinese Medicine, College of Chinese Medicine, China Medical University, 91 Hsueh-Shih Road, North District, Taichung, 404328, Taiwan
Tel +886-4-22052121 ext. 4561
Fax +886-4-22037690
Email [email protected]
Background: Depression is one of the most disabling disorders, which causes long-term complications such as neurodegenerative disorder and cerebrovascular disease. Some patients with depression seek acupuncture treatment. We aimed to investigate the association between acupuncture treatment and the risk of dementia in patients with depression from the perspective of real-world evidence.
Methods: Patients over 18 years old and newly diagnosed with depression between 1997 and 2010 were selected from the Taiwanese National Health Insurance Research Database and followed up until the end of 2013. Propensity score was used to match equal numbers of patients 1:1 (N = 16,609 per group) into acupuncture and non-acupuncture cohorts based on characteristics including sex, age, baseline comorbidity and drug use. The outcome measurement was the comparison of dementia incidence in the two cohorts.
Results: Compared with the non-acupuncture cohort, patients who received acupuncture treatment had a decreased risk of dementia (adjusted hazard ratio (aHR) = 0.54; 95% confidence interval (CI) = 0.50– 0.58, P < 0.001) after adjustment for age, sex, comorbidities and drug use. Compared with depression patients who did not receive acupuncture, the aHR of vascular dementia and Alzheimer’s disease incidences for patients who had acupuncture therapy was 0.59 (95% CI 0.48– 0.71) and 0.51 (95% CI 0.39– 0.67), respectively. The cumulative incidence of dementia was significantly lower in the acupuncture cohort than in the non-acupuncture cohort (Log rank test, p < 0.001).
Conclusion: The present study from real-world data revealed that acupuncture reduced the risk of dementia in depression patients, which supports healthcare decisions in clinical practice.
Keywords: acupuncture, Alzheimer’s disease, depression, dementia, National Health Insurance Research Database, NHIRD, traditional Chinese medicine
Introduction
Depression, also called major depressive disorder (MDD), is a condition characterized by a gloomy (depressed) mood or anhedonia, which means a loss of interest in usually pleasurable activities. The DSM-5 criteria for major depressive disorder (MDD) include the presence of either of those symptoms for at least two weeks, plus four or more following symptoms: low energy or fatigue, insomnia or hypersomnia, loss or increased appetite/weight, psychomotor retardation or agitation, poor concentration or indecisiveness, suicidal ideation, and pathological guilt or feelings of worthlessness.1,2 Depression is common among adults worldwide. The World Health Organization estimates that 350 million people globally have depressive episodes. The World Mental Health Survey conducted in 17 countries found that, on average, approximately 5% of people have had depressive episodes. Moreover, approximately 1 million people with depression lose their lives due to suicide yearly, which means 3000 suicide deaths per day.3
Dementia is one of the major causes of disability in old age. It is a condition that is characterized by a decrease in cognition involving one or more cognitive domains (learning and memory, language, executive function, complex attention, perceptual-motor function, social cognition)2,4 As of 2010, there were 35.6 million people with dementia worldwide. The number is predicted to reach 65.7 million in 2030 and 115.4 million in 2050.5 Dementia mainly affects older people, and its prevalence increases exponentially with age. Depression and dementia commonly occur together in elderly people. Recent studies indicate that early-life depression could be a risk factor for later dementia and that later-life depression is a prodrome of dementia.6 These findings show the importance of effective treatment for depression, which may reduce the prevalence of dementia.
The most common standard initial therapy for depression consists of psychotherapy and antidepressants such as SSRIs, MAOIs, TCAs, SNRIs, NDRIs, SARIs and NaSSAs.7 However, antidepressants may cause side effects such as weight gain, sedation, dry mouth, nausea, blurred vision, constipation, and tachycardia.8,9 Therefore, some patients who suffer from depression may seek complementary or alternative treatments. One American survey revealed that 34% of psychiatric outpatients with depression were using alternative therapies.10 Another survey showed that 20% of depressed Americans had used complementary and alternative medicine therapy, including acupuncture, for their depression.11 In addition, among people seeking acupuncture in the United Kingdom, psychological distress, including depression, was the second most common reason.12 Acupuncture is one of the most popular complementary therapies in Taiwan.13,14 Some previous studies have indicated the benefits of acupuncture for depression. Chan’s systematic review and meta-analysis indicated that acupuncture combined with antidepressants is effective against depression. The therapeutic efficacy of the combination was better than that of antidepressants alone.15 Similar results were also found in another systematic review and meta-analysis, which indicated that early treatment of primary depression using SSRIs combined with electroacupuncture therapy was more efficient than SSRIs alone and led to better and earlier control of depressive symptoms.16 Another systematic review and meta-analysis showed that the incidence of side effects of acupuncture intervention was significantly lower than that of antidepressants in depression patients.17 Recent research shows that acupuncture may also be safe for treating dementia and may enhance the positive effect of drugs on cognitive function, allowing dementia patients to go about their daily lives.18 However, none of them have shown the evidence regarding the effects of acupuncture on the progression to dementia in patients with depression.
Taiwan launched the National Health Insurance (NHI) program in 1995. This compulsory insurance program covers more than 99% of all residents in Taiwan, and it provides universal care to the people of Taiwan. The NHI program began reimbursing Western medical services in 1995 and traditional Chinese medicine (TCM) services in 1996. The NHI administration has established a National Health Insurance Research Database (NHIRD), which includes all claims data. These datasets provided real-world data with long-term follow-up information, reducing the potential for sampling bias.19 Our previous studies have also shown that acupuncture treatment is beneficial for patients with fibromyalgia,20,21 arthritis,22,23 and depression24 in the NHIRD. As recently noted, “real-world” data are not inferior to clinical trials and may provide useful information.25 Due to the shortage of existing long-term follow-up studies, our study aims to determine whether acupuncture can decrease the risk of progression to dementia in patients with depression by using a random sample of one million patients selected from the NHIRD.
