")
Back to Journals » Psychology Research and Behavior Management » Volume 11
Accurate empathy of romantic partners increases pain ratings but promotes recovery
Authors Sun B , Zhou L, Xiao W , Zhao X, Zhang W, Li W
Received 16 June 2018
Accepted for publication 17 August 2018
Published 27 September 2018 Volume 2018:11 Pages 403—410
DOI https://doi.org/10.2147/PRBM.S177457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Binghai Sun,1 Lingyan Zhou,1 Weilong Xiao,1 Xiaoqian Zhao,1 Wenhai Zhang,1,2 Weijian Li1
1School of Teacher Education, Zhejiang Normal University, Jinhua 321004, China; 2Mental Health Center, Yancheng Institute of Technology, Yancheng 224051, China
Background: Perceived empathy is a commonly used strategy to cope with pain and is crucial for maintaining intimacy in dyadic relationships.
Materials and methods: This study used the cold pressor test to investigate how perceived empathy and relationship type interact with the subjective perception of pain and objective measures of recovery time, using heart rate as an index. One hundred and ninety participants were recruited, including 49 friend dyads and 46 romantic partner dyads. Perceived empathy was manipulated by adopting three levels as the experimental conditions: high, accurate, and low.
Results: In the subjective perception stage, the results showed a significant interaction of relationship type and empathy with pain reporting, indicating that romantic partners reported more pain than friends under the accurate empathy condition. There were no differences between the two groups in the high and low perceived empathy conditions. In the self-recovery stage, the results showed that romantic partners had less pain tolerance than friends in all three perceived empathy conditions. On the other hand, romantic partners recovered faster than friends under the accurate empathy condition, but not under the high and low perceived empathy conditions.
Conclusion: These results suggest that perceived accurate empathy is necessary for romantic relationships when coping with pain. The findings deepen our understanding of the mechanism of perceived empathy, and the ways in which it modulates psychological and physiological responses in a social context.
Keywords: accurate empathy, recovery time, romantic relationship, cold pressor test
Introduction
Empathy is traditionally thought to be a particular ability of humans to feel, understand, and share the emotional state of others,1 and is also related to the social modulation of pain.2 Perceived empathy refers to a person’s perception of the extent to which an observer feels they can understand and share their feelings.3 A wealth of evidence suggests that perceiving empathy in others plays an important role in social interaction, ameliorates stress, and is associated with an individual’s health and well-being.4 However, little is known about how perceived empathy influences pain in different social relationships.5
A handful of studies have examined the causal relation between perceived empathy in painful situations and different relationship types (such as romantic attachments or friends) during dyadic interactions.3,5,6 These studies have produced conflicting results. For example, some studies using the cold pressor test have found that participants rated more pain in the alone condition than in the presence of a same-sex friend.7 Other studies demonstrated that there was no difference when individuals were witnessed by high-empathic or low-empathic observers.3 Another study showed that believing one’s romantic partner feels high empathy for one’s pain may lead individuals to undergo a higher intensity of pain.6 However, these studies focus on the two extreme levels (high vs low) of perceived empathy and ignore empathy accuracy; if participants did not perceive others’ empathy accurately, this might explain the inconsistent results. Empathic accuracy is defined as the extent to which an individual accurately infers the thoughts and feelings of another person.8 Perceiving empathy accurately is needed during painful situations and is important for relationships to function effectively.9
In classical empathic researches, the cold pressor task has been widely adapted to inducing pain. The cold pressor task is considered a safe and effective method of pain induction and has also been used in earlier social pain studies.5,10,11 However, the self-reporting of pain in the aforementioned studies is often criticized because of its subjectivity and unreliability.9 These studies using the cold pressor task measure psychological patterns only when participants experience pain in the first stage of the task (subjective perception). To the best of our knowledge, no experimental study has examined the effects of perceived empathy on pain recovery in the second stage of the pain task (self-recovery). Physiological measures have been shown to be accurate and reliable when the influence of other social variables on pain is considered.6 Additionally, some research has shown that vital signs can predict pain severity, although this has been contradicted by numerous other studies.12 Specifically, however, heart rate measures pain recovery time,13,14 and such measures were not included in previous studies of perceived empathy. Consequently, this study used heart rate to measure pain recovery time in the second stage of the cold pressor task, but not pain intensity in the first stage.
