")
Back to Journals » Patient Preference and Adherence » Volume 11
Acceptability and efficacy of interactive short message service intervention in improving HIV medication adherence in Chinese antiretroviral treatment-naïve individuals
Authors Ruan Y, Xiao X, Chen J, Li X, Williams AB, Wang H
Received 10 September 2016
Accepted for publication 4 November 2016
Published 10 February 2017 Volume 2017:11 Pages 221—228
DOI https://doi.org/10.2147/PPA.S120003
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Ye Ruan,1 Xueling Xiao,2 Jia Chen,2 Xianhong Li,2 Ann Bartley Williams,3 Honghong Wang2
1Nursing Department, Second Xiangya Hospital, 2Xiangya School of Nursing, Central South University, Changsha, Hunan, People’s Republic of China; 3School of Nursing, Yale University, West Haven, CT, USA
Aim: The aim of this study was to examine the acceptability and efficacy of interactive short message service (SMS) in improving medication adherence in antiretroviral treatment (ART)-naïve individuals living with HIV/AIDS in Hengyang, Hunan, China.
Background: SMS via mobile phone has emerged as a potential tool for improving ART adherence. However, most studies used SMS only as a medication reminder, with few studies exploring the effect of comprehensive, interactive SMS.
Patients and methods: In a randomized controlled trial, 100 HIV-positive patients on ART for <3 months were randomized into control or intervention arm. Participants in the control group received routine standard instruction for ART medication in the HIV clinics, while the intervention group received 6 months of an SMS intervention in addition to the standard care. A total of 124 text messages within 6 modules were edited, preinstalled, and sent to participants according to personalized schedules. Knowledge (of HIV and HIV medications), self-reported antiretroviral adherence (Visual Analog Scale [VAS] and Community Programs for Clinical Research on AIDS [CPCRA] Antiretroviral Medication Self-Report), and CD4 count were assessed at baseline and immediate post-intervention. Intervention participants were interviewed after completion of the study about their satisfaction with and acceptability of the SMS intervention.
Results: Baseline assessments were comparable between arms. Repeated-measures analysis showed that both HIV-related and ART medication knowledge of the intervention group showed better improvement over time than those of the control group after the intervention (P<0.0001). For the adherence measures, compared with the control group, participants in the intervention group had significantly higher VAS mean score (Z=2.735, P=0.006) and lower suboptimal adherence rate (Z=2.208, P=0.027) at the end of the study. The intervention had no effect on CD4 cell count. Almost all (96%) intervention participants reported satisfaction or high satisfaction with the SMS intervention, with 74% desiring to continue to receive the SMS intervention. The preferred frequency of messages was 1–2 messages per week.
Conclusion: An interactive SMS intervention with comprehensive content shows promising efficacy in promoting medication adherence in ART-naïve individuals. Future work might further refine its ability to optimally tailor the intervention for individual preferences.
Keywords: HIV, short message service, antiretroviral treatment, adherence, China
Introduction
Antiretroviral treatment (ART) was initiated in 1996 and has contributed greatly to the reduction in morbidity and mortality among people living with HIV (PLWH).1 The annual number of people dying from AIDS-related causes worldwide has dropped from 2.2 million in 2005 to 1.6 million in 2012, due to the well-developed and rapid scale-up of ART programs. The availability of and access to ART have turned the HIV infection from a fatal disease into a chronic and manageable one. ART also plays an important role in HIV prevention under the strategy of treatment-as-prevention.2 However, medication adherence is one of the most important determinants for treatment effectiveness. PLWH may need to maintain as much as 90% adherence to suppress the HIV replication.3 Nonadherence and incomplete adherence are of concern because suboptimal adherence to ART leads to failure of viral suppression, occurrence of resistant viral strains, advanced disease progress, and much higher health costs.4,5 Previous studies showed that the nonadherence rate to ART ranged from 20% to 40%.6–8
China has Asia’s second-largest HIV epidemic with an estimated 0.78 million of PLWH.9 According to China Center for Disease Prevention and Control, the accumulative reported cases of HIV/AIDS were 574,755 by the end of 2015.10 Although HIV prevalence in the general population is low, transmission among men having sex with men is increasing rapidly. A national program to provide free ART was launched in 2003, under which 448,196 PLWH are currently receiving ART, 50,124 (11.2%) on second-line ART and the rest on first-line regimens.10 However, the HIV epidemic continues to advance, with the number of AIDS cases still rising. By the end of 2014, among the 501,000 survived PLWH, 205,000 progressed to AIDS,11 suggesting a great need for ART interventions to improve the management of HIV infection.
