")
Back to Journals » International Journal of Women's Health » Volume 11
A Whole Life Of Threats: A Qualitative Exploration Of Lived Experiences Of Palestinian Women Suffering From Intimate Partner Violence
Authors Baloushah S , Mohammadi N , Taghizadeh Z, Taha AA , Farnam F
Received 24 May 2019
Accepted for publication 10 October 2019
Published 25 October 2019 Volume 2019:11 Pages 547—554
DOI https://doi.org/10.2147/IJWH.S216952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Suha Baloushah,1 Nooredin Mohammadi,2 Ziba Taghizadeh,3 Asma A Taha,4 Farnaz Farnam5
1Reproductive Health Department, School of Nursing and Midwifery, Tehran University of Medical Sciences, International Campus, Tehran, Iran; 2Nursing Care Research Center, Iran University of Medical Sciences, Tehran, Iran; 3Nursing and Midwifery Care Research Center, Tehran University of Medical Sciences, Tehran, Iran; 4School of Nursing, Oregon Health and Science University, Portland, OR, USA; 5Reproductive Health Department, Tehran University of Medical Sciences, Tehran, Iran
Correspondence: Ziba Taghizadeh
Tehran University of Medical Sciences, Tohid Square, Mirkhani St. Tehran 1419733171, Iran
Tel +982161054568
Email [email protected]
Background: Violence against women is a widespread public health problem in the Palestinian community considered to be a traditional community. It is usually underreported due to cultural and religious issues. The present study was carried out in order to deepen the understanding of the feelings, thoughts, and perceptions of Palestinian women living in the Gaza Strip and suffering from intimate partner violence.
Methods: Hermeneutic phenomenological study was conducted. The recruited 11 Palestinian women suffering from intimate partner violence were selected via purposive means. Semi-structured in-depth interviews conducted from May to Sept 2018 were used to understand their lived experience. Data was analyzed through the Van Manen method.
Results: In the process of data analysis, living in a threatening world was the main theme that was extracted from the data. The theme refers to the condition that participants were committed to their marriage and are compelled to remain in a threatening situation. That was interpreted as a whole life of threats, which was labeled as the main theme emerging from three sub-themes. This main theme included 3 subthemes namely “live in a physically threatening environment”, “live in psychologically threatening environment”, and “live in sexual threatening environment”.
Conclusion: As revealed in our study, the participant suffered extremely from intimate partner violence and its consequences, which negatively affected their lives. However, their concerns about their children and lack of support were barriers for them to get a divorce; therefore, abused women need help to deal with their current lives like access to social and psychological counseling.
Keywords: intimate partner violence, Palestine, qualitative study, phenomenology
Introduction
Intimate partner violence (IPV) is defined as a pattern of assaultive and coercive behaviors in intimate relationships, usually committed by men against women to obtain power, control, or authority.1,2 It is considered the most common type of violence against women and is estimated to be around 30% globally.3
It is reported that IPV is overwhelmingly prevalent and the main contributor to ill health among women.4 Intimate partner violence can lead to various adverse physical and psychological consequences that negatively influence the ability of the victims to carry out their daily activities efficiently.5 IPV can also be associated with psychological consequences such as depressive episodes,6 post-traumatic stress disorder, substance abuse.7 Physical consequences of IPV can include chronic pains, migraines, speech disorders, arthritis, ulcers, intestinal problems, sexually transmitted infections and pelvic pain.8 Although IPV is highly prevalent, few reports exist on its occurrence, which can partially contribute to the nature of this problem.9 IPV is considered mostly as a private affair between spouses. Therefore, victims do not usually report it to the police or the authorities.10 As a result, most victimized women choose to keep the violence as a secret and do not to talk about it.11 Moreover, they choose not to disclose IPV due to their belief that disclosing violence is a sign of disloyalty and also because of the danger of retaliation by the abusive partner.12
