")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Acceptance Of HIV Testing And Associated Factors Among Pregnant Women Attending Antenatal Care In Gunino Health Center, Southern Ethiopia 2019: An Institutional Based Cross-Sectional Study
Authors Atnafu Gebeyehu N, Yeshambel Wassie A , Gelaw KA
Received 5 August 2019
Accepted for publication 24 October 2019
Published 2 December 2019 Volume 2019:11 Pages 333—341
DOI https://doi.org/10.2147/HIV.S226077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Natnael Atnafu Gebeyehu, Addisu Yeshambel Wassie, Kelemu Abebe Gelaw
Department of Midwifery, College of Health Science and Medicine,Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Natnael Atnafu Gebeyehu
Department of Midwifery, College of Health Science and Medicine,Wolaita Sodo University, Wolaita Sodo, Ethiopia
Tel +251947326676
Email [email protected]
Background: Acceptance of human immune virus testing is an entry point of intervention to end mother to child transmission of the virus among pregnant women.
Methods: Institutional based cross-sectional study design with a sample size of 340 was conducted from May 20 to June 15, 2019. The data were collected by using systematic random sampling technique of interviewer administered questionnaire. Those candidate variables at bivariate analysis with a p-value <0.25 were moved to the multivariate analysis was considered as cutoff point.
Result: Among the total of 340 pregnant women who participated with a response rate of 96%, 234 (68.8%) accepted testing. The odds of acceptance of human immune virus testing was higher among respondents who had awareness about mother to child transmission (AOR=2.602, 95%; CI:1.408–4.809) than their counterparts. It was also higher among respondents who had perceived the benefit of testing (AOR=1.838, 95%; CI:1.089–3.104) than those who did not perceive the benefit of testing. Participants who were knowledgeable about the prevention of mother to child transmission were more likely to accept testing (AOR=1.715, 95%; CI:1.030–2.855) than their counterparts. Besides, the odds of acceptance of testing among pregnant women who attended two and above antenatal appointments were higher (AOR= 2.485, 95%; CI:1.462–4.224) than participants who attended only one appointment. Participants who had no formal education (AOR=0.393, 95%; CI:0.160–0.967) and had a primary level of education (AOR=0.357,95%; CI:0.152–0.842) were less likely to accept human immune virus testing than women who had a diploma and above level of educational status.
Conclusion: Acceptance of human immune virus testing among pregnant women attending antenatal care clinics was relatively low. Antenatal caregivers should place emphasis on reducing barriers to testing, like lack of awareness, knowledge, and educational background.
Keywords: pregnant women, acceptance of HIV testing, antenatal care
Introduction
Worldwide, there are 17.8 million people living with human immune virus were women’s above 15 years old.1 According to UNAIDS 2017 fact sheet, Ethiopia was one of the countries most affected by human immune virus infection with a total of 710,000 people living with the virus. Among this total population living with human immune virus, only 400,000 were women above the age of 15.2 The chance of being a victim of human immune virus infection was eight times higher among young women aged 15 to 24 years compared to their male counterparts.3
Mother to child transmission is one of the main sources for pediatric human immune virus infection. In the absence of any protective measures, the risk of a baby acquiring the virus from an infected mother ranges from 15 to 45%, which happens during pregnancy, childbirth or breastfeeding.4
Human immune virus testing at the time of pregnancy gives an insight into prevention of mother to child transmission, treatment, and care and support services when women are diagnosed with HIV.5 However, an estimated 30% of people living with human immune virus had no awareness of their human immune virus status at the end of 2016.6 In Ethiopia, universal human immune virus screening of pregnant women started in 2007,7 and nowadays, it is targeted to end mother to child transmission of human immune virus by 2020 and attain the 90-90-90 treatment aims endorsed in the 2016 United Nations political declaration on ending AIDS.8,9 Screening of human immune virus among pregnant women was provided as part of antenatal care services, and in Ethiopia, only 19% of antenatal care attendants received counseling of human immune testing and test results during their visits.10
To avert HIV/AIDS epidemic, prevention of mother to child transmission is a commonly used intervention designed to minimize the risk of a baby born with human immune virus infection. Among these interventions, human immune virus testing and counseling is a critical component and entry point for all pregnant mothers to learn and understand the implications of their status and provide an opportunity to reduce morbidity, mortality, and human immune virus transmission.11
In Ethiopia, females make up more than half (62%) of people living with human immune virus and are in reproductive age group with a prevalence of 1.2%. However, human immune virus epidemic is heterogeneous in terms of sex, geographic areas, and population groups. For example, widowed urban women 10.9%, divorced urban women 3.5%, female sexual workers 23%, distant drivers 4.9%, prisoners 4.2%, and mobile and resident workers in hotspot areas 1.5%.12 Among women, human immune virus prevalence is 3.6 percent in urban areas compared with 0.6 percent among women in rural areas. However, only 20 percent of women aged 15–49 had comprehensive knowledge about HIV transmission and prevention.10
A systematic review and meta-analysis finding on seroprevalence and mother to child transmission of human immune virus among pregnant women in Ethiopia showed 5.74% and 9.93% as a national prevalence respectively. However, regional analysis varies from Amhara region (9.5%) to SNNP (2.14%) and from Diredawa city administration (15.7%) to SNNP (4.16% for seroprevalence and mother to child transmission respectively).13,14
Recently, in limited studies done in different regions of Ethiopia, the acceptance rate and associated factors among pregnant women attending antenatal care services differ from one another both on the prevalence and associated factors.15–19 In addition to this, the study area is located among one of the regions of Ethiopia which has a great number of people living with human immune virus and research has not been done yet. Therefore, this study was conducted to assess the acceptance of HIV testing and associated factors among pregnant women that will assist policymakers, health planners and the decision-making process in the health of pregnant women living with human immune virus in a country with scarce resource settings.
