")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 13
Abdominal Intraluminal Gossypiboma: Demographics, Predictors of Intraluminal Site, Diagnostic and Treatment Measures
Authors Obeidat KA , Aleshawi AJ, Alebbini MM, Bani Yasin SN
Received 26 October 2019
Accepted for publication 17 February 2020
Published 27 February 2020 Volume 2020:13 Pages 65—72
DOI https://doi.org/10.2147/CEG.S236179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Everson L.A. Artifon
Khaled A Obeidat,1 Abdelwahab J Aleshawi,2 Mohanad M Alebbini,2 Saja N Bani Yasin2
1Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan; 2Faculty of Medicine, Jordan University of Science & Technology, Irbid 22110, Jordan
Correspondence: Khaled A Obeidat
Department of General Surgery and Urology, Faculty of Medicine, Jordan University of Science and Technology, P. O. Box: 3030, Irbid 22110, Jordan
Tel +962797707397
Fax +962 2 7201064
Email [email protected]
Objective: Intra-abdominal gossypiboma may present with variable clinical presentations. The clinical picture that the patient presents with depends on the site of the retained gauze in the abdomen, with transmural migration leading to intraabdominal gauze being a rare occurrence. We systemically analyze articles and reports related to the transmural migration of gossypiboma. In addition, we report a case of ileal transmigration of gossypiboma in a 53-year-old female.
Methods: A systematic literature review was conducted using Embase and Medline for articles pertaining to transmural migration of gossypiboma. Three of the authors extracted the data from the selected studies that relate to the topic. All articles included were in English language and published in peer-reviewed journals. This study was conducted according to the guidelines set out by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.
Results: A total of 93 cases of intraluminal gossypiboma were found in the literature. The mean age of the patients was 40.4 years and females (77.7%) were affected more than males. The obstetric and gynecologic surgeries were the leading causative operation (41.5%). However, cholecystectomy is the most common single surgery associated with intraluminal gossypiboma. The mean time from the causative operation was 35.16 months. Most patients presented as intestinal obstruction. CT scan was the most sensitive tool to detect any non-specific finding while the endoscopic interventions were the most specific. Ileum is the most common site for intraluminal for migration. Intra-gastric location is related mostly to the hepato-biliary operations. Laparotomy with segmental resection provides a primary treatment and cure.
Conclusion: Clinicians should keep the possibility of gossypiboma, including intraluminal, in their mind when a patient presents with abdominal pain, signs of infection, intestinal obstruction, or a palpable mass any time after abdominal surgery. Measures for prevention and education are the most useful tool to avoid such complications.
Keywords: gossypiboma, transmural migration, intra-abdominal, retained surgical sponge, surgical complication, textiloma
Introduction
Gossypiboma is a term that has been used when a gauze or sponge is left by mistake in the surgical field after a surgical procedure. Terms that have also been used to describe this situation are textiloma, cottonoid, cottonballoma, or gauzeoma.1,2 The term gossypiboma derives from the Latin word “gossypium” and the Swahili word “boma,” which means cotton and a “place of concealment,” respectively.1,2 Intra-abdominal gossypiboma is the term used when a sponge is accidentally left in the abdominal cavity.3 This complication can be serious and associated with life-changing outcomes.
The clinical presentation of intra-abdominal gossypiboma may vary according to the exact site where the retained gauze is located inside the abdomen. One rare scenario is the migration of the retained gauze into the lumen of the stomach, small bowel, or colon.3 In this article, we systemically analyze articles and reports related to the transmural migration of gossypiboma. Besides, we report a case of ileal transmigration of gossypiboma in a 53 years-old female.
Materials and Methods
Case Presentation
A 53-year-old hypertensive female presented to our center with severe central abdominal pain for 2 weeks, non-radiating, exacerbated by food and partially relieved by vomiting. The vomitus was food in content, three times daily, and without blood. Also, she complained of decreased appetite and significant weight loss of 12 Kgs (8%) over a period of 2 months. Her past surgical history was significant for hysterectomy 4 months earlier for uterine fibroid at an outside hospital.
Physical examination was remarkable for abdominal distension, mild diffuse tenderness, and active bowel sounds. No fever was reported. Despite microcytic anemia, all laboratory investigations were within normal range. Chest-Abdominal-Pelvic computed tomography (CT) was performed and revealed dilation of the distal bowel loops that contained impacted fecal material and multiple linear dense radiopaque material associated with fat stranding with suspected foreign body Figure 1. The decision was to go for surgery.
