")
Back to Journals » Clinical Epidemiology » Volume 6
Acromegaly according to the Danish National Registry of Patients: how valid are ICD diagnoses and how do patterns of registration affect the accuracy of registry data?
Authors Dal J, Skou N, Nielsen EH, Jørgensen JOL, Pedersen L
Received 8 March 2014
Accepted for publication 18 April 2014
Published 1 September 2014 Volume 2014:6 Pages 295—299
DOI https://doi.org/10.2147/CLEP.S63758
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Jakob Dal,1 Nikolaj Skou,1 Eigil Husted Nielsen,2 Jens Otto Lunde Jørgensen,1 Lars Pedersen3
1Department of Endocrinology, Aarhus University Hospital, Aarhus, 2Department of Endocrinology, Aalborg University Hospital, Aalborg, 3Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark
Background: The incidence of acromegaly is uncertain, since population-based studies are few. In the absence of a specific acromegaly registry, the Danish National Registry of Patients (DNRP) becomes a potential source of data for studying the epidemiology of acromegaly, by linking all hospital discharge diagnoses to the personal identification numbers of individual Danish inhabitants. The validity of the DNRP with respect to acromegaly, however, remains to be tested. The aim of this study was to validate the International Classification of Diseases (ICD) codes for acromegaly (ICD-8: 25300, 25301. ICD-10: E22.0) as used in the DNRP, and to assess the influence of various registration patterns on the accuracy of registry data.
Methods: We identified patients registered with ICD codes for the diagnosis of acromegaly or other pituitary disorders during the period 1991–2009. Data on the institutional origin of each registration and the number of relevant DNRP registrations were recorded, and systematic patient chart reviews were performed to confirm the diagnosis.
Results: In total, 110 cases of acromegaly were confirmed, compared with 275 registered cases, yielding a positive predictive value (PPV) of 40%. When restricting the search to the regional highly specialized department of endocrinology, the PPV increased to 53% with no loss of cases with confirmed acromegaly. With a requirement of at least one, two, or three DNRP registrations, the PPV increased, but with a concurrent loss of confirmed cases.
Conclusion: The DNRP seems to be a useful source for identifying new cases of acromegaly, especially when restricting the search to a relevant regional highly specialized department. The PPV of DNRP data used for this purpose can be increased by including only cases with several registrations. A similar approach may be successfully applied to other rare diseases in which continuity of care is provided by highly specialized departments.
Keywords: acromegaly, Danish National Registry of Patients, validation, epidemiology, incidence
Introduction
Acromegaly is a rare disease, and in the large majority of cases, is caused by a growth hormone-producing pituitary microadenoma or macroadenoma. The resulting excess growth hormone secretion affects multiple organ systems, and biochemical disease control is essential in order to reduce the mortality to the normal level of the background population.1 The severity and complexity of the disease warrant that all patients be offered lifelong follow-up at highly specialized centers.2
Denmark is privileged in having several national medical registries and databases through which routine collection of relevant health-related data is secured for administrative (eg, reimbursement) and quality surveillance purposes. These administrative registries enable us to rapidly assemble a cohort for epidemiologic studies and have the additional advantage of reducing the risk of certain types of bias, eg, recall bias or non-responder-related selection bias in the setting of questionnaire-based surveys.3,4 Finally, the registries have been shown to be characterized by a high completeness of registrations.4,5
As the quality of data collected for administrative purposes may not automatically translate into equally useful and valid data in a subsequent research setting, validation studies become a prerequisite before considering such use of registry data.5 So far, no studies have provided data regarding the quality of hospital discharge diagnoses of acromegaly. We therefore aimed to validate the International Classification of Diseases (ICD) codes for acromegaly as used in the Danish National Registry of Patients (DNRP). We wished to evaluate whether incident cases of acromegaly during a specific period of time could be correctly identified through the DNRP, and to estimate the positive predictive value (PPV) of ICD codes of relevance to a diagnosis of acromegaly, thereby evaluating the overall usefulness of the DNRP as a source for identifying patients with incident acromegaly. In addition, we aimed to examine the accuracy of the first registration with respect to the time of diagnosis and to give estimates of the acromegaly incidence rate as well as of age and sex distribution.