According to the results of the investigations into the causes of IPV, sociodemographic factors of structural inequality of societies and families have a significant effect on the occurrence of IPV.13 Socioeconomic status of families and the social structure of the society are other effective factors.14
However, since most people consider violence toward women as a normal occurrence in society, most victimized women do not seek help.15
Despite the high prevalence of IPV which negatively affects the quality of their lives, most of them choose to stay with their abusive partner because of different reasons including economic reliance, women’s greater loyalty to their relationship,16 fear of more violence,17 and concern about their children.18
IPV in traditional less-developed countries such as Sri Lanka,19 Palestine,20 and Jordan21 has been reported to be quite prevalent, which can be attributed to the traditional patriarchal beliefs dominating these societies. Assaf and Chaban (2013) reported that Palestinian men resort to religion as one of the remarkable excuses for committing IPV.22 The Palestinian community is considered to be one of the traditional Arab communities where values within a patriarchal family structure, and family cohesiveness are prioritized over individual rights and freedoms.23
The present study was a phenomenological qualitative investigation that was carried out to analyze the lived experiences of Palestinian women suffering from IPV in order to gain deeper understanding of their feelings, thoughts, and perceptions. A qualitative study aims at describing the phenomenon which no previous studies have dealt with and about which there is little preexisting knowledge in the Palestinian culture.24
The result of this study will add to the knowledge about the response of Palestinian women to IPV which will help the women to advocate agency to build an intervention program and strategies to help them reduce the adverse effects of living in an abusive relationship.
Materials And Methods
Design
This is a hermeneutic phenomenological study in which Van Manen’s six methodical activities were used to guide the researcher to carry out the study.
Participants
Through a purposive sampling method, 11 Palestinian women, with an age range between 20 and 51 years old took part in the study. In the research, the researcher referred to the women’s supporting organizations from all parts of the Gaza Strip, Palestine. The inclusion criteria for the participants included experience of intimate partner violence and participation willingness, living in the Gaza Strip, currently married. The target sample was selected purposively and we tried to achieve maximum variation to gain a deeper understanding of their experience related to the phenomena. The characteristics of the participants are in Table 1.
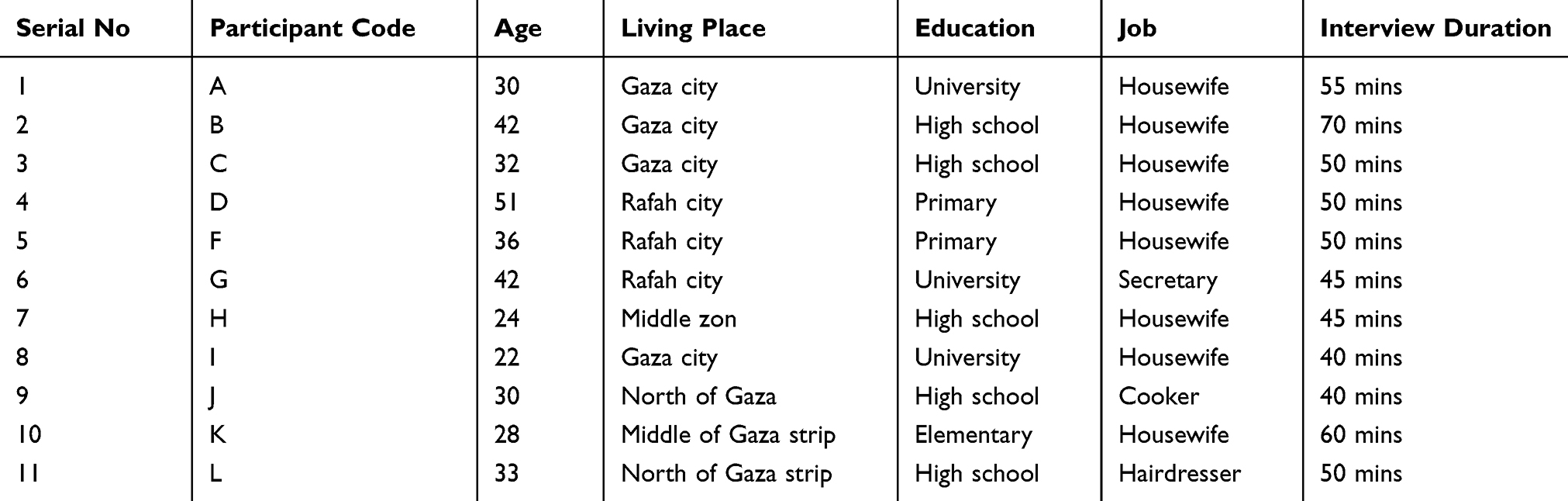 |
Table 1 Characteristic Of Study Participant |
Data Collection
To collect the required data on the participants’ lived experiences of intimate partner violence, in-depth semi-structured interviews were conducted. The potential participants were invited though psychosocial workers who provide counseling services for them in the selected research setting. The participants who showed willingness to participate were recruited in the study. Before commencing the interviews, the researcher provided the participants with necessary explanations about the aim of the study and obtained their written informed consent. The interviews were conducted in a private room at Aisha Institute for Mother and Child, Wefaq