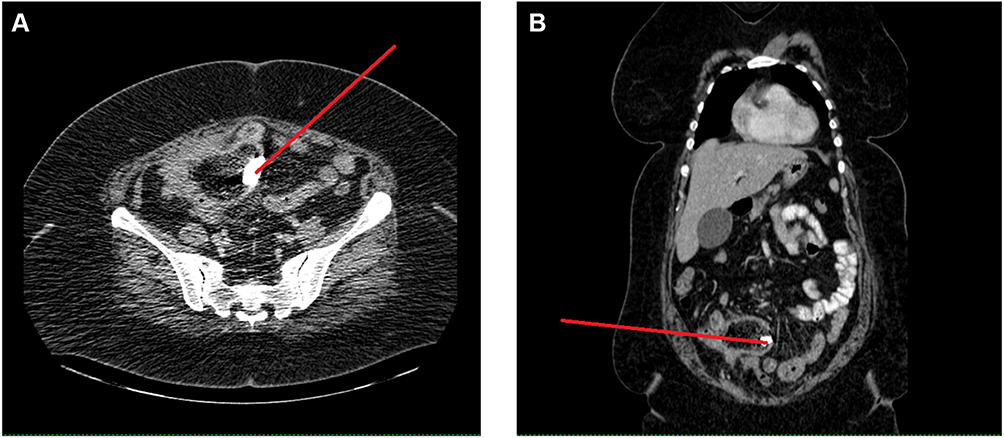 |
Figure 1 CT scan (A) axial view and (B) coronal view indicating dilation of the distal bowel loops that contained impacted fecal material and multiple linear dense radiopaque material (red arrow) associated with fat stranding with suspected foreign body. |
At laparotomy, extensive adhesions around the terminal ilium were detected with the surrounding small bowel loops fixed to the abdominal wall. Intraluminal foreign in the terminal ilium with small bowel contained perforation was observed. Small bowel loop mobilization and resection was performed and revealed intraluminal gauzoma in the terminal ilium Figure 2. The resultant histopathological examination revealed no significant findings within the gossypiboma and bowel loop.
 |
Figure 2 (A–C) Intraoperative laparotomy and sponge extraction. |
She was discharged 15 days after the operation in a good general health, active bowel function and tolerable food intake. Post-operatively, she was followed up one month, three months, and one year without any complication.
Method of Review
This study was done following the guidelines set out by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.4
The authors performed a systematic search in MEDLINE and EMBASE for cases reported in English literature with the last search on December 1st, 2018. The primary keywords used were “gossypiboma”, “gossypiboma and transmigration”, “transmural migration”, “intragastric migration”, “gauzoma textiloma,” retained surgical sponge textiloma, and “textiloma”.
Eligibility Criteria
Only cases reporting intraabdominal and intraluminal gossypiboma were included in the study.
Study Selection and Data Collection
Titles and abstracts containing the keywords and meeting the inclusion criteria were retrieved in full for further examination. References cited by these articles were also reviewed and those that were meeting the inclusion criteria were also included in our analysis. General demographic data, clinical features, causative operation, site of the intraluminal gossypiboma, diagnostic methods and treatment procedures for these cases were recorded, summarized and categorized so that the data can be analyzed using proper statistical methods. Three of the authors independently searched for and selected eligible studies then extracted and recorded the data after checking accuracy and assessing quality.
Statistical Analysis
Data were entered into a spreadsheet. The statistical analysis was performed with SPSS software, version 21.0 (IBM, Armonk, New York, USA). Categorical variables were presented as frequency distributions while continuous variables were presented as mean ± standard error of the mean (SE). Data were tested at a significance level of 0.05%. We used Pearson χ2 test to investigate the significance of association between categorical variables and used Student’s t-test and ANOVA to examine the significance level for continuous normally distributed variables. Kruskal–Walis test was applied for the abnormally distributed continuous variable. If a significant (P<0.05) relationship was found, then a posthoc residual analysis for categorical variables and a Fisher’s least significant difference test for continuous variables was applied to determine the exact significance between groups for each variable.
Results
Demographics and Patients’ Characteristics
A total of 93 cases of intraluminal gossypiboma were found in the English literature dating back to its first description in 1963.5–28 Including our case, we had a total of 94 cases of intraluminal gossypiboma.
