")
Back to Journals » OncoTargets and Therapy » Volume 15
A Unique Three-Way Variant Philadelphia Chromosome t(6;9;22)(p21.3;q34;q11.2) in a Newly Diagnosed Patient with Chronic Myeloid Leukemia Responded to Flumatinib
Authors Chen L, Zhang J , Yang N, Tan N, Meng D, Zhang F, Qi Y, Wu G, Li Z
Received 4 June 2022
Accepted for publication 30 August 2022
Published 20 September 2022 Volume 2022:15 Pages 1033—1037
DOI https://doi.org/10.2147/OTT.S377342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Lili Chen,1 Junling Zhang,2 Na Yang,1 Ningping Tan,1 Di Meng,1 Fei Zhang,1 Yuyang Qi,1 Guangqi Wu,1 Zhenyu Li3
1Department of Hematology, The Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, People’s Republic of China; 2The Medical Department, 3D Medicines Inc., Shanghai, People’s Republic of China; 3Department of Hematology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, People’s Republic of China
Correspondence: Zhenyu Li, Department of Hematology, The Affiliated Hospital of Xuzhou Medical University, Xuzhou, 221002, People’s Republic of China, Email [email protected] Guangqi Wu, Department of Hematology, The Affiliated Suqian Hospital of Xuzhou Medical University, Suqian, 223800, People’s Republic of China, Email [email protected]
Background: Chronic myeloid leukaemia (CML) is a clonal malignant disorder of a pluripotent hematopoetic stem cell characterized by the presence of Philadelphia (Ph) chromosome in more than 90% of patients. However, about 5– 10% of CML patients show a variant Ph translocation, involving one or more chromosomes in addition to 9 and 22. The treatment and prognostic impact of such additional abnormalities is not known. Herein, we report a unique case of a three-way translocation variant in CML and responded to flumatinib.
Case Presentation: A 22-year-old Asian female who presented with leukocytosis was diagnosed with CML. Cytogenetic karyotyping analysis showed 46,XX,t(6;9;22)(p21.3;q34;q11.2). She was treated with flumatinib, and MR5.0 (BCR-ABL1 IS≤ 0.001%, international scale) was achieved after three months of continuous treatment.
Conclusion: This was the 5th case of t(6;9;22), in particular, a new variant Ph translocation, and the first successful case treated with flumatinib in the world.
Keywords: t(6;9;22)(p21.3;q34;q11.2), CML, Philadelphia chromosome, flumatinib, case report
Introduction
Chronic myeloid leukemia (CML) is a malignant tumor formed by clonal proliferation of pluripotent hematopoietic stem cells, which accounts for about 15% of adult leukemia.1 It is characterized by the presence of a translocation between chromosomes 9 and 22, t(9;22)(q34;q11), known as the Philadelphia (Ph) chromosome, leads to the generation of BCR-ABL oncogenic fusion gene.2 The gene encodes a chimeric BCR-ABL protein with constitutive kinase activity, which affects the proliferation and apoptosis of bone marrow cells.3 Although more than 90% of CML patients are associated with typical t(9; 22)(q34; q11), but about 5–8% of newly diagnosed CML patients are associated with complex variant Ph (vPh) chromosome, involving one or more chromosomes in addition to 9 and 22.4 The mechanism of vPh chromosome translocations generation and its effect on prognosis is unclear, but may further classify CML in specific subsets requiring different therapeutic approaches. However, some previous studies have suggested that CML patients with vPh chromosome may have a worse prognosis than patients with typical translocations, including 3 cases with CML with three-way complex vPh t(6;9;22) chromosome translocations.5–8
For CML patients with Ph chromosome-positive and BCR-ABL1-positive, the emergence of tyrosine kinase inhibitors (TKIs) such as imatinib significantly improved the prognosis of patients.9 However, CML was associated with vPh t(6;9;22) whether patients could benefit from other TKI therapy has not been reported. Herein, we report a unique case of a three-way vPh chromosome translocation in CML and responded to flumatinib.