Organization of Women and Child Care and Women Health-Jabalia center, aimed at creating a comfortable atmosphere for the participants and making them more willing to give a thorough description of their lived experiences. The interviews started with general descriptive questions (e.g., “can you tell me about your marriage”) and guided through open-ended follow-up questions or requests (e.g., ”please tell me more about your feelings”, “tell me more about your relationship with your husband,” and so on). As a tactic to elicit more detailed information from the participants, after posing each question, the researcher kept silent and gave the participants enough time to think more carefully about the questions, express their feelings and thoughts, and relate their experiences of IPV. Each interview lasted 40 to 70 mins (65 mins on average). The interviews were conducted in the researcher and participants’ mother tongue, Arabic. They were recorded, and then transcribed verbatim, and finally translated into English by an experienced bilingual translator for further analysis.
Data Analysis
In the present hermeneutic phenomenological study, data analysis was carried out through the use of the six methodological steps proposed by Van Manen’s method (1990), which is a commonly utilized hermeneutic approach to analyze qualitative data and reach a high level of abstraction.25 This method consists of 6 methodological steps, which are “Turning to the nature of lived experience”, “Investigating experience as we live it”, “Reflecting on the essential themes which characterize the phenomenon”, “Describing the phenomenon in the art of writing and rewriting”, “Maintaining a strong and orientated relation to the phenomenon”, and “Balancing the research context by considering the parts and the whole”. MAXQDA software V.10 was used to manage data analysis.
Trustworthiness
Trustworthiness of the study was ensured through the accurate description of data analysis procedure and justification of the reliability of the results.26 Moreover, four operational techniques, namely transferability, confirmability, dependability, and credibility were taken into account.27 Dependability and conformability in this study was achieved by the audit trail. In order for an auditor to conduct a thorough audit trail. Transferability of this study was accomplished by selecting participants who experience the phenomena under investigation which is presented in Table 1. Furthermore, the credibility of the findings was achieved by maintaining a prolonged engagement with the data (over 6 months), referring to the women’s support organizations located in the Gaza Strip, communicating effectively with the participants, and employing the member- and peer-checking techniques.28 In addition, the principle researcher is a Ph.D. candidate in reproductive health and has a lot of experience in terms of violence and helping Palestinian women suffering from violence.
Ethical Considerations
For the sake of ethical considerations, the necessary approval was obtained from the Ethics Committee of Tehran University of Medical Sciences (with the ethical approval code: IR.TUMS.VCR.REC.1396.4250) and Helsinki committee for ethical approval in Palestinian health research council (Number: PHRC/HC/358/18). Before the final participants were selected and the interviews conducted, the aim of the study, the data collection method, and the participants’ freedom to quit the study were explained to them. Afterward, written informed consent was obtained from the participants. Moreover, the confidentiality of the collected data was ensured by assigning unique codes for each participant; all of the study’s results were kept with the main investigator. Information collected from the participant cannot be disclosed to other organizations or individuals without the consent of the participant. The recorded interviews were kept anonymous. The participants were navigated to the research setting safely for seeking psychosocial counseling and couple therapy without any hazards.
