")
Back to Journals » Cancer Management and Research » Volume 12
Acalabrutinib and Its Therapeutic Potential in the Treatment of Chronic Lymphocytic Leukemia: A Short Review on Emerging Data
Received 4 December 2019
Accepted for publication 5 March 2020
Published 19 March 2020 Volume 2020:12 Pages 2079—2085
DOI https://doi.org/10.2147/CMAR.S219570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Krista Isaac,1 Anthony R Mato2
1Division of Hematology and Oncology, University of Virginia Health System, Charlottesville, VA, USA; 2Chronic Lymphocytic Leukemia Program, Memorial Sloan Kettering Cancer Center, New York, NY, USA
Correspondence: Krista Isaac
University of Virginia, PO Box 800716, Charlottesville, VA 22908, USA
Tel +1 215 350 8369
Fax +1 434 243 5956
Email [email protected]
Abstract: Recently, the treatment landscape for chronic lymphocytic leukemia (CLL) has changed dramatically due to the development of drugs targeting proteins in the B cell antigen receptor (BCR) pathway. Acalabrutinib, a second-generation Bruton’s tyrosine kinase (BTK) inhibitor, was recently FDA approved for treatment of treatment naïve and relapsed refractory CLL. Acalabrutinib was designed as a more selective BTK inhibitor as compared to ibrutinib in an attempt to mitigate some of the treatment limiting toxicities seen with ibrutinib such as atrial fibrillation and bleeding. In preclinical studies, acalabrutinib was demonstrated to have efficacy in CLL in both patient blood samples and murine models. A multinational phase 1/2 study demonstrated the efficacy and safety of acalabrutinib monotherapy in treatment naïve, relapsed refractory and ibrutinib-intolerant CLL patients. Subsequent phase 3 studies, ASCEND and ELEVATE-TN, compared acalabrutinib monotherapy or combination acalabrutinib and obinutuzumab to standard of care treatments and demonstrated acalabrutinib’s improved efficacy and tolerability. Currently, a phase 3 study is ongoing to compare acalabrutinib to ibrutinib monotherapy (NCT02477696). In the setting of recent FDA approval, real-world evidence will help to elucidate the optimal use of acalabrutinib in the treatment of CLL.
Keywords: acalabrutinib, BTK inhibitors, CLL, treatment naïve CLL, relapsed refractory CLL, ibrutinib toxicity
Introduction
Chronic lymphocytic leukemia (CLL), the most common adult leukemia, is a clonal neoplasm composed of monomorphic small mature B cells that coexpress CD5 and CD23.1 The landscape of treatment of CLL has changed dramatically in recent years. Drugs targeting proteins in the B cell antigen receptor (BCR) pathway, such as ibrutinib, have demonstrated improvement in progression free and overall survival, including in patients with high-risk disease.2–4 Although these drugs have revolutionized the treatment paradigm in patients with CLL, treatment exposure and intensity with ibrutinib can be limited due to the side-effect profile and treatment-related toxicities.5,6 Acalabrutinib, a second generation and more selective Bruton’s tyrosine kinase (BTK) inhibitor, was developed to maximize efficacy while minimizing ibrutinib-associated adverse events hypothesized to be secondary to ibrutinib’s off-target effects.7–9 This review will summarize the development, pre-clinical evaluation, and key clinical trials that have demonstrated acalabrutinib’s efficacy and toxicity profile in CLL.
Role of Bruton’s Tyrosine Kinase Inhibitors in CLL
BCR signaling is integral in the proliferation and survival of B lymphocytes. Several downstream protein kinases such as BTK are critical in the BCR signaling cascade.10–12 Inactivating mutations in the BTK gene result in X-linked agammaglobulinemia.10,13,14 Patients with X-linked agammaglobulinemia have severe reduction in B cells with hypogammaglobulinemia, highlighting the importance of BTK on normal B cell development.13,15 BTK is essential for activation of several pathways that promote lymphocyte survival including Akt, extracellular signal-regular kinase, and NF-κb pathways.10,12,14,16 BTK also has an important role in chemokine secretion, specifically CCL3 and CCL4, and adhesion of B cells, through activation of phospholipase C-γ2.7,10,14 Due to the influence of BTK on cell proliferation and survival, it is an attractive target for inhibition to treat diseases such as CLL and other B-cell lymphomas.
