")
Back to Journals » Infection and Drug Resistance » Volume 16
A Visualized Mortality Prediction Score Model in Hematological Malignancies Patients with Carbapenem-Resistant Organisms Bloodstream Infection
Authors Qian C, Wu Q, Ruan Z, Liu F, Li W, Shi W, Ma L, Peng D, Yin H, Yao L, Li Z, Hong M, Xia L
Received 18 October 2022
Accepted for publication 30 December 2022
Published 7 January 2023 Volume 2023:16 Pages 201—215
DOI https://doi.org/10.2147/IDR.S393932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chenjing Qian,1,* Qiuling Wu,1,* Zhixuan Ruan,2 Fang Liu,1 Weiming Li,1 Wei Shi,1 Ling Ma,3 Danyue Peng,1 Hua Yin,1 Lan Yao,1 Zixuan Li,1 Mei Hong,1,4 Linghui Xia1
1Institute of Hematology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, 430022, People’s Republic of China; 2Faculty of Natural, Mathematical and Engineering Sciences, King’s College, London, UK; 3Department of Clinical Laboratory, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 4Collaborative Innovation Center of Hematology, Soochow University, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mei Hong; Linghui Xia, Institute of Hematology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Jiefang Road No. 1277, Wuhan, Hubei Province, People’s Republic of China, Tel +8613037137937 ; +8618627733999, Email [email protected]; [email protected]
Background: Bloodstream infection (BSI) due to carbapenem-resistant organisms (CROs) has emerged as a worldwide problem associated with high mortality. This study aimed to evaluate the risk factors associated with mortality in HM patients with CROs BSI and to establish a scoring model for early mortality prediction.
Methods: We conducted a retrospective cohort study at our hematological department from January 2018 to December 2021, including all HM patients with CROs BSI. The outcome measured was death within 30-day of BSI onset. Survivor and non-survivor subgroups were compared to identify predictors of mortality. Univariate and multivariate Cox regression analyses were used to identify prognostic risk factors and develop a nomogram.
Results: In total, 150 HM patients were included in the study showing an overall 30-day mortality rate of 56%. Klebsiella pneumonia was the dominant episode. Cox regression analysis showed that pre-infection length of stay was > 14 days (score 41), Pitt score > 4 (score 100), mucositis (score 41), CAR (The ratio of C-reactive protein to albumin) > 8.8 (score 57), early definitive therapy (score 44), and long-duration (score 78) were positive independent risk predictors associated with 30-day mortality, all of which were selected into the nomogram. Furthermore, all patients were divided into the high-risk group (≥ 160 points) or the low-risk group based on the prediction score model. The mortality of the high-risk group was 8 times more than the low-risk group. Kaplan-Meier analysis showed that empirical polymyxin B therapy was associated with a lower 30-day mortality rate, which was identified as a good prognostic factor in the high-risk group. In comparison, empirical carbapenems and tigecycline were poor prognostic factors in a low-risk group.
Conclusion: Our score model can accurately predict 30-day mortality in HM patients with CROs BSI. Early administration of CROs-targeted therapy in the high-risk group is strongly recommended to decrease mortality.
Keywords: carbapenem-resistant organisms, predictive model, nomogram, hematological malignancies, bloodstream infection
Introduction
In recent years, carbapenem-resistant organisms (CROs) infections have become a major global public health problem which is associated with increased mortality up to 50%, prolonged the hospital stay and additional medical costs.1–6 The hematological malignancies (HM) patients and the recipients of hematopoietic stem cell transplant (HSCT) might be particularly vulnerable to CROs infection. Because of intensive myelosuppressive or immunosuppressive-induced gastrointestinal mucositis, prolonged hospitalizations and neutropenia, and frequent use of broad-spectrum antibacterial agents.7 Especially, mucositis induced by chemotherapy promotes bacteria to penetrate through a mucosal barrier into the bloodstream to increase the incidence of CROs bloodstream infection (BSI).5,8 The course of CROs BSI in HM patients is usually abrupt and rapidly develops into shock, disseminated intravascular coagulation (DIC), and multiple organ dysfunction.9 High in-hospital mortality rate (65–100%) for CROs has been found in these highly immunocompromised population.7,10–13 Accurate identification of predictors associated with mortality in BSI patients is critical for early clinical interventions and, thus, improving clinical outcomes.
In this study, we collected the clinical data of 150 HM patients with CROs BSI and compared the clinical characteristics, laboratory tests, and treatment to explore the risk factors for the prognosis. The objective of this study is to established a visualized mortality prediction score model to produce forecasts of mortality in HM patients with CROs BSI and provide a reference for early clinical diagnosis and treatment.
Subjects and Methods
Study Design and Subjects
This study retrospectively reviewed the clinical and microbiological data of inpatient HM patients with CROs BSI from January 2018 to December 2021 in Wuhan Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. We recorded the demographic and clinical variables of patients diagnosed with CROs BSI. Exclusion criteria were age < 18 years and patients with polymicrobial bacteria including methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE) infections, or invasive fungal disease. Recurrent infections were excluded, and only the first CROs BSI episode per patient was included in our analysis. A retrospective cohort study design was employed. The outcome measure was death within 30 days of the first positive blood culture. Survivor and non-survivor subgroups were compared to identify the predictors of mortality. A Cox proportional hazard model was used to analyze the survival data and determine significant risk factors to develop a prediction model. This model was used to create a nomogram for predicting the survival rate of patients for up to 30 days.
The study was approved by the research ethics committee of Union Hospital. Written informed consent was waived due to the anonymized retrospective nature of the analysis.
Data Collection
Demographic and clinical data include gender, age, primary disease status, pre-infection length of stay, HSCT, hypoalbuminemia, mucositis, laboratory findings, empirical antimicrobial use in the 30 days before infection, Pitt bacteremia score at BSI onset, previous history of CROs colonization within 30 days before BSI onset, invasive devices (mechanical ventilation, sputum suction, bladder catheterization) and antimicrobial treatment and outcome. The primary outcome was all-cause 30-day mortality. For statistical purposes, patients discharged as terminally ill (life expectancy <1 week, as estimated by the attending physician) were considered to have died at the time of hospital discharge.14
Bacterial Identification and Drug Sensitivity Test
The isolation and identification of pathogenic bacteria were carried out strictly following the relevant provisions of the National Clinical Laboratory Procedures. Vitek® 2 automated system (France Biomerieux) and matrix-assisted laser-desorption ionization time-of-flight mass spectrometry (Bruker Daltonics Inc., Billerica, Massachusetts) were used to bacterial identification and drug sensitivity tests.15 The identification of drug resistance both by disk diffusion method (K-B method) and broth microdilution (BMD), BMD was used to determine MICs. For tigecycline and colistin, the European Committee on Antimicrobial Susceptibility Testing (EUCAST) breakpoint was used, the rest of antibiotics were interpreted according to the standard of the CLSI document.16,17
Related Definition
The CROs BSI was defined as a BSI documented by blood culture positivity (at least 1 specimen) for a CROs strain and clinical signs of systemic inflammatory response syndrome.18
Previous CROs colonization was defined as patients with CROs isolated from the rectal swab without symptoms and signs of invasive infection.
Neutropenia was defined as neutrophil cells <500 per microlitre of blood.
The ratio of C-reactive protein to albumin (CAR) was calculated using C-reactive protein (CRP) and albumin concentrations.
Antimicrobial exposure was defined as the use of antibiotics for more than 72 hours before CROs BSI.
Appropriate empirical therapy was defined as administering in vitro active antimicrobials against the isolates within 24 h of infection onset and at least 48 h.19
Definitive therapy referred to antimicrobial therapy after the susceptibility testing results were available, defined as appropriate therapy if at least one in vitro active antimicrobial was administered within 7 days of infection and for at least 48 h, or as inappropriate therapy if these criteria were not met.19 Early definitive therapy was considered to administer an in vitro active antimicrobial within 72 h of infection onset.