Materials and Methods
Data Source
The data in this study are selected from the Taiwanese NHIRD (https://nhird.nhri.org.tw/en/), which contains the registration files and original claims data for reimbursements, including demographic characteristics, diagnoses, clinical visits, hospitalizations, procedures, prescriptions, and the medical costs for reimbursement; this information is provided to scientists in Taiwan for research purposes. The NHI program covers TCM services, including Chinese herbal medicine, manipulative therapies and acupuncture. The diagnostic codes follow the format of the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM).
Study Population and Variables
The flowchart for enrolling patients with depression and dementia is shown in Figure 1. A sample of one million randomly selected individuals from the NHIRD database was used in this study. Patients (n = 65,569) with diagnosed depression (ICD-9-CM code: 296.2–296.3, 300.4, 311) between January 1997 and December 2010 were included in this study and then followed up until the end of 2013. Next, we narrowed the selection to patients who were newly diagnosed with depression between 1997 and 2010 and had at least 2 claims during that period. We excluded 1840 individuals who were younger than 18 years of age or who had missing information such as date of birth or sex. In addition, we excluded 3343 individuals whose date of dementia diagnosis (ICD-9-CM: 290, 294.1, 331.0–331.2) was before the date of depression diagnosis. In all, after these exclusions, there were 49,993 patients with newly diagnosed depression and at least 2 claims during the period from 1997 to 2010. The remaining patients were divided into two groups: those who received acupuncture treatment (n =23,149) and those who did not (n=26,844). We defined the date of first acupuncture treatment after the date of the new depression diagnosis as the index date for the acupuncture group, and we randomly chose a date between the date of the new depression diagnosis and the endpoint as the index date for the control group. The acupuncture treatment (n =16,609) group and the control (n=16,609) group were matched 1:1 for propensity score by age (in 5-year bins), sex, index year, initial year of diagnosis of depression, all comorbidities, and all drugs used (oral steroids; nonsteroidal anti-inflammatory drugs (NSAIDs); statins; and selective serotonin reuptake inhibitors (SSRIs: escitalopram, fluvoxamine, sertraline), monoamine oxidase inhibitors (MAOIs: selegiline, isocarboxazid, tranylcypromine, phenelzine, moclobemide), tricyclic antidepressants (TCAs: amoxapine, desipramine, imipramine, doxepin, clomipramine, trimipramine) and other antidepressant drugs (serotonin–norepinephrine reuptake inhibitors, SNRIs: venlafaxine, duloxetine, milnacipran; norepinephrine–dopamine reuptake inhibitor, NDRI: bupropion; serotonin antagonist and reuptake inhibitor, SARI: mesyrel; noradrenergic and specific serotonergic antidepressant, NaSSA: mirtazapine)) (Figure 1).
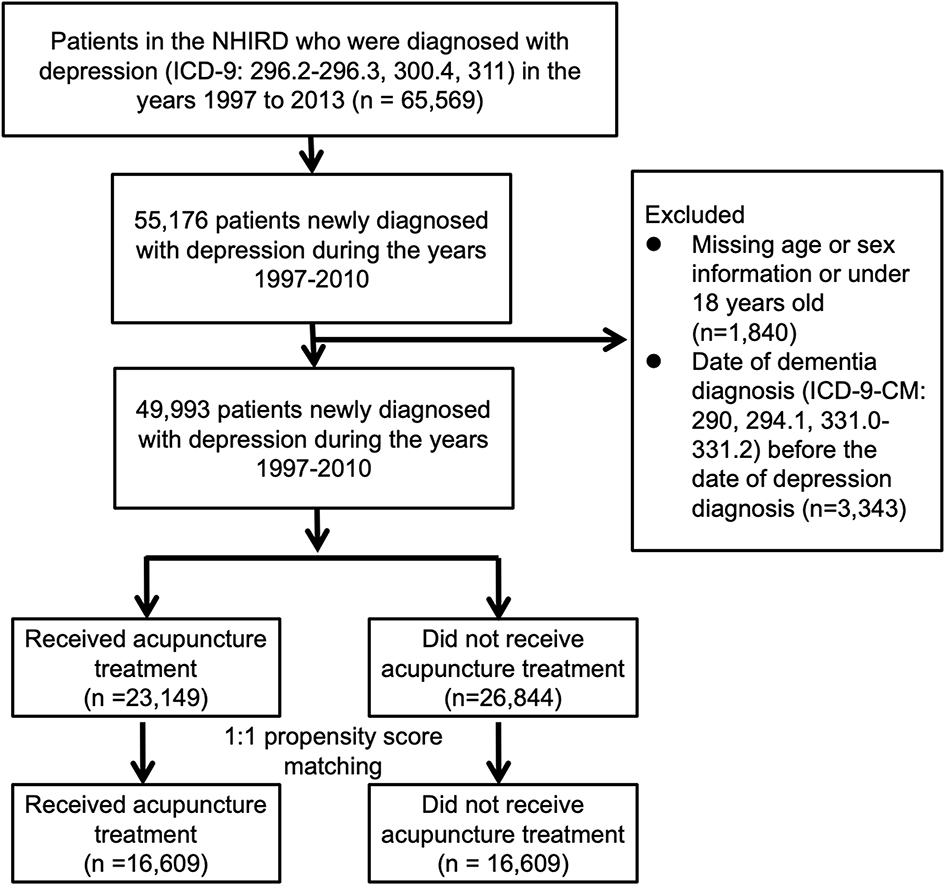 |
Figure 1 Flow chart of the selection of patients with depression from the National Health Insurance Research Database (NHIRD) between 1997 and 2000 in Taiwan. After excluding the patients who did not meet the inclusion criteria and matching by propensity score, the acupuncture and non-acupuncture cohorts each contained an equal number of patients. |
Ethical Considerations
The investigation was carried out in accordance with the latest version of the Declaration of Helsinki. The National Health Research Institutes encrypted all information that could be used to identify individuals or care providers before release; it is therefore impossible to identify any individuals or care providers in the database. The Research Ethics Committee of China Medical University and Hospital approved this study and waived the requirement for informed consent (CMUH104-REC2-115).