Mobile telephones have become a new tool in chronic disease management, including HIV infection.12,13 Interventions associated with information technology may include reminders for patients and the promotion of information transmission.14 Short message service (SMS) is a frequently used communication tool that has become a widespread medium for the delivery of behavioral interventions.15 A systematic review showed that the majority of published text-message interventions were effective in improving medication adherence to ART.16 SMS offers many advantages, such as low cost, easy and wide coverage, and the potential for individualized instant delivery. Surveys showed that >80% of the PLWH studied believed that SMS aided them in treatment adherence and indicated their willingness to receive SMS.17,18
SMS-based interventions have been tested in many countries, but only one study using real-time text-message reminders to improve adherence to ART has been conducted in China,19 which showed only the reminding function of SMS. Past studies mainly used SMS as a reminder for medication taking,19,20 and studies on more comprehensive functionality of SMS are lacking. In addition, information on the optimal content, frequency, and scheduling of SMS messages is limited.
In this study, we aimed to investigate the acceptability and efficacy of an SMS intervention via mobile phones in improving ART adherence in PLWH in China. Our goal was to create a more comprehensive support system based on our prior work in China.
Conceptual framework for the study
The conceptual model in this study was based on the Starks et al’s21 3-step adherence model that was formulated for the intervention program on medication adherence and within the context of tight-knit families and to address the environment of societal stigma (Figure 1). This model consisted of 3 steps to medication adherence, which is defined as the actual ingestion of the correct dose of ART at the appropriate time. First, patients ask for correct instructions to take their medications (a cognitive component). Second, patients have to be motivated to take the medications (a psychological component). Third, patients need to have the medication available and remember to take the medication at the appropriate time, by either an internal cue (they remember) or an external cue such as a prompt from a family member or an alarm (social/mechanical component). The current study addressed these 3 components via interactive and comprehensive SMS intervention.
 | Figure 1 Three steps to medication adherence. |
Patients and methods
Design, participants, and setting
We conducted a randomized controlled trial between March 2013 and March 2014, recruiting patients from an HIV clinic in Hengyang city, a major HIV clinic in Hunan Province, China. This clinic currently manages 3,900 patients, of whom 2,800 are on ART. Eligible individuals 1) were at least 18 years old; 2) had confirmed an HIV diagnosis; 3) were on ART for no more than 3 months; 4) were able to speak, understand, and read Mandarin; and 5) had their own mobile phone or regular access to a mobile phone. The study was approved by the institutional review board Committee of Xiangya School of Nursing, Central South University.
Participants who provided written informed consent were randomized into a control or intervention group. Patients in the control group received regular health education in the clinic, including informational pamphlets, psychological support, and personalized health education from nurses and physicians in the HIV clinic. Participants in the intervention group received the same usual care as the control group plus SMS for 6 months. Data were collected at the baseline (pretest) and at the end of the 6-month study (posttest).
SMS intervention
The SMS intervention was designed and planned in consultation with investigators, clinic staff, and patients and families regarding the content, frequency, and scheduling of the text messages. In total, 6 message modules and 124 text messages were edited and preinstalled, including introduction and holiday and weekend greetings (14 messages), medication reminders and skills for good adherence (47 messages), HIV/AIDS-related and medication knowledge (49 messages), humor jokes (14 messages), and motivation and encouragement (14 messages). The SMS intervention aimed to increase knowledge, enhance medication adherence, provide emotional support, and solve problems. All messages were <70 Chinese characters and did not specify HIV or AIDS to maintain the confidentiality of receivers’ HIV status (“virus” and “chronic illness” were used instead).
Scheduling of messages was determined by the interventionists and participants at the baseline visit. For the first 3 months of the intervention, 5 preinstalled text messages were sent to the participants every week, namely every Monday, Wednesday, Friday, and weekends, while for the last 3 months of the intervention, 3 text messages were sent to the participants every week, namely every Monday, Wednesday, and Saturday. Medication reminders were sent to the participants about half an hour before their medication time, while other messages were sent at 8 pm.
We adopted an interactive approach, with all text messages sent through the working phones of interventionists rather than the SMS platform, allowing the participants to reply to the text messages when needed. The interventionists chose multiple recipients (bulk messages) to improve the efficiency. The participants were instructed that they could text back any questions or comments to the interventionists.