Case Presentation
A 22-year-old female patient presented to a local hospital in August 2020 due to left abdominal distention and discomfort. Color ultrasound of abdomen showed splenomegaly (thickness: 57mm). Hematological analysis revealed white blood cell (WBC) was 330.08×109/L, neutrophils 295.65×109/L, lymphocytes 8.24×109/L, eosinophils 2.07×109/L, basophils 14.30×109/L, a hemoglobin level of 84 g/L, and platelet count of 229×109/L. Peripheral blood smear showed 3.0% lymphocytes, 0.5% monocytes, 1.0% eosinophils, 4.0% basophils, 4.0% promyelocytes, 20.0% mesogranulocyte, and 15.0% metamyelocytes, 48% band granulocyte, 5% segmented neutrocyte. In addition, the nucleated red cells were 2 per 100 cells (Figure 1). Aspartate aminotransferase is 47.5U/L, lactate dehydrogenase is 1903.3U/L. Genetic analysis results indicated that no obvious mutations on JAK-2 V617F, CALR, and MPL were observed. Cytogenetic analysis was performed utilizing bone marrow culture cells, and all analyzed cells showed a complex, three-way t(6;9;22)(p21.3;q34;q11.2) Ph chromosome translocation (Figure 2). Therefore, she was diagnosed with CML-CP, and her Sokal and EUTOS long-term survival (ELTS) score were 0.59 (low risk) and 1.577 (low risk), respectively.
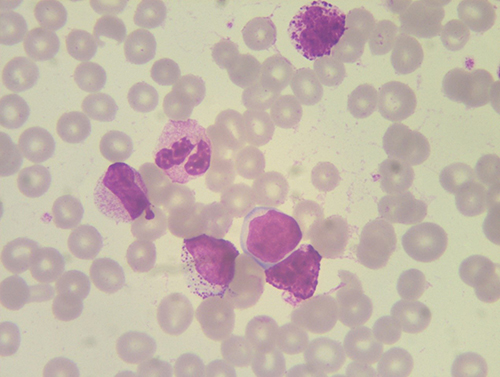 |
Figure 1 Peripheral blood smear result. |
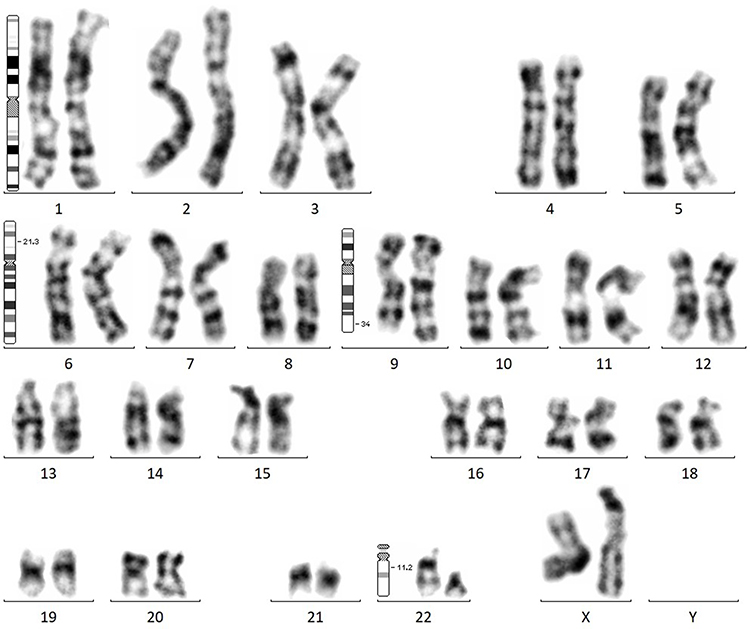 |
Figure 2 Cytogenetic analysis shows a variant three-way translocation 46,XX,t(6;9;22)(p21.3;q34;q11.2). |
Initially, she was treated with orally administered hydroxyurea at a daily dose of 1.0g bid on August 6, 2020. However, during the course of treatment, the WBC count dropped to 18×109/L. Therefore, hydroxyurea was discontinued, and flumatinib at a daily dose of 600 mg was administered on August 14, 2020. Her BCR-ABL/ABL international scale (IS) levels at 3, 6, 9 and 12 months were 0.249%, 0.000%, 0.000% and 0.000%, respectively. Molecular response (MR) of BCR-ABL1 gene was assessed by RT-PCR using ABL gene as reference gene in our central laboratory. Blood counts were measured during treatment. Three months after flumatinib treatment, molecular remission 5 (MR5) (BCR-ABL/ABL ≤ 0.001% IS) was achieved, and complete MR (CMR) remained until December 2021. Blood counts were normal (Table 1).