Methods And Materials
Study Area, Design, And Participation
Institutional based cross-sectional study was employed in Gunino health center, Southern Ethiopia, which is 362 from the capital city of Addis Ababa, from May 20 to June 15, 2019. The town has four small administrative units (kebeles), eight private clinics, two drug stores, three health posts, and a health center. According to the town information desk, the total population was 27,927 of which 6,360 (23.3%) were in the reproductive age group of females. All pregnant women who attended antenatal care services in Gunino health center were considered as a source of the population whereas all pregnant women who attended antenatal care in Gunino health center during the study period were study population. Those pregnant women who attended antenatal care during the study period and selected for the sampling procedure were study units. All voluntary antenatal care attending pregnant women who were available during the study period were included in the study. However, all pregnant women who were mentally and physically seriously ill during the study were excluded from the study.
Sample Size Determination
The sample size was determined by using a single population proportion formula by considering the following assumptions: 70.1% of the proportion of acceptance of HIV testing,19 95% confidence interval, 5% marginal error, and 10% non-response rate. Based on these, a total of 356 antenatal care attending pregnant women were taken as a final sample size.
Sampling Procedures
The systematic sampling technique was used in this study. The average number of pregnant women who attended antenatal care in Gunino health center for two months was 689 by reviewing their antenatal care registration. Then, by dividing the average number of antenatal care attendants by the total sample size yielded the sampling interval (K-value). During the selection process, the first study participant was selected by lottery method. The rest of study participants were included in the study using every other attendant until it reached the final sample size.
N=average number of pregnant women attending ANC per month before the study=689
n= sample =356
K=N/n =689/356=1.9=2
Data Processing And Analysis
The data were entered using Epi-data version 3.1 and exported to SPSS version 24 for analysis. Descriptive statistics were used to describe the study population concerning relevant variables. Bivariate and multivariate models were used to assess the presence of any association between each independent variable and the dependent variable. Crude and adjusted odds ratios were used to know and ascertain any association between the independent and dependent variables while significance was declared using a 95% Confidence interval. Those candidate variables at bivariate logistic regression with a p-value <0.25 were moved to the multivariate logistic regression model for the dependent variables to control for potential confounding variables. Those variables with P-value <0.05 at multivariate analysis were considered as statistically significant to this study.
Operational Definition
Acceptors
Pregnant women who responded positively (Yes) to the question “Did you take HIV testing today?” were considered as acceptors and those who answered negatively (No) were considered as non-acceptors.
Knowledge Of HIV AIDS
Knowledge index was built from the answers to 11 questions: three questions on knowledge of HIV prevention, four questions on knowledge of human immune virus transmission, and four questions on misconceptions about modes of human immune virus transmission. Based on the answers to these knowledge questions, the index was classified as knowledgeable (score 6–11) and not knowledgeable (score< 6).
Knowledge Of MTCT
Knowledge index was constructed from the answers to four (Yes/No) questions (ever heard of MTCT, MTCT during pregnancy, labor, and breastfeeding). According to this knowledge of MTCT questions, the index was classified as knowledgeable (score 4) and not knowledgeable of MTCT (score≤3).
Knowledge Of PMTCT
Knowledge index was constructed from the answers to four questions (ever heard of PMTCT, using ART drugs, safe delivery practice, and exclusive breastfeeding for 6 months). According to this knowledge of PMTCT was considered as knowledgeable (score 4) and considered as not knowledgeable (score≤3).