Measures
We collected “demographic information” (ie, age, gender, education level, housing condition, family yearly income, and marital status) as well as “disease-specific data” (ie, time since HIV diagnosis, time on ART, infection routes, and ART regimen).
We assessed “HIV-related knowledge” with a questionnaire originally developed in Mandarin and used in Chinese workers.22 Its 10 items query the nature of the disease, transmission routes, prevention measures, etc. Responses to the questions were “yes”, “no”, and “not clear”, with correct answers scoring 2 points and wrong answers scoring 0 to generate a total score from 0 to 20. “ART medication knowledge” was assessed with a 13-item measure originally developed and tested in China by Li23 and included items on ART functions, methods and requirements of medication taking, and management of side effects. The answers to each item were right, wrong, and not clear. Correct answers scored 1 point and other answers scored 0, with a total score range of 0 to 13.
“ART adherence” was measured using 2 approaches. The Community Programs for Clinical Research on AIDS (CPCRA) Adherence Self-Report Questionnaire was used to determine the percentage of doses taken in the 7 days before the interview for each ARV prescribed. Participants were asked to select 1 of 5 possible responses according to the original measure: 100%, 80%, 50%, 30%, and 0%. A Visual Analog Scale (VAS) was also used to measure the medication adherence, with which participants reported their adherence over the past 30 days on a 100-point scale (with no increments indicated): 0 for taking no medication and 100 for taking all of the prescribed medications. We measured the distance of the tick mark they used to indicate adherence and created a percentile score (a ratio-level variable). Responses were dichotomized for the VAS, with the threshold for optimal adherence set at 90% and above.24–26 Both measurements of ARV adherence have been used successfully by the authors in similar populations.27
The acceptability of the SMS intervention was assessed in semi-structured individual interviews with participants at the conclusion of the study. We assessed preferred message types, preferred time and frequency of receiving messages, and quality of messages. With 1 item, participants rated their satisfaction toward the message intervention as 1 (highly unsatisfied) to 4 (highly satisfied). In addition, all text-message communication between the interventionists and the participants was recorded in the study log. In addition, participants’ responses to messages were also recorded to calculate the response rate.
Data analysis
Independent-sample t-tests, χ2-tests, and Mann–Whitney U tests were used to compare the 2 study groups at the baseline. We used repeated-measures analysis of variance to compare the total score of medication knowledge in the 2 groups. Mann–Whitney U tests were used to compare the ART adherence. Independent-sample t-tests were used to compare the differences in CD4 cell counts between the 2 groups. The significance level used in the study was 0.05.
Results
Participant characteristics
From July 2013 to September 2013, 283 PLWH who came to the HIV clinic for medical service were screened: 180 PLWH did not meet the criteria and 33 participants declined participation (Figure 2). Totally, 100 PLWH completed the baseline questionnaire: 50 in the intervention group and 50 in the control group. During the 6-month follow-up, 2 participants died and 1 withdrew from the study in the intervention group, while 1 died and 2 lost to follow-up in the control group, with 94 participants completing the study.
