")
Back to Journals » Pragmatic and Observational Research » Volume 11
Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo
Authors Kabamba Nzaji M , Kabamba Ngombe L, Ngoie Mwamba G , Banza Ndala DB, Mbidi Miema J, Luhata Lungoyo C, Lora Mwimba B, Cikomola Mwana Bene A, Mukamba Musenga E
Received 28 July 2020
Accepted for publication 13 October 2020
Published 29 October 2020 Volume 2020:11 Pages 103—109
DOI https://doi.org/10.2147/POR.S271096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor David Price
Michel Kabamba Nzaji,1,2 Leon Kabamba Ngombe,1,3 Guillaume Ngoie Mwamba,4 Deca Blood Banza Ndala,5 Judith Mbidi Miema,2 Christophe Luhata Lungoyo,2 Bertin Lora Mwimba,2 Aimé Cikomola Mwana Bene,2 Elisabeth Mukamba Musenga2
1Department of Public Health, Faculty of Medicine, University of Kamina, Kamina, Democratic Republic of Congo; 2Ministry of Health, National Expanded Program for Immunization, Operational Research Unit, Kinshasa, Democratic Republic of Congo; 3Department of Epidemiology and Public Health, Nursing Care Section, Higher Institute of Medical Techniques of Lubumbashi, Lubumbashi, Democratic Republic of Congo; 4VillageReach, Kinshasa, Democratic Republic of Congo; 5Department of Epidemiology and Public Health, Community Health Section, Higher Institute of Medical Techniques of Mbuji-Mayi, Mbuji-Mayi, Democratic Republic of Congo
Correspondence: Michel Kabamba Nzaji Tel +243978467432
Email [email protected]
Purpose: This study aims to estimate the acceptability of a future vaccine against COVID-19 and associated factors if offered in Congolese health-care workers (HCWs), since they have the highest direct exposure to the disease.
Patients and Methods: We conducted an analytical cross-sectional study among 23 Congolese referral hospitals, including three university hospitals, located in three towns from March through 30 April 2020. The main outcome variable was healthcare workers’ acceptance of a future vaccine against COVID-19. The associated factors of vaccination willingness were identified through a logistic regression analysis.
Results: A sample of 613 HCWs participated in the study and completed the study questionnaire, including 312 (50.9%) men and 301 (49.1%) women. Only 27.7% of HCWs said that they would accept a COVID-19 vaccine if it was available. From the logistic regression analysis, male healthcare workers (ORa=1.17, 95% CI: 1.15– 2.60), primarily doctors (ORa=1.59; 95% CI:1.03– 2.44) and having a positive attitude towards a COVID-19 vaccine (ORa=11.49; 95% CI: 5.88– 22.46) were significantly associated with reporting willingness to be vaccinated.
Conclusion: For acceptability of vaccination against COVID-19 among others education among HCWs is crucial because health professionals’ attitudes about vaccines are an important determinant of their own vaccine uptake and their likelihood of recommending the vaccine to their patients.
Keywords: COVID-19 vaccine, health-care workers, HCWs, acceptability, DRC
Introduction
A massive global human disaster has been created by a recent contagious respiratory infectious disease caused by a novel coronavirus (SARS-CoV-2) which holds the same veiled RNA structure resembling SARS-CoV-1 that caused the Severe Acute Respiratory Syndrome (SARS) outbreak.1
Classified by the World Health Organization (WHO) as a pandemic On March 12, 2020. The first cases of COVID-19 were identified in Wuhan, China at the end of December 2019. The virus has now affected virtually every country across the world and the number of deaths continues to rapidly increase.2 As of May 3rd, 2020, over 3.5million cases and 245,258 deaths have been reported globally. At the time of the study, the African continent was the least affected with 43,909 cases and 1764 deaths, but the numbers were increasing. In the Democratic Republic of the Congo (DCR), located in Central Africa, cases have been reported since March 8th, 2020. As of July 03, 2020, the DRC has had 7379 cases and 182 deaths.