Favorable Attitude
Favorable attitude was constructed from the response to six questions (yes/no) concerning with positively living other pregnant women (advise on drug usage, baby feeding, PMTCT, against stigma and discrimination).
Data Collection Tool, Quality, And Procedures
A structured interviewer-administered questionnaire was used to collect the data by using every other interval of the client exit. It was translated from English to Amharic and then back to English with language experts to keep consistency. The questionnaire contained socio-demographic information, knowledge of human immune virus prevention and transmission, knowledge of human immune virus prevention of mother to child, mother to child transmission, the attitude of HIV testing acceptance and utilization of human immune virus testing questions. Four diploma-holding nurses and one Bachelor of science holder health officer were recruited and trained as data collectors and supervisors respectively. A pretest was conducted on 36 reproductive age pregnant women attending antenatal care in Areka town health center. Data were checked for completeness and consistency by the supervisors and principal investigator.
Ethical Consideration
Ethical clearance letter was obtained from Wolaita Sodo University, College of Health Sciences; Department of Midwifery institutional review board. The aim of the research was explained to the study participants. Informed written consent was obtained from each pregnant woman who was above 18 years whereas parental consent was obtained from pregnant women under 18 before collecting the data. The participants’ confidentiality and privacy were maintained.
Results
Socio-Demographic Characteristics Of Pregnant Women
Among the total 356 women expected to be included in the study, 340 had participated with the response rate of 96 percent. Of these, more than half of the respondents, 213 (62.8%), were categorized under the age of 25–35 years, 84 (24.8%) were 15–24 years, and the remaining 43 (24.3%) were greater than or equal to 36 years old. The mean age of the study participants was 27.94 with ±SD 5.78. With regards to ethnicity, the majority of the participants 285 (62.8%) were Wolaita and a few of the remaining (22 (6.5%) and 33 (9.7%)) were Gurage and others respectively. Half of the participants (172 (50.6%)) were Protestant, 129 (37.9%) Orthodox, 25 (7.4%) Muslim, and 14 (4.1%) were Catholic followers. Concerning marital status, the majority of antenatal care attendants (267 (78.5%)) were married and only 21 (6.2%) were unmarried.
Among the participants, 104 (30.6%) had no formal education whereas 100 (29.4%), 83 (24.4%), and 53 (15.6%) had primary school education, secondary school education, diploma and above respectively.
In the case of occupation, 137 (40%) antenatal care attendants were housewives, 107 (31.5%) had a private job, 57 (16.8%) were government workers, 10 (2.9%) were daily workers, and 29 (8.5%) were “other“. More than half of the study participants (189 (53.2%)) had two and above antenatal care visits during the study period. Two hundred and four (60%) reported that they had not perceived the benefit of human immune virus testing (Table 1).