Materials and methods
Study population
The study area covers the Central Region of Denmark with an average of 1.3 million inhabitants (23% of the Danish population) during the period January 1, 1991 to December 31, 2009. The geographic area is formally defined by the Danish region codes 65, 70, and 76; hence including former counties of Ringkøbing, Aarhus, and Viborg, respectively, in combination with hospital code 6006 (Horsens Hospital).
Data sources
Danish National Registry of Patients
Denmark has 5.6 million inhabitants, and the National Health Service provides universal tax-financed health care. All persons living permanently in Denmark are assigned a unique 10-digit personal identification number (the CPR number) of which six digits denote the date of birth and the sex is mirrored by the last digit. The CPR number is used for all purposes requiring exact person identification and remains unchanged throughout life.3 Since 1977, the DNRP has tracked Danish hospital admissions through linkage with the CPR number, recording dates of admission and discharge and up to 20 discharge diagnoses. Diagnoses are coded by hospital physicians using the Danish versions of the ICD: the 8th revision (ICD-8) was used from 1977 to 1993, while the 10th revision has been used since 1994. Since 1995, the DNRP also includes information on outpatient contacts and emergency room visits.6
We identified patients registered with one or more ICD codes of presumed relevance for a diagnosis of acromegaly. In addition to explicit acromegaly codes, we identified patients registered with other codes indicating a pituitary disorder, eg, various pituitary adenoma codes (Table 1). Data on the institutional origin of each registration and the number of relevant DNRP registrations for individual patients were also recorded and analyzed.
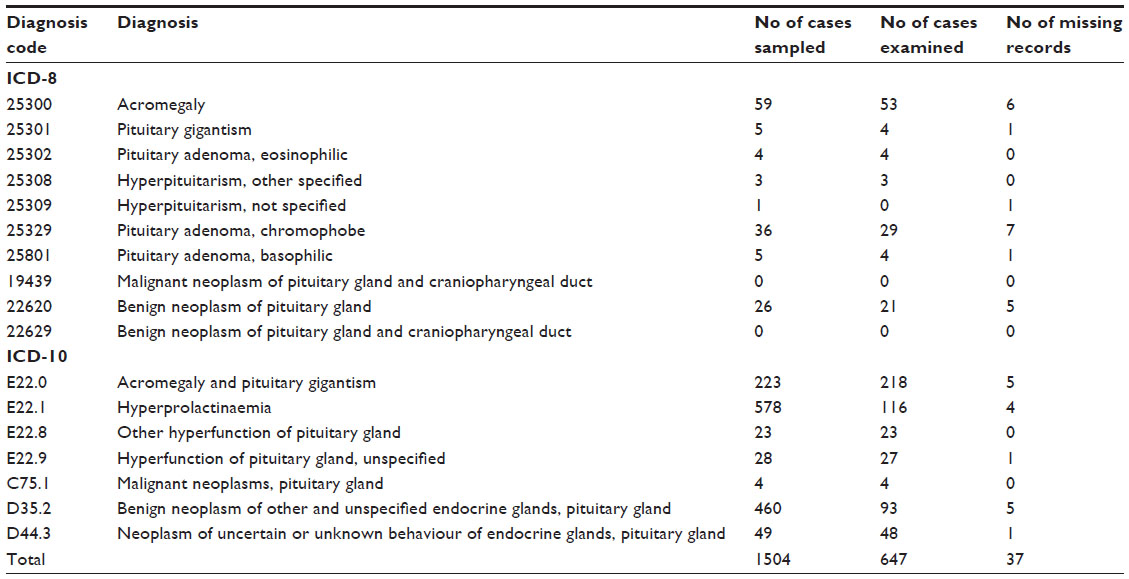 | Table 1 Distribution af all diagnosis codes for acromegaly and other pituitary disorders |
Hospital records and diagnostic information
Hospital records were retrieved and reviewed by a non-blinded physician. All available information in the medical records, including clinical symptoms and findings, written radiology reports, and results from laboratory tests was taken into consideration. A diagnosis of acromegaly was made when laboratory testing (elevated insulin-like growth factor 1 and nadir growth hormone serum concentrations) or imaging (visible pituitary adenoma) and treatment were in agreement with acromegaly. All cases with an uncertain diagnosis based on the available information were discussed with a specialist in endocrinology and acromegaly until a consensus was reached. Computerized journals were reviewed in all accessible cases, supplemented with a review of paper journals in patients within the study population. Electronic discharge records were in general accessible from the mid-1990s.