Several BTK inhibitors are currently commercially available or in development for treatment of CLL. Three BTK inhibitors are currently approved by the FDA: ibrutinib, acalabrutinib, and zanubrutinib. Ibrutinib is a first generation, irreversible BTK inhibitor that was approved in 2013.2,17,18 Ibrutinib has been studied extensively for treatment of CLL and is currently standard of care for treatment of treatment naïve and relapsed refractory CLL.2,17,18 Acalabrutinib, a second generation, irreversible BTK inhibitor, was developed as a selective BTK inhibitor to avoid the off-target side effects seen ibrutinib.7–9 Zanubrutinib, a next-generation, irreversible BTK inhibitor, was developed as a selective BTK inhibitor and has received approval for treatment of relapsed refractory mantle cell lymphoma.19 Studies are ongoing in evaluating the drug’s safety and efficacy in CLL.20
Development of Acalabrutinib
Acalabrutinib, formerly known as ACP-196, is an orally administered second generation, small-molecule irreversible inhibitor of BTK that covalently binds to Cys481.7 Acalabrutinib was developed as a selective BTK inhibitor when compared to ibrutinib with the goal of achieving similar therapeutic outcomes in patients with CLL without the off-target effects on other kinases such as TEC, EGFR, and ITK.7–9 Several pre-clinical studies have demonstrated the efficacy of acalabrutinib inhibition of BTK is similar to that seen with ibrutinib. These findings led to a phase 1/2 study to evaluate the efficacy and side-effect profile of acalabrutinib in CLL. At 42 months of follow-up, the side-effect profile appeared manageable (headache, diarrhea and upper respiratory tract infections) and there were few discontinuations due to adverse events.21 Subsequent phase 3 trials, ELEVATE-TN and ASCEND, led to the FDA approval of acalabrutinib for treatment of CLL and SLL.22,23
A treatment dose of 100 mg twice daily was considered the optimal dosage. At this dosing, acalabrutinib was demonstrated to bind to the C481 residue with evidence of complete BTK occupancy (99–100%) 4 hrs after dosing and 97% occupancy at 12 hrs post-dose.7,24 At increased dosing (200 mg BID), the BTK occupancy demonstrated higher interpatient variability (median BTK occupancy of 92% at trough with only 66% of patients >90%).24
Preclinical Studies of Acalabrutinib in CLL
Several preclinical studies demonstrated the efficacy of acalabrutinib on BTK inhibition. When tested on human whole blood, acalabrutinib had equipotent BTK inhibition as compared to ibrutinib.24 Ibrutinib was found to cause increased apoptosis of CLL cells as compared to acalabrutinib, which could be explained by the off-target effects of ibrutinib.25 Acalabrutinib had less of an effect on healthy T cells likely due to its selectivity compared to ibrutinib.25
The anti-tumor effects of acalabrutinib were evaluated in two murine CLL models: a TCL1 adoptive transfer model and a xenografted human CLL model. Acalabrutinib was demonstrated to inhibit BCR signaling and treatment with acalabrutinib was associated with a significant increase in survival compared with untreated mice (median 81 days vs 59 days, p = 0.02).26 Acalabrutinib also caused a significant reduction in proliferating cells and total tumor burden in the spleen.26
Acalabrutinib’s interaction with anti-CD20 monoclonal antibodies has also been evaluated. Ibrutinib may interfere with several of the mechanisms of action of the anti-CD20 antibodies specifically inhibiting antibody-dependent cellular cytotoxicity and phagocytosis which may decrease their anti-tumor effect.27 Golay et al evaluated the effects of acalabrutinib on antibody-dependent cellular cytotoxicity and phagocytosis and found that it did not interfere with these processes, likely due to the minimal off-target effects of acalabrutinib.27 Although the combination of acalabrutinib with an anti-CD20 monoclonal antibody has not been study in an in vivo model, several phase 2 and phase 3 studies are ongoing or have been completed that demonstrate the efficacy of acalabrutinib in combination with an anti-CD20 monoclonal antibody.23,28–30
Other acalabrutinib combinations have been studied in both in vitro and in vivo models. Acalabrutinib was combined with a PI3Kdelta inhibitor (ACP-319) in a murine CLL model and demonstrated greater reduction in tumor proliferation, NF-KB signaling and expression of BCL-xL and MCL-1 as compared to monotherapy.31 Blood samples obtained from CLL patients not enrolled in a clinical trial were treated with acalabrutinib and venetoclax.32 This combination was demonstrated to have increased apoptosis when compared to either drug alone, suggesting a synergistic relationship similar to that seen with ibrutinib and venetoclax.32 A subsequent in vivo experiment demonstrated prolonged survival in mice treated with both acalabrutinib and venetoclax as compared to either drug alone.32