Knowing that social distancing and quarantine may slow the spread of the virus and flatten the epidemic curve; it may not be sufficient to completely halt the spread of COVID-19, herd immunity gained by infection or vaccination will need to be well established within the population.3 The most effective way of controlling infectious diseases is often vaccination, while success is challenged by individuals and groups who choose to delay or refuse vaccines.4
Although immunisation has successfully reduced the global burden of illness and death, public confidence in vaccines can be affected by various concerns. As such, vaccine hesitancy can lead to delays and refusal and sometimes contribute to disease outbreaks.5
The most serious example is the 2003–04 northern Nigeria boycott of polio vaccination, which led to a resurgence of the disease6.6–8 The fundamental breakdown in public trust still affects polio eradication efforts in Nigeria.9 But, Nigeria has officially wiped out wild polio.
Maintaining confidence in vaccination depends on the interaction between patients and providers.10,11 Attitude and utilization of vaccination by healthcare professionals (HCP) is a major factor that is consistently associated with patient acceptance and vaccination, adherence to vaccination schedules, and reduced hesitation/aversion.12 In addition, vaccinated HCPs also have a noticeable effect on patients’ decision to take a vaccine.
Health professionals’ intention to use and to recommend the vaccine to their patients depends on their knowledge and attitudes about vaccines. It is well reported that healthcare professionals who have an unfavorable attitude, aversion or hesitation towards vaccinations transmit these hostile attitudes to vaccination to patients and tend to recommend vaccination less frequently.13 Furthermore, vaccine hesitancy observed in the general population has been consistently linked to the level of vaccine hesitancy among HCPs.14 In addition, the quality, content and dissemination of educational information about vaccines by healthcare professionals have been shown to be useful in improving patient acceptance of vaccinations, reducing reluctance, and guiding informed decisions about vaccination.15 Indeed, patients often trust and rely on healthcare professionals for information about vaccines and vaccine-preventable diseases, as well as the therapeutic and public health benefits associated with immunization12,15.
The major challenge for public health experts is the waning of public confidence in vaccines worldwide. Public confidence in vaccines worldwide is a cause for concern and a major challenge for public health experts.16 While there are a number of influencers, healthcare workers (HCWs) are an important group to consider. For example, nurses in South Africa felt that adolescents and young adults who accepted HPV vaccination were more likely to recommend it.17
The development of COVID-19 vaccines is a crucial challenge. At the time of the study, many were in “pre-clinical testing”,18 with a number already in Phase 1 Trials with promising results from animal studies. However, even with rapid development and experimentation, the estimated fastest time to develop a new vaccine will be at least 1 to 1.5 years.19 After its clinical development, another challenge is the distribution and acceptance of the vaccine in general population. The impact of the current pandemic on the intention to be vaccinated against COVID-19 with an approved vaccine has not made it unanimously accepted that if it were available it would be obviously adopted. Therefore, the objective of this study was to evaluate the acceptability of a future COVID-19 vaccine and associated factors if offered to Congolese HCWs, since they have the highest direct exposure to the disease.
Methodology
Study Design, Sites and Participants
An analytical cross-sectional study was conducted in 23 Congolese referral hospitals, including three university hospitals, located in three towns from 20 March through 30 April 2020: seven in Lubumbashi (Haut-Katanga province), nine in Mbuji-Mayi (Kasai Oriental province) and seven in Kamina (Haut-Lomami province). HCWs (doctors, nurses, midwives, and laboratory technicians) aged 18 years or older who accepted to participate, and working in referral hospitals located in above-mentioned towns were eligible for this study. Younger (aged less than 18 years) HCWs and those who were absent on the day of the survey were excluded.
Survey Questionnaire and Data Collection
Data were collected with the use of a self-administered questionnaire, which was developed based on the “Exposure Risk Assessment in the context of COVID-19”,20 in French language and consisted of two parts: demographics and KAPs. Demographic variables included age, gender, marital status, years of working experience and the source information related to COVID-19. The second part included 12 questions on COVID-19 related knowledge (clinical manifestations, disease transmission, patient care approach), three others on attitudes towards COVID-19 (confidence about overcoming the pandemic, willingness to get COVID-19 vaccine), and the last three questions were related to practices towards COVID-19 prevention (social distancing, general preventive measures, consistency of PPE use); each correct answer weighing one point (zero points for an incorrect answer).