The present research used the cold pressor task to explore how perceived empathy in two types of dyadic relationship (romantic attachments vs friends) interacts with pain reporting in the subjective perception of the task, and with the tolerance and recovery times in the recovery stage of cold pressor stimulation. Research has shown that the perceived empathy of a romantic partner can increase pain ratings, possibly because romantic partners are more likely to respond emotionally to each other, are more likely to express their feelings, and are more strongly attached than friends.6,15 Studies have also shown that expressing pain can promote recovery.16 Consequently, a review of the literature resulted in the following hypotheses: firstly, perceived accurate empathy would increase pain ratings in romantic partners vs friends compared to high and low perceived empathy levels; secondly, perceived empathy in romantic partners would reduce pain tolerance compared to friends; and thirdly, perceived accurate empathy would reduce recovery time in romantic partners vs friends compared to high and low perceived empathy levels.
Materials and methods
Participants
One hundred and ninety college students (84 men, 106 women; M=21.25 years, SD=2.08 years) were recruited from Zhejiang Normal University by advertising the study. Among the participants, there were 49 friend dyads (38 men, 60 women; M=20.94 years, SD=2.02 years) and 46 romantic partner dyads (46 men, 46 women; M=21.58 years, SD=2.10 years). None of the romantics were in same-sex relationships. Relationship durations ranged from 10 days to 72 months (M=16.70 months, SD=14.12 for the romantics; M=16.04 months, SD=12.82 for the friends). After providing written informed consent, all participants reported that they were healthy, were not suffering from chronic or acute pain; and had no history of blood disorders or other disorders relevant to this study. The study was approved by the Ethics Committee of the Department of Psychology at Zhejiang Normal University. It is worth noting that participants were selected based on their attachment style. Only persons with secure attachments were selected, as explained below.
The cold pressor task
Pain was induced by the cold pressor task, which is considered a safe and effective method to induce pain10 and has been used in previous dyadic pain studies.17 Participants came into the laboratory voluntarily. The pain-receiving participant engaged in the cold pressor task while the pain-observing participant observed his or her partner’s pain in the same room. The pain-receiving participant was asked to sit with his or her left hand next to the cold pressor device bin. The pain-observing participant was seated in front of the pain-receiving participant about a meter apart and facing each other. A music stand was placed in front of the participants so that they could rate their pain on the rating scales without seeing each other’s responses but still seeing their partner’s face. Both members of the romantics or friends were tested so that each participant experienced being the pain-receiver and the pain-observer in different trials. The sequence of the experimental roles was counterbalanced. The experiment lasted about 50 minutes.
In this experiment, the cold pressor task proceeded as follows. Pain-receiving participants first submerged their left hand in a washbasin at 32°C for 2 minutes to standardize their hand temperature.18 At the same time, participants were given standard instructions and were required to keep silent with no communication via language, gesturing, or signaling during the testing process. The participants were given the opportunity to ask any questions if they had any doubts about the process. The pain-receiving participant was then asked to articulate the tasks they need to do during the cold pressor task in their own words. The pain-receiving participant then submerged the left hand into the cold-water bath, which was kept at a constant temperature of 5°C, and was told to keep the hand in the cold water until the hand became too uncomfortable. The test adopted a period of 3 minutes as the recommended safety measure when using the cold pressor task.10 The pain-receiving participant was also instructed to raise his or her other hand when they began to feel pain in the hand still immersed in the water, and to rate his or her pain by marking a number with their other hand on an 11-point rating scale, where 0=“no pain” and 10=“pain as bad as it could be”. The pain-observing participant could not see the rating. At that point, the perceived empathy manipulation was implemented, as described below. The pain-receiving participant was asked to rate the pain again when they pulled their hand out of the cold water.
Procedures
The procedure for each cold pressor trial is shown in a schematic form in Figure 1. A between-subjects design was used in this study. The independent variables were two between-groups factors: perceived empathy levels (accurate perceived empathy vs low perceived empathy vs high perceived empathy, with the latter two conditions comprising inaccurate perceived empathy) and the type of relationship between the pain-receiver and the pain-observer (friend vs romantic partner). The dependent variables were the various pain responses and physiological indices from the cold pressor task, as described below.
 | Figure 1 A schematic representation of the procedure for each cold pressor trial. |
Pre-experimental procedures
At the start of the study, the participants provided written informed consent. The participants were then randomly assigned into three perceived empathy groups. The participants did not know which group they belonged to until the study finished. Before starting the cold pressor task, each person was asked to provide some demographic characteristics and to complete the Pain Catastrophizing Scale (PCS) questionnaire and the Experiences in Close Relationships (Revised) questionnaire (ECR-R). Heart rate and rate response interval were recorded continuously by using Biopac MP150 (BIOPAC, Goleta, CA, USA). Participants were asked to paste ECG electrodes below the clavicle and left rib before the test.