Acalabrutinib Monotherapy
The first trial evaluating acalabrutinib in CLL, ACE-CL-001, was initially published by Byrd et al in 2016.7 This was a phase 1/2, multicenter, multinational clinical trial conducted to assess whether selective targeting of BTK by acalabrutinib would be effective without the ibrutinib-related toxicities that led to ibrutinib discontinuation. Patients were eligible for the trial if they had a diagnosis of relapsed CLL or small lymphocytic leukemia (SLL), a need for treatment, and had received at least one prior therapy for CLL or were treatment naïve (did not want to receive chemoimmunotherapy or had a comorbidity that precluded chemoimmunotherapy). The study was designed with an initial dose escalation to determine the maximum tolerated dose, pharmacodynamics and pharmacokinetics. A subsequent dose expansion was completed to evaluate the overall response rate, progression-free survival and long-term side-effect profile. The dose chosen for the expansion phase was 100 mg twice daily. Patients enrolled in this study were analyzed in several cohorts including relapsed, treatment naïve, and ibrutinib-intolerant.
In total, 134 patients were treated in the relapsed cohort; 99 patients were treated in the treatment-naïve cohort; 33 patients were treated in the ibrutinib-intolerant cohort. The patient characteristics were similar between the cohorts. The median age of the three cohorts was 66 years old (range, 42–85), 64 years old (range, 33–85) and 64 years old (range, 50–82), respectively. More than half of patients in each of the cohorts had unmutated immunoglobulin variable-region heavy-chain gene (IGVH; 73% [n = 81] in relapsed, 62% [n = 57] in treatment-naïve, 81% [n = 25] in ibrutinib intolerant). Fewer patients in the treatment naïve cohort (10%, n = 9) had chromosome 17p13.1 deletion (del17p) as compared to the relapsed cohort (23%, n = 27) and ibrutinib intolerant cohort (38%, n = 12). Patients in the relapsed cohort had a median of two prior therapies (range, 1–13); patients in the ibrutinib intolerant cohort were heavily pretreated with a median of 4 prior therapies (range, 2–13).
The overall response rates (ORR) in the relapsed cohort and treatment naïve cohorts were similar. The ORR in the relapsed cohort was 94% (complete response in 4%, partial response in 84%, and partial response with lymphocytosis in 6%) and the ORR in the treatment naïve cohort was 95% (complete response in 32% [n = 6], partial response in 63% [n = 12]). Patients in the ibrutinib intolerant group had an ORR of 76% (complete response [n = 1], partial response [n = 19], and partial response with lymphocytosis [n = 5]); four patients (12%) in this cohort have discontinued therapy due to progressive disease (Richter transformation in 2 patients). In cross-trial comparison with similar follow up, when compared to ibrutinib monotherapy the overall response rates with acalabrutinib in the relapsed and treatment naïve cohorts appeared to be higher. Relapsed patients treated with ibrutinib had an ORR of 90% (complete response in 7% [n = 7], partial response in 80% [n = 81] and PR-l in 3% [n = 3]).3 Treatment naïve patients treated with ibrutinib monotherapy had an ORR of 86% (complete response in 4%, complete response with lymphoid nodules in the bone marrow in 1%, partial response in 77%, partial response with lymphocytosis in 4%).2
Adverse events were similar for acalabrutinib in patients treated in the front line, relapsed and ibrutinib intolerant settings. Acalabrutinib was overall well-tolerated and most adverse events were grade 1 or 2. The most common adverse events included headache (46% in relapsed, 44% in treatment naïve, 39% in ibrutinib intolerant), diarrhea (52% in relapsed, 47% in treatment naïve, 58% in ibrutinib intolerant), and upper respiratory tract infection (36% in relapsed, 33% in treatment naive, 24% in ibrutinib intolerant). Grade 3 or greater adverse events were infrequent and included neutropenia (14% in relapsed, 7% in treatment naive, 12% in ibrutinib intolerant), pneumonia (11% in relapsed, 4% in treatment naive, 6% in ibrutinib intolerant), and hypertension (7% in relapsed, 3% in treatment naïve, 6% in ibrutinib intolerant). Atrial fibrillation was infrequent across the three cohorts occurring in 7% in the relapsed cohort, 6% in the treatment naïve cohort, and 6% in the ibrutinib intolerant cohort. Grade 1 or 2 bleeding occurred in all cohorts; rare serious (grade 3 or greater) bleeding was reported in four patients in the relapsed cohort, two patients in the treatment naïve cohort, and one patient in the ibrutinib intolerant cohort.