Results
Data analysis in the present study led the researcher to interpret the participants’ lives with their abusive partner as one main theme labeled “A whole life of threats which was labeled as the main theme that emerged from three sub-themes, namely “live in a physically threatening environment”, “live in a psychologically threatening environment”, and “live in a sexually threatening environment.”
A Whole Life Of Threats
After losing all their hope in life as a result of living with their abusive intimate partners and undergoing different kinds of violence including physical, psychological, and sexual, the women in the present study experience a whole life of threats – physically, psychologically and sexually.
The participants’ lived experiences showed that their lives are always under threat and most of them have considered killing themselves.
Living In A Physical Threatening Environment
One of the most frequent forms of violence, as the results revealed, was physical violence. Almost all of the participants experienced the wish of committing suicide or homicide because of the physical violence inflicted on them, which was mostly in the form of hitting and throwing objects.
In this regard, Participant 1 stated,
I swear if suicide were not taboo, I would surely commit it. He beats me every day and I cannot tolerate it, but I cannot leave him for the sake of my children, my family does not support me, and I do not have a job.
Moreover, Participant 10 revealed,
One day, he entered our room. I was thinking of killing him. I was asleep and was surprised when he splashed my face with water and hit me and said he saw me kiss his father in the kitchen. But he lied as usual and accused me falsely.
Similarly, Participant 3 states,
I wish I could kill him, it was winter. He spattered cold water over me, threw a chair at me and pushed me away with his leg. Then he asked me to leave the house and go to my family’s. It was so hard for me.
Furthermore, Participant 5 reveals, “He was very angry and started beating and throwing the chair at me and the mobile at me. When I complained to my father, he said that I have to tolerate him, he did not support me.”
One of the participants (Participant 6) referred to severe physical violence by her intimate partner and said,
One day he beat me so hard and attacked me with a knife. He lost his mind completely. I was scared of him so much, so I ran to the bathroom and locked the door and said, ‘If you harm or do anything to me, I will kill myself.’
Living In A Psychologically Threatening Environment
The second subtheme that emerged from almost all of the participants’ lived experiences was psychological violence, which included acts that threatened the participants’ self-esteem, dignity and personality.
In this regard, Participant 1 referred to the fact that her husband and his family controlled everything in her life and said,
I feel there is no independence in my life, he deprived me of money, I do not have my own personality, and my life with him destroyed me psychologically. He keeps disrespecting me as a human, which makes me really upset.
Participant 10 also referred to the destruction of her personality by her husband and said, “He made my personality weak. He controls all my thoughts, mind, and erases my personality. He made me feel down.” Moreover, Participant 4 disclosed, “Mistreatment from my husband made me appear a weak and dependent personality in front of my children.”
Revealing that her husband threatened her dignity, Participant 2 said, “He considers me as something he bought from the market, not as his wife.” The same situation was described by Participant 3 who said, “I felt abused and humiliated. I felt like an object he bought with his money.” Similarly, Participant 5 revealed, “I do not feel like a human being. I do not feel that I have rights.”
One of the aspects of psychological violence referred to in this study was threatening women’s dignity. In this regard, Participant 2 said, “Even when I looked pretty and well dressed, he did not reveal that he liked me, he just wanted me to be like a prostitute, which really hurt my personality and dignity.”
Living In A Sexual Threatening Environment
The last subtheme that was referred to by the participants was sexual violence, which posed a threat to their personality and dignity and prevented them from enjoying their intercourse with their husbands.
In this regard, Participant 1 said,
The conflict started at the first night of our marriage when he tried to kiss me and had sex with me, I was shocked, I felt it against my agreement, it was the thing I did not want. I was not aroused.
She continued, “I’m just doing sex to avoid his anger, beating and insulting, he did not care if I liked having sex with him or not or if I enjoyed it or not.”