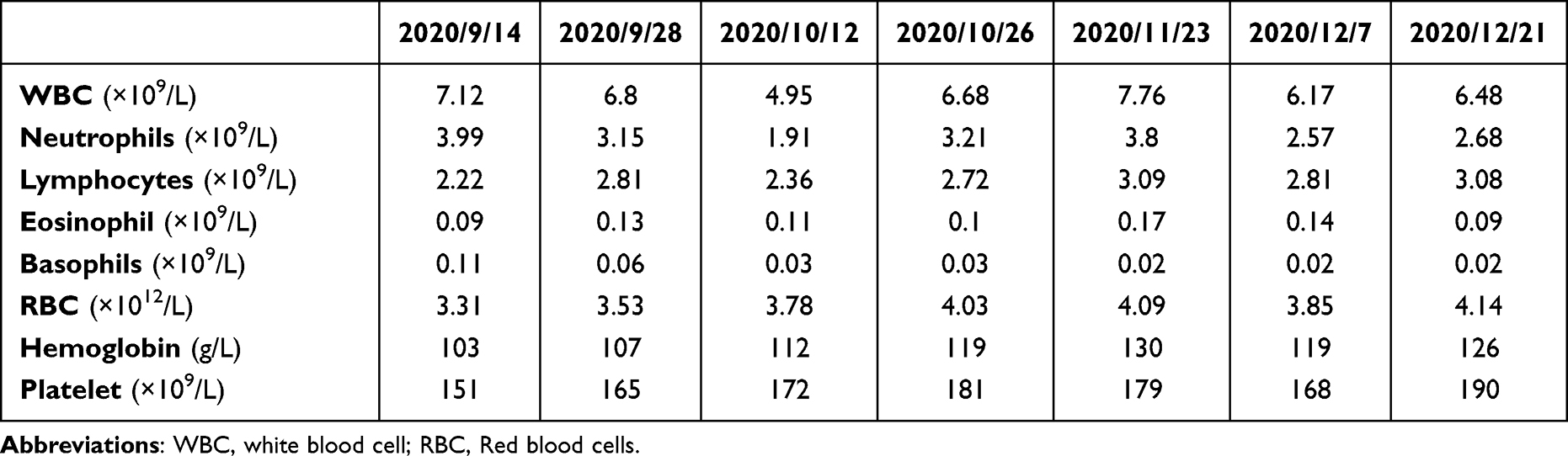 |
Table 1 The Hematological Analysis Result of the Patient During the Therapy |
Discussion
CML was associated with clone stem cell syndrome, and cytogenetic abnormality was acquired abnormality. Ph chromosomes, presented in more than 90% of cases, were later responsible for the production of the protein BCR-ABL gene fusion. More importantly, this fusion gene would interfere with WBC and weaken the immune system.10 However, 5–8% of CML patients’ present variant and complex translocation, in addition to chromosomes 9 and 22, known as vPh. Despite the genetically heterogeneous nature of these alterations, available data indicate that CML patients displaying complex variant translocations do not exhibit a less favorable outcome as compared to individuals presenting conventional Ph-positive CML.11 Di Raimondo et al found that two CML patients with complex variant translocations achieved an optimal response to tyrosine kinase inhibitors (TKI) treatment.12 In a retrospective study, 693 CML chromosomes were identified by conventional and molecular cytogenetics, of which 5% (32/693) had vPh chromosomes, and the most common variation was t(1;9;22) (p36;q34;q11.2), t(1;9;22)(q21;q34;q11.2), t(2;9;22)(p13;q34;q11.2), t(5;9,22)(q31;q34;q11.2), t(5;9;22)(q35;q34;q11,2), t(9;22;11)(q34;q11.2;q13), t(9;22;12)(q34;q11.2;p13) and t(9;22;15)(q34;q11.2;q22).13
The clinical significance and mechanism of vPh chromosome formation were still not clear. Some researchers predict a one-step mechanism, while others predict a two-step or multi-step mechanism.14 However, existing results suggested that the vPh translocation in CML patients may affect the response to imatinib treatment, thereby affecting the prognosis of patients.15 At the same time, the proportion of patients with vPh translocation CML in accelerated phase was higher than that of patients with classical translocation CML (56% vs 38%).16 Various side effects have been reported in patients treated with imatinib.17 Therefore, how to choose treatment for patients with complex karyotypes is a pain point in clinical treatment. At the same time, these patients may need to be closely monitored for treatment side effects and disease progression.