The side-effect profile seen with acalabrutinib appeared similar to that seen with ibrutinib. Common side effects that were reported with ibrutinib also included diarrhea. The most common grade 3 or higher adverse event was neutropenia, similar to that seen in ACE-CL-001. The rates of atrial fibrillation with ibrutinib were higher than those reported with acalabrutinib. Atrial fibrillation (grade 3 or higher) was reported in 6% of patients treated with ibrutinib compared with 3% of patients treated with acalabrutinib.3 Serious bleeding events (grade 3 or higher) were more common with ibrutinib occurring in 8% of patients as compared to 3% in patients treated with acalabrutinib.3,21
In the first head-to-head comparison of B cell receptor signal transduction antagonists, acalabrutinib monotherapy has been compared to idelalisib plus rituximab or bendamustine and rituximab in the phase 3 ASCEND trial.22 Patients were eligible for this trial if they had relapsed refractory CLL. A total of 310 patients were randomized to receive acalabrutinib (n = 155) or idelalisib plus rituximab or bendamustine and rituximab (n = 155). The median age was 67 years old (range, 32–90). Sixteen percent had del17p; 42% had Rai stage III/IV. Discontinuation due to adverse events was highest in the idelalisib plus rituximab group (49%) versus 11% in acalabrutinib group. The 12-month progression free survival rates were 88% for acalabrutinib and 68% for idelalisib plus rituximab or bendamustine and rituximab. The 12-month overall survival rates were 94% for the acalabrutinib and 91% idelalisib plus rituximab or bendamustine and rituximab groups. Patients were allowed to cross over to acalabrutinib in this study; a total of 23% of patients crossed over. All grade adverse events included headache (22%), neutropenia (19%), diarrhea (18%), anemia (15%) and cough (15%). Grade 3 or higher adverse events included neutropenia (16%), anemia (12%), and pneumonia (5%). This study demonstrated that acalabrutinib had a better safety profile than idelalisib plus rituximab.
Acalabrutinib Combinations
In a recent phase 2 single arm study, the efficacy and safety of triple therapy with acalabrutinib, venetoclax and obinutuzumab was evaluated.28 Patients were sequentially started on acalabrutinib (28 day lead-in), obinutuzumab (2 cycles of AO), and venetoclax (ramp beginning in C4) followed by 3 additional cycles of AVO. Obinutuzumab was continued for 6 months; acalabrutinib and venetoclax were continued through cycle 15. A total of 37 patients were enrolled on this trial with a median age of 63 years old (range, 41–78). Sixty-two percent (n = 23) of patients have unmutated IGVH; 27% (n = 10) had TP53 aberrant disease (either del17p and/or TP53 mutation). The ORR for 24 patients who have completed re-staging at cycle 8 is 100% (complete response in 25% [n = 5], partial response in 75% [n = 18]). Adverse events included fatigue (81%) and headache (76%). The most frequent grade 3 or higher adverse event reported is neutropenia (32% grade 3+). One patient had grade 3 atrial fibrillation and no cases of hemorrhage have been reported.