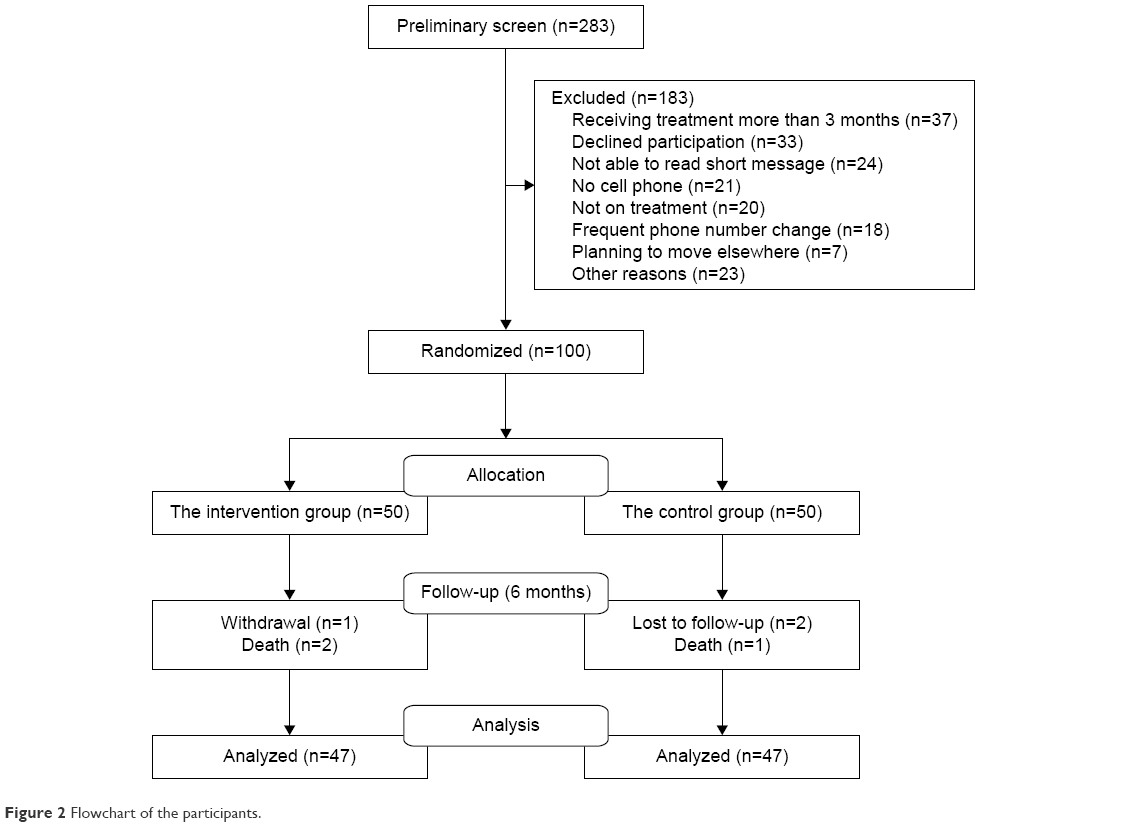 | Figure 2 Flowchart of the participants. |
As shown in Table 1, there were no significant differences in any demographic or disease-related variable between groups at the baseline. Overall, participants were aged 40.3 years; 41% female and 54% reporting heterosexual transmission.
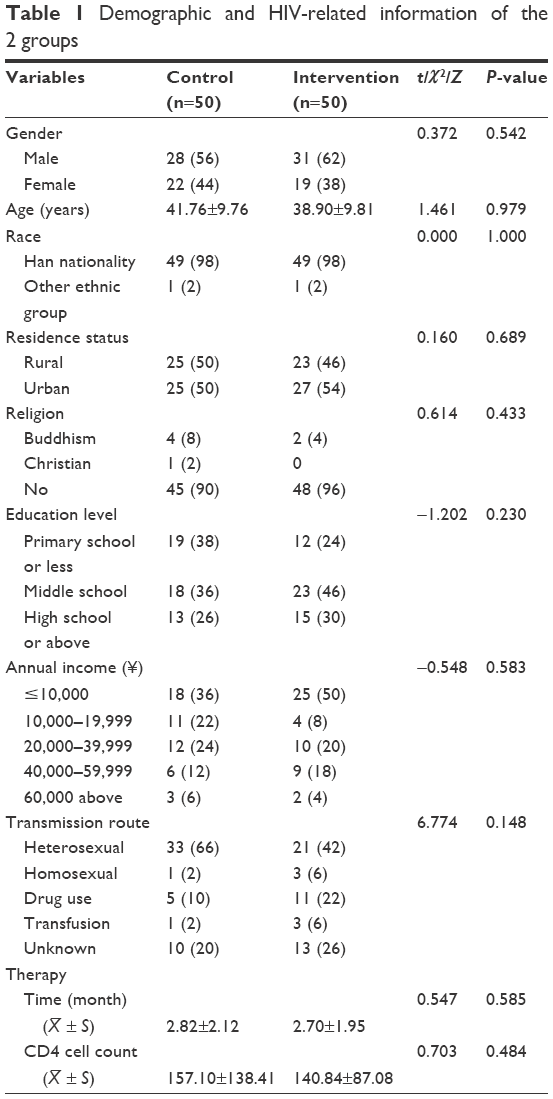 | Table 1 Demographic and HIV-related information of the 2 groups |
Intervention outcomes
Compared with the control group, the mean scores for both HIV-related and ART medication knowledge of the SMS intervention group demonstrated a better improvement over time than those of the control group after the intervention (P<0.0001). The effect size of SMS intervention over time for HIV-related knowledge and medication knowledge was 0.35 and 0.48, respectively (Table 2).