Flumatinib, a novel oral BCR-ABL1 TKI currently marketed in China, has better efficacy than imatinib in the treatment of newly diagnosed chronic phase CML. In the FESTnd study, the rate of major molecular response at 6 months and 12 months was significantly higher with flumatinib than with imatinib (33.7% vs 18.3%; P = 0.0006; 52.6% vs 39.6%; P = 0.0102, respectively). At 3 months, the rate of early molecular response was also significantly higher in patients receiving flumatinib than in those receiving imatinib (82.1% vs 53.3%; P < 0.0001). More patients receiving flumatinib achieved MR4 at 6, 9, and 12 months (8.7% vs 3.6%, P = 0.0358; 16.8% vs 5.1%, P = 0.0002; and 23.0% vs 11.7%, P = 0.0034, respectively). No patients had progression to accelerated phase or blast crisis in the flumatinib group vs 4 patients in the imatinib group by 12 months.18 Whether flumatinib is effective in CML patients with vPh chromosomes has not been reported in the literature.
In the present study, we report the first case of a complex three-way vPh chromosome t(6;9;22)(p21.3;q34;q11.2) successfully treated with flumatinib, which has not been described previously. This case provides a broader treatment for CML patients with vPh chromosomes, but whether it is effective for more complex vPh chromosomes needs to be verified by prospective clinical studies, and further explore the mechanism of vPh occurrence.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of The Affiliated Suqian Hospital of Xuzhou Medical University.
Consent for Publication
The patient provided written informed consent for the case details to be published.
Funding
There is no funding to report.
Disclosure
Junling Zhang is employee of 3D Medicines Inc. The authors report no other conflicts of interest in this work.