Perceived empathy manipulation
To test the effects of perceived empathy in this experiment, we adopted the following procedures to produce the three conditions of accurate perceived empathy, low perceived empathy, and high perceived empathy. The pain-receiving participant provided his or her own pain rating (not visible to the pain-observing partner), while at the same time the pain-observing participant was required to rate the amount of pain he or she felt the pain-receiver was feeling on an 11-point scale ranging from 0 (“no pain”) to 10 (“pain as bad as it could be”). Subsequently, the researcher checked the pain-observer’s immediate rating (out of sight of the pain-receiver), moved away from the pain-observer, and circled what participants believed to be the equivalent number on an identical pain scale in front of the pain-receiver.6 However, unbeknown to all participants, the pain-receivers were shown pain ratings that were manipulated by the researcher, and not the real pain ratings as provided by the observers. In the accurate perceived empathy condition, the pain rating was the same as the rating circled by the pain-receiver; in the low perceived empathy condition, the pain rating was 1 SD smaller than the rating circled by the pain-receiver; and in the high perceived empathy condition, the pain rating was 1 SD greater than the rating circled by the pain-receiver.19 The sequence of high, low, and accurate conditions was counterbalanced.
During and after the empathy manipulations, the pain-receiver kept their hand in the cold water until it became too uncomfortable to endure (or until 3 minutes had elapsed). When he or she removed their hand from the cold water, they were asked to rate their pain again by circling a number on an 11-point scale, where 0 = “no pain” and 10 = “maximum pain.”
Post-experimental procedures
After the task, participants were provided with a questionnaire designed to investigate their experience of being observed by their partners. The questions were as follows: 1) “How much pain did your partner think you were feeling during your experience of the cold pressor task?”; 2) “Irrespective of the ratings that your partner provided, how much empathy did you feel during the cold pressor task?”; and 3) “How much was your pain affected by your partner’s estimate of the amount of pain you were feeling?” Participants were required to rate their responses on an 11-point scale (0 = “not at all” to 10 = “maximum extent”). Participants’ ratings in these post-experiment questions were used to check whether the empathy manipulation had been successful. All participants completed the post-experiment empathy ratings and were then fully informed about the empathy manipulation.
Measures
The attachment style
The ECR-R is a 36-item questionnaire that measures attachment style and is widely used to assess relationships.20 The ECR-R includes two dimensions, attachment anxiety and attachment avoidance, which correspond to the existing model of attachment theory.21 The rating for each item is on a five-point Likert scale, ranging from 1 (“completely agree”) to 5 (“completely disagree”). Li and Kato (2006) designed a Chinese version of the ECR-R scale,22 and showed that the two subscales have good internal reliability. In this study, Cronbach’s alpha for attachment anxiety was 0.82, and Cronbach’s alpha for attachment avoidance was 0.77.
PCS
The PCS was developed to assess the chronic pain of clinical and nonclinical populations.23 The PCS consists of 13 items describing diverse feelings and thoughts concerning pain experience. Participants rate the frequency of their feelings and thoughts on a scale from 0 (“not a bit”) to 4 (“all the time”). The scale has been widely used in Europe and has good reliability and validity. The scale was introduced into China in 2008.24 The internal consistency was 0.93 in this sample.
Pain reporting and tolerance
Participants assessed their pain on a numerical rating scale (NRS) ranging from 0 (“no pain”) to 10 (“pain as bad as it could be”). The NRS is traditionally used as a measurement of pain. When the measure was tested across different temperature values, the internal consistency of Cronbach’s alpha was found to be 0.88.25 Participants were asked to rate their pain on two occasions: the first was when they began to feel pain (before the perceived empathy manipulation), and the second was when they could not bear the pain and removed their hand from the water. The time when participants marked they were feeling pain and the time when they removed their hand (pain tolerance) were noted to the nearest second.