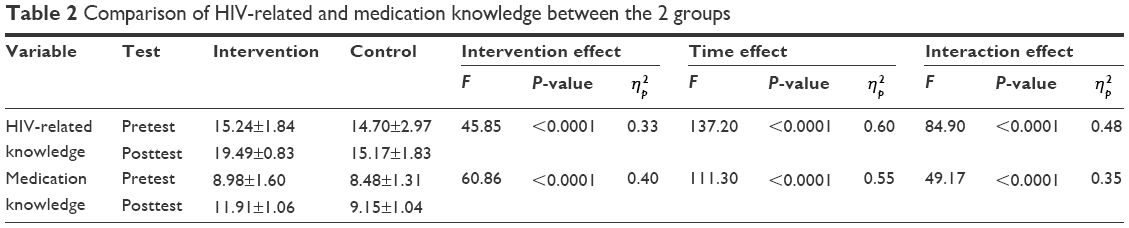 | Table 2 Comparison of HIV-related and medication knowledge between the 2 groups |
The participants reported VAS score of 98.72% in the SMS group at the end of the study, significantly higher than that in the control group (93.11%; P=0.006). Similar effect on CPCRA adherence was noticed. With no difference at the baseline, the percentage of people with suboptimal adherence in the control group (27%) was significantly higher than that in the intervention group (10.7%) in the posttest (P=0.027; Table 3).
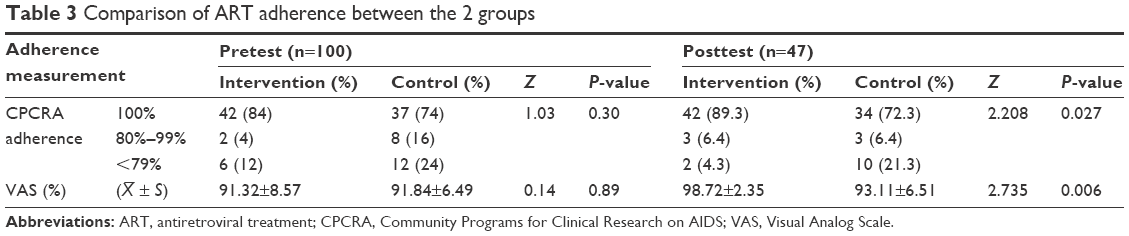 | Table 3 Comparison of ART adherence between the 2 groups |
CD4 cell counts of this sample showed a normal distribution according to the Kolmogorov–Smirnov tests. t-Test was used to analyze the treatment outcomes, and no statistical differences were found in either pretests or posttests between the 2 groups (P=0.623; Table 4).
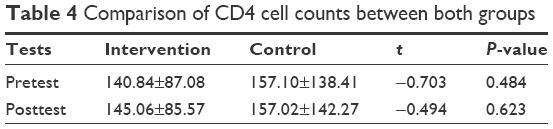 | Table 4 Comparison of CD4 cell counts between both groups |
Use and acceptability of SMS
The majority of the participants replied to the SMS, although response to each text message is not required. One patient never replied, with a response rate of 97.87% in total. Over half of the participants responded to 30%–50% of the messages. In average, almost every participant contacted the interventionist and replied 37 times. The topics of replying messages included asking whether they could stop medication if the CD4 cell count rose; how long they could live with AIDS; whether HIV could be transmitted through coughing, sneezing, or mosquito bites; how to deal with delayed medications; expressing appreciation for encouragement; and a good mood after receiving a humor or a joke.
Most participants (96%) in the intervention arm reported satisfaction or high satisfaction with the SMS intervention. Two participants (4%) were dissatisfied because they disliked the frequency of messages: one complained that the message bothered him too often, and the other said that he hoped to receive messages every day. Unexpectedly, 35 participants (74%) responded that they would like to continue to receive the SMS, indicating a good acceptability of the SMS.
Participants generally preferred disease and therapy-related knowledge topics, followed by greetings and jokes, emotional support, and reminders. The majority of participants preferred to receive 1–2 messages each week, followed by 3–5 messages per week (Table 5).