Long-duration treatment was defined as receiving antimicrobial treatment ≥10 days.
Statistical Analysis
Original data were expressed as number and percentage (n [%]), mean ± standard deviation, and median (interquartile range) due to the different shapes of continuous data collected. We compared patients’ demographic and clinical variables using the chi-square test and Fisher’s exact test. All laboratory indexes were converted to categorical variables according to the reference range, or the cut-off values of the above-combined indexes were identified by X-tile software. We used Kaplan–Meier curves for subgroup analysis. A Cox proportional hazard model was used to determine risk factors for mortality. The variables with P < 0.05 in univariate analysis were incorporated into the Cox proportional hazard model for multivariate analysis. We attempted to establish a parsimonious prediction model based on risk factors at the onset.
The candidate risk factors were included in the Cox proportional hazard model. The models were checked by a variance inflation factor (VIF) and C-index. All analyses were performed by R statistical software 4.0.1. A two-sided P < 0.05 indicated that the difference was statistically significant
Study Results
Microbiological Characteristics
The flow procedure is shown in Figure 1A. 453 HM patients with positive Gram-negative BSI were first included in this study, and 303 patients were classified into the Carbapenem-sensitive organisms (CSOs) BSI group and finally excluded from our study. The data from the remaining 150 patients were further analyzed, and the top three predominant pathogens of CROs BSI were Klebsiella pneumoniae (48.0%), and Pseudomonas aeruginosa (15.3%), Escherichia coli (14.0%), and Acinetobacter baumannii (14.0%). The other strains were Enterobacter cloacae (4.0%), Klebsiella oxytoca (2.3%), Salmonella Dublin (0.6%), Enterobacter polymeris (0.6%), Aeromonas hydrophila (0.6%) and Aeromonas sobria (0.6%) (Figure 1B).
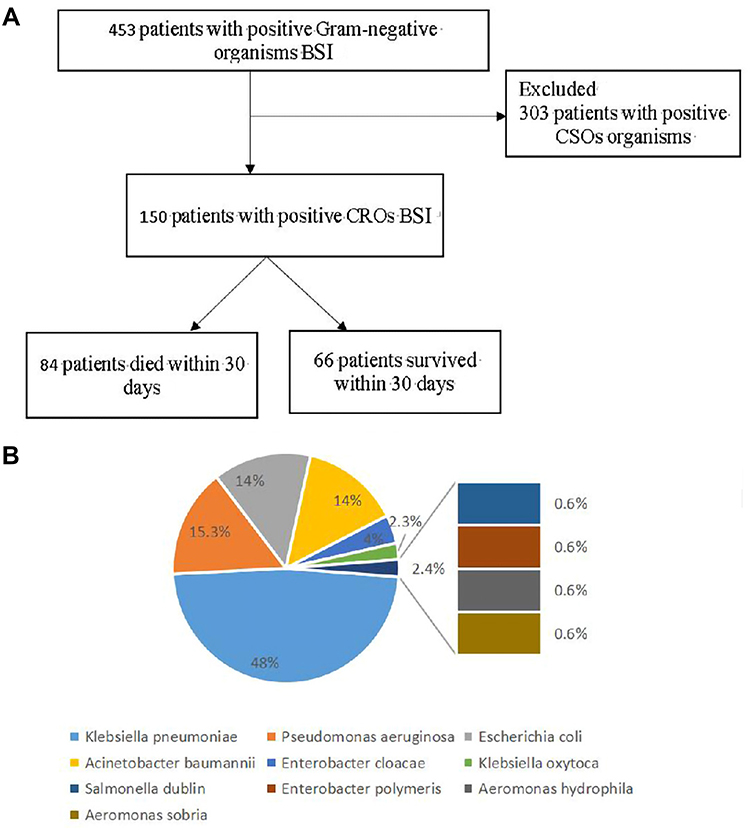 |
Figure 1 (A) Screening algorithm of the HM patients with Carbapenem-resistant Gram-negative organisms Bloodstream infection. In all, 453 hospitalized patients had positive Gram-negative organisms BSI, and a total of 150 eligible, unduplicated cases were recruited into this study. (B) Distribution of Carbapenem-resistant Gram-negative bacteria BIS. |
Baseline and Treatment Characteristics
150 patients with BSI caused by CROs were observed during the study period. As shown in Table 1, 59.3% (n=89) of the patients were males. In terms of disease distribution, acute myelocytic leukemia (AML) was the predominant primary disease (n=62, 41.3%). Bacterial classification included CRE (n=106, 70.7%), CARA (n=23, 15.3%), and CRAB (n=21, 14.0%). At the time of diagnosis, 30% of the patients presented with septic shock. Additionally, patients who died had worse clinical and laboratory indicators (higher temperature/CRP/procalcitonin (PCT) and lower neutrophil/hemoglobin/platelet count), while patients who survived had a longer length of antibiotic therapy (p<0.05). A total of 39.3% (n=59) of the patients accepted appropriate empirical therapy, and 54.7% (n=82) of the patients accepted early definitive therapy.
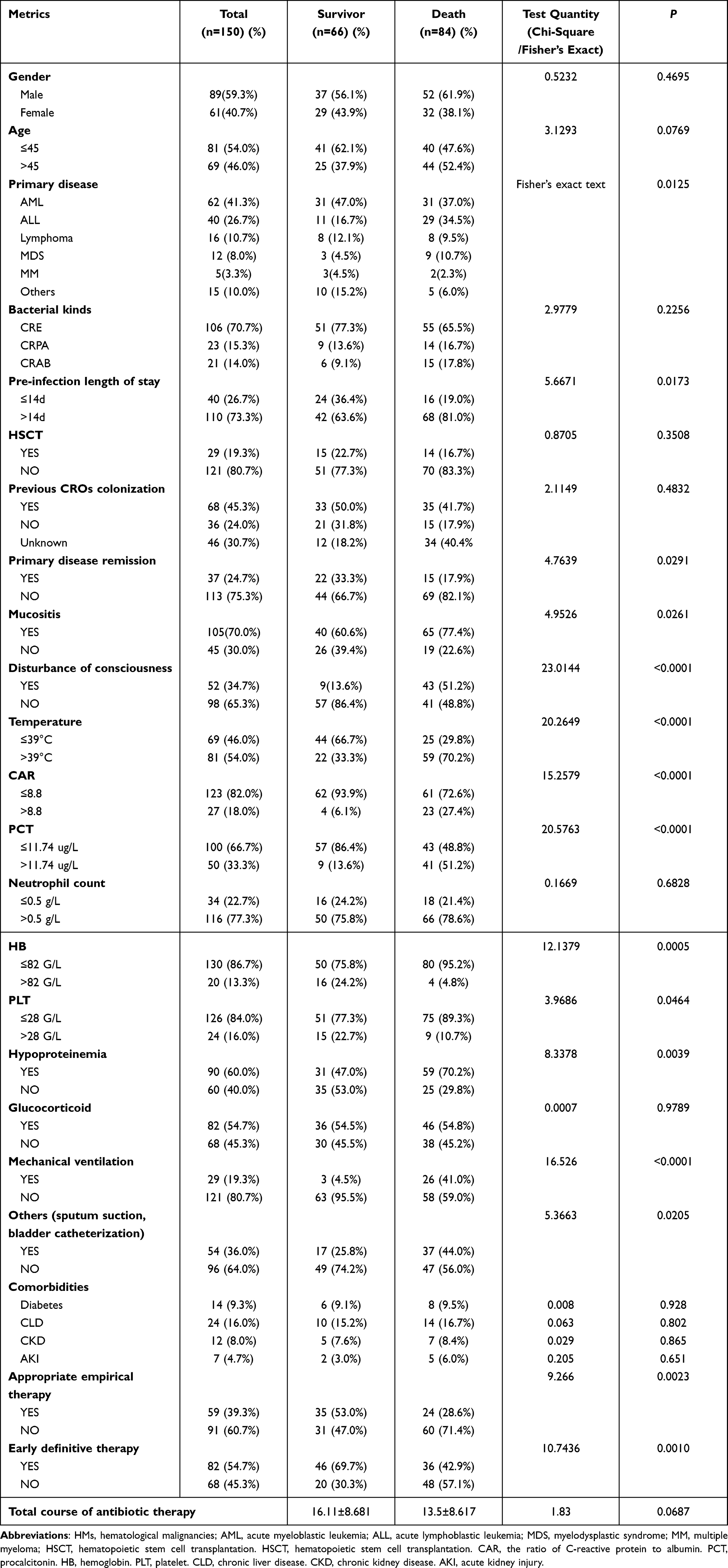 |
Table 1 Basic Clinical Characteristics of HM Patients with CROs BSI |
Risk Factors of Mortality
The univariate analysis results indicated the variables associated with mortality as follows: age, pre-infection length of stay >14 days, primary disease status, Pitt score >4, mucositis, laboratory findings including CAR >8.8, PCT >11.74 ug/L, HB <82 G/L, PLT <28 G/L, hypoalbuminemia, appropriate empirical therapy, early definitive therapy, long-duration treatment and invasive procedures (sputum suction, bladder catheterization) (p<0.05).