References
1. Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am J Hematol. 2020;95(6):691–709. doi:10.1002/ajh.25792
2. Minciacchi VR, Kumar R, Krause DS. Chronic myeloid leukemia: a model disease of the past, present and future. Cells. 2021;10(1):117. doi:10.3390/cells10010117
3. Manzella L, Tirrò E, Pennisi MS, et al. Roles of interferon regulatory factors in chronic myeloid leukemia. Curr Cancer Drug Targets. 2016;16(7):594–605. doi:10.2174/1568009616666160105105857
4. Gao L, Ren MQ, Tian ZG, et al. Management of chronic myeloid leukemia presenting with isolated thrombocytosis and complex Philadelphia chromosome: a case report. Medicine. 2021;100(35):e27134. doi:10.1097/MD.0000000000027134
5. Fabarius A, Leitner A, Hochhaus A, et al. Impact of additional cytogenetic aberrations at diagnosis on prognosis of CML: long-term observation of 1151 patients from the randomized CML Study IV. Blood. 2011;118(26):6760–6768. doi:10.1182/blood-2011-08-373902
6. Orciuolo E, Buda G, Galimberti S, et al. Complex translocation t(6;9;22)(p21.1;q34;q11) at diagnosis is a therapy resistance index in chronic myeloid leukaemia. Leuk Res. 2008;32(1):190–191. doi:10.1016/j.leukres.2007.02.001
7. Ciftciler R, Saglam EA, Inanc A, et al. A unique case of complex variant translocation of t(6;9;22)(p22;q34;q11.2), der(19) in a newly diagnosed patient with chronic myeloid leukemia. Cancer Genet. 2019;237:78–81. doi:10.1016/j.cancergen.2019.06.008
8. Asif M, Hussain A, Wali A, et al. A rare case of three-way complex variant translocation in chronic myeloid leukemia t(6;9;22)(p21;q34;q11): a case report. Biomed Rep. 2017;7(4):377–379. doi:10.3892/br.2017.967
9. O’Brien SG, Guilhot F, Larson RA, et al. Imatinib compared with interferon and low-dose cytarabine for newly diagnosed chronic-phase chronic myeloid leukemia. N Engl J Med. 2003;348(11):994–1004. doi:10.1056/NEJMoa022457
10. Zangari M, Anaissie E, Stopeck A, et al. Phase II study of SU5416, a small molecule vascular endothelial growth factor tyrosine kinase receptor inhibitor, in patients with refractory multiple myeloma. Clin Cancer Res. 2004;10:88–95. doi:10.1158/1078-0432.ccr-0221-3
11. Richebourg S, Eclache V, Perot C, et al. Mechanisms of genesis of variant translocation in chronic myeloid leukemia are not correlated with ABL1 or BCR deletion status or response to imatinib therapy. Cancer Genet Cytogenet. 2008;182:95–102. doi:10.1016/j.cancergencyto.2008.01.005
12. Stagno F, Vigneri P, Del Fabro V, et al. Influence of complex variant chromosomal translocations in chronic myeloid leukemia patients treated with tyrosine kinase inhibitors. Acta Oncol. 2010;49(4):506–508. doi:10.3109/02841861003660031
13. Costa D, Grau J, Espinet B, et al. Conventional and molecular cytogenetic studies to characterize 32 complex variant Philadelphia translocations in patients with chronic myeloid leukemia. Oncol Lett. 2019;17(6):5705–5710. doi:10.3892/ol.2019.10245
14. Lee J, Kim DS, Lee HS, et al. A novel t(9;22;11) translocation involving 11q24 in a patient with chronic myeloid leukemia: a case report. Oncol Lett. 2017;13(3):1711–1713. doi:10.3892/ol.2017.5668
15. Marzocchi G, Castagnetti F, Luatti S, et al. Variant Philadelphia translocations: molecular-cytogenetic characterization and prognostic influence on frontline imatinib therapy, a GIMEMA working party on CML analysis. Blood. 2011;117(25):6793–6800. doi:10.1182/blood-2011-01-328294
16. El-Zimaity MM, Kantarjian H, Talpaz M, et al. Results of imatinib mesylate therapy in chronic myelogenous leukaemia with variant Philadelphia chromosome. Br J Haematol. 2004;125(2):187–195. doi:10.1111/j.1365-2141.2004.04899.x
17. Malkan UY, Haznedaroglu IC. Discontinuation of imatinib mesylate could improve renal impairment in chronic myeloid leukemia. Open Med. 2018;14:22–24. doi:10.1515/med-2019-0004
18. Zhang L, Meng L, Liu B, et al. Flumatinib versus imatinib for newly diagnosed chronic phase chronic myeloid leukemia: a phase III, randomized, open-label, multi-center FESTnd study. Clin Cancer Res. 2021;27(1):70–77. doi:10.1158/1078-0432.CCR-20-1600
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.