Statistical analysis
The data validity was expressed as the PPV of individual ICD-8 or ICD-10 discharge codes, and 95% confidence intervals (CIs) were calculated. The PPV was defined as the proportion of patients having confirmed acromegaly when registered with a diagnosis of acromegaly in the DNRP. Normally distributed and non-Gaussian distributed data are presented as the mean and standard deviation or a median with 25% and 75% percentiles, respectively. The incidence rate was calculated assuming a Poisson distribution and given as number of new cases per million per year.
Results
Validity of ICD codes
Our DNRP search identified 287 patients in the study area who had been registered with ICD codes E22.0, 25300 or 25301, for whom records were accessible in 275 (96%) cases (Table 2). Overall, review of hospital records allowed the diagnosis of acromegaly to be confirmed in 149 cases, yielding a PPV of 54.2 (CI 48.3–60.0). In 110 cases, the patients were diagnosed within the Central Region of Denmark and within the chosen time frame with a PPV of 40.0 (95% CI 34.4–45.9). Diagnostic blood sample results for this group were available in 103 of 110 cases. The remaining 39 cases with confirmed acromegaly had either been diagnosed outside the study period (n=20), in another geographic region (n=16), were non-residents (n=2), or not evaluable due to missing data (n=1). The incidence rate of acromegaly within the study population was 4.5 (95% CI 3.6–5.5) per million per year and constant through the study period. The mean age at diagnosis was 49.6 (95% CI 46.8–53.4) years and a sex distribution with 48% female. The median time difference between the first DNRP registration and the diagnostic blood sample was one day (25-, 75-percentile: 1–20) in 103 cases.
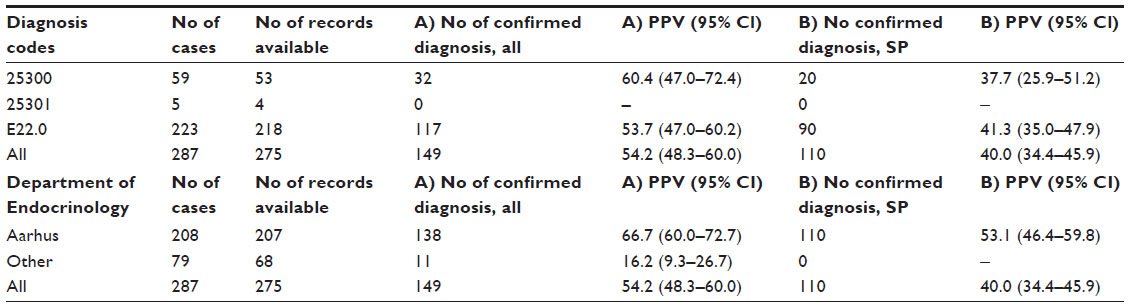 | Table 2 Validity of acromegaly diagnosis and the effect of restriction to selected departments of endocrinology |
Among the group of patients registered with the remaining relevant ICD codes related to various pituitary diseases, all available records were reviewed except those registered only with codes E22.1 “hyperprolactinaemia” or D35.2 “benign neoplasm of other and unspecified endocrine glands, pituitary gland”, among which 20% were randomly selected for review. In all, 372 cases were reviewed and no cases of acromegaly had been misclassified as other diseases. Discharge records were missing in 6% of cases (n=25). One case was recorded as E22.9 “hyperfunction of pituitary gland, unspecified” and only after the end of the study period was diagnosed with and recorded as E22.0 “acromegaly” (Table 1).