Availability of Data and Material
The datasets analyzed from NHIRD were provided by the National Health Insurance Administration and maintained by the National Health Research Institutes of Taiwan. The use of NHIRD is limited to research purposes only. Applicants must follow the Computer-Processed Personal Data Protection Law (http://www.winklerpartners.com/?p=987) and related regulations of the National Health Insurance Administration and National Health Research Institutes.
Statistical Analysis
We used SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA), to analyze the data from the NHIRD. Descriptive statistics were applied to determine the demographic characteristics, treatment modalities, and frequency of prescriptions for acupuncture. The diagnoses were coded according to the ICD-9-CM codes. Data missing the important information such as date of birth or sex were excluded. To present the overall structure of the study groups, we calculated the mean and standard deviation (SD) for age and the percentage for sex, comorbidity, drug use, and types of acupuncture. To evaluate the distribution differences between acupuncture and non-acupuncture users, we used Student’s t-test for continuous variables and the chi-squared test for categorical variables. The Cox proportional hazard regression model was applied to estimate the hazard ratio (HR) and 95% confidence interval (CI) of dementia in patients with depression who received acupuncture compared with non-acupuncture users. We also used the Kaplan-Meier method and the Log rank test to estimate the cumulative risk of dementia with depression between acupuncture users and non-acupuncture users.
Results
After propensity score-matching by age (per 5 years), sex, index year, initial year of diagnosis of depression, all comorbidities, and drugs used (oral steroids; NSAIDs; statins; and SSRIs, MAOIs, TCAs and other antidepressant drugs), the acupuncture users (n=16,609) and non-acupuncture users (n=16,609) had similar demographic characteristics. Most acupuncture users received manual acupuncture (87.14%), while some received electroacupuncture (2.97%) and others used a combination of manual acupuncture and electroacupuncture (9.89%) (Table 1).
 |