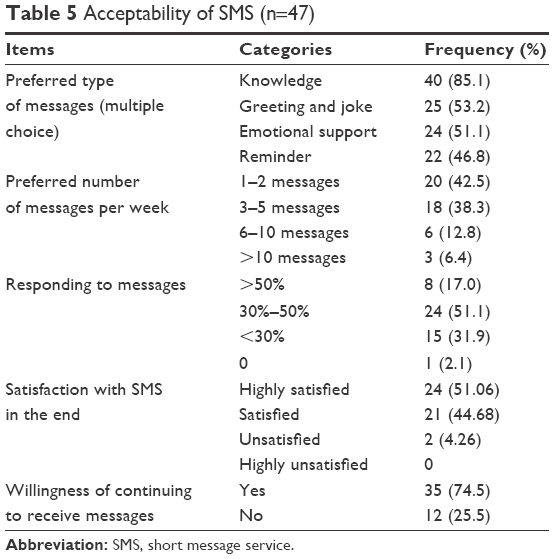 | Table 5 Acceptability of SMS (n=47) |
Discussion
This study shows that SMS intervention can improve HIV/AIDS-related knowledge and ART adherence. People who receive SMS are more likely to get higher scores and improve their ART adherence than patients who get the standard care alone.
SMS intervention can improve the level of HIV-related and ART management knowledge in ART-naïve individuals. Previous studies showed that patients with HIV/AIDS knew little about ART management, and only 57% of the prescriptions were correctly understood by PLWH.28,29 Although in the HIV clinic, PLWH receive routine teaching sessions for ART preparation and some pamphlets, at the initial stage of ART, SMS could regularly send drug use instructions to patients, and timely answer to their questions effectively improves the awareness of drug use.
Interactive text message showed promising effect in improving ART adherence. SMS intervention has shown a potential benefit in improving or keeping ART adherence in different areas.14 First, SMS could be used as a medication reminder to improve ART adherence confirmed by previous studies.12,19,20 Second, SMS intervention could improve the level of HIV-related knowledge and ART knowledge in ART-naïve individuals, which is associated with optimal medication adherence. Third, the interactive text message offered the ART-naïve individuals a conduit for timely communication with health care providers as to informational, emotional, and technical supports to overcome the multitude of barriers they faced at the start of ART. Miller et al29 claimed that SMS was used not only to remind or send information to PLWH but also, as a consistent and convenient way, to access emotional support from health care providers.
As to the frequency of message sending, the participants preferred 1–2 messages each week, followed by 3–5 messages each week. Since our participants were ART-naïve, we sent 5 messages in the first 3 months (2 pieces of knowledge and 3 reminder messages per week). Although our findings did not show what frequency had better effect, from our experiences and feedback from the participants we found daily message was not preferable. One of our participants complained of too much messages. Pop-Eleches et al’s study12 showed that weekly messages were more effective in improving the adherence than daily reminders. A survey also showed that participants favored the weekly message, no more and no less.30 Daily messages might be considered intrusive, might lead to habituation, and possibly decrease the responses to repeated stimuli. We also assessed the participants’ favorite message types. The participants preferred SMS regarding the intervention not only as a reminder but also as a useful source of information on HIV infection and medication management. Similar findings were shown in Georgette et al’s study,30 in which the participants reported a desire to have more varieties in the message contents and most of them would like to read more information about HIV medication in the messages.
Feedback from the participants of this study also demonstrated a good acceptability to interactive SMS. Most participants in the intervention group reported the help of text messages in taking their medication, satisfaction with the SMS education, and willingness to continue to receive SMS messages in the future. They used the interactive SMS as a tool for seeking information and consultation from health care providers. SMS intervention offers the participants a simple way to contact health care providers.17 It requires basic text-messaging skills and low cost to participate. A high response rate from this sample also showed the good involvement of the participants. This study, along with previous evidences,14,31 suggests that simple SMS intervention may be an important strategy to sustaining optimal ART responses, especially in the resource-limited settings.
We failed to find that the SMS had a significant impact on the increase in CD4 cell counts in the 6-month follow-up, which was not consistent with previous studies stating that SMS could improve ART adherence and the biological outcomes of ART, including suppressed viral load and increased CD4 cell counts.14,32 Mannheimer et al33 also claimed that the higher the ART adherence, the faster the CD4 cell growth. This study did not last long enough for us to observe the change in CD4 cell counts. In addition, Townsend et al34 showed that when ART adherence was >70%, with no correlation between the ART adherence and the increase in CD4 cell counts, it might partially explain the significant difference in CD4 cell count increase. We used CD4 cell count only as the biological outcome because patients could access only the test of CD4 cell counts every 6 months since viral load test was not routinely accessible. This limits the sensitivity for evaluating the biological outcome of SMS intervention, because viral load test is a more sensitive indicator for ART effectiveness.