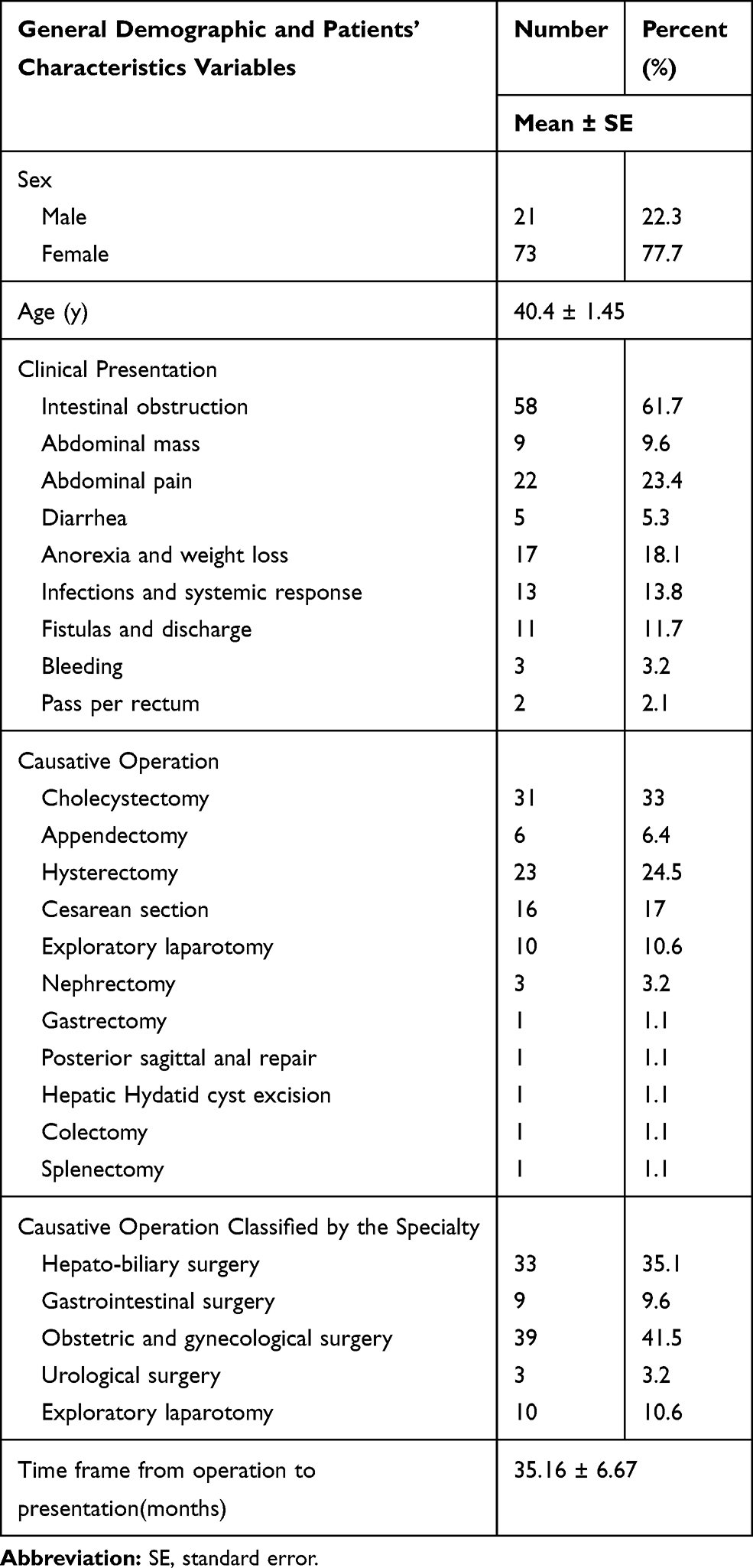 |
Table 1 General Demographic and Patients’ Characteristics |
The patient demographics and characteristics of the intraluminal gossypiboma are summarized in Table 1. The mean age of the patients was 40.4 year ranging from 3 to 75. Females were obviously more affected than males; 73 females and 21 males were reported.
The main clinical presentation features were found to be intestinal obstruction in more than 60% of the patients. Also, abdominal pain, weight loss and infections were observed in a significantly large number of patients. Other minor symptoms included abdominal mass, diarrhea, fistulas with discharge, and bleeding. In addition, two cases were incidentally passed per rectum.
The causative operations are the surgical operations that were assumed to be main setting where the gauze was forgotten within the patients. The causative operations were categorized into hepato-biliary surgery, gastrointestinal surgery, gynecological surgery, urological surgery, and exploratory laparotomy for traumatic patients. The gynecological surgeries were being the leading cause for gossypiboma and its intraluminal migration (41%) (this why the females were more reported). After that, the hepato-biliary surgeries were found in 35.1% of patients. Then, exploratory laparotomy, gastrointestinal surgeries and urological surgeries in 10.6%, 9.6% and 3.2%, respectively. However, if we look for the operation a specific organ surgery, we will find that cholecystectomy is most commonly associated with intraluminal gossypiboma. All causative operations are summarized in Table 1.
The mean time from the causative operation was 35.16 months. The shortest period was 1 week, and the longest period was 276 months.
Diagnostic and Treatment Measures
The diagnostic modalities that were reported to be utilized are barium studies, abdominal ultrasound, abdominal X-ray, CT scan, endoscopic procedure and in few cases MRI and PET scan (Table 2). The endoscopic assessment was conclusively diagnostic in 73.3% from a total 30 patients who underwent endoscopic procedures (It means the gastroscopy when the gauze located in the stomach or first or second part of duodenum. Also, it means the colonoscopy when the gauze in the colon or ileocecal region). It is followed by CT scan where it was diagnostic in 56.9%. Abdominal X-ray was diagnostic in 34.6%. The barium study and abdominal ultrasound were diagnostic in less than 10%. The diagnostic findings for each modality will be discussed later.