In the phase 3 ELEVATE-TN study, patients with treatment naïve CLL requiring treatment were randomized in a 1:1:1 fashion to receive acalabrutinib alone or in combination with obinutuzumab or obinutuzumab plus chlorambucil.23 A total of 535 patients was randomized with a median age of 70 years old (range, 41–91). The study included a significant proportion of high-risk or very high-risk patients based on CLL international prognostic index score (69% were high-risk, 12% were very high-risk). PFS has not been reached for the acalabrutinib and the acalabrutinib plus obinutuzumab groups. Obinutuzumab plus chlorambucil had a progression-free survival of 22.6 months (p < 0.0001) and was consistent with the median PFS reported in the CLL11 study.33 Median overall survival has not been reached in any arm. The ORR for acalabrutinib plus obinutuzumab was 94%, for acalabrutinib was 85% and for obinutuzumab plus chlorambucil was 79%. Adverse events in the acalabrutinib groups included headache (any grade, 40% in acalabrutinib plus obinutuzumab, 37% acalabrutinib), diarrhea (any grade, 39% in acalabrutinib plus obinutuzumab, 35% in acalabrutinib), neutropenia (any grade, 31% in acalabrutinib plus obinutuzumab, 11% in acalabrutinib), nausea (any grade, 20% in acalabrutinib plus obinutuzumab, 22% in acalabrutinib). Atrial fibrillation occurred in 3% of patients in the acalabrutinib plus obinutuzumab and 4% of patients in the acalabrutinib. Bleeding events (any grade) occurred in 43% of patients in the acalabrutinib plus obinutuzumab and in 39% of patients in the acalabrutinib group, with 2% bleeding events classified as grade 3 or higher. Hypertension (grade 3 or higher) occurred in 3% in the acalabrutinib plus obinutuzumab group and 2% in the acalabrutinib group. This study allowed crossed over to the acalabrutinib group for patients in the chlorambucil plus obinutuzumab group at disease progression.
Future Studies
From the reported current clinical trials, it appears that acalabrutinib is safe and effective in the front line and relapsed refractory settings in the management of patients with CLL. While it is tempting to speculate that acalabrutinib has similar efficacy to ibrutinib with a favorable side-effect profile, we note that no head-to-head comparative data between acalabrutinib and ibrutinib are available at this time and we caution such conclusions. An ongoing phase 3 trial which has completed enrollment, ELEVATE-RR (ACE-CL-006, NCT02477696), is evaluating acalabrutinib versus ibrutinib in previously treated, high-risk patients. Patients were included in this trial if they had del17p, del11q or both, active disease or one or more of the iwCLL 2008 criteria for requiring treatment, and had received at least 1 prior therapy for CLL. The primary outcome for this trial is 36 months progression-free survival. Secondary outcomes include treatment-emergent grade 3 or greater infections, incidence of Richter’s transformation, incidence of atrial fibrillation, and overall survival all evaluated at 36 months. Of note, since the study is not powered to show superiority of either agent and toxicity is a secondary endpoint, it may not fully address these data gaps regarding differences in efficacy and safety between these two agents.
Several other trials are also on going evaluating acalabrutinib with obinutuzumab and acalabrutinib with obinutuzumab and venetoclax. In the phase 2 MC168E study (NCT03516617), patients with high-risk early stage CLL were randomized to receive acalabrutinib with or without obinutuzumab.29 Patients are considered eligible for enrollment in the study if they are previously untreated and have early-stage CLL that does not meet 2018 iwCLL guidelines for treatment but are classified as high (4–6) or very high risk (7–10) using the CLL International Prognostic Index. The study will evaluate minimal residual disease negativity as its primary endpoint. A total of 28 patients have been enrolled; trial enrollment is ongoing.
In the phase 3 CL-311 (NCT03836261), patients with previously untreated CLL without del17p or TP53 mutation will be randomized to one of three arms: acalabrutinib and venetoclax; acalabrutinib, venetoclax and obinutuzumab; or chemoimmunotherapy (fludarabine/cyclophosphamide/rituximab or bendamustine/rituximab).30 The primary outcome for this study will be progression-free survival (evaluated by an independent review committee) of arm A compared to arm C. The trial is anticipating to enroll 780 patients; trial enrollment is ongoing. Ongoing clinical trials with acalabrutinib are listed in Table 1.