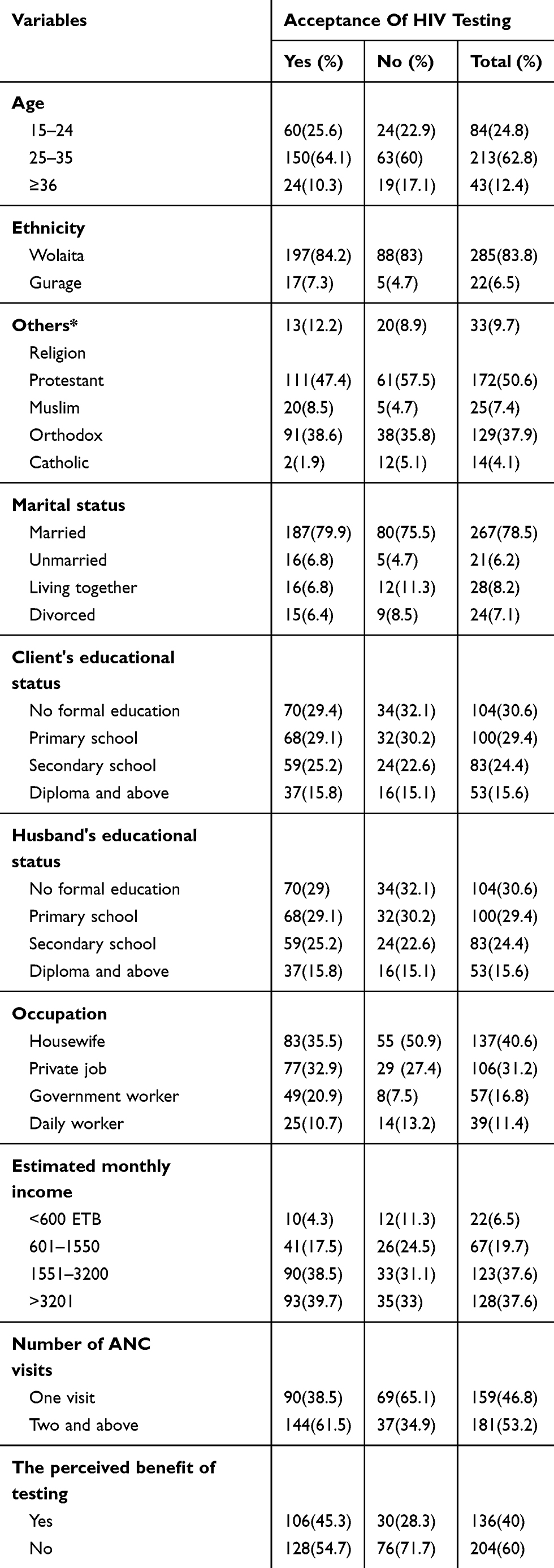 |
Table 1 Socio-Demographic Characteristics Of Pregnant Women Attending Antenatal Care Service In Gunion Town Health Center, Southern Region, Ethiopia, 2019 |
Acceptance Of HIV Testing
Among the total 340 study participants, 234 (68.8%) accepted HIV testing, while the remaining 106 (31.2%) rejected the human immune virus testing. Among the acceptors, 112 (47.7%) of respondents reported that the acceptance of human immune testing used to know themselves, 80 (34%) was for prevention of mother to child transmission, 42 (17.4%) for prevention of transmission to husband, and 2 (0.9%) had multiple reasons. Regarding non-acceptors, the reason for non-acceptance was fear of human immune virus positive test result in 37 (35.1%), not understanding advantage of testing in 20 (19%), fear of partner’s reaction to positive human immune virus result in 21 (20%), fear of stigma and discrimination in 24 (22.9%), and 3 (2.9%) had reported multiple reasons for refusal (Figure 1).
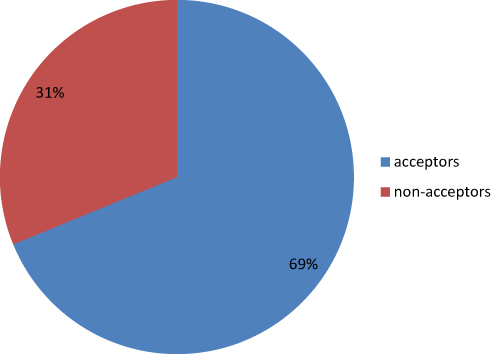 |
Figure 1 The proportion of acceptance and non-acceptance of HIV testing among pregnant women attending antenatal care in Gunino Health Center, Southern Ethiopia 2019. |
Knowledge And Attitude Related To Acceptance Of HIV Testing
Of the total respondents, 280 (82.4%) had awareness about human immune virus testing while the rest (60 (17.6%)) had not gained any information about human immune virus testing. More than half (203 (59.7%)) of the study participants had never heard about PMTCT, whereas 137 (40.3%) had never heard about PMTCT. The majority of participants (167 (49%)) heard from health providers followed by friends (97 (28.5%)), family (35(10.4%)), TV (28 (8.3%)), and multiple sources (13 (8.3%)). Two hundred and fifty-five (75%) of the respondents reported that transmission does not occur during pregnancy, while 85 (25%) explained transmission occurs during pregnancy. More than half (65.9%) believed that transmission does not occur during childbirth, but the remaining 116 (34.1%) believed that it could occur. Regarding breastfeeding, 281 (82.6%) explained that human immune virus transmission can occur during breastfeeding, but the rest (59 (17.4%)) did not realize this.
Concerning specific attitudes toward acceptance of human immune virus testing, 85 (36.6%) of acceptors, and 29 (27.4%) of non-acceptors agreed on use of drugs to prevent mother to child transmission for ANC clients, and 60 (25.6%) of acceptors, and 21 (19.8%) of non-acceptors believed that child transmission, exclusive breastfeeding prevent mother to child transmission. Forty-four (18.8%) of acceptors, and 24 (22.6%) of non-acceptors believed that stigmatization of HIV positive people exacerbates fear of newly infected people.
On the other hand, 98 (41.9%) of acceptors, and 31 (29.2%) of non-acceptors of antenatal care visit attendant pregnant women believed that testing acceptance was easier for clients to get testing. The majority (190 (81.2%)) of acceptors, and 72 (67.9%) non-acceptors lead people to avoid the fear of going to a health facility for human immune virus testing (Table 2).