Using Bloom’s cut-off point of 80%,21 a participant who provided correct answers to 80–100% of the 12 knowledge-related questions was considered having sufficient COVID-19 knowledge. Regarding attitudes and practices, a participant with a score higher than the mean score was considered to have positive attitudes or comply with good practices. The primary variable of interest in the KSP module was related to the statement, “If a COVID-19 vaccine was available, I would have it.”
Enrollment of participants took place at each service that provides patients’ care and medical laboratory unit of participating hospitals. Each participant received an anonymous questionnaire sheet after getting informed on the objectives and activities of this study.
Ethical Approval
All the HCWs were informed about the objectives of the study, and they agreed and signed a consent form before participation. The study was approved by the ethics committee of the School of Public Health (approval letter No UNILU/CEM/226/2020), University of Lubumbashi, DRC.
Statistical Analysis
Data were analyzed using SPSS 23.0 software. Categorical data related to demographic variables are presented as frequencies and proportions. The associations between independent variables and the primary outcomes (acceptance and intention to receive a COVID-19 vaccine) were tested using t-test or Chi-square test as appropriate. Variables that are associated (p<0.10) in the unadjusted analyses were further adjusted for demographic factors (ie, age) using stepwise logistic regressions. The level of significance was set to 0.05 (two-tailed).