The participants also revealed that their husbands watched porn videos, which affected their sexual relationship negatively. For example, Participant 1 said, “He watches porn movies, and forces me to watch movies with him and do like them. I cannot do like those porn stars, which is really annoying.”
Moreover, the participants referred to their husbands’ unusual acts during sexual intercourse such as anal sex. In this regard, Participant 2 said, “He forced me to have anal sex with him. He destroyed me. During sex, he asked me to do things I could not do.” And Participant 3 explained, “He asked for anal sex, but I refused.”. Also, Participant 3 said,
I did not feel any intimacy. I did not feel like any woman. I did not feel it was like the relationship between husband and wife. It is like rape. During the day, he was beating and insulting me, and in the night, he forced me to have sex with him.
Additionally, Participant 11 states, “He made me drink alcohol, exposed me to drug abuse, and forced me to anal sex, he destroyed me.”
Discussion
Analyzing the transcripts of lived experiences of the participants who suffered from IPV revealed that they drowned in violence, and their whole lives were under threat as a result of their intimate partners’ acts of violence which included physical, psychological, and sexual violence. When individuals lack sources of power such as professional status or income, they might resort to violence to obtain greater power in their relationships as it is presented in previous studies.29 Rigidity in gender role can lead to the conversion of emotions into anger which will ultimately result in violent acts.30
Suicide, which is considered by almost all IPV victims to be the severest consequence of violence by an intimate partner. Four of the participants in this study disclosed that they would kill themselves if suicide were not forbidden by Islam. Women suffering from IPV usually resort to suicide or at least consider committing it when they find themselves quite desperate and hopeless. This finding is also reported in other studies.31,32 Our findings are congruent with other studies concluding that thinking of or committing suicide can be the result of prolonged depression and addiction to alcohol and narcotics.33 The results of the present study also showed that the participants had suffered from IPV from the very beginning of their marriage, and their failure to change the situation or leave the abusive partner encouraged them to think of suicide.
As disclosed by the participants of the present study, they were suffering from physical violence by their intimate partners. This type of violence ranged from hitting and beating to throwing things at them and threatening them with a knife. Such acts of violence can lead to numerous physical pains and problems. Experiencing physical abuse in an intimate relationship significantly affects the psychological well-being of female victims and increases the probability of depression, anxiety, post-traumatic stress disorder (PTSD) and drug abuse.8,34 Our results are supported through a study that indicates that a prolonged exposure to psychological violence reported poorer mental health than physical violence.35 Our findings tally with reports on physical violence made by a similar study.36
Psychological violence was the most frequent type of IPV in the present study. This type of violence usually happened orally by cursing, shouting, and yelling, which hurt the participants’ personality, dignity, self-esteem, and religiosity. In their study, a similar investigation referred to this type of violence as the most frequent kind of IPV. Psychological violence was also reported in other studies.37,38 Consequences of this type of IPV can affect the victim mentally, leading to post-traumatic stress disorder, substance abuse, sleep disorders, phobias, nervousness, and hypersensitive startle responses.7,39 According to relevant research studies, women who are provided with psycho-educational support from counseling centers usually have higher self-esteem, self-efficacy, coping capacity, and assertiveness but lower levels of exposure to the negative consequences of violence.40,41
The last type of IPV the participants of the present study referred to was sexual violence, which almost all of the participants had experienced. They reported that their intimate partner showed weird sexual behaviors such as forcing their partners to act like porn stars, which hurt their personality and dignity and was against their values. Similar findings were reported by previous studies.36,37 Palestinian culture, which is a traditional culture, has beliefs and norms that promote men’s dominant role in sexual relationships.42
Despite suffering IPV deeply and unbearably, the participants of the present study said that they cannot leave their abusive partner. They attributed their decision to stay to personal and cultural reasons. First is their concern and worry about the future of their children with their abusive father. Second is the lack of support from both their families and society and their financial dependence on their abusive partner. A similar finding was reported by other researchers.17,18,43–45
Growing evidence are being uncovered on the effect of economic strengthening and gender transformative interventions to reduce women’s experiences of violence.46 This indicates that couple therapy can be an effective way to prevent intimate partner violence in certain situations.47
Conclusion
The results of the present study revealed that the participating Palestinian women are suffering from IPV in physical, psychological, and sexual forms which negatively influence their physical and mental health. Generalizability of the study’s result is not applicable in the qualitative study and it is considered one of the study’s weaknesses. However, despite suffering from IPV deeply, they choose to stay with their abusive partner because of their children, lack of support, and financial dependence. Therefore, to help such women deal with their situation and enhance the quality of their lives, their physical and mental health, they need to be heard by health officials, so in the future, the government could provide couple therapy and psycho-educational support in different counseling centers, which would promote their self-esteem, self-efficacy, and coping capacity. Establishing special psychosocial programs should be available to the wives of drug addicts who need psychosocial support and guidance to reduce the risk of exposure to addiction. In future research, we will need to study the role of psycho-educational support in different counseling centers in promoting self-esteem, self-efficacy, and coping capacity of violence survivor.