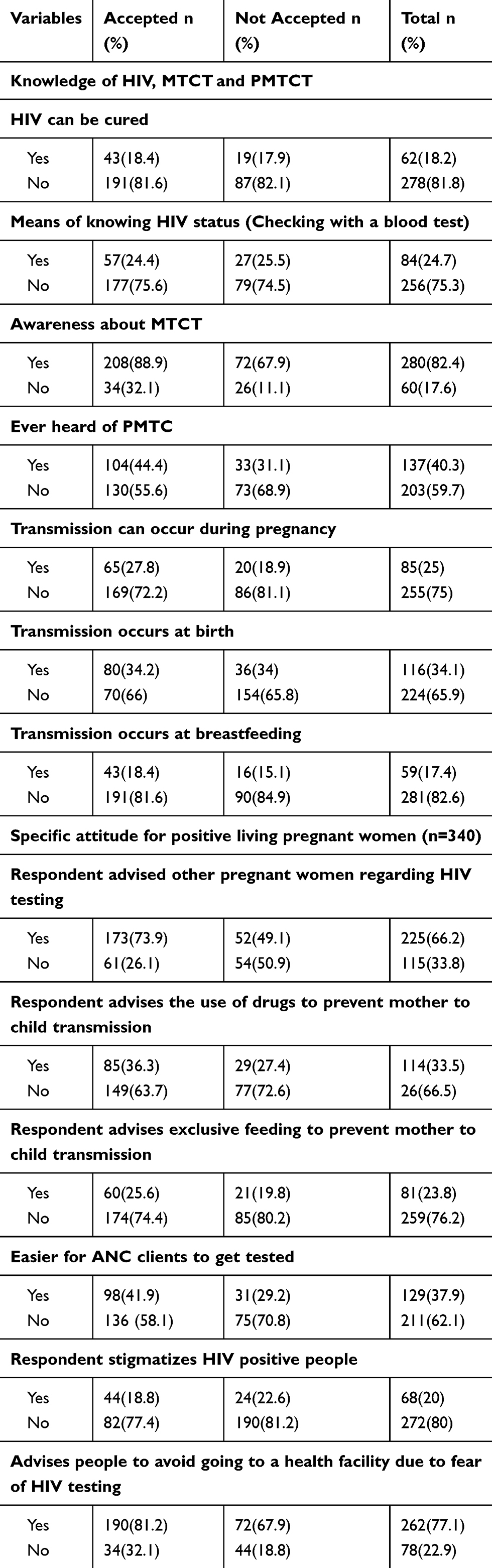 |
Table 2 Knowledge And Attitude Related To Acceptance Of HIV Testing Among Pregnant Women Attending Antenatal Care Clinic In Gunino Health Center, Southern Ethiopia 2019 |
Factors Associated With Acceptance Of HIV Testing Among Pregnant Women
On bivariate analysis, we found that no formal education, primary school level, secondary school level, private worker, government worker, awareness about HIV testing, using provider as source, using friend as source, perceived benefit of human immune virus testing, knowledge of prevention of mother to child transmission, and two and more antenatal care visits showed a statistically significant association with acceptance of human immune virus testing.
On multivariate analysis, the respondents with no formal education, primary level of education, awareness about human immune virus testing, perceived benefit of testing, knowledge of prevention of mother to child transmission, and one ANC visit were found to have statistically significant acceptance of human immune virus testing. Respondents who had no formal education (AOR= 0.393, 95% CI:0.160,0.967), and primary school education (AOR=0.357, 95% CI:0.152, 0.842) were 39% and 36% less likely to accept human immune virus testing than diploma and above educational status holders. Participants who had awareness of HIV testing were 2.6 times more likely to accept human immune virus testing than their counterparts (AOR=2.602, 95% CI:1.408, 4.809). Study participants who perceived the benefit of human immune virus testing were 1.8 times more likely to accept testing than their counterparts (AOR=1.838, 95% CI:1.809, 3.104). Those study participants who were knowledgeable about the prevention of mother to child transmission were 1.7 times more likely to accept human immune virus testing than their counterparts (AOR=1.715, 95% CI:1.030, 2.855). On the other hand, participants who had attended two and above antenatal care visits were 2.5 times more likely to accept HIV testing than those who attended only once (AOR=2.485, 95% CI:1.462, 4.224) (Table 3).