Table 1 Characteristics of Depression Patients According to Whether They Received Acupuncture |
Compared with depression patients who did not receive acupuncture treatment, the adjusted hazard ratio for dementia in patients who received acupuncture therapy was 0.54 (95% CI, (0.50–0.58), P < 0.001) (Table 2). The age-stratified results demonstrated that the risk of dementia increased with age. Depression patients over 60 years old had the highest risk of dementia (aHR, 26.51; 95% CI, (21.39–32.86), P < 0.001). Regarding comorbidities before the initial diagnosis date of depression, there was no significant relationship between the risk of dementia and anxiety, tobacco use or obesity. However, there was a significant relationship between the risk of dementia and comorbidities such as diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, and alcoholism. Depression patients with these comorbidities had an elevated risk of dementia (Table 2).
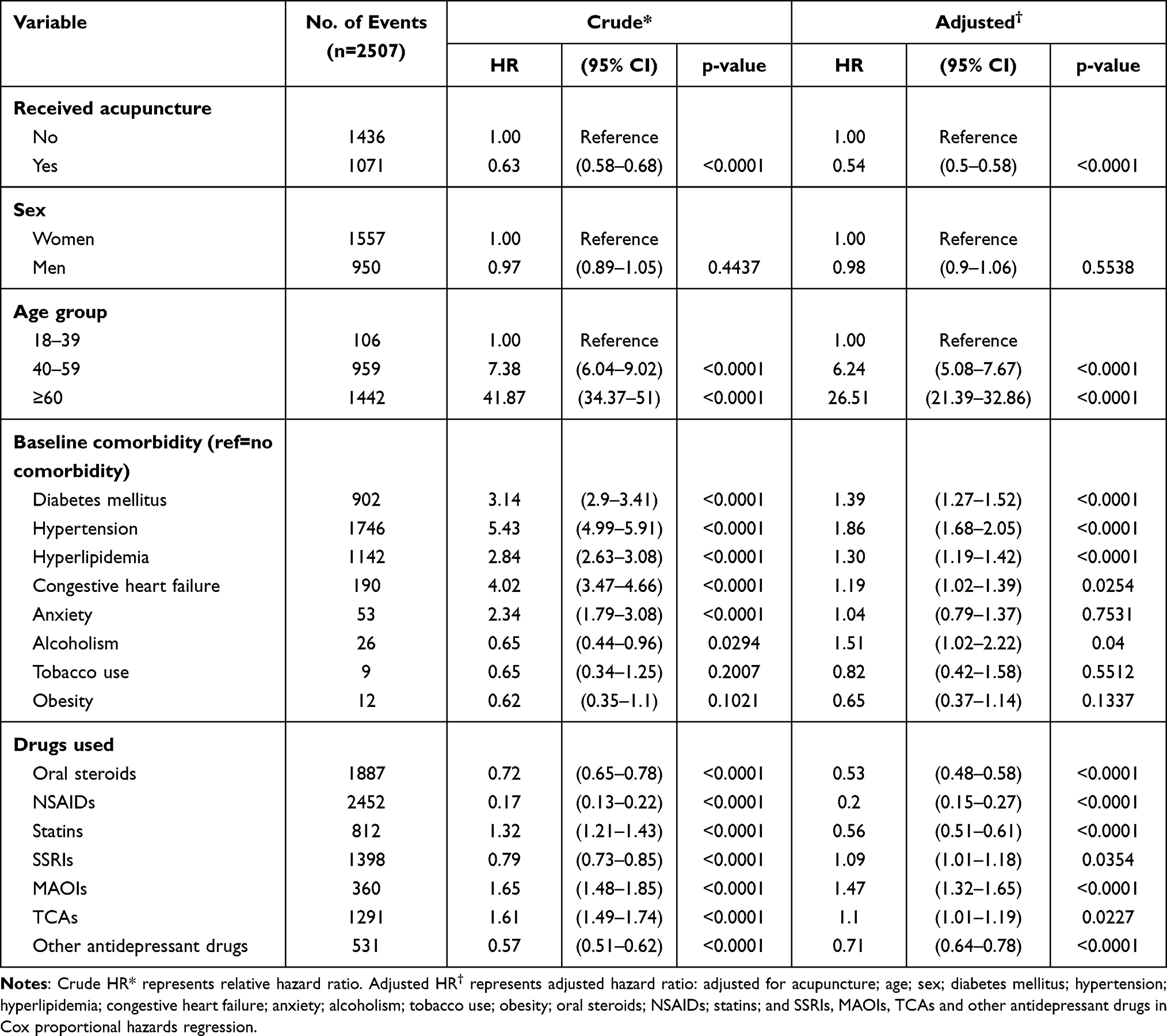 |
Table 2 Cox Model with Hazard Ratios and 95% Confidence Intervals of Dementia Associated with Acupuncture and Covariates Among Depression Patients |
In addition, there was a significant relationship between the risk of dementia and whether drugs were used to treat depression after diagnosis. Compared to the group who did not use drugs, the patients who used SSRIs, MAOIs and TCAs had an elevated aHR (1.09, 1.47 and 1.1). This may be because patients who used these antidepressants initially had more severe depression than those who did not take them. However, the patients who used oral steroids, NSAIDs, statins and other antidepressant drugs had reduced aHRs (0.53, 0.20, 0.56 and 0.71).
In this study, 1071 patients in the acupuncture cohort (12.11 per 1000 person-years) and 1436 patients in the non-acupuncture cohort (19.68 per 1000 person-years) developed dementia (Table 3). The beneficial effect of acupuncture on the incidence of dementia was noted in both female and male patients (female aHR, 0.53; 95% CI, 0.48–0.58; male aHR, 0.56; 95% CI, 0.49–0.63). Although the risk of dementia gradually increased with age, acupuncture significantly decreased the progression of dementia in all age groups. Acupuncture decreased the risk of dementia in patients with depression with and