Acknowledgments
The authors would like to thank all the selected participants for their participation in our study. Special thanks to Aisha Institute for Mother and Child, Wefaq Organization of Women and Child Care and Women Health-Jabalia center for facilitating the data collection process.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Modi MN, Palmer S, Armstrong A. The role of violence against women act in addressing intimate partner violence: a public health issue. J Women’s Health. 2014;23(3):253–259. doi:10.1089/jwh.2013.4387
2. Rhodes KV, Houry D, Cerulli C, Straus H, Kaslow NJ, McNutt L-A. Intimate partner violence and comorbid mental health conditions among urban male patients. Ann Fam Med. 2009;7(1):47–55. doi:10.1370/afm.936
3. WHO. Global and Regional Estimates of Violence Against Women: Prevalence and Health Effects of Intimate Partner Violence and Non-Partner Sexual Violence. World Health Organization; 2013.
4. Thabet AAT, Victoria AA, Vostanis T. PTSD, depression, and anxiety among Palestinian women victims of domestic violence in the Gaza Strip. BJESBS. 2015;11(2):1–13.
5. Rada C. Violence against women by male partners and against children within the family: prevalence, associated factors, and intergenerational transmission in Romania, a cross-sectional study. BMC Public Health. 2014;14(1):129. doi:10.1186/1471-2458-14-129
6. Postmus JL, Huang -C-C, Mathisen-Stylianou A. The impact of physical and economic abuse on maternal mental health and parenting. Child Youth Serv Rev. 2012;34(9):1922–1928. doi:10.1016/j.childyouth.2012.06.005
7. Karakurt G, Smith D, Whiting J. Impact of intimate partner violence on women’s mental health. J Fam Violence. 2014;29(7):693–702. doi:10.1007/s10896-014-9633-2
8. Lawrence E, Orengo-Aguayo R, Langer A, Brock RL. The impact and consequences of partner abuse on partners. Partner Abuse. 2012;3(4):406–428. doi:10.1891/1946-6560.3.4.406
9. Peek-Asa C, Wallis A, Harland K, Beyer K, Dickey P, Saftlas A. Rural disparity in domestic violence prevalence and access to resources. J Women’s Health. 2011;20(11):1743–1749. doi:10.1089/jwh.2011.2891
10. Ackerman J, Love TP. Ethnic group differences in police notification about intimate partner violence. Violence Against Women. 2014;20(2):162–185. doi:10.1177/1077801214521327
11. Katiti V, Sigalla GN, Rogathi J, Manongi R, Mushi D. Factors influencing disclosure among women experiencing intimate partner violence during pregnancy in Moshi Municipality, Tanzania. BMC Public Health. 2016;16(1):715. doi:10.1186/s12889-016-3345-x
12. Walz T A comparative analysis of intimate partner abuse among ever-married women in egypt and India. 2014.
13. Gashaw BT, Schei B, Magnus JH. Social ecological factors and intimate partner violence in pregnancy. PLoS ONE. 2018;13(3):e0194681. doi:10.1371/journal.pone.0194681
14. Vameghi R. Amir Ali Akbari S, Majd AlaviH, Sajedi F, Sajjadi H. The comparison of socioeconomic status, perceived social support and mental status in women of reproductive age experiencing and not experiencing domestic violence in Iran. J Inj Violence Res. 2018;10(1):35–44.