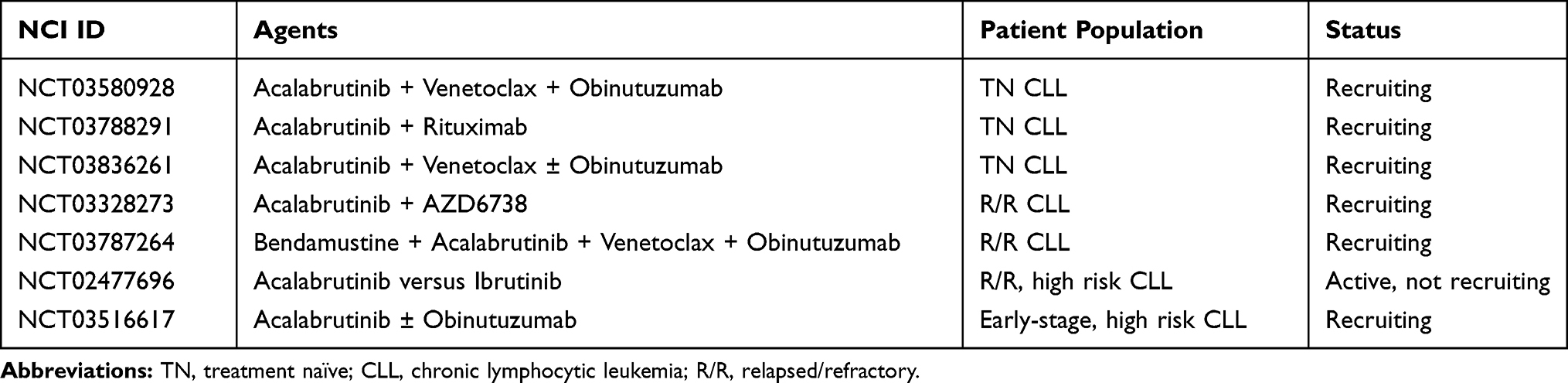 |
Table 1 Current Clinical Trials with Acalabrutinib |
Conclusions
In summary, the studies described demonstrate that acalabrutinib has significant efficacy in treatment of CLL, both treatment naïve and relapsed refractory. It is unclear whether the efficacy is equivalent or superior to ibrutinib and studies are ongoing in an attempt to further compare these agents. Although classic BTK-associated toxicities such as bleeding or atrial fibrillation events are relatively infrequent events, acalabrutinib does have a unique AE profile, particularly headache, which require careful monitoring and expertise in management. Data from ongoing studies evaluating combinations with acalabrutinib will help to further define its role in the management of CLL. Finally, with FDA approval, real-world experience with acalabrutinib will help to further define the toxicity profile.34
Disclosure
Anthony R Mato holds a consultancy role for TG Therapeutics (in addition Data Safety Monitoring Board), Abbvie, Pharamacyclics, Johnson & Johnson, Regeneron, Astra Zeneca, and Celgene and has received research funding from TG Therapeutics, Abbvie, Pharamacyclics, Johnson & Johnson, Regeneron, Portola, DTRM, and Acerta. Dr Mato also reports grants, personal fees, non-financial support from TG Therapeutics, grants, personal fees from AZ/Acerta, Genentech/Abbvie, Loxo, during the conduct of the study; receives grants, personal fees, and Data Safety Monitoring Board from TG Therapeutics, grants, personal fees from, and part of the Steering Committee for AZ, Genentech/Abbvie, Phamacoyclics/JJ, Verastem, personal fees from Celgene, grants, personal fees from LOXO, Sunesis, and Regeneron, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Chiorazzi N, Rai KR, Ferrarini M. Chronic lymphocytic leukemia. N Engl J Med. 2005;352(8):804–815. doi:10.1056/NEJMra041720
2. Burger JA, Tedeschi A, Barr PM, et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med. 2015;373(25):2425–2437. doi:10.1056/NEJMoa1509388
3. Byrd JC, Furman RR, Coutre SE, et al. Three-year follow-up of treatment-naive and previously treated patients with CLL and SLL receiving single-agent ibrutinib. Blood. 2015;125(16):2497–2506. doi:10.1182/blood-2014-10-606038
4. Barr PM, Robak T, Owen C, et al. Sustained efficacy and detailed clinical follow-up of first-line ibrutinib treatment in older patients with chronic lymphocytic leukemia: extended phase 3 results from RESONATE-2. Haematologica. 2018;103(9):1502–1510. doi:10.3324/haematol.2018.192328
5. Mato AR, Nabhan C, Thompson MC, et al. Toxicities and outcomes of 616 ibrutinib-treated patients in the United States: a real-world analysis. Haematologica. 2018;103(5):874–879. doi:10.3324/haematol.2017.182907
6. Maddocks KJ, Ruppert AS, Lozanski G, et al. Etiology of ibrutinib therapy discontinuation and outcomes in patients with chronic lymphocytic leukemia. JAMA Oncol. 2015;1(1):80–87. doi:10.1001/jamaoncol.2014.218
7. Byrd JC, Harrington B, O’Brien S, et al. Acalabrutinib (ACP-196) in relapsed chronic lymphocytic leukemia. N Engl J Med. 2016;374(4):323–332. doi:10.1056/NEJMoa1509981