The statistically significant risk factors from the univariate analysis above were chosen for further multivariate analysis. Early definitive therapy (HR=0.52; 95% CI, 0.32–0.86), long-duration treatment (HR=0.37; 95% CI, 0.21–0.64) were independent favorable prognostic factors for 30-day mortality, while pre-infection length of stay >14 days (HR=1.80; 95% CI, 1.02–3.17), Pitt score >4 (HR=3.32; 95% CI, 1.02–3.17), mucositis (HR=2.11; 95% CI, 1.20–3.70) and CAR >8.8 (HR=1.80; 95% CI,1.02–3.17) were independent negative prognostic factors for 30-day mortality (Table 2).
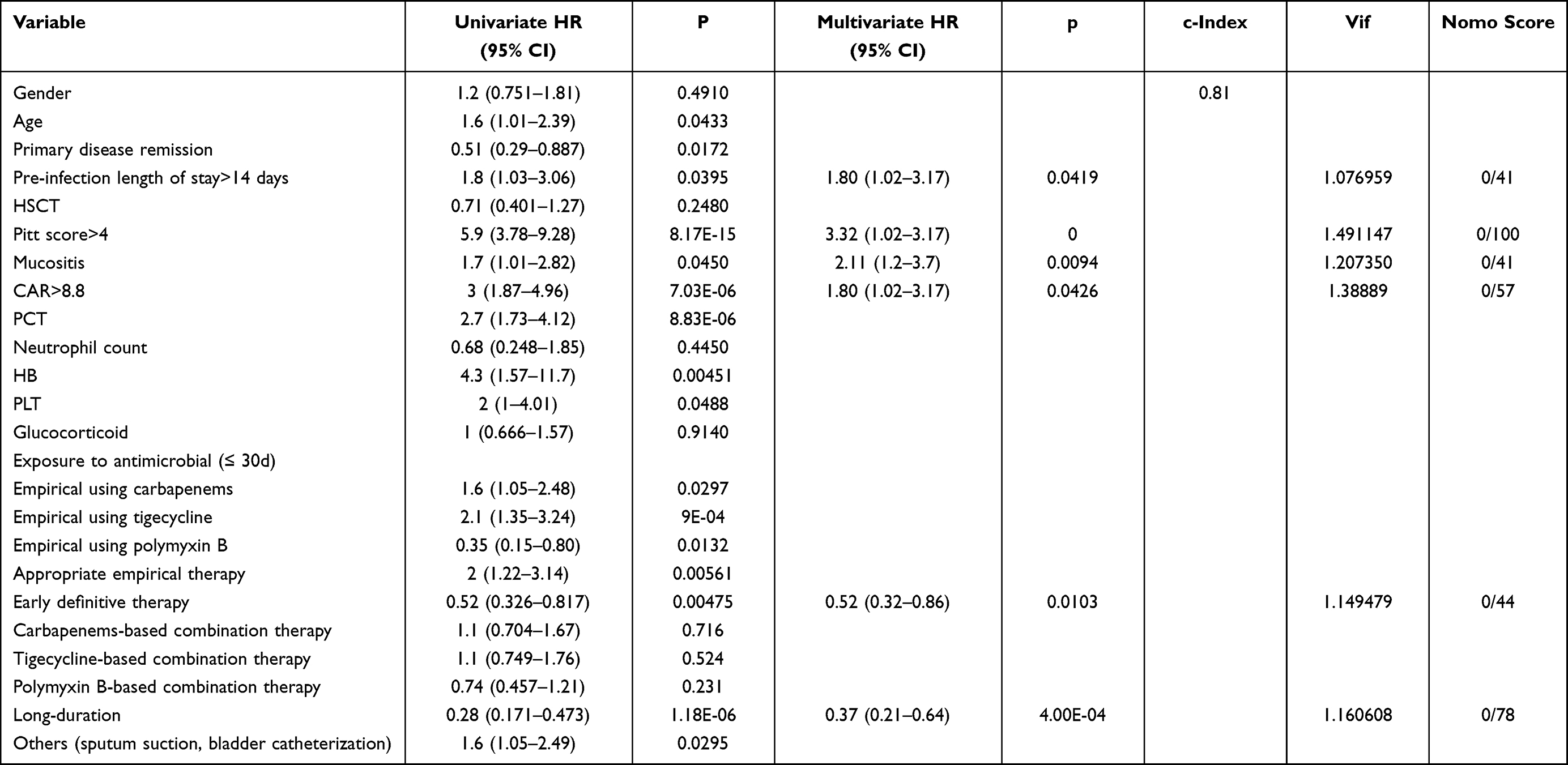 |
Table 2 Univariate and Multivariate Analysis of Factors Associated with All-Cause 30-Day Mortality of 150 HM Patients with with CROs BSI |
Establishment of a Risk Prediction Score Model of 30-Day Mortality in 150 HM Patients with CROs BSI
In addition, we also identified potential predictors with the highest coefficients based on permutation importance using the random forest algorithm. It was found that pre-infection length of stay >14 days (variable importance (VI), 2.12), Pitt score >4 (the most important VI, 16.05), mucositis (VI, 2.56), CAR>8.8 (VI, 3.60), early definitive therapy (VI, 4.39), and long-duration treatment (VI, 11.47) were independent predictors for 30-day mortality (Table 2). Then, the above six independent predictors of 30-day mortality were integrated into a 30-day mortality rate estimation nomogram (Figure 2A). The C-index of the nomogram was 0.81 (Table 2). The predictive performance of the nomogram, as measured by AUC value was 0.893, 0.901 and 0.885 for the 7-day,14-day, and 28-day OS, respectively (Figure 2B–D). Our study found that calibration plots showed good agreement between the predictions and actual observations (Figures 2E–G). Internal bootstrap validation is shown in Figure S1A. The nomogram by 1000 times bootstrap showed AUC of 0.889, 0.894, and 0.876 for the 7-day, 14-day, and 28-day OS, respectively, similar to the original prediction model. The Decision curve analysis (DCA) is presented in Figure S1B. In addition, the time-dependent AUC was used to determine whether the AUC or prediction accuracy changed significantly over time (Figure S1C). ROC analysis was conducted to evaluate the prognosis of patients, and the AUC was calculated. X-title software was used to determine the optimal cut-off point with the highest sensitivity and specificity to discriminate between low-risk and high-risk patients. With the threshold score of 160 for the 30-day mortality nomogram, 101 patients with total points ≤160 were defined as the low-risk group, and 49 patients>160 were defined as the high-risk group. The 30-day mortality of HM patients with CROs BSI in the high-risk group was significantly higher than that in the low-risk group (all patients: 33% vs 67%, p < 0.0001; HR: 8.28, 95% CI: 5.14–13.34) (Figures 2H).