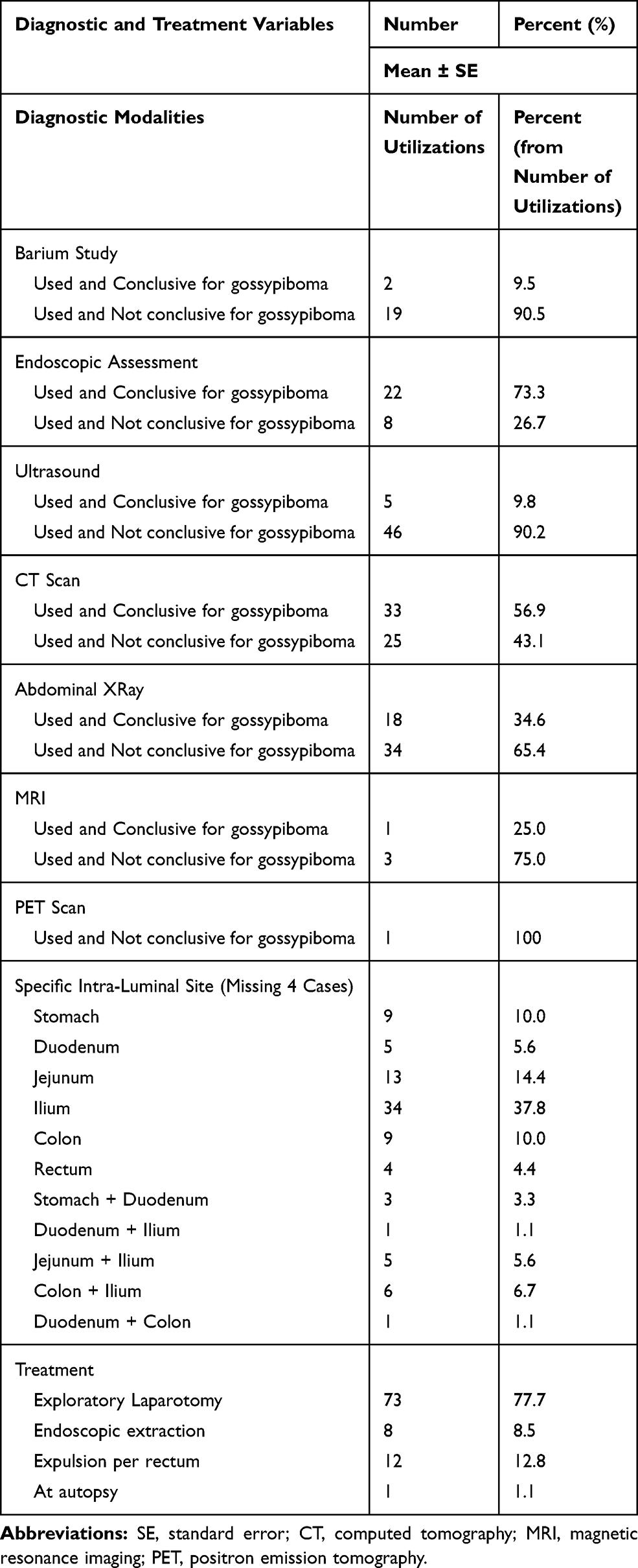 |
Table 2 Diagnostic and Treatment Measures |
In 34 (37.8%) of the patients, the gossypiboma was intra-ileal. Jejunum was the second luminal organ for the gossypiboma to migrate in 14.4%. Colon and stomach were the site for 10% of gossypiboma in each of them. Duodenum and rectum were least to be involved. Also, in many cases, the gossypiboma involved two intraluminal migration with intra-colonic and intra-ileal being mostly involved.
Exploratory laparotomy with or without resection was the main treatment step in 77.7%. Endoscopic retrieval was successfully performed in 8 patients. Expulsion per rectum spontaneously or induced was observed 12 patients.
Predictors for Intraluminal Site
First, the intraluminal site was categorized into stomach, small bowel, large bowel, small bowel and stomach together, and small and large bowel together. The predictors for the site of intraluminal migration were studied on multiple levels of data, the general demographic, clinical symptoms, and diagnostic methods.