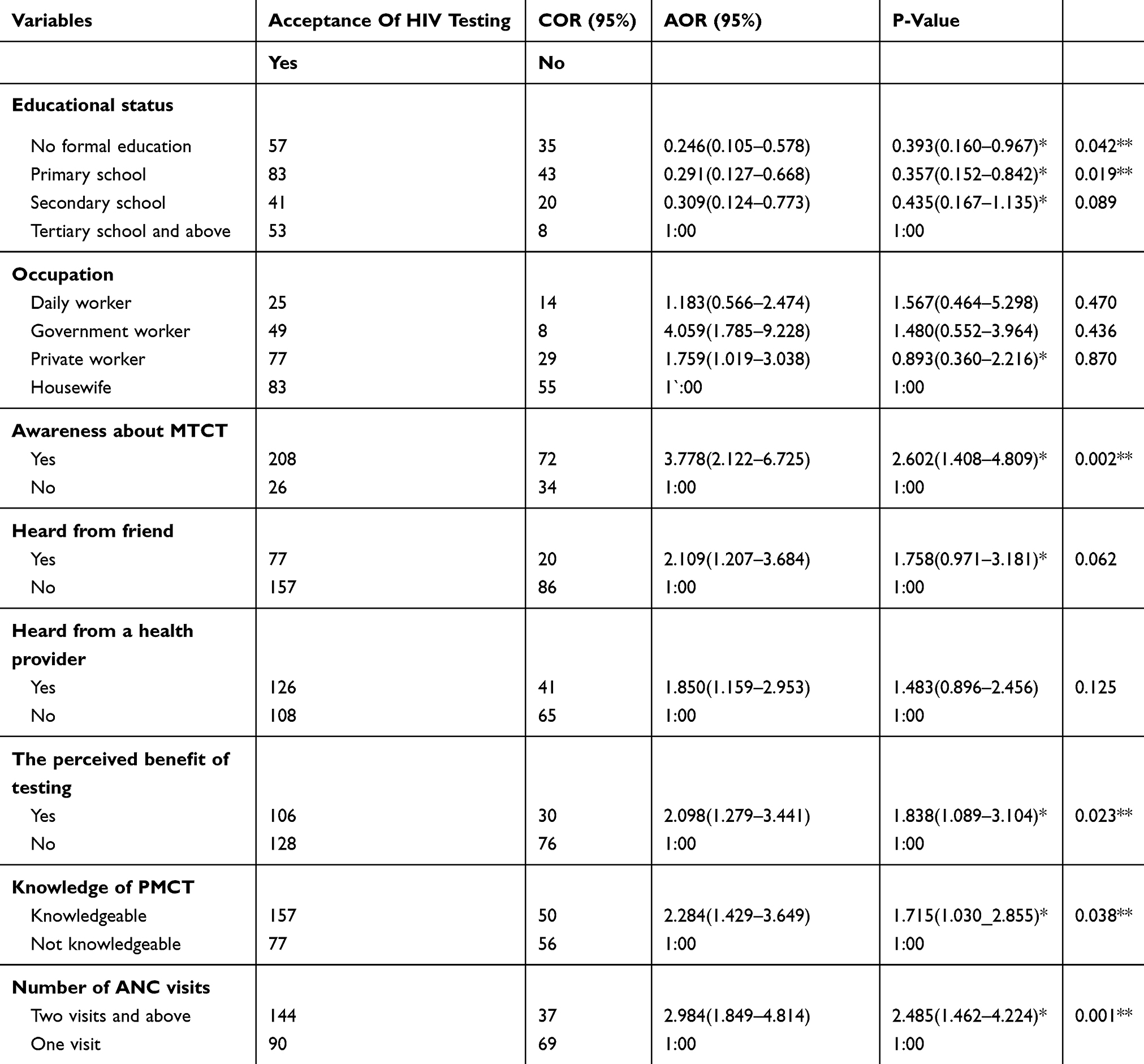 |
Table 3 Analysis Of Factors Associated With The Acceptance Of HIV Testing Among Pregnant Women Attending Antenatal Care In Gunino Health Center, Southern Ethiopia 2019 (n=340) |
Discussion
Human immune virus testing is one of the major strategies to prevent mother to child transmission among pregnant women attending the antenatal clinic. This study found that the acceptance rate of human immune virus testing among pregnant women was 68.8%, which was consistent with the acceptance rate of studies in the central part of Ethiopia; Adama (70.1%), and Mexico (70%).19,20 This finding was also higher than the acceptance rate of studies conducted in the Southwest part of Ethiopia; in Illubabor (27%), and Ghana (60%).21,22 The reason behind the higher acceptance rate could be the time gap between the studies, community sensitization, counseling sessions by health providers, and the presence of on-site rapid HIV testing and awareness through the community play a crucial role in the acceptance of human immune virus testing presently.
On the contrary, the finding of this study was also less than studies conducted in different parts of Ethiopia; Assosa (80.8%), Harar (82.4%), Hawassa (84.1%), Gondar (82.5%), and studies done in African countries; Congo(72%), and Cameroon (88.3%).15–17,23–25 The discrepancy was due to study setting in which the studies were conducted: in major towns of the country as compared with the present study. This enables study participants to have enough information, and access to human immune virus testing which in turn contributes to higher acceptance compared to the current study. In addition to this, there were differences in availability, accessibility, infrastructure, and socio-economic status between the present study and studies done in Congo and Cameroon.