Recovery time
We measured the time that it took for each participant’s indices to return to his or her own pre-test resting levels, according to Fredrickson’s (1998) measurements for the duration of cardiovascular reactivity.26 To do this, for each participant, and for each measure of physiological activity, we first calculated a baseline CI to represent pre-test baseline levels, defined by that participant’s own 60-second pre-test mean ±1 SD. The recovery time was defined as the time elapsed after the offset of the cold water until psychophysiological levels returned to the participant’s baseline CI and remained within this CI for at least five out of six consecutive seconds.26
Data analysis
For all participants, we calculated the PCS and ECR-R scores, mean pain report scores, mean times for pain tolerance, and recovery time with SDs during the cold pressor task. To explore the effects of perceived empathy and relationship type on pain reporting, mean pain report scores were subjected to one-way ANOVAs with perceived empathy and relationship type as independent factors. The effects of relationship type and perceived empathy on pain tolerance and recovery time in the cold pressor test were also analyzed by one-way ANOVA. We controlled for certain factors that have been proved to be considerable moderators of the relationship between social support variables and pain.2 Firstly, in all analyses, the effects of gender and sequence were regarded as covariates. Secondly, on the basis of the communal coping model of pain catastrophizing,27 individuals adopted interpersonal coping strategies to cope with pain to some extent, especially when others were present.27 Individual differences in pain catastrophizing were therefore considered as covariates. Thirdly, previous studies have shown that individual differences in attachment style are crucial for regulating the relationship between the social context of pain and the perception of pain.3 We were interested in a representative sample of those people who exhibit a secure attachment style; hence, we selected participants with experiences of secure attachments as measured by the ECR-R. Finally, to ensure our manipulation worked, we used the same method as described above to analyze the results of the post-test empathy questions. The factors of age, relationship duration, and relationship satisfaction had no statistical significance for our dependent measures and were not included in the latter analyses.
Results
Demographic data
The demographic information of the sample is presented in Table 1. No significant group differences were found for age [F (1,188)=0.36, P=0.547]; catastrophizing [F (1,188)=0.02, P=0.887]; relationship satisfaction [F (1,188)=3.52, P=0.062]; and relationship duration [F (1,188)=0.12, P=0.733].
 | Table 1 Descriptive data of demographic variables |
Post-experiment questions
The post-experiment ratings were used to verify whether the perceived empathy manipulation was successful. In response to the first question, the results suggest that all participants provided accurate scores for their partner’s pain ratings (M=7.12, SE=0.41).
Similarly, when asked to rate how much support they felt, irrespective of the pain ratings their partner actually gave, the participants felt less support in the low perceived empathy condition (M=5.58, SE=2.17) and high perceived empathy condition (M=5.74, SE=2.23), whereas the participants felt more support in the accurate perceived empathy condition [M=7.35, SE=1.66; F (2,184)=8.77, P<0.01; F (2,184)=6.73, P<0.01, respectively]. There were no significant differences among relationship type [F (1,184)=0.00, P>0.05], or in the interaction between relationship type and perceived empathy condition [F (2,184)=0.25, P>0.05]. These results indicate that the manipulation of perceived empathy had good validity.
Finally, there was no significant difference [F(2.184)=0.49, P>0.05] between the high perceived empathy condition (M=5.06, SE=2.78), accurate perceived empathy condition (M=4.90, SE=3.11), and low perceived empathy condition (M=4.85, SE=2.73) in how much participants felt that their pain was affected by their partner’s pain ratings. Neither were there significant differences among dyadic style groups [F(1,184)=3.43, P>0.05], or in the interaction between relationship type and perceived empathy condition [F (2,184)=1.800, P>0.05].
Effects of perceived empathy and relationship type on pain reports
To examine the effects of perceived empathy and group differences on pain reporting, we conducted an ANOVA with three levels of perceived empathy (accurate perceived empathy vs high perceived empathy vs low perceived empathy) and two relationship types (friend vs romantic partner) as between-group factors. We found a main effect of perceived empathy [F (2,184)=6.59, P<0.05, h2=0.41] and a significant interaction between perceived empathy and relationship type [F (2,184)=3.95, P<0.05, h2=0.34], as shown in Figure 2. Post hoc analysis showed that romantic partners circled higher pain ratings in the accurate empathy condition than in the low and high perceived empathy conditions (P<0.001). However, there were no significant effects for the friend relationship (P>0.05), and no other significant effects were found (all P>0.05).