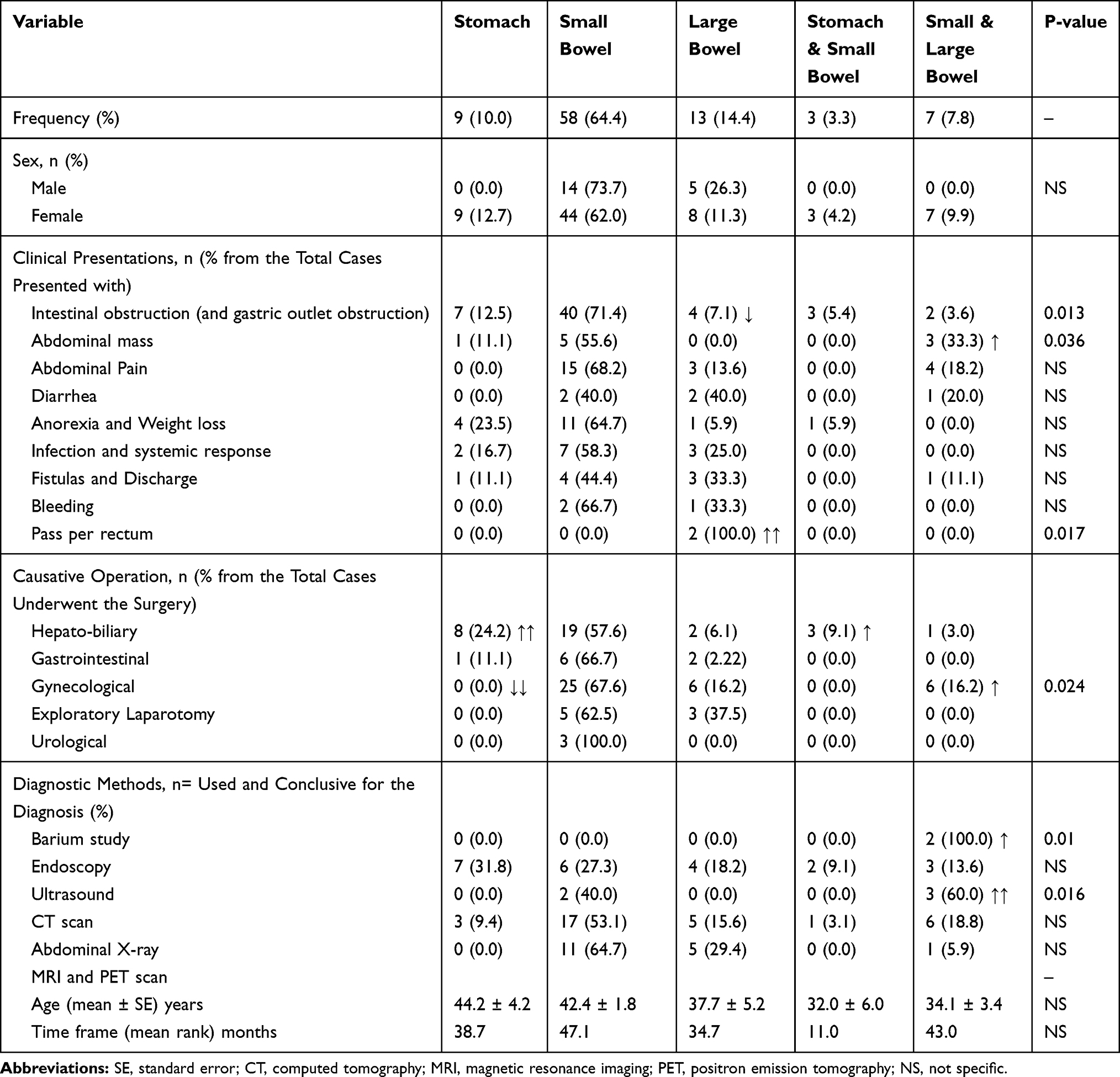 |
Table 3 Predictors for Intraluminal Migration Site |
Age and sex showed no significant association with the site of intraluminal gossypiboma. However, the causative operation was significantly associated with the intraluminal site (P< 0.05) as follows: the hepato-biliary surgeries were significantly associated with intragastric location for the gossypiboma with an adjusted residual Z-score and posthoc P value of 3.42 and 0.00, respectively. Similarly, the hepato-biliary surgeries were significantly associated with stomach and small intestine together. Also, the presence of gynecological surgeries decreases the chance for intragastric location significantly and increase the chance for small and large bowel together. Table 3 summarizes the remainder of the results.
Clinically, intestinal obstruction as a presentation was associated with small bowel location for intraluminal gossypiboma (P value = 0.013), whereas passage of gauze per rectum was associated with large bowel location (P value = 0.017). The combination of small and larger bowel was significantly associated with abdominal mass presentation (P value = 0.036). Non-obstructing abdominal pain, bleeding, diarrhea, infection and fistulas were not significant predictors for the site of intraluminal gossypiboma.
For the diagnosis of the gossypiboma and its site; no significant association was detected except for the barium study and ultrasound where they conclusively significantly diagnosed small and large bowel sites. However, the endoscopy was able to diagnose 7 intragastric gossypiboma, 6 in the small intestine (5 in the duodenum and 1 in the terminal ilium), and 4 intra-colonic gossypiboma.