without comorbidities (diabetes mellitus, hypertension, hyperlipidemia, congestive heart failure, anxiety, alcoholism, tobacco use, and obesity). Regardless of whether patients took oral steroids; NSAIDs; statins; or SSRIs, MAOIs, TCAs and other antidepressant drugs, fewer patients in the acupuncture cohort than in the non-acupuncture cohort developed dementia.
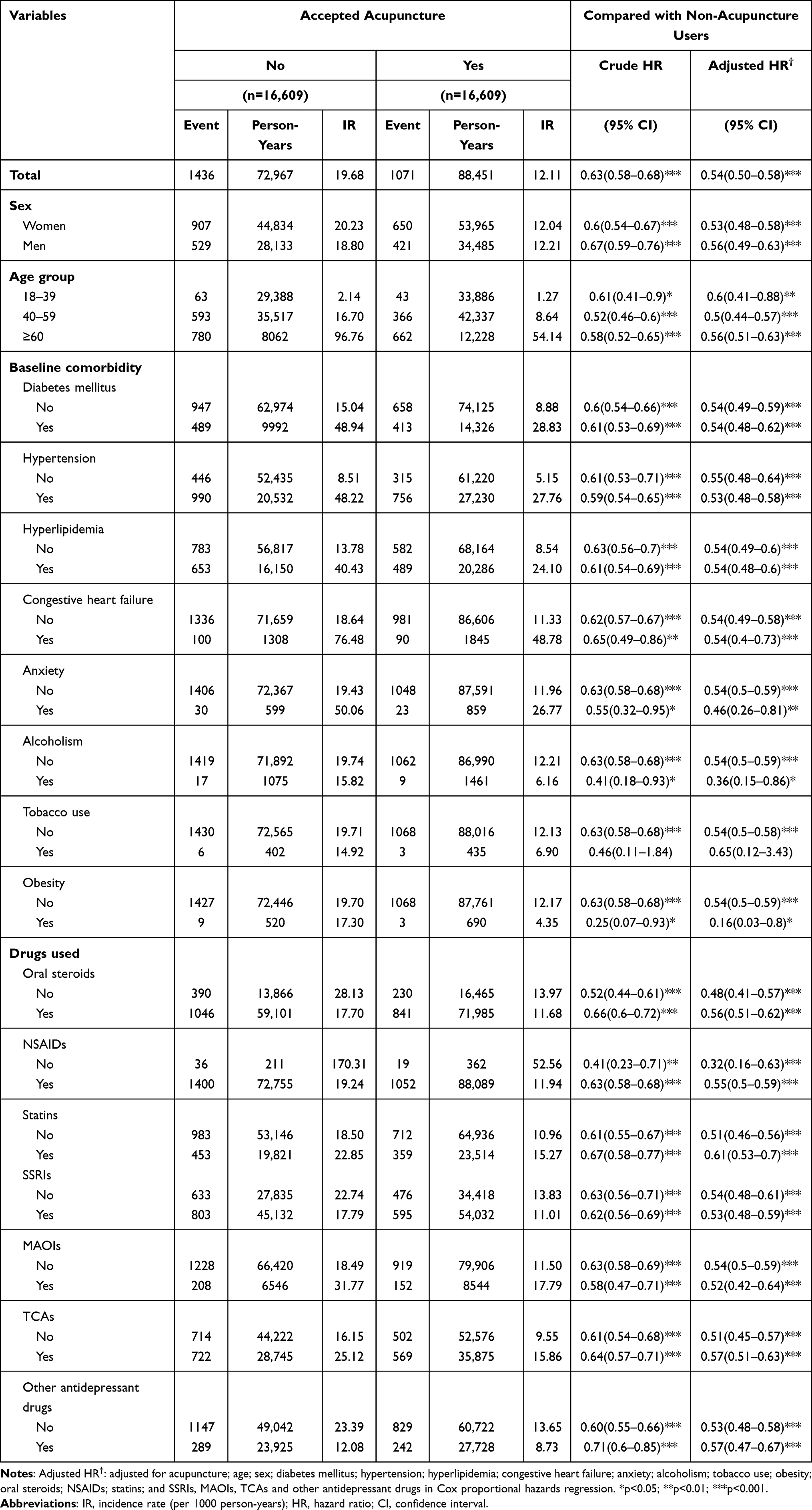 |
Table 3 Incidence Rates, Hazard Ratios and Confidence Intervals of Dementia for Those Depression Patients Who Received Acupuncture and Those Who Did Not, Stratified by Sex, Age, Comorbidities and Drug Use |
We also analyzed the incidence rates, hazard ratio and confidence intervals of vascular dementia (ICD-9-CM: 290.4) and Alzheimer’s disease (ICD-9-CM: 331.0) for depression patients who received acupuncture and those who did not. The acupuncture cohort had a reduced risk of vascular dementia and Alzheimer’s disease (Table 4). In this study, 193 patients in the acupuncture cohort (2.18 per 1000 person-years) and 226 patients in the non-acupuncture cohort (3.19 per 1000 person-years) developed vascular dementia. Compared with depression patients who did not receive acupuncture, the aHR of vascular dementia incidence for patients who had acupuncture therapy was 0.59 (95% CI 0.48–0.71). There were 96 patients in the acupuncture cohort (1.08 per 1000 person-years) and 126 patients in the non-acupuncture cohort (1.72 per 1000 person-years) who developed Alzheimer’s disease. Compared with depression patients who did not receive acupuncture, the aHR of Alzheimer’s disease incidence for patients who had acupuncture therapy was 0.51 (95% CI 0.39–0.67).
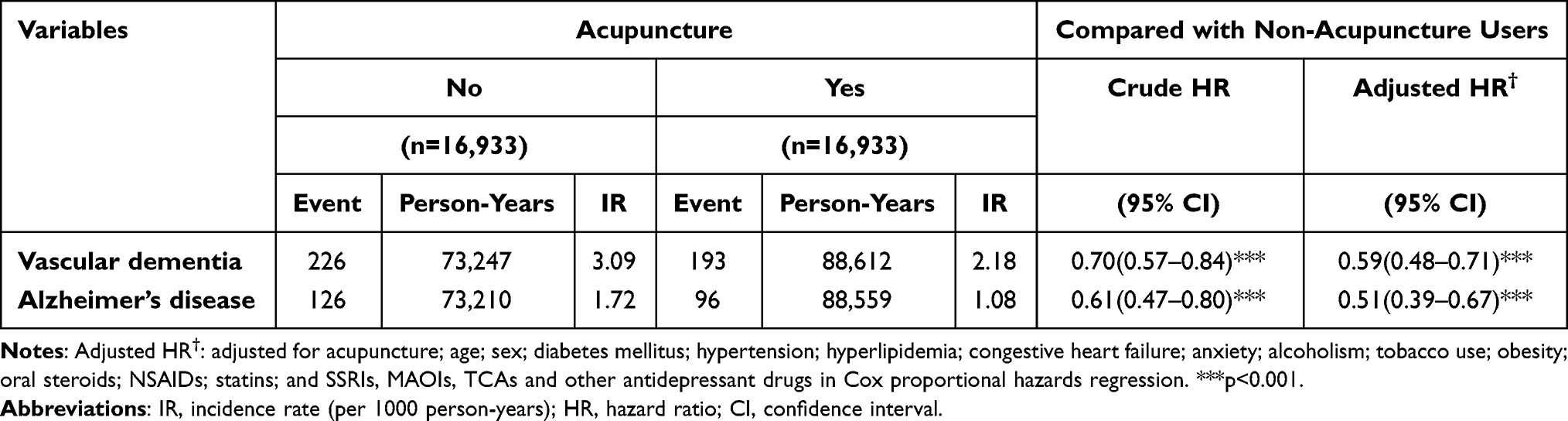 |
Table 4 Incidence Rates, Hazard Ratio and Confidence Intervals of Vascular Dementia (ICD-9-CM: 290.4) and Alzheimer’s Disease (ICD-9-CM: 331.0) for Those Depression Patients Who Received Acupuncture and Those Who Did Not, Stratified by Sex, Age, Comorbidities and Drug Use |
Figure 2 reveals the cumulative incidence of dementia. Overall, the results suggest that in patients with depression, the cumulative incidence of dementia was lower in acupuncture users than in non-acupuncture users during the follow-up period (Log rank test, P < 0.001).