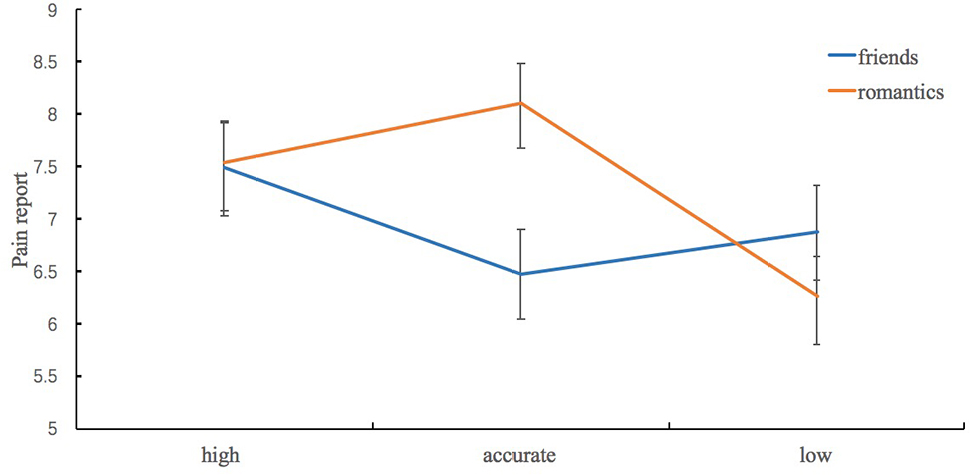 | Figure 2 Predictive means and standard error for pain report ratings by relationship type and perceived empathy condition. |
Effects of perceived empathy and relationship type on pain tolerance
Although there was no significant interaction between perceived empathy and relationship type with regard to pain tolerance [F (2,184)=0.04, P>0.05], we observed a significant effect of relationship type [F (1,184)=6.89, P<0.01, h2=0.66], as shown in Figure 3. Post hoc analyses indicated that friends endured more time than romantic partners and were more willing or more able to complete the task than romantic partners. No other significant effects were found (all P>0.05).
 | Figure 3 Predictive means and standard error for pain tolerance by relationship type and perceived empathy condition. |
Effects of perceived empathy and relationship type on recovery time
Consistent with our hypotheses, there was a main effect of perceived empathy on recovery time [F (2,184)=85.10, P<0.01, h2=0.48], as shown in Figure 4. Participants recovered more quickly in the accurate empathy condition than in the high and low perceived empathy conditions. Moreover, there was a significant interaction between perceived empathy and relationship type [F (2, 184)=5.61, P<0.05, h2=0.37], with post hoc tests showing that romantic partners needed less recovery time than friends in the accurate perceived empathy condition. However, there were no significant effects in the high and low perceived empathy conditions, and no other significant effects were found (all P>0.05).
 | Figure 4 Predictive means and standard error for recovery time by relationship type and perceived empathy condition. |
Discussion
The purpose of this study was to use the cold pressor test to demonstrate how relationship types (romantics vs friends) modulate psychological and physiological measures of pain under high, accurate, and low perceived empathy conditions. In the first stage of the pain task, the results were consistent with the hypothesis that perceived accurate empathy from a romantic partner leads to a significant increase in self-report pain scores compared to friends. In the second stage of the pain task, the results showed that romantic partners needed less recovery time than friends under the accurate empathy condition compared to both high and low perceived empathy conditions. At the same time, romantic partners had a lower pain tolerance than friends, regardless of high, accurate, or low perceived empathy conditions. Taken together, these results suggest that perceived accurate empathy plays a crucial role in the influence of romantic intimacy on an individual’s subjective perception of pain and their physiological recovery.