Discussion
To our knowledge, this is the most comprehensive review study indicating the clinical impact and relevance of gossypiboma and the intraluminal migration. The mean age of the patients was 40.4 years and the females affected more than males. The obstetric and gynecologic surgeries were the leading causative operation. Most patients presented as intestinal obstruction. CT scan is the most sensitive tool to detect any non-specific finding while the endoscopic interventions are the most specific. Laparotomy with segmental resection provides a primary treatment and cure.
The term “gossypiboma” means a sponge or gauze that is left accidentally in the surgical field after surgery. The exact incidence of this rare surgical complication is not known because of being under-reported. The reported incidence of gossypiboma varies between 1/100 and 1/3000 for all surgical interventions and from 1/1000 to 1/1500 for intra-abdominal operations.24,27-29 Wattanasirichaigoon performed an experimental study in which he placed cotton swabs at different locations in rats’ peritoneal cavity. Intraluminal migration of the sponge occurred in 10 out of 36 animals.30 In Bani-Hani et al study, 11 cases of retained gossypiboma were reported. Among them, one patient developed intraluminal migration.28 Patients with gossypiboma can have two main types of foreign body reactions. In the first type, there will be formation of foreign body granuloma which is usually clinically asymptomatic. This is thought to be mostly caused by a fibrous reaction to the gauze that results in adhesions and encapsulation of the foreign material. Eventually, the gossypiboma may undergo calcification, disruption, partial absorption, or diffusion. In the second type, there will be exudative inflammatory reaction with abscess formation. I this case, the body tries to get rid of the foreign material by eliciting extensive inflammatory response, which usually causes significant symptoms for the patient. Eventually, this may result foreign body sinus, enterocutaneous fistula formation, or transmigration of the foreign body into the gut, with resultant intestinal obstruction, or extrusion of the gossypiboma.8,23 Dhillon and Park suggested that an inflammatory reaction surrounds the foreign body, with abscess formation that erodes the surrounding tissues. Following this process, the foreign body may move forward by the peristalsis. This migration may occur mostly into the ileum.7 Wattanasirichaigoon et al described 4 stages in the process of migration: foreign body reaction, secondary infection, mass formation, and remodeling.30
The diagnosis of gossypiboma is largely based on imaging studies which demonstrate a retained sponge. Most of the time, clinicians start with plain X-ray films which may demonstrate a radiopaque material in the body. However, plain X-ray is neither specific nor sensitive in the diagnosis of gossypiboma. Also, it does not provide accurate information about the location of the foreign material. Because of that, computed tomography (CT) is considered as the preferred initial study when there is suspicion of retained foreign material. CT is highly sensitive and reasonably specific for diagnosis of retained sponge. A low-density heterogeneous mass with a spongiform pattern that contains gas bubbles is the characteristic appearance of gossypiboma on CT. In addition, CT provides good information about the location of foreign material and usually guides clinicians to suspect intraluminal gossypiboma. When there is suspicion of intraluminal gossypiboma, then barium studies and endoscopy may help confirm the diagnosis. In addition, ultrasonography, and magnetic resonance imaging (MRI) may be useful for diagnosis.12,14 The differential diagnosis of gossypiboma includes fecaloma, abscess formation, hematoma, and tumor. Regarding the fecaloma, it presents a spotted appearance on CT but has a recognizable colonic wall and lacks thick well-defined capsule. On the other hand, hematoma is located in the early postoperative period and demonstrated resorption later. An abscess is visualized as a mass of fluid density and has a well-defined enhancing wall. Also, the abscess differs in that the gas within it produces an air-fluid level rather than the spongiform pattern characteristic of gossypiboma. However, abscess formation can occur as a complication of gossypiboma formation.31
Even though prevention is the best line of management, the best-considered therapy for a retained gossypiboma in the abdomen when occurs is the surgical removal with resection mostly, which carries a 10% mortality rate if there is delay in treatment.9 In fact, the alternative methods such as percutaneous extraction are not that useful for the removal of gossypiboma from the abdomen, mainly because of the dense adhesions that are uniformly found between the gossypiboma and intra-abdominal organs.9
The problem of retained surgical instruments is not limited to the abdominal surgery. Turgut et al in their meta-analysis reported 58 cases of retained nonabsorbable hemostatic materials within or around the spinal canal after spinal surgeries.32 Koul et al reported an intrathoracic gossypiboma after pneumonectomy.33 Also, Mir and Singh reported another intrathoracic gossypiboma after lobectomy.34 Similarly, Haddad et al reported a tracheal migration of sponge after mediastinoscopy a 62-year-old lady.35 Moreover, Leppäniemi reported intravesical (inside the bladder) migration of swab after inguinal hernia repair in a 36-year-old man.36 According to Gawande et al study, gossypiboma was most commonly found in the abdomen (56%), pelvis (18%) and thorax (11%).37 In the systematic review of Zantvoord et al, they found 9 cases intrathoracic and intratracheal migration of the gauze out of 65 of intra-cavitary migration. Also, among the 65 cases, they found 4 cases of intravesical migration.12
As we have mentioned, the actual number is much lower than expected because of low reporting rate due to medicolegal implications. Gossypiboma is most commonly developed in cases of emergency situations, disorganization within the operation room, immediate unplanned change in the surgical procedure, change in surgical team or scrub nurses, quick sponge counts, long operations, inexperienced staff, unstable patient and obesity.38 In order to avoid the dilemma of any medicolegal consequences, prevention of gossypiboma can be done by several methods. Simply, it can be done by thorough pack count and tagging the packs with markers. Also, new technologies are being developed such as an electronic article surveillance system which uses a tagged surgical sponge that can be identified electronically has been examined.39
Our study is not without limitation. The main limitation is depending on previously reported cases and articles which limit our ability to study the outcome and prognosis of such important topic.