15. Varshney M, Mahapatra A, Krishnan V, Gupta R, Deb KS. Violence and mental illness: what is the true story? J Epidemiol Community Health. 2016;70(3):223–225. doi:10.1136/jech-2015-205546
16. Bell KM, Naugle AE. Understanding stay/leave decisions in violent relationships: a behavior analytic approach. Behav Social Issues. 2005;14(1):21–45. doi:10.5210/bsi.v14i1.119
17. Dufort M, Gumpert CH, Stenbacka M. Intimate partner violence and help-seeking–a cross-sectional study of women in Sweden. BMC Public Health. 2013;13(1):866. doi:10.1186/1471-2458-13-866
18. Sigalla GN, Mushi D, Gammeltoft T. “Staying for the children”: the role of natal relatives in supporting women experiencing intimate partner violence during pregnancy in northern Tanzania–a qualitative study. PLoS ONE. 2018;13(6):e0198098. doi:10.1371/journal.pone.0198098
19. Catani C, Schauer E, Neuner F. Beyond individual war trauma: domestic violence against children in Afghanistan and Sri Lanka. J Marital Fam Ther. 2008;34(2):165–176. doi:10.1111/j.1752-0606.2008.00062.x
20. Clark CJ, Everson-Rose SA, Suglia SF, Btoush R, Alonso A, Haj-Yahia MM. Association between exposure to political violence and intimate-partner violence in the occupied Palestinian territory: a cross-sectional study. The Lancet. 2010;375(9711):310–316. doi:10.1016/S0140-6736(09)61827-4
21. Lenze J, Klasen S. Does women’s labor force participation reduce domestic violence? Evidence from Jordan. Fem Econ. 2017;23(1):1–29. doi:10.1080/13545701.2016.1211305
22. Assaf S, Chaban S. Domestic violence against single, never-married women in the occupied Palestinian territory. Violence Against Women. 2013;19(3):422–441. doi:10.1177/1077801213486330
23. Hawcroft C, Hughes R, Shaheen A, et al. Prevalence and health outcomes of domestic violence amongst clinical populations in Arab countries: a systematic review and meta-analysis. BMC Public Health. 2019;19(1):315. doi:10.1186/s12889-019-6619-2
24. Neubauer BE, Witkop CT, Varpio L. How phenomenology can help us learn from the experiences of others. Perspect Med Educ. 2019;8(2):90–97. doi:10.1007/s40037-019-0509-2
25. Lichtman M. Qualitative Research in Education: A User’s Guide: A User’s Guide. Sage; 2012.
26. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
27. Forero R, Nahidi S, De Costa J, et al. Application of four-dimension criteria to assess rigour of qualitative research in emergency medicine. BMC Health Serv Res. 2018;18(1):120. doi:10.1186/s12913-018-2915-2
28. Speziale HS, Streubert HJ, Carpenter DR. Qualitative Research in Nursing: Advancing the Humanistic Imperative. Lippincott Williams & Wilkins; 2011.