8. Covey T, Barf T, Gulrajani M, et al. Abstract 2596: ACP-196: a novel covalent Bruton’s tyrosine kinase (Btk) inhibitor with improved selectivity and in vivo target coverage in chronic lymphocytic leukemia (CLL) patients. Cancer Res. 2015;75(15Supplement):2596 LP- 2596. doi:10.1158/1538-7445.AM2015-2596
9. Barf T, Covey T, Izumi R, et al. Acalabrutinib (ACP-196): a covalent bruton tyrosine kinase inhibitor with a differentiated selectivity and in vivo potency profile. J Pharmacol Exp Ther. 2017;363(2):240LP- 252. doi:10.1124/jpet.117.242909
10. Petro JB, Khan WN. Phospholipase C-γ2 couples Bruton’s tyrosine kinase to the NF-κB signaling pathway in B lymphocytes. J Biol Chem. 2001;276(3):1715–1719. doi:10.1074/jbc.M009137200
11. Wiestner A. Emerging role of kinase-targeted strategies in chronic lymphocytic leukemia. Blood. 2012;120(24):4684–4691. doi:10.1182/blood-2012-05-423194
12. Woyach JA, Bojnik E, Ruppert AS, et al. Bruton’s tyrosine kinase (BTK) function is important to the development and expansion of chronic lymphocytic leukemia (CLL). Blood. 2014;123(8):1207–1213. doi:10.1182/blood-2013-07-515361
13. Spaargaren M, Beuling EA, Rurup ML, et al. The B cell antigen receptor controls integrin activity through Btk and PLCgamma2. J Exp Med. 2003;198(10):1539–1550. doi:10.1084/jem.20011866
14. Burger JA. Nurture versus nature: the microenvironment in chronic lymphocytic leukemia. Hematology. 2011;2011(1):96–103. doi:10.1182/asheducation-2011.1.96
15. Tomlinson MG, Woods DB, McMahon M, et al. A conditional form of Bruton’s tyrosine kinase is sufficient to activate multiple downstream signaling pathways via PLC gamma 2 in B cells. BMC Immunol. 2001;2(1):4. doi:10.1186/1471-2172-2-4
16. Petro JB, Rahman SM, Ballard DW, Khan WN. Bruton’s tyrosine kinase is required for activation of IkappaB kinase and nuclear factor kappaB in response to B cell receptor engagement. J Exp Med. 2000;191(10):1745–1754. doi:10.1084/jem.191.10.1745
17. Byrd JC, Brown JR, O’Brien S, et al. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371(3):213–223. doi:10.1056/NEJMoa1400376
18. O’Brien S, Furman RR, Coutre S, et al. Single-agent ibrutinib in treatment-naive and relapsed/refractory chronic lymphocytic leukemia: a 5-year experience. Blood. 2018;131(17):1910–1919. doi:10.1182/blood-2017-10-810044
19. Syed YY. Zanubrutinib: first Approval. Drugs. 2020;80(1):91–97. doi:10.1007/s40265-019-01252-4
20. Tam CS, Trotman J, Opat S, et al. Phase 1 study of the selective BTK inhibitor zanubrutinib in B-cell malignancies and safety and efficacy evaluation in CLL. Blood. 2019;134(11):851–859. doi:10.1182/blood.2019001160
21. Furman RR, Wierda WG, Schuh A, et al. Acalabrutinib monotherapy in patients with relapsed/refractory chronic lymphocytic leukemia: 42-month follow-up of a phase 2 Study. Blood. 2019;134(Supplement_1):3039. doi:10.1182/blood-2019-128706
22. Ghia P, Pluta A, Wach M, et al. Acalabrutinib vs Rituximab Plus Idelalisib (IdR) or Bendamustine (BR) by Investigator Choice in Relapsed/Refractory (RR) chronic lymphocytic leukemia: phase 3 ASCEND Study. Hematol Oncol. 2019;37(S2):86–87. doi:10.1002/hon.54_2629