Conclusion
Clinicians should keep the possibility and suspicion of gossypiboma, including intraluminal, in their mind when a patient presents with abdominal pain, signs of infection, intestinal obstruction, or a palpable mass any time after abdominal surgery. This is very important for whom in the field of obstetrics and gynecology. Measures for prevention and education are the most useful tool to avoid such complications.
Ethics and Patient Consent
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. Patient confidentiality is preserved. Institutional Review Board approval is not required for this type of articles and it is not required to publish the case details and images.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Sistla SC, Ramesh A, Karthikeyan VS, et al. Gossypiboma presenting as coloduodenal fistula–report of a rare case with review of literature. Int Surg. 2014;99:126–131. doi:10.9738/INTSURG-D-13-00057.1
2. Srivastava KN, Agarwal A. Gossypiboma posing as a diagnostic dilemma: a case report and review of the literature. Case Rep Surg. 2014;2014:713428.
3. Margonis E, Vasdeki D, Diamantis A, et al. Intestinal obstruction and Ileocolic Fistula due to intraluminal migration of a gossypiboma. Case Rep Surg. 2016;2016:3258782.
4. Panic N, Leoncini E, de Belvis G, et al. Evaluation of the endorsement of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement on the quality of published systematic review and meta-analyses. PLoS One. 2013;8:e83138. doi:10.1371/journal.pone.0083138
5. Gupta NM, Chaudhary A, Nanda V, et al. Retained surgical sponge after laparotomy. Unusual presentation. Dis Colon Rectum. 1985;28:451–453. doi:10.1007/BF02560235
6. Silva CS, Caetano MR, Silva EA, et al. Complete migration of retained surgical sponge into ileum without sign of open intestinal wall. Arch Gynecol Obstet. 2001;265:103–104. doi:10.1007/s004040000141
7. Dhillon JS, Park A. Transmural migration of a retained laparotomy sponge. Am Surg. 2002;68:603–605.
8. Manikyam SR, Gupta V, Gupta R, et al. Retained surgical sponge presenting as a gastric outlet obstruction and duodeno-ileo-colic fistula: report of a case. Surg Today. 2002;32:426–428. doi:10.1007/s005950200068
9. Grassi N, Cipolla C, Torcivia A, et al. Trans-visceral migration of retained surgical gauze as a cause of intestinal obstruction: a case report. J Med Case Rep. 2008;2:17. doi:10.1186/1752-1947-2-17
10. Choi JW, Lee CH, Kim KA, et al. Transmural migration of surgical sponge evacuated by defecation: mimicking an intraperitoneal gossypiboma. Korean J Radiol. 2006;7:212–214. doi:10.3348/kjr.2006.7.3.212
11. Sharma D, Pratap A, Tandon A, et al. Unconsidered cause of bowel obstruction–gossypiboma. Can J Surg. 2008;51:E34–E35.
12. Zantvoord Y, van der Weiden RM, van Hooff MH. Transmural migration of retained surgical sponges: a systematic review. Obstet Gynecol Surv. 2008;63:465–471. doi:10.1097/OGX.0b013e318173538e
13. Tandon A, Bhargava SK, Gupta A, et al. Spontaneous transmural migration of retained surgical textile into both small and large bowel: a rare cause of intestinal obstruction. Br J Radiol. 2009;82:e72–e75. doi:10.1259/bjr/32683906
14. Patil KK, Patil SK, Gorad KP, et al. Intraluminal migration of surgical sponge: gossypiboma. Saudi J Gastroenterol. 2010;16:221–222. doi:10.4103/1319-3767.65195
15. Ogundiran T, Ayandipo O, Adeniji-Sofoluwe A, et al. Gossypiboma: complete transmural migration of retained surgical sponge causing small bowel obstruction. BMJ Case Rep. 2011;2011:bcr0420114073.
16. Erbay G, Koç Z, Calişkan K, et al. Imaging and clinical findings of a gossypiboma migrated into the stomach. Turk J Gastroenterol. 2012;23:54–57. doi:10.4318/tjg.2012.0309
17. Aydogan A, Akkucuk S, Yetim I, et al. Gossypiboma causing mechanical intestinal obstruction: a case report. Case Rep Surg. 2012;2012:543203.