Confidentiality is a great concern for SMS participants. Designing ethically appropriate text messages should be the focus to avoid unwanted disclosure of HIV status and protect the participants’ privacy. In our study, more than half of the participants were concerned about words such as AIDS or HIV that might appear in the text messages; some participants preferred to use “ABC” or “123” to replace or code these terms. Due to the customary use of mobile phones by more than 1 individual in some settings, cell phone messages need to continue to consider confidentiality issues. SMS involves risks and should not include any HIV-related terms in the messages.35
There are several limitations in this study. The relatively small sample size might weaken the power of the study. Participants of the 2 arms were recruited from the same HIV clinic and might share information, which might result in contamination. Furthermore, 6-month follow-up is not long enough to determine the effect of SMS intervention. A longer follow-up is preferred.
Conclusion
Interactive SMS intervention has a promised acceptability in ART-naïve individuals in China. It demonstrates the preliminary efficacy in improving HIV-related and medication knowledge and adherence to ART in PLWH. However, it fails to show significant effect on the increase in CD4 cell counts during the 6-month follow-up. Findings of this study suggest SMS program might be considered a key component in comprehensive ART adherence support. Ideal SMS program would be automated, easily customized and bidirectional communication with medical providers while maintaining confidentiality. Future studies should focus on exploring the integration of SMS into clinical settings. With the expansion of electronic medical records in clinical settings, integration of SMS within existing hospital record systems should be a priority of future research.
Acknowledgments
The authors would like to acknowledge all the physicians and nurses in the HIV clinic of the Third People’s Hospital of Hengyang, for their valuable input, designing the text messages, and their cooperation in the recruitment. The authors appreciate the active involvement of all the participants in this study. We also acknowledge Professor Jane M Simoni from the University of Washington, for helping us revise the manuscript and giving us permission to use the adherence model.
Disclosure
The authors report no conflicts of interest in this work.
References
Reynolds N. Adherence to antiretroviral therapies: state of the science. Curr HIV Res. 2004;2(3):207–214. | ||
Padian NS, McCoy SI, Karim SSA, et al. HIV prevention transformed: the new prevention research agenda. Lancet. 2011;378(9787):269–278. | ||
Rueda S, Park-Wyllie L, Bayoumi A, et al. Patient support and education for promoting adherence to highly active antiretroviral therapy for HIV/AIDS (Review). Cochrane Database Syst Rev. 2006;19(3):CD001442. | ||
Bangsberg DR, Acosta EP, Gupta R, et al. Adherence-resistance relationships for protease and non-nucleoside reverse transcriptase inhibitors explained by virological fitness. AIDS. 2006;20(2):223–231. | ||
Paterson D, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. | ||
Achappa B, Madi D, Bhaskaran U, Ramapuram J, Rao S, Mahalingam S. Adherence to antiretroviral therapy among people living with HIV. N Am J Med Sci. 2013;5(3):220–223. | ||
Hansana V, Sanchaisuriya P, Durham J, et al. Adherence to antiretroviral therapy (ART) among people living with HIV (PLHIV): a cross-sectional survey to measure in Lao PDR. BMC Public Health. 2013;13:617. | ||
Yu R, Sheng Y, Zhu S. The survey of antiretroviral adherence and related factors in AIDS patients. Chin J Clin. 2012;6(11):5. | ||
UNAIDS. UNAIDS Report on the Global AIDS Epidemic 2013. Geneva: Joint United Nations Programme on HIV/AIDS; 2013. | ||
China CDC. Update on the AIDS/STD epidemic in China and main response in control and prevention in October, 2015. Chin J AIDS STD. 2015;21(12):1003. | ||
The National Health and Family Planning Commission of the PRC [webpage on the Internet]. 2015 Update on China AIDS Prevention and Control; 2015. Available from: http://www.unaids.org/en/regionscountries/countries/china. Accessed August 6, 2016. | ||
Pop-Eleches C, Thirumurthy H, Habyarimana JP, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(6):825–834. | ||