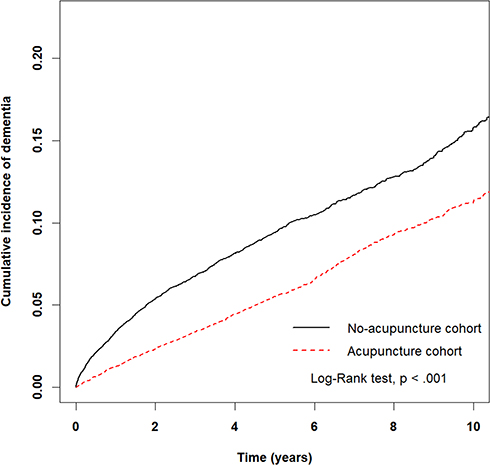 |
Figure 2 Cumulative incidence of dementia between the acupuncture cohort and the non-acupuncture cohort. The cumulative incidence of dementia was significantly lower in the acupuncture cohort than in the non-acupuncture cohort (Log rank test, p < 0.0001). |
Discussion
In this study, we provided some evidence, although not a clinical trial, from the “real-world” data demonstrating the association between the acupuncture treatments and the reduced risk of developing dementia in patients with depression. Our study has several strengths. The “real-world” data from the NHIRD provided large-scale cohort with long-term follow-up data.19 The current knowledge regarding the efficacy of clinical intervention is usually limited to clinical trials.25 None of the previous data regarding the utilization of acupuncture for depression are supported by large-scale “real-world” data. As all patients with depression were registered in the NHI program since 1995, we were able to use the database to perform this study. These datasets provide a nationwide population-based claim database with long-term follow-up data. Thus, this propensity-score matched data are highly reliable, reducing the potential for sampling and allocation bias.
As a popular alternative treatment for depression, acupuncture has been performed on patients with depression in several clinical trials. However, most previous studies have focused on the effectiveness and safety of acupuncture therapy in depressive disorders. In addition, current studies on the benefits of acupuncture for depression and dementia are limited. Systematic reviews have shown the disadvantages of recent clinical trials, such as small sample size, uncertain description of enrolment criteria, poor quality of randomization or blinding, and different forms of acupuncture. Our research showed that depression patients who received acupuncture had a lower risk of developing dementia than the non-acupuncture cohort. To the best of our knowledge, this is the first large-scale population-based cohort study to demonstrate a decreased dementia risk in depression patients receiving acupuncture therapy.
Acupuncture may be associated with a reduced risk of dementia in patients with depression for several reasons. Recent studies have presented some possible explanations for the benefits of acupuncture against dementia. In a series of studies using animal models of Alzheimer’s disease, electroacupuncture stimulation reduced mitochondrial damage and amyloid beta plaques in the hippocampal CA1 region and increased the levels of choline acetyltransferase (ChAT) in the brain, as well as the capacity for learning and memory.26–28 A previous mouse study found that acupuncture completely or partially reversed some aging-related changes in hippocampal gene expression profiles.29 Other mouse research also showed that acupuncture reduced cognitive deficits and neuronal loss in the hippocampal CA3 region and DG.30,31 In addition, a previous research indicated that electroacupuncture decreased Aβ protein expression and oxidative damage in the hippocampus of a rate model.32 Stem cell mobilization and progenitor cell proliferation in the central nervous system may also occur after acupuncture treatment for neurodegenerative diseases.31,33
A previous study using resting-state functional magnetic resonance imaging (RS-fMRI) found that acupuncture stimulation could modulate the activity of the default mode network in Alzheimer’s disease patients.34 Another fMRI study indicated that acupuncture could improve hippocampal connectivity in Alzheimer’s disease patients.35 It was also found that the right hemisphere (the temporal lobe, such as the hippocampal gyrus; the insula; and some areas of the parietal lobe) and left hemisphere (the temporal lobe, the parietal lobules, and some regions of the cerebellum) were activated after acupuncture therapy. The regions activated by acupuncture overlap with the areas of the brain that are impaired in Alzheimer’s disease patients.36
Alzheimer’s disease is the most common form of dementia in the elderly, accounting for 60–80% of cases.37 After Alzheimer’s disease, vascular dementia is the second most common form of dementia in most clinical series, accounting for 10–20% of cases in North America and Europe.38,39 In this study, we found that the acupuncture cohort with depression had a lower risk of vascular dementia and Alzheimer’s disease compared with depression patients who did not receive acupuncture. The common mechanism that acupuncture reduced the risk of both types of dementia still need further laboratory investigations.
It has to be point out that our research also has some limitations. First, the NHIRD did not provide data to measure the severity of depressive disorders. To minimize this confounding factor, we performed 1:1 propensity score matching to ensure that all the baseline characteristics of both cohorts (including the anti-depressants) were similar. Second, the lifestyles of the two cohorts could be different. The NHIRD did not provide data about patients’ lifestyles, such as smoking frequency, body mass index (BMI), stress, and exercise. Studies have indicated that many dementia cases are attributable to risk factors such as obesity, physical inactivity, and smoking.40 Since data on lifestyle factors were deficient, we had only a limited ability to study these personal habits and customs in connection with illness. We performed 1:1 propensity score matching including the diagnoses of tobacco use and obesity and found that the comorbidities of both cohorts were similar. However, the percentages of smoking and obesity were still underestimated in both cohorts. Third, patients who seek acupuncture may have an increased level of motivation to address depression. Although the co-pay of acupuncture therapy is low (5–7 USD per treatment) under the NHI program, it is still a burden for poor people to consult doctors frequently. Thus, acupuncture users may have greater financial ability to obtain tangible or intangible resources than non-users.