In the first stage, the results showed that romantic partners reported more pain than friends only in the accurate empathy condition. One possible reason is that believing one’s partner has empathy for one’s pain may function as an interpersonal signal that causes participants to focus their attention on the pain and increase pain ratings.6 The other possibility might be because facing one’s romantic partner increases activity in several reward-processing regions of the brain, and the activation of a neural reward system can reduce the sensation of pain.28 However, the two possibilities cannot explain why perceived accurate empathy from a romantic partner is associated with higher pain intensity whereas friends report a lower pain intensity. Another possibility is that romantic partners are more intimate and more willing to express their feelings than friends, whereas friends may not want to disclose pain during the task.5 Thus, the empathetic expression of pain from a romantic partner rather than a friend might increase the pain intensity rating. Similarly, Chambers et al observed that, in mother-daughter dyads, the girls’ intensity ratings for cold pressor pain increased when their mothers interacted with them in an empathetic way.28 Furthermore, because romantic partners express more pain than friends,6,15 they also had a lower pain tolerance than friends in the second stage of the task. Nevertheless, the results suggest that only under the accurate empathy condition does the expression of pain from a romantic partner seem to promote the subjective perception of pain.
Indeed, previous research has revealed that individual differences in attachment style are critical in moderating the relationship between the social context of pain and pain perception.3 In order to exclude the confounding of attachment style, we selected participants with experiences of secure attachment according to the ECR-R, and no significant differences between the two groups were found under high and low perceived empathy conditions. This finding contradicts previous studies.6 The inconsistency might be because these previous researches did not control for attachment style. In our study, high and low perceived empathy are construed as inaccurate perceived empathy for participants. Thus, the inaccurate perceived empathy may cancel the priority attributed to the precise expression of pain in romantics and friends, with the result that there is not the same effect as in perceived accurate empathy.
In the second stage, perceived accurate empathy in romantic partners was related to the shorter recovery time compared to friends. Previous research has demonstrated that the expression of pain aids the cognitive and physiological processing of pain and benefits pain recovery.16 Additionally, pain is communicated through nonverbal signs (such as facial expressions).29 When romantic partners express pain and perceive accurate empathy from their partners, the two processes arouse bottom-up sensory input (such as eye contact) and top-down expectations (for example, given past experiences that romantic partners help them overcome difficulties), both of which are essential for pain recovery.30 Finally, as romantic partners express more pain than friends, the parasympathetic nervous system of romantic partners acts as a stronger trigger, which leads to the romantic partner’s heart rate slowing down faster following pain compared to friends. Thus, romantic partners need less recovery time than friends. Taken together, these results suggest that perceived accurate empathy aids romantic dyads through the inherent characteristics (such as facial expressions) of the two physiological stages of pain and recovery.
Conclusion
To summarize, in the subjective perception of pain during the first stage of the cold pressor task, romantic partners reported higher pain intensities than friends when participants perceived accurate empathy. In the self-recovery stage of the cold pressor task, tolerance time for romantic partners was shorter than friends in the high, accurate, and low perceived empathy conditions. The recovery time was accelerated for romantic partners only under the accurate empathy condition. These results suggest that romantic intimacy plays a role only in perceived accurate empathy situations, where it modulates the subjective perception of pain and the subsequent recovery stage. These results could have clinical implications for puerperae who might benefit from support from romantic partners or friends and might have preferences concerning who is best suited to help, and how support should be provided.
Acknowledgment
This study was supported by the Social Sciences Projects in Zhejiang Universities of China (2018GH018).
Disclosure
The authors report no conflicts of interest in this work.