Shet A, Arumugam K, Rodrigues R, et al. Designing a mobile phone-based intervention to promote adherence to antiretroviral therapy in South India. AIDS Behav. 2010;14(3):716–720. | ||
Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–1845. | ||
Suffoletto B. Text message behavioral interventions: from here to where? Curr Opin Psychol. 2016;9:16–21. | ||
Hall AK, Cole-Lewis H, Bernhardt JM. Mobile text messaging for health: a systematic review of reviews. Ann Rev Public Health. 2015;36:393–415. | ||
da Costa TM, Barbosa BJP, Gomes e Costa DA, et al. Results of a randomized controlled trial to assess the effects of a mobile SMS-based intervention on treatment adherence in HIV/AIDS-infected Brazilian women and impressions and satisfaction with respect to incoming messages. Int J Med Inform. 2012;81(4):257–269. | ||
Skinner D, Rivette U, Bloomberg C. Evaluation of use of cellphones to aid compliance with drug therapy for HIV patients. AIDS Care. 2007;19(5):605–607. | ||
Sabin LL, Bachman DeSilva M, Gill CJ, et al. Improving adherence to antiretroviral therapy with triggered real-time text message reminders: the China adherence through technology study. J Acquir Immune Defic Syndr. 2015;69(5):551–559. | ||
Kalichman SC, Kalichman MO, Cherry C, Eaton LA, Cruess D, Schinazi RF. Randomized factorial trial of phone-delivered support counseling and daily text message reminders for HIV treatment adherence. J Acquir Immune Defic Syndr. 2016;73(1):47–54. | ||
Starks H, Simoni J, Zhao H, et al. Conceptualizing antiretroviral adherence in Beijing, China. AIDS Care. 2008;20(6):607–614. | ||
Cha M. Application of Mobile Phone Text Messages in HIV Prevention Education in Construction Workers. Kunming: Kunming Medical College; 2011. | ||
Li L. Dialogue Education in Improving Adherence to Antiviral Treatment in HIV/AIDS Patients. Changsha: School of Nursing, Central South University; 2012. | ||
Kobin AB, Sheth NU. Levels of adherence required for virologic suppression among newer antiretroviral medications. Ann Pharmacother. 2011;45(3):372–379. | ||
Giordano TP, Guzman D, Clark R, Charlebois E, Bangsberg D. Measuring adherence to antiretroviral therapy in a diverse population using a visual analogue scale. HIV Clin Trials. 2004;5(2):74–79. | ||
Kobin A, NU S. Levels of adherence required for virologic suppression among newer antiretroviral medications. Ann Pharmacother. 2011;45(3):372–379. | ||
Wang H, He G, Li X, et al. Self-reported adherence to antiretroviral treatment among HIV-infected people in Central China. AIDS Patient Care STDS. 2008;22(1):71–80. | ||
Chau I, Korb-Savoldelli V, Trinquart L, et al. Knowledge of oral drug treatment in immunocompromised patients on hospital discharge. Swiss Med Wkly. 2011;141:w13204. | ||
Miller LG, Liu H, Hays RD, et al. Knowledge of antiretroviral regimen dosing and adherence: a longitudinal study. Clin Infect Dis. 2003;36(4):514–518. | ||
Georgette N, Siedner MJ, Zanoni B, et al. The acceptability and perceived usefulness of a weekly clinical SMS program to promote HIV antiretroviral medication adherence in KwaZulu-Natal, South Africa. AIDS Behav. 2016;20(11):2629–2638. | ||
Lippman SA, Shade SB, Sumitani J, et al. Evaluation of short message service and peer navigation to improve engagement in HIV care in South Africa: study protocol for a three-arm cluster randomized controlled trial. Trials. 2016;17:68. | ||
Finitsis DJ, Pellowski JA, Johnson BT. Text message intervention designs to promote adherence to antiretroviral therapy (ART): a meta-analysis of randomized controlled trials. PLoS One. 2014;9(2):1–10. | ||
Mannheimer S, Friedland G, Matts J, Child C, Chesney M. The consistency of adherence to antiretroviral therapy predicts biologic outcomes for human immunodeficiency virus–infected persons in clinical trials. Clin Infect Dis. 2002;34:7. | ||
Townsend ML, Jackson GL, Smith R, Wilson KH. Association between pharmacy medication refill-based adherence rates and CD4 count and viral-load responses: a retrospective analysis in treatment-experienced adults with HIV. Clin Ther. 2007;29(4):711–716. | ||
Pérez GM, Hwang B, Bygrave H, Venables E. Designing text-messaging (SMS) in HIV programs: ethics-framed recommendations from the field. Pan Afr Med J. 2015;21:201. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.