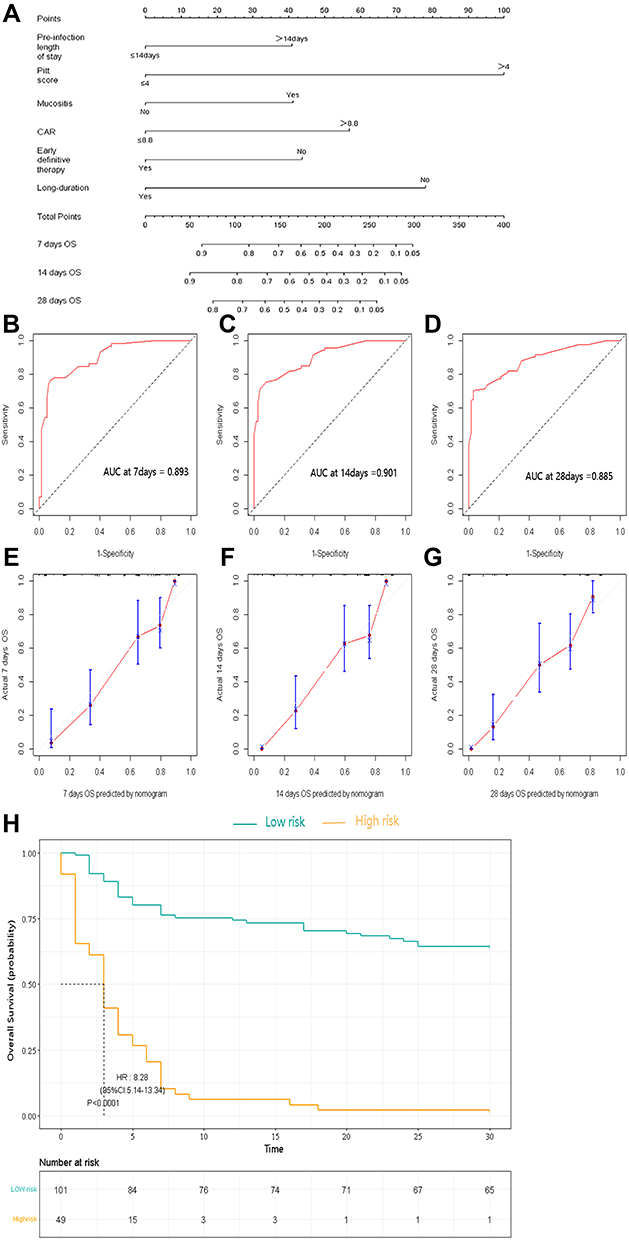 |
Figure 2 (A) A nomogram predicts the 7-day,14-day, and 28-day OS in 150 HM patients with CROs BSI. (B–D) The AUC of the nomogram for the 7-day,14-day, and 28-day OS. (E–G) The calibration curves for predicting the 7-day,14-day, and 28-day OS. (H) Kaplan-Meier survival curves of 30-day mortality. The diagonal gray lines could help to judge the agreement between predictions and actual observations in the AUC and calibration curves. The dotted lines drawn on the Kaplan–Meier curves were used to reveal the median survival time of patients when 50% of patients had the event. The data in the tables showed the number at risk and a cumulative number of events at specific time points. |
Effect of Different Empirical Antimicrobial Regimens on Different Risk Population
Different antimicrobial therapy had different effects on treatment outcomes, but the optimal antimicrobial therapy for CROs BSI has not been determined. Kaplan–Meier analysis showed that the patients who received empirical carbapenems and empirical tigecycline had poor prognostic (p=0.0297/p<0.0001) (Figure 3A and B), while the patients who received empirical polymyxin B had good prognostic (p=0.0132) (Figure 3C).
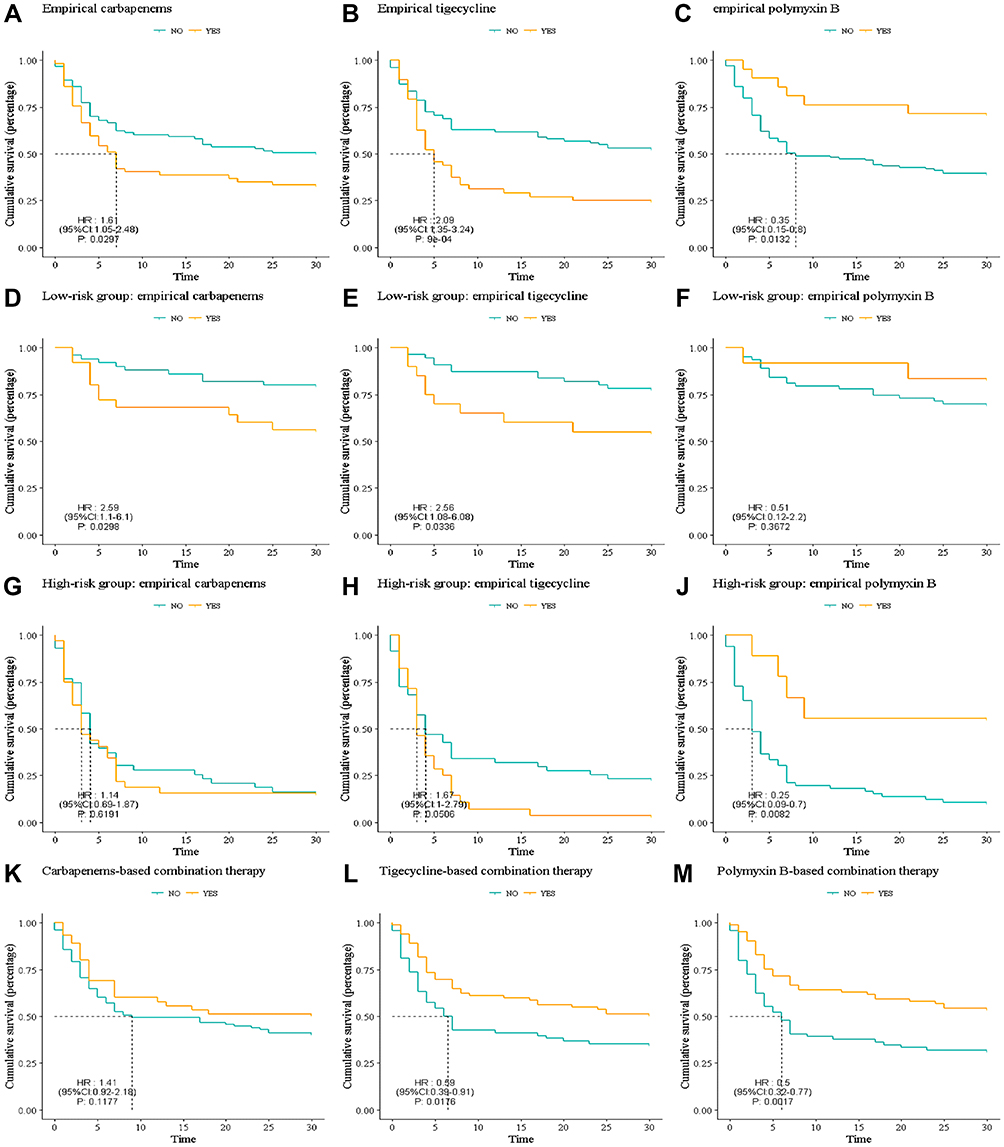 |
Figure 3 Kaplan–Meier curves showing the impact of different antimicrobial treatments. (A–C) The patients who received empirical carbapenems and empirical tigecycline had a 30-day poor prognostic, while the patients who received empirical polymyxin B had a 30-day survival benefit. (D–F) In the low-risk group, the patients who received empirical carbapenems and empirical tigecycline had a 30-day poor prognostic, and there was no difference in 30-day mortality among patients who received empirical polymyxin B. (G–I) In the high-risk group, there was no difference in 30-day mortality among patients who received empirical carbapenems and empirical tigecycline, while the patients who received empirical polymyxin B had a 30-day survival benefit.(K–M) The patients who received the carbapenem-based combination therapy had no difference in 30-day mortality. The patients who received tigecycline-based combination therapy had a 30-day dead benefit, and the patients who received polymyxin B-based combination therapy had a 30-day survival benefit. |
According to our novel risk predictive score model, we further evaluated the effect of empiric antimicrobial regimens on different risk populations. In the low-risk group, the patients who received empirical carbapenems and empirical tigecycline had poor prognostic (p=0.0298/p=0.0336) (Figure 3D and E), and there was no difference in 30-day mortality among patients who received empirical polymyxin B (p=0.3672) (Figure 3F). In the high-risk group, there was no difference in 30-day mortality among patients who received empirical carbapenems and empirical tigecycline (p=0.6191/p = 0.0506) (Figure 3G and H), while the patients who received empirical polymyxin B had good prognosis (p=0.0082) (Figure 3I). Therefore, polymyxin B-based therapy should be selected as early as possible in the patients in high-risk groups.