In this study, pregnant women with a primary and secondary level of education were less likely to accept testing than those with a diploma and above education level, which was in line with a study done in Ethiopia, Congo.24–26 However, this was in contrast with a finding of the study done in Northwest part of Ethiopia; in Gondar and Botswana more pregnant women with no education accepted HIV testing than women with basic education. The possible explanation is that education plays a key role in individual health-seeking behavior, and prevention of mother to child transmission, that promotes human immune virus testing.
A positive association was observed between awareness of mother to child transmission, and acceptability of HIV testing, which was in line with a previous study done in Ethiopia.26 Pregnant women with previous knowledge of prevention of mother to child transmission were more likely to accept human immune virus testing than their counterparts, similar to studies done in different parts of Ethiopia.16,23 This could be due to the higher perceived benefit of human immune virus testing among women who had a better knowledge of mother to child transmission, and prevention of mother to child transmission which in turn influences testing acceptance positively.
A study showed that pregnant women who perceived the benefit of human immune virus testing were more likely to accept testingthan those who did not perceive the benefit of testing. This finding showed a similar association as a study conducted in Eastern parts of Ethiopia; in Dire Dawa.18 This was because the perceived benefit of testing enhances acceptance of human immune virus testing, as explained by the health belief model which showed a positive association.
The findings of this study showed that pregnant women who attended two and above antenatal care visits had a positive association with acceptance of HIV testing compared to those who attended only one visit. It was in agreement with the finding of studies in Ethiopia,16–19,23 but in contrast with a study done in Cameroon.25 This was because the more antenatal care visits the pregnant women attended, the more they heard about PMTCT and MTCT, which contributes positively to the acceptance of testing.
The most frequent reasons for acceptance of human immune virus testing in this study were to prevent infection of their children (34%), and concern for their health (47.7%), and the main reasons for refusal of testing were fear of positive human immune virus result (35.1%), fear of stigma, and discrimination (22.9%) and fear of partners' reaction to positive result (20%). This was in agreement with the finding of a study of Northwest Ethiopia; in Gondar, and Harar.17,23
Conclusion
The finding of this study demonstrated that acceptance of antenatal HIV testing among pregnant women was low. It is therefore highly recommended that routine antenatal human immune virus testing should become a standard of care to achieve the 2020 set goal of Ethiopia as a country. More antenatal visits, awareness of mother to child transmission, perceived benefit of human immune virus testing, and knowledge about prevention of mother to child transmission affect acceptance of human immune virus testing positively. However, no formal education and primary level education affected the acceptance of testing negatively. Antenatal caregivers should place emphasis on reducing barriers to testing like lack of awareness, knowledge and educational background, the benefit of HIV testing, and the importance of antenatal care service during a counseling session.
Abbreviations
AIDS, acquired immune deficiency syndrome; ANC, antenatal care service; HIV, human immune virus; MTCT, mother to child transmission; PMTCT, prevention of mother to child transmission; SNNPRR, Southern nations nationalities and peoples region; UNAIDS, United Nation program on acquired immune deficiency syndrome.
Availability Of Data And Materials
The data that support the findings of this study are available, but some restrictions may apply to the availability of these data as there are some sensitive issues. However, data are available from the corresponding authors upon reasonable request.
Acknowledgments
We would like to thank Wolaita Sodo University, College of Health Sciences, and the Department of Public Health. Our deepest and special thanks go to Gunino town Administrator office for writing letters of permission to each kebele. We would also like to say thank you very much for their assistance with data collectors, supervisors and study participants.
Authors Information
Natnael Atnafu Gebeyehu, Kelemu Abebe Gelaw, and Addisu Yeshambel are Lecturers in the Department of Midwifery, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia.
Author Contributions
NA was involved in the conception, design, analysis, interpretation, report and manuscript writing. AY and KA were involved in drafting the article, design, analysis, interpretation and report writing. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. UNAIDS J. Fact Sheet—Latest Global and Regional Statistics on the Status of the AIDS Epidemic. Geneva: UNAIDS; 2017.
2. UNAIDS J. Country’s epidemiological fact sheet. ETHIOPIA, 2016. Geneva: UNAIDS, 2016.
3. Kharsany AB, Karim QA. HIV infection and AIDS in Sub-Saharan Africa: current status, challenges and opportunities. Open AIDS J. 2016;10:34. doi:10.2174/1874613601610010034
4. Federal Ministry of Health Ethiopia. Guidelines for the prevention of mother to child transmission of HIV in Ethiopia. Ministry of Health of Ethiopia; 2011.