18. Kato T, Yamaguchi K, Kinoshita K, et al. Intestinal obstruction due to complete transmural migration of a retained surgical sponge into the intestine. Case Rep Gastroenterol. 2012;6:754–759. doi:10.1159/000346285
19. Sozutek A, Yormaz S, Kupeli H, et al. Transgastric migration of gossypiboma remedied with endoscopic removal: a case report. BMC Res Notes. 2013;6:413. doi:10.1186/1756-0500-6-413
20. Singhal BM, Kumar V, Kaval S, et al. Spontaneous intraluminal migration of gossypiboma with intestinal obstruction. OA Case Rep. 2013;2:145.
21. Shekhar C, Kumar A, Chandra A. Transmural migration of surgical sponge into stomach with outlet obstruction: gossypiboma. Indian J Gastroenterol. 2013;32:208. doi:10.1007/s12664-013-0308-3
22. Kohli S, Singhal A, Tiwari B, et al. Gossypiboma, varied presentations: a report of two cases. J Clin Imaging Sci. 2013;3:11. doi:10.4103/2156-7514.107998
23. Lv YX, Yu CC, Tung CF, et al. Intractable duodenal ulcer caused by transmural migration of gossypiboma into the duodenum–a case report and literature review. BMC Surg. 2014;14:36. doi:10.1186/1471-2482-14-36
24. Agrawal H, Gupta N, Krishengowda U, et al. Transmural migration of gossypiboma: a rare cause of acute abdomen. Indian J Surg. 2018;80:84–86. doi:10.1007/s12262-017-1660-9
25. Agrawal V, Gupta P. Gossypiboma due to a retained surgical sponge following abdominal hysterectomy, complicated by intestinal migration and small bowel obstruction- a case report. Arch Surg Clin Res. 2018;2:015–017.
26. Patial T, Rathore N, Thakur A, et al. Transmigration of a retained surgical sponge: a case report. Patient Saf Surg. 2018;12:21. doi:10.1186/s13037-018-0168-y
27. De Campos FF, Franco F, Maximiano LF, et al. An iron deficiency anemia of unknown cause: a case report involving gossypiboma. Clinics (Sao Paulo). 2010;65:555–558. doi:10.1590/S1807-59322010000500014
28. Bani-Hani KE, Gharaibeh KA, Yagha RJ. Retained surgical sponges (gossypiboma). Asian J Surg. 2005;28:109–115. doi:10.1016/S1015-9584(09)60273-6
29. Dux M, Ganten M, Lubienski A, et al. Retained surgical sponge with migration into the duodenum and persistent duodenal fistula. Eur Radiol. 2002;12(suppl 3):S74–S77. doi:10.1007/s00330-002-1408-0
30. Wattanasirichaigoon S. Transmural migration of a retained surgical sponge into the intestinal lumen: an experimental study. J Med Assoc Thai. 1996;79:415–422.
31. Malik A, Jagmohan P. Gossypiboma: US and CT appearance. Indian J Radiol Imaging. 2002;12:503–504.
32. Turgut M, Akhaddar A, Turgut AT. Retention of nonabsorbable hemostatic materials (Retained surgical sponge, gossypiboma, textiloma, gauzoma, muslinoma) after spinal surgery: a systematic review of cases reported during the last half-century. World Neurosurg. 2018;116:255–267. doi:10.1016/j.wneu.2018.05.119
33. Koul PA, Mufti SA, Khan UH, Jan RA. Intrathoracic gossypiboma causing intractable cough. Interact Cardiovasc Thorac Surg. 2012;14(2):228–230. doi:10.1093/icvts/ivr058
34. Mir R, Singh VP. Retained intra- thoracic surgical pack mimicking as recurrent aspergilloma. J Clin Diagn Res. 2012;6(10):1775–1777. doi:10.7860/JCDR/2012/4688.2610
35. Haddad R, Judice LF, Chibante A, Ferraz D. Migration of surgical sponge retained at mediastinoscopy into the trachea. Cardiovasc Thorac Surg. 2004;3:637–640.
36. Leppäniemi AK. Intravesical foreign body after inguinal herniorrhaphy. Case report. Scand J Urol Nephrol. 1991;25(1):87–88. doi:10.3109/00365599109024538
37. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med. 2003;348:229–235. doi:10.1056/NEJMsa021721
38. Lata I, Kapoor D, Sahu S. Gossypiboma, a rare cause of acute abdomen: a case report and review of literature. Int J Crit Illn Inj Sci. 2011;1(2):157–160. doi:10.4103/2229-5151.84805
39. Fabian CE. Electronic tagging of surgical sponges to prevent their accidental retention. Surgery. 2005;137:298–301. doi:10.1016/j.surg.2004.10.003
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.