Conclusion
Patients who suffer from depression may utilize complementary therapies; in Taiwan, many patients choose acupuncture. Our study suggests that acupuncture treatment is associated with a reduced risk of dementia in patients with depression. We hope that additional clinical trials and research studies based on this study’s findings will be undertaken in the future. Further research is necessary to determine the mechanism behind the protective effect of acupuncture.
Data Sharing Statement
The datasets we used in this study were released by the Taiwan NHIRD (https://nhird.nhri.org.tw/en/), maintained and managed by National Health Research Institutes (http://www.nhri.org.tw/), Taiwan. The datasets are limited to be used for research purposes only. Applicants must follow the Computer-Processed Personal Data Protection Law (http://www.winklerpartners.com/?p= 987) and related regulations of National Health Insurance Administration and National Health Research Institutes, and the agreement must be signed by the applicant and his/her supervisor upon application submission. All applications are reviewed for approval of data release.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. Mei-Yao Wu and Hung-Rong Yen contributed equally as co-corresponding authors.
Funding
This work was financially supported by the Chinese Medicine Research Center, China Medical University, from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan (CMRC-CHM-2). This study was also partially supported by China Medical University (CMU103-BC-4-2, CMU105-BC-1-1, CM105-BC-1-2); the health and welfare surcharge of tobacco products, China Medical University Hospital Cancer Research Center of Excellence (MOHW110-TDU-B-212-144024), Taiwan; the Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW110-TDU-B-212-124004). None of the funders and institutions listed had a role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Thase ME. The multifactorial presentation of depression in acute care. J Clin Psychiatry. 2013;74(Suppl 2):3–8. doi:10.4088/JCP.12084su1c.01
2. Association AP. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5).
3. Marcus M, Yasamy MT, van Ommeren MV, Chisholm D, Saxena S. Depression: a global public health concern. [Internet] WHO Department of Mental Health and Substance Abuse; 2012 [cited 2021 Oct 30] p.6-8. Available from: https://who.int/mental_health/management/depression/who_paper_depression_wfmh_2012.pdf.
4. Sachdev PS, Blacker D, Blazer DG, et al. Classifying neurocognitive disorders: the DSM-5 approach. Nat Rev Neurol. 2014;10(11):634–642. doi:10.1038/nrneurol.2014.181
5. World Health Organization. Dementia: A Public Health Priority. World Health Organization; 2012.
6. Bennett S, Thomas AJ. Depression and dementia: cause, consequence or coincidence? Maturitas. 2014;79(2):184–190. doi:10.1016/j.maturitas.2014.05.009
7. Gelenberg AJ, Freeman MP, Markowitz JC, et al. Practice Guideline for the Treatment of Patients with Major Depressive Disorder (Third Edition).
8. Blier P. The pharmacology of putative early-onset antidepressant strategies. Eur Neuropsychopharmacol. 2003;13(2):57–66. doi:10.1016/S0924-977X(02)00173-6
9. Wu J, Yeung AS, Schnyer R, Wang Y, Mischoulon D. Acupuncture for depression: a review of clinical applications. Can J Psychiatry. 2012;57(7):397–405. doi:10.1177/070674371205700702
10. Knaudt PR, Connor KM, Weisler RH, Churchill LE, Davidson JR. Alternative therapy use by psychiatric outpatients. J Nerv Ment Dis. 1999;187(11):692–695. doi:10.1097/00005053-199911000-00007
11. Ernst E, Rand JI, Stevinson C. Complementary therapies for depression: an overview. Arch Gen Psychiatry. 1998;55(11):1026–1032. doi:10.1001/archpsyc.55.11.1026
12. MacPherson H, Sinclair-Lian N, Thomas K. Patients seeking care from acupuncture practitioners in the UK: a national survey. Complement Ther Med. 2006;14(1):20–30. doi:10.1016/j.ctim.2005.07.006
13. Wang C, Lee YC, Wu MY, et al. Trends in the utilization of acupuncture among children in Taiwan from 2002 to 2011: a nationwide population-based study. BMC Complement Altern Med. 2019;19(1):328. doi:10.1186/s12906-019-2753-8
14. Wu MY, Lee YC, Lin CL, Huang MC, Sun MF, Yen HR. Trends in use of acupuncture among adults in Taiwan from 2002 to 2011: a nationwide population-based study. PLoS One. 2018;13(4):e0195490. doi:10.1371/journal.pone.0195490
15. Chan YY, Lo WY, Yang SN, Chen YH, Lin JG. The benefit of combined acupuncture and antidepressant medication for depression: a systematic review and meta-analysis. J Affect Disord. 2015;176:106–117. doi:10.1016/j.jad.2015.01.048
16. Musil R, Zhang Y, Qu -S-S, et al. [Rapid onset of the effects of combined selective serotonin reuptake inhibitors and electroacupuncture on primary depression: a meta-analysis]. Dtsch Zeitschrift für Akupunkt. 2016;59(3):27–29. German. doi:10.1016/S0415-6412(16)30084-4
17. Zhang ZJ, Chen HY, Yip KC, Ng R, Wong VT. The effectiveness and safety of acupuncture therapy in depressive disorders: systematic review and meta-analysis. J Affect Disord. 2010;124(1–2):9–21. doi:10.1016/j.jad.2009.07.005