5. WHO. Consolidated Guidelines on HIV Testing Services. Geneva: Switzerland July; 2015.
6. UNAIDS. HIV testing services: new opportunities and ongoing challenges [Internet]; 2017
7. FHAPCO/FMOHE. Guidelines for HIV counseling and testing in Ethiopia; July 2007.
8. Federal HIV Prevention and Control Office of Ethiopia. HIV/AIDS strategic plan 2015–2020 in an investment case approach [Internet]; December 2014
9. UNAIDS. 90-90-90. An ambitious treatment target to help end the AIDS epidemic. [Internet]; 2014
10. Central Statically Agency (CSA) and ICF. Ethiopian demographic and health survey 2016. HIV Report Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2018.
11. Global AIDS response progress reporting. Monitoring the 2011 political declaration on HIV/AIDS: guidelines on construction of core indictors. Geneva: USAID; 2012. Available from: http://files.unaids.org/en/media/unaids/contentassets/documents/document/2011/JC2215_Global_AIDS_Response_Progress_Reporting_en.pdf
12. Federal HIV/AIDS Prevention and Control Office. HIV prevention in Ethiopia National Road Map 2018–2020; November 2018.
13. Kassa GM. Mother-to-child transmission of HIV infection and its associated factors in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2018;18:216. doi:10.1186/s12879-018-3126-5
14. Geremew D, Tajebe F, Ambachew S, Endalamaw A, Eshetie S. Seroprevalence of HIV among pregnant women in Ethiopia: a systematic review and meta-analysis. BMC Res Notes. 2018;11:908. doi:10.1186/s13104-018-4022-1
15. Abtew S, Awoke W, Asrat A. Acceptability of provider initiated HIV testing as an intervention for prevention of mother to child transmission of HIV and associated factors among pregnant women attending at public health facilities in Assosa Town, North Ethiopia. BMC Res Notes. 2015;8. doi:10.1186/s13104-015-1652-4
16. Gizaw R, Gebremedihn S. Acceptance of HIV counseling and testing among antenatal clinic attendees in Hawassa City, Southern Ethiopia. Ethiop J Health Sci. 2018;28(4):413.
17. Bekele Z, Omer A, Feleke D. Acceptability of provider initiated hiv testing as an intervention for prevention of mother to child transmission of HIV and associated factors among pregnant women attending at Public Health Facilities in Harar Town, North Ethiopia. J AIDS HIV Infect. 2018;4(2).
18. Demissie A, Deribew A, Abera M. Determinants of acceptance of voluntary HIV testing among antenatal clinic attendees at Dilchora Hospital, DireDawa, Ethiopia. Ethiop J Health Dev. 2009;23(2).
19. Gebremedihn KB, Tian B, Tang C, et al. Factors Associated with Acceptance Provider Initiated HIV Testing and Counseling among Pregnant Women in Adama, Ethiopia. Dove press; 2018.
20. Damian F, Plazola-Camacho N, Flores-medina S. Factors associated with non-acceptance of HIV screening test among pregnant women in Mexico. J HIV Retrovirus. 2016;2(3):27. doi:10.21767/2471-9676.100027
21. Kebede D, Alemayehu A, Biniam G, Wassie L, Yismaw D. Uptake and barriers of voluntary counseling and testing among antenatal care attendants, southwest Ethiopia. Ethiop J Health Sci. 2006;16(1).
22. Nyuzaghi J, Ohene S, Odoi-Agyarko K. Acceptability of routine offer of HIV testing among pregnant women in the Wa Municipality, Ghana. Med J. 2011;45(1).
23. Melayu MT, Alene GD. Assessment of utilization of provider initiated hiv testing and counseling as an intervention for prevention of mother to child transmission and associated factors among pregnant women in Gondar town, Northwest Ethiopia. BMC Public Health. 2012;12.
24. Ghoma-Linguissi LS, Ebourombi DF, Sidibe A, et al. Factors influencing acceptability of voluntary HIV testing among pregnant women in Gamboma, Republic of Congo. BMC Res Notes. 2015;8:652. doi:10.1186/s13104-015-1651-5
25. Kongnyuy E, Mbu E, Mbopi-Keou F, et al. Acceptability of intrapartum HIV counseling and testing in Cameroon. Available from: http://www.biomedcentral.com/1471-2393/9/9.
26. Ejigu Y, Tadesse B. HIV testing during pregnancy for prevention of mother to child transmission of HIV in Ethiopia. PLoS One. 2018;13(8). doi:10.1371/journal.pone.0201886
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.