Results
In the study, 613 HCWs participated and completed the questionnaire, including 312 (50.9%) men and 301 (49.1%) women (Table 1). Most participants were over 25 years of age (95.3%); the average age was 40.3 years (standard deviation [SD]: 11.7). The majority of participants were allied health workers (72.8%). They mostly had over 10 years of experience (53.5%) and were married (66.6%). Almost all (99.3%) of the participants agreed that they heard about COVID-19, but only 41.9% of them had an opportunity to attend lectures/discussions about COVID-19. Only 27.7% of HCWs said that they would get vaccinated if the COVID-19 vaccine was available.
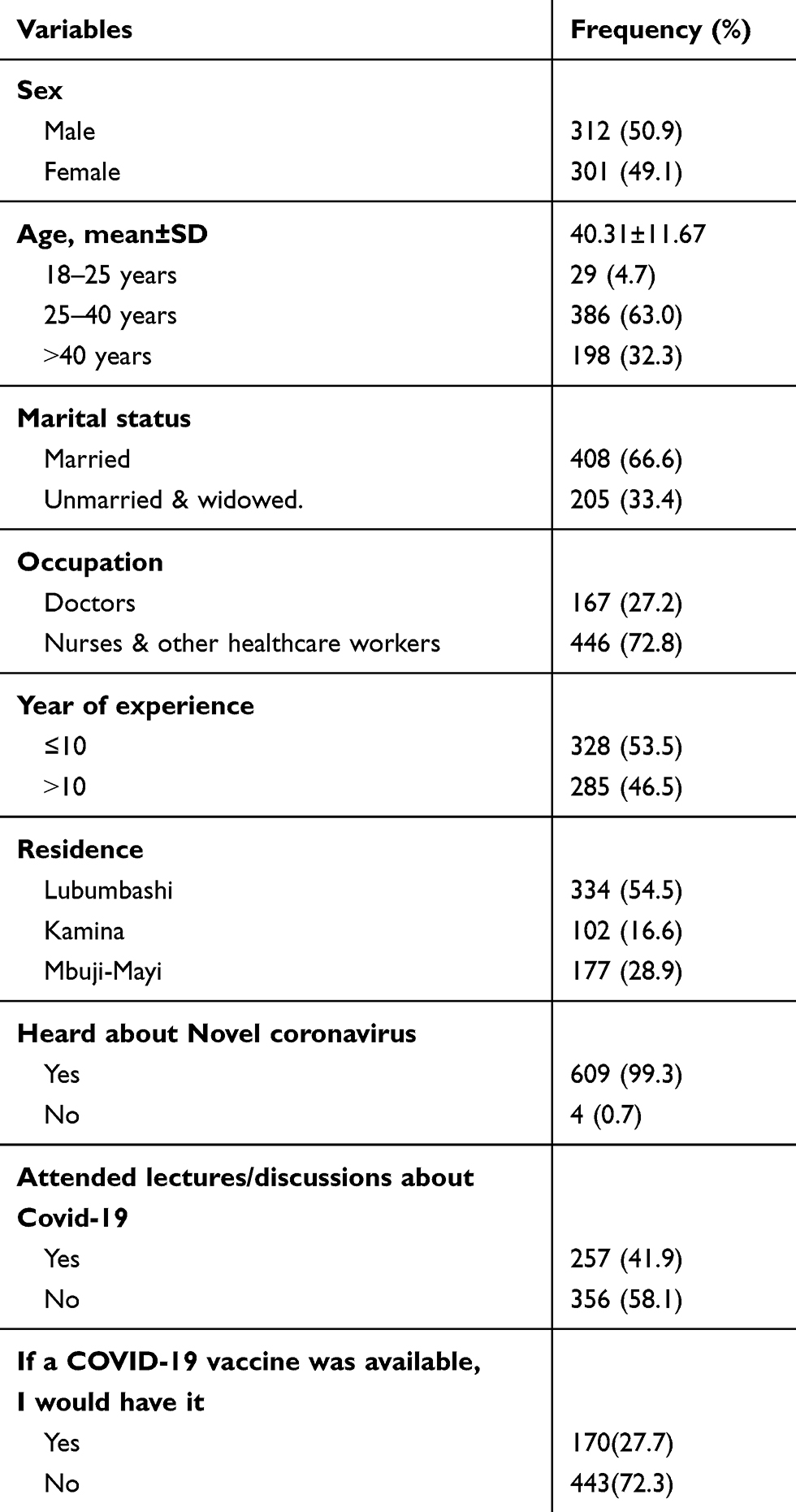 |
Table 1 Sociodemographic Characteristics of Healthcare Workers’ (N=613) |
Some variables were significantly associated with COVID-19 vaccine acceptance after stepwise selection including: older age, occupation, belief that isolation and treatment of people who are infected with COVID-19 are effective ways to reduce the spread of the virus, use the official OMS website, positive attitude and attended lectures/discussions about Covid-19 (Table 2).
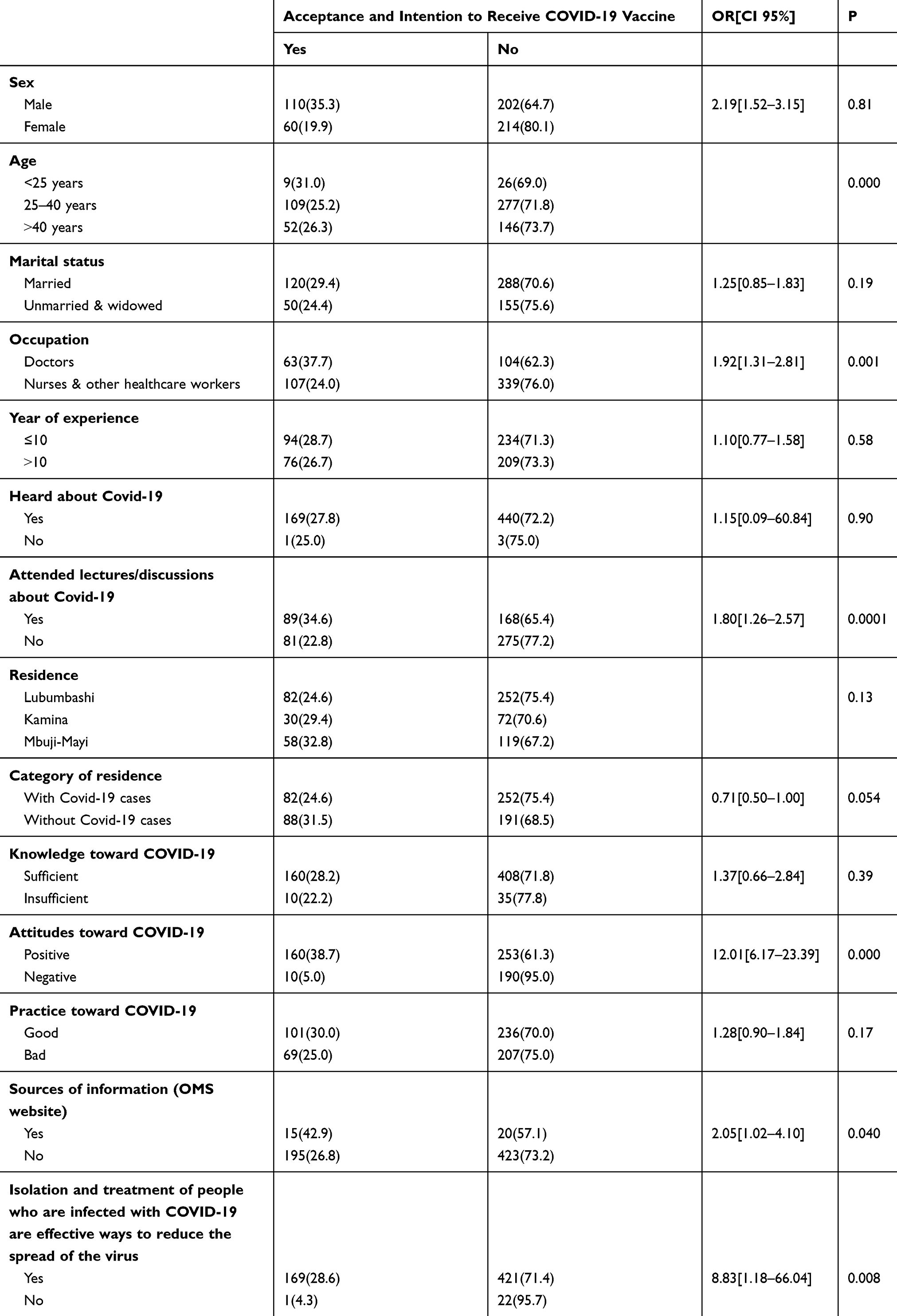 |
Table 2 Univariate Association of Variables Affecting the Intention to Accept COVID-19 Vaccine Among Healthcare Workers |
The variables that were significantly associated with reporting willingness after logistic regression were being a male healthcare workers (ORa=1.17, 95% CI: 1.15–2.60), being a doctor (ORa=1.59; 95% CI:1.03–2.44) and having a positive attitude towards COVID-19 (ORa=11.49; 95% CI: 5.88–22.46) (Table 3).
 |
Table 3 Logistic Regression Model for Intention to Accept COVID-19 Vaccine |
Discussion
In public health, vaccination is one of the most important advances. It is responsible for the eradication of smallpox and the control of infectious diseases in many parts of the world (eg, rubella, diphtheria, polio).22 As a result, scientists have been racing to develop and test new vaccines to protect against SARS-CoV-2 and the speed of scientific discovery related to COVID19 is unprecedented.23
In this survey, only 28% of the participants said that they would get a vaccine against COVID-19 if and when one becomes available. The willingness of Congolese healthcare workers to be vaccinated against COVID-19 virus is very low when compared with a comparable study done in France which found that 77.6% (95% CI 76.2–79%) of participants “probably agreed” to get vaccinated against COVID-19.19 This low acceptance in our study may be explained by the harm of social networks and spread of misinformation. Since the first COVID-19 cases, misinformation has spread across traditional media and social media, called by WHO an infodemic (ie, excessive amounts misinformation and rumours that make it difficult identify reliable sources of information).24 After hearing about poor vaccine quality and the false information conveyed by mass media which has included rumors on the extermination of the black race through vaccination, healthcare workers may have developed vaccine hesitancy, which can influence their decisions to get vaccinated and to promote the vaccine to their patients.