When applying the same DNRP search criteria but restricting the search to the highly specialized department of endocrinology at Aarhus University Hospital (code 7003.07x), 208 patients were found. In this search, all 110 confirmed cases of acromegaly within the study population were identified, whereas eleven other cases of confirmed acromegaly, all of whom were diagnosed in another geographic region, were lost. Thus, the PPV increased to 66.7% (95% CI 60.0–72.7) and 53.1% (95% CI 46.4–59.8) for all patients with acromegaly and for the study population, respectively (Table 2), at the cost of a decline in the number of identified cases with confirmed acromegaly from 100% to 92.6% (95% CI 87.3–95.8) in the group of all patients, but no loss of cases in the study population.
Patterns of hospital registration
The pattern of hospital registrations varied between different subgroups of patients identified by the original DNRP search. In three groups, ie, acromegaly cases within the study population, acromegaly outside the study population, and false positive cases, the median total number of per-patient registrations was 22.7, 11.3, and 3.3, respectively. Moreover, when applying a restriction of at least one, two, or three registrations to our DNRP search criteria, the PPV increased with a concurrent loss of cases with confirmed acromegaly (Table 3).
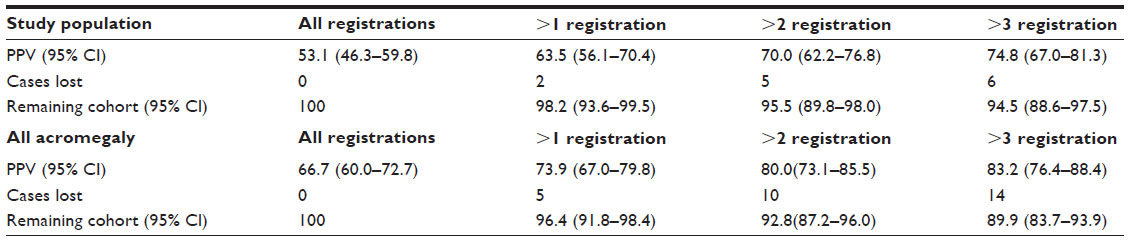 | Table 3 The effect of various registration patterns on the accuracy of the acromegaly diagnosis |
Discussion
We evaluated the data quality of the DNRP in relation to the diagnosis of acromegaly through a population-based cohort study including 1.3 million inhabitants in the Central Region of Denmark during the period 1991–2009. By reviewing 647 discharge records suggesting a diagnosis of acromegaly (n=275) or closely related pituitary diseases (n=372), as shown in Table 1, we were able to estimate the PPV values of the ICD-8 and ICD-10 codes used to identify new cases of acromegaly in a national hospital discharge registry. We identified 149 cases of acromegaly, including 110 cases diagnosed between 1991 and 2009 (ie, during the relevant study period) within the Central Region of Denmark. Since a thorough review of cases with only ICD codes indicating other or non-specific pituitary disease identified no additional cases of acromegaly, and since previous studies indicate a high degree of completeness of the DNRP, we believe that only very few cases of acromegaly, if any, may have been missed by our DNRP search. Moreover, although cases of acromegaly misclassified as non-related pituitary disease cannot be completely ruled out, repeated misclassification seems unlikely when taking into account that patients with acromegaly are offered lifelong follow-up at a highly specialized department. Admittedly, cases of acromegaly with cosecretion of prolactin diagnosed as a prolactinoma, rare cases of a somatotropinoma making its first appearance as a pituitary apoplexy with adenoma destruction, or cases of acromegaly where the diagnosis simply was not considered, cannot be ruled out.7,8 Likewise, some limitations must be taken into account regarding the diagnostic verification process that we applied to suspected cases of acromegaly. Firstly, the reviewer could not be blinded because all records were named according to the ICD codes. Secondly, in some cases the ICD code could not be confirmed during the manual review process. Instead, the electronic journal was reviewed and used to confirm or reject the diagnosis of acromegaly. However, in most cases, the relevant ICD code was identified and the particular hospital file was examined. When comparing the characteristics of our cohort of acromegaly with respect to the mean age at diagnosis (49.6 years), the sex distribution (48% female), and the incidence rate (4.5/million/year), our cohort seems comparable with other cohorts in the literature.2 However, a more precise estimate of the true incidence rate should be calculated on the basis of a larger population, ie, a national cohort.