References
Chen J. Empathy for Distress in Humans and Rodents. Neurosci Bull. 2018;34(1):216–236. | ||
Krahé C, Springer A, Weinman JA, Fotopoulou A. The social modulation of pain: others as predictive signals of salience - a systematic review. Front Hum Neurosci. 2013;7(30):386. | ||
Sambo CF, Howard M, Kopelman M, Williams S, Fotopoulou A. Knowing you care: effects of perceived empathy and attachment style on pain perception. Pain. 2010;151(3):687–693. | ||
Reblin M, Uchino BN. Social and emotional support and its implication for health. Curr Opin Psychiatry. 2008;21(2):201–205. | ||
Edwards R, Eccleston C, Keogh E. Observer influences on pain: an experimental series examining same-sex and opposite-sex friends, strangers, and romantic partners. Pain. 2017;158(5):846–855. | ||
Hurter S, Paloyelis Y, Williams AC, Fotopoulou A. Partners’ empathy increases pain ratings: effects of perceived empathy and attachment style on pain report and display. J Pain. 2014;15(9):934–944. | ||
Mcclelland LE, Mccubbin JA. Social influence and pain response in women and men. J Behav Med. 2008;31(5):413–420. | ||
Hodges SD, Kiel KJ, Kramer AD, Veach D, Villanueva BR. Giving birth to empathy: the effects of similar experience on empathic accuracy, empathic concern, and perceived empathy. Pers Soc Psychol Bull. 2010;36(3):398–409. | ||
Cramer D, Jowett S, Empathy P. Perceived empathy, accurate empathy and relationship satisfaction in heterosexual couples. J Soc Pers Relat. 2010;27(3):327–349. | ||
von Baeyer CL, Piira T, Chambers CT, Trapanotto M, Zeltzer LK. Guidelines for the cold pressor task as an experimental pain stimulus for use with children. J Pain. 2005;6(4):218–227. | ||
van Damme S, Crombez G, van Nieuwenborgh-de Wever K, Goubert L. Is distraction less effective when pain is threatening? An experimental investigation with the cold pressor task. Eur J Pain. 2008;12(1):60–67. | ||
Bendall JC, Simpson PM, Middleton PM. Prehospital vital signs can predict pain severity: analysis using ordinal logistic regression. Eur J Emerg Med. 2014;18(18):334–339. | ||
Morshedi-Meibodi A, Larson MG, Levy D, O’Donnell CJ, Vasan RS. Heart rate recovery after treadmill exercise testing and risk of cardiovascular disease events (The Framingham Heart Study. Am J Cardiol. 2002;90(8):848–852. | ||
Shetler K, Marcus R, Froelicher VF, et al. Heart rate recovery: validation and methodologic issues. J Am Coll Cardiol. 2001;38(7):1980–1987. | ||
Markey C, Markey P. Romantic partners, weight status, and weight concerns: an examination using the actor-partner interdependence model. J Health Psychol. 2011;16(2):217–225. | ||
Rattaz C, Dubois A, Michelon C, Viellard M, Poinso F, Baghdadli A. How do children with autism spectrum disorders express pain? A comparison with developmentally delayed and typically developing children. Pain. 2013;154(10):2007–2013. | ||
Vigil JM, Coulombe P. Biological sex and social setting affects pain intensity and observational coding of other people’s pain behaviors. Pain. 2011;152(9):2125–2130. | ||
Vervoort T, Caes L, Trost Z, Sullivan M, Vangronsveld K, Goubert L. Social modulation of facial pain display in high-catastrophizing children: an observational study in schoolchildren and their parents. Pain. 2011;152(7):1591–1599. | ||
Clark SM, Cano A, Goubert L, Vlaeyen JW, Wurm LH, Corley AM. Pain anxiety and its association with pain congruence trajectories during the cold pressor task. J Pain. 2017;18(4):396–404. | ||
Porter LS, Davis D, Keefe FJ. Attachment and pain: recent findings and future directions. Pain. 2007;128(3):195–198. | ||
Bartholomew K, Horowitz LM. Attachment styles among young adults: a test of a four-category model. J Pers Soc Psychol. 1991;61(2):226–244. | ||
Li T, Kato K. Measuring Adult Attachment: Chinese Adaptation of the ECR Scale. Acta Psychologica Sinica. 2006;38(3):399–406. | ||
Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. | ||
Yap JC, Lau J, Chen PP, et al. Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2008;9(2):186–195. | ||
Herr KA, Spratt K, Mobily PR, Richardson G. Pain intensity assessment in older adults: use of experimental pain to compare psychometric properties and usability of selected pain scales with younger adults. Clin J Pain. 2004;20(4):207–219. | ||
Fredrickson BL, Levenson RW. Positive emotions speed recovery from the cardiovascular sequelae of negative emotions. Cogn Emot. 1998;12(2):191–220. | ||
Sullivan MJ, Thorn B, Haythornthwaite JA, et al. Theoretical perspectives on the relation between catastrophizing and pain. Clin J Pain. 2001;17(1):52–64. | ||
Chambers CT, Craig KD, Bennett SM. The impact of maternal behavior on children’s pain experiences: an experimental analysis. J Pediatr Psychol. 2002;27(3):293–301. | ||
Walsh J, Eccleston C, Keogh E. Pain communication through body posture: the development and validation of a stimulus set. Pain. 2014;155(11):2282–2290. | ||
Decety J, Fotopoulou A. Why empathy has a beneficial impact on others in medicine: unifying theories. Front Behav Neurosci. 2014;8(37):457. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.