We further assessed the effects of combinational therapy. There was no difference in 30-day mortality among 60 patients who received the carbapenem-based combination therapy (p=0.1177) (Figure 3K). The patients who received tigecycline-based combination therapy had a 30-day dead benefit (p=0.0176) (Figure 3L). The patients who received polymyxin B-based combination therapy had a 30-day survival benefit (p=0.0017) (Figure 3M).
Discussion
Risk factors for CROs infection in HM patients include: CROs colonization, previous CROs infections, previous use of carbapenems, enzyme inhibitor compound agents, quinolones, aminoglycosides and cephalosporins, elderly patients, ICU admission, prolonged neutropenia (≥7d).20–22 Previous studies have reported that multiple clinical factors, including underlying medical conditions, previous antibiotic exposure, and severity of bacteremia, were independently associated with poor outcomes in patients with BSI.23,24 CROs BSI is associated with high mortality in HM patients with immunodeficiency, and many factors could affect the prognosis of patients, including septic shock, the severity of illness, pathogen characteristics, and the late onset of empirical antibiotic therapy.25,26 The current retrospective study found that pre-infection length of stay >14 days, Pitt score >4, mucositis, CAR >8.8, early definitive therapy, and long-duration treatment were independent predictors for 30-day mortality. A score of ≥160 suggests that HM patients with CROs BSI will have higher 30-day mortality. The results suggest that high-risk group patients had approximately 8 times the odds of dying within 30 days compared to patients in the low-risk group after accounting for the severity of illness on day 1 of bacteremia.
PCT is a commonly used inflammation-related biomarker for the diagnosis of bacterial infections. However, it has limited significance for diagnosing BSI in neutropenia patients since they have an impaired capacity for generating PCT compared with nonneutropenic patients.27 CRP is one of the acute-phase proteins released in inflammation. It is used for the diagnosis and follow-up of sepsis and for determining treatment efficacy.28,29 Prat et al30 found that CRP was more sensitive than PCT to predict bacteremia in patients with febrile neutropenia. Albumin is a negative acute-phase reactant. In critical care, the hypoalbuminemia grade correlates with infection-triggered inflammation.31 Using a ratio between CRP and albumin would provide a variable capable of merging the information provided by CRP and albumin into an index that correlated positively with infection, ie, a higher ratio indicates higher inflammatory status.32 CAR has also been shown to correlate with infection severity, a useful score based on inflammation and nutrition, reflecting not only systemic inflammation status but also nutritional status.33 CAR has recently been a prognostic marker for various solid tumors and chronic lymphocytic leukemia (CLL).34–36 Ranzani et al37 reported that on admission to the hospital, the CAR >2 showed the greatest sensitivity and specificity in predicting mortality at 90 days among patients with severe sepsis or septic shock. A retrospective cohort study showed CAR > 5.09 had the best sensitivity and specificity in predicting 180-day mortality in patients with severe sepsis and septic shock.38 Our study revealed an association of CAR > 8.8 with higher mortality, which might also reflect the severity of deaths caused by CROs BSI. Additional prospective studies with larger populations involving multiple centers are necessary to accurately evaluate the significance of CAR as a predictor of mortality.
In our study, an early definitive therapy (≤72h) and long-duration treatment (≥10 days) were independent favorable prognostic factors for 30-day mortality. Similarly, Wasan Katip et al found that patients who received long course of colistin therapy (≥14 days) had presented greater clinical and microbiological responses and lower 30-day mortality.39 Timely and appropriate antimicrobial therapy is critically important for treating patients with BSI.40,41 Delayed administration of definitive antibiotic therapy is associated with high mortality rates in patients with bacteremia and sepsis,42–44 and the probability of death increases with the number of hours of delay of antibiotic administration.44 Previous studies have shown that more rapid completion of a 3-h bundle of sepsis care and rapid administration of antibiotics was associated with lower risk-adjusted in-hospital mortality.40 Falcone et al suggested that appropriate antibiotic therapy was preferably initiated within the first 24-h after collection of the blood culture. Conversely, the risk of death progressively increased when appropriate antibiotic therapy was started 24–48 h (mortality rate 37.5%), 48–72 h (mortality rate 57.1%), and > 72 h (mortality rate 66.7%) from the index blood culture collection.45 However, the average time to obtain a blood culture result requires at least 24–48 hours.6,39 Recently, new laboratory methods for more rapid bacterial identification and antibiotic resistance, including NTS and carba have been developed and allow early administration of targeted definite antimicrobial treatment, thus potentially improving clinical outcomes.46
Appropriate empirical therapy is key to decreasing mortality.47,48 In our study, patients treated with appropriate empirical therapy had a better prognosis than those treated with inappropriate empirical therapy, similar to those reported in other studies.49 However, the optimal antimicrobial treatment for CROs BSI has not been determined. According to current guidelines,50 patients in our study received standard dose tigecycline (SDT) during empirical therapy of infection and once patients with a definitive diagnosis of CROs BSI, high dose tigecycline (HDT) were used. In our study, in all patients and those in the low-risk group, the empirical use of tigecycline was associated with higher mortality. Tigecycline is a bacteriostatic rather than bactericidal agent, which may limit its effectiveness in immunocompromised patients, and is not active against Pseudomonas aeruginosa.51 The US Food and Drug Administration (FDA) has approved its use for complicated intra-abdominal infections, skin and skin structure infections, and community-acquired pneumonia.52 However, tigecycline’s role in treating BSI is controversial because of its low serum concentration with standard dosing.53,54 In a non-comparative study, tigecycline appeared to be safe and efficacious in patients with difficult-to-treat serious infections caused by resistant Gram-negative organisms, the clinical cure rate was 72.2%, and the microbiological eradication rate was 66.7%.55 However, in some randomized trials, tigecycline increased mortality risk and clinical failure.56,57 The excess risk of death in the subset of tigecycline patients with BSI might be attributed to the persistence of bacteremia owing to low tigecycline serum concentrations, higher bacterial load in patients with primary bacteremia and/or insufficient dose.58 Besides, tigecycline is associated with a higher frequency of adverse events, especially vomiting, nausea, and acute pancreatitis,59,60 indicating that surveillance of adverse events from the digestive system is needed during treatment.