18. Zhou J, Peng W, Xu M, Li W, Liu Z. The effectiveness and safety of acupuncture for patients with Alzheimer disease: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2015;94(22):e933. doi:10.1097/MD.0000000000000933
19. Hsing AW, Ioannidis JP. Nationwide population science: lessons from the Taiwan national health insurance research database. JAMA Intern Med. 2015;175(9):1527–1529. doi:10.1001/jamainternmed.2015.3540
20. Huang MC, Yen HR, Lin CL, Lee YC, Sun MF, Wu MY. Acupuncture decreased the risk of stroke among patients with fibromyalgia in Taiwan: a nationwide matched cohort study. PLoS One. 2020;15(10):e0239703. doi:10.1371/journal.pone.0239703
21. Wu MY, Huang MC, Chiang JH, Sun MF, Lee YC, Yen HR. Acupuncture decreased the risk of coronary heart disease in patients with fibromyalgia in Taiwan: a nationwide matched cohort study. Arthritis Res Ther. 2017;19(1):37. doi:10.1186/s13075-017-1239-7
22. Ton G, Yang YC, Lee LW, et al. Acupuncture decreased the risk of coronary heart disease in patients with osteoarthritis in Taiwan: a Nationwide Matched Cohort Study. J Altern Complement Med. 2021;27(S1):S60–S70. doi:10.1089/acm.2020.0153
23. Wu MY, Huang MC, Liao HH, et al. Acupuncture decreased the risk of coronary heart disease in patients with rheumatoid arthritis in Taiwan: a Nationwide propensity score-matched study. BMC Complement Altern Med. 2018;18(1):341. doi:10.1186/s12906-018-2384-5
24. Chen LY, Yen HR, Sun MF, Lin CL, Chiang JH, Lee YC. Acupuncture treatment is associated with a decreased risk of developing stroke in patients with depression: a propensity-score matched cohort study. J Affect Disord. 2019;250:298–306. doi:10.1016/j.jad.2019.03.020
25. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-world evidence - what is it and what can it tell us? N Engl J Med. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
26. Xue WG, Ge GL, Zhang Z, Xu H, Bai LM. [Effect of electroacupuncture on the behavior and hippocampal ultrastructure in APP 695 V 717 I transgenic mice]. Zhen Ci Yan Jiu. 2009;34(5):309–314. Chinese.
27. Xue WG, Zhang Z, Bai LM, Xu H, Wu HX. [Effect of electroacupuncture on the behavior and the expression of amyloid beta-protein, amyloid precursor protein and ChAT in APP 695 V 717 I transgenic mice]. Zhen Ci Yan Jiu. 2009;34(3):152–158. Chinese.
28. Xue WG, Zhang Z, Xu H, Wu HX, Bai LM. [Effect of electroacupuncture on learning-memory ability, and abeta and LRP1 immunoactivity in hippocampal sulcus microvessels in APP transgenic mice]. Zhen Ci Yan Jiu. 2011;36(2):95–100. Chinese.
29. Ding X, Yu J, Yu T, Fu Y, Han J. Acupuncture regulates the aging-related changes in gene profile expression of the hippocampus in senescence-accelerated mouse (SAMP10). Neurosci Lett. 2006;399(1–2):11–16. doi:10.1016/j.neulet.2006.01.067
30. Li G, Zhang X, Cheng H, et al. Acupuncture improves cognitive deficits and increases neuron density of the hippocampus in middle-aged SAMP8 mice. Acupunct Med. 2012;30(4):339–345. doi:10.1136/acupmed-2012-010180
31. Cheng H, Yu J, Jiang Z, et al. Acupuncture improves cognitive deficits and regulates the brain cell proliferation of SAMP8 mice. Neurosci Lett. 2008;432(2):111–116. doi:10.1016/j.neulet.2007.12.009
32. Zhang P, Guan SS, Jiang GH. [Effects of electroacupuncture on expression of abeta positive cells of the hippocampus and SOD activity in rats with streptozocin-Alzheimer’s disease]. Zhongguo Zhen Jiu. 2010;30(12):1007–1010. Chinese.
33. Ho TJ, Chan TM, Ho LI, et al. The possible role of stem cells in acupuncture treatment for neurodegenerative diseases: a literature review of basic studies. Cell Transplant. 2014;23(4–5):559–566. doi:10.3727/096368914X678463
34. Liang P, Wang Z, Qian T, Li K. Acupuncture stimulation of taichong (Liv3) and Hegu (LI4) modulates the default mode network activity in Alzheimer’s disease. Am J Alzheimers Dis Other Demen. 2014;29(8):739–748. doi:10.1177/1533317514536600
35. Wang Z, Liang P, Zhao Z, et al. Acupuncture modulates resting state hippocampal functional connectivity in Alzheimer disease. PLoS One. 2014;9(3):e91160. doi:10.1371/journal.pone.0091160
36. Zhou Y, Jin J. Effect of acupuncture given at the HT 7, ST 36, ST 40 and KI 3 acupoints on various parts of the brains of Alzheimer’ s disease patients. Acupunct Electrother Res. 2008;33(1–2):9–17. doi:10.3727/036012908803861186
37. Hebert LE, Scherr PA, Bienias JL, Bennett DA, Evans DA. Alzheimer disease in the US population: prevalence estimates using the 2000 census. Arch Neurol. 2003;60(8):1119–1122. doi:10.1001/archneur.60.8.1119
38. Lobo A, Launer LJ, Fratiglioni L, et al. Prevalence of dementia and major subtypes in Europe: a collaborative study of population-based cohorts. Neurologic diseases in the elderly research group. Neurology. 2000;54(11 Suppl 5):S4–S9.
39. Fratiglioni L, Launer LJ, Andersen K, et al. Incidence of dementia and major subtypes in Europe: a collaborative study of population-based cohorts. Neurologic Diseases in the elderly research group. Neurology. 2000;54(11 Suppl 5):S10–S15.
40. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.