In our study, older HCWs accepted to get vaccinated. This may be due to the notion that older adults and people with serious comorbidities are particularly vulnerable to worse outcomes from COVID-19 can create considerable fear amongst the elderly.25 Carla Felice and al. demonstrated that 10% of the infected people in Italy are HCWs.26 Furthermore, 80 medical doctors and 25 nurses died from COVID-19 related complications in Italy. Many Italian HCWs were tested and many more may have been presenting with few symptoms, which underestimated the real impact of COVID-19 on this category.27 In terms of gender, our results were similar to other studies, and we observed that more men accepted to get vaccinated compared to women.19,28,29 This may be due to an increased risk perception of disease in men compared to women. However, people most likely at-risk for COVID-19 infection will accept vaccination. Perceptions of risk are an inherent part of the decision-making process. Data collected from Chinese death rates reveal that there exists a gender gap in causality rate; 64 per 100 men (4.7% mortality rate) compared to 36 per 100 women (2.8% mortality rate).30,31 In a recent study, scientists collected plasma samples of 331 COVID-19 positive patients; they found that women’s samples had more antibodies which may have an impact on their immune response compared to the men’s samples.32
Healthcare worker recommendations play an influential role in their patients’ vaccination behavior. They serve as an important source of information for the general public and their consultation can also be a key factor in patients’ decision to be vaccinated or not. In this context and with the low positive response for acceptability of vaccination in our participants, there is a significant need for addressing concerns and increasing awareness to improve chances for higher acceptance of a COVID-19 vaccine. Otherwise, there is an additional chance of mass rejection of COVID-19 vaccine in the general population when a vaccine becomes available.
Conclusion
Currently, during this COVID-19 pandemic, only approximately 28% of the HCWs interviewed said they would get a COVID-19 vaccine if available. In the context of a pandemic, vaccine hesitancy is a major barrier to implementing vaccination campaigns. To maintain the benefits of vaccination programmes, understanding and addressing vaccine hesitancy will be crucial to their successful implementation. Developing tailored strategies to address concerns identified in the study to decrease vaccine hesitancy will be the key to success.
Acknowledgment
We are grateful to Patricia Mechael for English proofreading.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Rahman A, Sathi NJ. Knowledge, attitude, and preventive practices toward COVID-19 among Bangladeshi internet users. Electron J Gen Med. 2020;17(5).
2. Sim MR. The COVID-19 Pandemic: Major Risks to Healthcare and Other Workers on the Front Line. 2020:281–282. doi:10.1136/oemed-2020-106567
3. Fu C, Wei Z, Pei S, Li S, Sun X, Liu P. Acceptance and preference for COVID-19 vaccination in health-care workers (HCWs). medRxiv. 2020;2962(548):
4. Paterson P, Paterson P, Meurice F, Stanberry LR, Glismann S, Rosenthal SL. Vaccine hesitancy and healthcare providers vaccine hesitancy and healthcare providers. Vaccine. 2016;34(October):6700–6706. doi:10.1016/j.vaccine.2016.10.042
5. Larson HJ, Smith DMD, Paterson P, et al. Measuring vaccine confi dence: analysis of data obtained by a media surveillance system used to analyse public concerns about vaccines. Lancet Infect Dis. 2013;13(7):606–613. doi:10.1016/S1473-3099(13)70108-7
6. Ghinai I, Willott C, Dadari I, Larson HJ. Listening to the rumours: what the northern Nigeria polio vaccine boycott can tell us ten years on. Glob Public Health. 2013;8(10):1138–1150. doi:10.1080/17441692.2013.859720
7. Kaufmann JR, Feldbaum H. Diplomacy and the polio immunization boycott in Northern Nigeria. Health Aff. 2009;28(4):1091–1101. doi:10.1377/hlthaff.28.4.1091
8. Heymann DL, Sutter RW, Aylward RB. Polio eradication: interrupting transmission, towards a polio-free world. Future Virol. 2006;1(2):181–188. doi:10.2217/17460794.1.2.181
9. Larson HJ, Ghinai I. Lessons from polio eradication. Nature. 2011;473(7348):446–447. doi:10.1038/473446a
10. Leask J, Kinnersley P, Jackson C, Cheater F, Bedford H, Rowles G. Communicating with parents about vaccination: a framework for health professionals. BMC Pediatr. 2012;12(1):1. doi:10.1186/1471-2431-12-154
11. Schmitt HJ, Booy R, Aston R, et al. How to optimise the coverage rate of infant and adult immunisations in Europe. BMC Med. 2007;5(1):1–8. doi:10.1186/1741-7015-5-11
12. Asma S, Akan H, Uysal Y, et al. Factors effecting influenza vaccination uptake among health care workers: a multi- center cross-sectional study. BMC Infect Dis. 2016:1–9. doi:10.1186/s12879-016-1528-9
13. Arda B, Durusoy R, Yamazhan T, Ta M, Pullukçu H. Did the pandemic have an impact on influenza vaccination attitude? A survey among health care workers. BMC Infect Dis. 2011;11(1). doi:10.1186/1471-2334-11-87