Our study found that the empirical use of polymyxin B was associated with survival benefits in all patients and those in the high-risk group. Polymyxin B is an antibiotic of the polymyxin family that demonstrated good results in the past decade for the treatment of multidrug-resistant (MDR) Gram-negative bacteria (GNB).61,62 In addition to the direct antibacterial activity, polymyxin B has potent anti-endotoxin activity.63 It has been the preferred agent in many hospitals in China based on its superior PK characteristics and decreased potential to cause nephrotoxicity.64 A retrospective study from China showed that for patients with carbapenem-resistant Klebsiella pneumonia BSI, irrespective of drug dosage and treatment duration, the early use of polymyxin B could effectively eliminate bacteria, improving 30-day and overall mortality.65 A more recent Japanese multicentre study showed that polymyxin B treatment of sepsis in 354 patients significantly reduced all-cause mortality.66 Our results suggest that polymyxin B-based therapy should be used as a first-line agent for the high-risk population in HM patients with CROs BSI. Some studies have found that combination antimicrobial therapy is preferred to monotherapy, particularly in severely ill patients.67–69 In our study, not only empirical using polymyxin B, but also, combination therapy based on polymyxin B had a 30-day survival benefit, which was similar to previous reports.25,68 Previous study showed the survival rate of patients in the LD colistin methane sulfonate (CMS) group was 1.7 times (adjusted HR) of those in the non-LD group (p=0.006), but renal function should be closely monitored in view of severe nephrotoxicity caused by polymyxin B.70 Likewise, LD polymyxin B were used in our study. Notably, an increasing number of novel potent molecules are being developed for CRO therapy, such as the novel β-lactam/β-lactamase inhibitor combinations, ceftazidime/avibactam, meropenem/vaborbactam, and imipenem/cilastatin/relebactam.71–75 Their role in the treatment of high-risk population should be furtherly studied.
This study has existing limitations, including its retrospective, observational design. First, we did not identify the enzyme type of the CROs strain, and the specific carbapenemases (KPC, OXA, etc.) were not identified in our studied population. Second, an external validation cohort is needed to assess its discriminatory ability and goodness of fit. Additionally, a limited number of samples were included. Large sample data and randomized controlled studies are needed to study the clinical characteristics and different antimicrobial therapeutic effects on patients with CROs BSI. Finally, it needs to be confirmed whether the established score model is reproducible through relevant prospective studies. In summary, Patients can be divided into low- and high-risk groups based on our mortality prediction score model. Therefore, in high-risk group, the early administration of proper CROs-targeted therapy is strongly recommended to decrease their mortality, especially polymyxin B-based combination therapy. On the contrary, for those patients with low-risk mortality, common treatment and close monitor might be enough. Taken together, our study contribute to the improvement of clinicians’ awareness about rational timing of treatment and precision drug selection, which can avoid antibiotic abuse, lower bacterial resistance rate and decrease healthcare costs.
Ethics Statements
The study was approved by the Union Hospital ethics committee for health research. Written informed consent was waived by the Union Hospital ethics committee for research in health due to the anonymized retrospective nature of the analysis. And this study followed the guidelines outlined in the Declaration of Helsinki.
Funding
This study was supported by the National Natural Science Foundation, P.R China (no. 81570193 and no. 81770219).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kois AK, Nicolau DP, Kuti JL. Unresolved issues in the identification and treatment of carbapenem-resistant Gram-negative organisms. Curr Opin Infect Dis. 2020;33(6):482–494. doi:10.1097/qco.0000000000000682
2. McConville TH, Sullivan SB, Gomez-Simmonds A, Whittier S, Uhlemann A-C, Lazzeri C. Carbapenem-resistant Enterobacteriaceae colonization (CRE) and subsequent risk of infection and 90-day mortality in critically ill patients, an observational study. PLoS One. 2017;12(10):e0186195. doi:10.1371/journal.pone.0186195
3. Lee H-J, Choi J-K, Cho S-Y, et al. Carbapenem-resistant Enterobacteriaceae: prevalence and risk factors in a single community-based hospital in Korea. Infect Chemother. 2016;48(3):166–173. doi:10.3947/ic.2016.48.3.166
4. Hovan MR, Narayanan N, Cedarbaum V, Bhowmick T, Kirn TJ. Comparing mortality in patients with carbapenemase-producing carbapenem resistant Enterobacterales and non-carbapenemase-producing carbapenem resistant Enterobacterales bacteremia. Diagn Microbiol Infect Dis. 2021;101(4):115505. doi:10.1016/j.diagmicrobio.2021.115505
5. Blijlevens NM, Donnelly JP, De Pauw BE. Mucosal barrier injury: biology, pathology, clinical counterparts and consequences of intensive treatment for haematological malignancy: an overview. Bone Marrow Transplant. 2000;25(12):1269–1278. doi:10.1038/sj.bmt.1702447
6. Zhang S, Zhang X, Yu W, Lin Z, Chen D. Infection biomarkers in assisting the judgement of blood stream infection and patient prognosis: a retrospective study incorporating principal components analysis. Ann Transl Med. 2020;8(23):1581. doi:10.21037/atm-20-3425
7. Satlin MJ, Jenkins SG, Walsh TJ. The global challenge of carbapenem-resistant Enterobacteriaceae in transplant recipients and patients with hematologic malignancies. Clin Infect Dis. 2014;58(9):1274–1283. doi:10.1093/cid/ciu052
8. Elting LS, Cooksley C, Chambers M, Cantor SB, Manzullo E, Rubenstein EB. The burdens of cancer therapy. Clinical and economic outcomes of chemotherapy-induced mucositis. Cancer. 2003;98(7):1531–1539. doi:10.1002/cncr.11671
9. Chakrabarti SR, Gupta S, Kumar RS, et al. Gut colonization with carbapenem resistant Enterobacteriaceae adversely impacts the outcome in patients with hematological malignancies: results of a prospective surveillance study. Mediterr J Hematol Infect Dis. 2018;10(1):e2018025. doi:10.4084/mjhid.2018.025
10. Stewardson AJ, Marimuthu K, Sengupta S, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study. Lancet Infect Dis. 2019;19(6):601–610. doi:10.1016/S1473-3099(18)30792-8
11. Falagas ME, Tansarli GS, Karageorgopoulos DE, Vardakas KZ. Deaths attributable to carbapenem-resistant Enterobacteriaceae infections. Emerg Infect Dis. 2014;20(7):1170–1175. doi:10.3201/eid2007.121004
12. Ara-Montojo MF, Escosa-García L, Alguacil-Guillén M, et al. Predictors of mortality and clinical characteristics among carbapenem-resistant or carbapenemase-producing Enterobacteriaceae bloodstream infections in Spanish children. J Antimicrob Chemother. 2021;76(1):220–225. doi:10.1093/jac/dkaa397
13. Trecarichi EM, Pagano L, Martino B, et al. Bloodstream infections caused by Klebsiella pneumoniae in onco-hematological patients: clinical impact of carbapenem resistance in a multicentre prospective survey. Am J Hematol. 2016;91(11):1076–1081. doi:10.1002/ajh.24489
14. Lou T, Du X, Zhang P, et al. Risk factors for infection and mortality caused by carbapenem-resistant Klebsiella pneumoniae: a large multicentre case–control and cohort study. J Infect. 2022;84(5):637–647. doi:10.1016/j.jinf.2022.03.010
15. Wu Q, Qian C, Yin H, et al. A novel risk predictive scoring model for predicting subsequent infection after carbapenem-resistant gram-negative bacteria colonization in hematological malignancy patients. Front Oncol. 2022;12:897479. doi:10.3389/fonc.2022.897479
16. (CLSI) CaLSI. Performance Standards for Antimicrobial Susceptibility Testing: Twenty-Four Informational Supplement. (CLSI) CaLSI; 2020.