23. Sharman JP, Banerji V, Fogliatto LM, et al. ELEVATE TN: phase 3 study of acalabrutinib combined with Obinutuzumab (O) or alone vs O Plus Chlorambucil (Clb) in Patients (Pts) with Treatment-Naive Chronic Lymphocytic Leukemia (CLL). Blood. 2019;134(Supplement_1):31. doi:10.1182/blood-2019-128404
24. Covey T, Gulranjani M, Cheung J, et al. Pharmacodynamic evaluation of acalabrutinib in relapsed/refractory and treatment-naive patients with Chronic Lymphocytic Leukemia (CLL) in the phase 1/2 ACE-CL-001 Study. Blood. 2017;130(Supplement1):1741. doi:10.1182/blood.V130.Suppl_1.1741.1741
25. Patel V, Balakrishnan K, Bibikova E, et al. Comparison of acalabrutinib, a selective bruton tyrosine kinase inhibitor, with ibrutinib in chronic lymphocytic leukemia cells. Clin Cancer Res. 2017;23(14):3734–3743. doi:10.1158/1078-0432.CCR-16-1446
26. Herman SEM, Montraveta A, Niemann CU, et al. The Bruton Tyrosine Kinase (BTK) inhibitor ACP-196 demonstrates clinical activity in two mouse models of chronic lymphocytic leukemia. Blood. 2015;126(23):2920. doi:10.1182/blood.V126.23.2920.2920
27. Golay J, Ubiali G, Introna M. The specific Bruton tyrosine kinase inhibitor acalabrutinib (ACP-196) shows favorable in vitro activity against chronic lymphocytic leukemia B cells with CD20 antibodies. Haematologica. 2017;102(10):e400–e403. doi:10.3324/haematol.2017.169334
28. Lampson BL, Tyekucheva S, Crombie JL, et al. Preliminary safety and efficacy results from a phase 2 study of acalabrutinib, venetoclax and obinutuzumab in patients with previously untreated Chronic Lymphocytic Leukemia (CLL). Blood. 2019;134(Supplement_1):32. doi:10.1182/blood-2019-127506
29. Parikh SA, Muchtar E, Laplant B, et al. A randomized phase 2 study comparing acalabrutinib with or without obinutuzumab in the treatment of early stage high risk patients with Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL). Blood. 2019;134(Supplement_1):4306. doi:10.1182/blood-2019-123824
30. Brown JR, Eichhorst BF, Ghia P, et al. A phase 3 trial comparing the efficacy and safety of acalabrutinib in combination with venetoclax with or without obinutuzumab, compared with investigator’s choice of chemoimmunotherapy in patients with previously untreated Chronic Lymphocytic Leukemia (CLL). Blood. 2019;134(Supplement_1):4318. doi:10.1182/blood-2019-123057
31. Niemann CU, Mora-Jensen HI, Dadashian EL, et al. Combined BTK and PI3Kdelta inhibition with Acalabrutinib and ACP-319 improves survival and tumor control in CLL mouse model. Clin Cancer Res. 2017;23(19):5814–5823. doi:10.1158/1078-0432.CCR-17-0650
32. Patel VK, Lamothe B, Ayres ML, et al. Pharmacodynamics and proteomic analysis of acalabrutinib therapy: similarity of on-target effects to ibrutinib and rationale for combination therapy. Leukemia. 2018;32(4):920–930. doi:10.1038/leu.2017.321
33. Goede V, Fischer K, Busch R, et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N Engl J Med. 2014;370(12):1101–1110. doi:10.1056/NEJMoa1313984
34. Yazdy MS, Mato AR, Roeker LE, et al. Toxicities and outcomes of acalabrutinib-treated patients with chronic lymphocytic leukemia: a retrospective analysis of real world patients. Blood. 2019;134(Supplement_1):4311. doi:10.1182/blood-2019-130062
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.