14. Naz H, Cevik F, Aykın N. Original Article Influenza Vaccination in Healthcare Workers. 2006.
15. Mereckiene J, Cotter S, Nicoll A, et al. The V project gatekeepers group. Seasonal influenza immunisation in Europe. Overview of recommendations and vaccination coverage for three. Euro Surveill. 2014;19(16):20780. doi:10.2807/1560-7917.ES2014.19.16.20780
16. Kumar D, Chandra R, Mathur M, Samdariya S, Kapoor N. Vaccine hesitancy: understanding better to address better. Isr J Health Policy Res. 2016;5(2):1–8. doi:10.1186/s13584-016-0062-y
17. Hoque ME, Monokoane S, Van HG. Knowledge of and attitude towards human papillomavirus infection and vaccines among nurses at a tertiary hospital in South Africa Knowledge of and attitude towards human papillomavirus infection and vaccines among nurses at a tertiary hospital in South Af. J Obstet Gynaecol. 2014;34(February):182–186. doi:10.3109/01443615.2013.861395
18. Lurie N, Saville M, Hatchett R, Halton J. Developing covid-19 vaccines at pandemic speed. N Engl J Med. 2020;1–5.
19. Detoc M, Bruel S, Frappe P, Botelho-Nevers E, Gagneux-Brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. medRxiv. 2020;1–14.
20. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. 2020;8(April):1–9. doi:10.3389/fpubh.2020.00181
21. Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice (KAP) study. AECS Illum. 2004;IV(1):7–9.
22. Dubé E. Addressing vaccine hesitancy: the crucial role of healthcare providers. Clin Microbiol Infect. 2017;23(5):279–280. doi:10.1016/j.cmi.2016.11.007
23. Mcateer J, Yildirim I, Chahroudi A. The vaccines act: deciphering vaccine hesitancy in the time of COVID-19. Clin Infect Dis. 2020;3–5. doi:10.1093/cid/ciaa433
24. Garrett L. COVID-19 the medium is the message. Lancet. 2020;395(January):1–3. doi:10.1016/S0140-6736(20)30600-0
25. Dubey S, Biswas P, Ghosh R, et al. Psychosocial impact of COVID-19. Diabetes Metab Syndr. 2020;14(January):779–788. doi:10.1007/s00134-020-05991-x.Bizzarro
26. Felice C, Luca G, Tanna D, Zanus G, Grossi U. Impact of COVID-19 outbreak on healthcare workers in italy: results from a national E-survey. J Community Health. 2020;45(0123456789):675–683. doi:10.1007/s10900-020-00845-5
27. Chirico F, Nucera G, Magnavita N. COVID-19: protecting healthcare workers is a priority. Infect Control Hosp Epidemiol. 2020;1:2020. doi:10.1017/ice.2020.148
28. Pulcini C, Massin S, Launay O, Verger P. Factors associated with vaccination for hepatitis B, pertussis, seasonal and pandemic influenza among French general practitioners: a 2010 survey. Vaccine. 2013;31(37):3943–3949. doi:10.1016/j.vaccine.2013.06.039
29. Jones M, Cook R. Intent to receive an HPV vaccine among university men and women and implications for vaccine administration. J Am Coll Health. 2008;57(1):23–32. doi:10.3200/JACH.57.1.23-32
30. Zhi ZLXBXZ. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Chin J Epidemiol. 2020;41(2):145–151. doi:10.3760/cma.j.issn.0254-6450.2020.02.003
31. Denis M, Vandeweerd V, Verbeke R, Laudisoit A, Wynants L. COVIPENDIUM: Information Available to Support the Development of Medical Countermeasures and Interventions Against COVID-19. 2020.
32. Biswas R. Are men more vulnerable to covid-19 as compared to women? Biomed J Sci Tech Res. 2020;27(2). doi:10.26717/BJSTR.2020.27.004481
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.