17. Åkerlund A, Jonasson E, Matuschek E, Serrander L, Sundqvist M, Kahlmeter G. EUCAST rapid antimicrobial susceptibility testing (RAST) in blood cultures: validation in 55 European laboratories. J Antimicrob Chemother. 2020;75(11):3230–3238. doi:10.1093/jac/dkaa333
18. Russell JA. Management of sepsis. N Engl J Med. 2006;355(16):1699–1713. doi:10.1056/NEJMra043632
19. Zhou C, Jin L, Wang Q, et al. Bloodstream infections caused by carbapenem-resistant enterobacterales: risk factors for mortality, antimicrobial therapy and treatment outcomes from a prospective multicenter study. Infect Drug Resist. 2021;14:731–742. doi:10.2147/idr.S294282
20. Satlin MJ, Cohen N, Ma KC, et al. Bacteremia due to carbapenem-resistant Enterobacteriaceae in neutropenic patients with hematologic malignancies. J Infect. 2016;73(4):336–345. doi:10.1016/j.jinf.2016.07.002
21. Li C, Li Y, Zhao Z, Liu Q, Li B. Treatment options and clinical outcomes for carbapenem-resistant Enterobacteriaceae bloodstream infection in a Chinese university hospital. J Infect Public Health. 2019;12(1):26–31. doi:10.1016/j.jiph.2018.08.002
22. Vinker-Shuster M, Stepensky P, Temper V, Shayovitz V, Masarwa R, Averbuch D. Gram-negative bacteremia in children with hematologic malignancies and following hematopoietic stem cell transplantation: epidemiology, resistance, and outcome. J Pediatr Hematol Oncol. 2019;41(8):e493–e498. doi:10.1097/mph.0000000000001556
23. Diallo K, Thilly N, Luc A, et al. Management of bloodstream infections by infection specialists: an international ESCMID cross-sectional survey. Int J Antimicrob Agents. 2018;51(5):794–798. doi:10.1016/j.ijantimicag.2017.12.010
24. Rac H, Gould AP, Bookstaver PB, Justo JA, Kohn J, Al-Hasan MN. Evaluation of early clinical failure criteria for gram-negative bloodstream infections. Clin Microbiol Infect. 2020;26(1):73–77. doi:10.1016/j.cmi.2019.05.017
25. Tumbarello M, Viale P, Viscoli C, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy. Clin Infect Dis. 2012;55(7):943–950. doi:10.1093/cid/cis588
26. Martin A, Fahrbach K, Zhao Q, Lodise T. Association between carbapenem resistance and mortality among adult, hospitalized patients with serious infections due to Enterobacteriaceae: results of a systematic literature review and meta-analysis. Open Forum Infect Dis. 2018;5(7):ofy150. doi:10.1093/ofid/ofy150
27. Reinhart K, Bauer M, Riedemann NC, Hartog CS. New approaches to sepsis: molecular diagnostics and biomarkers. Clin Microbiol Rev. 2012;25(4):609–634. doi:10.1128/cmr.00016-12
28. Póvoa P, Coelho L, Almeida E, et al. Early identification of intensive care unit-acquired infections with daily monitoring of C-reactive protein: a prospective observational study. Crit Care. 2006;10(2):R63. doi:10.1186/cc4892
29. Philip AGS, Mills PC. Use of C-reactive protein in minimizing antibiotic exposure: experience with infants initially admitted to a well-baby nursery. Pediatrics. 2000;106(1):E4. doi:10.1542/peds.106.1.e4
30. Prat C, Sancho JM, Dominguez J, et al. Evaluation of procalcitonin, neopterin, C-reactive protein, IL-6 and IL-8 as a diagnostic marker of infection in patients with febrile neutropenia. Leuk Lymphoma. 2008;49(9):1752–1761. doi:10.1080/10428190802258956
31. McMillan DC, Watson WS, O’Gorman P, Preston T, Scott HR, McArdle CS. Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr Cancer. 2001;39(2):210–213. doi:10.1207/S15327914nc392_8
32. Fairclough E, Cairns E, Hamilton J, Kelly C. Evaluation of a modified early warning system for acute medical admissions and comparison with C-reactive protein/albumin ratio as a predictor of patient outcome. Clin Med. 2009;9(1):30–33. doi:10.7861/clinmedicine.9-1-30
33. Wang Y, Lin Q, Chen Z, et al. Construction of a risk prediction model for subsequent bloodstream infection in intestinal carriers of carbapenem-resistant Enterobacteriaceae: a retrospective study in hematology department and intensive care unit. Infect Drug Resist. 2021;14:815–824. doi:10.2147/idr.S286401
34. Ishizuka M, Nagata H, Takagi K, Iwasaki Y, Shibuya N, Kubota K. Clinical significance of the C-reactive protein to albumin ratio for survival after surgery for colorectal cancer. Ann Surg Oncol. 2016;23(3):900–907. doi:10.1245/s10434-015-4948-7
35. Zhang W, Liu K, Ye B, Liang W, Ren Y. Pretreatment C-reactive protein/albumin ratio is associated with poor survival in patients with stage IB-IIA cervical cancer. Cancer Med. 2018;7(1):105–113. doi:10.1002/cam4.1270
36. Tang H-N, Pan B-H, Wang L, et al. C-reactive protein-to-albumin ratio is an independent poor prognostic factor in newly diagnosed chronic lymphocytic leukaemia: a clinical analysis of 322 cases. Transl Oncol. 2021;14(4):101035. doi:10.1016/j.tranon.2021.101035
37. Ranzani OT, Zampieri FG, Forte DN, Azevedo LCP, Park M, Salluh JIF. C-reactive protein/albumin ratio predicts 90-day mortality of septic patients. PLoS One. 2013;8(3):e59321. doi:10.1371/journal.pone.0059321
38. Kim MH, Ahn JY, Song JE, et al. The C-reactive protein/albumin ratio as an independent predictor of mortality in patients with severe sepsis or septic shock treated with early goal-directed therapy. PLoS One. 2015;10(7):e0132109. doi:10.1371/journal.pone.0132109
39. Katip W, Uitrakul S, Oberdorfer P. Short-course versus long-course colistin for treatment of carbapenem-resistant A. baumannii in cancer patient. Antibiotics. 2021;10(5):484. doi:10.3390/antibiotics10050484
40. Seymour CW, Gesten F, Prescott HC, et al. Time to treatment and mortality during mandated emergency care for sepsis. N Engl J Med. 2017;376(23):2235–2244. doi:10.1056/NEJMoa1703058
41. Bernhard M, Lichtenstern C, Eckmann C, Weigand MA. The early antibiotic therapy in septic patients - milestone or sticking point? Crit Care. 2014;18(6):671. doi:10.1186/s13054-014-0671-1
42. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi:10.1097/01.Ccm.0000217961.75225.E9
43. Ferrer R, Artigas A, Suarez D, et al. Effectiveness of treatments for severe sepsis: a prospective, multicenter, observational study. Am J Respir Crit Care Med. 2009;180(9):861–866. doi:10.1164/rccm.200812-1912OC
44. Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi:10.1097/ccm.0000000000000330
45. Falcone M, Bassetti M, Tiseo G, et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae. Crit Care. 2020;24(1):29. doi:10.1186/s13054-020-2742-9
46. Verroken A, Defourny L, Le Polain De Waroux O, et al. Clinical impact of MALDI-TOF MS identification and rapid susceptibility testing on adequate antimicrobial treatment in sepsis with positive blood cultures. PLoS One. 2016;11(5):e0156299. doi:10.1371/journal.pone.0156299