29. Conroy AA. Gender, power, and intimate partner violence: a study on couples from rural Malawi. J Interpers Violence. 2014;29(5):866–888. doi:10.1177/0886260513505907
30. Namy S, Carlson C, O’Hara K, et al. Towards a feminist understanding of intersecting violence against women and children in the family. Soc Sci Med. 2017;184:40–48. doi:10.1016/j.socscimed.2017.04.042
31. Cavanaugh CE, Messing JT, Del-Colle M, O’Sullivan C, Campbell JC. Prevalence and correlates of suicidal behavior among adult female victims of intimate partner violence. Suicide Life Threat Behav. 2011;41(4):372–383. doi:10.1111/j.1943-278X.2011.00035.x
32. Bahrami M, Shokrollahi P, Kohan S, Momeni G, Rivaz M. Reaction to and coping with domestic violence by Iranian women victims: a qualitative approach. Glob J Health Sci. 2016;8(7):100. doi:10.5539/gjhs.v8n7p100
33. Dragisic T, Dickov A, Dickov V, Mijatovic V. Drug addiction as risk for suicide attempts. Mater Sociomed. 2015;27(3):188–191. doi:10.5455/msm.2015.27.188-191
34. Antai D. Traumatic physical health consequences of intimate partner violence against women: what is the role of community-level factors? BMC Women’s Health. 2011;11(1):56. doi:10.1186/1472-6874-11-56
35. Friborg O, Emaus N, Rosenvinge JH, Bilden U, Olsen JA, Pettersen G. Violence affects physical and mental health differently: the general population based Tromsø study. PLoS One. 2015;10(8):e0136588–e0136588. doi:10.1371/journal.pone.0136588
36. Haj-Yahia MM, Clark CJ. Intimate partner violence in the occupied Palestinian territory: prevalence and risk factors. J Fam Violence. 2013;28(8):797–809. doi:10.1007/s10896-013-9549-2
37. Judie AB. Jayabharathi B., Sathish Kumar, J. A study of lived female intimate partner violence in Potheri, Kancheepuram District, India. RRJNHS. 2015;1(14):27–30.
38. Lovestad S, Love J, Vaez M, Krantz G. Prevalence of intimate partner violence and its association with symptoms of depression; a cross-sectional study based on a female population sample in Sweden. BMC Public Health. 2017;17(1):335. doi:10.1186/s12889-017-4222-y
39. Lagdon S, Armour C, Stringer M. Adult experience of mental health outcomes as a result of intimate partner violence victimisation: a systematic review. Eur J Psychotraumatol. 2014;5(1):24794. doi:10.3402/ejpt.v5.24794
40. Ahmad ZR, Yasien S, Ahmad R. Relationship between perceived social self-efficacy and depression in adolescents. Iran J Psychia Behav Sci. 2014;8(3):65.
41. Tahmassian K, Moghadam NJ. Relationship between self-efficacy and symptoms of anxiety, depression, worry and social avoidance in a normal sample of students. Iran J Psychia Behav Sci. 2011;5(2):91.
42. Morrell R, Jewkes R, Lindegger G. Hegemonic masculinity/masculinities in South Africa: culture, power, and gender politics. Men Masc. 2012;15(1):11–30. doi:10.1177/1097184X12438001
43. Karakurt G, Silver KE. Emotional abuse in intimate relationships: the role of gender and age. Violence Vict. 2013;28(5):804. doi:10.1891/0886-6708.VV-D-12-00041
44. Baloushah S, Mohammadi N, Taghizadeh Z, Taha A, Farnam F. Learn to live with it: lived experience of Palestinian women suffering from intimate partner violence. J Fam Med Prim Care. 2019;8(7):2332–2336. doi:10.4103/jfmpc.jfmpc_330_19
45. Morse DS, Paldi Y, Egbarya SS, Clark CJ. “An effect that is deeper than beating”: family violence in Jordanian women. Fam Syst Health. 2012;30(1):19–31. doi:10.1037/a0027137
46. Gibbs A, Washington L, Willan S, et al. The stepping stones and creating futures intervention to prevent intimate partner violence and HIV-risk behaviours in Durban, South Africa: study protocol for a cluster randomized control trial, and baseline characteristics. BMC Public Health. 2017;17(1):336. doi:10.1186/s12889-017-4223-x
47. Karakurt G, Whiting K, van Esch C, Bolen SD, Calabrese JR. Couples therapy for intimate partner violence: a systematic review and meta-analysis. J Marital Fam Ther. 2016;42(4):567–583. doi:10.1111/jmft.12178
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.