We found the overall PPV for acromegaly in the DNRP to be only 54%, and the PPV further decreased to 40% for truly positive (confirmed) cases within the study population as defined by geography and time period criteria. To improve the PPV, we refined the search criteria by restriction to a selected highly specialized department of endocrinology. Without losing any acromegaly cases from the study population, the PPV of ICD codes for acromegaly in the DNRP increased to 53% in the study population. Finally, when analyzing and further including the number of registrations into the search strategy, we found that patients with acromegaly both inside and outside the study population had higher numbers of registrations than patients in the false positive group (Table 3). When applying a restriction of at least one, two, or three registrations to the search, the PPV gradually increased from 53% to 75% in the study population, with a less pronounced decline in the percentage of identified cases with confirmed acromegaly from 100% to 95%. Cases of acromegaly with only a few registrations were characterized by recent diagnosis, older age, and the coexistence of other medical conditions. The findings are not surprising, given that acromegaly is a lifelong condition requiring continuity of care at a highly specialized endocrine department. Our study indicates that no or only very few patients with acromegaly fail to be registered by the regional highly specialized medical department of endocrinology, and that these patients typically are registered several times due to repeated hospital contacts. According to our study, the effect of applying both aspects of this knowledge to a search for new cases of acromegaly in a well defined geographic area and for a well defined time period will be a relative increase in PPV of the search result by almost 90% (from 40% to 75%) while preserving the identification of most cases of confirmed acromegaly.
Conclusion
In this study covering a recent 19-year period and including approximately one fourth of the Danish population, the DNRP appears to be a useful tool for identifying new cases of acromegaly, especially when restricting the search criteria to the regional highly specialized medical department of endocrinology. The initial PPV was well below 50%, but could be markedly increased by adding several registrations as a supplementary search criterion. We speculate that this approach in searching the DNRP may be successfully applied to other rare diseases in which continuity of care is provided by highly specialized departments.
Disclosure
The authors report no conflicts of interest in this work.
References
Holdaway IM, Bolland MJ, Gamble GD. A meta-analysis of the effect of lowering serum levels of GH and IGF-I on mortality in acromegaly. Eur J Endocrinol. 2008;159(2):89–95. | |
Ben-Shlomo A, Melmed S. Acromegaly. Endocrinol Metab Clin North Am. 2008;37(1):101–122. | |
Frank L. When an entire country is a cohort. Science. 2000;287(5462):2398–2399. | |
Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7):30–33. | |
Sorensen HT, Sabroe S, Olsen J. A framework for evaluation of secondary data sources for epidemiological research. Int J Epidemiol. 1996;25(2):435–442. | |
Sorensen HT, Christensen T, Schlosser HK, Pedersen L, editors. Use of Medical Databases in Clinical Epidemiology. 2nd ed. Aarhus, Denmark: Sun-Tryk, Aarhus University; 2009. | |
Dal J, Steffensen C, Hansen TK, Jørgensen JOL. [Acromegaly masked by symptomatic hyperprolactinemia]. Ugeskr Laeger. 2014;176(1):60–61. Danish. | |
Fraser L-A, Lee D, Cooper P, Van Uum S. Remission of acromegaly after pituitary apoplexy: case report and review of literature. Endocr Pract. 2009;15(7):725–731. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.