47. Kumar A, Zarychanski R, Light B, et al. Early combination antibiotic therapy yields improved survival compared with monotherapy in septic shock: a propensity-matched analysis. Crit Care Med. 2010;38(9):1773–1785. doi:10.1097/CCM.0b013e3181eb3ccd
48. Vallés J, Rello J, Ochagavía A, Garnacho J, Alcalá MA. Community-acquired bloodstream infection in critically ill adult patients: impact of shock and inappropriate antibiotic therapy on survival. Chest. 2003;123(5):1615–1624. doi:10.1378/chest.123.5.1615
49. Seo H, Lee SC, Chung H, et al. Clinical and microbiological analysis of risk factors for mortality in patients with carbapenem-resistant Enterobacteriaceae bacteremia. Int J Antimicrob Agents. 2020;56(4):106126. doi:10.1016/j.ijantimicag.2020.106126
50. Chinese Society of Hematology CM, Chinese Hematology Association, Chinese Medical Doctor Association. 血液肿瘤患者碳青霉烯类耐药的肠杆菌科细菌(CRE)感染的诊治与防控中国专家共识(2020年版) [Management of Carbapenem-resistant Enterobacteriaceae (CRE) infection in patients with hematological malignancies: Chinese consensus (2020)]. Zhonghua Xue Ye Xue Za Zhi. 2020;41(11):881–889. Chinese. doi:10.3760/cma.j.issn.0253-2727.2020.11.001
51. Livermore DM. Tigecycline: what is it, and where should it be used? J Antimicrob Chemother. 2005;56(4):611–614. doi:10.1093/jac/dki291
52. Doan T-L, Fung HB, Mehta D, Riska PF. Tigecycline: a glycylcycline antimicrobial agent. Clin Ther. 2006;28(8):1079–1106. doi:10.1016/j.clinthera.2006.08.011
53. Yaghoubi S, Zekiy AO, Krutova M, et al. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. Eur J Clin Microbiol Infect Dis. 2022;41(7):1003–1022. doi:10.1007/s10096-020-04121-1
54. Stein GE, Babinchak T. Tigecycline: an update. Diagn Microbiol Infect Dis. 2013;75(4):331–336. doi:10.1016/j.diagmicrobio.2012.12.004
55. Vasilev K, Reshedko G, Orasan R, et al. A Phase 3, open-label, non-comparative study of tigecycline in the treatment of patients with selected serious infections due to resistant Gram-negative organisms including Enterobacter species, Acinetobacter baumannii and Klebsiella pneumoniae. J Antimicrob Chemother. 2008;62(Suppl Supplement 1):i29–i40. doi:10.1093/jac/dkn249
56. Yahav D, Lador A, Paul M, Leibovici L. Efficacy and safety of tigecycline: a systematic review and meta-analysis. J Antimicrob Chemother. 2011;66(9):1963–1971. doi:10.1093/jac/dkr242
57. Cai Y, Wang R, Liang B, Bai N, Liu Y. Systematic review and meta-analysis of the effectiveness and safety of tigecycline for treatment of infectious disease. Antimicrob Agents Chemother. 2011;55(3):1162–1172. doi:10.1128/aac.01402-10
58. McGovern PC, Wible M, El-Tahtawy A, Biswas P, Meyer RD. All-cause mortality imbalance in the tigecycline phase 3 and 4 clinical trials. Int J Antimicrob Agents. 2013;41(5):463–467. doi:10.1016/j.ijantimicag.2013.01.020
59. Tasina E, Haidich A-B, Kokkali S, Arvanitidou M. Efficacy and safety of tigecycline for the treatment of infectious diseases: a meta-analysis. Lancet Infect Dis. 2011;11(11):834–844. doi:10.1016/S1473-3099(11)70177-3
60. Hung WY, Kogelman L, Volpe G, Iafrati M, Davidson L. Tigecycline-induced acute pancreatitis: case report and literature review. Int J Antimicrob Agents. 2009;34(5):486–489. doi:10.1016/j.ijantimicag.2009.05.004
61. Yahav D, Farbman L, Leibovici L, Paul M. Colistin: new lessons on an old antibiotic. Clin Microbiol Infect. 2012;18(1):18–29. doi:10.1111/j.1469-0691.2011.03734.x
62. Falagas ME, Kasiakou SK, Saravolatz LD. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clin Infect Dis. 2005;40(9):1333–1341. doi:10.1086/429323
63. Gough M, Hancock RE, Kelly NM. Antiendotoxin activity of cationic peptide antimicrobial agents. Infect Immun. 1996;64(12):4922–4927. doi:10.1128/iai.64.12.4922-4927.1996
64. Avedissian SN, Liu J, Rhodes NJ, et al. A Review of the Clinical Pharmacokinetics of Polymyxin B. Antibiotics. 2019;8(1):31. doi:10.3390/antibiotics8010031
65. Liang Q, Huang M, Xu Z. Early use of polymyxin B reduces the mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection. Braz J Infect Dis. 2019;23(1):60–65. doi:10.1016/j.bjid.2018.12.004
66. Cruz DN, Perazella MA, Bellomo R, et al. Effectiveness of polymyxin B-immobilized fiber column in sepsis: a systematic review. Crit Care. 2007;11(2):1–12. doi:10.1186/cc5780
67. Katip W, Oberdorfer P. Clinical efficacy and nephrotoxicity of colistin alone versus colistin plus vancomycin in critically ill patients infected with carbapenem-resistant Acinetobacter baumannii: a propensity score-matched analysis. Pharmaceutics. 2021;13(2):162. doi:10.3390/pharmaceutics13020162
68. Katip W, Uitrakul S, Oberdorfer P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: a Propensity Score-Matched Analysis. Antibiotics. 2020;9(10):647. doi:10.3390/antibiotics9100647
69. Katip W, Oberdorfer P, Kasatpibal N. Effectiveness and nephrotoxicity of loading dose colistin–meropenem versus loading dose Colistin–Imipenem in the treatment of carbapenem-resistant Acinetobacter baumannii infection. Pharmaceutics. 2022;14(6):1266. doi:10.3390/pharmaceutics14061266
70. Katip W, Uitrakul S, Oberdorfer P. Clinical efficacy and nephrotoxicity of the loading dose colistin for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients. Pharmaceutics. 2021;14(1):31. doi:10.3390/pharmaceutics14010031
71. Bush K. A resurgence of β-lactamase inhibitor combinations effective against multidrug-resistant Gram-negative pathogens. Int J Antimicrob Agents. 2015;46(5):483–493. doi:10.1016/j.ijantimicag.2015.08.011
72. van Duin D, Lok JJ, Earley M, et al. Colistin versus Ceftazidime-Avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae. Clin Infect Dis. 2018;66(2):163–171. doi:10.1093/cid/cix783
73. Pazzini C, Ahmad-Nejad P, Ghebremedhin B. Ceftolozane/tazobactam susceptibility testing in extended-spectrum betalactamase- and carbapenemase-producing gram-negative bacteria of various clonal lineages. Eur J Microbiol Immunol. 2019;9(1):1–4. doi:10.1556/1886.2019.00001
74. Vasques MRG, Bello AR, Da Cruz Lamas C, Correa J, Pereira JAA. β-lactamase producing enterobacteria isolated from surveillance swabs of patients in a cardiac intensive care unit in Rio de Janeiro, Brazil. Braz J Infect Dise. 2011;15(1):28–33.
75. Bassetti M, Ginocchio F, Mikulska M, Taramasso L, Giacobbe DR. Will new antimicrobials overcome resistance among Gram-negatives? Expert Rev Anti Infect Ther. 2011;9(10):909–922. doi:10.1586/eri.11.107
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.